Back to Journals » Clinical Ophthalmology » Volume 20
AI-Assisted UBM versus Conventional Sizing Approaches for ICL Implantation: A Retrospective Analysis of Vault Outcomes
Authors Ang RET ![]() , Glipo CER, Martinez GHA
, Glipo CER, Martinez GHA ![]() , Yutangco RJM, Cruz EM
, Yutangco RJM, Cruz EM
Received 6 March 2026
Accepted for publication 4 June 2026
Published 17 June 2026 Volume 2026:20 604669
DOI https://doi.org/10.2147/OPTH.S604669
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sotiria Palioura
Robert Edward T Ang,1,2 Cesar Emmanuel R Glipo,2 Gladness Henna A Martinez,2 Roquito Jose M Yutangco,1 Emerson M Cruz1
1Cornea and Refractive Surgery Section, Asian Eye Institute, Makati City, Philippines; 2Department of Ophthalmology, Cardinal Santos Medical Center, San Juan City, Philippines
Correspondence: Emerson M Cruz, Cornea and Refractive Surgery Section, Asian Eye Institute, Makati City, Philippines, Email [email protected]
Introduction: To compare the effectiveness of an ultrasound biomicroscopy (UBM)–based nomogram with a white-to-white (WTW) nomogram in predicting postoperative vault in myopic patients undergoing implantable collamer lens (ICL) implantation.
Methods: This retrospective, single-center study included 227 eyes from 116 myopic patients (mean age 28.9 ± 7.3 years). ICL sizing was determined using either the WTW OCOS nomogram (WTW group, 117 eyes, 60 patients) or the UBM ICL Guru nomogram (UBM group, 110 eyes, 56 patients). Postoperative evaluation at 1 month included uncorrected and corrected visual acuity, refraction, anterior chamber depth, axial length, intraocular pressure, and vault.
Results: Demographic data showed 56 patients (36% male, 64% female) had a mean age of 28.82 ± 7.73 for the UBM group and, among 60 patients (43% male, 57% female), had a mean age of 28.98 ± 6.88 for the WTW group. Postoperative uncorrected and corrected visual acuity and refractive outcomes were comparable between the UBM and WTW groups, with no statistically significant differences observed. Mean vault differed significantly among the groups. The UBM group showed a lower average vault (472.3 ± 170.0 μm) compared with the WTW group (560.4 ± 251.7 μm, p < 0.1). Undervault (< 250 μm) occurred in 9.1% of UBM versus 11.1% of WTW eyes. Overvault (750– 1000 μm) was less frequent with UBM (3.6%) than with the WTW group (14.5%). Seven percent in the WTW group had excessively high vaults of greater than 1000 μm, with 6 eyes undergoing ICL exchange. Prediction error with the UBM nomogram was within 383 μm across all eyes at 1 month.
Conclusion: Visual and refractive outcomes were similarly good in both the WTW group and the UBM group. While visual outcomes were similar, the UBM based ICL Guru nomogram achieved more precise postoperative vaulting than the WTW-based OCOS method. OCOS resulted in more overvaults and ICL exchanges, making ICL Guru the superior choice for consistent, ideal vault targeting.
Keywords: implantable collamer lens, ICL sizing, ICL guru, Ultrasound biomicroscopy, Vault, Artificial Intelligence
Introduction
Myopia, or nearsightedness, has seen a dramatic global increase over the past few decades, with projections indicating that nearly 50% of the world’s population will be affected by 2050, as shown in a study by Holden.1 This surge is particularly pronounced in East Asian countries, where myopia prevalence among young adults now exceeds 80% due to a combination of genetic predisposition and environmental factors such as prolonged near work and limited outdoor activity.1,2 The incidence and prevalence of adult myopia in the Philippines have shown a significant upward trend in recent years. A nationwide survey reported that approximately 30% of Filipino adults aged 20 to 40 years are myopic, with urban residents exhibiting higher rates than their rural counterparts exhibiting prevalence rates up to 40–50%, reflecting lifestyle factors like increased near work and less outdoor activity. The age of onset for myopia is decreasing, with some adults developing high myopia after the age of 30. The rising incidence underscores a growing public health concern, projecting that myopia could affect over 60% of the Filipino adult population by 2030.3 A study by Tideman suggested that urbanization and increased educational pressures contribute significantly to the rising incidence, reinforcing the need for early interventions, including optical and behavioral strategies, to mitigate myopia progression.4
Surgical treatment has become an integral part of myopia management.5 Refractive surgery techniques target either the cornea or internal optics to refocus the light on the retina. Laser vision correction (LVC) involves reshaping of the cornea by removing part of the corneal stroma. Laser in Situ Keratomileusis (LASIK) in particular has become one of the most popular procedures for myopia because it provides high patient satisfaction owing to it being an outpatient procedure typically done on both eyes and rapid visual recovery. However, LVC is contraindicated in patients with high myopia and thin or abnormal corneas.6,7
In light of the limitations of LVC, Implantable Collamer Lens (ICL) has gained global prominence as an alternative for myopia correction. It provides a removable and exchangeable option for myopia correction without permanently altering the corneal structure. The redesign of ICL incorporating a central hole (KS Aquaport) improved patient safety/satisfaction by removing the need for a YAG laser iridotomy.6 An ICL is implanted in the eye behind the iris in the sulcus space above the natural lens. In addition to ICL power determination, appropriate selection of ICL size is crucial to optimize the fit of the lens into the intended space. Vault is the distance between the posterior surface of the ICL and anterior lens surface. Vault measurement represents the appropriateness of the size and position of the ICL. While the manufacture recommendation is 250–900 microns; the ideal postoperative vault should be between 250 and 750 microns.8 Under vaulting, a vault measurement of less than 250 microns, is usually associated with cataract formation due to contact and rubbing of the ICL to the natural lens. Overvaulting, a vault measurement in excess of 750 μm, can lead to angle closure, increased intraocular pressure, iris pigment dispersion, uveitis and corneal decompensation. Although under and overvaulting are not direct causes for these complications, they may increase the risk of unwanted postoperative problems. Inappropriate postoperative vault may necessitate another surgical procedure for the patient, most likely an ICL exchange or removal.6
The importance and controversy of ICL size determination is highlighted by the various nomograms being used in different parts of the world.6 The manufacturer-recommended STAAR OCOS (Online Calculation and Ordering System) nomogram utilizes Anterior Chamber Depth (ACD) and White-to-White (WTW) corneal diameter to obtain a recommended ICL size for implantation. WTW, visible and easily measurable, is used as a surrogate for the Sulcus-to-Sulcus (STS) because STS measurement is difficult to access and is dynamic due to lens and iris movements. WTW measurements can be obtained manually using calipers during preoperative assessments. To reduce variability, manual WTW can be alternatively measured using Orbscan, IOLMaster, and/or Pentacam. However, a study by Ang has shown that these automated WTW measurements with the different devices were not interchangeable.9 WTW does not always correlate precisely with the internal STS dimension, which can lead to suboptimal sizing outcomes.8,10–14
Ultrasound Biomicroscopy (UBM) allows for detailed visualization of the anterior segment, including the ciliary sulcus, iris configuration, and the ciliary body. Several studies have shown that UBM significantly improves the accuracy of vault predictions and reduces the incidence of ICL exchanges. However, the widespread adoption of STS measurements has been hindered by the lack of standardized protocols and the operator-dependent nature of UBM imaging.15
Artificial Intelligence (AI) has increasing applications in the medical field and, in a study by Shen shows promising results particularly for ICL sizing and vault prediction.16 The VUMAX HD (Sonomed Escalon UBM system, New Hyde Park, NY) has upgraded its platform that enables auto capture of real-time measured corneal thickness, ACD, lens thickness, angle to angle (ATA) and STS distance.
ICLGuru is a novel nomogram that integrates measures taken through UBM and processed with an AI algorithm utilizing deep learning for sizing calculation that ideally provides an accurate ICL sizing recommendation with a predicted vault. The ICLGuru nomogram employs a dual-algorithm approach consisting of a vault estimation algorithm and a safety band calculation algorithm to predict central (distance between the crystalline lens and ICL) and peripheral (separation between the ICL and the lens) vaults. ICLGuru further generates prediction data categorized by risk level based on published information to aid the user in minimizing vaulting error and improve clinical outcomes.17 Over the past 10 years, we have used the WTW-based OCOS nomogram to calculate the lens size for the ICL we used on each patient. The UBM-AI algorithm, which features assistance with AI/machine learning features, was introduced one year ago, and we had been using it to calculate the ICL size as of this writing. This retrospective study aims to determine the performance of this novel nomogram in ICL sizing by analyzing our vault outcomes and comparing it with the vault outcomes of the WTW-based nomogram we previously used. This involves the evaluation of records of adult myopic patients who underwent ICL implantation. Patients will be grouped by the use of the WTW-based nomogram or by the novel UBM-based nomogram for calculation of implant size. Demographics and post-operative findings are evaluated for significant differences between the two groups to determine effectiveness.
Materials and Methods
This is a retrospective cohort single center study of patients who underwent ICL implantation in one or both eyes performed by a single experienced surgeon. Patients were implanted with an ICL wherein the size was determined either by a UBM-based nomogram or a WTW-based nomogram. This study followed the tenets of the Declaration of Helsinki and secured the approval from the Cardinal Santos Medical Center Review Committee (approval no. 2025–038). Due to the retrospective nature of the study and the use of fully anonymized data, the requirement for informed consent was formally waived by the committee.
Medical records of all myopic patients who underwent ICL implantation from January 1, 2022, to March 31, 2025, were retrieved and retrospectively reviewed. Inclusion criteria were adults aged 18 to 60 years, eyes with myopia and myopic astigmatism from −1.00 to −18.00 spherical equivalent, ACD of at least 2.80 mm, endothelial cell count of at least 2000 mm2, a follow-up of at least one month, and postoperative data availability including visual acuity, refraction, intraocular pressure (IOP), axial length (AL), ACD, and vault. Exclusion criteria were eyes with hyperopia, notable corneal opacities or irregularities in corneal topography, eye surface disorders, binocular vision issues affecting either distance or near vision, traumatic implantation, improper haptic positioning requiring repositioning, significant postoperative ICL rotation requiring reoperation, postoperative pupillary block, postoperative cataract formation, uncontrolled intraocular pressure elevation, or incomplete postoperative data due to complication-related follow-up loss.
The EVO Visian ICL V4c (STAAR Surgical Company, Monrovia, CA, USA) model for the correction of myopia was used as the implant in this study. The Visian ICL is a phakic collamer intraocular lens with a foldable hydrophilic collamer plate-haptic model featuring a central convex/concave optical zone. The V4c model features a 0.35 mm central port for aqueous humor flow to minimize the risk of secondary cataract development. The foldable nature of the ICL allows for insertion through a 3.2 mm incision and is positioned within the posterior chamber. The lens is ideally placed between the iris and crystalline lens once implanted.17
The STAAR Surgical Online Calculation and Ordering System (OCOS; STAAR Surgical Company, Monrovia, CA, USA) software was used for the WTW group based on ACD and WTW measurements obtained through uniform caliper measurements. These measurements are encoded into the OCOS ordering system, which would give a size recommendation (i.e., 12.1, 12.6, 13.2, or 13.7 mm) and power with an expected postoperative refraction value. The STAAR Surgical OCOS software generates a single recommended ICL size based primarily on WTW and ACD measurements encoded into the ordering system. An Implantation Orientation Diagram was also generated for toric lenses to determine the axis required after insertion of the lens in the eye which can provide optimal astigmatic correction.
The VuMAX HD (Sonomed Escalon, USA) ophthalmic ultrasound system with “UBM-AI alignment” was used to obtain imaging for the biometric parameters needed. This system utilizes the ICLGuru nomogram which uses biometric data from UBM images and is processed with AI algorithms and mathematical models. The ICLGuru nomogram integrates multiple biometric parameters obtained from UBM imaging, including sulcus anatomy, ciliary body configuration, anterior chamber dimensions, and crystalline lens relationships. The system applies AI-assisted image alignment and filtering algorithms to exclude poor-quality images prior to analysis. The data is then automatically filtered using a dynamic link library to ensure adequate image quality prior to final calculation. The algorithm excluded low visibility of key structures (corneal apex, sulcus, ciliary body), artifacts, and misalignments to yield high quality data for the calculations. The filtered data is processed by the ICLGuru to give ICL size recommendations with predicted central vault, peripheral vault, and angle measurement.
The ICLGuru nomogram may generate more than one acceptable lens size recommendation. Final lens selection was determined by the operating surgeon using the predicted central vault, peripheral vault, anterior chamber angle metrics, and safety band analysis provided by the software. Among the acceptable recommendations, the surgeon preferentially selected the ICL size predicted to achieve a postoperative central vault closest to approximately 500 µm while remaining within the acceptable safety range. A color-coded safety band calculation is provided in the printout, categorizing vault prediction according to risk level based on the displayed color. Green indicates an ideal range with optimal outcomes. Yellow and blue represent low and elevated vaults, respectively, which are still considered acceptable. Red signifies a very low vault with a high risk of contact with the natural lens, while magenta denotes a very high vault associated with a high risk of iris contact.17
This study analyzed patients that were grouped based on the sizing calculation software used for implantation. Patients whose ICL sizing was determined using the STAAR OCOS nomogram were designated as the “WTW Group,” whereas those whose sizing was based on the ICLGuru nomogram with ultrasound biomicroscopy (UBM) data integration were designated as the “UBM Group.” The institution had been using the white-to-white (WTW)-based OCOS calculator for approximately 10 years, including the duration of this study. In contrast, the UBM-based AI platform with ICLGuru for ICL size determination was introduced into clinical use approximately one year prior to the study period. The WTW-based OCOS nomogram generates a single recommended ICL size, whereas the ICLGuru nomogram provides multiple potential size options along with predicted central vault, peripheral vault, and angle metrics for each recommendation. Prior to June 1, 2024, ICL sizing was performed exclusively using the WTW-based OCOS nomogram. From June 1, 2024, to March 31, 2025, both WTW-based and UBM-based calculations were performed for each eye; however, surgical decision-making during this period was guided by the UBM AI with ICLGuru output, with lens selection based on achieving a predicted central vault closest to 500 µm.
The OCOS nomogram continued to be generated during this period but was used for reference purposes only. Importantly, this study utilized the version of the ICLGuru nomogram available during the data collection period, specifically the non-Pro version in clinical use from approximately May/June 2024 through July/August 2025. The updated ICLGuru Pro platform, introduced in late August 2025 and incorporating further algorithmic refinements and enhanced predictive capabilities, was not used in the dataset analyzed. Patient demographics and preoperative parameters, including uncorrected visual acuity (UCVA), best corrected visual acuity (BCVA), manifest refractive spherical equivalent (MRSE), white-to-white (WTW) distance, axial length (AL), and anterior chamber depth (ACD), as well as postoperative outcomes including UCVA, BCVA, MRSE, AL, ACD, vault, intraocular pressure (IOP), and overall treatment outcomes, were recorded and analyzed.
Preoperative
All patients undergoing refractive screening were evaluated for the suitability of ICL implantation, which was included as part of the counseling process regarding available treatment options. All biometric and clinical measurements were performed by trained ophthalmic technicians and optometrists who were not involved in surgical decision-making. Standardized preoperative refraction and visual acuity testing were performed using calibrated automated refractors (HRK-1 Autorefractor, Huvitz Co., Ltd., Korea) and Snellen/LogMAR charts under mesopic conditions. Intraocular pressure was measured using Goldmann applanation tonometry at each visit, while anterior chamber depths were obtained using Orbscan IIz (Bausch & Lomb, Rochester, NY, USA). Endothelial cell counts were measured using non-contact specular microscopy (Konan Cellcheck, Konan Medical, Irvine, CA, USA). All imaging and measurements were performed following a uniform protocol to ensure inter-operator consistency.
Those undergoing UBM required an additional 10–20 minutes to complete the screening procedure for both eyes. With the patient in the supine position, topical anesthetics are instilled in one eye, after which a suction cup is applied and Balanced Salt Solution (BSS) is introduced. The UBM probe is then positioned directly over the cornea for approximately 5 minutes. The biometric images are automatically captured for analysis using the UBM AI algorithm. The same step is done on the fellow eye.
Surgical Technique
All surgical procedures were performed by a single surgeon and conducted under intravenous sedation. A paracentesis and temporal main incision were created. Intracameral lidocaine and methylcellulose viscoelastic agent were injected. The ICL was inserted into the anterior chamber and the four-haptics positioned under the iris. In cases involving toric ICL implantation, the surgeon marked the cornea, indicating the correct axis at the slit lamp preoperatively. Intraoperatively, the lens was dialed to align with the corresponding axis. The viscoelastic was then removed via manual irrigation. After surgery, the patient was asked to instill antibiotic, steroid, and NSAID eyedrops until the drops were consumed.
Postoperative
Following surgery, patients were instructed to remain in the supine position for 30 minutes. Postoperative management included the administration of topical antibiotics and anti-inflammatory eyedrops. ICL axis alignment and IOP were assessed every hour for the first 2 hours using the slit lamp microscope and applanation tonometer. Patients were discharged if the IOP was less than 10 mmHg and the ICL was aligned with the intended axis, with instructions for follow-up at 1 day, 1 week, and 1 month postoperatively. At each follow-up visit, routine evaluations included visual acuity, refraction, IOP measurement, iTrace analysis, and anterior segment optical coherence tomography (AS-OCT) to measure vault.
Statistical Analysis
Based on a similar study by Zhang, which evaluated a UBM-based nomogram in determining lens sizing, the vault prediction showed accuracy within 100, 300, and 500 μm in 40.48%, 88.10%, and 100% of eyes.18 Using a 95% confidence interval and 5% margin of error, the required sample size for this study was determined to be at least 102 eyes. Categorical data for both the UBM and WTW groups were summarized using frequencies and percentages to identify significant similarities in pre- and postoperative measures. Continuous data were expressed as means with standard deviations. Pearson’s correlation analysis was applied to evaluate the relationship between predicted and postoperative vaults in the UBM group at 1 month. Additionally, the relationship between 1-month postoperative vault and preoperative WTW, AL, ACD, MRSE, and postoperative IOP was analyzed using Pearson’s correlation in both the UBM and WTW groups, serving as a means of evaluating the two nomograms. Correlations between preoperative WTW, AL, ACD, and MRSE and postoperative IOP with coefficients below 0.30 are considered weak; those between 0.30 and 0.50 are considered moderate, while those above 0.50 are considered indicative of a strong correlation. A p-value of less than 0.05 is regarded as statistically significant. All analyses were carried out using STATA version 16.1 (StataCorp, College Station, TX, USA) and Microsoft Excel.
Results
Background Characteristics
The study included 227 eyes from 116 patients. The UBM group had 110 eyes from 56 patients, while the WTW group had 117 eyes from 60 patients. The mean age was similar at 28 years, and there were more females than males in both groups.
Preoperatively, the mean uncorrected visual acuity (UCVA) of the UBM group was 1.31 ± 0.42 logMAR, while it was 1.50 ± 0.44 logMAR in the WTW group. Manifest refractive spherical equivalent (MRSE) was −7.98 ± 4.52D in the UBM group, while it was −7.75 ± 3.21D in the WTW group. The UBM group mean axial length was 26.66 ± 2.06 mm, and ACD was 3.04 ± 0.22 mm. The WTW group had a mean axial length of 26.78 ± 1.34 mm and an ACD of 3.08 ± 0.25 mm (Table 1).
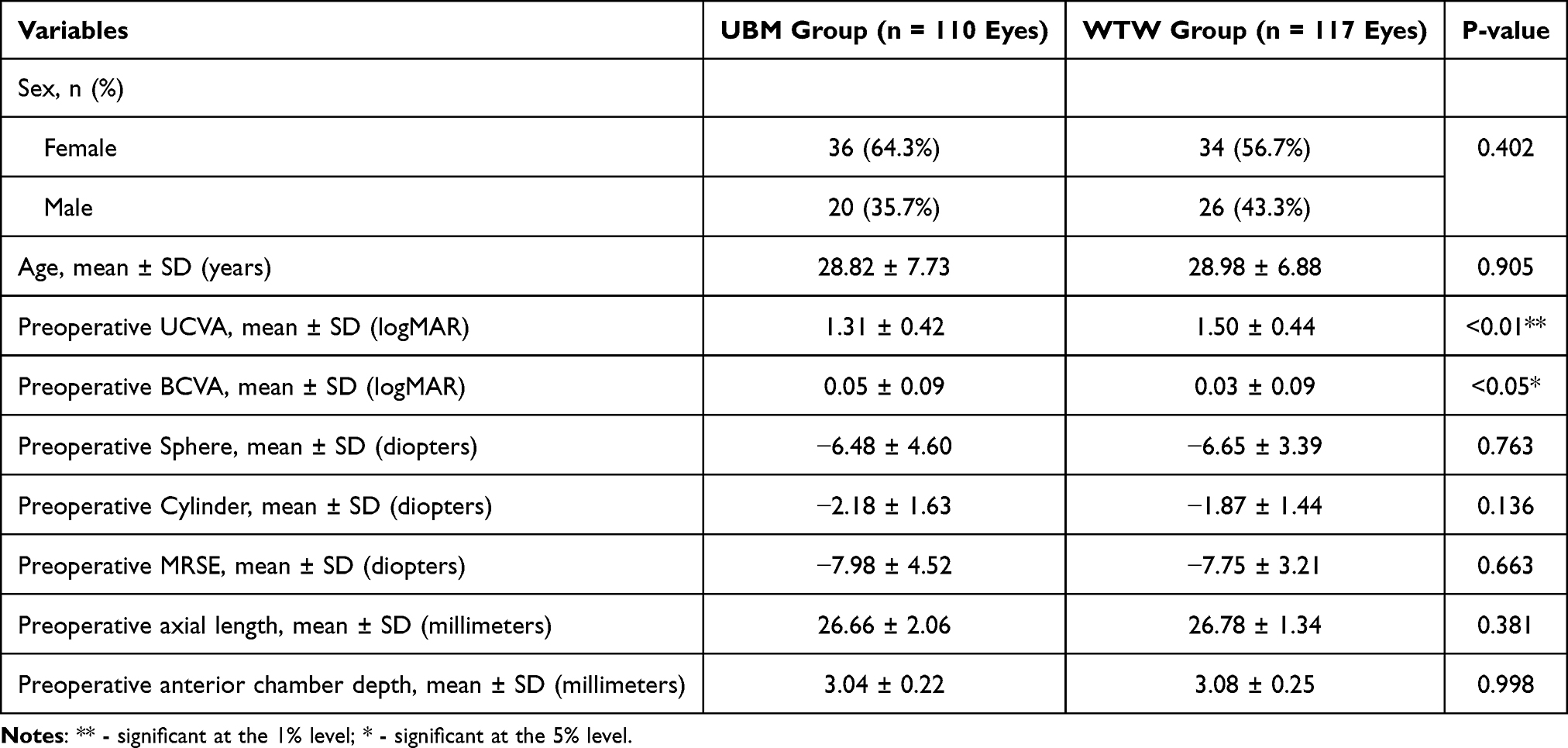 |
Table 1 Baseline Demographics and Preoperative Visual Acuity and Refractive Measurements of Eyes in the UBM and WTW Groups |
Postoperatively, the mean UCVA was 0.05 ± 0.13 logMAR in the UBM group and 0.03 ± 0.10 in the WTW group. The MRSE was −0.46 ± 1.20 in the UBM group and −0.30 ± 0.39 D in the WTW group. There were no statistically significant differences between groups for these measures. The vault measurements had a statistical difference showing 472.25 ± 169.7 µm for the UBM group versus 557.78 ± 246.73 µm in the WTW group. The mean intraocular pressure was similar at 14 mmHg in both groups (Table 2).
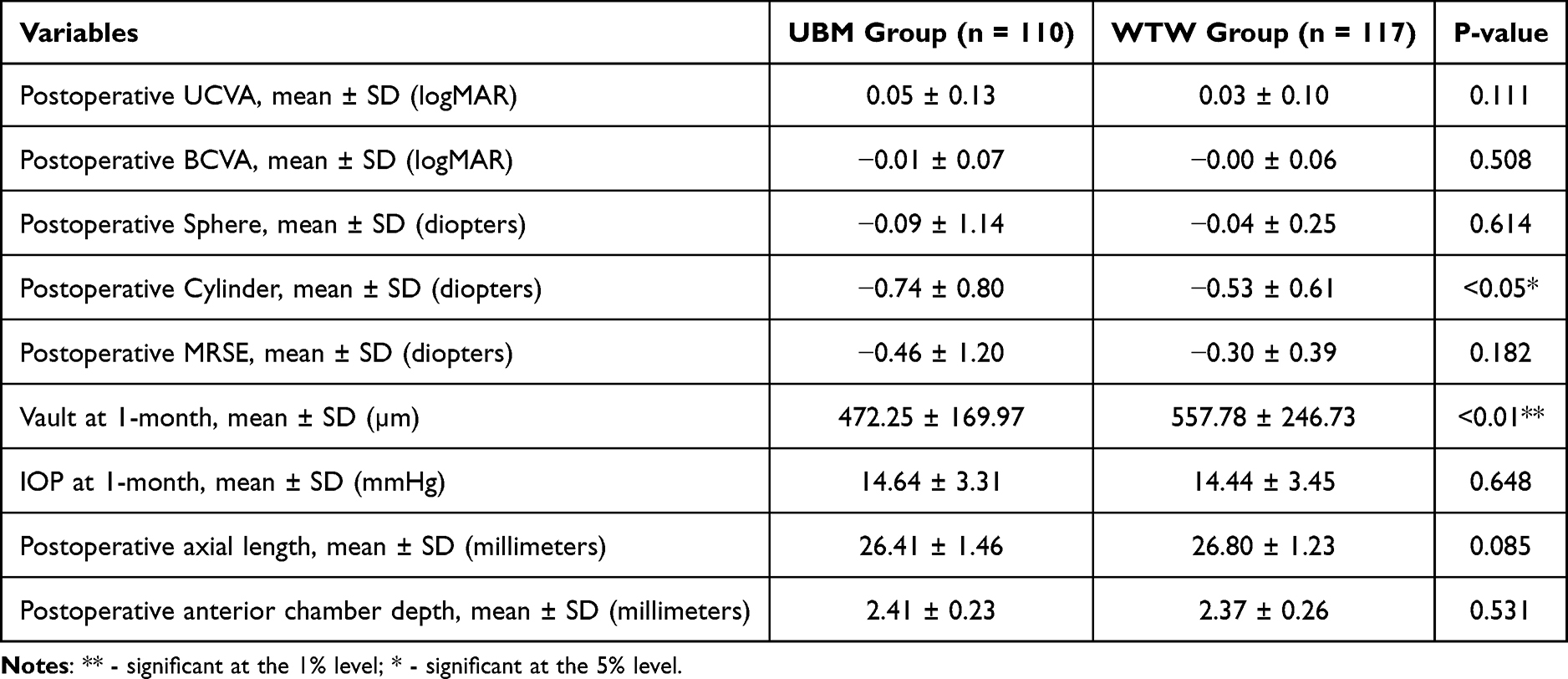 |
Table 2 Postoperative Visual Acuity and Refractive Measurements of Eyes in the UBM and WTW Group |
Treatment Outcomes
Postoperatively, in the UBM group, 93 eyes (84%) reached 20/30 UCVA while 74 eyes (68%) reached 20/20 or better UCVA. In the WTW group, 114 eyes (98%) reached 20/30 while 92 eyes (79%) achieved 20/20 UCVA.
Complications
A total of 19 adverse events were recorded postoperatively for both groups. About 14 events occurred in the WTW group, including elevated intraocular pressure (IOP > 21 mmHg) in 6 eyes, ICL rotation in 2 eyes, and ICL exchange in 6 eyes. In contrast, there were only 2 cases of elevated IOP and 3 cases of ICL rotation in the UBM group. The higher incidence of elevated IOP in the WTW group is likely indirectly related to vault distribution, particularly cases with excessive vault (>1000 µm), which may induce anterior chamber crowding, impaired aqueous circulation, or angle compromise. However, since overall correlation analysis did not show a strong linear relationship between vault and IOP in either group, this suggests that IOP elevation is multifactorial and not solely vault-dependent. Other contributing factors may include transient postoperative inflammation, steroid response, and ICL rotation. Indications for all ICL rotations in both groups were due to axis misalignment. Indications for all ICL exchanges in the WTW group were due to high vaults (>1000), wherein the ICLs were changed to smaller sizes. These differences were statistically significant with a p-value of <0.05 (Table 3).
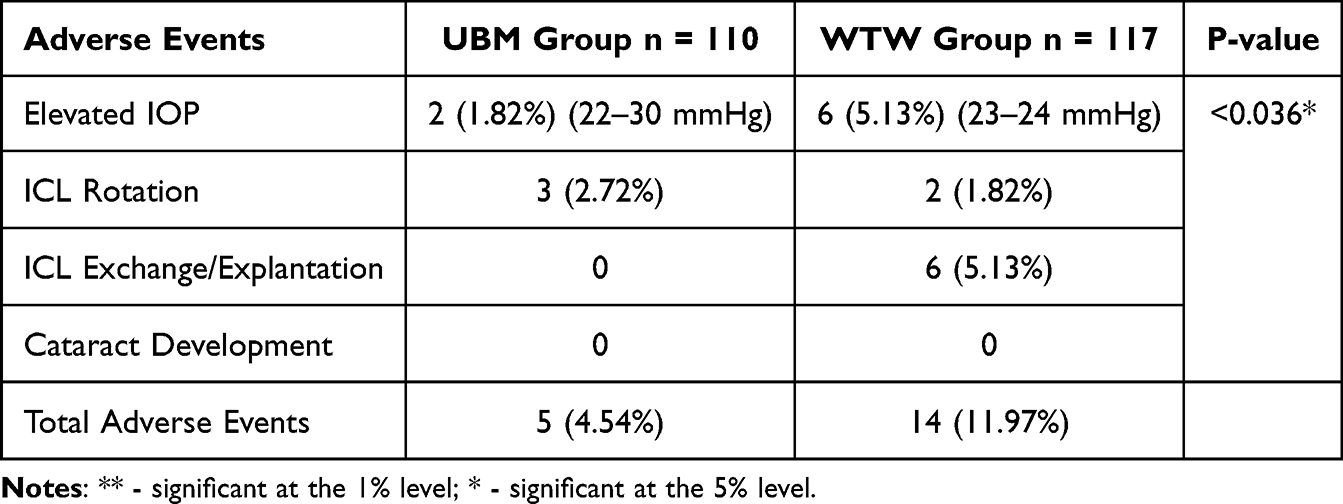 |
Table 3 Adverse Events for the UBM and WTW Group at the Post Operative Period |
Postoperative Vault
The ideal postoperative vault of 250–750 μm was achieved in 87.3% of eyes in the UBM group and 68.3% of eyes in the WTW group. There were 10 eyes (9.1%) in the UBM group and 13 eyes (11.1%) in the WTW group with a vault less than 250 μm. There were 4 eyes (3.6%) in the UBM group and 17 eyes (14.5%) in the WTW group that were within 750–1000 μm. Lastly, there were 7 eyes (6.8%) in the WTW group that had a postoperative vault of more than 1000 μm and none in the UBM group. These differences were statistically significant with a p-value of <0.01 (Table 4). The clinical relevance lies not in the mean difference alone, but in the distribution of extreme values, particularly the higher proportion of excessive vaults (>1000 µm) in the WTW group, which directly contributed to ICL exchanges. Thus, the statistical difference reflects measurement variability and outlier risk rather than a uniform clinically meaningful shift in vault behavior. Since the UBM Group had the benefit of both the WTW-based OCOS and UBM-AI algorithm measurements, we sought to determine if both nomograms showed similar size recommendations. In our study, WTW and UBM recommended the same ICL size in 90.9% (n = 100) of cases. In 7.3% (n = 8) of eyes, however, WTW recommended a larger size compared with UBM, while in 1.8% (n = 2) of eyes, UBM recommended a larger size compared to WTW. The absolute difference between the predicted vault and actual vault when using the UBM-based ICL size recommendation was within 100 μm in 50.9% of eyes, 200 μm in 79.1% and within 383 μm in 100% of eyes.
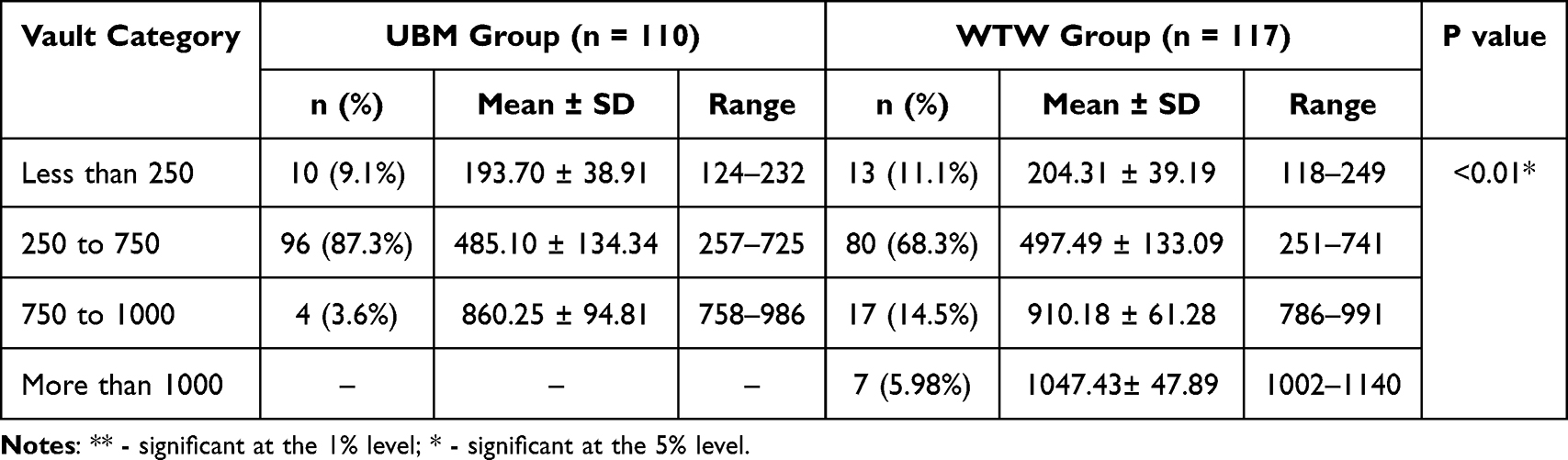 |
Table 4 Mean Vault at 1 Month According to Vault Categories in the UBM and WTW Groups |
WTW and UBM Group Assessment
Vault ranges were stratified based on the size of ICL implanted. For the UBM group, 96 out of 110 eyes were implanted with ICL sizes of 12.1 and 12.6. There were no eyes implanted with an ICL size of 13.7. The WTW group had 87 out of 117 eyes implanted with ICL sizes of 12.6 and 13.2. There were 26 eyes implanted with ICL of size 12.1 and 4 eyes implanted with 13.7. The mean postoperative vault per ICL size was closer to the median in the ICL group compared to the WTW group. For ICL sizes of 12.6 and 13.2, there was a wider range of postoperative vault measurements in the WTW group, indicating a wider scatter of vault outcomes (Figures 1a and b).
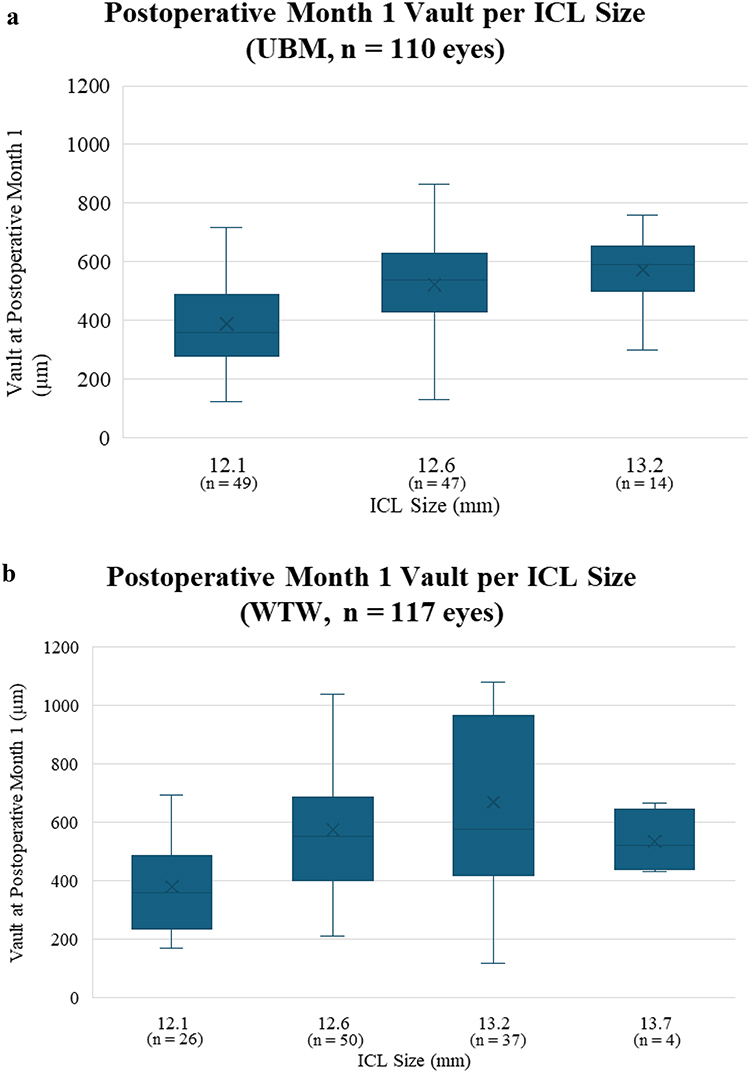 |
Figure 1 (a) Postoperative Month 1 Vault per ICL size for UBM Group. (b) Postoperative Month 1 Vault per ICL size for WTW group. |
WTW measurements were analyzed against the 1-month postoperative vault for both groups. Statistical analysis showed no significant correlation of WTW measurement to vault (UBM group R2 = 0.0133; WTW group R2 = 0.0287). Trends show that the WTW group had a wider distribution of postoperative vault measurements compared to the UBM group (Figures 2a and b).
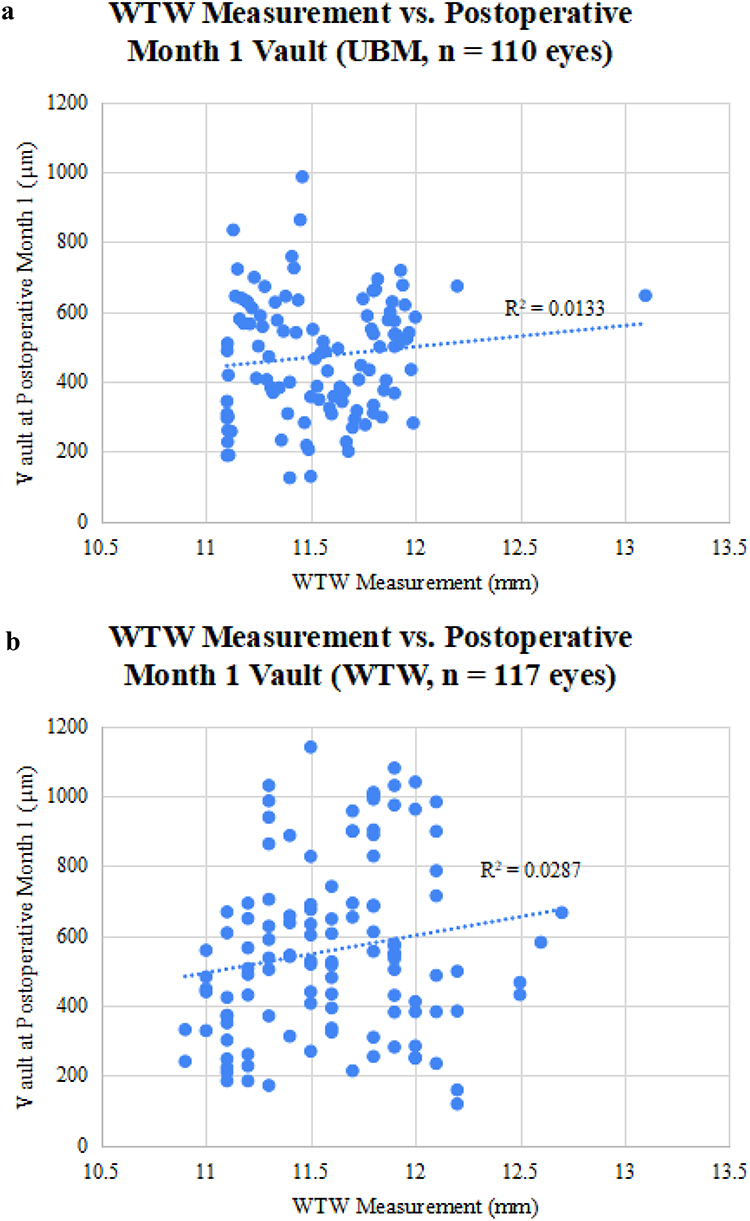 |
Figure 2 (a) WTW Measurement vs. Postoperative Month 1 Vault for UBM group. (b) WTW Measurement vs. Postoperative Month 1 Vault for WTW group. |
Preoperative MRSE for both groups was analyzed and did not have any statistically significant correlation with postoperative vault in both groups (UBM group R2 = 0.00006; WTW group R2 = 0.0029) (Figures 3a and b). Postoperative IOP was analyzed and showed no significant correlation with postoperative vault (UBM group R2 = 0.0009; WTW group R2 = 0.01). One eye in the UBM group had an IOP of 30 mmHg at 1 month postoperatively (Figure 4a and b).
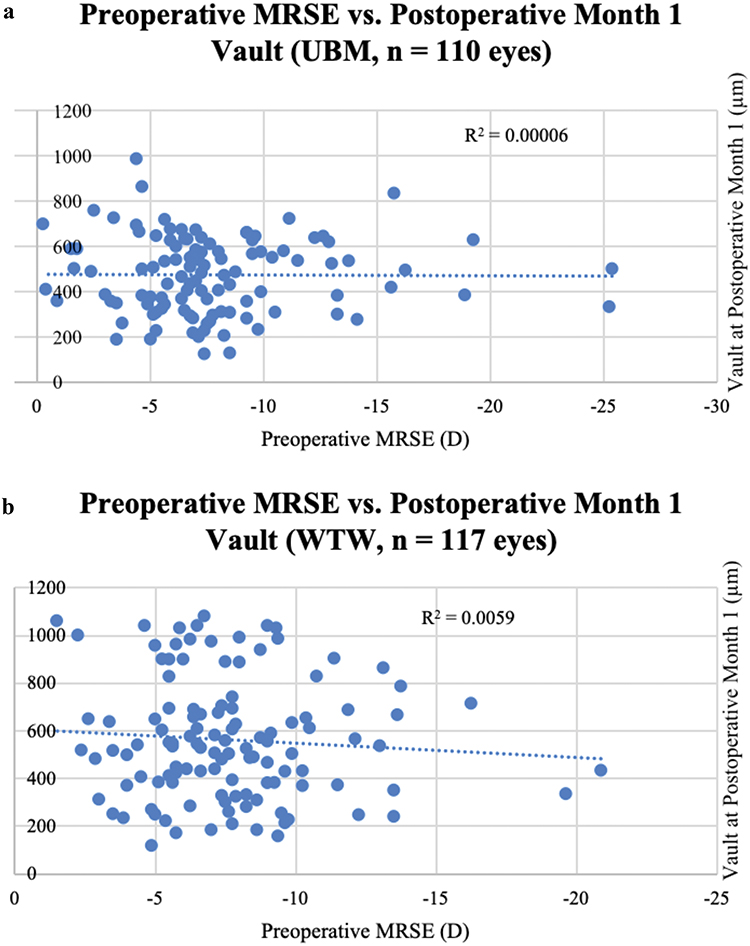 |
Figure 3 (a) Preoperative MRSE vs. Postoperative Month 1 Vault for UBM group. (b) Preoperative MRSE vs. Postoperative Month 1 vault for WTW group. |
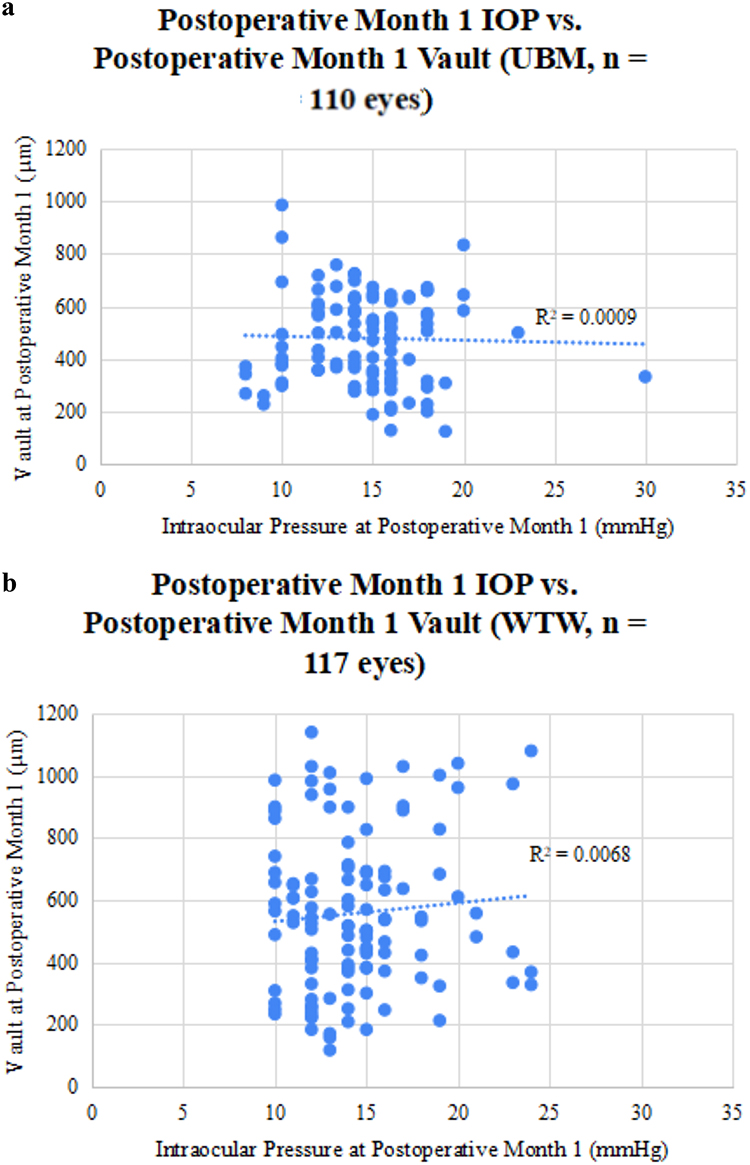 |
Figure 4 (a) Postoperative Month 1 IOP vs. Postoperative Month 1 Vault for UBM group. (b) Postoperative Month 1 IOP vs. Postoperative Month 1 Vault for WTW group. |
Preoperative axial length was analyzed and showed no significant correlation with the postoperative vault with both UBM and WTW groups (UBM group R2 = 0.0003; WTW Group R2 = 0.0038) (Figure 5a and b). Preoperative ACD was analyzed and showed a weak correlation with the postoperative vault in the UBM group but no significant correlation in the WTW group (UBM group R2 = 0.2257; WTW Group R2 = 0.0483) (Figure 6a and b).
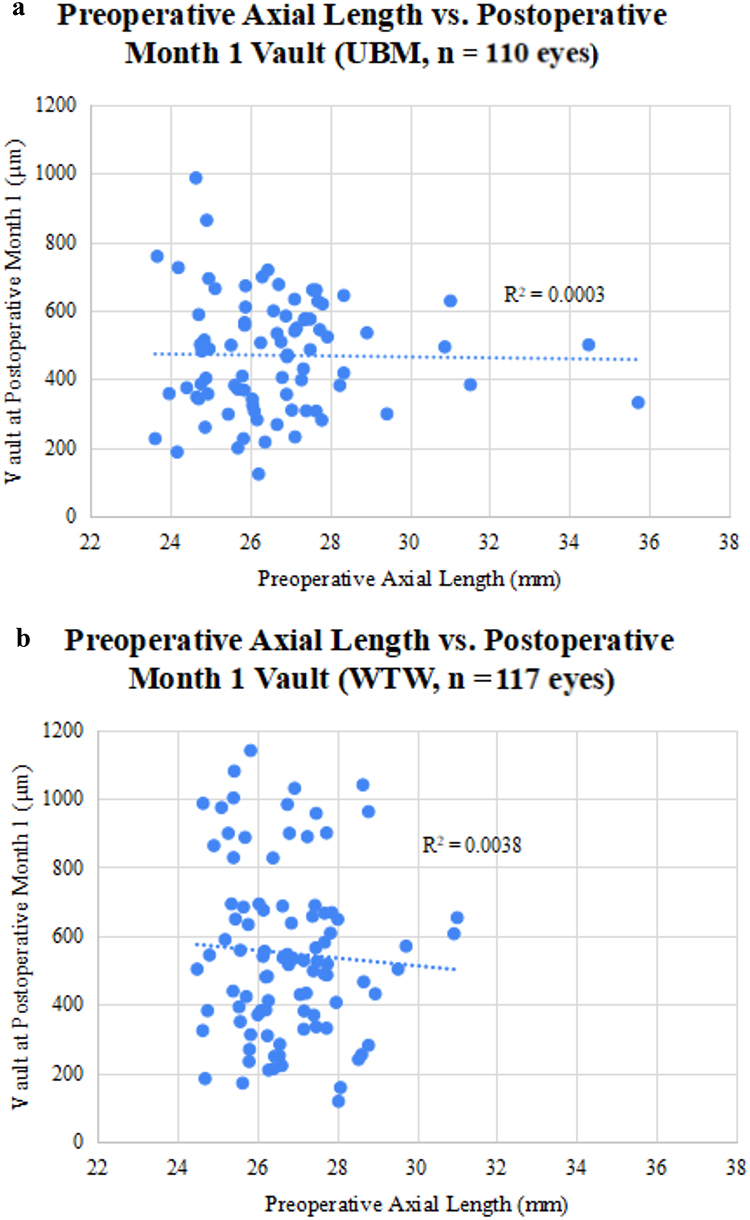 |
Figure 5 (a) Preoperative Axial Length vs. Postoperative Month 1 Vault for UBM group. (b) Preoperative Axial Length vs. Postoperative Month 1 Vault for WTW group. |
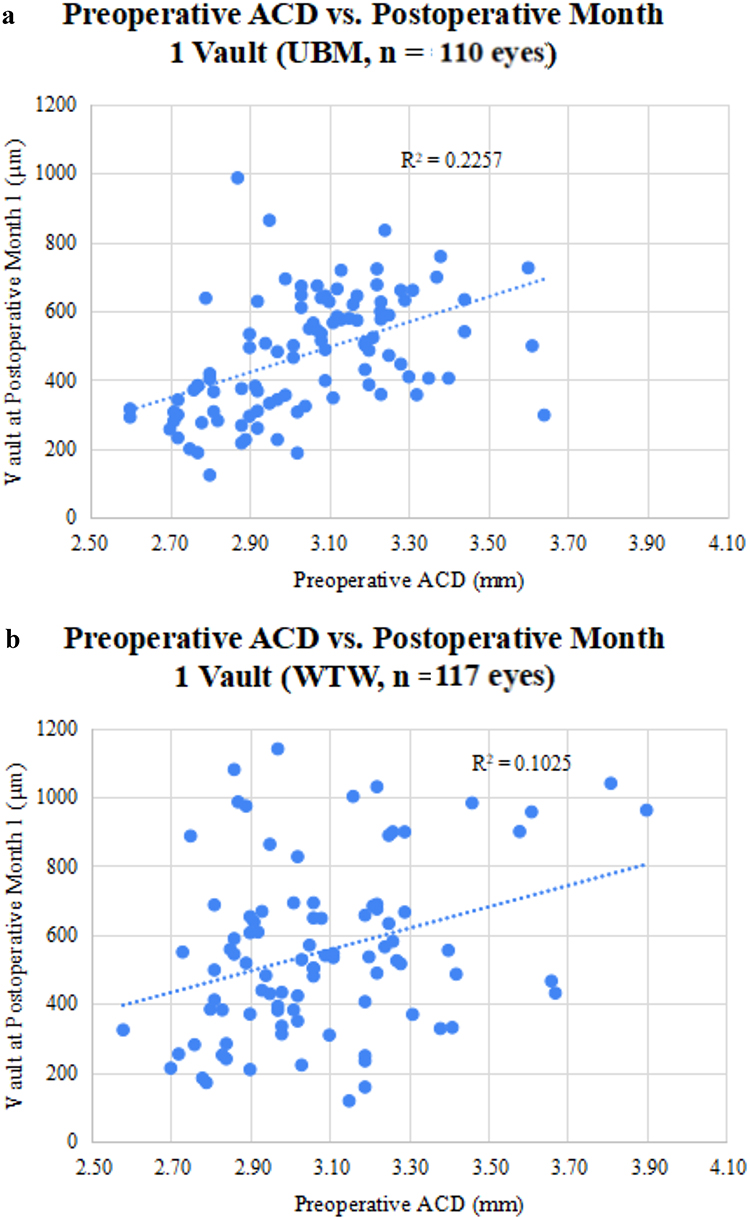 |
Figure 6 (a) Preoperative ACD vs. Postoperative Month 1 vault for the UBM Group. (b) Preoperative ACD vs. Postoperative Month 1 vault for the WTW Group. |
Discussion
ICL implantation in myopic patients is an established and effective treatment modality, as demonstrated in numerous studies by Packer, Chan, Du, and Qian.19–23 with similar or superior outcomes in correcting myopia compared to LVCs in a study reported in a study by Goes.19–24 The results showed comparable outcomes for both the UBM and WTW groups in terms of visual acuity. However, it also showed statistically significant differences for the postoperative vault. One of the most critical parameters for success in ICL implantation is achieving the ideal vault, as complications can occur if this is not optimized. An undersized ICL may result in low vault, potentially leading to cataract formation and ICL instability, which can cause rotations. Conversely, an oversized ICL can produce a high vault, increasing the risk of a narrow angle or angle-closure glaucoma, and thereby elevating intraocular pressure. The findings of the study showed that for the UBM group, there was increased incidence of patients being within the ideal vault range.
The meta-analysis by Packer examined the outcomes of the Visian V4c ICL. The analysis identified adequate patient satisfaction and favorable visual outcomes across all reported sizing methods at that time.5 In the FDA trial study by Packer assessing ICL effectiveness, the STAAR OCOS nomogram resulted in a UDVA gain at the 6-month follow-up for 629 eyes. Postoperative UDVA was −0.059 ± 0.10 logMAR, and the mean spherical equivalent (SE) was −0.079 ± 0.33 D. Notably, 90.5% of eyes were within ±0.50 D, and 98.9% within ±1.00 D of the intended target.19 Similarly, Chan reported that, in a 1-year follow-up of 83 eyes implanted with ICL, 77 eyes (93.4%) achieved 20/40 UDVA and 42 eyes (50.8%) achieved 20/20 vision.21 Similarly, a study by Du evaluated 1834 eyes over a one-year period showed a mean UDVA of −0.02 ± 0.09 logMAR and CDVA of −0.03 ± 0.08 logMAR, with safety and efficacy indices of 1.12 ± 0.17 and 1.10 ± 0.19, respectively. Approximately 85% of eyes achieved UDVA of 20/20 or better at 1 month.22 A recent study by Zaldivar evaluated outcomes of ICL implantation using the ICLGuru nomogram in 347 eyes. The visual outcomes were comparable, with 67% of eyes (232) reaching UDVA of 20/20, and most gaining lines in BCVA.17 In our study, visual outcomes were comparable between the WTW and UBM groups. The WTW group, utilizing the STAAR OCOS nomogram, demonstrated a 1-month postoperative UDVA of 0.03 ± 0.10 logMAR, CDVA of −0.00 ± 0.06 logMAR, and an MRSE of −0.04 ± 0.25 D, with 79% of eyes reaching 20/20 UDVA. The UBM group, using the ICLGuru nomogram, achieved similar results: 1-month postoperative UDVA of 0.05 ± 0.13 logMAR, CDVA of −0.01 ± 0.07 logMAR, and MRSE of −0.09 ± 1.14 D, with 68% reaching 20/20 UDVA. Our findings reinforce the conclusion of Packer’s study that outcomes remain consistent across different ICL sizing nomograms.5
Complication rates are minimal, as confirmed by the FDA trials by Packer, which reported adverse events such as elevated IOP, ICL exchange, and ICL rotation. The study by Du noted adverse events in 20.6% of 1834 eyes, including transient postoperative IOP elevation (9%), vault abnormalities (9.5%), ICL explantation due to capsular opacity (0.1%), and ICL rotation (2%). These were transient, with age identified as a risk factor.22 The FDA trial by Packer reported adverse events in 19.5% of eyes, primarily transient IOP elevation on day 1 postoperatively (18%) and steroid-induced IOP rise (1%). It is also noted that there was one case of ICL exchange due to development of a nuclear sclerotic cataract. No cases of pupillary block, angle-closure glaucoma, pigment dispersion, or anterior subcapsular cataract were observed in that study.19
Our study had a cumulative adverse event rate of 8.4% (19/227), confirming that minimal adverse events occur with ICL implantation. A total of 14 complications were observed in the WTW group at the 1-month postoperative period, comprising 6 eyes with transient elevated IOP, 2 eyes requiring ICL rotation, and 6 eyes requiring ICL exchange. The 2 cases of ICL rotation were due to ICL misalignment from the intended axis. The 6 eyes that underwent ICL exchange were paired eyes from three patients, all of whom demonstrated overvaulting, resulting in the need for a smaller size. In contrast, only 5 complications were observed in the UBM group, comprising 2 eyes with elevated IOP (2%) and 3 eyes requiring ICL rotation (3%). The UBM group had fewer IOP elevations at 1 month postoperatively involving both eyes of a single patient. The ICL size for both eyes was 12.1 with postoperative vaults of 500 μm and 332 μm. The increased IOP was managed medically with topical anti-glaucoma medication and was discontinued after IOP returned to normal levels on subsequent follow-up. In the UBM group, 3 eyes from 3 different patients required rotation due to misalignment from the intended axis. None required ICL exchange in the UBM group. No cataract formation was noted in both groups. Overall, the WTW group had more complications, specifically with elevated IOP and ICL exchange. Our study findings suggest that safety improved when we shifted to using the UBM-AI algorithm nomogram.
Packer found that implantation using different nomograms yielded similar results regarding vault and complication rates. Specifically, the meta-analysis showed that from 2005 onwards, there were no significant differences in vault outcomes between UBM STS-based and WTW-based nomograms (two-sample, two-sided t-test, pooled means and standard deviations; t(2594) = 1.33; P = 0.18).5 WTW-based nomograms reported by Packer showed a 1-month postoperative mean vault of 518 ± 232 μm and 502 ± 192 μm for the two studies evaluating ICL outcomes. The study by Du had a mean 6-month postoperative vault of 524.4 ± 102.8 μm for those with no increase in IOP and 535.9 ± 128.1 μm for those with higher IOPs.22 In a study by Qian of 163 eyes, the average vault at 3 months postoperatively was 388.01 ± 135.28 μm.23 In our study, the WTW-based nomogram had a mean vault of 557.78 ± 246.73 μm. These studies show that WTW-based nomograms can deliver vault measurements within the ideal range of 250–750 μm.
Using a UBM-based nomogram, Kojima reported a wide postoperative vault range of 150–1000 μm in 38 eyes.25 The ZZ nomogram developed by Zhang showed a mean vault of 528 ± 193 μm in 168 eyes.18 In a recent study by Zaldivar, using the same UBM-AI algorithm nomogram in our study, the vault measured at 1 month postoperatively was 484.81 ± 233.43 μm (range: 166–1031 μm) for 347 eyes.17 In our study, the UBM group showed a comparable mean vault of 472.25 ± 169.97 μm (range: 124–986 μm). Although this was statistically lower than the WTW group, the results remained within the clinically acceptable vault range in the majority of cases, indicating consistent and predictable achievement of target vault outcomes using the UBM-AI algorithm nomogram. Further analysis in our study revealed that the UBM group had a predictive accuracy within 383 μm of the intended vault across all eyes and 79% within 200 μm using the ICLGuru nomogram (Table 5).
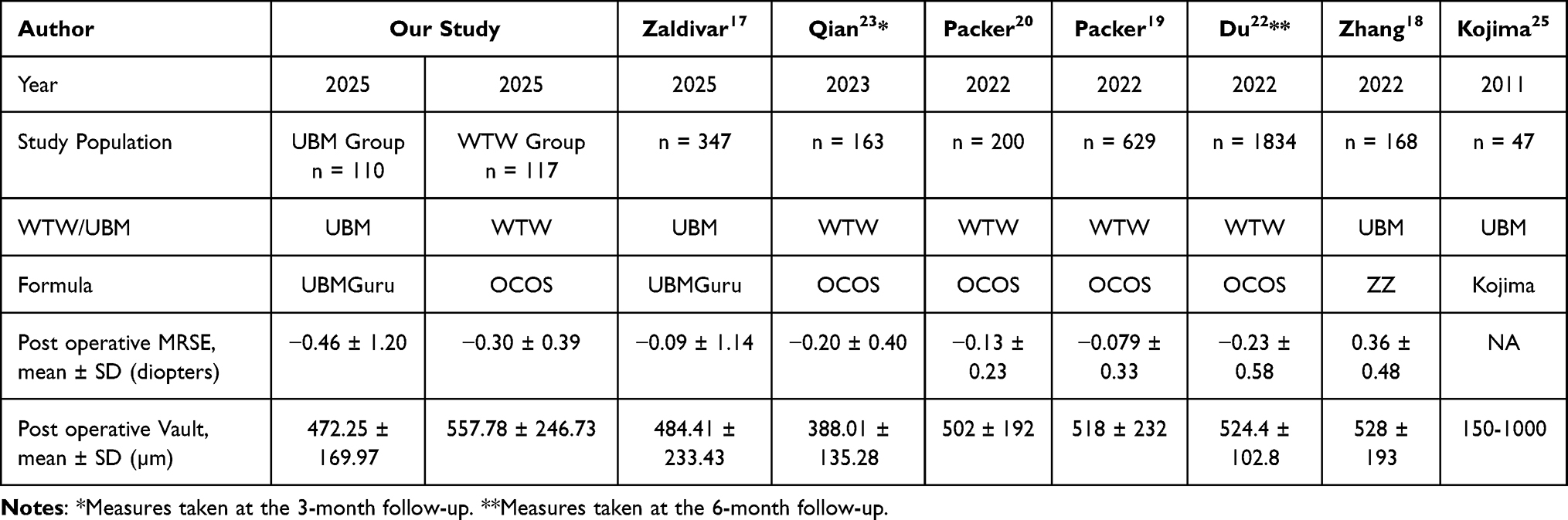 |
Table 5 Comparison of UBM and WTW Group with Other Studies |
The main objective of our study was to determine if the UBM-AI algorithm nomogram should be adopted as our standard of care in determining ICL size. There was a statistical difference between the mean vault with the UBM group at 472.25 ± 169.97 μm versus 557.78 ± 246.73 μm with the WTW group. Even if both mean vault measurements look similar, more importantly, 87.3% in the UBM group fall within the ideal vault range compared to 68.3% in the WTW group and this difference was statistically significant. Moreover, 7 eyes in the WTW group had vaults more than 1000 μm compared to none in the UBM group. This resulted in 6 eyes undergoing ICL exchange in the WTW group and none in the UBM group. Therefore, in terms of predictability in achieving the ideal vault range, safety, and avoidance of secondary surgical interventions, switching to the UBM-AI algorithm is the logical step going forward.
Our study tried to determine if there were preoperative parameters that could influence the postoperative vault. Our findings showed that the WTW, MRSE, IOP, and axial length (AL) had no correlation, while anterior chamber depth (ACD) had a mild correlation to postoperative vault. WTW measurements are inputted into the STAAR OCOS nomogram to determine the ICL size. Multiple studies have shown that the WTW-based nomograms achieve acceptable vault ranges with minimal safety issues. The UBM-AI algorithm produced vault measurements that had a higher incidence of achieving the ideal vault range compared to the WTW-based nomogram we had been using. Overvault and ICL exchange incidences were reduced with the use of the UBM-based nomogram.
Our study had several limitations. The WTW-based OCOS nomogram is dependent on different sources of WTW measurements, whether manual calipers or devices. We used a manual caliper to measure WTW, which is dependent on the person doing the measurements. The OCOS nomogram only recommends the ICL size but does not show a predicted vault. Therefore, we cannot directly compare the two nomograms in terms of predictive accuracy in the same eye. There are further improvements in the UBM-AI algorithm prediction software that were not used in the eyes in this study.
Conclusion
Visual and refractive outcomes were similarly good in both the WTW group and the UBM group. While the mean postoperative vaults were similar, there were more eyes in the UBM group within the ideal vault range. More incidence of overvaults in the WTW group resulted in more ICL exchanges. WTW measurements are inputted into the STAAR OCOS nomogram to determine the ICL size. Multiple studies have shown that the WTW-based nomograms achieve acceptable vault ranges with minimal safety issues. The UBM-AI algorithm produced vault measurements with a higher proportion of eyes achieving the ideal vault range compared to the WTW-based nomogram. While the mean vault values were comparable between the two methods, the UBM-based method approach demonstrated improved distributional accuracy, with fewer cases of overvault and a reduced need for ICL exchange.
Abbreviations
Units of Measurement: µm, micrometers; mm, millimeters; D, diopters; mmHg, millimeters of mercury. Symbols: UBM, Ultrasound Biomicroscopy; WTW, White-to-White; ICL, Implantable Collamer Lens; LVC, Laser Vision Correction; LASIK, Laser In Situ Keratomileusis; ACD, Anterior Chamber Depth; AL, Axial Length; IOP, Intraocular Pressure; STS, Sulcus-to-sulcus; ATA, Angle-to-angle; OCOS, Online Calculation & Ordering System.
Disclosure
Robert Edward Ang reports grants and personal fees from Staar Surgical, personal fees from Sonomed, personal fees from Heidelberg Engineering, grants, and personal fees from Bausch and Lomb during the conduct of the study; grants from Acevision, grants from Alcon, grants from Bausch and Lomb, grants from Glaukos, grants from Hoya, grants from Staar Surgical, grants from Vialase, grants from Spyglass, grants from Forsight Robotics, and grants from Teclens outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036–17. PMID: 26875007. doi:10.1016/j.ophtha.2016.01.006
2. Tideman JWL, Polling JR, Vingerling JR, et al. Axial length growth and the risk of developing myopia in European children. Acta Ophthalmol. 2018;96(3):301–309. PMID: 29265742; PMCID: PMC6002955. doi:10.1111/aos.13603
3. Philippine Eye Research Institute. National Institutes of Health. Philippine National Survey of Blindness and Eye Disease Study Project: study Results. [Internet] 2018 [Cited August 5, 2025] Available from: https://bit.ly/PEDS2018.
4. Flitcroft DI. The complex interactions of retinal, optical and environmental factors in myopia aetiology. Prog Retin Eye Res. 2012;31(6):622–660. Epub 2012 Jul 4. PMID: 22772022. doi:10.1016/j.preteyeres.2012.06.004
5. Packer M. Meta-analysis and review: effectiveness, safety, and central port design of the intraocular collamer lens. Clin Ophthalmol. 2016;10:1059–1077. PMID: 27354760; PMCID: PMC4907705. doi:10.2147/OPTH.S111620
6. Thompson V, Cummings AB, Wang X. Implantable collamer lens procedure planning: a review of global approaches. Clin Ophthalmol. 2024;18:1033–1043. PMID: 38601168; PMCID: PMC11005927. doi:10.2147/OPTH.S456397
7. Kamiya K, Shimizu K, Igarashi A, et al. Posterior chamber phakic intraocular lens implantation: comparative, multicentre study in 351 eyes with low-to-moderate or high myopia. Br J Ophthalmol. 2018;102(2):177–181. PMID: 28611132. doi:10.1136/bjophthalmol-2017-310164
8. Alfonso JF, Fernández-Vega L, Lisa C, Fernandes P, Jorge J, Montés Micó R. Central vault after phakic intraocular lens implantation: correlation with anterior chamber depth, white-to-white distance, spherical equivalent, and patient age. J Cataract Refract Surg. 2012;38(1):46–53. PMID: 22153092. doi:10.1016/j.jcrs.2011.07.035
9. Ang RET, Reyes EKF, Ayuyao FAJ Jr, Umali MIN, Cruz EM. Comparison of white-to-white measurements using four devices and their determination of ICL sizing. Eye Vis. 2022;9(1):36. PMID: 36182955; PMCID: PMC9526955. doi:10.1186/s40662-022-00308-z
10. Choi KH, Chung SE, Chung TY, Chung ES. Ultrasound biomicroscopy for determining visian implantable contact lens length in phakic IOL implantation. J Refract Surg. 2007;23(4):362–367. doi:10.3928/1081-597X-20070401-08
11. Baumeister M, Terzi E, Ekici Y, Kohnen T. Comparison of sulcus-to-sulcus diameter and anterior chamber depth in high myopia. Ophthalmology. 2004;111(6):1040–1045. doi:10.1016/j.ophtha.2003
12. Reinstein DZ, Lovisolo CF, Archer TJ, Gobbe M. Comparison of postoperative vault height predictability using white-to-white or sulcus diameter-based sizing for the visian implantable collamer lens. J Refract Surg. 2013;29(1):30–35. PMID: 23311739. doi:10.3928/1081597X-20121210-02
13. Rocamora L, Orlando JI, Lwowski C, Kohnen T, Mertens E, Van Keer K. Postoperative vault prediction for phakic implantable collamer lens surgery: LASSO formulas. J Cataract Refract Surg. 2023;49(2):126–132. doi:10.1097/j.jcrs.0000000000001079
14. Reinstein DZ, Archer TJ, Silverman RH, Rondeau MJ, Coleman DJ. Correlation of anterior chamber angle and ciliary sulcus diameters with white-to-white corneal diameter in high myopes using Artemis VHF digital ultrasound. J Refract Surg. 2009;25:185–194. doi:10.3928/1081597X-20090201-03
15. Elfalah M, Mohammad M, Toro MD, Abu-Yaghi N, Rejdak R, Yousef YA. Anterior ocular biometrics as measured by ultrasound biomicroscopy. Healthcare. 2022;10(7):1188. PMID: 35885715; PMCID: PMC9318338. doi:10.3390/healthcare10071188
16. Shen Y, Wang L, Jian W, et al. Big-data and artificial-intelligence-assisted vault prediction and EVO-ICL size selection for myopia correction. Br J Ophthalmol. 2023;107(2):201–206. PMID: 34489338; PMCID: PMC9887372. doi:10.1136/bjophthalmol-2021-319618
17. Zaldivar R, Cummings A, Mertens B, et al. Evaluating the predictive accuracy of an ai-based tool for postoperative vault estimation in phakic intraocular lens implantation. Clin Ophthalmol. 2025;19:1945–1956.
18. Zhang J, Shao J, Zheng L, Zhao X, Chen S. Implantable collamer lens sizing based on measurement of the sulcus-to-sulcus distance in ultrasound biomicroscopy video clips and ZZ ICL formula. BMC Ophthalmol. 2022;22(1):363. PMID: 36071422; PMCID: PMC9454160. doi:10.1186/s12886-022-02583-9
19. Packer M. Evaluation of the EVO/EVO+ sphere and toric visian ICL: six month results from the united states food and drug administration clinical trial. Clin Ophthalmol. 2022;16:1541–1553. PMID: 35645557; PMCID: PMC9132105. doi:10.2147/OPTH.S369467
20. Packer M. The EVO ICL for moderate myopia: results from the US FDA clinical trial. Clin Ophthalmol. 2022;16:3981–3991. PMID: 36510599; PMCID: PMC9738966. doi:10.2147/OPTH.S393422
21. Chan AT, Zauberman NA, Chan CC, Rootman DS. Outcomes after implantable collamer lens surgery in a Canadian cohort. Can J Ophthalmol. 2017;52(2):150–154. PMID: 28457282. doi:10.1016/j.jcjo.2016.08.015
22. Du J, Zhou W, Zhao T, et al. Efficacy and safety of implantable collamer lens V4c implantation in 1834 myopic eyes for 1 year of follow-up. J Refract Surg. 2023;39(10):694–704. PMID: 37824302. doi:10.3928/1081597X-20230908-02
23. Qian T, Du J, Ren R, et al. Vault-correlated efficacy and safety of implantable collamer lens V4c implantation for myopia in patients with shallow anterior chamber depth. Ophthalmic Res. 2023;66(1):445–456. PMID: 36596292. doi:10.1159/000528616
24. Goes S, Delbeke H. Posterior chamber toric implantable collamer lenses vs LASIK for myopia and astigmatism: systematic review. J Cataract Refract Surg. 2022;48(10):1204–1210. doi:10.1097/j.jcrs.000000000000100
25. Kojima T, Yokoyama S, Ito M, et al. Optimization of an implantable collamer lens sizing method using high-frequency ultrasound biomicroscopy. Am J Ophthalmol. 2012;153(4):632–7637.e1. PMID: 22245462. doi:10.1016/j.ajo.2011.06.031
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evaluation of the EVO/EVO+ Sphere and Toric Visian ICL: Six Month Results from the United States Food and Drug Administration Clinical Trial
Packer M
Clinical Ophthalmology 2022, 16:1541-1553
Published Date: 21 May 2022
Photorefractive Keratectomy Enhancement (PRK) After Small-Incision Lenticule Extraction (SMILE)
Moshirfar M, Parsons MT, Chartrand NA, Lau CK, Stapley S, Bundogji N, Ronquillo YC, Hoopes PC
Clinical Ophthalmology 2022, 16:3033-3042
Published Date: 12 September 2022
Visual Acuity Improvement in Low, Moderate and High Myopia After Posterior-Chamber Phakic Implantable Collamer Lens Surgery in a Large Patient Cohort
Zaldivar R, Zaldivar R, Gordillo CH, Adamek P
Clinical Ophthalmology 2023, 17:1179-1185
Published Date: 18 April 2023
Influence of Preoperative Parameters on the Ratio of Keratometric Change per Diopter of Attempted Spherical Equivalent (∆K/∆SEQ) for Myopic Correction Within LASIK, PRK, and SMILE
Moshirfar M, Theis JS, Cha DS, Porter KB, Payne CJ, Hoopes PC
Clinical Ophthalmology 2023, 17:2563-2573
Published Date: 29 August 2023
A Comprehensive Retrospective Analysis of EVO/EVO+ Implantable Collamer Lens: Evaluating Refractive Outcomes in the Largest Single Center Study of ICL Patients in the United States
Albo C, Nasser T, Szynkarski DT, Nguyen N, Mueller B, Libfraind L, Parkhurst G
Clinical Ophthalmology 2024, 18:69-78
Published Date: 9 January 2024