Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Accurate Identification and Intervention System Construction of Treatable Traits in Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease: Protocol for a Randomized Controlled Study
Authors Ma Y, Meng W, Zong D ![]() , Zeng H, Chen Y
, Zeng H, Chen Y ![]()
Received 6 May 2026
Accepted for publication 10 July 2026
Published 17 July 2026 Volume 2026:21 622504
DOI https://doi.org/10.2147/COPD.S622504
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Zijing Zhou
Yiming Ma,1– 4 Weiwei Meng,1– 4 Dandan Zong,1– 4 Huihui Zeng,1– 4 Yan Chen1– 4
1Department of Pulmonary and Critical Care Medicine, The Second Xiangya Hospital of Central South University, Changsha, Hunan, People’s Republic of China; 2Research Unit of Respiratory Disease, Central South University, Changsha, Hunan, People’s Republic of China; 3Clinical Medical Research Center for Pulmonary and Critical Care Medicine in Hunan Province, The Second Xiangya Hospital of Central South University, Changsha, Hunan, People’s Republic of China; 4Diagnosis and Treatment Center of Respiratory Disease in Hunan Province, The Second Xiangya Hospital of Central South University, Changsha, Hunan, People’s Republic of China
Correspondence: Yan Chen, Email [email protected]
Background: Considerable heterogeneity exists in patients experiencing acute exacerbation of chronic obstructive pulmonary disease (AECOPD) concerning etiology, clinical manifestations, phenotypic features, comorbidities, and treatment responsiveness. The concept of "treatable traits” is adapted to evaluate the clinical features of patients with chronic airway diseases from multiple dimensions and ultimately guiding precision treatment strategies. This prospective randomized controlled study mainly aims to evaluate the impact of accurate identification and intervention strategies guided by "treatable traits” on the prognosis of AECOPD patients.
Methods: This prospective randomized controlled study will be performed in 6 centers in China, with a planned enrollment of 314 AECOPD participants. 314 participants will be randomly assigned to either the precision intervention group or the control group with a ratio of 1:1. During admission, participants in the precision intervention group will receive accurate identification and intervention based on "treatable traits”, while patients in the control group receive conventional medical treatment as usual. Patients will be followed up at 6 and 12 months after discharge. Primary outcomes of the study include the incidence of total acute exacerbations and hospitalizations due to acute exacerbations during follow-up. Secondary outcomes involve changes in CAT scores and mMRC classification, and the occurrence of death during follow-up.
Discussion: By employing standardized, multi-dimensional baseline and follow-up assessments, the study seeks to develop a comprehensive framework of treatable traits encompassing pulmonary, extrapulmonary, and socio-behavioral domains for AECOPD. It will further evaluate the prognostic impact of precision interventions tailored to these treatable traits in AECOPD patients for the first time.
Keywords: chronic obstructive pulmonary disease, acute exacerbation, treatable traits, identification, intervention
Introduction
Background and Rationale
Chronic obstructive pulmonary disease (COPD) is a prevalent chronic airway condition that is both preventable and treatable. Despite this, COPD is associated with high rates of mortality and disability, making it a significant global public health problem.1,2 Spirometry-confirmed COPD exhibits a notably high prevalence among the Chinese adult population; The overall prevalence rate of spirometry-diagnosed COPD stands at 8.6%, equating to approximately 99.9 million individuals living with COPD in China.3 Notably, the incidence of young COPD patients continues to escalate annually, imposing a substantial socioeconomic burden.4
Despite receiving treatment, COPD patients still suffer a considerable burden mainly owning to exacerbations and comorbidities, which leads to a substantial use of healthcare resources.5 Acute exacerbation of chronic obstructive pulmonary disease (AECOPD) denotes a phase of the disease marked by a rapid deterioration in respiratory symptoms, necessitating supplementary treatment.6 This deterioration associates with expedited decline of lung function, impairment of quality of life, and elevated risk of mortality.7,8 In addition, patients experiencing AECOPD exhibit considerable heterogeneity in terms of etiology, clinical presentations, phenotypic traits, comorbid conditions, and responsiveness to treatment.9,10 Therefore, systematically discerning the clinical attributes of AECOPD patients and formulating personalized intervention strategies hold substantial practical value in enhancing patient prognosis.
“Treatable traits” is a concept in the field of precision medicine. This innovative concept serves as a multi-dimensional framework for evaluating the clinical traits of patients with chronic airway diseases, pinpointing core characteristics that correlate with clinical outcomes, and ultimately promoting precision treatment strategies.11 Different from traditional “one size fits all” stepwise treatment model, treatable traits can help distinguish the individual phenotypes and underlying causal molecular mechanisms (endotypes), and further identify key therapeutic targets.12,13 The treatable traits in chronic airway disease can be specifically categorized into pulmonary, extra-pulmonary, and social behavior traits.14 Data from the NOVELTY study cohort have demonstrated that patients with COPD have an average of 5.4 treatable traits, which is more complex compared with asthma.15 Of note, core TTs in COPD patients can be predictors of future decline in lung function and quality of life.16 A randomized controlled study revealed that patients with severe asthma typically exhibit an average of 10.44 treatable traits, encompassing 3.01 pulmonary traits, 4.85 extra-pulmonary traits, and 2.58 social behavior traits. Follow-up data collected after 16 weeks demonstrated that, in comparison to the conventional intervention group, individualized precision treatment targeting treatable traits significantly enhanced health-related quality of life and asthma control among patients with severe asthma; These findings offer a novel approach for managing severe asthma.17 Previous studies mainly focused on the TTs in patients during the stable phase of chronic airway diseases. Translating the treatable traits framework to exacerbation episode of COPD is also justified. Biologically, an exacerbation often represents the acute decompensation of underlying, modifiable pathological traits. For example, an exacerbation may be triggered by the trait of “eosinophilic airway inflammation” or “virus infection”.18,19 Identifying and treating these traits during the exacerbation targets the root cause, not just the symptom. Clinically, the exacerbation period is a unique opportunity for intervention, as it is a time of heightened patient awareness and healthcare contact, allowing for comprehensive assessment and the immediate initiation of targeted therapies.20 This treatable traits framework aims not only to resolve the current episode more effectively but also to implement preventive strategies that reduce the risk of future events. Thus, the “treatable traits” framework that traditionally applied in the management of stable chronic airway disease is also applicable to AECOPD.
However, to date, no prospective randomized controlled studies have been undertaken to explore the impact of treatable traits on the prognosis of patients with AECOPD. This study hypothesizes that, compared with the traditional generalized intervention mode in AECOPD, the precision intervention strategy based on multi-dimensional treatable traits has superior clinical value in improving the long-term outcomes in AECOPD patients and reducing the risk of acute exacerbation recurrence.
Objectives
This study innovatively integrates the new concept of treatable traits in precision medicine into the whole-process management of patients with AECOPD. For the first time, a prospective randomized controlled study will be conducted to explore the impact of precision identification and intervention based on treatable traits on AECOPD patients. Ultimately, the study may help to develop an all-encompassing map of treatable traits, covering pulmonary, extrapulmonary, and socio-behavioral dimensions specifically for AECOPD. Additionally, the research is expected to assess how precision intervention strategies, customized according to these treatable traits, influence the prognosis of AECOPD patients, including future acute exacerbation, mortality and clinical symptoms.
Patients and Methods
Study Setting
This prospective randomized controlled study will be performed in 6 centers in Hunan Province (including The Second Xiangya Hospital of Central South University, Shaodong People’s Hospital, Zhuzhou Central Hospital, Liuyang People’s Hospital, Qiyang People’s Hospital and Hengshan People’s Hospital), with a planned enrollment of 314 AECOPD participants. 314 participants will be randomly assigned to either the precision intervention group or the control group with a ratio of 1:1. The flowchart of the study is demonstrated in Figure 1. The study protocol follows the standards of SPIRIT.21 Schedule of enrollment, interventions, and assessments of the study are summarized in Table 1.
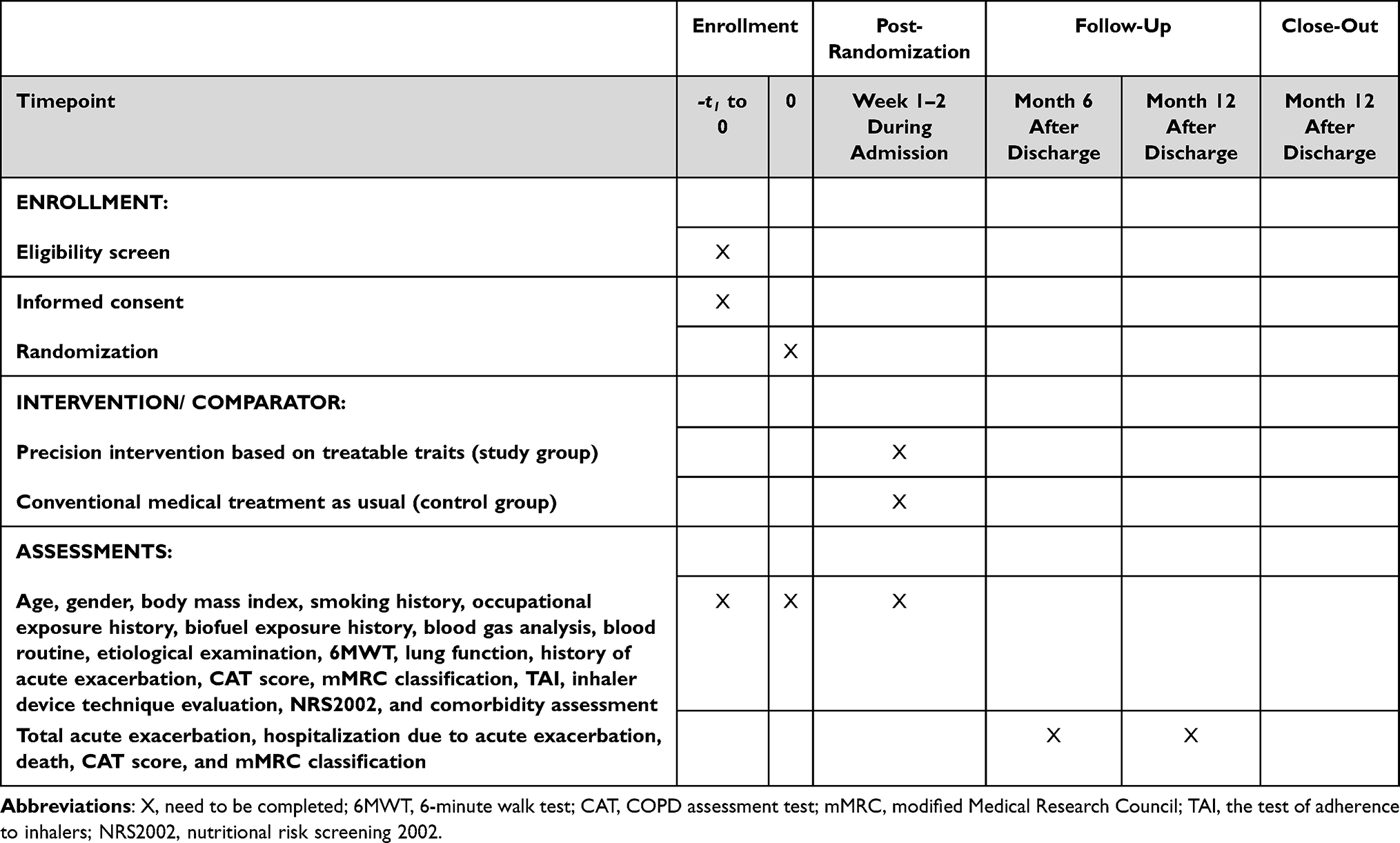 |
Table 1 Schedule of Enrollment, Interventions, and Assessments |
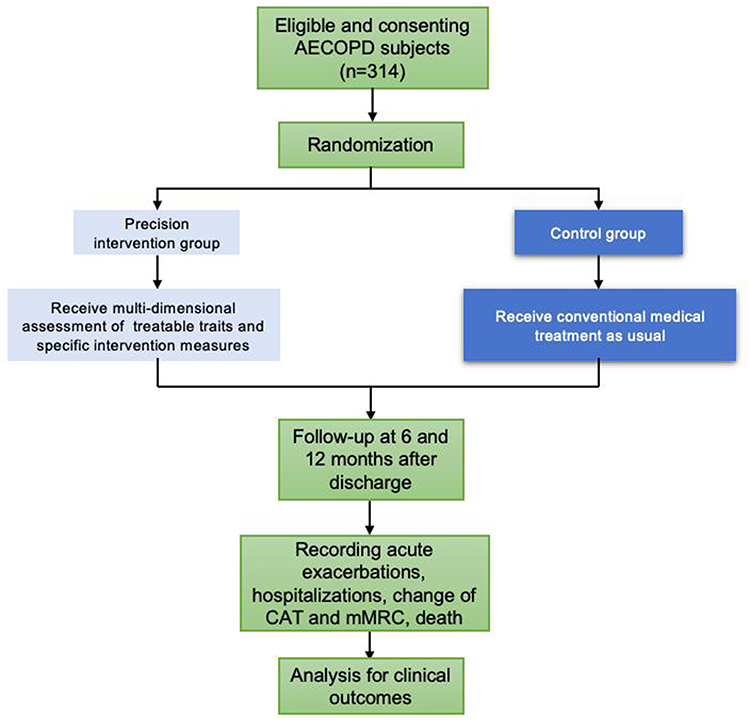 |
Figure 1 Flowchart of the study. Abbreviations: AECOPD, acute exacerbation of chronic obstructive pulmonary disease; CAT, COPD assessment test; mMRC, modified Medical Research Council. |
Participants
In this study, we will recruit hospitalized AECOPD patients. AECOPD is defined as an acute worsening of respiratory symptoms in patients, necessitating additional treatment. According to severity, AECOPD can be classified: (1) Mild: only requiring short-acting bronchodilators; (2) Moderate: using short-acting bronchodilators and antimicrobial agents, with or without the addition of oral glucocorticoids; (3) Severe: requiring hospitalization or treatment in the emergency department and intensive care unit (ICU).22
Inclusion Criteria
- Age ≥40 years old;
- Meet the diagnostic criteria for AECOPD in the 2021 Chinese COPD guidelines;
- Can independently complete COPD assessment test (CAT), modified Medical Research Council (mMRC) and other questionnaires.
Exclusion Criteria
(1) Patients with lung cancer and other malignant tumors;
(2) Patients with severe intellectual or cognitive impairments;
(3) Participate in other clinical trials involving interventions.
Randomization and Allocation Concealment
Patients who meet the eligibility criteria will be randomly assigned to either the precision intervention group or the control group. The randomization process for this study was carried out by an impartial researcher, who employed a computer - generated random number sequence to ensure a 1:1 allocation ratio between the two groups. Treatment allocation is concealed prior to participant recruitment.
Blinding
Given the inherent nature of this study, neither the intervention practitioner nor the participant can remain blinded to the treatment plan. Therefore, blinding can only be applied during the data collection and evaluation processes. The multidimensional assessment for treatable traits will be performed by independent investigator, and physicians will be blinded to the results of the multidimensional assessment for treatable traits in the control group. While physicians will be informed about the results of the multidimensional assessment for treatable traits in the intervention group.
Grouping and Interventions
Grouping
The subjects will be randomly assigned to the precision intervention group based on treatable traits and the control group using a random allocation method as previously described.
Interventions
Study Group
To identify their treatable traits individually, comprehensive and multi-dimensional assessment of the intervention group of AECOPD patients will be performed based on the evaluation criteria for treatable traits related to pulmonary, extrapulmonary, and social behavior listed in Table 2. A multidisciplinary expert discussion involving clinicians, pulmonary rehabilitation therapists, clinical nutritionists, psychological counselors, nurses and relatives of patients is conducted to summarize the treatable traits identified in patients with AECOPD in the intervention group and develop feasible individualized intervention strategies, the schematic diagram is shown in Figure 2. The multidisciplinary expert discussion will be performed on days 3–7 after admission, and necessary individual specialist consultations will be conducted before discharge when new data emerge (eg a positive microbial test). The precise intervention strategies proposed by multidisciplinary experts will be performed on participants. Specific intervention measures are shown in Table 2.
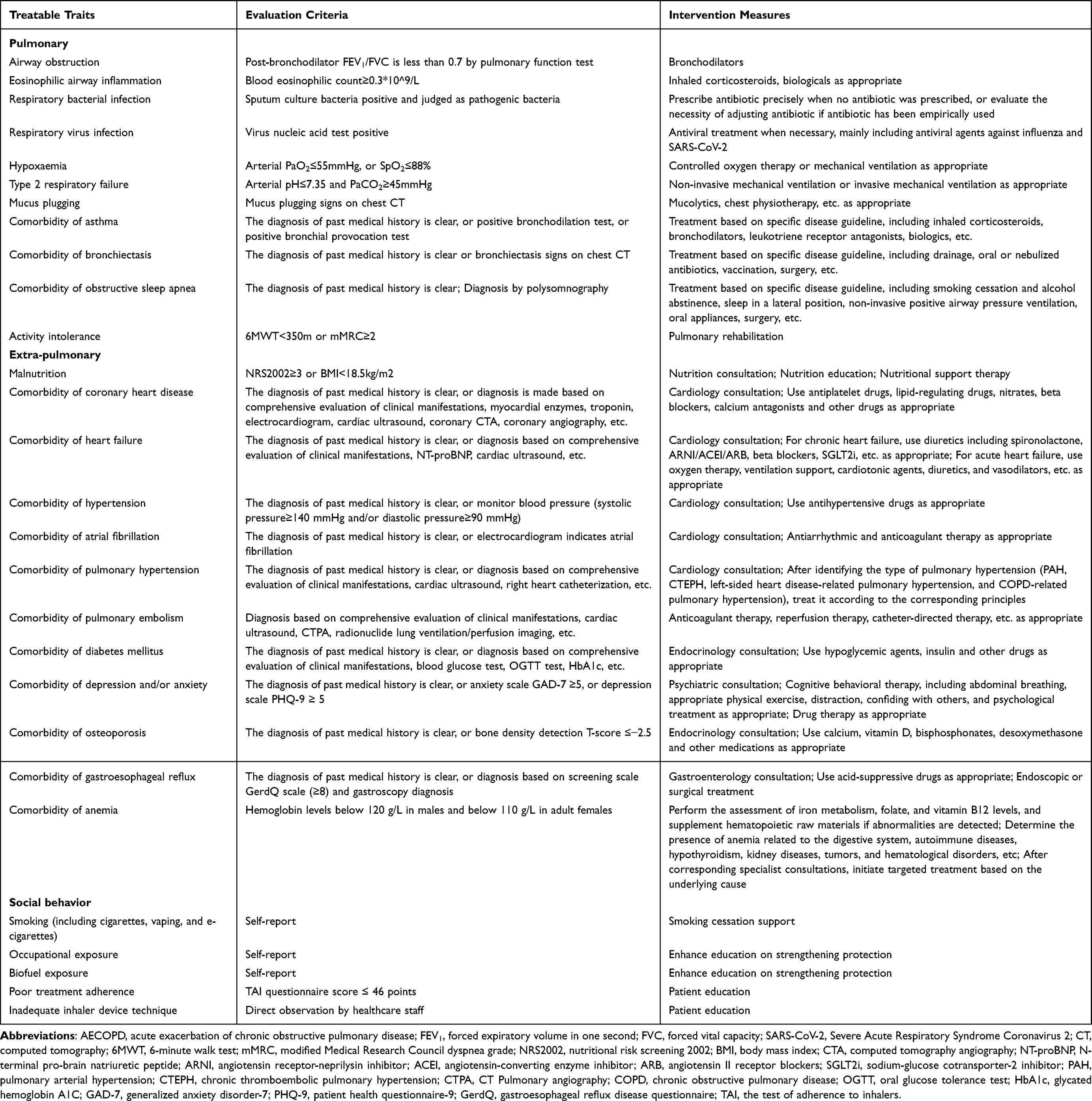 |
Table 2 Treatable Traits, Evaluation Criteria, and Intervention Measures for Patients with AECOPD |
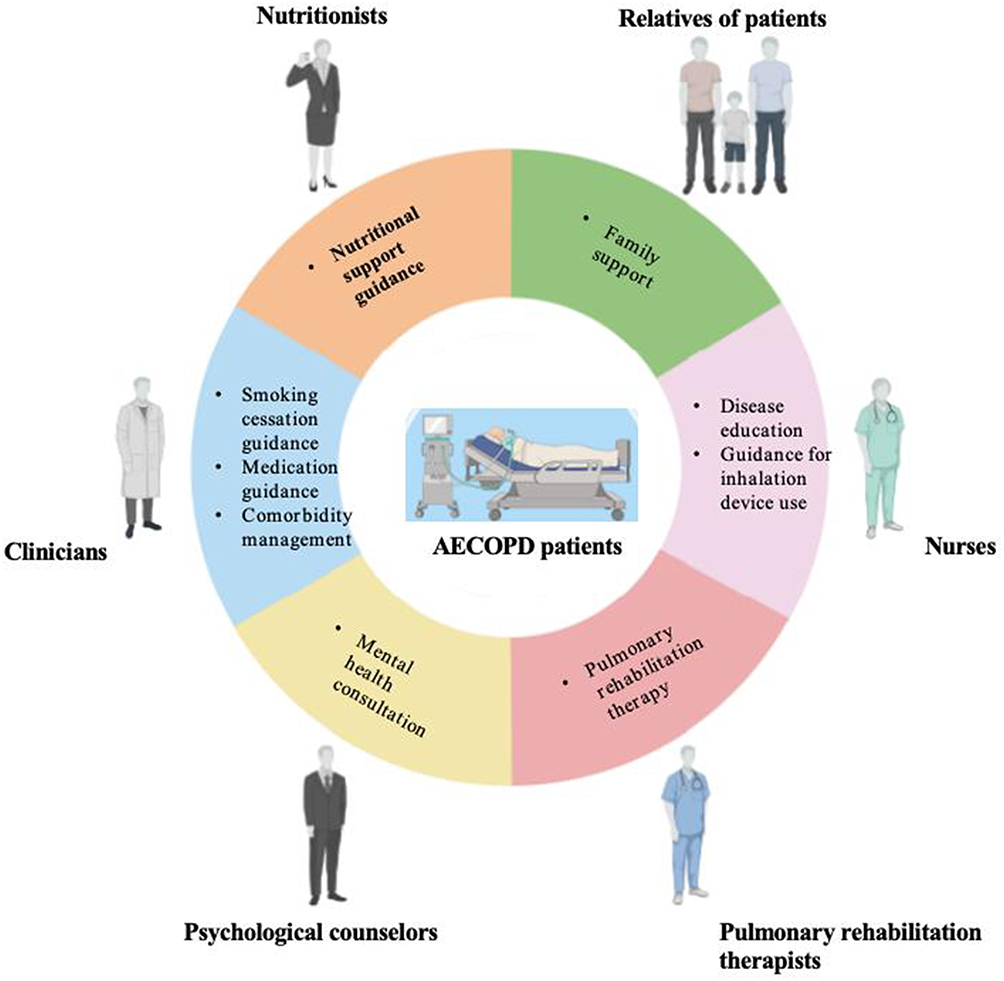 |
Figure 2 The schematic diagram of feasible “treatable traits”-guiding individualized intervention strategies by multidisciplinary experts. This figure was created with BioRender.com. Abbreviation: AECOPD, acute exacerbation of chronic obstructive pulmonary disease. |
Control Group
Patients in the control group do not receive the above interventions for study group and receive conventional medical treatment as usual. Conventional medical treatment in the control group will follow the guideline,22 mainly including pharmacological treatment (bronchodilators, glucocorticoids, antibiotics, etc.) and respiratory support.
Outcomes
Patients will be followed up at 6 and 12 months after discharge. Clinical outcomes include total acute exacerbation, hospitalization due to acute exacerbation, death, CAT score, and mMRC classification changes. During the follow-up period, the time interval between two acute exacerbations is at least 14 days. All relevant data will be obtained by research assistants through direct interviews with patients, patient self-management diaries, review of medical records, or telephone contact with family members.
Primary Outcome Measures
Primary outcomes include the incidence of total acute exacerbations and hospitalizations due to acute exacerbations during the follow-up period.
Secondary Outcomes
Secondary outcomes of the study involve changes in CAT scores and mMRC classification during follow-up, and the occurrence of death during follow-up.
Data Collection and Management
The following information was collected at admission: age, gender, body mass index, smoking history, occupational exposure history, biofuel exposure history, blood gas analysis, blood routine, etiological examination, 6-minute walk test (6MWT), lung function, history of acute exacerbation, CAT score, mMRC classification, the test of adherence to inhalers (TAI), inhaler device technique evaluation, nutritional risk screening 2002 (NRS2002), and comorbidity assessment. All medical records and assessment data gathered from the participants will be securely stored within an electronic data capture system. Informed consent for participation in the study will be obtained from all participants in written forms. Access to the study data will be granted exclusively to authorized research assistants, and research assistants will fully inform the patients of the intervention measures to improve adherence to intervention protocols. According to the participant’s request, the participant has the right to withdraw from the trial during the trial phase.
Data Monitoring
To safeguard data integrity, independent investigators will be responsible for data error detection and correction. Statistical analyses will be carried out under the guidance of professional statisticians, adhering to stringent methodological criteria. Additionally, any substantial change to the research protocol will undergo approval from the research ethics committee. These changes will then be promptly communicated to the research team, updated in relevant registries, and disclosed to participants as and when necessary. In this study, we will strictly follow the intention-to-treat principle for primary efficacy analysis, and all randomized participants will be accounted for in their originally assigned groups. We will use multiple imputation to handle missing data, and conduct sensitivity analysis to verify the stability of results. In the submitted manuscript reporting final study outcomes, a complete participant flow chart will be added to show the number of participants excluded, lost to follow-up and finally included in the analysis.
Harms
During the whole trial phase, investigators plan to collect, assess, report, and manage solicited and spontaneously reported adverse events and other unintended effects of trial interventions.
Auditing
This study will receive audits from the research ethics committee annually, and the research ethics committee has the access to these interim results and make the final decision to terminate the trial.
Sample Size Estimation
Sample size calculation was performed by “Tests for the Ratio of Two Negative Binomial Rates” in the software of PASS 2025. We calculated the sample size based on the estimated results of hospitalization due to acute exacerbation during the one-year follow-up period, which is also the primary endpoint of this study. Based on the results of the preliminary study, we anticipated a mean hospitalization rate due to acute exacerbation during the one-year follow-up period in control group of 1.25 (λ1); We anticipated a mean hospitalization rate due to acute exacerbation during the one-year follow-up period in intervention group of 0.75 (λ2). Thus, the event rate ratio (RR) is 0.6. Other calculation parameters used were: α=0.05, power=0.8, the negative binomial dispersion parameter=1. The sample size calculated using these parameters was 125 cases in each group, and 250 cases in total. Considering the expected loss of 20% of the sample, we used 314 cases as the final estimated sample size.
Statistical Analysis
The statistical analysis will be conducted using SPSS version 22.0. Baseline characteristics including age, gender, body mass index, smoking history, occupational exposure history, biofuel exposure history, blood gas analysis, blood routine, etiological examination, 6MWT, lung function, history of acute exacerbation, CAT score, mMRC classification, TAI, inhaler device technique evaluation, NRS2002, and comorbidity assessment will be compared. Measurement data that conform to normal distribution will be expressed as mean ± standard deviation (Mean±SD), and those that do not conform to normal distribution will be expressed as median [interquartile range] (Median [IQR]). The categorical data will be described by the composition ratio of the number of cases, and count data such as exacerbations will be assessed by negative binomial model. The comparison between groups for continuous variables will be performed using t-tests and Mann Whitney U nonparametric tests, while the comparison between groups for categorical variables will be performed using chi-square tests. For the count outcome (number of acute exacerbations), the final negative binomial model will adjust for baseline covariates including age, gender, smoking history, baseline lung function, etc. For time-to-event outcomes including acute exacerbation, hospitalization and all-cause death during follow-up, we will first plot the Kaplan–Meier survival curves to visualize the dynamic trajectory of event occurrence in each group, and perform the Log rank test for preliminary unadjusted between-group comparison. Subsequently, we will construct a Cox regression model to adjust for confounding variables and center effects, to estimate the adjusted hazard ratio (HR) and corresponding 95% confidence interval (CI) for the intervention. p<0.05 will be considered statistically significant.
Discussion
The disease burden of COPD persists at a high level due to the intricate complexity and marked heterogeneity.23 Thus, it is necessary to move forward in identifying and targeting treatable traits, so as to provide personalized treatment for each patient and transcend the narrow confines of the disease labels they have been given.24 Adopting approaches centered on treatable traits shows great potential for enhancing clinical outcomes and elevating the quality of life for individuals grappling with COPD.25 Importantly, COPD patients carrying a heavier exacerbation burden exhibited poorer lung function at the time of diagnosis and experienced a more rapid subsequent decline in lung function, and this underscores the urgent necessity for developing improved treatment strategies.26
Our previous study demonstrated that treatable traits can be systematically identified in Chinese patients hospitalized due to AECOPD, with certain traits being linked to future exacerbation-related readmissions including O2 desaturation, eosinophilic airway inflammation, pathogen colonization and gastroesophageal reflux etc.27 Of note, there are currently no precision intervention studies based on treatable traits in patients with AECOPD, and this research plans to take the lead in conducting a multicenter, prospective, randomized controlled trial. Through standardized and multi-dimensional assessment and follow-up assessments, the study aims to construct a comprehensive map of treatable traits encompassing pulmonary, extrapulmonary, and socio-behavioral aspects for AECOPD and evaluate the impact of precision intervention strategies tailored to treatable traits on the prognosis of patients with AECOPD. The relevant research findings are expected to fill the research gaps and may provide reference for future COPD guidelines. Besides, our proposed precision intervention based on multi-dimensional treatable traits is not restricted to the Chinese healthcare system. The core assessment logic and intervention principles are compatible with international COPD management guidelines, and the study population represents typical AECOPD cases that are widely encountered globally. Also, the application of this multi-domain “treatable traits” approach beyond clinical trials requires consideration of practical barriers. These barriers encompass resource constraints, staffing limitations for multidisciplinary collaboration, and suboptimal sustainability of patient engagement. Addressing these feasibility issues is a crucial next step for wider adoption.
This study has limitations that should be acknowledged. First, we tailored the intervention modules to match each patient’s unique treatable traits. While this improves the clinical relevance of the intervention, it also introduces some variability across different delivery plans. All interventions follow unified standard protocols, and we conduct regular checks to ensure implementation quality. Future studies can further analyze how each module contributes to outcomes, to improve the consistency of the strategy across different patient groups. Second, as a multi-center study conducted across 6 centers, potential residual center effects may exist. Differences in local routine AECOPD management workflows, regional medication availability, and unmeasured institutional care cultures may introduce unobserved clustering effects on study outcomes. To mitigate this limitation, we implemented standardized, site-wide training for all interventionists prior to study initiation, ensuring uniform delivery of the intervention protocol across all participating centers. Third, full blinding of participants is not feasible due to the inherent nature of the personalized intervention design. To minimize the potential performance bias, blinding is strictly enforced in data collection and evaluation stages. Specifically, the multidimensional assessment of treatable traits will be completed by an independent investigator who is not involved in subsequent intervention allocation and patient management. Fourth, the multidisciplinary discussion was scheduled between hospital days 3 and 7. This window was chosen to ensure that discussions were informed by a complete set of assessment data, thereby enhancing the precision and relevance of the personalized plans. We acknowledge that this may introduce some variability in the exact timing of the multidisciplinary discussion.
In conclusion, this multicenter, randomized controlled trial will evaluate the efficacy and feasibility of a personalized, “treatable traits”-based management strategy for patients hospitalized with AECOPD. The findings may provide a practical framework for implementing personalized care in acute settings and generate novel insights into the phenotypic heterogeneity of AECOPD, ultimately aiming to improve prognosis in this high-risk population.
Data Sharing Statement
No datasets were generated or analyzed during the current study.
Ethics Approval and Consent to Participate
This study underwent a review by Ethics Committee of Second Xiangya Hospital of Central South University. Following the evaluation, it was determined that the research protocol adheres to the standards of scientific inquiry, takes into full account the rights and interests of participants, aligns with the principles outlined in the Declaration of Helsinki and other ethical guidelines, and will ensure the procurement of informed consent from all study participants. Consequently, the research protocol has been formally approved for implementation (ethical approval number: LYEC2026-0013). The protocol version is 1.2 (Date: Jan 28th, 2026). This study was registered in https://www.chictr.org.cn/ with the identifier ChiCTR2500097186. The findings of this study are slated for publication in a peer-reviewed journal.
Acknowledgment
This study has been registered at the Chinese Clinical Trials.gov on February 13, 2025. Trial Registration Number: ChiCTR2500097186.
Funding
This work is supported by Noncommunicable Chronic Diseases-National Science and Technology Major Project (2023ZD0516400), the Science and Technology Innovation Program of Hunan Province (2025RC3062), National Clinical Key Specialty Major Scientific Research Project (Z2023164).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Boers E, Allen A, Barrett M. et al. Forecasting the Global Economic and Health Burden of COPD From 2025 Through 2050. Chest. 2025;168(4):880–12. doi:10.1016/j.chest.2025.03.029
2. Naeem S, Wang F, Mubarak R, et al. Mapping the Global distribution, risk factors, and temporal trends of COPD incidence and mortality (1990–2021): ecological analysis. BMC Med. 2025;23(1):210. doi:10.1186/s12916-025-04014-0
3. Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): a national cross-sectional study. Lancet. 2018;391(10131):1706–1717. doi:10.1016/S0140-6736(18)30841-9
4. Li Y, Yan F, Jiang L, Zhen W, Li X, Wang H. Epidemiological trends and risk factors of chronic obstructive pulmonary disease in young individuals based on the 2021 global burden of disease data (1990–2021). BMC Pulm Med. 2025;25(1):174. doi:10.1186/s12890-025-03630-z
5. Soler-Cataluña JJ, Izquierdo JL, Juárez Campo M, Sicras-Mainar A, Nuevo J. Impact of COPD Exacerbations and Burden of Disease in Spain: AVOIDEX Study. Int J Chron Obstruct Pulmon Dis. 2023;18:1103–1114. doi:10.2147/COPD.S406007
6. Zhang J, Chen F, Wang Y, Chen Y. Early detection and prediction of acute exacerbation of chronic obstructive pulmonary disease. Chin Med J Pulm Crit Care Med. 2023;1(2):102–107. doi:10.1016/j.pccm.2023.04.004
7. Halpin DM, Miravitlles M, Metzdorf N, Celli B. Impact and prevention of severe exacerbations of COPD: a review of the evidence. Int J Chron Obstruct Pulmon Dis. 2017;12:2891–2908. doi:10.2147/COPD.S139470
8. Ritchie AI, Wedzicha JA. Definition, Causes, Pathogenesis, and Consequences of Chronic Obstructive Pulmonary Disease Exacerbations. Clin Chest Med. 2020;41(3):421–438. doi:10.1016/j.ccm.2020.06.007
9. Pratt AJ, Purssell A, Zhang T, et al. Complexity in clinical diagnoses of acute exacerbation of chronic obstructive pulmonary disease. BMC Pulm Med. 2023;23(1):298. doi:10.1186/s12890-023-02587-1
10. MacDonald MI, Osadnik CR, Bulfin L, et al. MULTI-PHACET: multidimensional clinical phenotyping of hospitalised acute COPD exacerbations. ERJ Open Res. 2021;7(3):00198–2021. doi:10.1183/23120541.00198-2021
11. Agusti A, Bel E, Thomas M, et al. Treatable traits: toward precision medicine of chronic airway diseases. Eur Respir J. 2016;47(2):410–419. doi:10.1183/13993003.01359-2015
12. Morishima Y, Hizawa N. Clinical Benefits of Targeting Treatable Traits in Asthma and Chronic Obstructive Pulmonary Disease. Intern Med. 2025;64(1):17–23. doi:10.2169/internalmedicine.3353-23
13. Agusti A, Gibson PG, McDonald VM. Treatable Traits in Airway Disease: from Theory to Practice. J Allergy Clin Immunol Pract. 2023;11(3):713–723. doi:10.1016/j.jaip.2023.01.011
14. McDonald VM, Fingleton J, Agusti A, et al. Treatable traits: a new paradigm for 21st century management of chronic airway diseases: treatable Traits Down Under International Workshop report. Eur Respir J. 2019;53(5):1802058. doi:10.1183/13993003.02058-2018
15. Agustí A, Rapsomaniki E, Beasley R, et al. NOVELTY Study Investigators: treatable traits in the NOVELTY study. Respirology. 2022;27(11):929–940. doi:10.1111/resp.14325
16. Sarwar MR, McDonald VM, Abramson MJ, Paul E, George J. Treatable traits in an English cohort: prevalence and predictors of future decline in lung function and quality of life in COPD. ERJ Open Res. 2021;7(2):00934–2020. doi:10.1183/23120541.00934-2020
17. McDonald VM, Clark VL, Cordova-Rivera L, Wark PAB, Baines KJ, Gibson PG. Targeting treatable traits in severe asthma: a randomised controlled trial. Eur Respir J. 2020;55(3):1901509. doi:10.1183/13993003.01509-2019
18. Tu Y, Chen Y, Li X, et al. Advances in acute COPD exacerbation: clarifying specific immune mechanisms of infectious and noninfectious factors. Ther Adv Respir Dis. 2025;19:17534666241308408. doi:10.1177/17534666241308408
19. Lee YL, Heriyanto DS, Yuliani FS, et al. Eosinophilic inflammation: a key player in COPD pathogenesis and progression. Ann Med. 2024;56(1):2408466. doi:10.1080/07853890.2024.2408466
20. Ramakrishnan S, Janssens W, Burgel PR, et al. Standardisation of Clinical Assessment, Management and Follow-Up of Acute Hospitalised Exacerbation of COPD: a Europe-Wide Consensus. Int J Chron Obstruct Pulmon Dis. 2021;16:321–332. doi:10.2147/COPD.S287705
21. Chan A-W, Tetzlaff JM, Gøtzsche PC, et al. SPIRIT 2013 Explanation and Elaboration: guidance for protocols of clinical trials. BMJ. 2013;346:e7586. doi:10.1136/bmj.e7586
22. Chronic Obstructive Pulmonary Disease Group of Chinese Thoracic Society, Chronic Obstructive Pulmonary Disease Committee of Chinese Association of Chest Physician. Guidelines for the diagnosis and management of chronic obstructive pulmonary disease (revised version 2021). Zhonghua Jie He He Hu Xi Za Zhi. 2021;44:170–205.
23. Agusti A, Gibson PG, Heaney LG, Thomas M. Thomas M: change is in the air: key questions on the ‘Treatable Traits’ model for chronic airway diseases in primary care. NPJ Prim Care Respir Med. 2024;34(1):21. doi:10.1038/s41533-024-00381-y
24. Duszyk K, McLoughlin RF, Gibson PG, McDonald VM. The use of treatable traits to address COPD complexity and heterogeneity and to inform the care. Breathe. 2021;17(4):210118. doi:10.1183/20734735.0118-2021
25. Kumar A, Kant S, Niranjan V. Phenotype to Treatable Traits-Based Management in Chronic Obstructive Pulmonary Disease. Cureus. 2024;16:e60423.
26. Kerkhof M, Voorham J, Dorinsky P, et al. The Long-Term Burden of COPD Exacerbations During Maintenance Therapy and Lung Function Decline. Int J Chron Obstruct Pulmon Dis. 2020;15:1909–1918. doi:10.2147/COPD.S253812
27. Meng W, Wu J, Wang J, et al. Treatable traits identified in Chinese patients hospitalized with AECOPD: a Multicenter Cohort Study. Int J Med Sci. 2025;22(9):2227–2236. doi:10.7150/ijms.111294
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Multivariable Prediction Model to Identify Acute Exacerbation of COPD and Its Severity for COPD Management in China (DETECT Study): A Multicenter, Observational, Cross-Sectional Study
Yin Y, Xu J, Cai S, Chen Y, Chen Y, Li M, Zhang Z, Kang J
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2093-2106
Published Date: 5 September 2022
The Influence of Influenza Virus Infections in Patients with Chronic Obstructive Pulmonary Disease
Liao KM, Chen YJ, Shen CW, Ou SK, Chen CY
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2253-2261
Published Date: 14 September 2022
Effectiveness of Hospital Pharmacist Interventions for COPD Patients: A Systematic Literature Review and Logic Model
Lin G, Zheng J, Tang PK, Zheng Y, Hu H, Ung COL
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2757-2788
Published Date: 25 October 2022
Analyses of Factors Associated with Acute Exacerbations of Chronic Obstructive Pulmonary Disease: A Review
Qian Y, Cai C, Sun M, Lv D, Zhao Y
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2707-2723
Published Date: 24 November 2023
The Relationship of Fractional Exhaled Nitric Oxide in Patients with AECOPD
Xu X, Zhou L, Tong Z
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:3037-3046
Published Date: 21 December 2023