Back to Journals » Clinical Ophthalmology » Volume 16
Photorefractive Keratectomy Enhancement (PRK) After Small-Incision Lenticule Extraction (SMILE)
Authors Moshirfar M ![]() , Parsons MT
, Parsons MT ![]() , Chartrand NA
, Chartrand NA ![]() , Lau CK
, Lau CK ![]() , Stapley S
, Stapley S ![]() , Bundogji N, Ronquillo YC
, Bundogji N, Ronquillo YC ![]() , Hoopes PC
, Hoopes PC ![]()
Received 6 July 2022
Accepted for publication 29 August 2022
Published 12 September 2022 Volume 2022:16 Pages 3033—3042
DOI https://doi.org/10.2147/OPTH.S381319
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Majid Moshirfar,1– 3 Mark T Parsons,4 Nicholas A Chartrand,4 Chap-Kay Lau,4 Seth Stapley,5 Nour Bundogji,2 Yasmyne C Ronquillo,1 Phillip C Hoopes1
1Hoopes Vision Research Center, Hoopes Vision, Draper, UT, USA; 2John A. Moran Eye Center, University of Utah School of Medicine, Salt Lake City, UT, USA; 3Utah Lions Eye Bank, Murray, UT, USA; 4University of Arizona College of Medicine – Phoenix, Phoenix, AZ, USA; 5Arizona College of Osteopathic Medicine, Midwestern University, Glendale, AZ, USA
Correspondence: Majid Moshirfar, Hoopes Vision Research Center, 11820 S. State Street Suite #200, Draper, UT, 84020, USA, Tel +1 801-568-0200, Fax +1 801-563-0200, Email [email protected]
Purpose: To determine rates of enhancement and visual prognosis following photorefractive keratectomy (PRK) enhancement of small-incision lenticule extraction (SMILE).
Patients and Methods: This retrospective, single-site study reviewed all cases of primary SMILE at Hoopes Vision in Draper, Utah between March 14, 2017 and April 8, 2022 to identify any cases that required follow-up enhancement. Primary SMILE was performed using Visumax 500 kHz femtosecond laser (Carl Zeiss Meditec, Jena, Germany). All enhancements were performed with alcohol-assisted PRK, using a WaveLight EX500 excimer laser (Alcon Laboratories, Inc., Fort Worth, TX).
Results: Four hundred and five eyes underwent primary SMILE, of which 15 later underwent PRK enhancement (enhancement rate of 3.7%). No significant difference in pre-SMILE data was identified between the enhancement and non-enhancement groups. The average age of those who underwent PRK enhancement was 33.8± 6.3 years old and ranged from 25 to 45. Following primary SMILE, 13 eyes (87%) had an uncorrected distance visual acuity (UDVA) of 20/40 or better, and none had a UDVA of 20/20 or better. After one year of post-enhancement follow-up, all eyes had a UDVA of 20/40 or better, and 13 eyes (87%) had a UDVA of 20/20 or better (Figure 1). All were within one diopter of target spherical equivalent (SEQ), 13 (87%) were within 0.50 D, and 10 (67%) were within 0.25 D. Of those with 12-month follow-up data, none had UDVA worse than corrected distance visual acuity (CDVA), and none had lost lines of CDVA. Efficacy and safety indices were 1.03 and 0.99, respectively.
Conclusion: Following SMILE, ophthalmologists may anticipate an enhancement rate of one to seven percent. In these cases, PRK is a safe and effective procedure for enhancement of SMILE.
Keywords: retreatment, LASIK, refractive surgery, myopia, astigmatism, SMILE
Introduction
Small-incision lenticule extraction (SMILE) is a refractive procedure approved by the United States Food and Drug Administration (FDA) for the correction of myopia and myopic astigmatism in 2016 and 2018, respectively.1–3 The procedure is performed using the VisuMax Laser System (Carl Zeiss AG, Jena, Germany) and uses a femtosecond laser to incise and carve a lenticule within the corneal stroma without creating a corneal flap. The lenticule is then excised from the cornea to achieve refractive correction.1 According to Zeiss, over four million SMILE procedures had been performed worldwide as of June 2021.4
As with other refractive surgeries, a subset of SMILE patients requires follow-up enhancement. While well studied in laser-assisted in-situ keratomileusis (LASIK), less literature exists regarding enhancement of SMILE.5 Enhancement may be required due to a delayed myopic regression or an initial under- or overcorrection.5 In these cases, the most common enhancement procedures are photorefractive keratectomy (PRK) and LASIK,6,7 though there are some reports of repeat SMILE.8
This retrospective, single-site review seeks to determine rates of enhancement and visual prognosis following PRK enhancement of SMILE.
Materials and Methods
Patient Selection
This retrospective study includes all patients who underwent SMILE at Hoopes Vision in Draper, Utah, USA between March 14, 2017 and April 8, 2022. Primary outcomes were rate of enhancement, post-enhancement uncorrected distance visual acuity (UDVA), and post-enhancement corrected distance visual acuity (CDVA). Data collected for all patients included age at SMILE, gender, pre-SMILE target refraction, SMILE laser set values, and pre-SMILE sphere, cylinder, axis, UDVA, CDVA, keratometry, and pachymetry. For those who underwent PRK enhancement, the same data was collected pre-PRK and at three and 12 months post-PRK. Spherical equivalent (SEQ) was calculated by adding the sphere value to half of the cylinder value in diopters (D).
Primary SMILE Procedure
SMILE procedures were performed using Visumax 500 kHz femtosecond laser (Carl Zeiss Meditec, Jena, Germany). Preoperatively, the limbus was marked at 3 and 9 o’clock with a surgical marking pen while the patient was seated and upright. Intraoperatively, the cornea was marked at the corresponding 3 and 9 o’clock positions inside the limbus using a caliper set at 8 mm and while the patient was supine. Suction was applied for fixation, and the interface cone was gently rotated manually to correct any cyclotorsion noted. Settings included a 120 µm cap thickness and a 7.5 mm cap diameter. The hinge was placed superiorly with a 60-degree hinge angle and a 90-degree side-cut angle. Diameter of the lenticule was 6.5 mm with 4.4 µm spot separation. Lenticule side-cut, flap, and flap side-cut had spot separations of 2.0 µm, 3.0 µm, and 2.0 µm, respectively. Laser-bed energy was 130 nJ. Post-operative regimen included fluoroquinolone antibiotic drops four times daily for one week and 1% prednisolone acetate drops four times daily for one week. After the first week, prednisolone was tapered over the subsequent three weeks.
PRK Enhancement Procedure
Enhancement was performed via alcohol-assisted PRK. Epithelial debridement was performed with 18% alcohol for 25 seconds, followed by stromal ablation with a WaveLight EX500 excimer laser (Alcon Laboratories, Inc., Fort Worth, Texas, USA). Laser settings included an ablation zone of 6.5 mm and a transitional zone of up to 9.0 mm. Mitomycin C 0.02% was applied for 20 seconds whenever ablation depth exceeded 65 microns. After the procedure, a bandage contact lens was placed for one week. Post-operative regimen included topical moxifloxacin 0.5% four times daily for one week and prednisolone acetate 1% four times daily for one month. After one month, prednisolone acetate was replaced with fluorometholone 0.1% four times daily, which was then tapered until 12 weeks post-operative.
Statistical Analysis
A two-sample, two-tailed (unpaired/independent) t-test was used to compare age, sphere, cylinder, SEQ, UDVA, CDVA, keratometry, and pachymetry between pre-SMILE enhancement and non-enhancement groups (Table 1). Gender and laterality of operated eyes were assessed using a chi-squared test. In comparing pre-enhancement and post-enhancement parameters, a paired, two-tailed t-test was used (Table 2). This t-test was performed using the 12-month follow-up data as the post-enhancement data. If there was no 12-month follow-up for a patient, the latest post-operative visit available was used. We also stratified the enhancement group by those whose SMILE procedure resulted in spherical overcorrection versus undercorrection and performed the same paired, two-tailed t-test. Efficacy and safety indices were calculated by dividing the mean post-operative UDVA by the mean pre-operative CDVA, and by dividing the mean post-operative CDVA by the mean pre-operative CDVA, respectively. Statistical analyses were performed using Microsoft Excel 2016. P-values less than 0.05 were considered statistically significant.
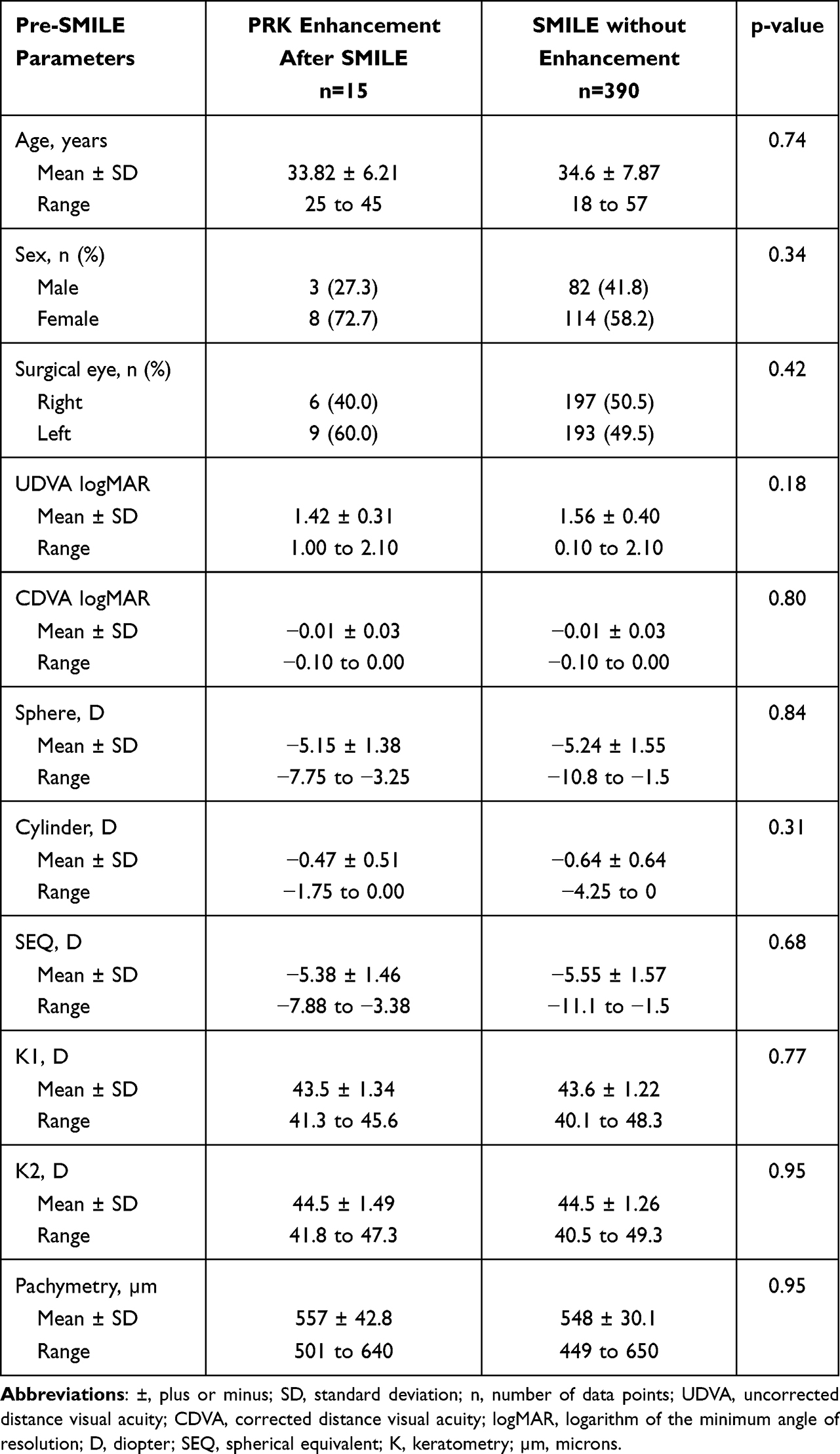 |
Table 1 Demographic/Preoperative Comparisons Between the Enhancement and Non-Enhancement Groups |
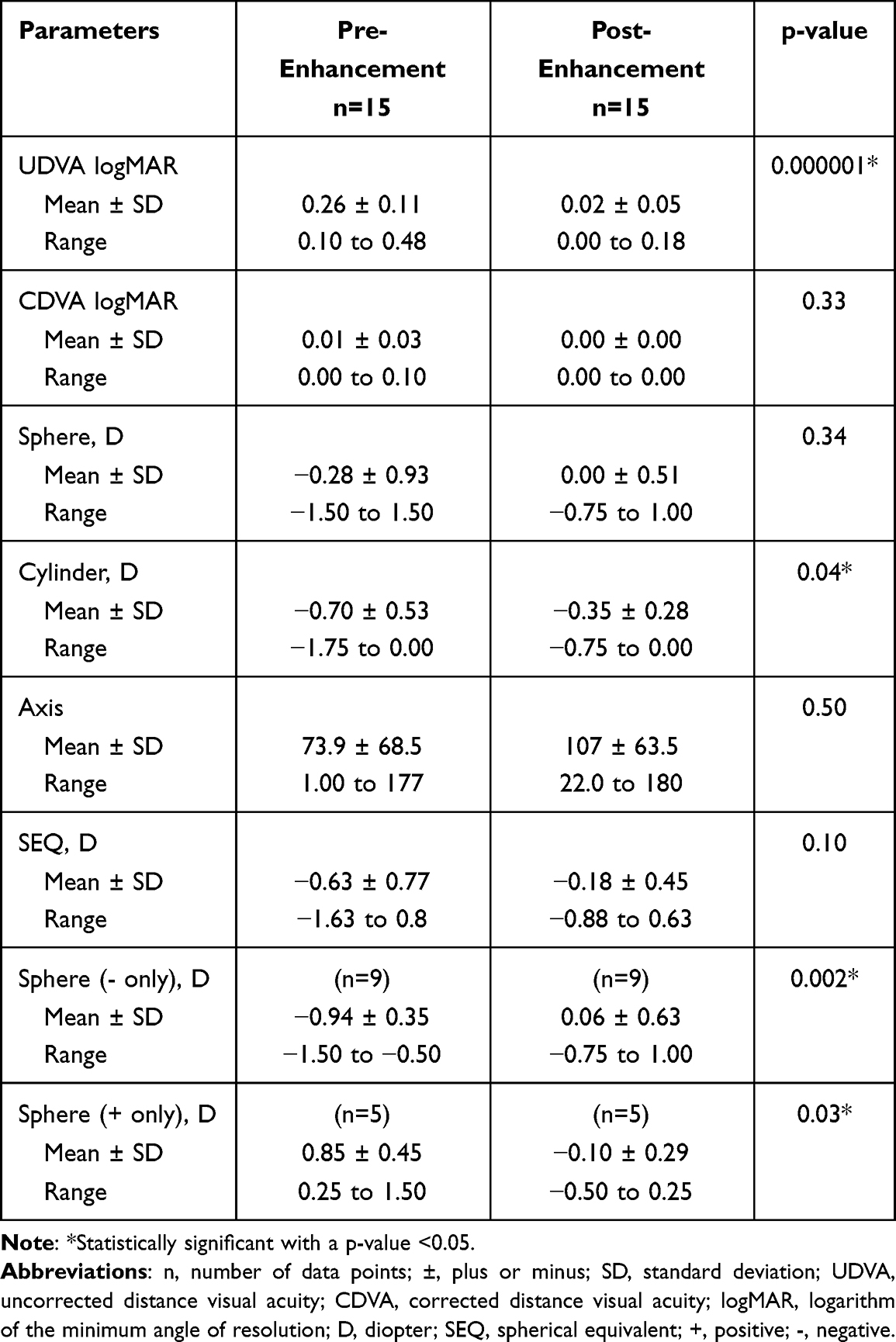 |
Table 2 Pre-Enhancement and Post-Enhancement Parameters |
Results
Following primary SMILE, 15 out of 405 eyes (11 out of 207 patients) underwent PRK enhancement, equating to a 3.7% rate of enhancement. The mean time between SMILE and the most recent follow-up visit after PRK enhancement was 27±18.9 months (range: 2 to 63). Considering only those patients with one and two years of follow-up, we identified a 1 and 2-year rate of enhancement of 1.3% and 7.3%, respectively. The mean time between primary SMILE and PRK enhancement was 15.9±6.94 months (range five to 26 months). Eight out of eleven patients (73%) who underwent enhancement were female.
Rates of enhancement were also stratified by the year initial SMILE was performed. Though the mean time between SMILE and enhancement was the same, the rate of enhancement decreased from 10% to 2% between 2019 and 2020. Additionally, we calculated a normalized rate of enhancement of 1.8 enhancements per 100 person-years.
No statistically significant differences were found in age, gender, laterality, or pre-SMILE sphere, cylinder, SEQ, UDVA, CDVA, keratometry, or pachymetry between the enhancement and non-enhancement groups (Table 1). The average age of patients who underwent PRK enhancement was 33.8±6.3 years (range 25 to 45), compared to 34.6±7.8 years (range 18 to 57) in the non-enhancement group. 73% of patients in the enhancement group were female, compared to 58% in the non-enhancement group. When the enhancement group was stratified into those whose SMILE resulted in undercorrection and in overcorrection, there was no statistical significance between these groups in age, SEQ, UDVA, or CDVA before SMILE, though the mean SEQ was less myopic in the overcorrection group (−5.03±1.44 D versus −5.56±1.51 D; p = 0.52).
Following primary SMILE, 13 eyes (87%) had a UDVA of 20/40 or better, and none had a UDVA of 20/20 or better. Nine eyes (60%) were within 1.0 D of target SEQ, and two (13%) were within 0.5 D. Mean SEQ was −0.63±0.77 D and mean cylinder was −0.70±0.53 D (Table 2). Nine eyes (60%) had spherical undercorrection, five (33%) had spherical overcorrection, and one was spherically plano (7%). While all eyes had a CDVA of 20/40 or better, 14 eyes (93%) had a post-SMILE CDVA of 20/20 or better.
After one year of post-enhancement follow-up, all eyes had a UDVA of 20/40 or better, and 13 eyes (87%) had a UDVA of 20/20 or better (Figure 1). All were within one diopter of target SEQ, 13 (87%) were within 0.50 D, and 10 (67%) were within 0.25 D. We identified statistically significant improvements in UDVA and cylinder, with a final UDVA of 0.02±0.05 and a final cylinder of −0.35±63.5 D (Table 2). Mean sphere did not show a significant change for the group as a whole. When sphere was stratified into groups of either negative or positive spheres, significant improvements were seen for each. Mean SEQ improved from −0.63±0.77 D to −0.18±0.45 D but was not statistically significant (p = 0.10). Of those with 12-month follow-up data, none had UDVA worse than CDVA, and none had lost lines of CDVA. Efficacy and safety indices were 1.03 and 0.99, respectively.
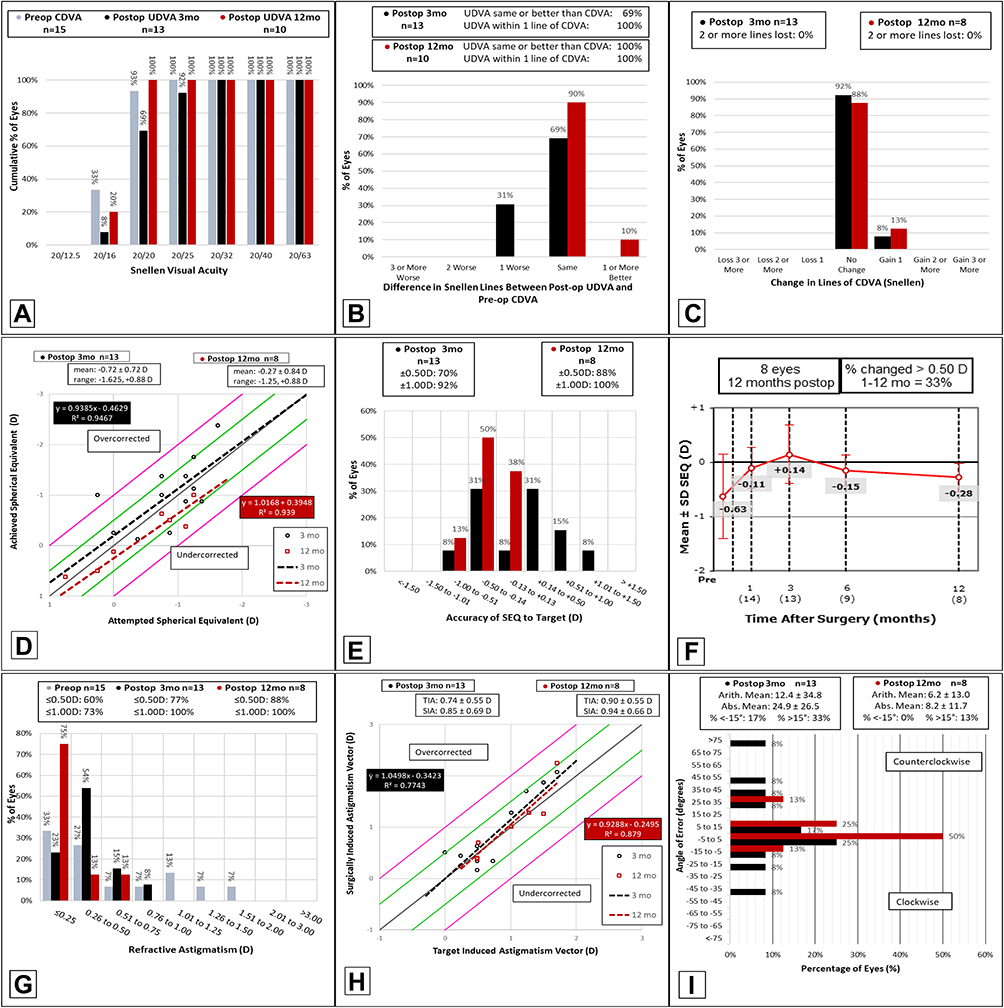 |
Figure 1 Standard nine graphs of refractive surgery for PRK-enhancement of SMILE. (A) Cumulative preoperative Snellen CDVA (gray), postoperative UDVA at three months (black), and postoperative UDVA at 12 months (red). (B) Difference in number of Snellen lines between postoperative UDVA and preoperative CDVA at three months (black) and 12 months (red) postoperative. (C) Postoperative change in number of Snellen lines of CDVA at three months (black) and 12 months (red), as compared to preoperative CDVA. (D) Attempted versus achieved postoperative spherical equivalent refraction at three months (black points) and 12 months (red points). Black and red dotted lines are the lines of best fit at three and 12 months, respectively, with their parameters (mathematical formula and R-squared, the coefficient of determination) given in the black and red boxes. The gray line represents the points where achieved equals attempted correction. The green line represents the points where achieved correction is ±0.5 D from attempted correction. The magenta line represents where achieved correction is ±1.0 D from attempted correction. (E) Accuracy of postoperative spherical equivalent refraction relative to target at three months (black) and 12 months (red). (F) Refractive stability as demonstrated by mean spherical equivalent refraction at one, three, six, and 12 months. (G) Refractive astigmatism preoperatively (gray), three months postoperatively (black), and 12 months postoperatively (red). (H) Target versus surgically induced postoperative astigmatism at three months (black points) and 12 months (red points). Black and red dotted lines are the lines of best fit at three and 12 months, respectively, with their parameters (mathematical formula and R-squared, the coefficient of determination) given the black and red boxes. The gray line represents the points where surgically induced equals target. The green line represents the points where surgically induced astigmatism is ±0.5 D from target induced astigmatism. The magenta line represents the points where surgically induced astigmatism is ±1.0 D from target. (I) Refractive astigmatism angle of error at three months (black) and 12 months (red) postoperative. Abbreviations: CDVA, corrected distance visual acuity; UDVA, uncorrected distance visual acuity; mo, months; VA, visual acuity; D, diopters; ±, plus or minus; SEQ, spherical equivalent; TIA, target induced astigmatism; SIA, surgically induced astigmatism; arith. mean, arithmetic mean; abs. mean, absolute mean. |
Discussion
Between the first published trials of SMILE in 2011 and June 2022,9 we identified twelve studies in the literature that present cases of enhancement following SMILE (Table 3).5,8,10–18 Of these, eight identified rates of enhancement following SMILE. In a 2017 study in Singapore, Liu et al found a prevalence, 1-year incidence, and 2-year incidence of enhancement of 2.7%, 2.1%, and 2.9%, respectively.5 These rates differ somewhat but are comparable to those in our study (3.5%, 1.3%, and 7.3%). Other reported rates are similar, ranging from 1.1% to 4.4%. Additionally, Liu et al calculated a median time of 10.5 months between primary SMILE and enhancement (range 7–22 months), lower than but comparable to our findings (median 17 months, range 5–26 months).5
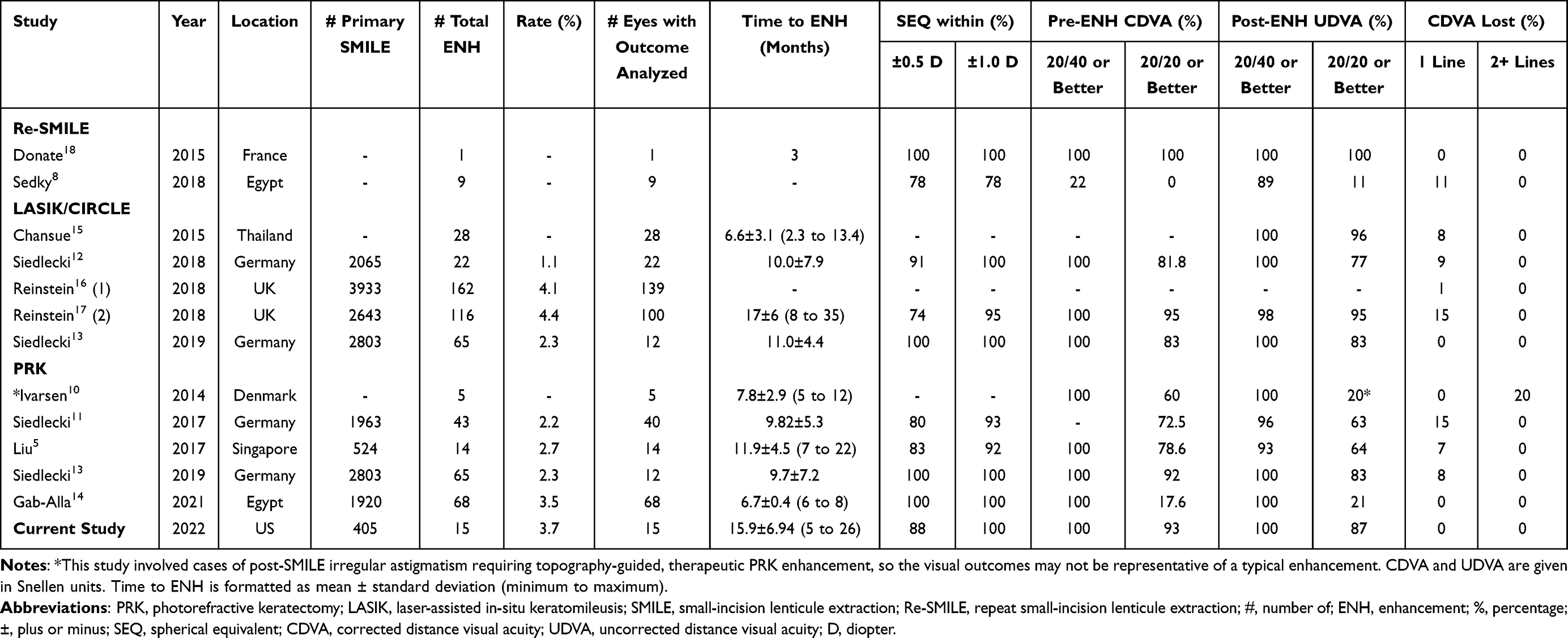 |
Table 3 Published Literature Concerning Visual Outcomes of SMILE Enhancement |
When rates of enhancement were stratified by year in which primary SMILE was performed, 2020 and 2021 had lower rates (2% and 0%, respectively) than 2017 and 2019 (9% and 10%, respectively). Note that 2018 had a rate of 0% but had a disproportionately small sample size (18 eyes). The mean time between SMILE and enhancement was similar for each year and was within follow-up time. Though further follow-up is necessary to support this finding, this suggests that SMILE outcomes have improved since the procedure began. This could be attributable to both increased surgical experience and refinement of the surgical nomogram. In the first year, 2017, only spherical correction was available in the United States.1 In 2018, SMILE was approved for myopic astigmatism.3 By 2020, the nomogram had been refined, improving the achieved refractive accuracy.
Patients who underwent enhancement tended to have unsatisfactory refractive outcomes following primary SMILE, with most having residual refractive error and none having a UDVA of 20/20 or better. Other studies note the same. Liu et al reported that pre-enhancement UDVA ranged from 20/80 to 20/25 with most cases due to undercorrection,5 and Siedlecki et al reported a mean pre-enhancement spherical equivalent of −0.51±1.08 D, with 32% within 1.00 D of target refraction.12 Most of the cases in our study were due to undercorrection, though a few were cases of overcorrection. While there was no statistically significant difference in pre-SMILE data between the over- and undercorrection groups, the small sample size makes this distinction difficult. However, it is reasonable to consider that patients with less significant myopia may be more likely to be overcorrected.
We found no statistical difference between the enhancement and non-enhancement groups pre-SMILE. In contrast, Liu et al found statistically significant differences between these groups for eye laterality, age at SMILE, pre-operative SEQ, myopia, and astigmatism despite having a similar sample size (14 eyes).5 They reported that the most significant risk factor for enhancement was age greater than 35 years (odds ratio: 5.58). Other significant risk factors in their study arranged in order of decreasing odds ratio included right-sided laterality, high preoperative SEQ or astigmatism, and intraoperative suction loss.
In this study, PRK resulted in the successful enhancement of SMILE with respect to indices of both safety and efficacy. Other studies reported similar results, whether the enhancement procedure was PRK or LASIK (Table 3). Outcomes of efficacy in the literature include a rate of 74–100% of patients reporting a post-enhancement SEQ within 0.50 D of target and 92–100% within one diopter. Additionally, 93–100% of patients are reported to have a post-enhancement UDVA of 20/40 or better, and 20–95% with 20/20 or better. Reported safety outcomes include 0–15% with one line of CDVA lost and 0–20% with two or more lines lost. These reports are similar to the present study, where 88% were within 0.5 D of target, 100% within 1.0 D, 100% with UDVA 20/40 or better, 75% 20/20 or better, and no eyes lost lines of CDVA.
Five studies used PRK, five used LASIK or CIRCLE, and two used Re-SMILE for the enhancement. One of the Re-SMILE studies is a single case report,18 and the other was a series of nine cases.8 Though this small sample size makes comparison with Re-SMILE difficult, the outcomes of the PRK and LASIK studies can be compared. The earliest of these, a 2014 study by Ivarsen et al, involved therapeutic enhancement following five cases of SMILE complicated by post-operative irregular astigmatism.10 Considering this complication, visual outcomes are poorer than in the other studies and may not be representative of a typical enhancement. Excluding this study, the visual outcomes between the PRK and LASIK studies are comparable. However, some trends can be identified. Measures of safety are similar in both groups, but loss of two or more lines of CDVA was only reported in PRK. Regarding efficacy, LASIK studies had higher post-enhancement rates of 20/20 UDVA, though UDVA in one PRK study was limited by poor pre-CDVA.14 Accuracy of achieved SEQ was comparable between the two groups. Notably, we did not distinguish between cases of thin-flap LASIK and CIRCLE, so we cannot suggest whether the trends above represent only one or both methods.
Though our literature search suggests that LASIK enhancement may have a marginally higher safety and efficacy than PRK enhancement, there is not enough data to make this conclusion. A few considerations need to be discussed when comparing PRK enhancement with other enhancement methods. Electing to have LASIK after receiving SMILE defeats the biomechanical advantages that SMILE offers by avoiding a flap. Furthermore, in LASIK/CIRCLE, there is a risk of corneal weakening due to the damage of Bowman’s layer and anterior corneal cap,19 and a subset of patients may be unable to receive LASIK/CIRCLE due to insufficient residual stromal depth. Conversely, PRK enhancement offers several advantages over LASIK/CIRCLE, including stronger biomechanical properties and preservation of the stromal bed. It is also considered the most straightforward approach compared to the other methods. A drawback of PRK enhancement post-SMILE is increased inflammatory and apoptotic cells compared to other methods of enhancement; however, this can be controlled with mitomycin-C.20 Ophthalmologists who are working with patients seeking enhancement after SMILE should consider the advantages and disadvantages of each retreatment method to ensure high efficacy and safety.7
Though SMILE has been FDA-approved in the United States since 2016, relatively little information has been reflected on this topic from North America. Considering the sparsity of research done in this region, the authors believe this work adds value and supports the existing literature in other parts of the world. Limitations of this study include the small sample size and non-linear follow-up data. Another limitation is the changing experience of surgeons after SMILE procedures began and the refinement of the surgical nomograms as more procedures were carried out over time. Future studies can be conducted with larger sample sizes and more structured follow-up visits.
Conclusion
This study retrospectively reviewed 15 cases of PRK enhancement following SMILE. The rate of enhancement was 3.7%. Though limited by the small sample size and retrospective nature of the study, this result fits within the range reported in the literature, which suggests that ophthalmologists may anticipate an enhancement rate of one to seven percent following SMILE. In these cases, PRK is a safe and effective procedure for enhancement of SMILE.
Abbreviations
PRK, photorefractive keratectomy; SMILE, small-incision lenticule extraction; LASIK, laser-assisted in-situ keratomileusis; ENH, enhancement; FDA, food and drug administration; UDVA, uncorrected distance visual acuity; CDVA, corrected distance visual acuity; SEQ, spherical equivalent; D, diopter; logMAR, logarithm of the minimum angle of resolution; K, keratometry.
Ethics Approval and Informed Consent
This study was approved by the Hoopes Vision Ethics Board and adhered to the tenets outlined in the Declaration of Helsinki. The study was HIPAA-compliant, with a routine surgical informed consent obtained from all patients involved. It was an IRB-approved study by the Biomedical Research Alliance of New York (BRANY, New Hyde Park, NY, IRB number: #A20‐12‐547‐823) in accordance with research standards and state law. Patient data were de-identified prior to analysis.
Consent for Publication
We have not included any images, videos, or recordings requiring consent.
Acknowledgments
We thank the patients who were part of this retrospective study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for the publication of this article.
Disclosure
All authors report no conflicts of interest in this work.
References
1. Dishler JG, Slade S, Seifert S, Schallhorn SC. Small-Incision Lenticule Extraction (SMILE) for the correction of myopia with astigmatism: outcomes of the United States food and drug administration premarket approval clinical trial. Ophthalmology. 2020;127(8):1020–1034. doi:10.1016/J.OPHTHA.2020.01.010
2. Chow SSW, Chow LLW, Lee CZ, Chan TCY. Astigmatism correction using SMILE. Asia-Pacific J Ophthalmol. 2019;8(5):391. doi:10.1097/01.APO.0000580140.74826.F5
3. Carl Zeiss Meditec AG. FDA approval for SMILE astigmatism. Available from: https://www.zeiss.com/meditec-ag/media-news/press-releases-hcp/2018/fda-approval-for-smile-astigmatism.html.
4. Seeing your own technology in a new light. Available from: https://www.zeiss.com/corporate/int/newsroom/zeiss-stories/smile.html.
5. Liu YC, Rosman M, Mehta JS. Enhancement after small-incision lenticule extraction: incidence, risk factors, and outcomes. Ophthalmology. 2017;124(6):813–821. doi:10.1016/j.ophtha.2017.01.053
6. Siedlecki J, Luft N, Priglinger SG, Dirisamer M. Enhancement options after myopic small-incision lenticule extraction (SMILE): a review. Asia Pac J Ophthalmol. 2019;8(5):406–411. doi:10.1097/APO.0000000000000259
7. Moshirfar M, Shah TJ, Masud M, Linn SH, Ronquillo Y, Hoopes PC. Surgical options for retreatment after small-incision lenticule extraction: advantages and disadvantages. J Cataract Refract Surg. 2018;44(11):1384–1389. doi:10.1016/J.JCRS.2018.07.047
8. Sedky AN, Wahba SS, Roshdy MM, Ayaad NR. Cap-preserving SMILE enhancement surgery. BMC Ophthalmol. 2018;18(1). doi:10.1186/S12886-018-0712-7
9. Reinstein DZ, Archer TJ, Gobbe M. Small incision lenticule extraction (SMILE) history, fundamentals of a new refractive surgery technique and clinical outcomes. Eye Vis. 2014;1(1). doi:10.1186/S40662-014-0003-1
10. Ivarsen A, Hjortdal J. Topography-guided photorefractive keratectomy for irregular astigmatism after small incision lenticule extraction. J Refract Surg. 2014;30(6):429–432. doi:10.3928/1081597X-20140508-02
11. Siedlecki J, Luft N, Kook D, et al. Enhancement after myopic small incision lenticule extraction (SMILE) using surface ablation. J Refract Surg. 2017;33(8):513–518. doi:10.3928/1081597X-20170602-01
12. Siedlecki J, Luft N, Mayer WJ, et al. CIRCLE enhancement after myopic smile. J Refract Surg. 2018;34(5):304–309. doi:10.3928/1081597X-20180308-02
13. Siedlecki J, Siedlecki M, Luft N, et al. Surface ablation versus circle for myopic enhancement after SMILE: a matched comparative study. J Refract Surg. 2019;35(5):294–300. doi:10.3928/1081597X-20190416-02
14. Gab-Alla AA. SmartSurfACE transepithelial photorefractive keratectomy with mitomycin C enhancement after small incision lenticule extraction. Eye Vision. 2021;8(1). doi:10.1186/s40662-021-00254-2
15. Chansue E, Tanehsakdi M, Swasdibutra S, McAlinden C. Safety and efficacy of VisuMax® circle patterns for flap creation and enhancement following small incision lenticule extraction. Eye Vis. 2015;2(1):21. doi:10.1186/s40662-015-0031-5
16. Reinstein DZ, Carp GI, Archer TJ, Vida RS. Inferior pseudo-hinge fulcrum technique and intraoperative complications of laser in situ keratomileusis retreatment after small-incision lenticule extraction. J Cataract Refract Surg. 2018;44(11):1355–1362. doi:10.1016/J.JCRS.2018.07.051
17. Reinstein DZ, Carp GI, Archer TJ, Vida RS. Outcomes of re-treatment by LASIK after SMILE. J Refract Surg. 2018;34(9):578–588. doi:10.3928/1081597X-20180717-02
18. Donate D, Thaëron R. Preliminary evidence of successful enhancement after a primary SMILE procedure with the sub-cap-lenticule-extraction technique. J Refract Surg. 2015;31(10):708–710. doi:10.3928/1081597X-20150928-04
19. Kling S, Spiru B, Hafezi F, Sekundo W. Biomechanical weakening of different re-treatment options after small incision lenticule extraction (SMILE). J Refract Surg. 2017;33(3):193–198. doi:10.3928/1081597X-20161221-01
20. Riau AK, Liu YC, Lim CHL, et al. Retreatment strategies following Small Incision Lenticule Extraction (SMILE): in vivo tissue responses. PLoS One. 2017;12(7):e0180941. doi:10.1371/JOURNAL.PONE.0180941
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evaluation of the EVO/EVO+ Sphere and Toric Visian ICL: Six Month Results from the United States Food and Drug Administration Clinical Trial
Packer M
Clinical Ophthalmology 2022, 16:1541-1553
Published Date: 21 May 2022
Visual and Topographic Outcomes of Corneal Collagen Cross Linking for Post LASIK Ectasia
Nasef MH, El Emam SY, Haleem TI, Shalaby WS, Allam WA
Clinical Ophthalmology 2022, 16:2025-2032
Published Date: 20 June 2022
Prospective, Randomized, Fellow Eye-Controlled Study of Postoperative Pain and Inflammation Control with an Intracanalicular Dexamethasone 0.4 mg Ophthalmic Insert Following Small Incision Lenticule Extraction
Jee KJ, Ling J, Bafna S, Chester T, Augustine J, Wiley WF
Clinical Ophthalmology 2022, 16:3895-3904
Published Date: 22 November 2022
A Comprehensive Retrospective Analysis of EVO/EVO+ Implantable Collamer Lens: Evaluating Refractive Outcomes in the Largest Single Center Study of ICL Patients in the United States
Albo C, Nasser T, Szynkarski DT, Nguyen N, Mueller B, Libfraind L, Parkhurst G
Clinical Ophthalmology 2024, 18:69-78
Published Date: 9 January 2024
Three-Month Outcomes of SMILE Pro with the VISUMAX 800 for Myopic Astigmatism in a Large Population
Cung HS, Tran LHT, Tran TN
Clinical Ophthalmology 2025, 19:417-425
Published Date: 7 February 2025