Back to Journals » Drug Design, Development and Therapy » Volume 20
Anti-Vascular Endothelial Growth Factor Combined with Dexamethasone Implant Therapy for Macular Edema: A Randomized Controlled Trial
Authors Ma Y, Wang J, Yuan M, Zeng Z, Tan Y, Cao L, Sun X
Received 7 December 2025
Accepted for publication 8 February 2026
Published 3 March 2026 Volume 2026:20 587166
DOI https://doi.org/10.2147/DDDT.S587166
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Muzammal Hussain
Yunxi Ma, Junwen Wang, Mingzhu Yuan, Zimeng Zeng, Yuhe Tan, Lu Cao, Xufang Sun
Department of Ophthalmology, Hubei Key Laboratory of Otolaryngologic and Ophthalmic Diseases, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China
Correspondence: Xufang Sun, Department of Ophthalmology, Hubei Key Laboratory of Otolaryngologic and Ophthalmic Diseases, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China, Email [email protected]
Purpose: To compare the efficacy and safety of intravitreal conbercept monotherapy versus conbercept combined with dexamethasone implant in eyes with macular edema (ME).
Methods: Patients diagnosed with ME secondary to diabetic retinopathy or retinal vein occlusion were enrolled and randomized 1:1 to the combined or monotherapy group. In initial 12 weeks, the combined group received 1 loading dose of conbercept concomitantly with dexamethasone implant (DEX), while the monotherapy group received 3 monthly loading doses of conbercept. Following initial phases, all patients received intravitreal injections of conbercept on demand, assessed every 4 weeks over a 48-week follow-up period. The primary outcome measure was changes in best-corrected visual acuity (BCVA). Secondary outcome measures encompassed changes in optical coherence tomography (OCT) biomarkers and the total number of injections administered. Clinical safety was evaluated based on the incidence and severity of adverse events.
Results: 70 patients (70 eyes) were randomized to monotherapy (n=36) or combination therapy (n=34). Mean (SD) baseline BCVA and CMT were 44.60 (7.34) letters and 555.55 (150.87) μm in monotherapy group; 37.61 (13.47) letters and 581.80 (145.87) μm in combined group. The combined group showed greater BCVA improvement by week 8 and CMT reduction at weeks 4 and 8, and OCT biomarkers also improved more substantially during the first 12 weeks. The combination therapy required significantly fewer injections (P < 0.001) overall but a higher incidence of ocular hypertension. Outcomes of BCVA and CMT correlated with Hard Exudate (HE).
Conclusion: Conbercept combined with DEX is an efficient and safe treatment for ME by providing accelerated visual and anatomical improvements in short term and maintaining similar long-term efficacy with fewer injections compared to conbercept monotherapy. OCT biomarkers display prognostic value. HE is associated with poor visual prognosis.
Keywords: conbercept, dexamethasone implant, combination therapy, optical coherence tomography, biomarkers
Introduction
Macular edema (ME) is a major complication of ocular fundus diseases that leads to severe vision impairment.1,2 Although monthly injections of anti–vascular endothelial growth factor (VEGF) are the current mainstay of treatment, the frequent treatment and poor adherence pose significant challenges to long-term benefits in the real world.3–6 Nevertheless, many patients with ME show poor prognoses to standardized anti-VEGF therapy in clinical practice.7–9 Jaffe et al10 reported that approximately 65% of ME patients experienced persistent edema during long-term anti-VEGF treatment, with limited vision improvement. Therefore, an innovative strategy that maximizes clinical benefits and reduces treatment burden is needed.
Dexamethasone implant (DEX) is a sustained-release corticosteroid with broad-spectrum anti-inflammatory efficacy.11,12 DRCR net13 confirmed the effectiveness for ME. The pathology of ME is complex and characterised by multiple inflammatory factors.14,15 The combination of anti-VEGF and corticosteroid agents enables multi-pathway targeting, with synergistic effects that may yield superior outcomes.16–19
While best-corrected visual acuity (BCVA) and central macular thickness (CMT) are standard clinical endpoints for ME in assessing visual function and foveal morphology,20 they provide limited insight into treatment-induced changes in the intraocular microenvironment.21 Moreover, the retina’s intricate layered architecture means that single parameters like CMT cannot fully capture the anatomical response, as it represents a simplified view.22 Conversely, technological advances in optical coherence tomography (OCT) have greatly enhanced the detailed characterization of retinal microstructures.23–25 Given that vision loss in ME stems from fluid-related structural disruption,26 OCT biomarkers are emerging as critical tools for evaluating therapeutic impact on retinal anatomy and clinical outcomes.27,28
In this prospective study, we evaluated treatment response in ME eyes receiving intravitreal conbercept combined with DEX or conbercept monotherapy. OCT biomarkers were employed for quantitative analysis, enabling assessments of visual and structural changes throughout treatment and clarifying potential mechanisms. The findings would offer innovative indicators for monitoring therapeutic response in ME and provide evidence to optimize treatment strategies.
Materials and Methods
Trial Design
This is a prospective, randomized, controlled trial (ChiCTR2100046511) implemented at Tongji Hospital, Tongji Medical College. The study adhered to the Declaration of Helsinki and received approval from the Medical Ethics Committee of Tongji Hospital. Written informed consent was obtained before enrollment. An independent clinical research team monitored safety data. Data analysis was completed at the week 48 visit. The trial was conducted and reported in compliance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines.
Trial Population
Participants over 40 years old diagnosed with treatment-naïve ME (no history of invasive or pharmacological therapy) secondary to diabetic retinopathy (DR) or retinal vein occlusion (RVO) were eligible (e-Table 1 and 2 in Supplement). Exclusion criteria comprised a history of intravitreal injections (anti-VEGF or steroids) or laser photocoagulation for ME. Additionally, individuals with any other coexisting ocular pathologies known to compromise visual function severely were excluded.
Trial Procedures
Patients were randomly allocated in a 1:1 ratio to either the monotherapy or combination therapy group. Patients in the monotherapy group received 3 intravitreal injections of 0.5 mg conbercept (Conbercept, Chengdu Kanghong Biological Co, Ltd) at loading doses every 4 weeks through week 12. Patients in the combined group received 1 same-day injection of 0.5 mg conbercept and 0.7 mg dexamethasone implant (DEX; OZURDEX, Allergan) followed by the remaining doses of conbercept loading regimen. From week 12 to week 48, supplementary injections (conbercept, 0.5 mg) or laser photocoagulation were administered every 4 weeks if pre-specified criteria for on-demand treatment were met (e-Table 3 in Supplement).
Outcomes
The primary outcome was the change in best-corrected visual acuity (BCVA) from baseline to the 48-week visit. The secondary outcome included changes in OCT biomarkers. Safety outcomes included incidence and severity of adverse events (AEs; corneal inflammation, intraocular hypertension, cataract, macular epiretinal membrane, dry eye, optic atrophy, endophthalmitis).
OCT Biomarker Analysis
Spectra-Domain OCT (SD-OCT; Spectralis, Heidelberg, Germany) examinations were performed at each follow-up visit (e-Table 4 and 5 in Supplement). Two blinded experts independently analyzed images. Quantitative analysis of the imaging was conducted using ImageJ2 software (Version 1.54f, Bethesda, MD, USA) to measure the length shown in the retinal cross-section (e-Figure 1 in Supplement).
OCT biomarkers involved in this trial were as follows: (1) central macular thickness (CMT), defined as the perpendicular distance from the inner retina to the retinal pigment epithelium (RPE) at the foveal center; (2) subfoveal choroidal thickness (SFCT), defined as vertical thickness from the outer RPE to the choroid-sclera interface beneath the fovea; (3) external limiting membrane (ELM), defined as Hyperreflective line representing the photoreceptor-Müller cell junction. Defect appears as its discontinuity or loss; (4) ellipsoid zone (EZ), defined as hyperreflective band corresponding to the photoreceptor inner/outer segment junction. Defect appears as its discontinuity or loss; (5) outer plexiform layer (OPL), defined as a medium-reflective synaptic layer. Defect manifests as thinning, disorganization, or disruption; (6) neurosensory detachment (NSD), defined as hyporeflective, fluid-filled space between the neurosensory retina and the RPE; (7) hyperreflective retinal foci (HRFs), defined as punctate hyperreflective lesions (≤30 μm) within retinal layers, without posterior shadowing; (8) hard exudate (HE), defined as larger hyperreflective deposits (>30 μm), often in outer retina, typically with posterior shadowing; (9) disorganization of retinal inner layers (DRIL), defined as loss of normal laminar architecture in the inner retina within the central 1-mm foveal area (e-Figure 2 in Supplement).
Statistical Analysis
An estimated sample size of 78 participants was determined to be adequate, assuming a standard deviation of 7.4 and a significance level of 0.05, to provide greater than 80% power to demonstrate the noninferiority of combined therapy to monthly conbercept, with a noninferiority margin of 5 letters. The primary analysis was performed on the efficacy population, including all patients completing the 12-month visit. Data from May 18, 2021, to August 1, 2024, were analyzed.
Data were analyzed with SPSS Statistics (Version 25.0, IBM, NY, USA). Kolmogorov–Smirnov test was used for normality. Continuous variables were expressed as mean (SD) or median (IQR), and categorical variables as n (%). T-tests or chi-square tests were used for baseline comparisons. Longitudinal changes in functional and anatomical outcomes (BCVA, OCT biomarkers) were evaluated by repeated-measures ANCOVA, adjusting for baseline indicators. DRIL changes were analyzed with chi-square tests, within-group comparisons with paired t-tests or chi-square tests, and correlations with Pearson or Spearman coefficients. ImageJ2 and Prism (Version 9.0, GraphPad, CA, USA) were utilized for image analysis and graphing, respectively. P < 0.05 was considered statistically significant.
Results
Clinical Characteristics
From May 2021 to July 2023, 106 participants were screened, of whom 78 eligible individuals were enrolled and randomized to the combined group (DEX + conbercept, 39) or monotherapy group (conbercept, 39). Among those, 4 participants were lost to follow-up, 2 withdrew consent, and 1 discontinued intervention (Figure 1). The primary analysis comprised 70 eyes of 70 participants (combined group: n=34; monotherapy group: n=36). The mean (SD) age of 70 patients was 54.41 (9.75), 52.9% were male, 51.4% had diabetes, 42.9% had hypertension, the mean (SD) BCVA was 41.2 (15.86) letters, and the mean (SD) CMT was 568.3 (147.98) μm. Among OCT biomarkers, the mean (SD) SFCT was 255.6 (42.85) μm, and disruption lengths of ELM, EZ, and OPL were 395.53 (205.37) μm, 471.11 (202.03) μm, and 591.55 (176.98) μm, respectively. The mean (SD) NSD was 277.39 (121.79) μm. The mean (SD) counts for HRFs and HEs were 17.2 (7.44) and 3.17 (1.96). DRIL was observed in 95.7% of eyes. Demographics and clinical characteristics were balanced at baseline (Table 1).
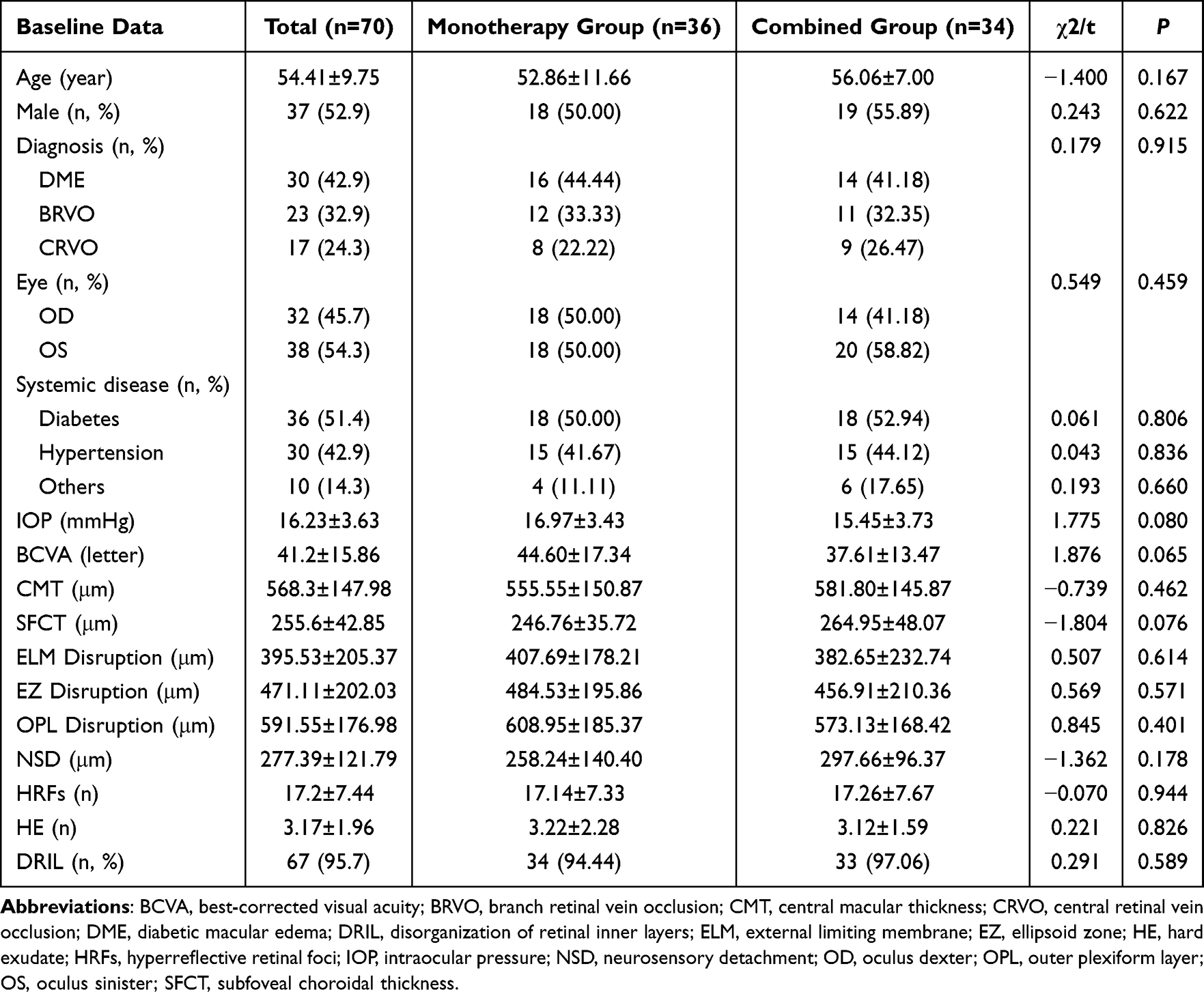 |
Table 1 Baseline Characteristics |
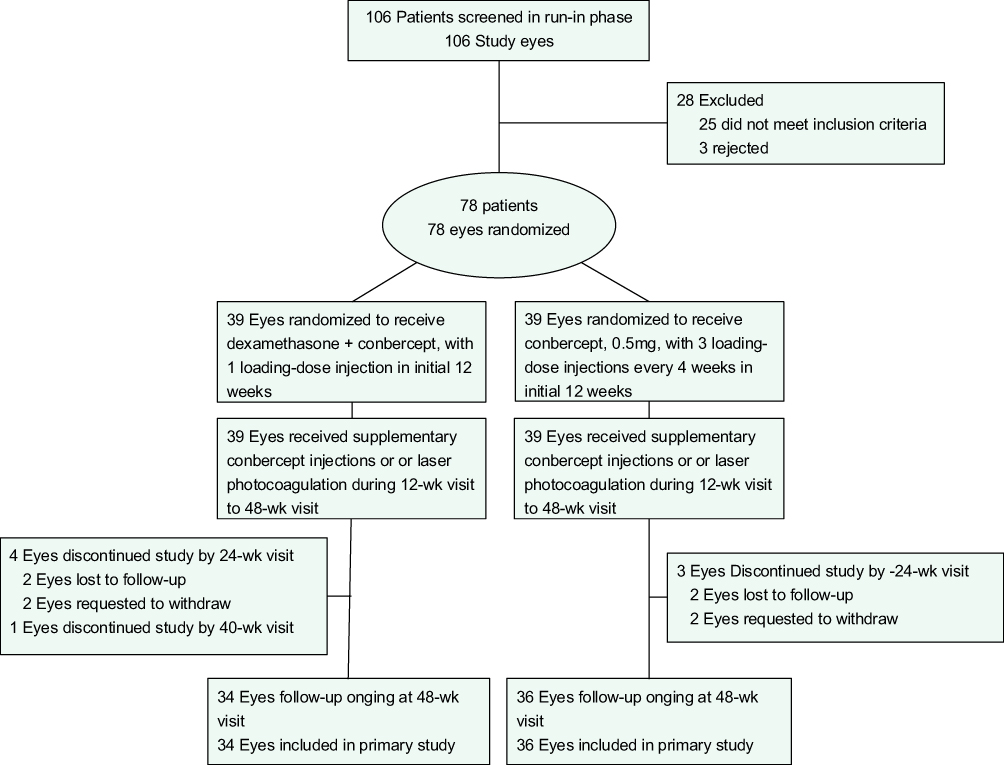 |
Figure 1 Flowchart of the trial. Abbreviation: wk, week. |
Treatment
The total mean (SD) number of intravitreal injections was significantly higher in the monotherapy group (7.5 [2.31]) than in the combined group (4.09 [1.11]; P < 0.001). During the 48-week visit, 17 patients (47.22%) in the monotherapy group and 15 (44.12%) in the combined group underwent laser photocoagulation (P = 0.794). No eyes required non-protocol macular edema therapy (e-Table 6 in Supplement).
BCVA
At the 48-week visit, the mean (SD) BCVA scores were 61.56 (14.13) letters in the combined group and 60.25 (15.03) letters in the monotherapy group (e-Table 7 in Supplement). Mean (SD) improvement from baseline to week 48 was 23.95 (16.14) in the combined group and 15.65 (15.63) in the monotherapy group (F=1.73, P=0.193).
Improvements in visual acuity were obtained throughout follow-up visits (Figure 2). Significant between-group differences were identified at an early stage (e-Table 8 in Supplement). The combined therapy group showed a mean improvement of 17.82 letters at 4 weeks, compared to 7.33 letters in the monotherapy group (F=11.01, P=0.002). By week 8, the upgrades were 24.86 and 9.54 letters, respectively (F=25.02, P<0.001). No significant differences were found between the groups at subsequent visits (P>0.05).
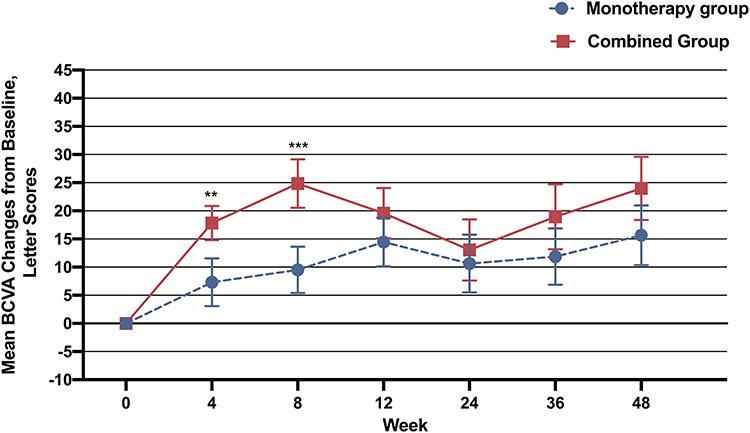 |
Figure 2 Mean BCVA change on SD-OCT in 48 weeks. Error bars indicate 95% CIs, **P<0.01, ***P<0.001. Abbreviations: BCVA, best-corrected visual acuity; SD-OCT, Spectra-Domain optical coherence tomography. |
Subgroup analyses are summarized in Supplement. Visual acuity improved over the 48 weeks. In the combined group, significant improvements were observed within the first 8 weeks (P < 0.001), followed by a slight decline in the mean change at week 12 (P = 0.029). In the monotherapy group, significant improvements from baseline were noted at week 4 (P < 0.01) and week 12 (P = 0.039).
OCT Biomarkers
CMT
At week 48, the mean (SD) CMT scores were 257.73 (87.67) μm in the combined group and 250.04 (89.25) μm in the monotherapy group (e-Table 9 in Supplement). The mean (SD) reduction in CMT from baseline to week 48 was 324.07 (157.45) μm for the combination group and 305.51 (185.79) μm for the monotherapy group (F=0.009, P=0.923).
Reductions in CMT were observed over follow-up visits (Figure 3). Significant between-group differences were identified from week 8 to week 16. At week 8, the mean reduction was −318.31 μm in the combined group, significantly greater than −244.96 μm in the monotherapy group (F=5.33, P=0.024). This significant intergroup difference persisted at week 12 (combination: −350.29 μm; monotherapy: −291.38 μm; F=6.26, P=0.015). At week 16, Mean CMT decline was −199.43 for combined therapy and −254.63 for monotherapy (F=6.49, P=0.013). Detailed results for the additional CMT outcomes are provided in e-Table 10 in Supplement.
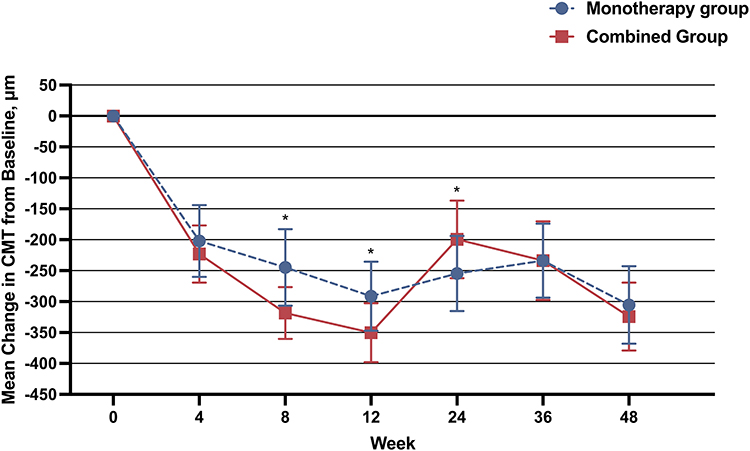 |
Figure 3 Mean CMT change on SD-OCT in 48 weeks. Error bars indicate 95% CIs, *P<0.05. Abbreviations: CMT, central macular thickness; SD-OCT, Spectra-Domain optical coherence tomography. |
Subgroup analyses are presented in Supplement. A reduction in CMT was observed in participants over the 48-week study. In the combined group, CMT decreased significantly within the first 8 weeks (P < 0.001), followed by a rebound at week 24 (P < 0.001) and a subsequent reduction at week 48 (P = 0.017). In the monotherapy group, significant CMT reductions from baseline occurred at week 4 (P < 0.01) and week 12 (P = 0.007).
Other Biomarkers
OCT biomarkers demonstrated significant improvement from baseline to week 48 in both groups, with substantial differences appearing in the early phase (e-Figure 3 in Supplement). At week 4, the mean (SD) number of HE significantly reduced in the combined group (1.59 [1.28]) than in the monotherapy group (2.69 [2.21]; P=0.002). DRIL resolution was also higher in the combined group (19/34 eyes, 55.89%) than in the monotherapy group (10/36 eyes, 27.78%; P=0.032). At week 8, the combined group maintained a lower HE (P < 0.0001), a lower SFCT (P=0.031), and a higher rate of DRIL resolution (P=0.031). At week 12, the combined group showed further advantages in decreasing HE (P=0.038), HRFs (P=0.008), and SFCT (P=0.035). By week 24, SFCT in the combined group is higher compared to monotherapy group (P = 0.048). Nevertheless, the disruption in EZ, ELM, OPL, and NSD showed no substantial difference between the two groups. (e-Table 11 to 18 in Supplement)
Baseline SD-OCT Biomarkers as Correlates of BCVA
Baseline BCVA demonstrated significant inverse correlations with the defect lengths of ELM (R = −0.256, P = 0.033) and NSD (R = −0.239, P = 0.046). No other baseline OCT biomarkers were correlated with initial vision. At the study endpoint, the number of HE remained the sole significant correlate of BCVA (R = −0.26, P = 0.03). (e-Table 19 in Supplement). After adjustment for clinical characteristics, all factors remained significantly associated with visual acuity in the multivariable model.
Baseline SD-OCT Biomarkers as Correlates of CMT
At baseline, CMT showed significant positive correlations with SFCT (R = 0.534, P < 0.001), as well as with the defect lengths of EZ (R = 0.406, P < 0.001), ELM (R = 0.396, P = 0.001), OPL (R = 0.512, P < 0.001), and NSD (R = 0.746, P < 0.001). No significant correlations were observed with other OCT biomarkers. At the endpoint, the final CMT was correlated with the number of HE (R = 0.249, P = 0.038). (e-Table 20 in Supplement). In the multivariable model adjusted for clinical characteristics, all these factors remained independently associated with CMT.
Discussion
As first-line therapy, anti-VEGF agents improve both visual and anatomical outcomes in ME.7,20,29 However, the recommendation for monthly injections imposes significant treatment burdens, and the complex pathogenesis often limits the efficacy of anti-VEGF monotherapy.30,31 Given these challenges, combination therapy with corticosteroids has emerged as a promising strategy, with potential synergistic effect to achieve better clinical outcomes.13,27,32,33
This prospective trial evaluated the efficacy of anti-VEGF monotherapy versus its combination with DEX for ME. Both regimens significantly improved visual and anatomical outcomes, consistent with other trials.13,20,34 Notably, the combined therapy showed early superiority in this study, enhancing visual and anatomical function with fewer injections. However, long-term efficacy did not differ significantly between the two groups.35
The combined therapy showed a more pronounced effect on short-term visual improvement. In this study, patients receiving the combined therapy exhibited a steady increase in BCVA within the first two months, significantly superior to anti-VEGF monotherapy. This finding aligns with the results of the DRCR net.29 In contrast, Mehta et al35 reported no additional benefit from combined medications. This discrepancy may be attributed to the predominant use of triamcinolone acetonide (TA).35 In this study, we employed DEX, which possesses a stronger potent anti-inflammatory effect and lower retinal toxicity than TA.12,36 The distinct pharmacological properties may contribute to the enhanced therapeutic efficacy.
OCT biomarkers are considered essential for anatomical evaluation of clinical response in ME, effectively complementing functional measurements.37 To move beyond the limitations of qualitative analyses,38–40 this study prospectively quantified two categories of OCT biomarkers, including anatomical parameters (CMT, SFCT, ELM, EZ, OPL, DRIL) and hyperreflective features (HRFs, HE). The results indicated reversible structural damage in ME and significant improvement following treatment. The combination therapy demonstrated superior early efficacy in reducing CMT, SFCT, HRFs, HE, and DRIL. Therefore, integrating quantitative OCT biomarkers may provide a more comprehensive evaluation of therapeutic response. This trial recommended that OCT biomarkers be considered critical components of efficacy indicators for ME clinical trials and management.
In this study, combination therapy showed significantly greater improvement in CMT at weeks 8 and 12 compared to anti-VEGF monotherapy. These findings suggest a more rapid resolution of macular edema in the initial phases, aligning with previous research.18,41 The extended-release formulation of dexamethasone provides sustained suppression of key inflammatory factors, such as prostaglandins and interleukins.12,13,42 This action contributes to the stabilization of the blood-retinal barrier, suggesting early benefits of the combined regimen for both anatomical integrity and visual function.
SFCT is utilized to evaluate morphological changes in the choroid.43 In this study, both anti-VEGF monotherapy and combination therapy significantly decreased SFCT in ME patients, with the combined regimen achieving a greater reduction in the early phase. The result is consistent with studies by Nourinia et al44 and Moon et al,28 which may result from synergistic drug effects that strongly suppress VEGF levels, thereby improving choroidal vascular permeability and alleviating obstruction.28 The results indicate that combination therapy offers potential advantages for optimizing choroidal circulation.
HRFs and HE are proposed as key inflammatory biomarkers in retinal diseases for evaluating clinical outcomes.26,27,37 This study showed a greater effect of adding steroids, aligning with the findings of Hwang et al45 and Vujosevic et al.46 While anti-VEGF and DEX alone reduce HRFs, their combination results in a more pronounced early decline,47 which may effectively target persistent microstructural inflammation and enhance overall therapeutic benefits.37,48 The role of HE in ME remains unclear, with limited and conflicting evidence about its response to treatment. Srinivas et al49 found faster HE regression with DEX therapy compared to anti-VEGF, while Rübsam et al50 suggested no early reduction. Interestingly, although the decline was gradual, both treatment strategies significantly reduced HE counts, with combination therapy achieving better early clearance. Additionally, baseline HE showed a negative association with final visual outcomes, indicating its potential as a prognostic marker.49 The current variability of HE reported in retrospective studies highlights the need for prospective validation in larger groups to assess its clinical utility.
DRIL, a biomarker indicating inner retinal disorganization linked to poor vision, often persists with anti-VEGF therapy, but responds better to DEX.44,51,52 This study evaluated changes in DRIL under various treatment regimens. Both anti-VEGF (44.4% improvement) and combined therapy (50% improvement) proved effective. The findings showed that combined therapy resulted in significantly better DRIL improvement than anti-VEGF alone, although long-term outcomes were similar. This early advantage may be attributed to the neuroprotective effects of DEX.53
EZ, ELM, and OPL are essential for photoreceptor function and signal transmission.26,27 In this study, either anti-VEGF or combination therapies promote reversible repair of outer retinal structures. The VISTA trial51 supported it, suggesting EZ defect resolution after anti-VEGF therapy, and Hwang et al45 also reported significant improvements in EZ and ELM integrity following either therapy. However, no significant difference in improvement of these layers was observed between the two treatments. This finding contrasts with the report by Cavalleri et al,54 which indicated that DEX offered better substantial efficacy. The discrepancy may be attributable to methodological differences: we administered fewer DEX injections (1 vs 1.6 ± 0.8) with a larger sample size (70 vs 28), and included patients with lower baseline BCVA (37.61 ± 13.47 vs 60.3 ± 21.8). Given the current limited and heterogeneous literature on quantitative analysis of OCT biomarkers, larger prospective studies are needed for further validation.
Over the 48-week follow-up, the combined group required significantly fewer injections than the anti-VEGF monotherapy group (4.09 ± 1.11 vs 7.50 ± 2.31). This supports the study by Cai et al,55 which also indicated a reduced injection frequency with combination therapy during long-term management (4.72 ± 1.54 vs 6.30 ± 0.31). Despite the fewer treatments, the results indicate that the combination approach is not inferior to anti-VEGF monotherapy in long-term effectiveness. Therefore, combining anti-VEGF therapy with DEX could be an effective and promising treatment that provides visual and anatomical benefits while alleviating injection burden.
Although ME initially responded well, both groups experienced recurrence after week 24, with more severe cases in the combined group, possibly due to the decline in intraocular dexamethasone levels following its peak at two months.56,57 Cai et al55 also reported recurrence at 24 weeks. The average number of injections in the combined group (4.09 ± 1.11) was consistent with other research,55,58 but was lower than the guidelines provided by EURETINA.59 To ensure sustained long-term control, we recommend that patients on combined therapy receive an additional intravitreal anti-VEGF at 6 months. Studies have also noted ME recurrence despite continuous anti-VEGF therapy.60,61 Anti-VEGF therapy shows poor efficacy in patients with low-to-normal VEGF and elevated inflammatory markers, and its long-term benefits for chronic ME are limited.60 Therefore, switching to DEX therapy may benefit patients with suboptimal response to anti-VEGF monotherapy. Additionally, regular follow-up visits (≤4 weeks) are suggested to maintain optimal prognosis.
The safety profiles of the two treatments varied, guiding clinical decisions. The combined therapy group experienced an increase in steroid-related side effects such as cataracts and elevated IOP, all of which were manageable. This highlights the importance of regular IOP and lens examinations for patients receiving dexamethasone.62 The monotherapy group showed a tendency for more ocular surface complications, reflecting the cumulative local trauma from frequent injections. Severe complications were rare but occurred in both groups, with one case of optic nerve atrophy reported in each, which may result from progression of underlying systemic vascular disease rather than direct drug toxicity.34,63,64 Therefore, close follow-up should encompass both ocular response and systemic control.
This study has several limitations. First, the single-center randomized controlled design and relatively homogeneous population may introduce selection bias and limit the generalizability. Second, the small sample size restricts subgroup analysis by etiology in ME. As a result, potential differences in treatment responses based on underlying mechanisms remain unexamined. Third, external factors such as costs, healthcare burdens, and differences in socioeconomic status, which influence management of systemic comorbidities and treatment adherence, contributed to a higher rate of adverse events. Despite this, high protocol adherence improved internal consistency. Future multicenter studies with larger samples and advanced imaging are necessary to validate findings and explore mechanistic differences.
Conclusion
In conclusion, anti-VEGF combined with DEX is an effective and safe treatment for ME. It provides better visual and anatomical recovery in the short term while maintaining noninferior long-term efficacy with a lower treatment burden than anti-VEGF alone. Additionally, OCT biomarkers are essential for evaluating efficacy. HE is associated with poor visual prognosis.
Abbreviations
AEs, adverse events; BCVA, best-corrected visual acuity; BRVO, branch retinal vein occlusion; CMT, central macular thickness; CONSORT, Consolidated Standards of Reporting Trials; CRVO, central retinal vein occlusion; DEX, dexamethasone implant; DME, diabetic macular edema; DR, diabetic retinopathy; DRIL, disorganization of retinal inner layers; ELM, external limiting membrane; EZ, ellipsoid zone; HE, hard exudate; HRFs, hyperreflective retinal foci; IOP, intraocular pressure; OD, oculus dexter; OCT, optical coherence tomography; OPL, outer plexiform layer; OS, oculus sinister; RPE, retinal pigment epithelium; RVO, retinal vein occlusion; SD-OCT, Spectra-Domain optical coherence tomography; SFCT, subfoveal choroidal thickness; NSD, neurosensory detachment; VEGF, vascular endothelial growth factor.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval Statement
This prospective, randomized controlled trial was reviewed and approved by the Ethics Committee of Tongji Hospital (TJ-IRB20210641) and registered with the Chinese Clinical Trial Registry (ChiCTR2100046511). Registration date: 05/18/2021. Written informed consent was obtained from each patient before the surgery.
Acknowledgments
We appreciate the participants enrolled in this trial and the research team for their vital contributions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Key Research and Development Program of China (2024YFC2510803) and the National Natural Science Foundation of China (82471103).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Abdel-Maboud M, Menshawy E, Bahbah EI, Outani O, Menshawy A, Vavvas DG. Intravitreal bevacizumab versus intravitreal triamcinolone for diabetic macular edema–Systematic review, meta-analysis and meta-regression. PLoS One. 2021;16(1):e0245010. doi:10.1371/journal.pone.0245010
2. Bhambra N, Sayal AP, Popovic MM, Muni RH, Kertes PJ. Combination intravitreal anti-vascular endothelial growth factor inhibitors and macular laser photocoagulation relative to intravitreal injection monotherapy in macular oedema secondary to retinal vein occlusion: a meta-analysis of randomized controlled trials. Eye. 2022;36(12):2271–12. doi:10.1038/s41433-021-01833-2
3. Fleckenstein M, Schmitz-Valckenberg S, Chakravarthy U. Age-related macular degeneration: a review. JAMA. 2024;331(2):147. doi:10.1001/jama.2023.26074
4. Ashraf M, Souka A, Adelman R. Predicting outcomes to anti-vascular endothelial growth factor (VEGF) therapy in diabetic macular oedema: a review of the literature. Br J Ophthalmol. 2016;100(12):1596–1604. doi:10.1136/bjophthalmol-2016-308388
5. Zehden JA, Mortensen XM, Reddy A, Zhang AY. Systemic and ocular adverse events with intravitreal anti-VEGF therapy used in the treatment of diabetic retinopathy: a review. Curr Diab Rep. 2022;22(10):525–536. doi:10.1007/s11892-022-01491-y
6. Chatziralli I. Ranibizumab for the treatment of diabetic retinopathy. Expert Opin Biol Ther. 2021;21(8):991–997. doi:10.1080/14712598.2021.1928629
7. Baker CW, Glassman AR, Beaulieu WT, et al. Effect of initial management with aflibercept vs laser photocoagulation vs observation on vision loss among patients with diabetic macular edema involving the center of the macula and good visual acuity: a randomized clinical trial. JAMA. 2019;321(19):1880–1894. doi:10.1001/jama.2019.5790
8. Brown DM, Wykoff CC, Boyer D, et al. Evaluation of intravitreal aflibercept for the treatment of severe nonproliferative diabetic retinopathy: results from the PANORAMA randomized clinical trial. JAMA Ophthalmol. 2021;139(9):946. doi:10.1001/jamaophthalmol.2021.2809
9. Li X, Li C, Huang H, et al. Anti-vascular endothelial growth factor drugs combined with laser photocoagulation maintain retinal ganglion cell integrity in patients with diabetic macular edema: study protocol for a prospective, non-randomized, controlled clinical trial. Neural Regen Res. 2024;19(4):923–928. doi:10.4103/1673-5374.382104
10. Jaffe GJ, Ying GS, Toth CA, et al. Macular morphology and visual acuity in year five of the comparison of age-related macular degeneration treatments trials. Ophthalmology. 2019;126(2):252–260. doi:10.1016/j.ophtha.2018.08.035
11. Al-khersan H, Salehi-Had H, Hariprasad SM. Dexamethasone and Anti-VEGF combination therapy for the treatment of diabetic macular edema. Ophthalmic Surg Lasers Imaging Retina. 2019;50(1):4–7. doi:10.3928/23258160-20181212-01
12. Chawan-Saad J, Wu M, Wu A, Wu L. Corticosteroids for diabetic macular edema. Taiwan J Ophthalmol. 2019;9(4):233. doi:10.4103/tjo.tjo_68_19
13. Maturi RK, Glassman AR, Liu D, et al. Effect of adding dexamethasone to continued ranibizumab treatment in patients with persistent diabetic macular edema: a DRCR Network Phase 2 randomized clinical trial. JAMA Ophthalmol. 2018;136(1):29. doi:10.1001/jamaophthalmol.2017.4914
14. El Zaoui I, Behar-Cohen F, Torriglia A. Glucocorticoids exert direct toxicity on microvasculature: analysis of cell death mechanisms. Toxicol Sci. 2015;143(2):441–453. doi:10.1093/toxsci/kfu243
15. Huang Z, Liang J, Chen S, et al. RIP3-mediated microglial necroptosis promotes neuroinflammation and neurodegeneration in the early stages of diabetic retinopathy. Cell Death Dis. 2023;14(3):227. doi:10.1038/s41419-023-05660-z
16. Chen C, Wang Z, Yan W, et al. Anti-VEGF combined with ocular corticosteroids therapy versus anti-VEGF monotherapy for diabetic macular edema focusing on drugs injection times and confounding factors of pseudophakic eyes: a systematic review and meta-analysis. Pharmacol Res. 2023;196:106904. doi:10.1016/j.phrs.2023.106904
17. Adams OE, Sodhi GS, Vagaggini T, et al. Clinical outcomes of acute endophthalmitis after intravitreal delivery of vascular endothelial growth factor inhibitors versus steroids. Retina. 2023;43(6):947–954. doi:10.1097/IAE.0000000000003748
18. Chiu CY, Huang TL, Chang PY, et al. Combined intravitreal ranibizumab and posterior subtenon triamcinolone acetonide injections for patients with diabetic macular edema refractory to intravitreal ranibizumab monotherapy. Taiwan J Ophthalmol. 2021;11(3):251. doi:10.4103/tjo.tjo_31_20
19. Romano F, Lamanna F, Gabrielle PH, et al. Update on retinal vein occlusion. Asia-Pac J Ophthalmol. 2023;12(2):196–210. doi:10.1097/APO.0000000000000598
20. Gabrielle PH, Mehta H, Barthelmes D, et al. From randomised controlled trials to real-world data: clinical evidence to guide management of diabetic macular oedema. Prog Retinal Eye Res. 2023;97:101219. doi:10.1016/j.preteyeres.2023.101219
21. Haensli C, Fasler K, Barthelmes D, Zweifel SA. Characterizing flow and structure of diabetic retinal neovascularization after intravitreal Anti-VEGF using optical coherence tomography angiography: a pilot study. J Ophthalmol. 2021;2021:1–16. doi:10.1155/2021/2942197
22. Gucciardo E, Loukovaara S, Salven P, Lehti K. Lymphatic vascular structures: a new aspect in proliferative diabetic retinopathy. Int J Mol Sci. 2018;19(12):12. doi:10.3390/ijms19124034
23. Alagorie AR, Nittala MG, Velaga S, et al. Association of intravitreal aflibercept with optical coherence tomography angiography vessel density in patients with proliferative diabetic retinopathy: a secondary analysis of a randomized clinical trial. JAMA Ophthalmol. 2020;138(8):851. doi:10.1001/jamaophthalmol.2020.2130
24. Chang YC, Huang YT, Hsu AY, et al. Optical coherence tomography biomarkers in predicting treatment outcomes of diabetic macular edema after ranibizumab injections. Medicina. 2023;59(3):629. doi:10.3390/medicina59030629
25. Chou HD, Wu CH, Chiang WY, et al. Optical coherence tomography and imaging biomarkers as outcome predictors in diabetic macular edema treated with dexamethasone implant. Sci Rep. 2022;12(1):3872. doi:10.1038/s41598-022-07604-7
26. Daruich A, Matet A, Moulin A, et al. Mechanisms of macular edema: beyond the surface. Prog Retinal Eye Res. 2018;63:20–68. doi:10.1016/j.preteyeres.2017.10.006
27. Sorour OA, Levine ES, Baumal CR, et al. Persistent diabetic macular edema: definition, incidence, biomarkers, and treatment methods. Survey Ophthalmol. 2023;68(2):147–174. doi:10.1016/j.survophthal.2022.11.008
28. Moon KY, Choi SY, Song JH. Changes in subfoveal choroidal thickness after intravitreal dexamethasone implant therapy for diabetic macular edema. Retina. 2021;41(6):1283–1292. doi:10.1097/IAE.0000000000003029
29. Bressler NM, Beaulieu WT, Bressler SB, et al. Anti–vascular endothelial growth factor therapy and risk of traction retinal detachment in eyes with proliferative diabetic retinopathy: pooled analysis of five DRCR retina network randomized clinical trials. Retina. 2020;40(6):1021–1028. doi:10.1097/IAE.0000000000002633
30. Mettu PS, Allingham MJ, Cousins SW. Incomplete response to Anti-VEGF therapy in neovascular AMD: exploring disease mechanisms and therapeutic opportunities. Prog Retinal Eye Res. 2021;82:100906. doi:10.1016/j.preteyeres.2020.100906
31. Gale R, Pikoula M, Lee AY, et al. Real world evidence on 5661 patients treated for macular oedema secondary to branch retinal vein occlusion with intravitreal anti-vascular endothelial growth factor, intravitreal dexamethasone or macular laser. Br J Ophthalmol. 2021;105(4):549–554. doi:10.1136/bjophthalmol-2020-315836
32. Bressler NM, Odia I, Maguire M, et al. Association between change in visual acuity and change in central subfield thickness during treatment of diabetic macular edema in participants randomized to aflibercept, bevacizumab, or ranibizumab: a post hoc analysis of the protocol t randomized clinical trial. JAMA Ophthalmol. 2019;137(9):977–985. doi:10.1001/jamaophthalmol.2019.1963
33. Eriş E, Perente I, Vural E, et al. Evaluation of the effect of combined intravitreal ranibizumab injection and sub-tenon steroid injection in the treatment of resistant diabetic macular edema. Int Ophthalmol. 2019;39(7):1575–1580. doi:10.1007/s10792-018-0977-0
34. Wells JA, Glassman AR, Ayala AR, et al. Aflibercept, Bevacizumab, or Ranibizumab for Diabetic Macular Edema. Ophthalmology. 2016;123(6):1351–1359. doi:10.1016/j.ophtha.2016.02.022
35. Mehta H, Hennings C, Gillies MC, Nguyen V, Campain A, Fraser-Bell S. Anti-vascular endothelial growth factor combined with intravitreal steroids for diabetic macular oedema. Cochrane Eyes and Vision Group, ed. Cochrane Database Syst Rev. 2018;2018(4). doi:10.1002/14651858.CD011599.pub2
36. Chang-Lin JE, Burke JA, Peng Q, et al. Pharmacokinetics of a sustained-release dexamethasone intravitreal implant in vitrectomized and nonvitrectomized eyes. Invest Ophthalmol Vis Sci. 2011;52(7):4605. doi:10.1167/iovs.10-6387
37. SKh S, TYy L, Vujosevic S, et al. Optical coherence tomography in the management of diabetic macular oedema. Prog Retinal Eye Res. 2024;98:101220. doi:10.1016/j.preteyeres.2023.101220
38. Savur F, Kaldırım H, Atalay K, Öğreden T, Hayat ŞÇ. Treatment results of diabetic macular edema with different choroidal thickness with intravitreal anti vascular endothelial growth factor. BMC Ophthalmol. 2022;22(1):508. doi:10.1186/s12886-022-02721-3
39. Maggio E, Mete M, Sartore M, et al. Temporal variation of optical coherence tomography biomarkers as predictors of anti-VEGF treatment outcomes in diabetic macular edema. Graefes Arch Clin Exp Ophthalmol. 2022;260(3):807–815. doi:10.1007/s00417-021-05387-7
40. Hui VWK, Szeto SKH, Tang F, et al. Optical coherence tomography classification systems for diabetic macular edema and their associations with visual outcome and treatment responses - an updated review. Asia Pac J Ophthalmol. 2022;11(3):247–257. doi:10.1097/APO.0000000000000468
41. Limon U. Early effect of simultaneous intravitreal dexamethasone and bevacizumab combination treatment in patients with persistent diabetic macular edema. J Fr Ophtalmol. 2021;44(6):849–854. doi:10.1016/j.jfo.2020.08.033
42. Gaballa SA, Kompella UB, Elgarhy O, et al. Corticosteroids in ophthalmology: drug delivery innovations, pharmacology, clinical applications, and future perspectives. Drug Deliv Transl Res. 2021;11(3):866–893. doi:10.1007/s13346-020-00843-z
43. Campos A, Campos EJ, Do Carmo A, et al. Choroidal thickness changes stratified by outcome in real-world treatment of diabetic macular edema. Graefes Arch Clin Exp Ophthalmol. 2018;256(10):1857–1865. doi:10.1007/s00417-018-4072-z
44. Nourinia R, Ahmadieh H, Nekoei E, Malekifar P, Tofighi Z. Changes in central choroidal thickness after treatment of diabetic macular edema with intravitreal bevacizumab correlation with central macular thickness and best-corrected visual acuity. Retina. 2018;38(5):970–975. doi:10.1097/IAE.0000000000001645
45. Hwang HS, Chae JB, Kim JY, Kim DY. Association between hyperreflective dots on spectral-domain optical coherence tomography in macular edema and response to treatment. Invest Ophthalmol Vis Sci. 2017;58(13):5958. doi:10.1167/iovs.17-22725
46. Vujosevic S. Diabetic macular edema with neuroretinal detachment: OCT and OCT-angiography biomarkers of treatment response to anti-VEGF and steroids. Acta Diabetologica. 2020;57(3):287–296.
47. Chatziralli IP, Sergentanis TN, Sivaprasad S. Hyperreflective foci as an independent visual outcome predictor in macular edema due to retinal vascular diseases treated with intravitreal dexamethasone or ranibizumab. Retina. 2016;36(12):2319–2328. doi:10.1097/IAE.0000000000001070
48. Qin S, Zhang C, Qin H, et al. Hyperreflective foci and subretinal fluid are potential imaging biomarkers to evaluate Anti-VEGF effect in diabetic macular edema. Front Physiol. 2021;12:791442. doi:10.3389/fphys.2021.791442
49. Srinivas S, Verma A, Nittala MG, et al. Effect of intravitreal ranibizumab on intraretinal hard exudates in eyes with diabetic macular edema. Am J Ophthalmol. 2020;211:183–190. doi:10.1016/j.ajo.2019.11.014
50. Rübsam A, Wernecke L, Rau S, et al. Behavior of SD-OCT detectable hyperreflective foci in diabetic macular edema patients after therapy with Anti-VEGF agents and dexamethasone implants. J Diab Res. 2021;2021:1–13. doi:10.1155/2021/8820216
51. Ehlers JP, Yeh S, Maguire MG, et al. Intravitreal pharmacotherapies for diabetic macular edema. Ophthalmology. 2022;129(1):88–99. doi:10.1016/j.ophtha.2021.07.009
52. Kocapınar Y, Kaplan FB, Demirciler Sönmez A, Açıkalın B. Evaluation of the efficacy of anti-vascular endothelial growth factors in diabetic macular edema with retinal inner and outer layers disorganization. Acta Diabetol. 2023;60(10):1391–1398. doi:10.1007/s00592-023-02121-z
53. Bandello F, Augustin A, Tufail A, Leaback R. A 12-month, multicenter, parallel group comparison of dexamethasone intravitreal implant versus ranibizumab in branch retinal vein occlusion. Eur J Ophthalmol. 2018;28(6):697–705. doi:10.1177/1120672117750058
54. Cavalleri M, Cicinelli MV, Parravano M, et al. Prognostic role of optical coherence tomography after switch to dexamethasone in diabetic macular edema. Acta Diabetol. 2020;57(2):163–171. doi:10.1007/s00592-019-01389-4
55. Cai X, Zhao J, Dang Y. Combination therapy with Anti-VEGF and intravitreal dexamethasone implant for macular edema secondary to retinal vein occlusion. Current Eye Rese. 2024;49(8):872–878. doi:10.1080/02713683.2024.2343055
56. Whitcup SM, Cidlowski JA, Csaky KG, Ambati J. Pharmacology of corticosteroids for diabetic macular edema. Invest Ophthalmol Vis Sci. 2018;59(1):1–12. doi:10.1167/iovs.17-22259
57. Kishore K, Bhat PV, Venkatesh P, Canizela CC. Dexamethasone intravitreal implant for the treatment of macular edema and uveitis: a comprehensive narrative review. OPTH. 2022;16:1019–1045. doi:10.2147/OPTH.S209395
58. Liang X, Shen B, Ou Z, An H, Li L. Comparison of intravitreal ranibizumab monotherapy vs. ranibizumab combined with dexamethasone implant for macular edema secondary to retinal vein occlusion. Front Med. 2022;9:930508. doi:10.3389/fmed.2022.930508
59. Schmidt-Erfurth U, Garcia-Arumi J, Gerendas BS, et al. Guidelines for the management of retinal vein occlusion by the European society of retina specialists (EURETINA). Ophthalmologica. 2019;242(3):123–162. doi:10.1159/000502041
60. Vitiello L, Salerno G, Coppola A, et al. Switching to an intravitreal dexamethasone implant after intravitreal Anti-VEGF therapy for diabetic macular edema: a review. Life. 2024;14(6):725. doi:10.3390/life14060725
61. Vitiello L, Lixi F, Coppola A, et al. Intravitreal dexamethasone implant switch after Anti-VEGF treatment in patients affected by retinal vein occlusion: a review of the literature. JCM. 2024;13(17):5006. doi:10.3390/jcm13175006
62. Hengge UR, Ruzicka T, Schwartz RA, Cork MJ. Adverse effects of topical glucocorticosteroids. J Am Acad Dermatol. 2006;54(1):1–15. doi:10.1016/j.jaad.2005.01.010
63. Noma H, Yasuda K, Shimura M. Cytokines and pathogenesis of central retinal vein occlusion. JCM. 2020;9(11):3457. doi:10.3390/jcm9113457
64. Chi SC, Kang YN, Huang YM. Efficacy and safety profile of intravitreal dexamethasone implant versus antivascular endothelial growth factor treatment in diabetic macular edema: a systematic review and meta-analysis. Sci Rep. 2023;13(1):7428. doi:10.1038/s41598-023-34673-z
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Peripapillary and Subfoveal Choroidal Thickness in Retinal Vein Occlusions
Moleiro AF, Godinho G, Madeira C, Faria Pereira A, Brandão E, Falcão-Reis F, Beato JN, Penas S
Clinical Ophthalmology 2022, 16:3775-3783
Published Date: 16 November 2022
Advances of Drug-Loaded Microsphere Technology for Targeted Immunotherapy Against Prostate Cancer
Feng W
International Journal of Nanomedicine 2025, 20:11479-11489
Published Date: 20 September 2025
Mechanisms and Emerging Strategies to Overcome Immunotherapy Resistance in Cold Tumours of Colorectal Cancer
Zhu X, Ge B, Wen L
OncoTargets and Therapy 2026, 19:621109
Published Date: 15 June 2026