Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Antibiotic Prescriptions in Hospitalized Patients with an Exacerbation COPD and a Proven Influenza or RS Virus Infection
Authors van Brummelen S, Tramper-Stranders G, Jonkman K, de Boer G, in 't Veen J ![]() , Braunstahl GJ
, Braunstahl GJ ![]()
Received 23 February 2022
Accepted for publication 19 May 2022
Published 1 June 2022 Volume 2022:17 Pages 1261—1267
DOI https://doi.org/10.2147/COPD.S361841
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Sigrid van Brummelen,1 Gerdien Tramper-Stranders,2 Kelly Jonkman,1 Geertje de Boer,1,3 Johannes in ’t Veen,1,3 Gert-Jan Braunstahl1,3
1Department of Pulmonology, Franciscus Gasthuis and Vlietland, Rotterdam, 3045 PM, the Netherlands; 2Department of Pediatrics, Franciscus Gasthuis and Vlietland, Rotterdam, 3045 PM, the Netherlands; 3Department of Pulmonology, Erasmus Medical Center, Rotterdam, 3015 GD, the Netherlands
Correspondence: Sigrid van Brummelen, Department of Pulmonology, Franciscus Gasthuis and Vlietland, Kleiweg 500, Rotterdam, 3045 PM, the Netherlands, Email [email protected]
Background: COPD exacerbations (AE-COPD) add up to over 200,000 hospitalization days annually in the Netherlands. Viral respiratory infections play a role in about half of COPD exacerbations. Although the prevalence of bacterial superinfection is estimated 10– 40% in admitted AE-COPD patients with an influenza infection, the majority is treated with antibiotics. Current national and international guidelines provide limited guidance regarding antibiotic use in hospitalized patients with an AE-COPD with proven viral respiratory pathogens.
Study Goal: We aimed to investigate antibiotic prescription in hospitalized patients with a COPD exacerbation and an influenza- or RS virus infection.
Patients and methods: We performed a retrospective cohort study in patients admitted with an AE-COPD and influenza- or RS virus infection. We compared clinical characteristics of patients with and without antibiotic treatment on admission and estimated adequacy of antibiotic prescriptions.
Results: We included 134 patients. Seventy-nine (59%) received antibiotics on admission. Chest X-ray infiltrates and plasma CRP level (≥ 50 mg/L) were correlated with the prescription of antibiotics. Outcomes, such as number of hospitalized days and mortality, were not significantly different between the groups with and without antibiotic treatment. Antibiotic treatment was considered “probably adequate” in 52/79 (65.8%) patients; “not necessary” in 12/79 patients (15.2%) and “probably not necessary” in another 15/79 patients (19.0%).
Conclusion: Prescription of antibiotics in hospitalized COPD patients is common practice despite a proven viral infection on admission. A significant antibiotic reduction of 34.2% in these patients seems feasible. Future guidelines should include recommendations regarding antibiotic stewardship in hospitalized patients with AE-COPD with a proven viral respiratory infection.
Keywords: COPD, exacerbation, influenza virus, antibiotic treatment, RS virus
Introduction
Annual epidemics of influenza and RS virus lead to considerable morbidity and mortality among COPD patients, despite an embedded influenza vaccination strategy.1 During each winter season in the pre COVID19 era COPD exacerbations (AE-COPD) add up to over 200.000 hospitalization days in the Netherlands.2
Data about the prevalence of bacterial superinfections in influenza patients are scarce and very heterogeneous. They are estimated to be present in 10–40% of all admitted influenza patients.3,4 No data are available for an estimation of the prevalence of bacterial superinfection in hospitalized COPD patients with a proven viral respiratory infection specifically. Furthermore, a golden standard for defining bacterial superinfection in an emergency room setting is lacking.
In the current Dutch guideline for hospitalized patients with an AE-COPD, antibiotics are recommended in case of clinical or radiological signs of bacterial infection and for consideration in patients with severely reduced FEV1, the elderly and in patients with severe comorbidity (all not specified). However, there are no specific recommendations on antibiotic treatment in AE-COPD patients with a proven viral respiratory infection, present in about 50% of these patients.5 Furthermore, the supposed possible beneficial effect of antibiotic treatment for the whole group of hospitalized AE-COPD patients is based only on two studies with a limited number of patients.6,7 The most recent international ATS/ERS guideline advises antibiotic prescription in ambulatory patients with an AE-COPD, but do not formulate any recommendation of antibiotic prescription in hospitalized patients, let alone in case of proven viral infection.8
Unnecessary antibiotic treatment contributes to antibiotic resistance, prolonged hospitalization, and unwanted side effects. Therefore, antibiotic prescriptions should be critically assessed in COPD patients, especially in those with proven viral infections. Hence, we aimed to investigate antibiotic prescriptions in hospitalized AE-COPD patients with a proven viral infection and to evaluate the necessity of those prescriptions.
Methods
Study Design
The local Research Ethics Committee (Medical research Ethics Committees United (MEC-U), Saint Antonius hospital Nieuwegein, W18.110) provided a waiver for formal ethical approval and informed consent for this retrospective study. The study was conducted in accordance with the principles of the Declaration of Helsinki and General Data Protection Regulation (GDPR).
Patients
We selected patients with assistance from our Business Intelligence department. We included COPD patients of all ages hospitalized for an AE-COPD with a confirmed influenza A or B- or RS virus infection using a point of care PCR test (Xpress Flu/RSV kit: GeneXpert Cepheid®). They were admitted in a large teaching hospital with two locations in the Netherlands during two consecutive winter seasons (2017/2018 and 2018/2019). Patients fulfilled the diagnosis of COPD according to the Global Initiative for Chronic Obstructive Lung Disease or had a doctor′s diagnosis from their general practitioner. In the first season, only influenza PCR was performed; in the second season RS virus PCR was added to the influenza PCR.
Exclusion criteria included the presence of a concomitant diagnosis of bronchiectasis, hypogammaglobulinaemia or other immune deficiency, lung cancer, thoracic cage deformity or a history of pneumonectomy.
Data
Data were collected from the electronic health patient files. All patient records were screened for eligibility and checked for meeting inclusion and exclusion criteria. Following data were anonymously entered in an electronic data capture system (CASTOR EDC): baseline demographics, medical history, COPD severity, co-morbidity, medication use, sputum cultures three months before admission, pre-treatment in primary care (antibiotics and prednisolone), symptoms, laboratory results (leucocyte count and CRP level), proven viral infection, antibiotic treatment, hospitalized days, ICU admission and death.
Possible determinants were defined for the prescription of antibiotics at presentation at the emergency department (ED). These were COPD severity, fever, increased sputum quantity or purulence, primary care antibiotic prescription, chest X-ray infiltrates and level of CRP on admission (cut-off 50 mg/L).
Following the Dutch national guideline, we defined antibiotic treatment to be “probably adequate” in case of an infiltrate on the chest X-ray and/or the presence of COPD Gold stage 4. Antibiotic treatment was considered “not necessary” in case of absence of an infiltrate on the chest X-ray, no COPD Gold 4 and a plasma CRP level < 50 mg/L. Daniels et al, the main study referred to in the Dutch national guideline, showed no beneficial effect of doxycycline in hospitalized AE-COPD patients with a plasma CRP level < 50 mg/L.7 In all other cases antibiotic treatment was considered “probably not necessary”, comprising a group of COPD patients with no COPD Gold 4, no infiltrate and a CRP level ≥ 50 mg/L. The choice of antibiotic was based on our local protocol and was mostly amoxicillin/ clavulanic acid or cefuroxime.
Analysis
Analysis was performed using SPSS version 26. We used Chi square tests for categorical data, unpaired t-tests or Mann–Whitney U-tests on numerical data depending on the data normality to analyze differences between the group with antibiotic treatment and without antibiotic treatment on admission. A binary logistic regression analysis was performed on the predefined possible determinants for starting antibiotics (severity of COPD, fever, sputum quantity and/ or purulence, chest X-ray infiltrates and CRP level).
Results
Baseline Characteristics and Demographic Data
We screened 146 eligible patients. Twelve patients were excluded due to wrong ICD coding (no COPD) or duplicate registration because of readmission (Figure 1). We selected 134 patients for analysis, from which 79 patients (59%) started or continued antibiotics.
 |
Figure 1 Selection of hospitalized COPD patients with an influenza or RS virus infection, divided in two groups with and without antibiotic treatment. |
Demographic data are shown in Table 1. There were no differences between the groups with or without antibiotics in duration of symptoms before admission, ICS use, coughing, sputum quantity, sputum purulence, fever, headache, muscle ache, prescribed antibiotics or prednisolone in primary care and blood eosinophil level on admission.
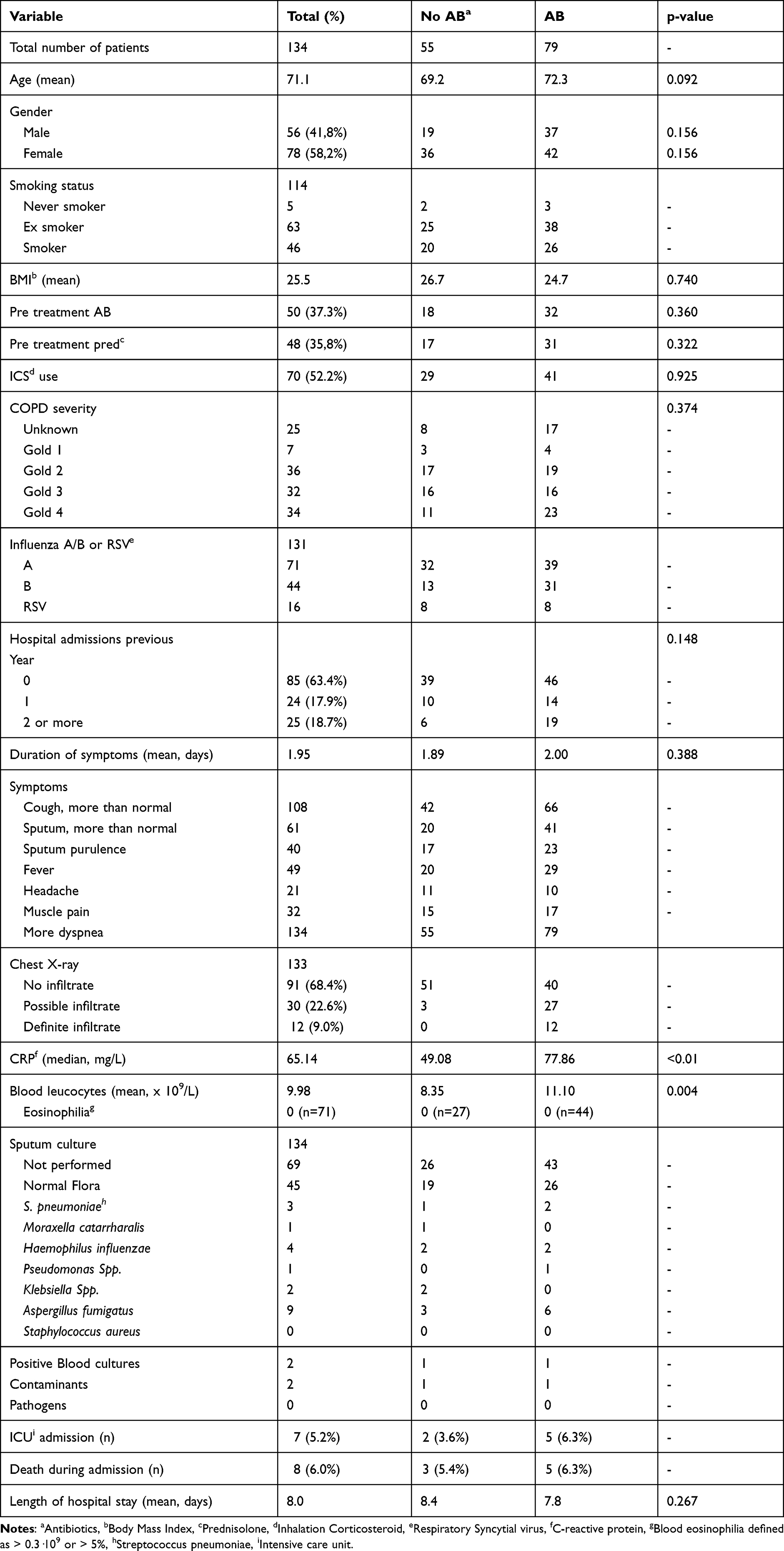 |
Table 1 Demographic Data and Clinical Characteristics |
There were no statistically significant differences in the group without versus with antibiotic treatment in terms of mean duration of hospitalization (8.4 vs 8.7 days, p= 0.267), ICU admissions (n=2 vs n=5) and mortality (n=3 vs n=5).
Predictive Factors for Antibiotic Prescription
In the group with antibiotic treatment there were more patients with a COPD Gold 4 or a COPD with unknown severity compared to the group without antibiotic treatment (67.6% vs 32.2%). The plasma CRP level was higher in the group with antibiotics compared to the group without antibiotics (median 77.86 mg/L vs 49.08 mg/L, p<0.01). Also there was a higher leucocyte count in the group with antibiotics (mean 11.10·109/L vs 8.35·109/L).
The presence of a chest X-ray infiltrate and a CRP level ≥ 50 mg/L were correlated with the prescription of antibiotics on admission (r=0.262 (p=0.01) and r=0.359 (p=0.01) respectively).
Justification of Antibiotic Prescription
We considered the feasibility of future reduction of antibiotic treatment in hospitalized AE-COPD patients with a proven viral infection. Antibiotics were prescribed in 27/79 (34.2%) patients without chest X-ray infiltrate and without COPD Gold 4. CRP levels were < 50 mg/L in about half of these cases (12/79 (15.2%)) (Table 2).
 |
Table 2 Presumed Necessity of Antibiotics Based on COPD Severity, Presence of an Infiltrate and CRPa Level |
In the three months before hospitalization there were positive sputum cultures in nine patients. This were all patients with a COPD Gold 3 or 4 or with a COPD of unknown severity. Three of these patients had a CRP level above 50 mg/L. Three patients were pre-treated with antibiotics, which were all continued on admission. In total, antibiotics were prescribed on admission in seven of these nine patients (including pre-treated patients).
Fifty patients (34.2%) were treated with antibiotics prior to hospitalization prescribed by their general practitioner. In 18 cases antibiotics were discontinued and in 32 cases antibiotics were continued. In most cases where antibiotics were discontinued there was absence of chest X-ray infiltrate (17/18), a low CRP level (14/18) or no COPD Gold 4 (17/18). In the group who continued prior antibiotics (N=32), 19 patients had a possible or definite infiltrate on the chest X-ray, 14 patients showed high CRP level on admission and 18 patients had a COPD Gold 4 or a COPD of unknown severity.
In our study, very few positive sputum culture results were found on and during admission, so this was not affecting antibiotic prescriptions (Table 1).
Summarizing, our results suggest unnecessary antibiotic prescriptions in 12/79 patients and another 15/79 probably unnecessary antibiotic prescriptions. Thus, we deem a reduction of 34.2% in antibiotic prescriptions possible in hospitalized patients with AE-COPD and a proven viral infection.
Discussion
We found a high antibiotic prescription rate in AE-COPD patients (59%) with a PCR confirmed influenza A/B or RS virus infection. The observed percentage of antibiotic treatment is much higher than the expected percentage of 10–40% bacterial superinfection in influenza patients based on available literature.3,4 Our study results therefore dispute the necessity of antibiotics in many hospitalized AE-COPD patients with a proven respiratory viral infection.
The Dutch national guideline on hospitalized AE-COPD patients recommends antibiotic treatment in patients with clinical or radiological evidence of a bacterial infection and to consider antibiotic treatment in COPD patients with a very severe COPD (FEV1< 30%), in the very elderly and in COPD with severe comorbidity. There are some smaller studies that suggest that antibiotic treatment leads to lower mortality and shorter admission time in hospitalized COPD patients with low FEV1 values <30%.5 The respiratory reserves in these patients are critical: “better be safe than sorry” is the adage. Outcomes in terms of hospitalized days, ICU admission and mortality did not differ between patients who did receive antibiotics and those who did not. Whether this is post aut propter antibiotic treatment remains unclear.
Unfortunately, there is no golden standard for diagnosing bacterial superinfection in the ER setting. The presence of chest X-ray infiltrate raises the suspicion of a secondary bacterial pneumonia, although infiltrates can also be seen in a primary viral pneumonia.
In a prospective trial of Prins et al, CRP is used as a biomarker to identify patients that can withheld antibiotic treatment. In patients with CRP level< 50 mg/L no antibiotics were given in the group with biomarker-guided treatment. Fewer patients in the CRP group were treated with antibiotics compared to the “GOLD” group in which antibiotic prescription was based on COPD Gold classification (31.7% versus 46.2%).9
Other studies showed a potential role for procalcitonin as well as CRP, but cut-off points should be carefully predetermined to optimize sensitivity and specificity of these tests.3,9–15 When we would have applied CRP guided treatment, as in the trial of Prins et al, this would have resulted in 47% antibiotic treatment in our study cohort instead of the present 59%. If we would have withheld antibiotic treatment in patients without chest X-ray infiltrate and COPD gold 4 and a CRP < 50 mg/L this would lead to withholding antibiotic treatment in twelve patients (15.2% reduction).
There are some limitations in this study, among other a limited sample size and its retrospective nature. Furthermore, in the first influenza season there were no RS virus results recorded so the percentage of RS virus infection is under-represented in the overall study population and might have caused some bias. In our judgement this bias was limited, and we attributed greater importance to a larger sample size than we would have had without the patients with RS virus infection.
In conclusion, we assume that a significant antibiotic reduction is safe in hospitalized COPD patients with a confirmed viral respiratory infection such as influenza of RS virus and contributes to the limitation of antibiotic resistance worldwide. In our opinion the recommendations on antibiotic treatment in hospitalized patients with AE-COPD in the current national and international guidelines should be overhauled for patients with a PCR proven viral respiratory infection.
Funding
No funding was received for this study.
Disclosure
Dr Johannes in ‘t Veen reports grants from Chiesi and Astra Zeneca; personal fees from Novartis and Sanofi, outside the submitted work. Dr Gert-Jan Braunstahl reports grants and/or personal fees from GSK, Sanofi, AstraZeneca, Chiesi, ALK ABello, Novartis, and Teva, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Thompson WW, Shay DK, Weintraub E, et al. Mortality associated with influenza and respiratory syncytial virus in the United States. JAMA. 2003;289(2):179–186. doi:10.1001/jama.289.2.179
2. LBZ. Ziekenhuisopnamen COPD. 2017; Available from: https://www.volksgezondheidenzorg.info/onderwerp/copd/preventie-zorg/zorg#node-ziekenhuisopnamen-copd.
3. Ahn S, Kim WY, Kim S-H, et al. Role of procalcitonin and C-reactive protein in differentiation of mixed bacterial infection from 2009 H1N1 viral pneumonia. Influenza Other Respir Viruses. 2011;5(6):398–403. doi:10.1111/j.1750-2659.2011.00244.x
4. Falsey AR, Becker KL, Swinburne AJ, et al. Bacterial complications of respiratory tract viral illness: a comprehensive evaluation. J Infect Dis. 2013;208(3):432–441. doi:10.1093/infdis/jit190
5. LAN/NVALT. Diagnostiek en behandeling COPD-longaanval in het ziekenhuis. 2017; Available from: https://richtlijnendatabase.nl/richtlijn/behandeling_copd-longaanval_in_het_ziekenhuis/startpagina_copd-longaanval_met_ziekenhuisopname.html.
6. Alonso Martinez JL, Rubio Obanos MT, Sampériz Legarre AL, et al. [Antibiotic treatment for acute episodes of chronic obstructive pulmonary disease]. An Med Interna. 1992;9(8):377–380. Spanish.
7. Daniels JM, Snijders D, de Graaff CS, et al. Antibiotics in addition to systemic corticosteroids for acute exacerbations of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2010;181(2):150–157. doi:10.1164/rccm.200906-0837OC
8. Wedzicha JA, Miravitlles M, Hurst JR, et al. Management of COPD exacerbations: a European Respiratory Society/American Thoracic Society guideline. Eur Respir J. 2017;49(3):1600791. doi:10.1183/13993003.00791-2016
9. Prins HJ, Duijkers R, van der Valk P, et al. CRP-guided antibiotic treatment in acute exacerbations of COPD in hospital admissions. Eur Respir J. 2019;53(5):1802014. doi:10.1183/13993003.02014-2018
10. Haran JP, Beaudoin FL, Suner S, et al. C-reactive protein as predictor of bacterial infection among patients with an influenza-like illness. Am J Emerg Med. 2013;31(1):137–144. doi:10.1016/j.ajem.2012.06.026
11. Bafadhel M, Clark TW, Reid C, et al. Procalcitonin and C-reactive protein in hospitalized adult patients with community-acquired pneumonia or exacerbation of asthma or COPD. Chest. 2011;139(6):1410–1418. doi:10.1378/chest.10-1747
12. Christ-Crain M, Jaccard-Stolz D, Bingisser R, et al. Effect of procalcitonin-guided treatment on antibiotic use and outcome in lower respiratory tract infections: cluster-randomised, single-blinded intervention trial. Lancet. 2004;363(9409):600–607. doi:10.1016/S0140-6736(04)15591-8
13. Mathioudakis AG, Chatzimavridou-Grigoriadou V, Corlateanu A, et al. Procalcitonin to guide antibiotic administration in COPD exacerbations: a meta-analysis. Eur Respir Rev. 2017;26(143):160073. doi:10.1183/16000617.0073-2016
14. Wu MH, Lin -C-C, Huang S-L, et al. Can procalcitonin tests aid in identifying bacterial infections associated with influenza pneumonia? A systematic review and meta-analysis. Influenza Other Respir Viruses. 2013;7(3):349–355. doi:10.1111/j.1750-2659.2012.00386.x
15. Stolz D, Christ-Crain M, Bingisser R, et al. Antibiotic treatment of exacerbations of COPD: a randomized, controlled trial comparing procalcitonin-guidance with standard therapy. Chest. 2007;131(1):9–19. doi:10.1378/chest.06-1500
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Pulmonologists’ Opinion on the Use of Inhaled Corticosteroids in Chronic Obstructive Pulmonary Disease Patients in Spain: A Cross-Sectional Survey
Miravitlles M, González-Torralba F, Represas-Represas C, Pomares X, Márquez-Martín E, González C, Amado C, Forné C, Alonso S, Alcázar B, Barrecheguren M, Jurado Mirete JM, Naval E
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1577-1587
Published Date: 12 July 2022
Lack of COPD-Related Follow-Up Visits and Pharmacological Treatment in Swedish Primary and Secondary Care
Sandelowsky H, Janson C, Wiklund F, Telg G, de Fine Licht S, Ställberg B
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1769-1780
Published Date: 9 August 2022
The Effect of Maintenance Treatment with Erdosteine on Exacerbation Treatment and Health Status in Patients with COPD: A Post-Hoc Analysis of the RESTORE Dataset

Calverley PMA, Papi A, Page C, Rogliani P, Dal Negro RW, Cazzola M, Cicero AF, Wedzicha JA
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1909-1920
Published Date: 22 August 2022
Cost-Effectiveness Analysis of Triple Therapy with Budesonide/ Glycopyrronium/ Formoterol Fumarate versus Dual Therapy in Patients with Chronic Obstructive Pulmonary Disease in Spain
Trigueros JA, Garin N, Baloira A, Aceituno S, Calvo A, Prades M, Touron C, Martínez A, Torres C
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2905-2917
Published Date: 15 November 2022
Recalibrating Perceptions and Attitudes Toward Nebulizers versus Inhalers for Maintenance Therapy in COPD: Past as Prologue
Dhand R, Hess MW, Yohannes AM
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:2571-2586
Published Date: 28 November 2024