")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Lack of COPD-Related Follow-Up Visits and Pharmacological Treatment in Swedish Primary and Secondary Care
Authors Sandelowsky H , Janson C , Wiklund F , Telg G , de Fine Licht S , Ställberg B
Received 26 April 2022
Accepted for publication 18 July 2022
Published 9 August 2022 Volume 2022:17 Pages 1769—1780
DOI https://doi.org/10.2147/COPD.S372266
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Zhang
Hanna Sandelowsky,1– 3 Christer Janson,4 Fredrik Wiklund,5 Gunilla Telg,6 Sofie de Fine Licht,6 Björn Ställberg7
1Department of Medicine, Solna, Division of Clinical Epidemiology, Karolinska Institutet, Stockholm, Sweden; 2Department of Neurobiology, Care Sciences and Society, Division of Family Medicine and Primary Care, Karolinska Institutet, Solna, Sweden; 3Academic Primary Health Care Centre, Region Stockholm, Stockholm, Sweden; 4Department of Medical Sciences: Respiratory, Allergy and Sleep Research, Uppsala University, Uppsala, Sweden; 5Statisticon AB, Uppsala, Sweden; 6AstraZeneca Nordic, Stockholm, Sweden; 7Department of Public Health and Caring Sciences, Family Medicine and Preventive Medicine, Uppsala University, Uppsala, Sweden
Correspondence: Hanna Sandelowsky, Department of Medicine, Solna, Division of Clinical Epidemiology, Karolinska Institutet, Stockholm, Sweden, Tel +46738902565, Email [email protected]
Objective: The Swedish guidelines recommend that patients with chronic obstructive pulmonary disease (COPD) on maintenance treatment are monitored annually, and within six weeks after an exacerbation. We describe the patterns of COPD-related visits in Sweden, both regular follow-up and post-exacerbation visits.
Methods: Patients (> 40 years) with a first-time COPD diagnosis between 2006 and 2017 were identified in primary care medical records and linked to hospital contacts and administered drug data. The index date was defined as the first collection of inhaled COPD maintenance treatment after the diagnosis. Regular COPD visits within 15-months after the index, and post-exacerbation visits for COPD within six weeks and 15-months after an exacerbation were estimated using the cumulative incidence function adjusted for competing risk. Visits without a ICD code for COPD were not included in the analyses.
Results: A total of 19,857 patients (mean age 69 years, 57% females) were included. The overall probability of having a regular follow-up visit for COPD within 15 months post-index was 39.1%. In total, 15,095 (76%) patients experienced at least one COPD exacerbation during the observation period. Among them, the probability of having a post-exacerbation visit was 7.0% within six weeks and 29.7% within 15-months. Patients without a regular COPD follow-up visit claimed significantly more oral corticosteroids (25.6% vs 15.6%), more respiratory antibiotics (39.1% vs 23.1%), and less maintenance treatment (10.9% vs 16.5%).
Conclusion: Only 39% of COPD patients attended a regular follow-up visit within 15-months from the COPD diagnosis and one-third had a post-exacerbation visit. The adherence to guideline recommendations need to be improved.
Keywords: COPD, follow-up visit, exacerbation, guidelines
Introduction
Chronic obstructive pulmonary disease (COPD) is a heterogeneous and progressive disease characterized by chronic airflow limitation.1,2 It affects approximately 384 million people worldwide.1 Multimorbidity is prevalent in people with COPD.3–5 Especially, cardiovascular disease is common, and known to be associated with an increased risk of hospitalization and mortality.6
In Sweden, most patients with COPD are managed in primary care. The importance of routine follow-ups (annual COPD reviews) is highlighted in guidelines.1,7 COPD patient reviews should include monitoring of the frequency and types of exacerbations, changes in dyspnea, activity limitations, sleep disturbances, fatigue, signs of chronic bronchitis and smoking status. Additionally, inhaled treatment should be monitored including a control of the inhaler technique, and appropriate adjustments to the pharmacological treatment should be made. A routine, regular follow-up visit should also include spirometry to identify patients with fast decline of lung function (“rapid decliners”), as these patients have a particularly poor prognosis. According to the Swedish guidelines, patients who have had a COPD exacerbation should be followed up within 6 weeks.7 The importance of postexacerbation visits has also been highlighted by European COPD experts in a Europe-wide consensus report.8 Frequent outpatient visits have been reported to be an independent factor for preventing COPD exacerbations.9
The aim of this study was to describe the patterns of COPD-related follow-up visits in primary and secondary care in Sweden, both regarding regular follow-up visits and post-exacerbation follow-up visits in a COPD population treated with inhaled maintenance medications, and to relate the findings to applicable COPD management guidelines. In addition, the study aimed to describe the patterns of pharmacological treatments in COPD patients with and without follow-up visits.
Materials and Methods
In this observational cohort study, COPD patients were identified in primary care medical records and linked to the National Patient Registry and the Swedish Prescribed Drug Registry by the Swedish National Board of Health and Welfare. The primary health-care centers that were included in the study were either publicly funded (Region Stockholm) or both publicly and privately funded (Region Uppsala), and covered approximately 2.7 million inhabitants. The linked database was managed by the Department of Medical Sciences, Respiratory Medicine at Uppsala University, Sweden. The study protocol was reviewed and approved by the regional ethics committee in Uppsala, Sweden (reference number 2016/486).
Study Population
The study included patients with a recorded COPD diagnosis between January 2006 and December 2017. The index date was defined as the first collection of an inhaled COPD maintenance treatment after the COPD diagnosis (Supplementary Figure 1). All patients aged >40 years with a diagnosis of COPD (ICD-10 J45) registered in primary care medical records (as well as in secondary care in Region Uppsala), who had had at least one collection of inhaled COPD maintenance treatments (long-acting β-agonists [LABA], long-acting muscarinic antagonists [LAMA], inhaled corticosteroids [ICS] or any combination of these) after the diagnosis of COPD was registered were included. Patients who had a record of a COPD diagnosis prior to 2006 and patients who were not residents in either of the two regions at the index date were excluded. Also, patients with comorbid diseases commonly treated with oral corticosteroids (OCS) (Crohn’s disease, ulcerative colitis, rheumatoid arthritis or polymyalgia rheumatica), and patients with malignant neoplasm (except for basal cell carcinoma) during the year before the index date were excluded.
Outcomes and Variables
The primary outcome was COPD-related visits to either a primary care nurse or physician, or an outpatient visit in secondary care. These visits were defined as visits with a COPD diagnosis code registered in the medical records or registries. The number of regular COPD follow-up visits within the 15-month period after the index date was described. Additionally, the number of post-exacerbation visits due to COPD were collected both within six weeks and 15 months after an acute exacerbation. Acute visits in primary care that resulted in collection of OCS and/or antibiotics on the same day and visits without a ICD code for COPD were not included in the analyses.
Moderate exacerbations were defined as COPD-related emergency room visits and/or administration of OCS and/or respiratory antibiotics. Severe exacerbations were defined as COPD-related hospitalizations. Recurrent exacerbations within 14 days were combined and considered as one exacerbation.
COPD medications were identified in the Prescribed Drug Registry (ATC codes) as collections of prescribed medications.
Comorbidities were identified from the available data up to five years prior to the index date by using ICD-10 codes. The Charlson comorbidity index was calculated at index date and date of first exacerbation for each patient using the ICD-10 coding algorithm developed by Quan et al10,11 by summing the weighted scores for all comorbidities. All comorbidities were retrieved one year prior to index and first exacerbation.
Statistical Analyses
Baseline characteristics were described as mean (standard deviation [SD]) for continuous variables and absolute and relative frequencies for categorical variables. For each individual, the follow-up period for regular follow-up visits started on the index date (first inhaled medication collection) and ended after 15 months. Two follow-up periods for post-exacerbation visits were studied: one started on the registered date of the exacerbation and ended six weeks later, and the other started on the registered date of the exacerbation and ended 15 months later. To evaluate the proportion of patients who had had regular follow-up visits within 15 months, the probability of regular and post-exacerbation visits was estimated using the cumulative incidence function with corresponding 95% confidence intervals (CI) adjusting for competing risk of exacerbation and death.12
To explore the effects of sex and age (40–55, >55–70, >70–85, >85) on regular follow-up visits, the calendar year was used as a continuous variable and the incidence rate ratios (IRR) of follow-up visits with 95% CI were calculated using a negative binomial regression model.
When assessing number of regular COPD follow-up visits after index date, patients were censored at the time of first exacerbation. Similarly, patients were censored at the time of second exacerbation when assessing number of post-exacerbation visits after the first exacerbation.
Post-exacerbation follow-up visits after moderate and severe exacerbations were analyzed separately.
Time trends in regular follow-up visits and post-exacerbation follow-up visits were explored by calculating the probability of a visit within 15 months for each year separately (2006–2017) using the cumulative incidence function with 95% CIs.
Results
A total of 19,857 patients (mean age 69 years, 57% females) with a first-time diagnosis of COPD in primary care (n = 10,464) or secondary care (n = 9393) between 2006 and 2017 were included at the date of the first collection of inhaled maintenance treatment after the diagnosis (ie, the index date) (Table 1). At the index date (baseline), the majority of patients (45.5%) collected a LABA or a LAMA. A combination of LABA, LAMA, and ICS, either in fixed combination or separate inhalers, was collected by 10.6%. The most common comorbidities were hypertension (47.4%), asthma (20.1%), upper respiratory tract infections (18,1%), metabolic disorders (17.7%) and pneumonia (15.4%) (Table 1). A Charlson comorbidity index of two or more was observed in 41.8% of the patients. Overall, 1054 (5.3%) of the patients had less than 15 months of follow-up: 695 (3.5%) died, 143 (0.7%) emigrated and 216 (1.1%) developed OCS-related diseases.
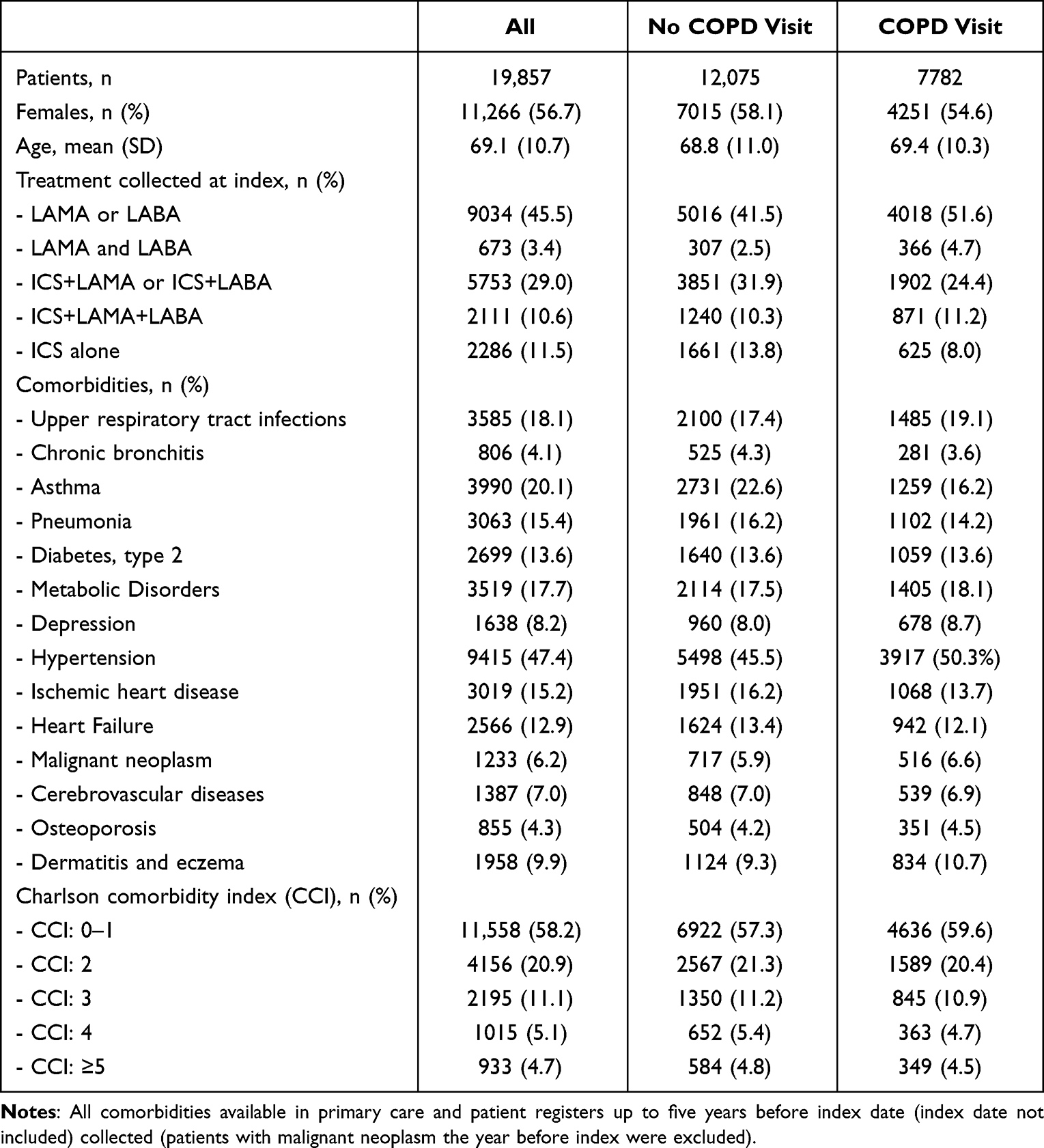 |
Table 1 Baseline Characteristics of the Study Population |
Regular Follow-Up Visits
During the 15-month follow-up period after the index date, 7782 of 19,857 patients had at least one regular follow-up visit with a COPD diagnosis. Of these patients, 3824 had two or more visits (Table 2). The overall probability of having a regular follow-up visit within 15 months post-index was 39.1% (95% CI: 38.4–39.7). The majority of these visits occurred in primary care (35.7%, 95% CI: 35.0–36.3) (Figure 1). Male sex, increasing age, the Charlson comorbidity index equal to or more than five, and the year of inclusion were associated with a higher probability (expressed as incidence rate ratio [IRR]) of regular follow-up visits after the index date (Supplementary Table 1). The probability of having a regular follow-up visit did not increase markedly when the observation period was extended from 15 to 30 months (44.9%, 95% CI: 44.2–45.6) (Figure 1).
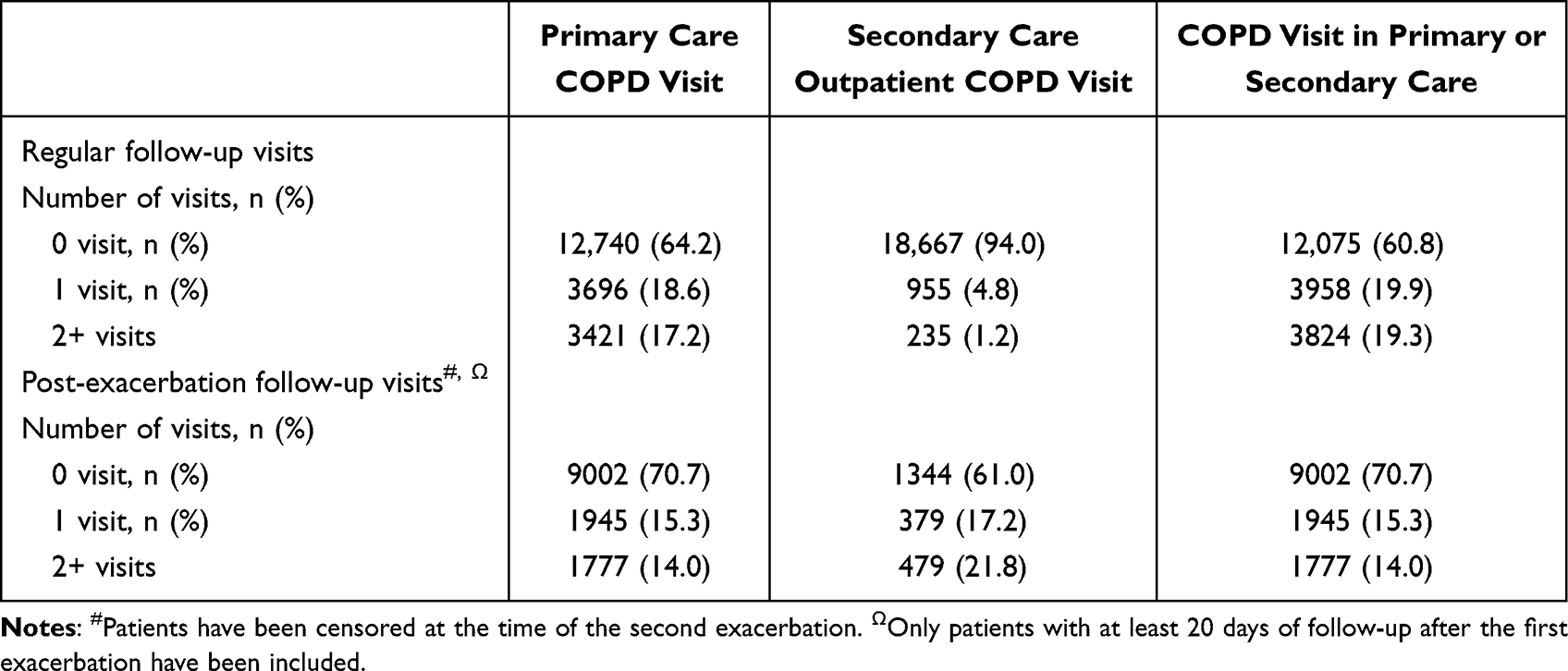 |
Table 2 Regular Follow-Up Visits for COPD (Within 15 Months Post-Index) and Post-Exacerbation Visits (Within 15 Months Post-Exacerbation) in Primary and Secondary Care and in Total |
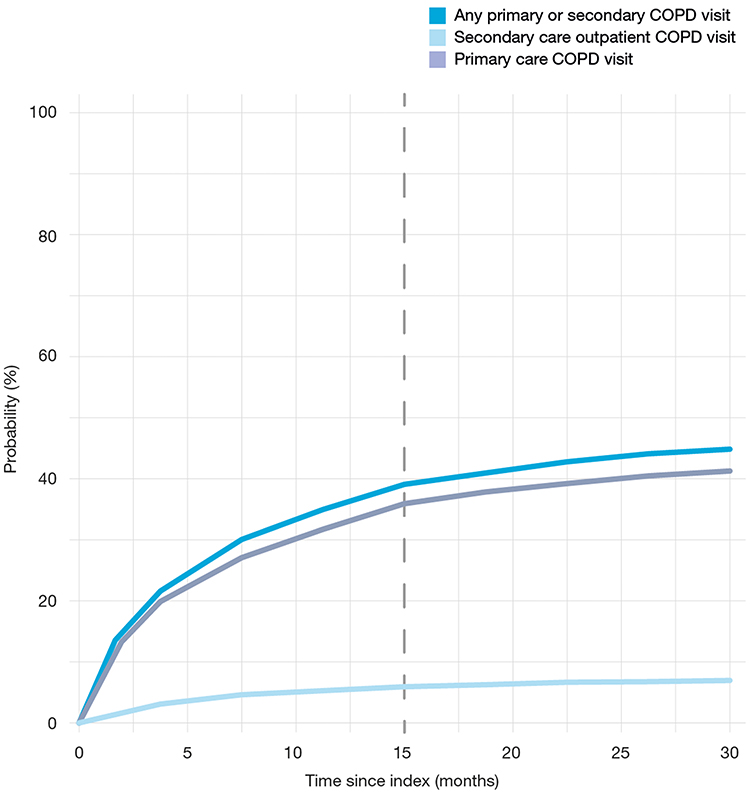 |
Figure 1 Probability of COPD-related follow-up visit after index date accounting for competing risks (exacerbation and death). |
Post-Exacerbation Visits
In total, 15,095 (76%) of the 19,857 COPD patients experienced at least one moderate or severe COPD exacerbation during the observation period. Of those experiencing an exacerbation, 11,732 (78%) also experienced a second exacerbation (58% of all patients). The median time from the index date to the first COPD exacerbation was 12.0 months (IQR 3.8–28.6), and from the first to the second exacerbation 7.0 months (IQR 2.3–17.7). Of patients with a first exacerbation, 3352 (22.2%) died within 15 months after the exacerbation.
In patients who experienced a first COPD exacerbation, the overall probability of having a post-exacerbation visit within six weeks was 7.0%. After a moderate exacerbation, this probability was 6.2% (95% CI: 5.8–6.6%) and after a severe exacerbation 11.9% (95% CI: 10.6–13.3%). The overall probability of having a post-exacerbation follow-up visit within 15 months was 29.7%. After a moderate exacerbation, this probability was 28.4% (95% CI: 27.6–29.2) (Figure 2A) and after a severe exacerbation 36.9% (95% CI: 34.9–39.0 (Figure 2B). Of patients who had a post-exacerbation follow-up visit within 15 months, 3722 (25%) had had at least one, and 1777 (12%) two or more such visits.
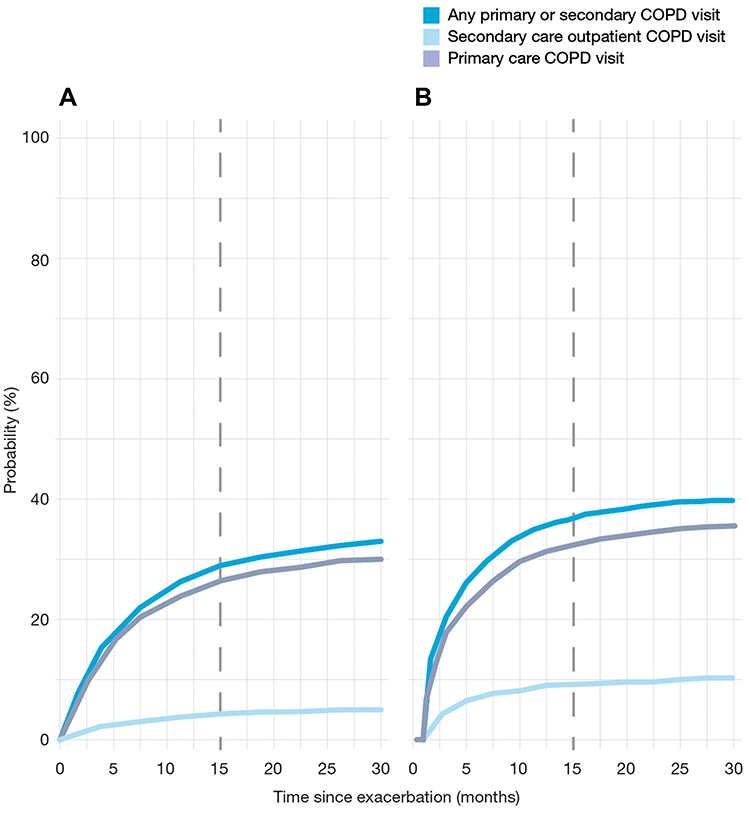 |
Figure 2 Probability of COPD-related follow-up visit after the first exacerbation (A) moderate, (B) severe) accounting for competing risks (exacerbation and death). |
Patients with severe exacerbations had a higher probability of having a post-exacerbation follow-up visit within 15 months than those with moderate exacerbations. Male sex, increasing age, the Charlson comorbidity index equal to or more than five, the year of inclusion, and treatments with LAMA+LABA or ICS+LABA+LAMA were associated with a higher probability of post-exacerbation visits (Supplementary Table 1). The overall probability of having a visit after a COPD exacerbation increased slightly (from 29.7% to 33.7%, p < 0.001) when the observation period was extended from 15 to 30 months (Figure 2).
Changes in Visit Patterns Over 10 Years
The probability of having at least one regular follow-up visit within 15 months after the index date increased from 17.4% in 2006 to 53.4% in 2017 (Figure 3). In the same time period, the probability of having a post-exacerbation follow-up visit increased from 11.0% to 38.3% (data not shown in Figure 3). The probability of having a moderate to severe exacerbation decreased from 54.8% to 40% (Figure 3).
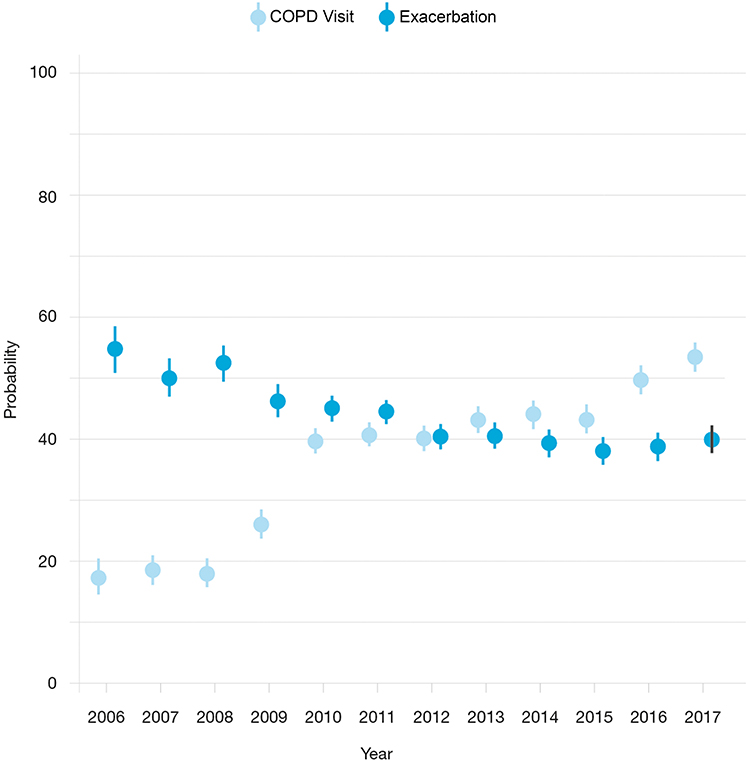 |
Figure 3 Probability of COPD follow-up visits and exacerbation within 15 months after the event, across calendar year accounting for competing risks (exacerbation and death). |
Pharmacological Treatment
At the index date, all patients collected an inhaled maintenance treatment. In the last three months of the 15 month follow-up period, the proportion of patients collecting these treatments had decreased to 59% (Figure 4). At the index date, 24% of the patients collected a combination of LABA + LAMA + ICS. This proportion decreased to 16% the last three months of the follow-up period (Figure 4). The proportion of patients without any collection of maintenance treatment after the index date was higher in patients without regular follow-up visits (Figure 4A) than in patients with a visit (16.5% vs 10.9%, p < 0.001) (Figure 4B). Additionally, patients without regular follow-up visits claimed more OCS (25.6% vs 15.6%, p < 0.001) and more respiratory antibiotics (39.1% vs 23.1%, p < 0.001) than patients who had a regular follow-up visit within 15 months after the index (data not shown in Figure 4).
 |
Figure 4 COPD treatment patterns during follow-up at 0–3, 3–6, 6–9, 9–12 and 12–15 months after index date stratified by (A) without COPD visit (n=11,387) and (B) with COPD visit (n=7416). |
Discussion
In this Swedish study of almost 20,000 patients with COPD, we found that the probability of having a regular follow-up visit either in primary or secondary care within 15 months after the patient had started a maintenance inhaled medication (the index date) was 39%. The vast majority of visits, 36%, were conducted in primary care. Three of four patients experienced a COPD exacerbation within 15 months after the index date. The overall probability of a post-exacerbation follow-up visit within six weeks was 7.0% and within 15 months it was 29.7%. Patients without a follow-up visit collected less ICS, and more OCS and respiratory antibiotics than patients with a visit. Although approximately 75% of the patients had experienced a COPD exacerbation, less than one-fourth collected pharmacological treatment with a LAMA+LABA+ICS combination. However, a positive finding in this study was that the probability of having any kind of COPD-related visit increased from 2006 to 2017. Simultaneously, the proportion of patients who experienced a COPD exacerbation decreased.
Although the overall probability of any follow-up visit was low, an alarming finding was that the probability of attending a post-exacerbation follow-up visit was lower than that of a regular (annual) follow-up visit. One possible explanation to this is that more than 20% of patients who exacerbated died during the 15-month observation time, which illustrates the prognostic severity related to COPD exacerbations.13,14 The probability of having a medical review of COPD within six weeks after an exacerbation was very low. In fact, when prolonging the follow-up to 15 months after the exacerbation, only 37% of the patients with a severe exacerbation and even fewer of those with a moderate exacerbation had had a follow-up visit regardless of whether they were seen at primary or secondary care. Our findings are in line with a recent study from Sweden that showed that less than 30% of the patients had an outpatient secondary care follow-up visit within the first year after they have been hospitalized due to a severe COPD exacerbation.15 A follow-up visit provides the physician or the COPD nurse the opportunity to evaluate symptoms and treatment effects, assess future risks, and make necessary adjustments to the treatment, including management of comorbidities. Additionally, patient’s subjective physical, emotional, and social needs can be addressed, thus laying ground for person-centered care.16 Feelings of loss, hopelessness, and uncertainty are common particularly after an acute exacerbation, increasing patients’ call for support at these times.17 Moreover, COPD exacerbations lead to impaired quality of life,18 and an increased risk of developing depression and/or anxiety,19 which should be monitored by health-care professionals. There is a strong evidence that continuity of care plays a key role in preventing COPD exacerbations and improving both health status and quality of life.20–23 A structured, inter-professional COPD management, including follow-up visits as recommended by the guidelines leads to improved health status and fewer exacerbations.20 However, most primary health-care centers do not offer their patients such specialized COPD care. In fact, COPD is often undertreated and undermanaged in primary care.20,24 Moreover, managing multimorbidity is a complex task and may often lead to de-prioritization of COPD in clinical practice.25 Under these circumstances, adhering to guideline recommendations about reviewing COPD patients may be difficult.
Patients with regular follow-up visits used more inhaled maintenance treatments and less OCS and antibiotics treatments than those without regular visits, which can be attributed to the lower rate of exacerbations in patients who had been regularly reviewed by their physicians/nurses. By definition, all patients in our study population were on maintenance treatment with inhaled LAMA, LABA and/or ICS at the index. However, our findings indicate that patients were generally undertreated with inhaled medications. This is in line with findings from a Swedish primary care study from the same time period as our study: 35% of the COPD patients had no maintenance treatment.26 As prescriptions of medications for chronic diseases in Sweden are usually issued for 12 months with collections at the pharmacy every third month, changes in medications found by analyzing the data from the Prescribed Drug Registry do not have to involve a patient visit or other contact with the prescriber. At the end of the 15-month observation time, only 59% of the patients in our study had collected any medication for maintenance treatment during the preceding three months. Similar phenomena of undertreatment have previously been observed in asthma studies.27–29
More than 75% of the patients in our study population had at least one moderate or severe exacerbation during the observation period of 15 months. The high prevalence of exacerbations in COPD populations who are on maintenance treatments has been demonstrated in previous studies.30,31 However, less than one-fourth of the patients in our study had treatment with LAMA+LABA+ICS. This so-called triple therapy has been shown to lead to a significant reduction of exacerbations and mortality when compared to dual therapies with LABA/LAMA or ICS/LABA.32,33 It is crucially important to monitor and adjust the patient’s treatment after an exacerbation and thus optimize the pharmacological and non-pharmacological treatment improve chances to prevent future exacerbations as the mortality risk increases rapidly by each exacerbation.13,14 In a 2020 Swedish study, only 42% of the patients, who had been hospitalized due to a severe COPD exacerbation, received treatment escalation to prevent future exacerbations.15 Furthermore, patients whose medication optimization is delayed experience a greater risk of future exacerbations and significant higher risk of future exacerbations, hospitalizations and higher comorbidity burden than patients whose pharmacotherapy is optimized within 30 days after the exacerbation.34–36
In the present study, we found that the proportion of COPD patients that had regular follow-up visits and post-exacerbation visits increased from 2006 to 2017. In parallel, the proportion of patients having an exacerbation decreased. This positive development is in line with what has previously been reported for the time period between 1999 and 2009 in the Swedish PATHOS study.37 One explanation for this positive development may be that the update of the Swedish national guidelines for COPD management was published in 2015,7 which contributed to increased awareness of COPD in health-care professionals and the patients.
COPD with multiple chronic comorbidities is associated with impaired health status, increased risk of exacerbations, and increased mortality.38,39 Multimorbidity often contributes to problems with guideline adherence and thus complexity in the management of COPD, thus increasing the need of individualized care. In our study, only a high Charlson comorbidity index (equal to or more than five, ie, a heavy multimorbidity burden) was associated with an increased probability of having a regular or post-exacerbation follow-up visit related to COPD. This suggests that the vast majority of patients with COPD in our study, who have a moderate burden of comorbidity, are not sufficiently reviewed regarding their COPD. Whether COPD reviews are de-prioritized in primary care at the expense of reviews of other common chronic diseases was not the scope of this paper but would be an interesting subject of future research.
A strength of this study was that we were able to study a large, unselected, and population-based cohort of COPD patients, which enabled exploring real-world data from both primary and secondary care. Primary care electronic medical records data were linked with national health-care registries with high quality and coverage, thus providing solid and unique data, although clinical data, such as lung function values and information about smoking and cough, were not available.
This study also comes with some methodological limitations. Acute visits in primary care without a collection of OCS and/or an antibiotic at the same day were regarded as regular visits, as the ICD-10 code for acute exacerbation (J441) is normally not used in Swedish primary care settings. This may potentially have led to an over-estimate of the regular follow-up visits. On the other hand, some COPD reviews and prescriptions may have taken place over remote consultations, visits may have occurred outside the regions that were included in our study, and visits may have been misclassified or taken place without registration of a COPD diagnosis. Any of these courses of events could have contributed to an under-estimation of the number of follow-up visits. However, we assess that such possible biases were not likely to be of significance as the reimbursement system in Swedish primary care gives a strong incentive for GPs to register all diagnoses in the medical records at every visit. Finally, as always in observational studies like this, the level of actual use of medication remains unknown.
Conclusions
We found that only two in five of the COPD patients had a regular follow-up visit for COPD within 15-months, and only one-third had a post-exacerbation visit. COPD was generally undertreated and undermanaged. The adherence to the recommendations of global and national guidelines was thus insufficient. Our results highlight the need for improved adherence to guidelines to optimize COPD care.
Abbreviation
ATC, Anatomical Therapeutic Chemical code; CCI, Charlson Comorbidity Index; CI, Confidence Intervals; COPD, Chronic Obstructive Pulmonary Disease; ICD, International Classification of Diseases; ICS, Inhaled corticosteroids; IQR, Interquartile Range; IRR, Incidence Rate Ratio; LABA, Long, acting β, agonists; LAMA, Long, acting muscarinic antagonists; OCS, Oral corticosteroids; SD, Standard Deviation.
Data Sharing Statement
The dataset supporting the conclusions of this article can be available upon request.
Ethics Approval and Informed Consent
This study was performed in accordance with applicable legislation on non-interventional studies and/or observational studies. The study was approved by the Uppsala regional ethics committee (reference number 2016/486). The linkage of registers data was approved and performed by the Swedish National Board of Health and Welfare. Individual patient consents to participate were not collected as they are not required in Sweden when de-identified public register data is used for research.
Consent for Publication
All authors read and approved the final manuscript. All authors gave consent to publish these data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was sponsored by AstraZeneca.
Disclosure
GT and SdFL are employed by AstraZeneca. SdFL has private stock ownership in AstraZeneca. FW is employed at Statisticon for which AstraZeneca is a client.
CJ has received payments for educational activities from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Novartis, and Teva, and has served on advisory boards arranged by AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Novartis, and Teva.
BS has received honoraria for educational activities and lectures from AstraZeneca, Boehringer Ingelheim, Chiesi, Meda, Novartis and Teva, and has served on advisory boards arranged by AstraZeneca, Novartis, Meda, GlaxoSmithKline, Teva and Boehringer Ingelheim.
HS has received honoraria for educational activities from Boehringer Ingelheim, Novartis, AstraZeneca, Chiesi, and TEVA, an unrestricted research grant from AstraZeneca, and has served on advisory boards arranged by AstraZeneca, Novartis, Chiesi, and GlaxoSmithKline. The authors report no other conflicts of interest in this work.
References
1. Global Initiative for Chronic Obstructive Lung Disease. 2020 Report: global strategy for the diagnosis, management and prevention of COPD; 2020. Available from: https://goldcopd.org.
2. Calverley P, Bellamy D. The challenge of providing better care for patients with chronic obstructive pulmonary disease: the poor relation of airways obstruction? Thorax. 2000;55(1):78–82. doi:10.1136/thorax.55.1.78
3. Chetty U, McLean G, Morrison D, et al. Chronic obstructive pulmonary disease and comorbidities: a large cross-sectional study in primary care. Br J Gen Pract. 2017;67(658):e321–e328. doi:10.3399/bjgp17X690605
4. Sin DD, Anthonisen NR, Soriano JB, et al. Mortality in COPD: role of comorbidities. Eur Respir J. 2006;28(6):1245–1257. doi:10.1183/09031936.00133805
5. Andell P, Koul S, Martinsson A, et al. Impact of chronic obstructive pulmonary disease on morbidity and mortality after myocardial infarction. Open Heart. 2014;1(1):e000002. doi:10.1136/openhrt-2013-000002
6. Divo M, Cote C, de Torres JP, et al. Comorbidities and risk of mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186(2):155–161. doi:10.1164/rccm.201201-0034OC
7. National Board of Health and Welfare. Nationella riktlinjer för astma och KOL; 2020. Available from: www.socialstyrelsen.se.
8. Ramakrishnan S, Janssens W, Burgel P-R, et al. Standardisation of clinical assessment, management and follow-up of acute hospitalised exacerbation of COPD: a Europe-Wide Consensus. Int J Chron Obstruct Pulmon Dis. 2021;16:321–332. doi:10.2147/COPD.S287705
9. Park HJ, Byun MK, Kim T, et al. Frequent outpatient visits prevent exacerbation of chronic obstructive pulmonary disease. Sci Rep. 2020;10(1):6049. doi:10.1038/s41598-020-63064-x
10. Quan H, Li B, Couris CM, et al. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am J Epidemiol. 2011;173(6):676–682. doi:10.1093/aje/kwq433
11. Quan H, Sundararajan V, Halfon P, et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care. 2005;43(11):1130–1139. doi:10.1097/01.mlr.0000182534.19832.83
12. Fine JP, Gray RJ. A proportional hazards model for the subdistribution of a competing risk. J Am Stat Assoc. 1999;94(446):496–509. doi:10.1080/01621459.1999.10474144
13. Larsson K, Janson C, Lisspers K, et al. The impact of exacerbation frequency on clinical and economic outcomes in Swedish COPD patients: the arctic study. Int J Chron Obstruct Pulmon Dis. 2021;16:701–713. doi:10.2147/COPD.S297943
14. Rothnie KJ, Müllerová H, Smeeth L, et al. Natural history of chronic obstructive pulmonary disease exacerbations in a general practice-based population with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;198(4):464–471. doi:10.1164/rccm.201710-2029OC
15. Janson C, Nwaru BI, Wiklund F, et al. Management and risk of mortality in patients hospitalised due to a first severe COPD exacerbation. Int J Chron Obstruct Pulmon Dis. 2020;15:2673–2682. doi:10.2147/COPD.S276819
16. Fawcett J. The metaparadigm of nursing: present status and future refinements. Image J Nurs Sch. 1984;16(3):84–89. doi:10.1111/j.1547-5069.1984.tb01393.x
17. Rosa F, Bagnasco A, Ghirotto L, et al. Experiences of older people following an acute exacerbation of chronic obstructive pulmonary disease: a phenomenological study. J Clin Nurs. 2018;27(5–6):e1110–e1119. doi:10.1111/jocn.14189
18. Camac ER, Voelker H, Criner GJ. Impact of COPD exacerbations leading to hospitalization on general and disease-specific quality of life. Respir Med. 2021;186:106526. doi:10.1016/j.rmed.2021.106526
19. Long J, Ouyang Y, Duan H, et al. Multiple factor analysis of depression and/or anxiety in patients with acute exacerbation chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2020;15:1449–1464. doi:10.2147/COPD.S245842
20. Lisspers K, Johansson G, Jansson C, et al. Improvement in COPD management by access to asthma/COPD clinics in primary care: data from the observational PATHOS study. Respir Med. 2014;108(9):1345–1354. doi:10.1016/j.rmed.2014.06.002
21. Swanson JO, Vogt V, Sundmacher L, et al. Continuity of care and its effect on readmissions for COPD patients: a comparative study of Norway and Germany. Health Policy. 2018;122(7):737–745. doi:10.1016/j.healthpol.2018.05.013
22. Lin IP, Wu SC, Huang ST. continuity of care and avoidable hospitalizations for chronic obstructive pulmonary disease (COPD). J Am Board Fam Med. 2015;28(2):222–230. doi:10.3122/jabfm.2015.02.140141
23. Hsieh PL, Yang FC, Hu YF, et al. Continuity of care and the quality of life among patients with Type 2 diabetes mellitus: a cross-sectional study in Taiwan. Healthcare. 2020;8:486.
24. Spyratos D, Chloros D, Michalopoulou D, et al. Underdiagnosis, false diagnosis and treatment of COPD in a selected population in Northern Greece. Eur J Gen Pract. 2021;27(1):97–102. doi:10.1080/13814788.2021.1912729
25. Sandelowsky H, Hylander I, Krakau I, et al. Time pressured deprioritization of COPD in primary care: a qualitative study. Scand J Prim Health Care. 2016;34(1):55–65. doi:10.3109/02813432.2015.1132892
26. Sundh J, Åberg J, Hasselgren M, et al. Factors influencing pharmacological treatment in COPD: a comparison of 2005 and 2014. Eur Clin Respir J. 2017;4(1):1409060. doi:10.1080/20018525.2017.1409060
27. Rabe KF, Vermeire PA, Soriano JB, et al. Clinical management of asthma in 1999: the Asthma Insights and Reality in Europe (AIRE) study. Eur Respir J. 2000;16(5):802–807. doi:10.1183/09031936.00.16580200
28. Janson C, Accordini S, Cazzoletti L, et al. Pharmacological treatment of asthma in a cohort of adults during a 20-year period: results from the European Community Respiratory Health Survey I, II and III. ERJ Open Res. 2019;5(1):00073–2018. doi:10.1183/23120541.00073-2018
29. Ekström M, Nwaru BI, Wiklund F, et al. Risk of rehospitalization and death in patients hospitalized due to asthma. J Allergy Clin Immunol Pract. 2021;9(5):1960–1968.e4. doi:10.1016/j.jaip.2020.12.030
30. Hurst JR, Vestbo J, Anzueto A, et al. Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) Investigators; Susceptibility to exacerbation in chronic obstructive pulmonary disease. New Engl J Med. 2010;363(12):1128–1138. doi:10.1056/NEJMoa0909883
31. Tashkin DP, Celli B, Senn S, et al. A 4-year trial of tiotropium in chronic obstructive pulmonary disease. N Engl J Med. 2008;359(15):1543–1554. doi:10.1056/NEJMoa0805800
32. Lipson DA, Barnhart F, Brealey N, et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N Engl J Med. 2018;378(18):1671–1680. doi:10.1056/NEJMoa1713901
33. Rabe KF, Martinez FJ, Ferguson GT, et al. Triple inhaled therapy at two glucocorticoid doses in moderate-to-very-severe COPD. N Engl J Med. 2020;383(1):35–48. doi:10.1056/NEJMoa1916046
34. Tkacz J, Evans KA, Touchette DR, et al. PRIMUS - Prompt initiation of maintenance therapy in the US: a real-world analysis of clinical and economic outcomes among patients initiating triple therapy following a COPD exacerbation. Int J Chron Obstruct Pulmon Dis. 2022;17:329–342. doi:10.2147/COPD.S347735
35. Bogart M, Glassberg MB, Reinsch T, et al. Impact of prompt versus delayed initiation of triple therapy post COPD exacerbation in a US-managed care setting. Respir Med. 2018;145:138–144. doi:10.1016/j.rmed.2018.10.013
36. Coutinho AD, Lokhandwala T, Boggs R, et al. Prompt initiation of maintenance treatment following a COPD exacerbation: outcomes in a large insured population. Int J Chron Obstruct Pulmon Dis. 2016;11:1223–1231. doi:10.2147/COPD.S102570
37. Stallberg B, Janson C, Johansson G, et al. Management, morbidity and mortality of COPD during an 11-year period: an observational retrospective epidemiological register study in Sweden (PATHOS). Prim Care Respir J. 2014;23(1):38–45. doi:10.4104/pcrj.2013.00106
38. Patel AR, Hurst JR. Extrapulmonary comorbidities in chronic obstructive pulmonary disease: state of the art. Expert Rev Respir Med. 2011;5(5):647–662. doi:10.1586/ers.11.62
39. Smith MC, Wrobel JP. Epidemiology and clinical impact of major comorbidities in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2014;9:871–888. doi:10.2147/COPD.S49621
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.