Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Effectiveness of Hospital Pharmacist Interventions for COPD Patients: A Systematic Literature Review and Logic Model
Authors Lin G, Zheng J, Tang PK ![]() , Zheng Y, Hu H
, Zheng Y, Hu H ![]() , Ung COL
, Ung COL ![]()
Received 3 August 2022
Accepted for publication 11 October 2022
Published 25 October 2022 Volume 2022:17 Pages 2757—2788
DOI https://doi.org/10.2147/COPD.S383914
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Guohua Lin,1,* Jiaqi Zheng,1,* Pou Kuan Tang,1 Yu Zheng,1 Hao Hu,1,2 Carolina Oi Lam Ung1,2
1Institute of Chinese Medical Sciences, University of Macau, Taipa, Macao SAR, People’s Republic of China; 2Department of Public Health and Medicinal Administration, Faculty of Health Sciences, University of Macau, Taipa, Macao SAR, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Carolina Oi Lam Ung, Institute of Chinese Medical Sciences, University of Macau, Taipa, Macao SAR, People’s Republic of China, Email [email protected]
Purpose: This review aimed to summarize empirical evidence about pharmacist-led interventions for chronic obstructive pulmonary disease (COPD) patients in hospital settings and to identify the components of a logic model (including input, interventions, output, outcome and contextual factors) to inform the development of hospital pharmacist’s role in COPD management.
Methods: A systematic review of literature retrieved from four English databases (PubMed, Web of Science, Scopus, ScienceDirect) and one Chinese database (CNKI) were conducted to identify eligible studies published from inception to March 2022. Studies concerning pharmacist and COPD were identified to screen for randomized controlled studies that focused on pharmacist interventions for COPD at the hospital setting.
Results: Twenty-nine studies were included in this review. The components of interventions identified were categorized according to the six service domains in the International Pharmaceutical Federation’s Basel Statements, and mainly concerned prescribing, preparation, administration and monitoring but not procurement and training. Extended interventions were also identified including life guidance, psychological counseling, and respiratory function exercise. The most common outputs reported were improvement in medication adherence, rational drug use, level of knowledge, and inhalation technique. The clinical outcomes (symptomatic control, lung function, rates of hospital readmission, length of hospital stay, and adverse drug adverse reactions), humanistic outcomes (quality of life and patient satisfaction), and economic outcomes (drug costs, hospitalization costs, antibiotic costs, and direct costs) were reported only in some studies. The contextual factors mainly included geographical factors, education level of patients, socio-economic factors, and no-smoking policy.
Conclusion: The evidence for hospital pharmacists’ interventions in improving COPD patients’ outcome is growing. However, considering the challenges of COPD management, hospital pharmacists should further leverage the advantages of cross-sector and multi-disciplinary collaboration in order to provide more comprehensive support to better address the needs of their patients.
Keywords: chronic obstructive pulmonary disease, hospital pharmacist, systematic review, intervention, output, outcome, logic model
Introduction
Chronic obstructive pulmonary disease (COPD) is a major health challenge typically associated with an irreversible decline in lung function, progressive functional disability, and a significant impact on the quality of life. Worldwide, it is estimated that COPD affects around 300 million people (4% of the world’s population) causing at least 3 million deaths each year1,2 and will become the fourth leading cause of death by 2030.3 The high prevalence, severity and high mortality rates of COPD also cause great economic burden on the patients and the overall health system.4 For instance, the annual direct medical cost per COPD patient was estimated as $10,367 in the US.5 The mean hospitalization cost per COPD patient per admission was $3669 in China.6 The hospitalization rates,7 primary care visits,8 length of hospital stay8 and ICU admissions9 were found to be associated with the severity of the illness.
Many patients with COPD cannot control the progress of the disease effectively, which inevitably contributes to periodic exacerbations in which symptoms of breathlessness and sputum production deteriorate rapidly, requiring emergency room visits and hospitalizations.10,11 In fact, acute exacerbation of COPD (AECOPD) is the principal reason for unscheduled hospital visits among COPD patients, and one of the most common reasons for hospitalization across the countries.12–15 AECOPD exerts a significant impact on patients’ health status and accelerates disease progression, leading to in-hospital mortality and post-discharge mortality. One of the important treatment goals during COPD hospitalization is to manage the symptoms and reduce the risk and severity of future exacerbations.
Pharmacist interventions at the hospital settings, both during hospitalization and at discharge, have been reported to be effective in improving the management of COPD for patients suffering from exacerbation or ready for discharge.16 For instance, a pharmaceutical care programme initiated at the emergency department could reduce the number and prevalence of drug-related negative outcomes leading to clinical benefits for the patients.17 Early in-hospital pharmacist-led medication review could optimize the pharmacotherapy and thus reduce the median length of hospital stay by at least 8% or up to 11% for patients >80 years of age).18 The pharmacist-driven COPD bundled-care could also improve outpatient management in patients with COPD.19 Pharmacists, as a member of a multidisciplinary team, also played a crucial role in hospital-based transitions of care (TOC) at the time of discharge to reduce COPD readmissions.20
Despite the emerging evidence for the benefits of improved patient outcomes associated with hospital pharmacist intervention, much of the current literature designates a prime focus on the role of pharmacist at the community level for COPD management.21,22 Indeed, within the scope of COPD, the disease is deemed preventable should risk factors such as tobacco smoking and air pollution can be avoided, while under-diagnosis and mis-diagnosis are often common, which are areas best addressed at the community setting.23 Nevertheless, COPD patients also receive care in the hospitals during specialist consultation, ICU admission and hospitalization. It is also important to systematically evaluate the role of hospital pharmacists in COPD management to supplement the current knowledge about the evidence-base approaches to the challenges of long-term COPD management and hospital readmissions.
The objective of this study was to analyze the current evidence about pharmacist-led interventions for COPD patients in hospital settings and to identify the corresponding input, output, outcome and contextual factors guided by the logic modelling framework. This will enable a better understanding of the contributions that hospital pharmacists can make and help inform strategies that support them developing their role in COPD management.
Methods
This systematic literature review was conducted and reported in compliance with the PRISMA 2020 statement.24 For searching the literature. The literature search was completed in April 2022. Articles published from inception to March 2022 were included.
Search Strategy
A systematic search of peer-reviewed published literature was performed via five electronic databases, including four English databases (PubMed, Web of Science, Scopus, ScienceDirect) and one Chinese database (China National Knowledge Infrastructure (CNKI)), were searched. The three primary search concepts were “pharmacist”, “COPD” and “hospital”. To identify appropriate key words, in addition to Medical Subject Headings (MeSH) terms, common phrases used in the literature were utilized to develop a comprehensive search strategy (Table 1). The terms within “pharmacist”, “COPD” and “hospital” were combined with OR, and the following results from each concept were combined with AND. The reference lists and citations of included articles were examined for any potential publications relevant to the objective of the current study.
 |
Table 1 Search Term Identifiers |
Inclusion and Exclusion Criteria
To be considered eligible for inclusion in the study, the literature must comply with all of the following criteria: (1) the studies must be original research limited to randomized controlled trials (RCT); (2) the main intervention providers should be pharmacists in hospital settings; (3) the pharmacist intervention should be specifically described in the article; (4) the main target disease should be COPD; (5) the full text must be available; (6) the publications must be original articles published in English or Chinese; and (7) for papers identified in CNKI, only articles published in journals listed on the 2012 Institute of Scientific and Technical (S&T) Information of China (2013a) Core Journal List were included. Exclusion criteria were: (1) observational studies, reviews, commentaries and publication types other than RCT; and (2) the main target disease of the studies was other diseases or COPD combined with other diseases.
Study Selection Procedure
The screening process was separately completed by 2 of the authors (LG and ZJ) according to the inclusion and exclusion criteria outlined above. The whole study selection procedure is shown in Figure 1. First, we yielded 1670 articles from the English databases and 44 articles from the Chinese database. After removal of duplications, 1479 articles were further screened for inclusion based on title, abstract and full-text. This screening process was conducted separately by two of the authors separately and the screening results were compared for any discrepancies. Disputes were first discussed between these 2 authors and final agreement was made upon confirmation by the senior author (COLU).
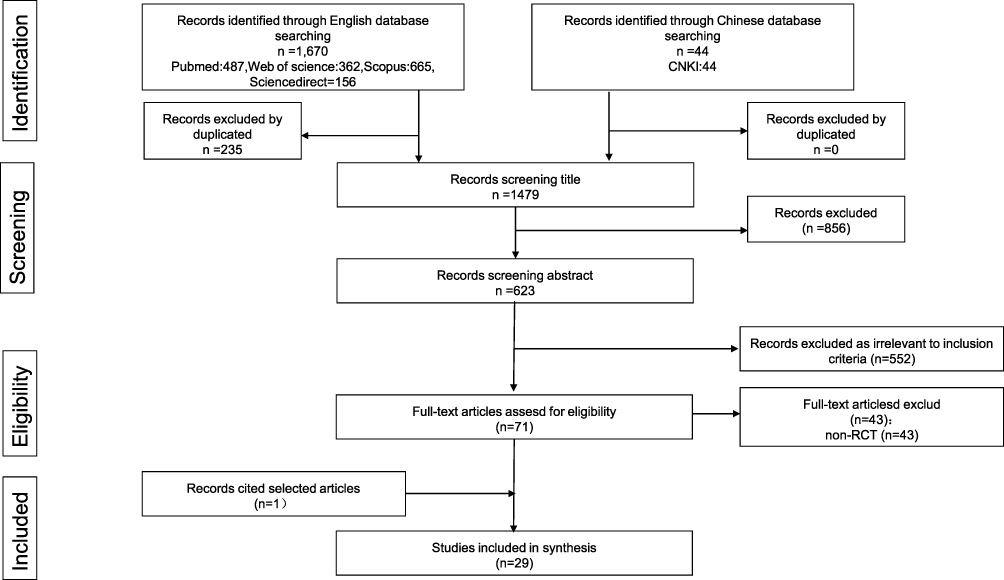 |
Figure 1 PRISMA flow chart of systematic review. Note: Adapted from Page MJ, Moher D. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372:23. Open Access.24 |
Data Extraction and Analysis
A standard extraction form was used to extract relevant data from the eligible trials, which contained the name of the first author, study location, sample size, intervention from pharmacists, outputs, and outcomes. The types of interventions were classified according to the 2015 version of the Basel Statements hosted by the Global Conference on the Hospital Pharmacy Section of the International Pharmaceutical Federation (FIP) (the Basal Statements), which covered all areas of the medicine use process in hospitals (including: (1) Procurement, (2) Prescribing, (3) Preparation and Delivery, (4) Medicine administration, (5) Monitoring of Medicine Use, and (6) Human Resources, Training and Development. The category “(7) Others” was added to accommodate any possible interventions beyond the 6 areas of the medicine use process described in the Basal Statements. Moreover, for the purpose of this study, the output of interventions referred to observations not directly related to disease conditions or management such as medication adherence, changes in blood test results, improvement of inhalation technique, etc. Patient outcomes were defined according to the ECHO model and might be grouped into economic outcomes, clinical outcomes, and/or humanistic outcomes.
Study Appraisal
For quality evaluation, we chose the CONSORT 2010 checklist25 as an evaluation tool to evaluate the validity of the results of each article. The CONSORT 2010 checklist contains 25 items to cover all important aspects of the experiment, some of which are divided into sub-items a and b. If the item was fully met, we defined it as “Fully satisfied”, and if only a sub-item was met, we defined it as “Partially satisfied”. We aggregated the numbers of “Fully satisfied”, “Partially satisfied”, “Not satisfied”, and “Not applicable” per study to assess the quality of the study. The greater the number of “fully satisfied”, the better the quality of the article. Two authors (LG and ZJ) independently appraised the quality of the included studies based on the CONSORT 2010 checklist. When there were differences and conflicts in the evaluation results, the third researcher (COLU) participated in the evaluation process and made the final evaluation.
Results
According to the inclusion and exclusion criteria, 15 English articles and 14 articles in Chinese were included in this evaluation (Table 2). The research covered ten countries and regions with China being the most common study country (n=19), followed by the United States (n=4),26,27,32,44 India (n=3),37,41,48 Jordan (n=1),29 Spain (n=1)17 and Thailand (n=1).52 The research site was mainly based on a single hospital (n=28) and only 1 study were conducted based on a collaboration of hospital44 and community pharmacy. In all studies, hospital pharmacists participated in the intervention, either as the sole healthcare profession (n=25) or as a member of a multi-disciplinary team (n=4).28,32,36,44 The duration of intervention ranged from 1 month to two years, and all the interventions were directed at patients.
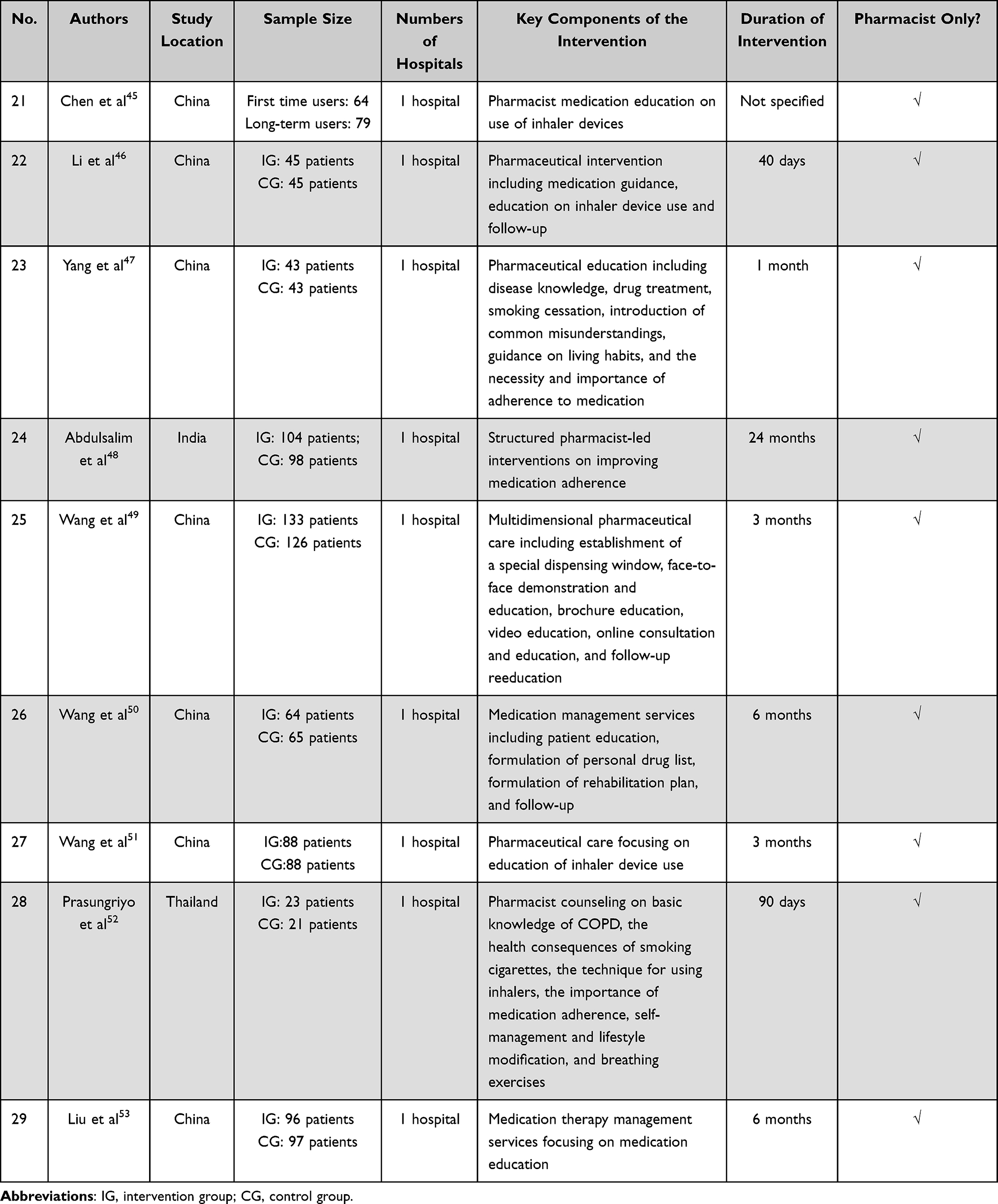 |
Table 2 Summary of Basic Information of Selected Articles |
Types of Interventions for COPD Patients Provided by Hospital Pharmacists
As shown in Table 3, pharmacists played multiple roles in COPD management in the hospital setting, most of which focused on prescribing,17,27–29,32,34,35,39,40,43,44,50,52,53 medicine administration,17,26,27,29–53 monitoring of medicine use17,26,27,29–43,46,47,50,52,53 and other non-pharmacologic therapy management.27,29,30,35,37–39,41–43,46–48,50,52 As a member of the medical team, hospital pharmacists collaborated with clinicians to formulate treatment plans. They provided recommendations for the types, indications, doses, frequency of administration, and possible side effects for each prescribed medication. Furthermore, COPD was usually complicated by a variety of primary conditions, such as diabetes and heart disease. The combination use of medications was complex, and pharmacists reviewed and adjusted the medications according to the patients’ conditions. For COPD patients requiring transition of care to primary care institutions after discharge, hospital pharmacists also ensured that the transfer of accurate information about the medication used by the patients at discharge.32,44
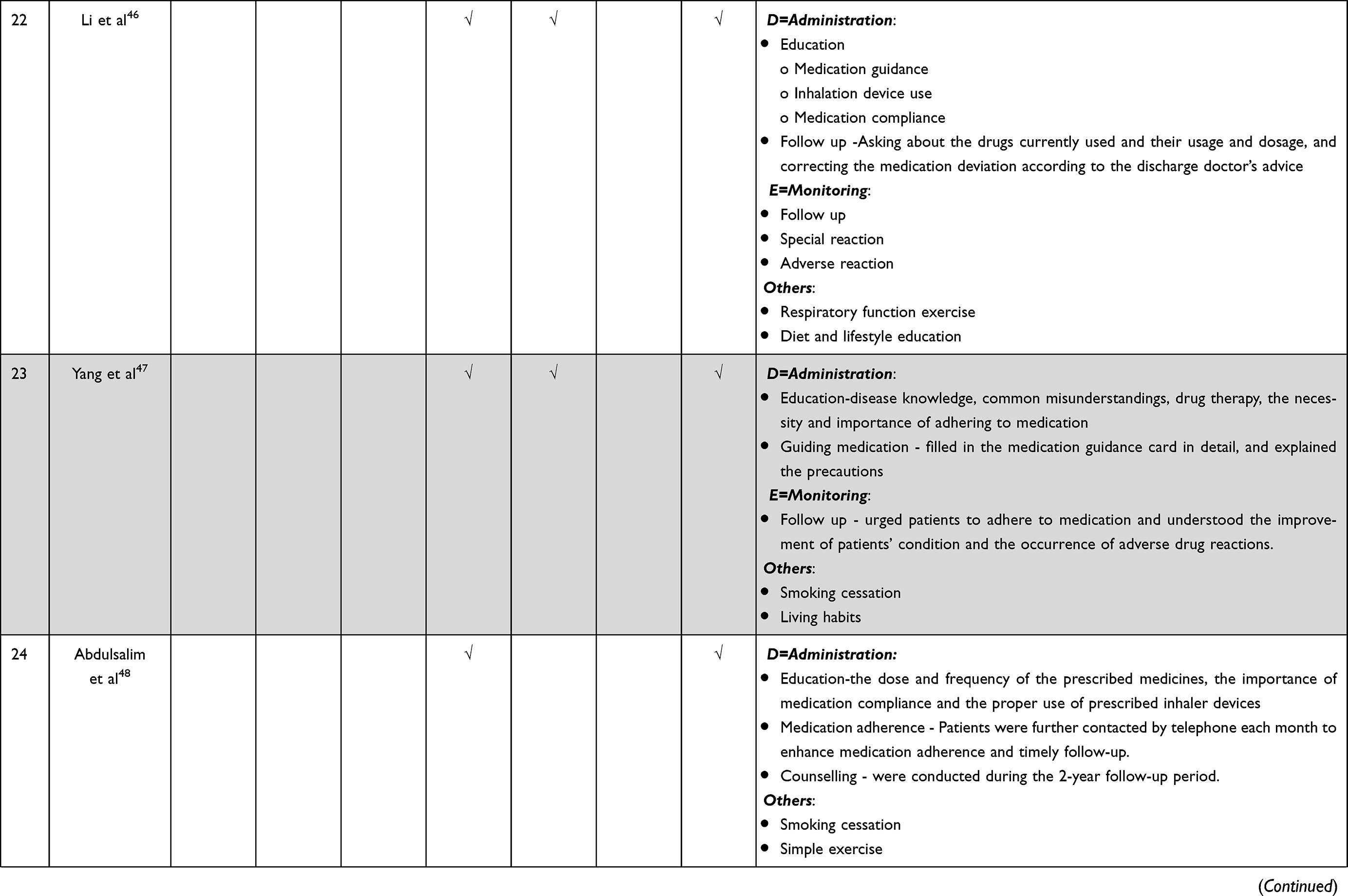 |
Table 3 Interventions Implemented by Hospital Pharmacists for COPD Patients |
Most of the pharmacist services related to medicine administration included in this review were through education. Such education intervention was primarily directed at patient instruction, including information about: 1) COPD, COPD medicines, administration and dosing, management of COPD symptoms, possible adverse reactions;27,29–33,35–53 2) rational use of specific antibiotics;27,39 and 3) proper inhaler use.27,36–39,41,48,49,51,52 In terms of educational methods, in addition to face-to-face communication,29–32,35–52 pharmacists also provided relevant reading materials for patients27,29,37,38,40–43,49,51,52 or started a WeChat or online interactive platform,42,49,51 or conducted follow-up phone calls,30–32,38,40,41,44,49,51 in order to resolve doubts during medication administration, optimize compliance and monitor for drug-related problems.
Pharmacists recorded the patients’ relevant responses to the drug treatment, COPD knowledge, medication adherence, drug-drug interactions, and adverse drug reactions for monitoring purposes.17,26,27,29–43,46,47,50,52,53 Other non-pharmacologic therapy management responsibilities for pharmacists included human resources management, training, and development, in order to continuously improve their competence and knowledge. Besides, since COPD treatment was a process that required patient self-management, pharmacists also tried to help support patients improving their lifestyles and habits particularly with smoking cessation education.27,29,37–39,41,42,47,48,50,52 More details about the intervention of hospital pharmacists are shown in Table 3.
Input of Hospital Pharmacist’ Interventions for COPD Patients
The most common inputs included in the studies were educational materials, including booklets,27,29 patient information leaflets,37,41 videos,42,49,52 popular science articles,42,49,51 brochures42,49 and printed materials.52 In addition, various forms of face-to-face education were also common, including lectures,30 interviews,31 counselling sessions,37,41 and classroom teaching.43 Some studies played the role of the network, and input WeChat interactive platform,42 online consulting platform.49,51 In addition, the inputs in the studies also included labels,26 mediation lists,32,50 and special distribution window.49
Output and Outcome of Hospital Pharmacist’ Interventions for COPD Patients
16 studies measured the output and outcome of COPD-intervention by hospital pharmacists among inpatients, 8 on outpatients26,27,29–31,42,51,59 5 on both.17,32,39,48,53 The duration of intervention reported ranged from 1 month to 24 months. Only 4 studies28,32,36,44 reported about multi-disciplinary intervention, while the others pharmacist-specific intervention.
A range of output had been reported including adherence, rational drug use, level of knowledge, drug serum level, health resources utilization, inhalation technique and success of smoking cessation. Among them, the most common change due to hospital pharmacist interventions was the improvement of patient medication adherence.26,27,29–31,38–42,46,47,49–51 The second common output reported was improved rational use of drugs.28,33,35,40,46,50,53 However, Farris et al32 reported there were no statistically significant differences in medication appropriateness. Some studies which assessed changes in the knowledge of medication and knowledge of disease management27,29,30,43,46 showed positive effects. The benefits of pharmacist intervention were also demonstrated in such areas as maintaining drug serum levels26, improving inhalation technique,36,42,43,45,49,51 reducing health resource utilizations,27,29 and promoting smoking cessation.38
All but three studies26,41,45 also measured changes in the patient outcome (clinical, economic and humanistic) upon hospital pharmacist intervention. The most commonly used clinical tests were a reduction in CAT score or mMRC grading score, or an increase in SGRQ score in the intervention group to demonstrate a better clinical outcome after pharmacist involvement in the intervention.34,35,37,38,47,49,50,52,53 An increase in the FEV1/ FEV1% was also a common test to demonstrate positive clinical outcomes.27,29,42,43,47 Other clinical outcome measured included: reduced rates of hospital readmission,27,30,32,35,39,43,45 the length of stay,17,27,28,33,53 decrease in dyspnea36,38,42 and reduced adverse drug adverse reactions.30,35,39,40,43 Regarding humanistic outcomes, some related studies showed that pharmacists provided helpful services and improved patients’ satisfaction with medical institutions.36,40,46,49,51 Several studies showed positive effects in terms of quality of life.27,31,49 However, two studies showed interventions by hospital pharmacists failed to improve patients’ quality of life.29,50 Regarding economic outcomes, five studies suggested that pharmacist services could help lower healthcare expenditures, including drug costs, costs of hospitalization, and antibiotic costs.28,33,43,48,50 Two studies showed there were no statistically significant differences in total hospitalization costs, antibacterial drug costs, daily costs, and direct costs.46,52 More details about the output and outcome of hospital pharmacist’ interventions for COPD patients are shown in Table 4.
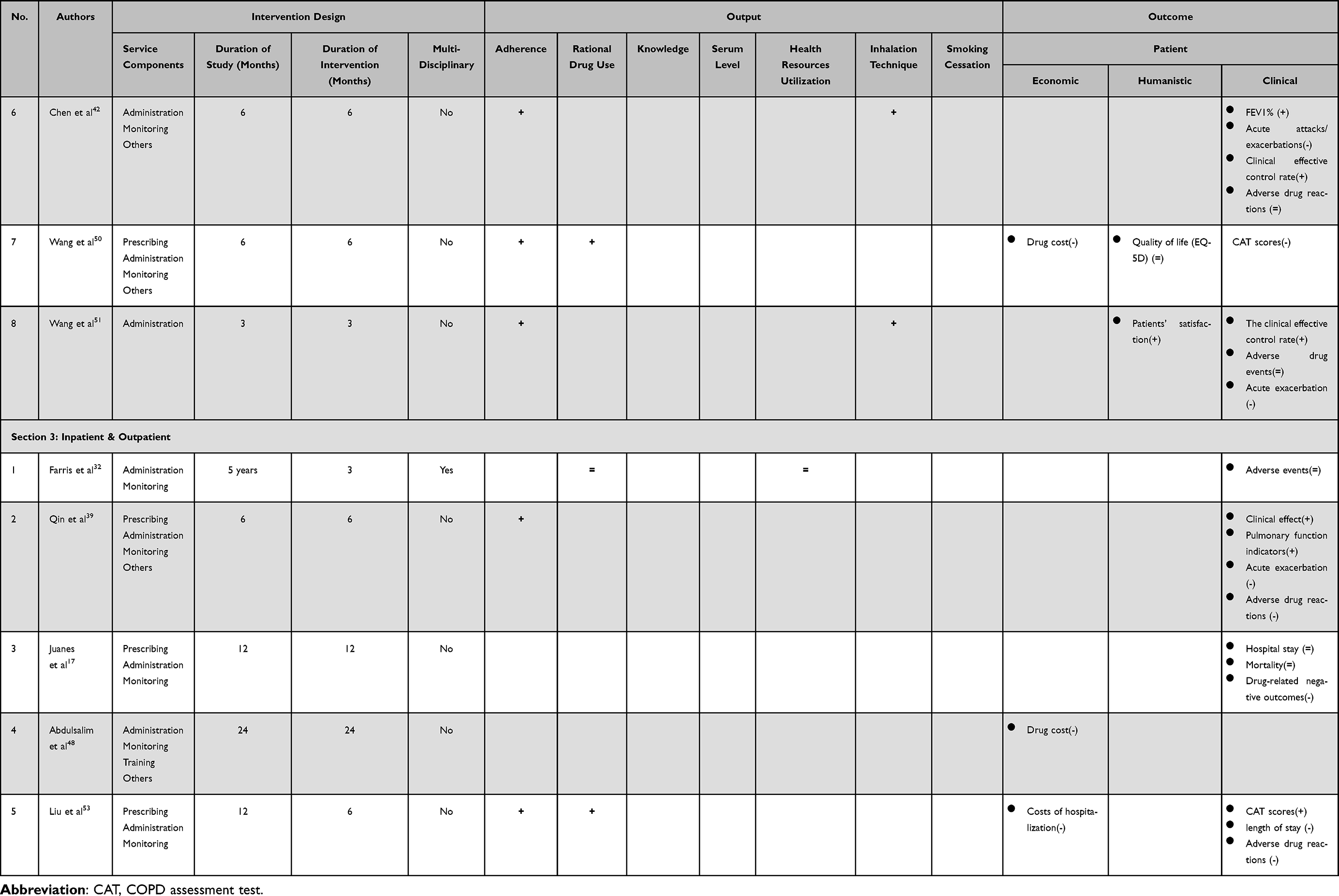 |
Table 4 Output and Outcome of Hospital Pharmacist Intervention |
Contextual Factors
Among the included literature, the contextual factors affecting the hospital pharmacists’ interventions and their effectiveness can be summarized into four factors: geographical factors;17,48 education level of patients;45 socio-economic factors;48,51 and no-smoking policy.48 With different healthcare institutes in different areas, the professional skills of medical staff, patient management, and access to certain medications varied and might have affect the outcomes.17,48 Besides, the education level of patients could affect the effect of pharmacist education, thus affecting the improvement in medication compliance.45 The presence of policies that mandated the price of cigarettes and the prohibition of smoking in public places also aided in reducing COPD and its aggravation.48
Quality Assessment
Most of the studies included in this review fully satisfied 1/3 of the CONSORT items (Figure 2). The details were as follows: (1) Title and abstract - Few articles (n=7)17,31,32,37,38,41,52 specified in their titles that they were RCTs, but most articles (n=22) provided structured abstracts; (2) Introduction - Almost all articles (n=27) reported the trial background and purpose; (3) Methods - The inclusion and exclusion criteria for study subjects were relatively well reported (n=26). Only 2 articles39,44 clearly reported the trial design, 5 articles27,32,37,40,52 fully described the details and timing of the trial intervention, 2 articles32,53 specified the exact definition of the intended primary and secondary outcome indicators and their measurement methods, and 6 articles indicated the measurement time and sample size.17,27,29,37,41,48 * In terms of randomization procedures, no articles were considered “fully satisfied”, with the most common problems including not reporting the method used to generate the type of randomization (n=15),29–33,35,36,41,45,46,49–53 allocation concealment mechanisms (n=10),26,30,33,40,45,46,49,50,52,53 blinding and who was blinded after the implementation of the blinded allocation intervention (n=16);27,29,30,33,35,39,40,43,45–47,49–53 (4) Results - Most papers described the baseline demographic and clinical characteristics (n=22), and the number of participants (denominator) included in each analysis (n=24); (6) Discussion - All articles (n=29) discussed the generalizability of the trial findings and considered other relevant evidence to make a reasonable interpretation of the trial findings. However, less than half of the articles considered trial limitations and analyzed them; (8) Other information - Few articles reported study registration (n=7),17,27,32,37,38,41,42 study protocols (n=1),44 and 14 articles reported funding.27,29,31,32,37–40,42–45,50,52,53
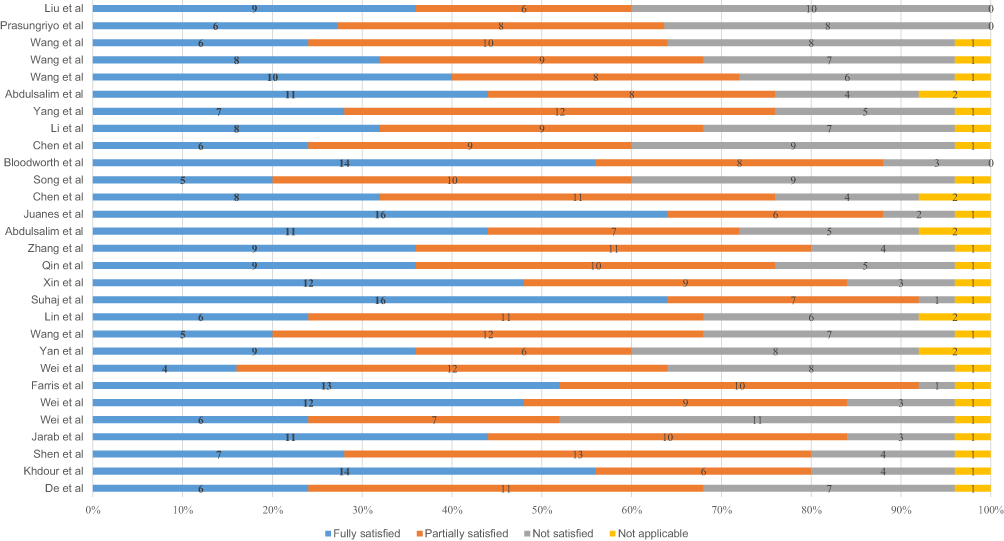 |
Figure 2 Reporting quality of the included studies according to the CONSORT Guideline (n=29). |
Discussion
This systematic literature review included 29 articles which reported the results of RCTs investigating the impact of interventions provided by hospital pharmacists on COPD patients. The findings provide a detailed summary of the evidence pertaining to the role hospital pharmacists could play in COPD management. An overview of the types of interventions, the output and outcome measures and the contextual factors identified was depicted following the logic modelling framework (Figure 3). In accordance with the general recommendations listed in the Basel statements, interventions by hospital pharmacists for COPD patients identified in this study mainly included preparation, prescribing, administration, and monitoring (but not so much about procurement and training). Extended interventions were also identified including lifestyle guidance, psychological counseling, and respiratory function exercise. Overall, hospital pharmacists’ COPD-interventions had been shown to be beneficial to patient care in terms of a range of output (patient medication adherence,26,27,29–31,38–42,46,47,49–51 rational use of drugs,28,33,35,40,46,50,53 knowledge,27,29,30,43,46 serum levels,26 inhalation technique,36,42,43,45,49,51 health resource utilizations,27,29 and smoking cessation38), as well as clinical outcome (CAT score or mMRC grading score, SGRQ,34,35,37,38,47,49,50,52,53 FEV1/FEV1%,27,29,42,43,47 rates of hospital readmission,27,30,32,35,39,43,45 the length of stay,17,27,28,33,53 dyspnea36,38,42 and adverse drug adverse reactions30,35,39,40,43), economic outcome (drug costs,33,46,48,50 hospitalization costs,28,33,46,53 antibiotic costs,28,33,43,46 daily costs,46 total costs,43 and direct costs52) and humanistic outcome (patients’ satisfaction,36,40,46,49,51 quality of life27,29,31,49,50). This logic model may serve as a foundation for coordinating, promoting and evaluating hospital pharmacists’ initiatives to strengthen COPD patient management.
 |
Figure 3 The logic model of hospital pharmacist interventions for COPD patients. |
According to the National Institute of Clinical Excellence (NICE) clinical guideline,54 COPD patients are in need of various support: advising patients about how to effectively use inhaled medications, educate patients about how to effectively manage their symptoms and exacerbations, support patients to quit smoking, promote healthy living and exercise, and help monitor antibiotic and corticosteroid use. As reported in the included studies in this review, which also echoed with the findings from a previous study,55 hospital pharmacists were well-positioned to cover all these areas through the provision of pharmaceutical care to support the management and care of patients with COPD.17,26,27,29–53 COPD patients seeking help at the hospital setting, whether it be for specialist consultation, ER visits or hospitalizations, were usually prone to more severe cases of the disease requiring more complex medication use. Advising about pharmacotherapy regimen tailored to individual patients, taking into account their full medical and medication history and their most recent clinical presentations, were considered important to both prescribers and the patients.17,27–29,32,34,35,39,40,43,44,50,52,53
Hospital pharmacists were trained as a custodian of drug safety.56 Having access to patients’ full medical record, they were positioned to evaluate the rationale of drug use, determine and prevent any avoidable adverse drug reactions and drug interactions, and monitor for any unforeseeable drug related problems for timely management. This was especially the case when patients were prescribed to use medicines with narrow therapeutic index or great potentials to interact (eg theophylline).28,33,35,40,46,50,53 Informing the patients about the importance of compliance with the use of preventer inhaler, and gargling after the use of inhaled corticosteroid medication to reduce the risks of common side effects (eg oral thrush) was some of the basic actions pharmacists should take when caring for COPD patients.26,27,29–31,38–42,46,47,49–51 In 2 studies, pharmacists’ monitoring of patient proper use of antibiotics and oral corticosteroids for acute exacerbations also demonstrated benefits in quality of life, severe exacerbations and hospitalizations.27,39 Educating the patients about the technique of using different inhaled medications, and supporting the correct use of such medication even after discharge were also found to be important for symptomatic control and reducing readmission.27,36–39,41,48,49,51,52
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2022 report repeatedly emphasizes on the importance of compliance to COPD medications and the accuracy of inhaler technique for patients to achieve control of the disease.57 However, incorrect use of the inhaled medications remain a long-standing challenge in the management of COPD and the prevalence of correct inhaler use remains unacceptably low,58 which were associated with poor disease control and frequent disease exacerbation.59 Critical errors in inhalation device technique for different types of inhalers (pressurized metered dose inhaler (pMDI), dry powder inhaler (DPI), soft mist inhaler (SMI)) had been well-documents for pharmacists to deliver more targeted counselling.58,60 Moreover, hospital pharmacists could also offer advice to the prescribers about the choice of inhaler device considering individual patients preference, needs and abilities.61,62 The benefits of improved adherence26,27,29–31,38–42,46,47,49–51 due to hospital pharmacists’ intervention were observed in both outpatients and inpatients.
Improvements in patient medication adherence were the most common outcome change.26,27,29–31,38–42,46,47,49–51,53 The indicators for evaluating medication adherence were mixed. The Morisky scale was used most, and it was used in seven articles.27,30,39,41,47,50,53 Besides, the Medication Adherence Questionnaire (MAQ),41 the BMQ score,49 medication refill adherence scores38 and pill counts plus direct interview26 were also used. However, one Chinese study45 did not specify the method of measuring medication adherence. Although we believed that the care of hospital pharmacists could improve the compliance of patients, the standards for measuring the degree of improvement in medication adherence were different, making it challenging to compare study results and the effectiveness of different pharmacist interventions. Besides, we were unable to determine whether the patient’s medication compliance may be improved for a longer period of time after the completion of the care plan. COPD generally requires long-term treatment time. The improvement of patient compliance must be sustained over a long period of time, and more studies on this topic are anticipated in the future.
This review also showed that hospital pharmacists’ role in supporting the management and care of COPD patients extended beyond drug treatment. As recommended previously,63,64 the hospital pharmacists involved in this review were often actively involved in patient counseling about the disease, drug use and control of symptoms,17,26,27,29–35,37–44,46–53 lifestyles and habits particularly with smoking cessation education.27,29,37–39,41,42,47,48,50,52 Smoking cessation, in particular, has a major influence on the disease course65 and pharmacists could play an important role in the effective delivery of smoking cessation counseling.66 As reported in one of the studies in this review, patients who attended the pharmacist-managed clinic were more likely to quit smoking. This is in line with other previous findings that even brief pharmacist-led counseling sessions were found to be associated with long periods of persistent quitting.66 As such, even pharmacists in the hospital settings should take every opportunity to provide smoking cessation counseling and discuss with the patients about the tobacco cessation drug therapy.67
On contrary, this review also uncovered a number of areas about hospital pharmacists’ role in COPD management that were under-researched. Firstly, only 1 study in this review investigated the effect of the cooperation by hospital pharmacists with pharmacies in the community setting.44 Transition of care (TOC) refers to the various points where a patient moves to, or returns from, a particular physical location for the purposes of receiving health care.68 It had been estimated that about 60% of all medication errors occur during TOC.69 It was of particular importance that hospital pharmacists were able to identify patients in need of post-discharge support and engage in communication and collaboration with their community pharmacists.70 Upon patients’ consent, programs that involved the sharing of information about medication therapy, monitoring requirements and other precautions between hospital pharmacists and community pharmacists. There is a need for more research to determine if such cross-sector collaboration would be beneficial to the patients’ long-term disease control such as reduction in medication errors and even readmission in order to support the overall practices in COPD management during TOC.71,72
Secondly, the extent of physician-pharmacist collaboration for COPD management in the hospital setting was under-reported as only 2 studies in the review focused on multi-disciplinary intervention involving these 2 healthcare professions.28,36 In a multidisciplinary approach, pharmacists played an important role in managing drug therapy and were thus integral members of healthcare professional (HCP) teams.21 They were well-equipped to make inter-professional contribution by providing evidence-based pharmaco-therapeutic recommendations, and establishing and maintaining an effective medication reconciliation process in the hospital setting.73 Patients being looked after via physician-pharmacist collaborative practices were likely to demonstrate improved disease control.74 Program design involving physician-pharmacist collaboration required more research about its effect on patient outcome which would serve as evidence that further encouraged physicians’ increased rate of acceptance of pharmacist interventions.
Thirdly, hospital pharmacists’ role in pulmonary rehabilitation was not fully evaluated according to the findings of this review as only 3 studies explored this extended role.46,50,52 Pulmonary rehabilitation is a specialized programme of exercise and education designed to help people with lung problems such as COPD and had been shown to effectively improve symptomatic control and reduce hospital readmissions, and improve patients’ quality of life.75 It had been suggested that pharmacists’ participation in pulmonary rehabilitation for COPD patients might be beneficial with patient education about the use of medications, dosage, inhalation technique, symptoms and adverse drug reaction monitoring, and support to lifestyle changes leading to enhanced quality of life for the patients.76 Fourthly, pharmacists’ active role in improving the rates of vaccination against influenza through identifying predisposing factors and patient education might help to decrease the risk of lower respiratory tract infections triggering exacerbation of COPD.76 However, no study in this review had explored the benefits of hospital pharmacists’ involvement on vaccination intention. Further research is needed to allow the leverage of hospital pharmacists’ contribution in promotion seasonal influenza vaccine in the overall COPD management.
This study has some limitations. Firstly, this study is a systematic literature review which included exclusively findings of RCTs. While the quality of evidence for hospital pharmacists’ interventions derived from RCTs was considered the highest, this review was not able to capture any emerging trend or practice reported in other publication types. Future study could collect information from other sources, including cross-sectional studies and qualitative studies to validate and enrich the logic model developed in this study. Secondly, the included studies were heterogeneous in design and outcome of interest which made it difficult to compare results across studies. Thirdly, most of the studies included in this review were of moderate quality. However, the concerns about the quality of the included articles was not viewed to have significant import on the overall findings about the current landscape of hospital pharmacists’ participation in COPD management. Despite the above-mentioned limitations, it is believed that this systematic review provided a comprehensive insight into a growing body of important literature that demonstrates the beneficial role of hospital pharmacists in COPD management.
Conclusion
Hospital pharmacists’ interventions are effective for the management and care of COPD. Although the availability of high-quality, robust RCTs evaluating the impact of their interventions on patient outcomes is limited, the growing body of evidence identified in this study suggested that hospital pharmacists played a crucial role in the care of both COPD inpatients and outpatients, during their study in the hospital and even after discharge. Indeed, this current study has provided specific examples of interventions including pharmacists-only interventions and multi-disciplinary approach improving patients’ clinical, humanistic and economic outcomes; however, study designs were highly variable highlighting a lack of standardized approach to COPD management by pharmacists at the hospital setting. Future research should focus on providing strong evidence to support the development of standardized approach and thus good practices for pharmacists when caring for COPD patients in the hospital setting.
Data Sharing Statement
All the data for this systematic review has been included into the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was financed by the University of Macau (SRG2021-00007-ICMS) and the Science and Technology Development Fund, Macau SAR (SKL-QRCM(UM)-2020-2022), and did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
Guohua Lin and Jiaqi Zheng are co-first authors for this work. The authors declare no conflicts of interest in this work.
References
1. Soriano JB, Kendrick PJ, Paulson KR. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/S2213-2600(20)30105-3
2. Li X, Cao X. Trends and risk factors of mortality and disability adjusted life years for chronic respiratory diseases from 1990 to 2017: systematic analysis for the Global Burden of Disease Study 2017. BMJ. 2020;368:34.
3. World Health Organization. Chronic respiratory diseases: burden of COPD. Available from: https://www.who.int/respiratory/copd/burden/.
4. Iheanacho I, Zhang S, King D, Rizzo M, Ismaila AS. Economic burden of chronic obstructive pulmonary disease (COPD): a systematic literature review. Int J Chron Obstruct Pulmon Dis. 2020;15:439. doi:10.2147/COPD.S234942
5. Menzin J, Boulanger L, Marton J. The economic burden of chronic obstructive pulmonary disease (COPD) in a US Medicare population. Respir Med. 2008;102(9):1248–1256. doi:10.1016/j.rmed.2008.04.009
6. Li M, Wang F. Factors contributing to hospitalization costs for patients with COPD in China: a retrospective analysis of medical record data. Int J Chron Obstruct Pulmon Dis. 2018;13:3349. doi:10.2147/COPD.S175143
7. Merinopoulou E, Raluy-Callado M, Ramagopalan S, MacLachlan S, Khalid JM. COPD exacerbations by disease severity in England. Int J Chron Obstruct Pulmon Dis. 2016;11:697. doi:10.2147/COPD.S100250
8. Thomas M, Radwan A. COPD exacerbation frequency, pharmacotherapy and resource use: an observational study in UK primary care. COPD. 2014;11(3):300–309.
9. Xu X, Knight T. Patient characteristics, health resource utilization (HRU) and treatment costs of chronic obstructive pulmonary disease (COPD) patients treated in hospital facilities for exacerbations. In: B45. Exacerbations of COPD: Prevention, Treatment and Outcomes. American Thoracic Society; 2012:A3047.
10. Pauwels RA, Rabe KF. Burden and clinical features of chronic obstructive pulmonary disease (COPD). Lancet. 2004;364(9434):613–620. doi:10.1016/S0140-6736(04)16855-4
11. Mathers CD, Loncar D, Samet J. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):e442. doi:10.1371/journal.pmed.0030442
12. Perera PN, Armstrong EP, Sherrill DL, et al. Acute exacerbations of COPD in the United States: inpatient burden and predictors of costs and mortality. COPD. 2012;9(2):131–141. doi:10.3109/15412555.2011.650239
13. Liang L, Li C, Shen Y, et al. Long-term trends in hospitalization and outcomes in adult patients with exacerbation of chronic obstructive pulmonary disease in Beijing, China, from 2008 to 2017. Int J Chron Obstruct Pulmon Dis. 2020;15:1155. doi:10.2147/COPD.S238006
14. Rothnie KJ, Müllerová H, Thomas SL, et al. Recording of hospitalizations for acute exacerbations of COPD in UK electronic health care records. Clin Epidemiol. 2016;8:771. doi:10.2147/CLEP.S117867
15. Overbeek JA, Penning-van Beest FJA, Balp MM, et al. Burden of exacerbations in patients with moderate to very severe COPD in the Netherlands: a real-life study. COPD. 2015;12(2):132–143. doi:10.3109/15412555.2014.898053
16. Mohammed MA, Moles RJ, Chen TF. Impact of pharmaceutical care interventions on health-related quality-of-life outcomes: a systematic review and meta-analysis. Ann Pharmacother. 2016;50(10):862–881. doi:10.1177/1060028016656016
17. Juanes A, Garin N, Mangues MA, et al. Impact of a pharmaceutical care programme for patients with chronic disease initiated at the emergency department on drug-related negative outcomes: a randomised controlled trial. Eur J Hosp Pharm. 2018;25(5):274–280. doi:10.1136/ejhpharm-2016-001055
18. Hohl CM, Partovi N, Ghement I, et al. Impact of early in-hospital medication review by clinical pharmacists on health services utilization. PLoS One. 2017;12(2):e0170495. doi:10.1371/journal.pone.0170495
19. Smith AL, Palmer V, Farhat N, et al. Hospital-based clinical pharmacy services to improve ambulatory management of chronic obstructive pulmonary disease. J Pharm Technol. 2017;33(1):8–14. doi:10.1177/8755122516675635
20. Gentene AJ, Guido MR, Woolf B, et al. Multidisciplinary team utilizing pharmacists in multimodal, bundled care reduce chronic obstructive pulmonary disease hospital readmission rates. J Pharm Pract. 2021;34(1):110–116. doi:10.1177/0897190019889440
21. Van der Molen T, van Boven JFM, Maguire T, et al. Optimizing identification and management of COPD patients–reviewing the role of the community pharmacist. Br J Clin Pharmacol. 2017;83(1):192–201. doi:10.1111/bcp.13087
22. Hu Y, Yao D, Ung COL, et al. Promoting community pharmacy practice for Chronic Obstructive Pulmonary Disease (COPD) management: a systematic review and logic model. Int J Chron Obstruct Pulmon Dis. 2020;15:1863. doi:10.2147/COPD.S254477
23. Forum of International Respiratory Societies. The Global Impact of Respiratory Disease.
24. Page MJ, Moher D. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372:23.
25. Moher D, Hopewell S, Schulz KF, et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. Int J Surg. 2012;10(1):28–55. doi:10.1016/j.ijsu.2011.10.001
26. De Tullio PL, Kirking DM, Arslanian C, et al. Compliance measure development and assessment of theophylline therapy in ambulatory patients. J Clin Pharm Ther. 1987;12(1):19–26.
27. Khdour MR, Kidney JC, Smyth BM, et al. Clinical pharmacy‐led disease and medicine management programme for patients with COPD. Br J Clin Pharmacol. 2009;68(4):588–598. doi:10.1111/j.1365-2125.2009.03493.x
28. Shen J, Sun Q, Zhou X, et al. Pharmacist interventions on antibiotic use in inpatients with respiratory tract infections in a Chinese hospital. Int J Clin Pharm. 2011;33(6):929–933. doi:10.1007/s11096-011-9577-z
29. Jarab AS, AlQudah SG, Khdour M, et al. Impact of pharmaceutical care on health outcomes in patients with COPD. Int J Clin Pharm. 2012;34(1):53–62. doi:10.1007/s11096-011-9585-z
30. Wei L, Li J, Luo H, et al. Effects of pharmaceutical care on drug compliance of patients with chronic obstructive pulmonary disease in stable phase. China Pharm. 2013;24(14):1316–1318.
31. Wei L, Yang X, Li J, et al. Effect of pharmaceutical care on medication adherence and hospital admission in patients with chronic obstructive pulmonary disease (COPD): a randomized controlled study. J Thorac Dis. 2014;6(6):656. doi:10.3978/j.issn.2072-1439.2014.06.20
32. Farris KB, Carter BL, Xu Y, et al. Effect of a care transition intervention by pharmacists: an RCT. BMC Health Serv Res. 2014;14(1):1–13. doi:10.1186/1472-6963-14-406
33. Wei B, Tang L, Deng B, et al. Comparative analysis of antibacterial drugs therapy for COPD inpatients. Chin Pharm. 2014;25(34):3172–3174.
34. Yan Y, Jiang X, Ting X. The clinical therapeutic effect of pharmaceutical care on old patients with chronic obstructive pulmonary disease. Chin J Hosp Pharm. 2014;34(06):489–491.
35. Wang Y, Yu L, Cui H. Effect of pharmaceutical care on the efficacy of senior patients with Chronic Obstructive Pulmonary. Chin Pharmacist. 2015;2015:1760–1762.
36. Lin Q, Dai W, Zheng B, et al. Study on the application of oxygen-driven aerosol inhalation in chronic obstructive pulmonary disease patients and pharmaceutical care in our hospital. Chin Pharm. 2015;26;02:276–278.
37. Suhaj A, Manu MK, Unnikrishnan MK, et al. Effectiveness of clinical pharmacist intervention on health‐related quality of life in chronic obstructive pulmonary disorder patients–a randomized controlled study. J Clin Pharm Ther. 2016;41(1):78–83. doi:10.1111/jcpt.12353
38. Xin C, Xia Z, Jiang C, et al. The impact of pharmacist-managed clinic on medication adherence and health-related quality of life in patients with COPD: a randomized controlled study. Patient Prefer Adherence. 2016;10:1197. doi:10.2147/PPA.S110167
39. Qin Q, Chen R, Zhang Y, et al. Clinical evaluation and implement of grading pharmaceutical care on patients with asthma and COPD. Chin Pharmaceut J. 2017;2017:1460–1464.
40. Zhang L, Dong H. Evaluation of intervention effects of standardized pharmaceutical care on clinical treatment of AECO-PD patients. Chin Pharm. 2017;32:2847–2851.
41. Abdulsalim S, Unnikrishnan MK, Manu MK, et al. Structured pharmacist-led intervention programme to improve medication adherence in COPD patients: a randomized controlled study. Res Soc Admin Pharm. 2018;14(10):909–914. doi:10.1016/j.sapharm.2017.10.008
42. Chen R, Zhou L, Qin Q, et al. Study on practice and effect of SIMPLE pharmaceutical care mode in Chronic Disease Management of Bronchial asthma and COPD patients. Chin Pharm. 2018;32:1400–1403.
43. Song Z, Zheng C, Xing S, et al. Integrated pharmaceutical care for asthma-COPD overlap syndrome patients. Herald Med. 2018;2018:319–322.
44. Bloodworth LS, Malinowski SS, Lirette ST, et al. Pharmacist linkage in care transitions: from academic medical center to community. J Am Pharm Assoc. 2019;59(6):896–904. doi:10.1016/j.japh.2019.08.011
45. Chen J, Lei M, Li S, et al. Evaluating and analyzing the use of inhalation devices in chronic obstructive pulmonary disease patients. Chin J Clin Pharmacol. 2019;35;11:1179–1182.
46. Li Z, Zhong H, Ouyang A. Pharmaceutical intervention in evaluation of clinical pathway for patients with chronic obstructive pulmonary disease effect. Chin J Hosp Pharm. 2019;39(05):525–527+540.
47. Yang X, Zhu Q. Application effect of clinical pharmacist developing pharmaceutical service in patients with Chronic Obstructive Pulmonary Disease. J Chongqing Univ Technol. 2019;33(03):184–188.
48. Abdulsalim S, Unnikrishnan MK, Manu MK, et al. Impact of a clinical pharmacist intervention on medicine costs in patients with chronic obstructive pulmonary disease in India. Pharmacoeconomics-Open. 2020;4(2):331–342. doi:10.1007/s41669-019-0172-x
49. Wang W, Xu T, Qin Q, et al. Effect of a multidimensional pharmaceutical care intervention on inhalation technique in patients with asthma and COPD. Can Respir J. 2020;2020:1–10. doi:10.1155/2020/8572636
50. Wang Y, Wu Q, Chen H, et al. Evaluation of the effectiveness of medication management services in patients with chronic obstructive pulmonary disease. Chin J Hosp Pharm. 2020;40(23):2453–2458.
51. Wang W, Zhou L, Chen R. Practice and exploration of characteristic pharmaceutical care model in patients with asthma and Chronic Obstructive Pulmonary Disease. Herald Med. 2020;39(12):1735–1741.
52. Prasungriyo N, Sooksai N. Effect of pharmacy counseling on readmissions in patients with acute exacerbations of COPD: a randomized controlled trial. J Health Sci Med Res. 2021;39(6):467–479.
53. Liu M, Liu J, Geng Z, et al. Evaluation of outcomes of medication therapy management (MTM) services for patients with chronic obstructive pulmonary disease (COPD). Pak J Med Sci. 2021;37(7):1832–1836. doi:10.12669/pjms.37.7.4518
54. Chronic obstructive pulmonary disease in over 16s: diagnosis and management. Available from: https://www.nice.org.uk/guidance/ng115.
55. Detoni KB, Oliveira IV, Nascimento MMG, Caux TR, Alves MR, Ramalho-de-oliveira D. Impact of a medication therapy management service on the clinical status of patients with chronic obstructive pulmonary disease. Int J Clin Pharm. 2017;39(1):95–103. doi:10.1007/s11096-016-0402-6
56. Hepler CD, Strand LM. Opportunities and responsibilities in pharmaceutical care. Am J Hosp Pharm. 1990;21:533–543.
57. Global strategy for prevention, diagnosis and management of COPD: 2022 Report. Available from: https://goldcopd.org/2022-gold-reports-2/.
58. Sanchis J, Gich I, Pedersen S. Systematic review of errors in inhaler use: has patient technique improved over time? Chest. 2016;150(2):394–406. doi:10.1016/j.chest.2016.03.041
59. Molimard M, Raherison C, Lignot S. Chronic obstructive pulmonary disease exacerbation and inhaler device handling: real-life assessment of 2935 patients. Eur Respir J. 2017;49(2):1601794. doi:10.1183/13993003.01794-2016
60. Ding B, Siddiqui S, DePietro M, Petersson G, Martin UJ. inhaler usability of a pressurized metered dose inhaler and a soft mist inhaler in patients with COPD: a simulated-use study. Chron Respir Dis. 2018;16:1479972318787914. doi:10.1177/1479972318787914
61. Mäkelä MJ, Backer V, Hedegaard M, Larsson K. Adherence to inhaled therapies, health outcomes and costs in patients with asthma and COPD. Respir Med. 2013;107(10):1481–1490. doi:10.1016/j.rmed.2013.04.005
62. Hodder R. Patient preferences for inhaler devices in chronic obstructive pulmonary disease: experience with Respimat® Soft Mist™ Inhaler. Int J Chron Obstruct Pulmon Dis. 2009;107:381. doi:10.2147/COPD.S3391
63. Eisenhower C. Impact of pharmacist-conducted medication reconciliation at discharge on readmissions of elderly patients with COPD. Ann Pharmacother. 2014;48(2):203–208. doi:10.1177/1060028013512277
64. Hudd TR. Emerging role of pharmacists in managing patients with chronic obstructive pulmonary disease. Eur Respir J. 2020;77(19):1625–1630. doi:10.1093/ajhp/zxaa216
65. Global initiative for Chronic Obstructive Lung Disease. GOLD 2020 guidelines. Available from: https://goldcopd.org/.
66. Bock BC, Hudmon KS, Christian J, Graham AL, Bock FR. A tailored intervention to support pharmacy-based counseling for smoking cessation. Nicotine Tob Res. 2010;12(3):217–225. doi:10.1093/ntr/ntp197
67. Adams AJ, Hudmon KS. Pharmacist prescriptive authority for smoking cessation medications in the United States. J Am Pharm Assoc. 2018;58(3):253–257. doi:10.1016/j.japh.2017.12.015
68. Transitions of care. Available from: https://apps.who.int/iris/bitstream/handle/10665/252272/9789241511599-eng.pdf.
69. Kirwin J, Canales AE, Bentley ML; American College of Clinical Pharmacy. Process indicators of quality clinical pharmacy services during transitions of care. Pharmacotherapy. 2012;32(11):e338–e347. doi:10.1002/phar.1214
70. Bethishou L, Herzik K, Fang N, Abdo C, Tomaszewski DM. The impact of the pharmacist on continuity of care during transitions of care: a systematic review. J Am Pharm Assoc. 2020;60(1):163–177. doi:10.1016/j.japh.2019.06.020
71. Ensing HT, Koster ES, Dubero DJ, van Dooren AA, Bouvy ML. Collaboration between hospital and community pharmacists to address drug-related problems: the HomeCoMe-program. Res Soc Admin Pharm. 2019;15(3):267–278. doi:10.1016/j.sapharm.2018.05.001
72. Li J, Young R, Williams MV. Optimizing transitions of care to reduce rehospitalizations. Cleve Clin J Med. 2014;81(5):312–320. doi:10.3949/ccjm.81a.13106
73. Thoma MM. ASHP statement on the pharmacist’s role in medication reconciliation. Eur Respir J. 2013;70(5):453–457.
74. Hwang AY, Gums TH, Gums JG. The benefits of physician-pharmacist collaboration. J Fam Pract. 2017;66(12):E1–E8.
75. NHS. Treatment - Chronic obstructive pulmonary disease (COPD). Available from: https://www.nhs.uk/conditions/chronic-obstructive-pulmonary-disease-copd/treatment/#:~:text=Pulmonary%20rehabilitation%20is%20a%20specialised,self%2Dconfidence%20and%20emotional%20wellbeing.
76. Arabyat RM, Raisch DW, Bakhireva L. Influenza vaccination for patients with chronic obstructive pulmonary disease: implications for pharmacists. Res Soc Admin Pharm. 2018;14(2):162–169. doi:10.1016/j.sapharm.2017.02.010
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prognostic Value of Pace Variability, a Novel 6MWT-Derived Feature, in Patients with Chronic Obstructive Pulmonary Disease
Huang CT, Ruan SY, Lai F, Chien JY, Yu CJ
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1555-1564
Published Date: 21 July 2023
Accurate Identification and Intervention System Construction of Treatable Traits in Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease: Protocol for a Randomized Controlled Study
Ma Y, Meng W, Zong D, Zeng H, Chen Y
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:622504
Published Date: 17 July 2026