Back to Journals » Breast Cancer: Targets and Therapy » Volume 14
Pyrotinib for Elderly Patients with Advanced HER2-Positive Breast Cancer
Authors Li Y, Ma X, Zhao Z, Li L, Gao C, Liu D, Li B, Zhao B
Received 27 July 2022
Accepted for publication 16 November 2022
Published 6 December 2022 Volume 2022:14 Pages 405—415
DOI https://doi.org/10.2147/BCTT.S383272
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Yan Li, Xiaoping Ma, Zhenhui Zhao, Li Li, Chunyan Gao, Dan Liu, Bingyu Li, Bing Zhao
Department of Breast Cancer, Affiliated Tumor Hospital of Xinjiang Medical University, The Clinical Research Center of Breast Tumor and Thyroid Tumor in Xinjiang Uygur Autonomous Region, Urumqi, Xinjiang, 830011, People’s Republic of China
Correspondence: Bing Zhao, Affiliated Tumor Hospital of Xinjiang Medical University, No. 789 Suzhou East Street, Urumqi, Xinjiang, 830011, People’s Republic of China, Tel +86 991 781 9142, Email [email protected]
Introduction: According to the latest global cancer data released by WHO in 2020, the incidence of breast cancer (BC) has been the most prevalent, and the mortality rate of female malignant tumor ranks the first.
Methods: To evaluate toxicity and efficacy regarding oral Pyrotinib for elderly patients with advanced HER2-positive breast cancer (BC) in Xinjiang, 45 elderly patients having advanced HER2-positive BC with age ≥ 65 years and receiving Pyrotinib-based combined therapy from January 2019 to May 2021 in Xinjiang were enrolled in this study. PFS, CBR, ORR and drug-related adverse events (AE) of oral Pyrotinib in the patients were retrospectively analyzed. All 45 patients completed the efficacy evaluation.
Results: Total ORR and CBR of the whole group was 37.8% and 77.8%, respectively. There were 14 patients with brain metastases (31.1%), with a median PFS of 6.8 months (95% CI: 5.4~9.8). In terms of the number of treatment lines, mPFS for line 1– 2 was 8.3 months (95% CI: 6.3~11.4), and mPFS for line ≥ 3 was 3.3 months (95% CI: 2.7~5.1). At the final maintenance dose, mPFS at standard doses of 400mg, 320mg and 240mg were 9.1 months (95% CI: 4.1~9.5), 8.3 months (95% CI: 4.3~12.2) and 4.8 months (95% CI: 2.1~7.5), respectively.
Discussion: Applying Pyrotinib in elderly patients, the main adverse reaction was diarrhea, accounting for 88.9% (40/45). Pyrotinib is safe and effective for elderly patients with advanced HER2 positive BC.
Keywords: HER2, breast cancer, Pyrotinib, toxicity, adverse events, elderly
Introduction
According to the latest global cancer data released by WHO in 2020, the incidence of breast cancer (BC) has been the most prevalent, and the mortality rate of female malignant tumor ranks the first.1 BC is also the first major malignant tumor that threatens the health of Chinese women. Chinese women aged 70~74 are facing another peak of BC.2 However, elderly BC patients are often complicated with chronic underlying diseases such as cardiovascular and cerebrovascular diseases, with poor compensatory ability of organ function, poor tolerance of antitumor therapy, and high risk of treatment-related complications. Therefore, the treatment selections for patients in advanced ages are different from those for young patients. Human epidermal growth factor receptor-2 (HER2) positive BC accounts for about 15%~20% of the total BC patient numbers, and this type of BC is highly invasive with poor prognosis.3 In recent years, with the development of targeted anti-HER2 therapies, the prognosis of patients with this type of BC has improved significantly. For elderly BC patients with over-expression regarding HER2 gene, there is no direct evidence to support that the benefits and risks regarding the therapies are different from young patients. In this regard, continuous anti-HER2 therapy is needed in the treatments.
As a small molecule anti-HER2-targeting drug that independently developed in China according to national standard, Pyrotinib is an irreversible tyrosine kinase inhibitor, which can inhibit the autophosphorylation by covalently binding to ATP binding sites in intracellular kinases of HER1, HER2 and HER4, thus blocking the activation of downstream signaling pathways to inhibit tumor cell growth.4,5 Pyrotinib has been confirmed to be effective, safe and controllable in previous Phase II clinical studies and large Phase III clinical studies of PHENIX and PHOEBE,6–8 which has become the standard second-line treatment for advanced HER2-positive BC. This study retrospectively analyzed 45 patients aged ≥65 years who were treated with Pyrotinib in Xinjiang, aiming to explore the efficacy and safety of Pyrotinib in treatment for elderly patients with advanced HER2-positive BC and to provide clinical data for applications of Pyrotinib regarding elderly patients in the nation.
Materials and Methods
Objects
This study collected 45 patients with advanced HER2-positive BC aged ≥65 years from eight hospitals, say, Cancer Hospital affiliated to Xinjiang Medical University, Traditional Chinese Medicine Hospital affiliated to Xinjiang Medical University, People’s Hospital of Xinjiang Uygur Autonomous Region, Cancer Hospital of Hami, Bazhou People’s Hospital, Yili Prefecture Friendship Hospital, DuShanZi People’s Hospital and Aksu Regional People’s Hospital. Patients met the inclusion criteria and were treated with Pyrotinib from January 1, 2019 to May 31, 2021. The last time of follow-up was December 31, 2021. Ethics committee in The 3rd Affiliated Teaching Hospital of XinJiang Medical University (Affiliated Tumor Hospital) approved this study (approval no. [2018]05–228-06). We obtained the informed consent from the study participants prior to study commencements. Our study complies with the Declaration of Helsinki.
Inclusion Criteria
i) Stage IV HER2-positive BC patients who were confirmed by histopathology and were postoperative recurrence, metastasis or inoperable at diagnosis (Positive HER2 was defined as immunohistochemistry 3+ or 2+, and FISH indicated gene amplification). ii) Eastern Cooperative Oncology Group (ECOG) Performance Status (PS) ≤2. iii) The expected survival was ≥3 months. iv) Organ function was normal, blood routine and liver and kidney function were normal before treatment, and there was no contraindication. v) There was at least one measurable target lesion according to RECIST1.1 criteria.
Exclusion Criteria
i) Age <65 years old. ii) Prior treatment with Pyrotinib. iii) Treatment information is missing. The screening process is detailed in Figure 1.
 |
Figure 1 Flow diagram of case screening. |
Treatments
All patients received oral Pyrotinib Maleate Tablets (80mg/tablet; AiRuiNi, Jiangsu Hengrui Pharmaceutical Group Co., Ltd.) targeted therapy-combined chemotherapy. The effects were evaluated every 2 cycles (21 days for a cycle). For monotherapy, combined endocrine therapy, or combined with other targeted drugs (except ADC), the efficacy was evaluated every 2 months, and patients were required to return to the hospital for evaluation at any time if disease progression was considered.
Response Evaluation
According to the “RECIST1.1 Response Evaluation Criteria in Solid Tumors”, the efficacy of measurable lesions was evaluated by B-ultrasound, CT, MRI and other examinations. Some evaluation criteria were as follows.
Complete response (CR): All the target lesions disappeared; Partial response (PR): The sum of the length and diameter of the baseline lesions decreased ≥30%.
Stable disease (SD): The sum of the long diameter of the baseline lesions decreased but did not reach PR or increased without reaching PD.
Progressive disease (PD): The sum of the long diameter of baseline lesions increased ≥20% or new lesions appeared.
Indicators
The primary end points were PFS and OS, which were defined as the time from initial treatment of Pyrotinib to confirmation of disease progression confirmed by imaging such as CT/MRI or death from any causes. Secondary endpoints included ORR, CBR, OS, and security. ORR was the proportion of patients with complete response (CR) or partial response (PR), ie, ORR = CR+PR. The disease control rate was the proportion of patients with CR, PR and stable disease (SD), ie CBR = CR+PR+SD. OS was defined as the time from initiation of Pyrotinib therapy to death from any causes or to the last follow-up. According to the National Cancer Institute-Common Terminology Criteria for Adverse Events version 4.0 (NCI-CTC v4.0), the severity of adverse reactions was determined with grade ranging in interval [0, 4].
Follow-Up
As of December 31, 2021, 35 patients had discontinued Pyrotinib treatment with observed PFS, and 10 patients were currently continuing the Pyrotinib regimen.
Statistical Method
SPSS software (version 25.0) was used for statistical analysis. Clinical characteristics of patients were analyzed using descriptive statistics (percentages). The chi-square test was used to compare the recent efficacy. Kaplan–Meier survival curve was plotted, and median survival time along with 95% confidence interval (CI) was calculated. P < 0.05 was considered statistically significant. Survival analysis and visualization were performed by R language (version 4.1.2).
Results
Baseline Characteristics
From January 1, 2019 to May 31, 2021, 45 elderly patients with advanced HER2-positive BC that treated with Pyrotinib were studied. See Table 1 for specific baseline data. The median age was 67 (65~87) years, and 19 patients (42.2%) were positive hormone receptor. There was 1 patient (2.2%) with micropapillary carcinoma. ECOG scores were mainly 1, with 32 cases (71.1%). Eleven patients were initially treated at stage IV, accounting for 24.4%. Visceral metastasis occurred in 38 cases (84.4%). In terms of previous anti-HER2-targeted therapy, 42 patients (93.3%) received previous Trastuzumab treatment in this study. Ten cases (22.2%) received previous Lapatinib treatments, and 6 cases (13.3%) previously received Pertuzumab treatment. Three cases (6.7%) did not receive anti-HER2 therapy (Table 1).
 |
Table 1 Patient Characteristics at Baseline |
Treatment and Dose Adjustment
Twenty-five patients (55.6%) were treated with Pyrotinib at initial standard dose of 400mg/d. Initial dose reduction was given in 20 patients (44.4%). During the whole treatment procedure, there were 21 patients who were treated with dose reduction on the basis of the initial dose, and 11 patients were maintained at the standard dose of 400mg/d accounting for 24.4%. For 16 patients, 320 mg/d was maintained (35.6%). Eighteen patients (40.0%) were maintained at 240mg/d (Table 2).
 |
Table 2 Treatment Administration |
Short-Term Effects
All 45 patients completed efficacy evaluation, including 17 patients (37.8%) with PR; 18 cases (40.0%) with SD; 10 cases (16.7%) with PD. There are 3 patients (6.7%) who received fewer than 2 cycles of Pyrotinib. There are no CR cases. The total ORR of the whole group was 37.8% (17/45). CBR was 77.8% (35/45) (Table 3; Figure 2).
 |
Table 3 Subgroup Analysis Regarding Short-Term Response |
 |
Figure 2 Summary of Pyrotinib-based therapy response in elder HER2-positive metastatic BC patients. |
The ORR of 1–2 line using combined therapy with Pyrotinib was significantly higher than that of therapy ≥3 line (41.7% vs 22.2%), and the CBR of therapy in 1–2 line was significantly higher than that of therapy ≥3 line (80.6% vs 66.7%). The final difference was not statistically significant (P = 0.282, P = 0.370).
In terms of maintenance dose, the standard dose ORR regarding 400mg was higher than that of the reduced dose (45.5% versus 43.8% versus 27.8%), and the CBR standard dose was significantly higher than that of the reduced dose group (81.8% versus 81.3% versus 72.2%). There was no statistical significance between the three groups (P > 0.5).
The ORR and CBR of those aged ≥65 and <70 were 43.3% and 80.0%, which were higher than those of those aged ≥70 (ORR: 26.7%; CBR: 73.3%). There was no significant difference between the two groups (P = 0.277, P = 0.61).
The median follow-up time in present study was 11 months (2–35 months), and 35 (77.8%) and 8 (17.8%) events reached PFS and OS, respectively. The overall median PFS was 6.8 months (95% CI: 5.4–9.8), without reaching the median OS (Figure 3). There were 14 patients with brain metastases (BMs) (31.1%), and the median PFS was 5.8 months (95% CI: 3.6–8.1) (Figure 4). In terms of the number of treatment lines, mPFS for line 1-2 was 8.3 months (95% CI: 6.3~11.4), and mPFS for line ≥3 was 3.3 months (95% CI: 2.7~5.1). Difference between two groups is significant (P = 0.0028) (Figure 5A), inferring that Pyrotinib should also be used as early as possible for elderly patients with advanced HER2-positive BC.
 |
Figure 3 Progression free survival of 45 patients. |
 |
Figure 4 Progression free survival of 14 patients with brain metastasis. |
At the final maintenance dose, mPFS at standard doses of 400mg, 320mg and 240mg were 9.1 months (95% CI: 4.1~9.5), 8.3 months (95% CI: 4.3~12.2) and 4.8 months (95% CI: 2.1~7.5), respectively. mPFS in the standard dose group were longer than those in the reduced dose group, with a statistically significant difference between the three groups (P = 0.025) (Figure 5B).
 |
Figure 5 (A) Progression free survival for the different line. (B) Progression free survival for the different keeping dose. (C) Progression free survival for the different age groups. |
mPFS with age ≥65 and <70 were 8.0 months (95% CI: 5.4~11.4), which were longer than mPFS with age ≥70 years (6.3 months, 95% CI: 3.2~9.4). And there was no statistically significant difference between the two groups (P = 0.23) (Figure 5C).
Toxicity and Adverse Effects
All 45 patients had distinguished degrees of AE, which were mainly within the grade 1–2. The most common adverse event was diarrhea in 40 patients (88.1%) and 5 patients (11.1%) reported grade 3 diarrhea. Grade 3 AE included 3 neutropenia (6.7%), 1 anemia (2.2%), and 1 hand-foot syndrome (2.2%). No grade 4 AE was observed (Table 4).
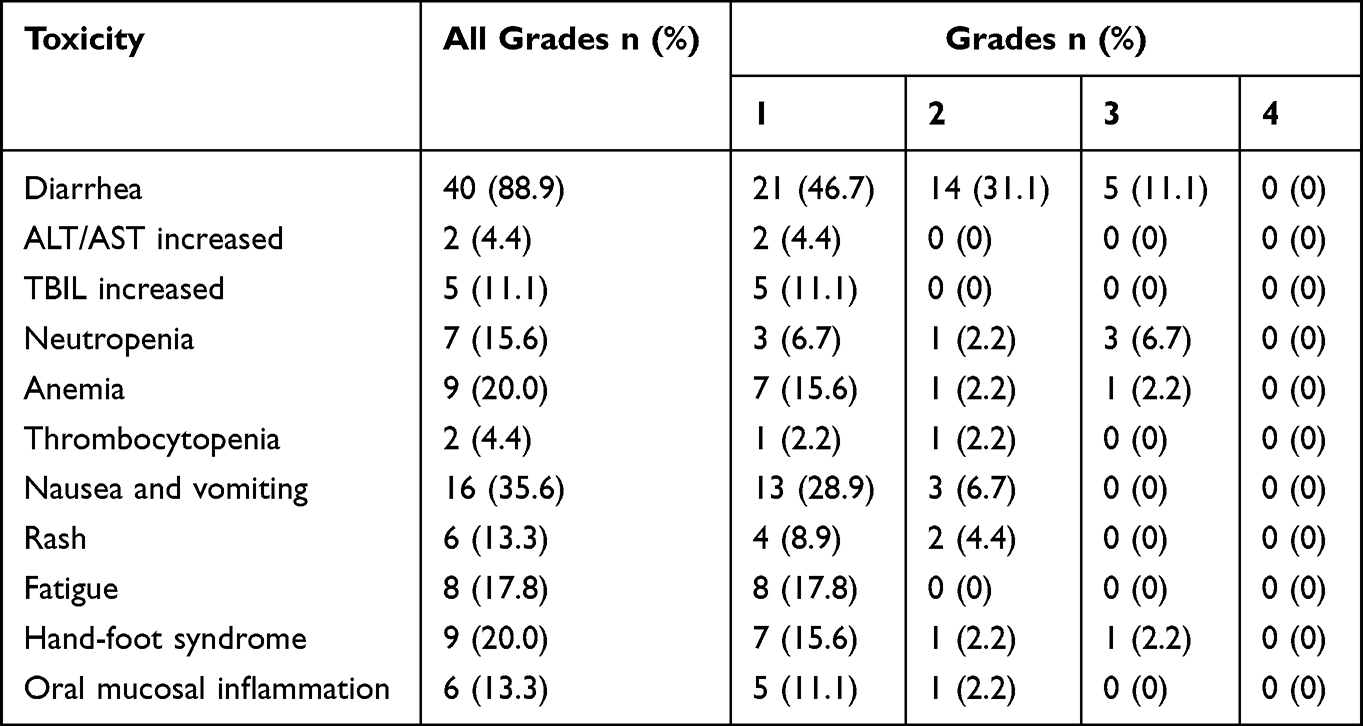 |
Table 4 Treatment-Related Toxicities of 26 Patients |
Discussion
BC is the most common malignant tumor amongst females, which is the main cause of cancer mortality for women under 60 years old and is the second leading cause of death in women over 60 years old.9 Previous data showcase that the incidence of elderly patients is increasing year by year, and the advanced the age, the worse the survival outcome.10 But in practice, as patients get older, the motivation for treatment is significantly affected. According to the report,11 22% of elderly solid tumor patients over 70 years old did not receive anti-tumor therapy, while 12% of the patients between 60 and 69 years old did not receive anti-tumor therapy. HER2-positive patients with advanced BC have poorer prognosis and shorter survival time than other BC patients. Without treatment against HER2, only 13.2% of BC patients survived more than 5 years.12 However, in prospective clinical studies exploring anti-HER2 therapy, the proportion of enrolled elderly patients was significantly insufficient, so it is impossible to draw absolute conclusions about its clinical application.
Pyrotinib was a small molecule anti-HER2-targeting drug that developed in China, which was recommended for second-line treatment of advanced HER2-positive BC based upon Class 2A evidence in the Guidelines of Chinese Society of Clinical Oncology (CSCO) on Diagnosis and Treatment of Breast Cancer (2019 version). In present investigation, 21 patients (46.7%) were treated with Pyrotinib. Elderly patients with advanced BC may have more concerns regarding the intravenous chemotherapy treatments because of their chronic underlying diseases. Tyrosine kinase inhibitors (TKI) have advantages of oral administration and low cardiotoxicity,13 which are more acceptable for elderly patients. About 44.4% of the patients received varying degrees of reduction in the initial dose, and most of the patients were over 70 years old or with underlying diseases such as hypertension, diabetes, coronary heart disease, etc. Even patients who were given 400 mg initially were given different levels of reduction during later treatment because they could not tolerate side effects (mainly diarrhea), and only 24.4% of patients ended up with maintaining the therapeutic dose of 400 mg.
In this study, we observed that the ORR of the whole group was 37.8% (17/45); CBR was 77.8% (35/45), mPFS was 6.8 months (95% CI: 5.4–9.8), which were lower than the results achieved in clinical studies regarding Phase II–III Pyrotinib.6–8 In the current study, 42 patients accounting for 93.3% were previously treated with Trastuzumab. In Pyrotinib Phase II study, 53.8% of the patients had received Trastuzumab during adjuvant therapy or metastasis. The median age of the PHOEBE study was 50 years (42–55), where elderly patients were not included. In addition, 84.4% (38/45) patients in our study had visceral metastasis, which was higher than the proportion in previous clinical studies indicating that the patients had relatively heavy tumor load. Nevertheless, Pyrotinib achieved mPFS of 6.8 months, which further suggested the effectiveness of Pyrotinib for elderly patients. In our study, we observed that mPFS ≤2 lines of pyrotinib were significantly better than mPFS ≥3 lines of pyrotinib (8.3 vs 3.3 months, p = 0.0028). This suggests that pyrotinib should be applied as early as possible for elder women with HER2-positive advanced breast cancer.
In the subgroup analysis, the standard dose of 400mg mPFS was longer than that in the reduction group (9.1 vs 8.3 vs 4.8 months), and the difference among the three groups was statistically significant (P = 0.025). This indicates that the efficacy is dose-dependent, and the standard dose has the best efficacy. However, we can also see from the data that the maintenance dose of 240 mg achieved mPFS of 4.8 months.
In addition, for elderly patients with advanced HER2-positive BC, we observed that mPFS of patients that treated with Pyrotinib of lines ≤2 were significantly better than that of patients treated with Pyrotinib ≥3 lines (8.3 vs 3.3 months, P = 0.0028), inferring that Pyrotinib should also be used as early as possible for elderly patients with advanced HER2-positive BC.
In the era of Trastuzumab-based treatment, about 30–50% of patients with HER2-positive advanced BC will suffer from BMs,14–16 resulting in poor prognosis. At present, the treatment of BMs is still dominated by local treatment methods, including surgical resection, stereotactic radiotherapy and whole-brain radiotherapy.17,18 However, the recurrence rate is high within 6–12 months post local treatment, and adverse reactions such as cognitive decline may occur.19 Other studies have found that radiotherapy can damage the blood–brain barrier, so the concentration of some drugs for BM is higher than that in other brain tissues, which are not enough to reach the level of cytotoxicity,20 thus affecting the efficacy. Compared with traditional large-molecule anti-HER2 monoclonal antibodies, small-molecule TKIs have been proved to have better blood–brain barrier permeability and clear anti-intracranial tumor activity.21,22 Other TKIs are available for brain metastases, in particular tucatinib as per the HER2 Climb trial, but neratinib/capecitabine also showed a good ORR in the CNS. Lapatinib could also be mentioned although less commonly used now. Results of PERMEATA23 showcased that for HER2-positive BC BM, Pyrotinib combined with capecitabine could effectively control intracranial and extracranial lesions, especially for patients who had not received previous local craniocerebral radiotherapy, with mPFS of 11.3 months (95% CI: 7.7–14.6). In our study, 14 elderly patients with BM (31.1%) had a median PFS of 5.8 months (95% CI: 3.6–8.1), saying that Pyrotinib may provide a systemic treatment option for patients who need to postpone local therapy. In this regard, data from our small study can be considered supportive to the clinical trial data from PERMEATE.
In terms of toxic and side effects, although all the 45 patients showed varying degrees of AE, they were mainly at grade 1–2, and no grade 4 AE was observed. Diarrhea was the most common adverse event, accounting for 88.9%, with grade 3 diarrhea in 5 patients (11.1%). This result is consistent with previous clinical studies7,8 since diarrhea is characterized by high frequency of early occurrence and recovery, etc. While the sample size is small (45), this might be a limit of current study. Most diarrhea is reversible through suspension of medication or reduction of drug dose and symptomatic treatment. In addition to diarrhea, nausea and vomiting were the second most common adverse reactions in this study, accounting for 35.6% (16/45). In addition to diarrhea, grade 3 AE was hematologic toxicity, with 3 cases of neutropenia (6.7%) and 1 case of anemia (2.2%). Hematologic toxicity mainly occurred in patients that treated with Pyrotinib in combination with CDK4/6. In general, Pyrotinib is safe for elderly patients without drug withdrawal due to diarrhea or other adverse reactions.
Conclusion
In clinical practice for elderly (aged ≥65 years) HER2-positive BC patients in Xinjiang, we found that Pyrotinib was safe and effective as a small molecule targeting drug against HER2. For elderly patients, 240 mg is an acceptable maintenance dose. 240 mg is an alternative therapeutic dose for elderly patients where the standard dose of pyrotinib could not be tolerated in the assessment of poor general conditions. Certainly, there are still some deficiencies in current investigation. Firstly, the sample size of the study is small, and clinical studies are unmet to verify our findings. Secondly, this study is retrospective rather than prospective, and there are selection and information bias. Thirdly, it is a retrospective rather than a prospective study, and there are selection and information biases. Since the study was a retrospective study and part of the information was obtained through telephone follow-up, the AE analysis would be subjective to a certain extent. The sample size of this study is moderate, and we look forward to future clinical studies with larger samples to verify our findings.
Acknowledgment
This study was supported by Youth Scientific and Technological Innovation Talents Training Project of Xinjiang Uyghur autonomous region (grant no. QN2016YX0274). We would like to express gratitude to anonymous reviewers’ comments, which help us improve this presentation.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Li N, Zheng SR, Zhang SW, et al. Analysis and prediction of breast cancer incidence trend in China. Chin J Preventive Med. 2012;46(8):703–707.
3. Waks AG, Winer EP. Breast cancer treatment. JAMA. 2019;321(3):288. doi:10.1001/jama.2018.19323
4. Ma F, Li Q, Chen S, et al. Phase I study and biomarker analysis of pyrotinib, a novel irreversible pan-ErbB receptor tyrosine kinase inhibitor, in patients with human epidermal growth factor receptor 2-positive metastatic breast cancer. J Clin Oncol. 2017;35(27):3105–3112. doi:10.1200/JCO.2016.69.6179
5. Li Q, Guan X, Chen S, et al. Safety, efficacy, and biomarker analysis of pyrotinib in combination with capecitabine in HER2 positive metastatic breast cancer patients: a phase I clinical trial. Clin Cancer Res. 2019;25(17):5212–5220. doi:10.1158/1078-0432.CCR-18-4173
6. Ma F, Ouyan Q, LI W, et al. Pyrotinib or lapatinib combined with capecitabine in HER2-positive metastatic breast cancer with prior taxanes, anthracyclines, and/or trastuzumab: a randomized phase II Study. J Clin Oncol. 2019;37(29):2610–2619. doi:10.1200/JCO.19.00108
7. Yan M, Bian L, Hu X, et al. Pyrotinib plus capecitabine for human epidermal growth factor receptor 2-positive metastatic breast cancer after trastuzumab and taxanes (PHENIX): a randomized double-blind placebo-controlled Phase 3 study. Transl Breast Cancer Res. 2020;1:13. doi:10.21037/tbcr-20-25
8. Xu B, Yan M, Ma F, et al. Pyrotinib plus capecitabine versus lapatinib plus capecitabine for the treatment of HER2-positive metastatic breast cancer (PHOEBE): a multicenter, open-label, randomized, controlled phase 3 trial. Lancet Oncol. 2021;22(3):351–360. doi:10.1016/S1470-2045(20)30702-6
9. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7–30. doi:10.3322/caac.21590
10. Soto-Perez-de-Celis E, Li D, Yuan Y, et al. Functional versus chronological age: geriatric assessments to guide decision making in older patients with cancer. Lancet Oncol. 2018;19(6):e305–e316. doi:10.1016/S1470-2045(18)30348-6
11. Won HS, Lee KE, Sung SH, et al. Topoisomerase II alpha and microtubule associated protein-tau as a predictive marker in axillary lymph node positive breast cancer. Tumori. 2014;100(1):80–86. doi:10.1177/1430.15820
12. Blair HA. Pyrotinib: first global approval. Drugs. 2018;78(16):1751–1755. doi:10.1007/s40265-018-0997-0
13. Jun-cheng Xuhong XQ. Mechanism, safety and efficacy of three tyrosine kinase inhibitors lapatinib, neratinib and pyrotinib in HER2-positive breast cancer. Am J Cancer Res. 2019;9(10):2103–2119.
14. Gori S, Rimondini S, De Angelis V, et al. Central nervous system metastases in HER2 positive metastatic breast cancer patients treated with trastuzumab: incidence, survival, and risk factors. Oncologist. 2007;12(7):766–773. doi:10.1634/theoncologist.12-7-766
15. Brufsky AM, Mayer M, Rugo HS, et al. Central nervous system metastases in patients with HER2 positive metastatic breast cancer: incidence, treatment, and survival in patients from registHER. Clin Cancer Res. 2011;17(14):4834–4843. doi:10.1158/1078-0432.CCR-10-2962
16. Olson EM, Najita JS, Sohl J, et al. Clinical outcomes and treatment practice patterns of patients with HER2-positive metastatic breast cancer in the post-trastuzumab era. Breast. 2013;22(4):525–531. doi:10.1016/j.breast.2012.12.006
17. Ramakrishna N, Temin S, Chandarlapaty S, et al. Recommendations on disease management for patients with advanced human epidermal growth factor receptor 2–positive breast cancer and brain metastases: ASCO clinical practice guideline update. J Clin Oncol. 2018;36(27):2804–2807. doi:10.1200/JCO.2018.79.2713
18. Cardoso F, Paluch-Shimon S, Senkus E, et al. 5th ESO-ESMO international consensus guidelines for advanced breast cancer (ABC 5). Ann Oncol. 2020;31(12):1623–1649. doi:10.1016/j.annonc.2020.09.010
19. Tanguturi S, Warren L. The current and evolving role of radiation therapy for central nervous system metastases from breast cancer. Curr Oncol Rep. 2019;21(6):50. doi:10.1007/s11912-019-0803-5
20. Brosnan EM, Anders CK. Understanding patterns of brain metastasis in breast cancer and designing rational therapeutic strategies. Ann Transl Med. 2018;6(9):163. doi:10.21037/atm.2018.04.35
21. Sullivan O, Davarpanah NN, Abraham J, et al. Current challenges in the management of breast cancer brain metastases. Semin Oncol. 2017;44(2):85–100. doi:10.1053/j.seminoncol.2017.06.006
22. Garcia-Alvarez A, Papakonstantinou A, Oliveira M. Brain metastases in HER2-positive breast cancer: current and novel treatment strategies. Cancers. 2021;13(12):2927. doi:10.3390/cancers13122927
23. Yan M, Ouyang Q, Sun T, et al. Pyrotinib plus capecitabine for patients with human epidermal growth factor receptor 2-positive breast cancer and brain metastases (PERMEATE): a multicentre, single-arm, two-cohort, Phase 2 trial. Lancet Oncol. 2022;23(3):353–361. doi:10.1016/S1470-2045(21)00716-6
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Safety of Pyrotinib in Human Epidermal Growth Factor Receptor 2-Positive Advanced Breast Cancer: A Multicenter, Retrospective, Real-World Study
Zhang X, Li Z, Han L, Lv Z, Teng Y, Cui X, Zhou C, Wu H, Fang W, Xu L, Zhao S, Song C, Zheng Y, Gao T, Li M
OncoTargets and Therapy 2022, 15:1067-1078
Published Date: 28 September 2022
Real-World Outcome and Prognostic Factors Among HER2-Positive Metastatic Breast Cancer Patients Receiving Pyrotinib-Based Therapy: A Multicenter Retrospective Analysis
Liu J, Sun X, Du Q, Yao J, Dai M, Cheng Q, Xu H, Li Y, Liu X, Zhang M, Zhou Y, Yang Y
Breast Cancer: Targets and Therapy 2022, 14:491-504
Published Date: 21 December 2022
The Combined Effect of Nanobubble-IR783-HPPH-Affibody Complex and Laser on HER2-Positive Breast Cancer
Cai W, Lv W, Meng L, Duan Y, Zhang L
International Journal of Nanomedicine 2023, 18:339-351
Published Date: 19 January 2023
Invasive Breast Cancer with HER2 ≥4.0 and <6.0: Risk Classification and Molecular Typing by a 21-Gene Expression Assay and MammaPrint Plus BluePrint Testing

Bai Q, Lv H, Bao L, Yang Y, Zhang X, Chang H, Xue T, Ren M, Zhu X, Zhou X, Yang W
Breast Cancer: Targets and Therapy 2023, 15:563-575
Published Date: 3 August 2023
A Structured Classification of Pyrotinib-Containing Neoadjuvant Regimens for HER2-Positive Breast Cancer: Efficacy, Safety, and Regimen Selection
Liu J, Peng X, Yang Y, Huang X, Du Y, Liu K
Breast Cancer: Targets and Therapy 2026, 18:600575
Published Date: 20 May 2026