Back to Journals » Nature and Science of Sleep » Volume 17

Inflammation in Obstructive Sleep Apnea: A Global Bibliometric Perspective
Authors Fan H, Niu H ![]() , Zhao B, Gao X
, Zhao B, Gao X ![]()
Received 24 July 2025
Accepted for publication 29 August 2025
Published 22 September 2025 Volume 2025:17 Pages 2275—2295
DOI https://doi.org/10.2147/NSS.S554362
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marco Veneruso
Haixia Fan,1,* Huiyan Niu,2,* Bomeng Zhao,2 Xiaoling Gao3
1Department of Sleep Center, First Hospital of Shanxi Medical University, Taiyuan, Shanxi Province, People’s Republic of China; 2Second College of Clinical Medicine, Shanxi Medical University, Taiyuan, Shanxi Province, People’s Republic of China; 3Department of Sleep Center, Second Hospital of Shanxi Medical University, Taiyuan, Shanxi Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaoling Gao, Department of Sleep Center, Second Hospital of Shanxi Medical University, Taiyuan, Shanxi Province, People’s Republic of China, Tel +86 13513607801, Email [email protected]
Purpose: Obstructive sleep apnea (OSA) is increasingly recognized as a systemic disorder in which inflammation plays a pivotal role in its pathophysiology and comorbidities. This study aimed to conduct the first comprehensive bibliometric analysis of global research on inflammation in OSA, in order to map knowledge structures, identify influential contributors, and highlight emerging research trends.
Patients and Methods: Publications related to OSA and inflammation were retrieved from the Web of Science Core Collection (WoSCC) (1996– 2025). After exclusions, 2,075 articles and reviews were analyzed using bibliometric tools including CiteSpace, VOSviewer, and the bibliometrix R package. Citation frequencies, co-citation networks, and collaboration patterns among countries, institutions, authors, and journals were examined.
Results: The number of publications has shown robust growth (annual rate 12.11%). China and the United States were the leading contributors, with Harvard University, the University of Chicago, and Institut National De La Sante Et De La Recherche Medicale (INSERM) among the most productive institutions. Influential authors included Gozal D, Kheirandish-Gozal L, and Khalyfa A. Sleep and Breathing was the most prolific journal, while Circulation and American Journal of Respiratory and Critical Care Medicine were highly co-cited sources. Highly cited works established the link between intermittent hypoxia, systemic inflammation, and cardiovascular/metabolic consequences. Thematic clusters revealed major research focuses on cardiovascular disease, metabolic syndrome, oxidative stress, neuroinflammation (including microglial activation), and therapeutic strategies such as continuous positive airway pressure (CPAP), adenotonsillectomy, and bariatric surgery. Emerging topics included gut microbiota, vitamin D, and neurodegenerative diseases.
Conclusion: Research on inflammation is evolving from mechanistic insights toward clinical management and interdisciplinary exploration. Looking ahead, priority should be given to biomarker discovery and the development of anti-inflammatory therapeutic strategies. These findings provide a roadmap for targeted research and clinical translation in the field of OSA-related inflammation, ultimately improving patient outcomes.
Keywords: obstructive sleep apnea, inflammation, bibliometric analysis, mechanisms, comorbidities, treatment
Introduction
Obstructive sleep apnea (OSA) is an increasingly common disorder of repeated upper airway collapse during sleep, which leads to oxygen desaturation and disrupted sleep.1 Since the first description of OSA in the 1960s,2 and with further understanding of the pathophysiology of upper airway collapse and the hemodynamic effects of OSA in the 1980s,3 along with the introduction of continuous positive airway pressure (CPAP) as an effective treatment,4 it is estimated that approximately 1 billion adults worldwide may suffer from OSA, with an estimated 425 million individuals having moderate to severe OSA up to now. The most affected population is in China, followed by the United States, Brazil, and India.5 OSA is associated with an increased risk of work-related and traffic accidents, more frequent health-related absenteeism, and a decline in quality of life.6 Therefore, research on OSA is of great significance.
Accumulating evidence supports that OSA is a chronic low-grade inflammatory condition, in which inflammation may play a pivotal role in its pathophysiology, comorbidities, and associated oxidative stress.7 The literature by A.N. Vgontzas indicates that the hypoxic-ischemic response induced by OSA leads to elevated levels of various pro-inflammatory cytokines, such as tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6), which play critical roles in oxidative stress and endothelial dysfunction.8 Takuya Yokoe’s research further shows that inflammatory markers, such as C-reactive protein (CRP) and IL-6, are significantly elevated in OSA patients, and these elevated levels are closely linked to the occurrence of cardiovascular events.9 Therefore, a comprehensive and up-to-date analysis of OSA and its relationship with inflammation is of great importance.
Bibliometric analysis, which makes use of citation data to quantitatively evaluate the spread and influence of scientific works across various sectors within a specific discipline, has become a highly useful approach for analyzing research trends and scholarly contributions.10,11 This method plays a key role in providing a more precise and up-to-date perspective on scientific advancements related to OSA, thereby assisting in evidence-based decision-making and informing the development of research strategies and policies.12 The primary aim of this study was to explore the progression of research on OSA and inflammation in recent decades, employing co-citation network analysis to pinpoint influential studies and identify emerging areas of inquiry. A secondary aim was to comprehensively map the research environment surrounding OSA and inflammation, quantifying the contributions of significant entities such as countries, institutions, authors, and journals. In addition, this analysis intends to uncover existing gaps in research, limitations, and unexplored avenues, providing valuable insights for shaping future research directions and formulating targeted policy measures in the OSA and inflammation field.
Materials and Methods
Database and Search Strategy
The Web of Science Core Collection (WoSCC), a widely used dataset in bibliometrics,13 was retrieved for this study. Searches were performed on April 16, 2025, using terms related to inflammation14 and OSA15,16 in the title (TI), abstract (AB), and author keywords (AK). Detailed search terms are provided in Supplementary Table 1. The initial search yielded 1,294,829 inflammation-related records and 63,736 OSA-related records. Intersecting the two datasets resulted in 2,394 publications. After excluding proceeding papers, corrections, early access articles, news items, book chapters, retractions, reprints, biographical items, book reviews, meeting abstracts, editorial materials, and letters, and restricting to English-language articles and reviews, 2,075 studies remained for analysis (Figure 1).
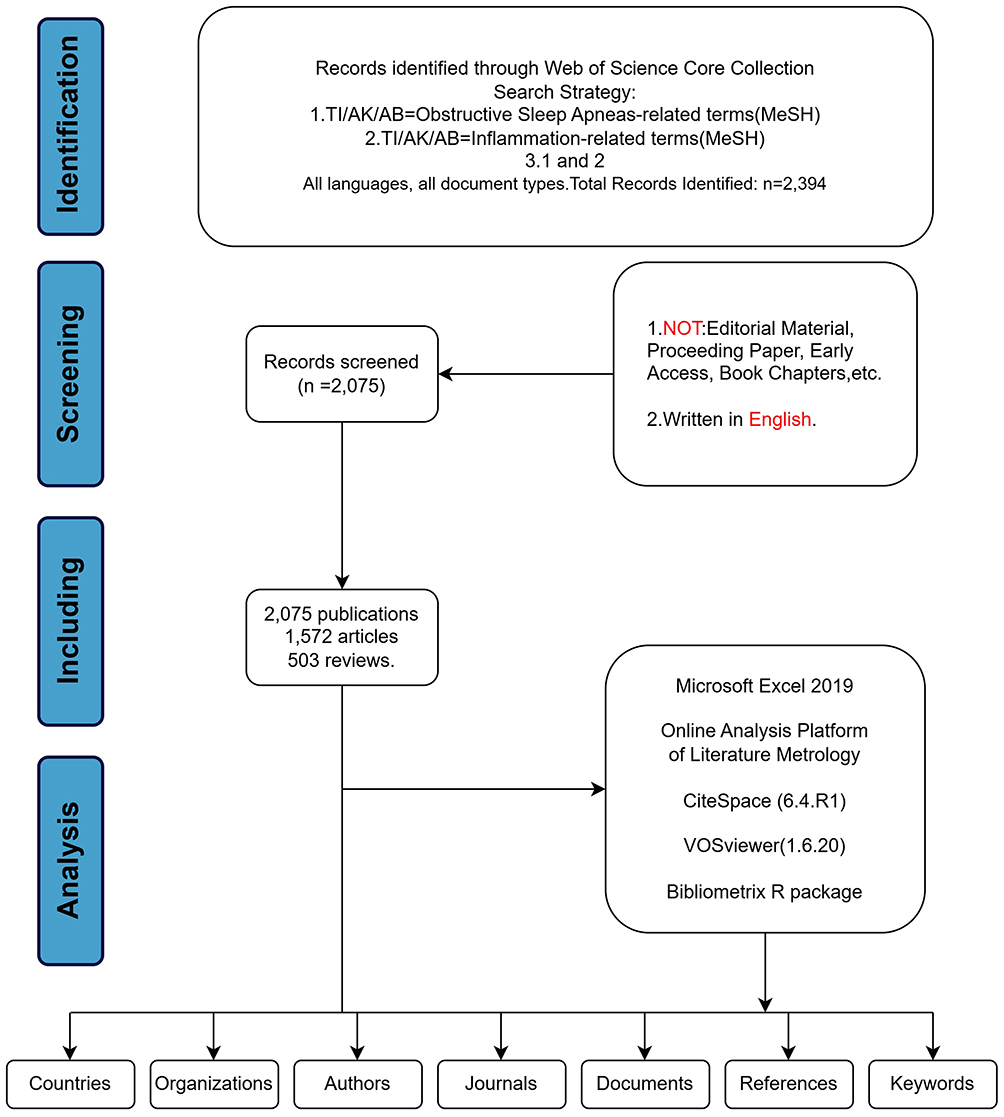 |
Figure 1 Flowchart of Literature Search, Screening, Inclusion, and Analysis. Abbreviations: TI, Title; AK, Author keywords; AB, Abstract. |
Data Processing
The data covered the period from 1 January 1996 to 16 April 2025, with the data segmented into one-year time slices for detailed analysis. All records from the WoSCC were exported as “full records and cited references” in plain text format and Tab format.17 We utilized Microsoft Excel 2019, Online Analysis Platform of Literature Metrology (OALM) (http://bibliometric.com/), CiteSpace (6.4.R1, 64-bit Advanced Edition), VOSviewer (1.6.20), and the bibliometrix R package for network and citation analysis, including the generation of knowledge maps, cluster analysis, network visualization, and historiographic tracking of trends in journals and authors.18 Key metrics such as the g-index,19 h-index,20 number of citations (NC), and number of publications (NP) were also calculated.21
Results
Publication Trends and General Characteristics
Figure 2A displays the annual count of publications and corresponding citations from 1996 to 2025. The number of publications has increased steadily over the years, reaching over 158 by 2024. The number of citations, on the other hand, surged significantly starting in 2005, peaking at nearly 9,000 in 2023 and 2024. Notably, these documents exhibit an impressive annual growth rate of 12.11%, indicating a robust increase in scholarly outputs. The significant decline in the volume of documents in 2025 may be due to the fact that the data only included records up to April 16, 2025. As of the retrieval date, 2,075 papers sourced from 693 different sources were published over the last 40 years. Among them, articles account for the majority. There were 1,572 articles, accounting for 75.76%, and 503 reviews, accounting for 24.24% of the papers (Figure 2B and Supplementary Table 2). Additionally, Figure 2C shows the cumulative number of publications over the study period, depicting an exponential growth trend that is consistent with the general rise in scientific productivity. Figure 2D shows the annual publication count for each country. The stacked bars show how the contributions from each country evolve over time. From 1996 to the early 2000s, the number of publications was relatively low, starting around 2010, there was a sharp rise in publications, indicating a growing research output. By 2020 and beyond, the total number of publications per year reached over 100. Overall, these findings demonstrate a steady growth of research activity with a marked acceleration in the past decade, highlighting the increasing scholarly attention to OSA and inflammation and its emerging significance as a sustained research hotspot.
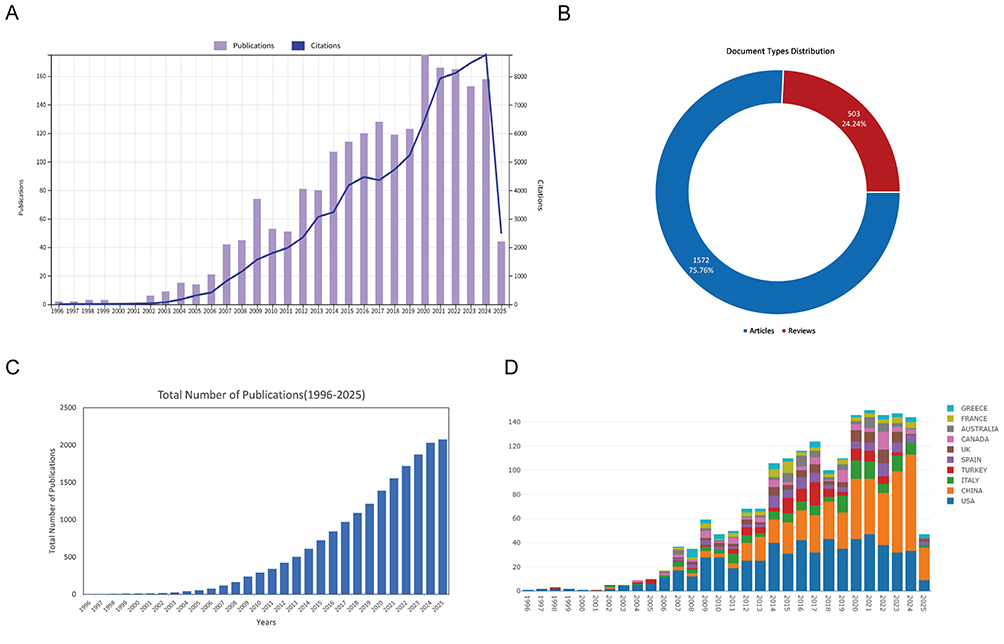 |
Figure 2 Overview of Publications and Citations on Inflammation in Obstructive Sleep Apneas (1996–2025). (A) Annual number of publications (purple bars) and citations (blue line). (B) Distribution of document types, including articles (blue) and reviews (red). (C) Cumulative number of publications from 1996 to 2025. (D) Annual number of publications by country, with different colors representing different countries. |
Collaboration Among Countries/ Regions
Our analysis of WoSCC data reveals that, 2,075 publications originated from 73 countries, highlighting the collaborative nature of research worldwide. The country collaboration map (Figure 3A) illustrates strong international partnerships, particularly between the US, Europe, and Asia, with the US and China standing out as the dominant players. Figure 3B emphasizes the preeminent role of US and China, aligning with the network visualization in Figure 3A. China and the United States are global leaders in academic output. From 1996 to 2025, the two countries published 516 articles (24.6%) and 488 articles (23.5%), far outpacing other countries such as Italy and Turkey, which published 122 articles (15.9%) and 103 articles (5%), respectively (Figure 3C). The analysis of the most cited countries further emphasizes impact, with the US leading in both the number of publications and citations (28,361), followed by China (8,214) and the Canada (4,622) (Figure 3D). The trend toward multi-country collaborations is particularly evident, reflecting a global shift towards more integrated and cross-border research endeavors. Figure 3C distinguishes between single-country publications (SCP) and multiple-country publications (MCP). China has shown remarkable performance in single-country publications, highlighting its strength in both independent research and growing influence in the academic world. The United States dominates in multi-country publications, demonstrating its strength in international collaboration (Supplementary Table 3). In summary, the analysis reveals that China and the United States are not only leading contributors but also key drivers of both independent and collaborative research, underscoring the importance of international partnerships in shaping the global research landscape.
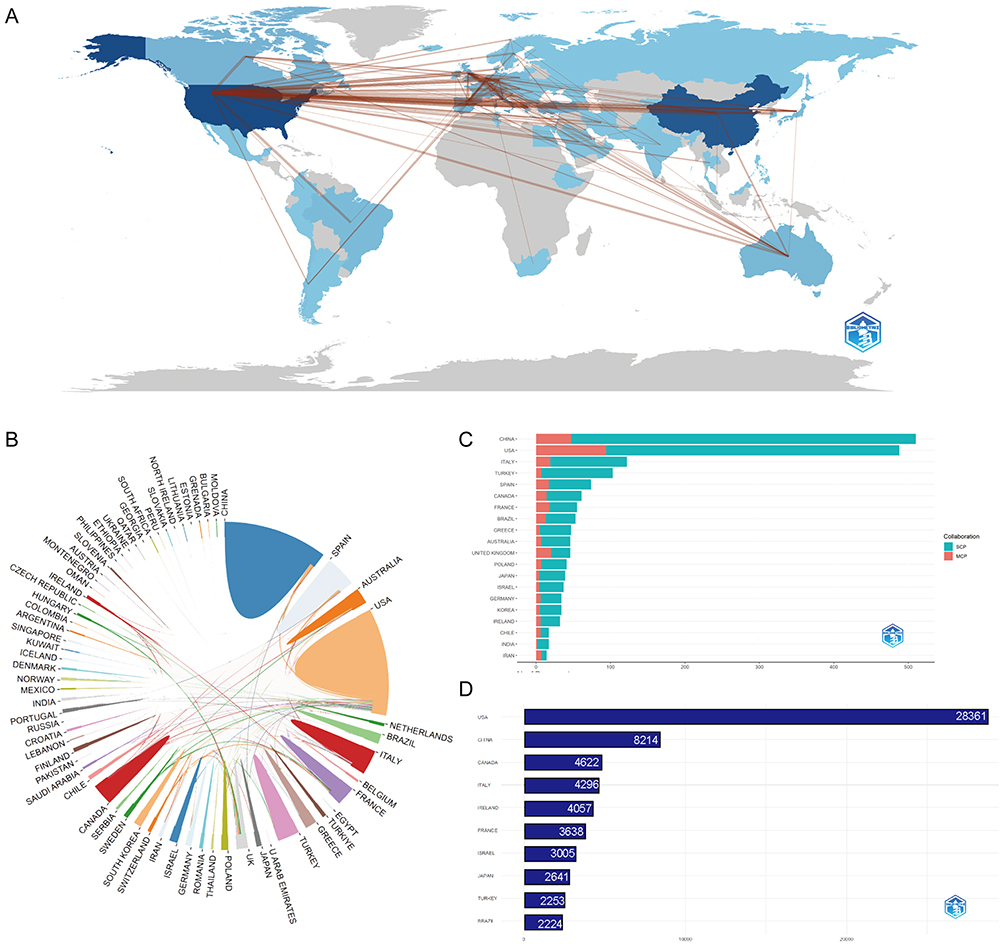 |
Figure 3 Global Trends and Collaboration Networks in Scientific Publications on Inflammation in Obstructive Sleep Apneas. (A) Global collaboration map of co-authorship networks, with darker blue indicating higher publication output and lines representing international collaboration. (B) Circular plot of international collaboration among countries. (C) Top 10 countries by number of publications, classified as single-country publications (SCP, red) or multiple-country publications (MCP, green). (D) Country influence measured by total citation counts. Abbreviations: MCP, Multiple-Country Publications; SCP, Single-Country Publications. |
Institutional Collaboration and Author/Co-Author Networks
In addition to identifying leading institutions, our analysis explores their collaborative networks. Figure 4A highlight the top 5 institutions by research productivity over time: Harvard University (157,7.56%), University of California System (118,5.68%), Harvard University Medical Affiliates (103,4.96%), Chang Gung Memorial Hospital (95,4.57%), Institut National De La Sante Et De La Recherche Medicale (INSERM) (88,4.24%) and University of Chicago (88,4.24%) are tied for fifth place. Figure 4B further reveals a complex interaction network, with Harvard Medical School and the University of Chicago appearing as key nodes, highlighting their pivotal roles in global research collaboration. This collaboration trend is driven by the complex nature of modern scientific challenges, which require diverse expertise, and results in enhanced visibility, citation impact, and interdisciplinary innovation. Notably, European institutions display a stronger tendency toward multi-institutional partnerships, likely driven by European Union research funding policies that encourage international collaboration.
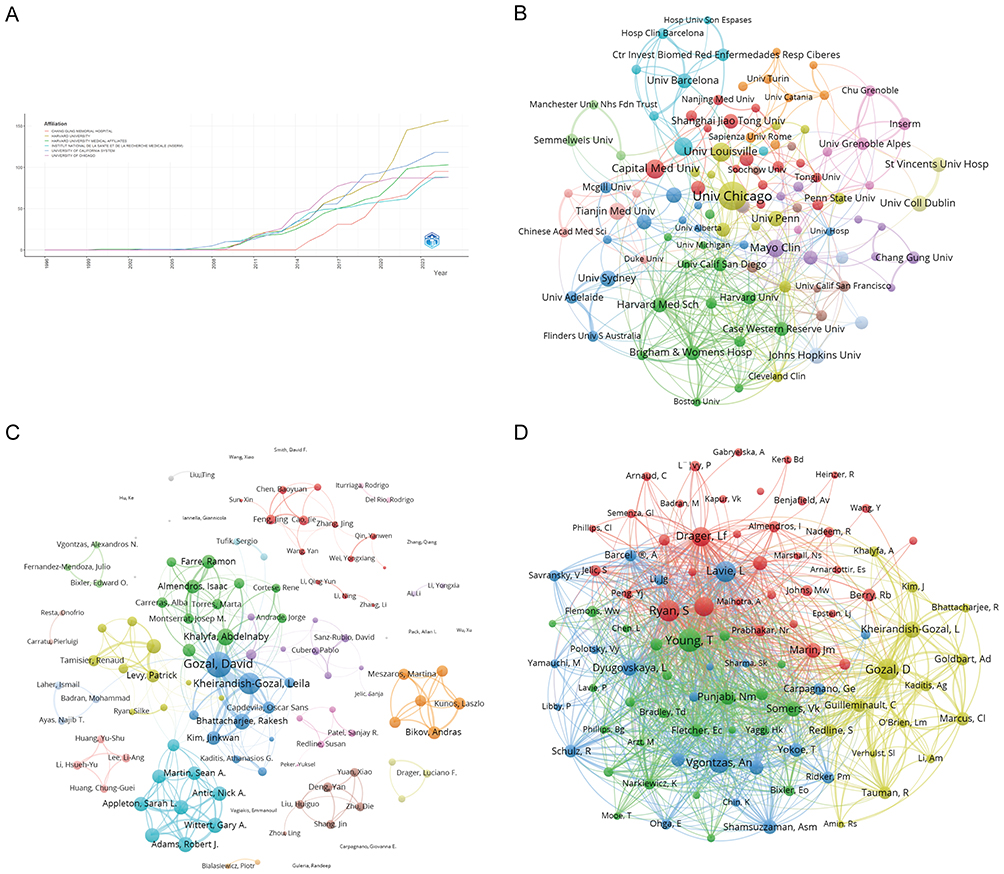 |
Figure 4 Institutional Contributions, Collaboration Networks and Authorship Analyses on Inflammation in Obstructive Sleep Apneas. (A) Institutional publication trends over time. The x-axis represents years, and the y-axis indicates publication counts. (B) Institutional collaboration network, where node size reflects collaboration extent and colors represent institutional clusters. (C) Co-authorship network: nodes represent authors (sized by publication count), and colors indicate collaboration clusters. (D) Co-cited authorship network: nodes represent authors who are frequently cited together; edge thickness reflects co-citation strength, and colors represent research groups. |
The contributions of authors to the academic landscape are substantial, with 9,147 individuals contributing to these documents. Of these, 52 authors have produced single-authored works, resulting in a total of 66 single-authored documents. Collaboration is prominent, as evidenced by an average of 6.45 co-authors per document and 18.51% of documents involving international co-authorship (Supplementary Table 2).
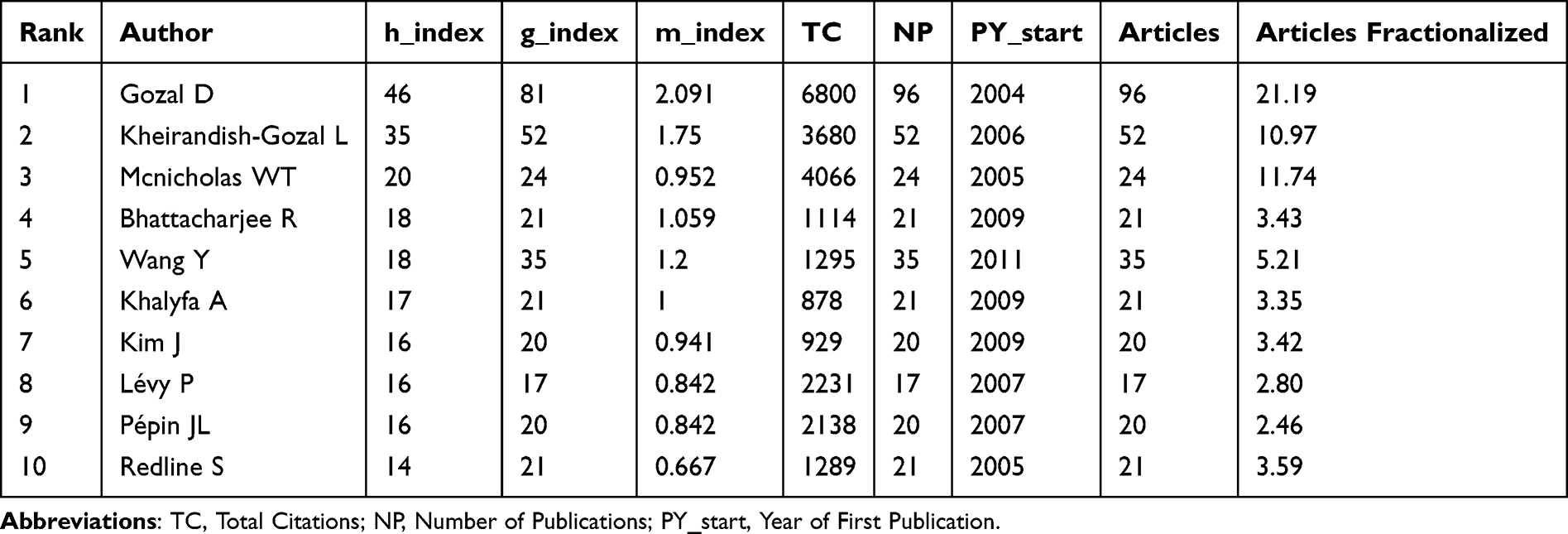 |
Table 1 Top 10 Authors on Inflammation in Obstructive Sleep Apneas Research (1996–2025) |
In Figure 4C, distinct clusters represent specialized research communities, with authors like Gozal, David, Khalyfa, Abdelnaby, and Wittert, Gary A. at the center, indicating their significant roles. The proximity of these clusters suggests overlapping research areas and interdisciplinary connections. Figure 4D depicts the co-cited author network, emphasizing the collective influence of key figures such as Young, T, Lavie, L, and Gozal, D, who form foundational hubs with dense inter-author connections. Table 1 quantifies author influence using metrics such as publication count, h-index, g-index, and citation frequency. The h-index and g-index are both bibliometric indicators used to assess a researcher’s productivity and citation impact. However, the h-index identifies the largest number h such that a researcher has h papers with at least h citations each, without giving extra weight to highly cited papers.20 In contrast, the g-index is defined as the largest number g such that the total citations of the top g papers are at least g², giving more emphasis to highly cited works.19 Table 1 shows that, Gozal D has an h-index of 46 and a g-index of 81, while Kheirandish-Gozal L has an h-index of 35 and a g-index of 52, reflecting their substantial impact. Mcnicholas WT’s high co-authorship count, coupled with an h-index of 20 and g-index of 24, highlights his significant collaborative contributions. Bhattacharjee R and Wang Y, with an h-index of 18, have a high publication count and high citation frequencies, underscoring their influence, collaborative impact and roles as central figures in the literature. Collectively, these results demonstrate that institutional and author collaborations are highly clustered around a few influential centers and scholars, which drive the intellectual development and research impact of the field.
Top Journals and Co-Citation Patterns
Figure 5A ranks journals by the number of published articles, with the “Sleep and Breathing” leading (149 articles), followed by the “ Sleep Medicine” (60 articles) and “Sleep” (46 articles), which both contribute significantly to the literature. Bradford’s Law, illustrated in Figure 5B, reveals a skewed distribution of scholarly output: a small number of journals contribute disproportionately to the number of articles. Core sources, represented in the shaded region, include prominent journals like “Journal of Clinical Sleep Medicine” “Sleep Medicine Reviews” and “Journal of Sleep Research” marking these as primary venues for critical advancements and scholarly discussions in sleep science. Figure 5A and B both indicate that the “Sleep and Breathing” is a key source, in terms of the number of documents published and citation frequency. Figure 5C shows the cumulative number of articles over time, with consistent growth in output from leading journals. Notably, “Sleep and Breathing” has exhibited steady growth since 2010, “Sleep Medicine” has steadily increased since 2015, reaching nearly 50 articles by 2022. Both the “Journal of Clinical Sleep Medicine” and “Sleep” have shown slower growth, but still exhibit a notable accumulation of articles. Overall, the number of publications began to rise after 2000, with a significant acceleration after 2010, reflecting the expansion of research in the field. This trend indicates that the association between OSA and inflammation has become a research hotspot, likely driven by the clinical significance of OSA, the deeper exploration of inflammatory mechanisms, and advancements in related technologies (Table 2). The journal citation network (Figure 5D) identifies clusters of journals that are frequently cited together, indicating strong research communities around specific themes. The co-citation network (Figure 5E) further highlights the strength of these relationships, with prominent nodes like “Circulation” and “American Journal of Respiratory and Critical Care” acting as central hubs. Together, these findings suggest that a limited number of core journals dominate the dissemination of knowledge on OSA and inflammation, thereby shaping the primary avenues for scholarly communication in this field.
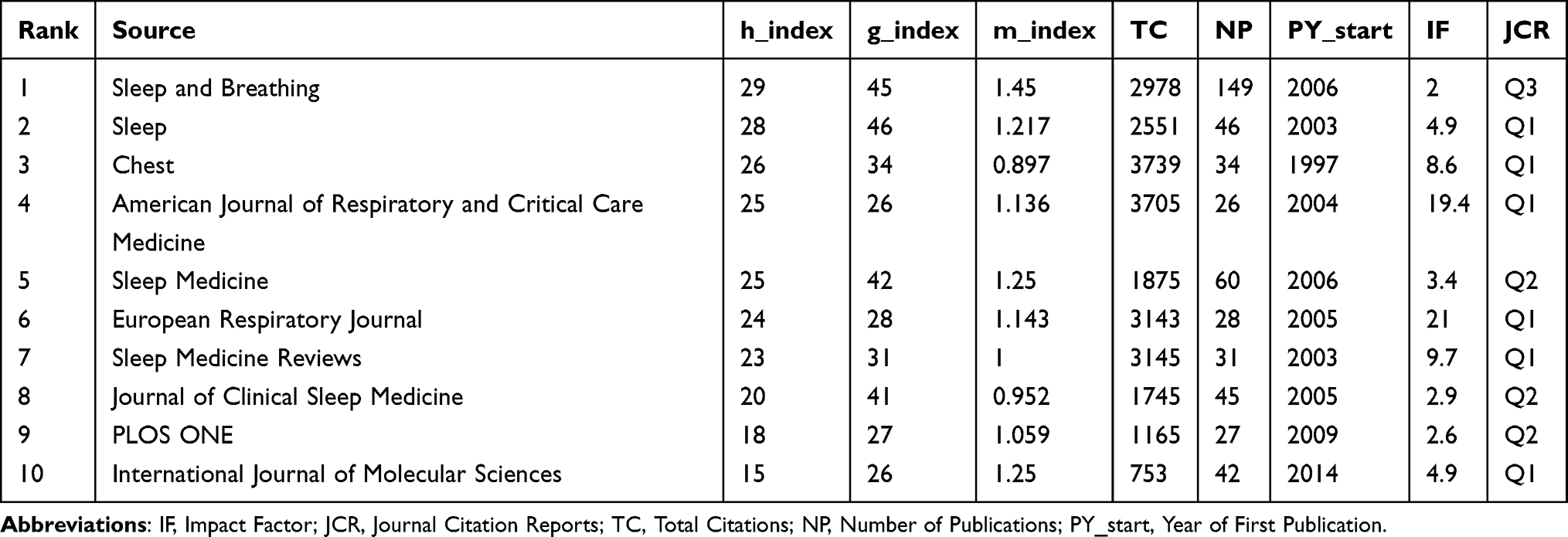 |
Table 2 Top 10 Influential Journals on Inflammation in Obstructive Sleep Apneas Research (1996–2025) |
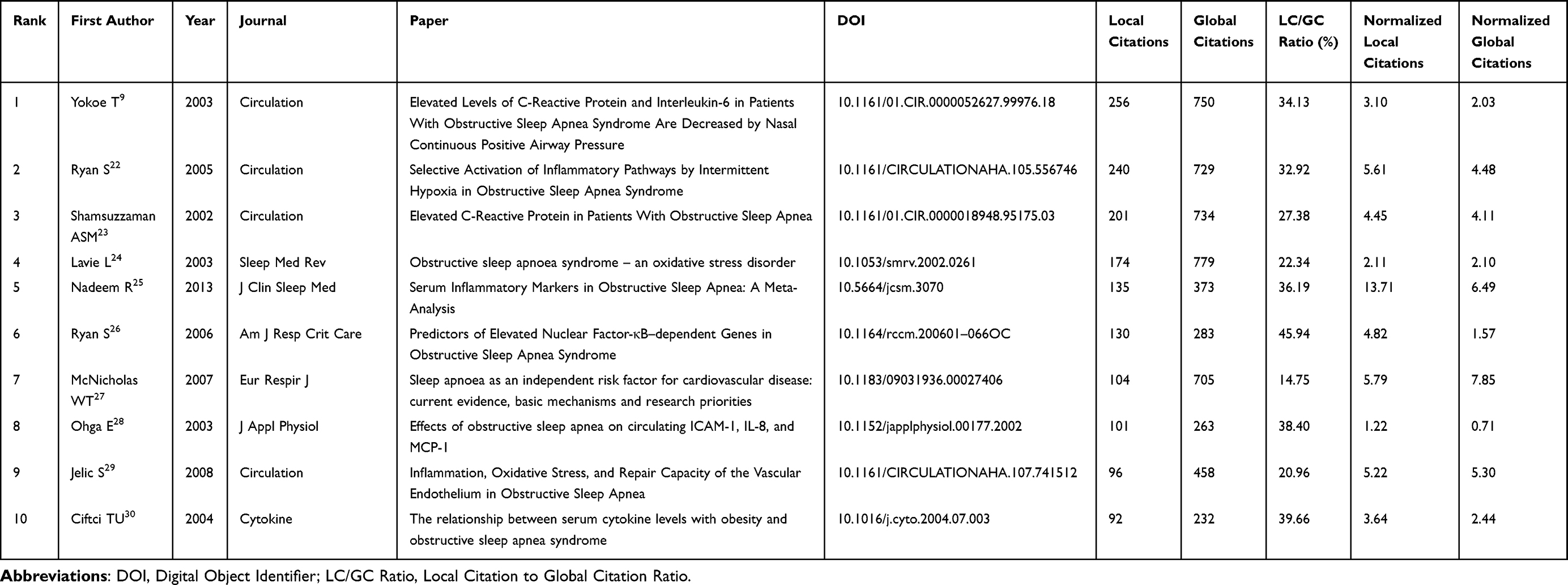 |
Table 3 Top 10 Most Cited Publications Based on Bibliometrix Analysis (1996–2025) |
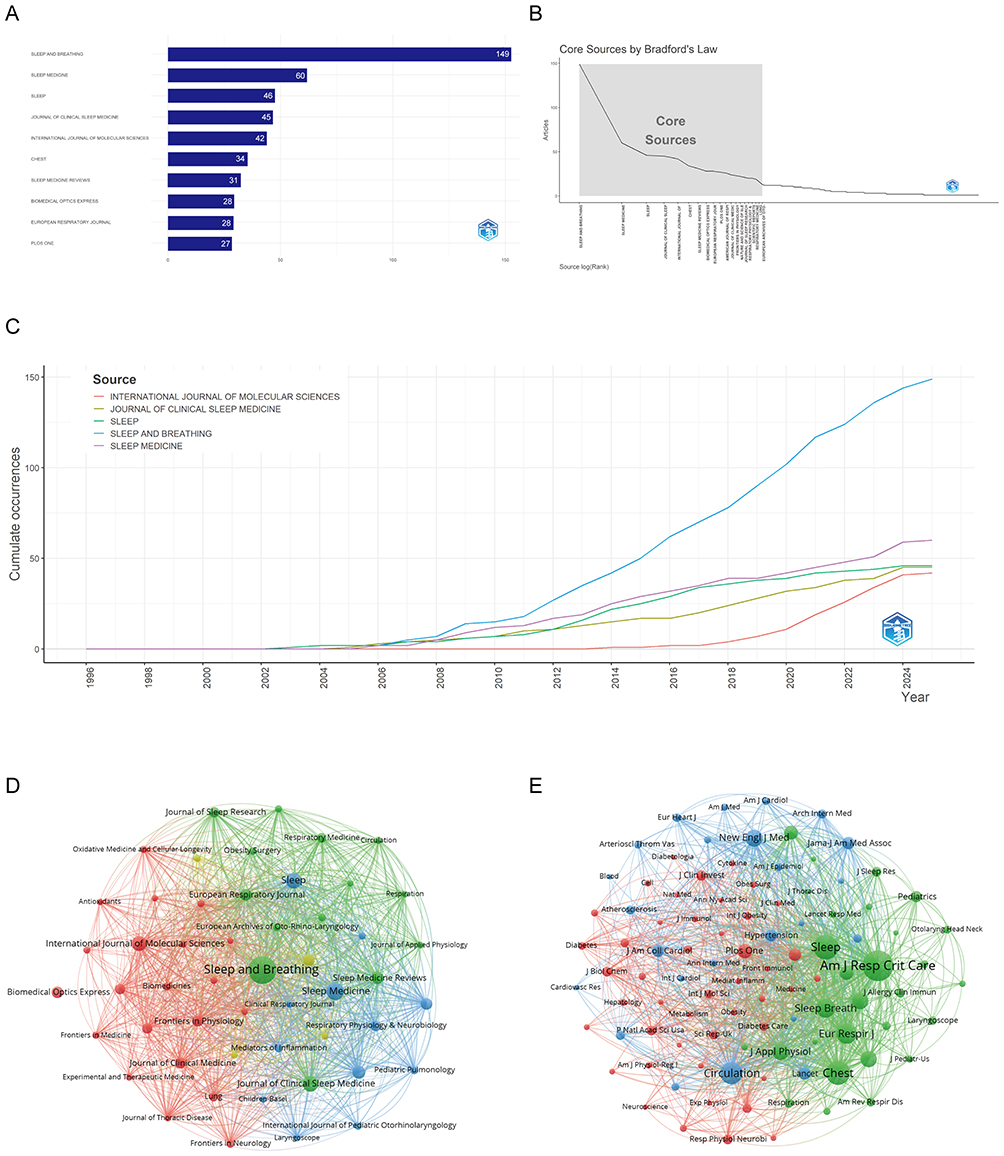 |
Figure 5 Analysis of Journals and Citation Networks Related to Inflammation in Obstructive Sleep Apneas. (A) Top journals ranked by publication count. (B) Bradford’s Law analysis identifying core journals. (C) Publication trends of the top five journals over time. (D) Journal citation network, where nodes represent journals connected by citation links; colors indicate thematic clusters. (E) Journal co-citation network, where node size reflects co-citation frequency and colors represent clusters of commonly co-cited journals. |
Highly Cited Studies and Thematic Clustering
In total, the dataset includes 2,075 documents and 71,34 references (Supplementary Table 2). The average age of these documents is 7.84 years, while each document has been cited 39.67 times, reflecting their substantial impact within the academic community. Table 3 display that the most frequently cited documents with major contributions from groundbreaking studies such as “Elevated Levels of C-Reactive Protein and Interleukin-6 in Patients With Obstructive Sleep Apnea Syndrome Are Decreased by Nasal Continuous Positive Airway Pressure”9 and “Selective Activation of Inflammatory Pathways by Intermittent Hypoxia in Obstructive Sleep Apnea Syndrome”22 in Circulation, with 256 and 240 local citations respectively. The high yearly citation rates demonstrate their substantial impact on advancing the understanding of Obstructive Sleep Apneas and Inflammation. Other influential studies, such as “Elevated C-Reactive Protein in Patients With Obstructive Sleep Apnea”23 and “Obstructive sleep apnoea syndrome–an oxidative stress disorder”,24 have also made significant contributions, each with over 170 local citations. These works have been pivotal in elucidating the mechanisms of activation of inflammatory pathways and the elevation of CRP levels in OSA.
Figure 6A reveals distinct thematic clusters in OSA and Inflammation research. Cluster 0 (“fat-laden hepatocyte”) serves as a core theme, with dense connections to other clusters, highlighting the critical role of fat-laden hepatocytes in the inflammatory mechanisms associated with OSA and the overall pathology. Cluster 1 (“cardiovascular consequence”) emphasizes the association between OSA-induced inflammation and cardiovascular complications such as hypertension and atherosclerosis, reflecting the pivotal role of inflammation in the long-term health consequences of OSA. Cluster 10 (“intermittent hypoxia”) suggests that intermittent hypoxia (IH), a core pathological feature of OSA, accelerates disease progression by inducing oxidative stress and inflammatory responses. Other important clusters include Cluster 8 (“continuous positive airway pressure”), where CPAP provides significant evidence for the clinical treatment and management of inflammation in OSA by improving nocturnal intermittent hypoxia. Cluster 2 (“metabolic syndrome”) highlights metabolic disorders such as insulin resistance, hypertension, and dyslipidemia as important comorbidities and inflammation-driving factors in OSA. Taken together, Figures 6A illustrates not only the major research hotspots but also the interconnections among pathophysiological mechanisms, clinical consequences, and therapeutic strategies. The clustering patterns highlight that OSA-related inflammation is a multifactorial process involving metabolic, cardiovascular, and respiratory pathways. These insights underscore the central role of inflammation in linking OSA to systemic comorbidities and point toward potential translational directions for targeted interventions.
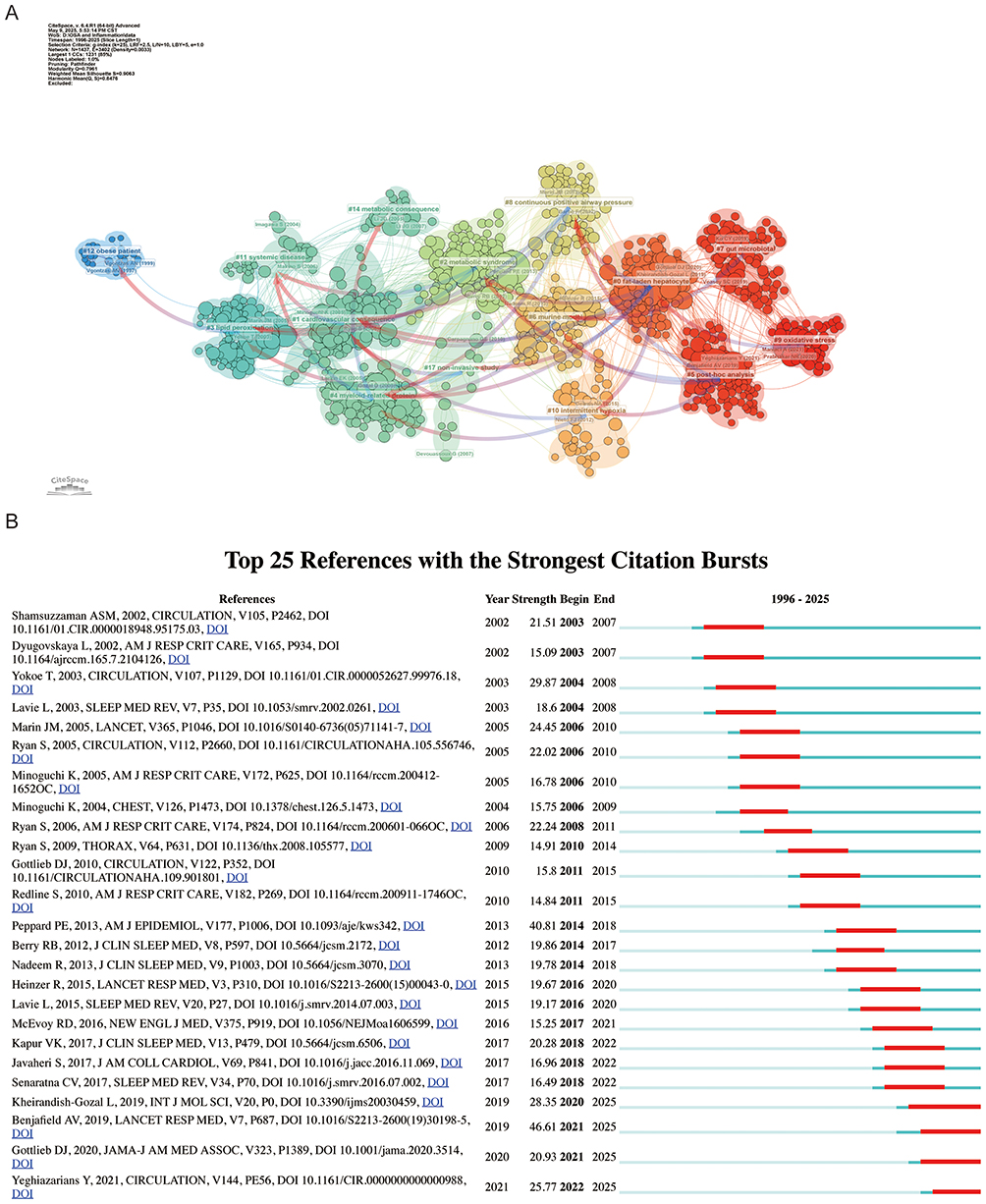 |
Figure 6 Reference Co-citation Analysis and Citation Burst Detection on Inflammation in Obstructive Sleep Apnea. (A) Clustered co-citation network, where node size reflects citation frequency, edge thickness indicates co-citation strength, and colors represent major thematic clusters labeled by keywords. (B) Top 25 references with strongest citation bursts over time, with red segments indicating periods of heightened attention. |
Figure 6B has shown the top 25 references in the field, ranked by the strength of their citation bursts between 2003 and 2025. The citation burst strength is a dynamic measure that reflects the frequency and intensity of citations during a given period. For instance, Benjafield’s 2019 article5 stands out with a remarkable citation burst strength of 46.61 in 2021, suggesting its pivotal role in shaping subsequent research on OSA and inflammation. In contrast, more recent papers, such as those by Yeghiazarians31 and Gottlieb,32 show bursts in citation strength around 2022 and 2021 respectively, reflecting ongoing developments and growing interest in their work on OSA and inflammation. Overall, the most influential studies and thematic clusters converge on the mechanisms, comorbidities, and clinical management of OSA-related inflammation, reflecting both the historical foundations and evolving frontiers of the field.
Keyword Co-Occurrence and Research Themes
The keyword analysis reveals significant trends and focal points in OSA research. Specifically, we identified 3,894 Keywords plus alongside 3,250 author keywords, enhancing the effective indexing and retrieval of scholarly content (Supplementary Table 2).
Figure 7A depicts the overall keyword networks, with distinct clusters emerging around themes of OSA, inflammation, and intermittent hypoxia. Figure 7B, the word cloud, further highlights key themes, reflecting the network visualizations in Figure 7A. As Figure 7C show “obstructive sleep apnea” (1063 occurrences, total link strength = 2050) (Figure 7C, cluster 4 and 7) pathology is at the center of current sleep medicine. “inflammation” (475 occurrences, total link strength = 1195) and “oxidative stress” (150 occurrences, total link strength = 38) are central to the “pathophysiology” (15 occurrences, total link strength = 45) mechanisms of OSA. “Chronic intermittent hypoxia” (63 occurrences, total link strength = 125) induces an inflammatory response by activating the “nuclear factor-kappa b” (20 occurrences, total link strength = 48) signaling pathway, increasing the expression of systemic “inflammatory markers” (16 occurrences, total link strength = 35) such as “c-reactive protein” (56 occurrences, total link strength = 170) (Figure 7C, cluster 8), “interleukin-6” (46 occurrences, total link strength = 126) (Figure 7C, cluster 9), “tumor necrosis factor-alpha” (33 occurrences, total link strength = 97), thereby leading to “endothelial function” (14 occurrences, total link strength = 40) impairment and “tissue” (Figure 7C, cluster 5) damage. OSA can also lead to significant airway inflammation (Figure 7C, cluster 2).
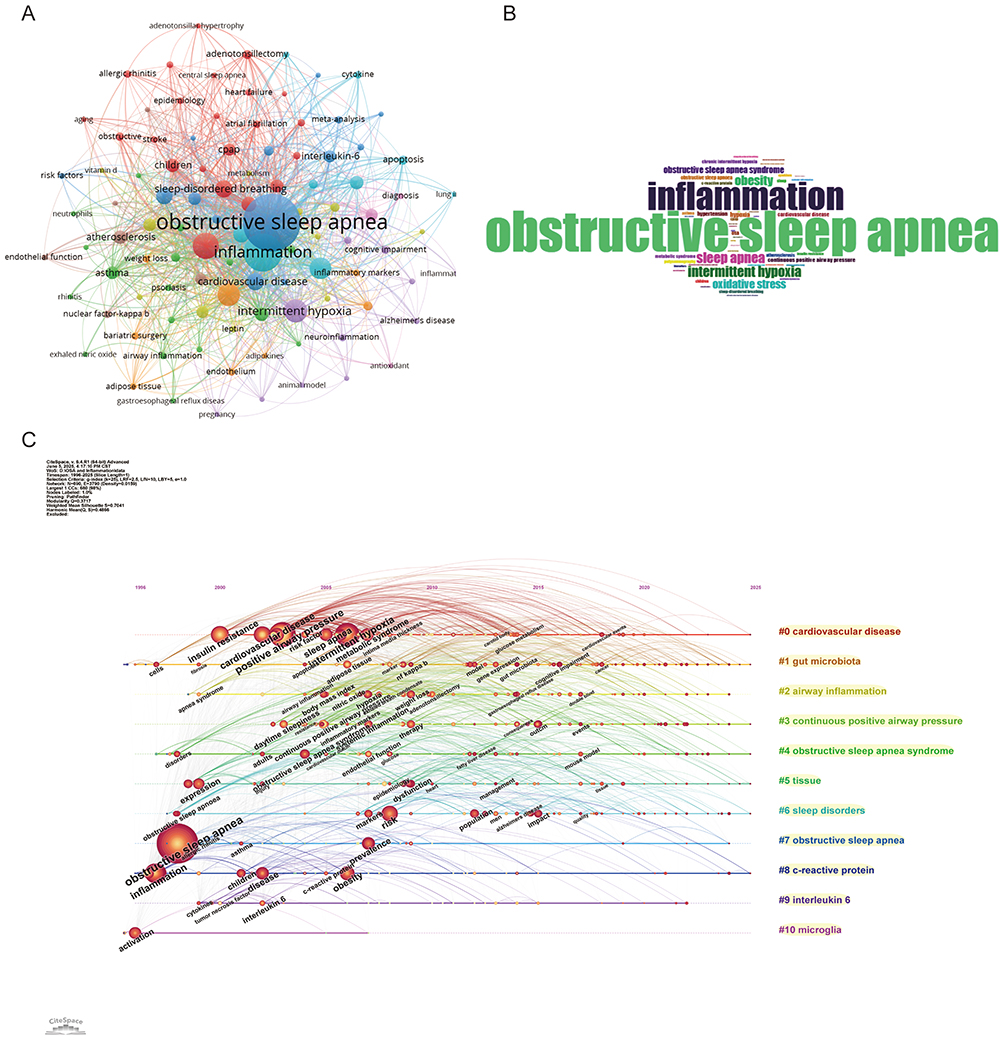 |
Figure 7 Keywords Mapping of Inflammation in Obstructive Sleep Apneas. (A) Keyword co-occurrence network, where nodes represent keywords (sized by frequency), edges indicate co-occurrence, and colors denote thematic clusters. (B) Word cloud of title keywords, with word size reflecting frequency. (C) Keyword timeline showing major clusters and their evolution over time; node size indicates frequency, node color represents time, and connections indicate co-occurrence relationships. |
“Hypertension” (73 occurrences, total link strength = 216), “atherosclerosis” (58 occurrences, total link strength = 163), “endothelial dysfunction” (27 occurrences, total link strength = 81), “atrial fibrillation” (21 occurrences, total link strength =60), “stroke” (17 occurrences, total link strength = 53), “coronary artery disease” (10 occurrences, total link strength = 38) suggest a close association between OSA and “cardiovascular disease” (95 occurrences, total link strength = 256) (Figure 7C, cluster 0). IH and inflammatory markers significantly increase “cardiovascular risk” (29occurrences, total link strength = 72) through inflammation and sympathetic nervous activation. “Metabolic syndrome” (64 occurrences, total link strength = 190), “diabetes” (18 occurrences, total link strength = 59), “adipose tissue” (15 occurrences, total link strength = 47), “adiponectin” (12 occurrences, total link strength = 28) and “non-alcoholic fatty liver disease” (28 occurrences, total link strength = 79) reflects the interaction between OSA and metabolic disorders. “Obesity” (167 occurrences, total link strength = 470) is a major risk factor for OSA and OSA exacerbates “insulin resistance” (47 occurrences, total link strength = 150) and “dyslipidemia” (12 occurrences, total link strength = 42) through inflammation and dysregulation of “adiponectin” (12 occurrences, total link strength = 28).
“Excessive daytime sleepiness” (11 occurrences, total link strength = 34), “insomnia” (14 occurrences, total link strength = 39) and “sleep disorders” (Figure 7C, cluster 6) highlights the disruption of sleep quality by OSA and its impact on cognitive function such as “cognitive impairment” (25 occurrences, total link strength = 64) and mental health such as “depression” (17 occurrences, total link strength = 52). “Polysomnography” (56 occurrences, total link strength = 133) and “bariatric surgery” (19 occurrences, total link strength = 38) suggest that research on the “diagnosis” (14 occurrences, total link strength = 40) and treatment of OSA is a key area of research. “Continuous positive airway pressure” (89 occurrences, total link strength =246) (Figure 7C, cluster 3), as the standard treatment, can significantly improve the “apnea-hypopnea index” (18 occurrences, total link strength = 44). Research on OSA in “children” (59 occurrences, total link strength = 168) and OSA during “pregnancy” (10 occurrences, total link strength = 23) have gradually gained attention. Adenotonsillectomy (30 occurrences, total link strength = 80) is the primary treatment for pediatric OSA.
Research on OSA is expanding into multidisciplinary fields, with a potential association between OSA and “Alzheimer’s disease” (12 occurrences, total link strength = 26), “cancer” (9 occurrences, total link strength = 30), “gut microbiota” (17 occurrences, total link strength = 37) (Figure 7C, cluster 1) “microglia” (18 occurrences, total link strength =23) (Figure 7C, cluster 10), and “vitamin d” (11 occurrences, total link strength = 30).
In conclusion, the keyword analysis highlights that research on OSA and inflammation spans mechanisms, comorbidities, and treatments, while also expanding into emerging multidisciplinary domains, thereby underscoring its growing clinical and scientific relevance.
Discussion
The incidence and prevalence of OSA have increased substantially worldwide, posing a growing burden on healthcare systems and raising significant public health concerns. In this study, we conducted the first comprehensive bibliometric analysis of research on OSA-related inflammation. This bibliometric analysis is not intended to replace systematic reviews or mechanistic studies, but rather to provide a complementary perspective by mapping the knowledge structure and identifying underexplored research areas. Our results provide an integrated overview of publication trends, international collaborations, influential authors and institutions, landmark studies, and emerging research themes. Beyond presenting novel bibliometric patterns, these findings offer relevant insights into how the field has evolved, the intellectual structure that underpins it, and the potential directions for future exploration. Such insights are particularly valuable for guiding new research initiatives, fostering cross-disciplinary collaborations, and identifying underexplored areas with clinical and translational importance.
Placing these bibliometric findings into the clinical context is essential for understanding their significance. The increasing recognition of inflammation as a central mechanism in OSA pathophysiology helps explain why this research domain has become a sustained hotspot, bridging basic science with clinical practice. Current management strategies for OSA primarily aim to alleviate symptoms, with CPAP therapy being the most widely used intervention to mitigate the effects of intermittent hypoxia. Although such treatments improve sleep quality and provide short-term relief, they do not address the underlying inflammatory processes associated with OSA. As the link between OSA and systemic inflammation becomes clearer, there is growing interest in the role of inflammatory pathways in disease progression. In particular, the release of pro-inflammatory cytokines in response to hypoxic episodes is increasingly recognized as a central factor contributing to the long-term cardiovascular and metabolic complications observed in OSA patients. Understanding this intricate relationship between OSA and inflammation may pave the way for novel therapeutic strategies that target inflammatory mechanisms, potentially reducing the broader health impacts of OSA.
Research Highlights
The results of keyword and reference clustering analysis highlight the primary areas of interest for researchers. Combining these findings with our understanding of the field, we succinctly summarize several major research hotspots, including mechanism, comorbidities and treatment.
Mechanism
OSA is increasingly recognized as a systemic disorder linked to chronic inflammation and oxidative stress, with profound implications for both peripheral and central nervous system (CNS) health. The intermittent hypoxia caused by OSA activates various inflammatory pathways, primarily through the upregulation of nuclear factor kappa-B (NF-κB), which subsequently enhances the production of pro-inflammatory cytokines such as IL-6, IL-8, and TNF-α.33 These cytokines are central to the development of systemic inflammation and tissue damage, which are implicated in the exacerbation of comorbidities, including cardiovascular diseases and cognitive impairment.34,35 Additionally, OSA has been found to promote the polarization of M1 macrophages via NF-κB activation, further intensifying the inflammatory response and increasing susceptibility to disorders such as atrial fibrillation.36 Moreover, the apnea index in OSA patients correlates positively with systemic inflammation markers, indicating that OSA may serve as a catalyst for chronic inflammatory states that further complicate metabolic health.37 Evidence also suggests that CPAP therapy, a common treatment for OSA, can significantly reduce levels of inflammatory markers such as CRP, IL-6, and TNF-α, supporting the link between OSA and systemic inflammation.38
A particularly important aspect of OSA’s neurobiological impact is its influence on microglial activation within the CNS. The blood-brain barrier (BBB), a vital protective structure, was once thought to shield the brain from peripheral inflammation and playing a crucial role in maintaining brain homeostasis.39 However, emerging research indicates bidirectional communication between peripheral inflammation and neuroinflammation, challenging this notion.40 Chronic peripheral inflammation has been shown to disrupt endothelial cell function, compromising the BBB’s integrity and permeability, which triggers neuroinflammation.41 In response to OSA-induced hypoxia, microglia, the brain’s resident immune cells, are activated, leading to neuroinflammation. This activation is marked by increased levels of neuroinflammatory markers, which are associated with cognitive impairments.42 Additionally, chronic intermittent hypoxia (CIH), a hallmark of OSA, results in changes to microglial function, including alterations in their numbers and gene expression, which may link OSA to neurodegenerative diseases like Alzheimer’s disease (AD).43 Furthermore, microglia exhibit a dual role in inflammation, acting as both promoters and regulators depending on the disease context. In neurodegenerative diseases, for instance, microglia switch between pro-inflammatory and anti-inflammatory states,44,45 highlighting their complex involvement in the inflammatory response.
In conclusion, the complex interplay between OSA, systemic inflammation, and neuroinflammation, with microglia as central mediators, underscores the necessity of addressing these pathways in OSA management. Given the complexity of this network, further research into therapeutic strategies targeting inflammation and microglial activation may offer potential to alleviate the broader health risks associated with OSA.
Comorbidities
First, OSA and metabolic syndrome exhibit a strong interrelationship, where OSA may worsen the key components of metabolic syndrome, including obesity, insulin resistance, and dyslipidemia. The intermittent hypoxia and disrupted sleep patterns inherent in OSA may trigger an elevation in sympathetic nervous system activity and systemic inflammation, thereby further disrupting metabolic processes. Conversely, the presence of metabolic syndrome can exacerbate the occurrence and severity of OSA, resulting in a bidirectional interaction that complicates the clinical management and treatment of both disorders. Patients with obesity hypoventilation syndrome, a form of OSA, show significantly higher rates of metabolic syndrome, as evidenced by increased waist circumference and triglyceride levels, suggesting a strong association between the two conditions.46 Two large cross-sectional epidemiological studies demonstrated that obstructive sleep apnea is independently associated with both metabolic abnormalities and an increased risk of developing diabetes, regardless of other risk factors.47,48 Additionally, individuals with metabolic syndrome exhibit mixed treatment preferences for OSA, indicating a complex relationship, though not providing strong evidence of a direct association.49
Second, OSA is closely associated with cardiovascular disease (CVD), primarily through inflammatory mechanisms. Patients with OSA often present with elevated pulse wave velocity, a marker linked to increased all-cause and cardiovascular mortality, highlighting the significant cardiovascular risks posed by this condition.50 Additionally, myocardial dysfunction, such as reduced left ventricular global longitudinal strain, is frequently observed in moderate-to-severe OSA cases, further emphasizing its cardiovascular impact.51 Inflammation plays a crucial role in this connection, as it accelerates atherosclerosis and contributes to the progression of other cardiovascular diseases.52 OSA is also strongly correlated with an increased risk of stroke, with a high prevalence of OSA observed in patients with ischemic stroke.53 This relationship is further supported by the identification of shared differentially expressed genes, such as DUSP1, which are upregulated in both conditions.54 Inflammation is a key mediator in this association, as systemic inflammation disrupts blood-brain barrier integrity and promotes thrombosis, thus increasing the likelihood of cerebrovascular events.55 Moreover, inflammation following ischemic stroke exacerbates neural damage through mechanisms like pyroptosis, highlighting the bidirectional relationship between stroke and inflammation.56
Additionally, OSA is increasingly recognized for its complex interplay with systemic inflammation and comorbid respiratory diseases, particularly asthma and allergic rhinitis. Studies have demonstrated a significantly higher prevalence of asthma among individuals with OSA, suggesting a meaningful association between the two conditions.57 The inflammatory pathophysiology underlying allergic rhinitis—driven primarily by Th2 immune responses—has been shown to exacerbate asthma symptoms, contributing to the heightened inflammatory burden observed in patients with OSA.58 This systemic inflammation is corroborated by elevated levels of circulating inflammatory markers, which show a positive correlation with OSA severity.37 Moreover, the relationship between OSA and chronic obstructive pulmonary disease (COPD) has emerged as a critical area of concern. OSA frequently coexists with stable COPD, and this overlap is associated with increased right ventricular systolic pressure, indicating adverse cardiovascular consequences.59 In COPD, persistent inflammation characterized by elevated biomarkers such as C-reactive protein and interleukin-6 is strongly linked to disease progression and severity.60 Asthma, a known risk factor for COPD, further supports the hypothesis of a shared inflammatory continuum bridging these respiratory conditions.61 Together, these findings underscore the intricate pathophysiological connections among OSA, asthma, allergic rhinitis, and COPD, mediated through common inflammatory pathways.
What’s more, OSA has emerged as a notable risk factor for the development and progression of several neurodegenerative diseases, most prominently AD. The hallmark feature of OSA—CIH—is strongly associated with enhanced neuroinflammatory responses, which are increasingly recognized as central to the pathophysiology of cognitive decline and AD. Experimental and clinical studies have demonstrated that CIH leads to upregulation of pro-inflammatory cytokines and elevated oxidative stress levels, both of which contribute to neuronal injury and impaired cognitive performance.62 Moreover, cognitive dysfunction is frequently observed in OSA patients, with a clear correlation between OSA severity and amyloid-β deposition, as well as increased markers of neuroinflammation.63 In addition, the prevalence studies indicate that there may be an increased prevalence of OSA in individuals with major depressive disorder. Studies of treatment of OSA indicate an improvement in both OSA and psychiatric symptoms.64 Depression is commonly co-morbid with OSA and has been shown to accelerate cognitive deterioration in AD, potentially through mechanisms involving amplified neuroinflammation and increased amyloid plaque burden.65 Furthermore, elevated inflammatory biomarkers have been identified in individuals with depressive symptoms, and these markers are closely associated with worsening cognitive outcomes.66 Collectively, these observations suggest that targeting neuroinflammatory processes may offer dual benefits—amelioration of depressive symptoms and attenuation of cognitive decline—in patients affected by OSA and related neuropsychiatric conditions.67
Treatment
CPAP therapy, a common treatment for OSA, has been shown to significantly reduce inflammatory markers, indicating its role in mitigating inflammation associated with OSA.38 Adenotonsillectomy, a surgical intervention for OSA, also reduces systemic inflammation, as demonstrated by decreased levels of inflammatory biomarkers such as interleukin-8 and C-C chemokine ligand 5, which contribute to improvements in apnea-hypopnea index (AHI).68 OSA is typically characterized by a low-grade inflammatory state, which contributes to its cardiovascular comorbidities. Although CPAP therapy remains the cornerstone of OSA management, adjunctive approaches such as weight loss and antioxidant-rich diets—including vitamins A, B, C, D, and E—have shown promise in alleviating the pathophysiology of OSA and mitigating cardiovascular risks69 Weight loss, whether achieved through lifestyle changes or surgical means, is generally associated with a reduction in pro-inflammatory macrophages and an increase in anti-inflammatory cells, contributing to better management of OSA.70 Moreover, bariatric surgery has a profound impact on systemic inflammation, with patients often experiencing reductions in inflammatory markers. These changes are typically associated with improvements in metabolic conditions.71 However, it is important to note that weight loss may also trigger increased inflammation in certain contexts, such as during infections.72 Thus, the relationship between weight loss and inflammation is complex, but overall, it appears to benefit OSA outcomes by reducing the respiratory burden and systemic inflammation.53 In conclusion, the management of OSA requires a multifaceted approach that incorporates surgical interventions like adenotonsillectomy, the use of CPAP therapy, and lifestyle modifications, such as weight loss. These combined strategies not only help reduce inflammation but also significantly improve patient outcomes.
Future Research Directions
OSA has been increasingly recognized for its complex interactions with systemic and neuroinflammation, which play a crucial role in the pathogenesis of various comorbidities associated with OSA. As research in this field continues to evolve, there is growing interest in understanding how OSA-induced inflammation contributes to disease progression and the development of long-term health complications. Our findings suggest that investigating the molecular pathways through which OSA triggers inflammatory responses, and how these pathways affect various organs, could provide novel insights into potential therapeutic strategies. Future research should focus on identifying specific biomarkers and therapeutic targets within inflammatory pathways that are activated by OSA, which may lead to the development of more effective interventions for mitigating inflammation and preventing the chronic effects of OSA. Additionally, exploring the potential of anti-inflammatory treatments as adjuncts to existing OSA therapies could open new avenues for improving patient outcomes and reducing associated health risks.
Biomarker Discovery
Research should focus on identifying reliable biomarkers to improve early diagnosis, patient stratification, and treatment monitoring. The discovery of these biomarkers is gaining increasing attention, as recent studies suggest that these markers may not only improve the diagnosis of OSA but also provide deeper insights into its underlying mechanisms. For instance, Galectin-3 has been identified as a potential biomarker for sleep health, underscoring the role of inflammatory pathways in OSA.73 Similarly, the chemokine Eotaxin has been linked to an increased risk of OSA, further highlighting the importance of inflammation in disease progression.74 Genetic variants, such as those in the FTO gene, have also been associated with OSA, suggesting potential applications in both diagnostic and prognostic assessment.75 Moreover, circulating non-coding RNAs (ncRNAs) have shown promise as diagnostic biomarkers for OSA hypoventilation syndrome, offering new opportunities for early detection and monitoring.76 In addition, OSA-related sleep fragmentation contributes to cardiovascular alterations, with elevated levels of matrix metalloproteinase-9 (MMP9) and oxidized low-density lipoprotein (ox-LDL) suggesting a role in cardiovascular remodeling.77 Elevated levels of CHI3L1-Ab have also been observed in OSA patients compared to healthy controls, indicating its potential as an independent diagnostic biomarker.78 Overall, these findings underscore the critical role of biomarker discovery in advancing the understanding and management of OSA.
Neuroinflammation-Targeted Therapy
Targeted therapeutic approaches that modulate neuroinflammation and microglial activity hold promise for improving cognitive function and mitigating long-term neurological complications in OSA. Ongoing research into neuroinflammation-targeted interventions seeks to address the underlying biological mechanisms, offering potential strategies to complement existing OSA treatments and reduce its neurocognitive burden. IH has been shown to elevate inflammatory markers and induce cognitive impairment.79 Certain interventions can counteract these effects; for instance, melatonin reduces pro-inflammatory cytokines and enhances synaptic plasticity, thereby improving hypoxia-related cognitive deficits,80 while the glucagon-like peptide-1 receptor (GLP-1R) agonist liraglutide alleviates cognitive dysfunction by activating the nuclear factor erythroid 2-related factor 2 (Nrf2)/ heme oxygenase-1 (HO-1) pathway and inhibiting mitogen-activated protein kinase (MAPK)/NF-κB signaling.81 These findings suggest that neuroinflammation-targeted strategies may serve as valuable adjuncts to conventional treatments such as continuous positive airway pressure, potentially reducing the neurocognitive burden of OSA.82
Limitations
The analysis of inflammation in OSA presents several notable advantages. First, it is a groundbreaking attempt to systematically examine the research landscape of inflammation in OSA through bibliometric methods, facilitating a quantitative assessment of the field’s development. The study’s extensive coverage of OSA literature offers a well-rounded view of the subject. By utilizing various bibliometric tools, it delivers an in-depth understanding of the research landscape, highlighting key contributors, thematic trends, and existing gaps. The incorporation of software such as VOSviewer and CiteSpace bolsters the objectivity and reproducibility of the analysis, establishing a solid foundation for guiding future research.
Nevertheless, the study has limitations that should be recognized. A major concern is the potential bias from the choice of specific databases. Solely relying on sources like WoSCC may result in the omission of relevant studies indexed in other databases such as PubMed, Scopus, or the Cochrane Library. Additionally, the emphasis on English-language publications might lead to an underrepresentation of research conducted in other languages, distorting the understanding of the global OSA research landscape. Data consistency issues, including discrepancies in author names or institutional affiliations, could also compromise the accuracy of the analysis. Lastly, the coverage may not encompass the latest research due to the delay between data collection and publication.
Conclusion
Our study highlights the remarkable progress that has been made in understanding inflammation in OSA, underscoring the importance of international collaboration, the contributions of leading institutions and scholars, the influence of high-impact journals, and the evolution of research priorities. Future work should focus on elucidating the molecular mechanisms underlying OSA, improving the management of comorbidities, and developing novel therapeutic strategies. These advances will require sustained interdisciplinary collaboration among clinicians in sleep medicine, cardiology, and neurology, together with basic scientists, public health professionals, and data scientists. Equally crucial is the effective translation of research findings into clinical practice to enhance diagnostic approaches, refine therapeutic interventions, and ultimately improve long-term outcomes for patients with OSA.
Abbreviations
OSA, Obstructive Sleep Apnea; WoSCC, Web of Science Core Collection; INSERM, Institut National De La Sante Et De La Recherche Medicale; CPAP, Continuous Positive Airway Pressure; OSAS, Obstructive Sleep Apnea Syndrome; TNF-α, Tumor Necrosis Factor-alpha; IL-6, Interleukin-6; CRP, C-reactive protein; TI, Title; AB, Abstract; AK, Author Keywords; OALM, Online Analysis Platform of Literature Metrology; NC, Number of Citations; NP, Number of Publications; SCP, Single-country Publications; MCP, Multiple-country Publications;; IH, Intermittent Hypoxia; NF-κB, Nuclear Factor Kappa-B; IL-8, Interleukin-8; BBB, Blood-brain Barrier; CNS, Central Nervous System; CIH, Chronic Intermittent Hypoxia; AD, Alzheimer’s Disease; T2DM, Type 2 Diabetes Mellitus; CVD, Cardiovascular Disease; COPD, Chronic Obstructive Pulmonary Disease; AHI, Apnea-hypopnea Index; ncRNAs, Non-coding RNAs; MMP9, Matrix Metalloproteinase-9; ox-LDL, Oxidized Low-Density Lipoprotein; GLP-1R, Glucagon-Like Peptide-1 Receptor; Nrf2, Nuclear Factor Erythroid 2-Related Factor 2; HO-1, Heme Oxygenase-1; MAPK, Mitogen-Activated Protein Kinase.
Data Sharing Statement
The request for original data that support this paper’s conclusions can be directed to the corresponding authors.
Acknowledgments
The authors would like to thank the editors and the anonymous reviewers for their valuable comments and suggestions to improve the quality of the paper.
Author Contributions
Haixia Fan: Writing – Review & Editing, Writing – Original Draft Preparation, Conceptualization, Supervision, Formal Analysis. Huiyan Niu: Writing – Review & Editing, Writing – Original Draft Preparation, Conceptualization, Formal Analysis. Bomeng Zhao: Writing – Review & Editing, Writing – Original Draft Preparation, Formal Analysis. Xiaoling Gao: Writing – Review & Editing, Conceptualization, Data curation, Methodology, Funding Acquisition, Supervision, Project Administration. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China General Program (Grant No. 82370091); the Shanxi Province Science and Technology Achievement Transformation Guided Program (Grant No. 202204021301068); Shanxi Province Higher Education “Billion Project” Science and Technology Guidance Project (Grant No. BYJL029); Scientific Research Project from the Shanxi Provincial Health Commission (Grant No. 2023XG027); Fund Program for the Scientific and Activities of Selected Returned Overseas Professionals in Shanxi Province (Grant No. 20250052).
Disclosure
There are no disclosed conflicts of interest for the authors.
References
1. Jordan AS, McSharry DG, Malhotra A. Adult obstructive sleep apnoea. Lancet. 2014;383(9918):736–747. doi:10.1016/s0140-6736(13)60734-5
2. Bickelmann AG, Burwell CS, Robin ED, Whaley RD. Extreme obesity associated with alveolar hypoventilation; a Pickwickian syndrome. Am J Med. 1956;21(5):811–818. doi:10.1016/0002-9343(56)90094-8
3. Dempsey JA, Veasey SC, Morgan BJ, O’Donnell CP. Pathophysiology of sleep apnea. Physiol Rev. 2010;90(1):47–112. doi:10.1152/physrev.00043.2008
4. Sullivan CE, Issa FG, Berthon-Jones M, Eves L. Reversal of obstructive sleep apnoea by continuous positive airway pressure applied through the nares. Lancet. 1981;1(8225):862–865. doi:10.1016/s0140-6736(81)92140-1
5. Benjafield AV, Ayas NT, Eastwood PR, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med. 2019;7(8):687–698. doi:10.1016/s2213-2600(19)30198-5
6. Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365(9464):1046–1053. doi:10.1016/s0140-6736(05)71141-7
7. Kheirandish-Gozal L, Gozal D. Obstructive Sleep Apnea and Inflammation: proof of Concept Based on Two Illustrative Cytokines. Int J Mol Sci. 2019;20(3):459. doi:10.3390/ijms20030459
8. Vgontzas AN, Papanicolaou DA, Bixler EO, Kales A, Tyson K, Chrousos GP. Elevation of plasma cytokines in disorders of excessive daytime sleepiness: role of sleep disturbance and obesity. J Clin Endocrinol Metab. 1997;82(5):1313–1316. doi:10.1210/jcem.82.5.3950
9. Yokoe T, Minoguchi K, Matsuo H, et al. Elevated levels of C-reactive protein and interleukin-6 in patients with obstructive sleep apnea syndrome are decreased by nasal continuous positive airway pressure. Circulation. 2003;107(8):1129–1134. doi:10.1161/01.cir.0000052627.99976.18
10. Marginson S. Global science and national comparisons: beyond bibliometrics and scientometrics. Article Comp Educ. 2022;58(2):125–146. doi:10.1080/03050068.2021.1981725
11. McBurney MK, Novak PL. What is bibliometrics and why should you care? IEEE. 2002;2022:108–114.
12. Adams J. Bibliometrics: the citation game. Nature. 2014;510(7506):470–471. doi:10.1038/510470a
13. AlRyalat SAS, Malkawi LW, Momani SM. Comparing Bibliometric Analysis Using PubMed, Scopus, and Web of Science Databases. J Visualized Exp. 2019;152:e58494. doi:10.3791/58494
14. Wang H, Chen Y, Gou Y, Yang D, Xiong L. Chronic kidney diseases and inflammation research: a bibliometric analysis. Front Med. 2024;11:1388665. doi:10.3389/fmed.2024.1388665
15. Dong J, Yu X, Wang Y, Zhang H, Guo R. Obstructive sleep apnea and cognition: insights gleaned from bibliometric analysis. Front Psychiatry. 2023;14:1259251. doi:10.3389/fpsyt.2023.1259251
16. Niu Y, Cai H, Zhou W, et al. Research trends in hypertension associated with obstructive sleep apnea: a bibliometric analysis. Sleep Breathing. 2023;27(2):411–419. doi:10.1007/s11325-022-02637-8
17. Chen CM. CiteSpace II: detecting and visualizing emerging trends and transient patterns in scientific literature. Article J Am Soc Inf Sci Technol. 2006;57(3):359–377. doi:10.1002/asi.20317
18. Arruda H, Silva ER, Lessa M, Proença Jr D, Bartholo R. VOSviewer and Bibliometrix. J Med Library Assoc. 2022;110(3):392–395. doi:10.5195/jmla.2022.1434
19. Egghe L. Theory and practise of the g-index. Article. Scientometrics. 2006;69(1):131–152. doi:10.1007/s11192-006-0144-7
20. Hirsch JE. An index to quantify an individual’s scientific research output. Article. Proc Natl Acad Sci U S A. 2005;102(46):16569–16572. doi:10.1073/pnas.0507655102
21. Aria M, Cuccurullo C. bibliometrix: an R-tool for comprehensive science mapping analysis. Article J Informetr. 2017;11(4):959–975. doi:10.1016/j.joi.2017.08.007
22. Ryan S, Taylor CT, McNicholas WT. Selective activation of inflammatory pathways by intermittent hypoxia in obstructive sleep apnea syndrome. Circulation. 2005;112(17):2660–2667. doi:10.1161/circulationaha.105.556746
23. Shamsuzzaman AS, Winnicki M, Lanfranchi P, et al. Elevated C-reactive protein in patients with obstructive sleep apnea. Circulation. 2002;105(21):2462–2464. doi:10.1161/01.cir.0000018948.95175.03
24. Lavie L. Obstructive sleep apnoea syndrome--an oxidative stress disorder. Sleep Med Rev. 2003;7(1):35–51. doi:10.1053/smrv.2002.0261
25. Nadeem R, Molnar J, Madbouly EM, et al. Serum inflammatory markers in obstructive sleep apnea: a meta-analysis. J Clin Sleep Med. 2013;9(10):1003–1012. doi:10.5664/jcsm.3070
26. Ryan S, Taylor CT, McNicholas WT. Predictors of elevated nuclear factor-kappaB-dependent genes in obstructive sleep apnea syndrome. Am J Respir Crit Care Med. 2006;174(7):824–830. doi:10.1164/rccm.200601-066OC
27. McNicholas WT, Bonsigore MR. Management Committee of EU COST ACTION B26. Sleep apnoea as an independent risk factor for cardiovascular disease: current evidence, basic mechanisms and research priorities. Eur Respir J. 2007;29(1):156–178. doi:10.1183/09031936.00027406
28. Ohga E, Tomita T, Wada H, Yamamoto H, Nagase T, Ouchi Y. Effects of obstructive sleep apnea on circulating ICAM-1, IL-8, and MCP-1. J Appl Physiol. 2003;94(1):179–184. doi:10.1152/japplphysiol.00177.2002
29. Jelic S, Padeletti M, Kawut SM, et al. Inflammation, oxidative stress, and repair capacity of the vascular endothelium in obstructive sleep apnea. Circulation. 2008;117(17):2270–2278. doi:10.1161/CIRCULATIONAHA.107.741512
30. Ciftci TU, Kokturk O, Bukan N, Bilgihan A. The relationship between serum cytokine levels with obesity and obstructive sleep apnea syndrome. Cytokine. 2004;28(2):87–91. doi:10.1016/j.cyto.2004.07.003
31. Yeghiazarians Y, Jneid H, Tietjens JR, et al. Obstructive Sleep Apnea and Cardiovascular Disease: a Scientific Statement From the American Heart Association. Circulation. 2021;144(3):e56–e67. doi:10.1161/cir.0000000000000988
32. Gottlieb DJ, Punjabi NM. Diagnosis and Management of Obstructive Sleep Apnea: a Review. JAMA. 2020;323(14):1389–1400. doi:10.1001/jama.2020.3514
33. Wang YG, Lin C, Huang M, Fang XL, Chen GH, Ye SN. Overexpression of YKL40, IL-6, IL-8, TNF-α in tonsils and the role of YKL40 in childhood with obstructive sleep apnea syndrome. Sci Rep. 2024;14(1):26283. doi:10.1038/s41598-024-74402-8
34. Yamauchi M, Kimura H. Oxidative stress in obstructive sleep apnea: putative pathways to the cardiovascular complications. Antioxid. Redox Signal. 2008;10(4):755–768. doi:10.1089/ars.2007.1946
35. Eldin MS, Alahmer M, Alkashlan E, et al. Alterations in Inflammatory Markers and Cognitive Ability after Treatment of Pediatric Obstructive Sleep Apnea. Medicina. 2023;59(2):204. doi:10.3390/medicina59020204
36. He H, Zhou Z, Zhang L, Lu Z, Li B, Li X. HIF1α/MIF/CD74 signaling mediated OSA-induced atrial fibrillation by promoting M1 macrophages polarization. Int Immunopharmacol. 2025;149:114248. doi:10.1016/j.intimp.2025.114248
37. Zirih T, Ozergin Coskun Z, Şahin Ü, et al. Pan Immune Inflammation Index: a New Biomarker for Diagnosis and Monitoring of Obstructive Sleep Apnea. J Craniofacial Surg. 2025. doi:10.1097/scs.0000000000011544
38. Zhu Q, Luo Q, Wang Z, Chen S, Chen G, Huang S. Effects of continuous positive airway pressure therapy on inflammatory markers in patients with obstructive sleep apnea: a meta-analysis of randomized controlled trials. Sleep Breathing. 2025;29(2):182. doi:10.1007/s11325-025-03348-6
39. Abdullahi W, Tripathi D, Ronaldson PT. Blood-brain barrier dysfunction in ischemic stroke: targeting tight junctions and transporters for vascular protection. Am J Physiol Cell Physiol. 2018;315(3):C343–c356. doi:10.1152/ajpcell.00095.2018
40. Louveau A, Smirnov I, Keyes TJ, et al. Structural and functional features of central nervous system lymphatic vessels. Nature. 2015;523(7560):337–341. doi:10.1038/nature14432
41. Riedel B, Browne K, Silbert B. Cerebral protection: inflammation, endothelial dysfunction, and postoperative cognitive dysfunction. Current Opinion Anaesthesiol. 2014;27(1):89–97. doi:10.1097/aco.0000000000000032
42. Kong Y, Ji J, Zhan X, et al. Tet1-mediated 5hmC regulates hippocampal neuroinflammation via wnt signaling as a novel mechanism in obstructive sleep apnoea leads to cognitive deficit. J Neuroinflam. 2024;21(1):208. doi:10.1186/s12974-024-03189-2
43. Marino KM, Ewald AC, Lash JN, et al. Chronic intermittent hypoxia exposure induces a unique microglial transcriptome in 5XFAD mice. Res Square. 2025. doi:10.21203/rs.3.rs-6203482/v1
44. Hansen DV, Hanson JE, Sheng M. Microglia in Alzheimer’s disease. J Cell Biol. 2018;217(2):459–472. doi:10.1083/jcb.201709069
45. AmeliMojarad M, AmeliMojarad M. The neuroinflammatory role of microglia in Alzheimer’s disease and their associated therapeutic targets. CNS Neurosci Ther. 2024;30(7):e14856. doi:10.1111/cns.14856
46. Çiftçioğlu U, Kerget B, Akgün M. Differential diagnosis of chronic obstructive pulmonary disease and obesity hypoventilation syndrome in patients presenting with hypercapnic respiratory failure. Sleep Breathing. 2025;29(3):201. doi:10.1007/s11325-025-03367-3
47. Punjabi NM, Shahar E, Redline S, Gottlieb DJ, Givelber R, Resnick HE. Sleep-disordered breathing, glucose intolerance, and insulin resistance: the Sleep Heart Health Study. Am J Eepidemiol. 2004;160(6):521–530. doi:10.1093/aje/kwh261
48. Togeiro SM, Carneiro G, Ribeiro Filho FF, et al. Consequences of obstructive sleep apnea on metabolic profile: a Population-Based Survey. Obesity. 2013;21(4):847–851. doi:10.1002/oby.20288
49. Kraiwattanapong J, Rattanaarun K, Cunteerasup A, Papassornsiri T, Balankura T, Pavarajarn S. Clinical characteristics and treatment preferences of obstructive sleep apnea. Sci Rep. 2025;15(1):18976. doi:10.1038/s41598-025-03816-9
50. Lin H, Zheng H, Lin T, Chen L. Association of estimated pulse wave velocity with all-cause mortality and cardiovascular mortality in obstructive sleep apnea patients: results from NHANES. Front Cardiovasc Med. 2025;12:1571610. doi:10.3389/fcvm.2025.1571610
51. Pei C, Ding Z, Hu L, Gui S. Prediction of early myocardial damage in obstructive sleep apnea patients using combined logistic regression and QUEST decision tree models. Braz J Med Biol Res. 2025;58:e14757. doi:10.1590/1414-431X2025e14757
52. Xia B, Peng J, Ding J, et al. ATF3 regulates inflammatory response in atherosclerotic plaques in mice through the NF-κB signaling pathway]. Nan fang yi ke da xue xue bao =. J Southern Med Univ. 2025;45(6):1131–1142. doi:10.12122/j.issn.1673-4254.2025.06.03
53. Hassan MG, Hassan DG, Hassan GA. Tirzepatide gains US Food and Drug Administration approval for the management of obstructive sleep apnea: implications for oral health care providers. J Am Dental Assoc. 2025;156(8):620–625. doi:10.1016/j.adaj.2025.05.007
54. Zhou L, Ye P, Wang Y. Exploring the potential biomarkers between stroke and obstructive sleep apnea by WGCNA and machine learning. Sleep Breathing. 2025;29(4):219. doi:10.1007/s11325-025-03369-1
55. Ding R, Ren X, Sun Q, et al. Air Pollution and Stroke: an Emerging Challenge From Cardio-Cerebrovascular Multimorbidity. J Am Heart Assoc. 2025;14(13):e041848. doi:10.1161/jaha.124.041848
56. Gu Y, Sun Z, Li T, Ding X. Huanglian Jiedu Decoction Treats Ischemic Stroke by Regulating Pyroptosis: insights from Multi-Omics and Drug-Target Relationship Analysis. Pharmaceuticals. 2025;18(6):775. doi:10.3390/ph18060775
57. Hand C, Bohn C, Angotti M, Eilen H, Varano M, Forsythe B. Effects of obstructive sleep apnea on postoperative outcomes following total shoulder arthroplasty: a matched cohort analysis. J Orthopaedics. 2025;64:163–168. doi:10.1016/j.jor.2025.04.009
58. Valcovici M, Iacob MS, Sharma A, et al. The Junction of Allergic Inflammation and Atherosclerosis: pathways and Clinical Implications-A Review. Life. 2025;15(6):964. doi:10.3390/life15060964
59. Prakash V, Kumar A, Saini LK, et al. Proportion of sleep-related breathing disorders and their association with echocardiographic parameters in stable patients with chronic obstructive pulmonary disease: a cross-sectional observational exploratory study. Monaldi Arch Chest Disease. 2024. doi:10.4081/monaldi.2024.2815
60. Rus LA, Popețiu RO, Borta SM, et al. Lower Vitamin D During Acute Exacerbation Is Associated with Very Severe Chronic Obstructive Pulmonary Disease. Medicina. 2025;61(6):979. doi:10.3390/medicina61060979
61. Subedi S, Guntipally M, Suwal N, et al. Cellular senescence in chronic obstructive pulmonary disease: molecular mechanisms and therapeutic interventions. Ageing Res Rev. 2025;110:102813. doi:10.1016/j.arr.2025.102813
62. Cheung EC, Escobar JB, Alber BR, et al. Chronic intermittent hypoxia-mediated cognitive dysfunction in ovariectomized rats. Exp Physiol. 2025;110(8):1154–1163. doi:10.1113/ep092018
63. Durak B, Özol D, İ D, Saraç S. Is β- amyloid a reliable marker for assessing neurocognitive functions in middle-aged OSAS patients? Sleep Breathing. 2025;29(2):185. doi:10.1007/s11325-025-03353-9
64. Gupta MA, Simpson FC. Obstructive sleep apnea and psychiatric disorders: a systematic review. JCSM. 2015;11(2):165–175. doi:10.5664/jcsm.4466
65. Liu X, Wang H, Tian X, et al. Depression exacerbates AD pathology through lactate-dependent activation of microglial Kv1.3 to promote Aβ-containing exosome spreading. J Neuroinflam. 2025;22(1):166. doi:10.1186/s12974-025-03488-2
66. Majid H, Islam SU, Kohli S, Nidhi. Neuroinflammation and metabolic dysregulation as predictors of cognitive impairment, depression, and quality of life in type 2 diabetes mellitus patients on SGLT2 inhibitors and sulfonylureas. Inflammopharmacol. 2025;33(8):4749–4758. doi:10.1007/s10787-025-01824-9
67. Soltaninejad F, Golastaneh R, Ghahfarokhi PI, Salmasi M, Amra B. Continuous positive airway pressure treatment for sleep apnea in elderly patients systematic review and meta-analysis. Sleep Breathing. 2025;29(3):210. doi:10.1007/s11325-025-03362-8
68. Huang CG, Hsu JF, Chuang LP, et al. Adenotonsillectomy-related changes in systemic inflammation among children with obstructive sleep apnea. J Chin Med Assoc. 2023;86(6):596–605. doi:10.1097/jcma.0000000000000921
69. Archontogeorgis K, Nena E, Steiropoulos P. Roles of vitamins and nutrition in obstructive sleep apnea. Expert Rev Resp Med. 2025;19(2):145–163. doi:10.1080/17476348.2025.2462192
70. Kim AR, Jeon SG, Park SJ, et al. Alleviation of Adipose Tissue Inflammation and Obesity Suppression by a Probiotic Strain That Induces GLP-1 Secretion. Microorganisms. 2025;13(6):1211. doi:10.3390/microorganisms13061211
71. Bernard A, Richard C, Radoi L, Boidot R, Ledoux S, Besnard P. Fat taste sensitivity in women with obesity: transcriptomic analysis of fungiform papillae before and after bariatric surgery. Obesity. 2025;33(8):1518–1528. doi:10.1002/oby.24325
72. Ismael S, Umar M, Ouvrier B, et al. SARS-CoV-2 (MA10) Infection Aggravates Cerebrovascular Pathology in Endothelial Nitric Oxide Synthase-Deficient Mice. Viruses. 2025;17(6):784. doi:10.3390/v17060784
73. Andersen ML, Moyses-Oliveira M, Tufik S. Unlocking the role of Galectin-3: implications for sleep disorders and health. Sleep Med. 2024;124:110–114. doi:10.1016/j.sleep.2024.09.016
74. Sun X, Wang C, He Y, Chen K, Miao Y. Effect of inflammatory cytokines and plasma metabolome on OSA: a bidirectional two- sample Mendelian randomization study and mediation analysis. Front Immunol. 2024;15:1416870. doi:10.3389/fimmu.2024.1416870
75. Li B, Wang L, Du M, He H. FTO in oral diseases: functions, mechanisms, and therapeutic potential. FASEB J. 2024;38(20):e70115. doi:10.1096/fj.202401406RR
76. Li J, Sun L, Zhao Y. Advances in non-coding RNA as a biomarker for obstructive sleep apnoea hypoventilation syndrome. Sleep Breathing. 2024;28(5):1899–1908. doi:10.1007/s11325-024-03109-x
77. Nathalie P, Pauline G, Chloe M, et al. A pilot study on the effect of severe sleep fragmentation on aorta remodelling, neuroinflammation in a rat model. Sci Rep. 2025;15(1):27250. doi:10.1038/s41598-025-10721-8
78. Hao J, Zhao Y, Wang Z, et al. Circulating CHI3L1 autoantibodies serve as a diagnostic biomarker in patients with obstructive sleep apnea. Sci Rep. 2025;15(1):27087. doi:10.1038/s41598-025-11537-2
79. Puech C, Badran M, Barrow MB, Gozal D. Cognitive Function, Sleep, and Neuroinflammatory Markers in Mice Exposed to Very Long-Term Intermittent Hypoxia. Int J Mol Sci. 2025;26(5):1815. doi:10.3390/ijms26051815
80. Wei RM, Zhang MY, Fang SK, et al. Melatonin attenuates intermittent hypoxia-induced cognitive impairment in aged mice: the role of inflammation and synaptic plasticity. Psychoneuroendocrinology. 2025;171:107210. doi:10.1016/j.psyneuen.2024.107210
81. Lv R, Zhao Y, Wang X, et al. GLP-1 analogue liraglutide attenuates CIH-induced cognitive deficits by inhibiting oxidative stress, neuroinflammation, and apoptosis via the Nrf2/HO-1 and MAPK/NF-κB signaling pathways. Int Immunopharmacol. 2024;142(Pt B):113222. doi:10.1016/j.intimp.2024.113222
82. Altuna M, García-Sebastián M, Ecay-Torres M, et al. Prevalence and Misperception: exploring the Gap Between Objective and Subjective Assessment of Sleep Apnea in a Population at Increased Risk for Dementia. J Clin Med. 2025;14(8):2607. doi:10.3390/jcm14082607
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Study on Relationship Between Carotid Intima-Media Thickness and Inflammatory Factors in Obstructive Sleep Apnea
Ji P, Kou Q, Zhang J
Nature and Science of Sleep 2022, 14:2179-2187
Published Date: 14 December 2022
Lack of Clinical Control in COPD Patients Depending on the Target and the Therapeutic Option
Soler-Cataluña JJ, Huerta A, Almagro P, González-Segura D, Cosío BG
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1367-1376
Published Date: 6 July 2023
The Role and Mechanism of Metformin in Inflammatory Diseases
Lin H, Ao H, Guo G, Liu M
Journal of Inflammation Research 2023, 16:5545-5564
Published Date: 23 November 2023
Quercetin: A Flavonoid with Potential for Treating Acute Lung Injury

Huang M, Liu X, Ren Y, Huang Q, Shi Y, Yuan P, Chen M
Drug Design, Development and Therapy 2024, 18:5709-5728
Published Date: 6 December 2024
Clinical Features, Mechanisms, and Management of Anxiety in Youth with Tic Disorders: A Narrative Review
Zhang S, Han F, Chen J, Shen X, Li Y
Neuropsychiatric Disease and Treatment 2026, 22:582875
Published Date: 3 March 2026