Back to Journals » Journal of Inflammation Research » Volume 19
A Predictive Nomogram for Severe RSV Infection in Children: A Retrospective, Single-Center Development and Validation Study
Authors Li W, Wang S, Wang X, Niu X, Guo Y, Zou Y
Received 20 November 2025
Accepted for publication 21 March 2026
Published 12 April 2026 Volume 2026:19 580432
DOI https://doi.org/10.2147/JIR.S580432
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Tara Strutt
Wanyi Li,1,* Shuying Wang,2,* Xuelin Wang,1,* Xiaoyin Niu,1 Yongsheng Guo,1 Yingxue Zou1
1Children’s Hospital, Tianjin University/Tianjin Children’s Hospital, Tianjin, People’s Republic of China; 2Department of Pediatrics, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yingxue Zou, Children’s Hospital, Tianjin University/Tianjin Children’s Hospital, Tianjin, People’s Republic of China, Email [email protected]
Background: Respiratory syncytial virus (RSV) is a leading cause of severe lower respiratory tract infections in children, and early identification of high-risk patients is critical for improving outcomes. This study aimed to retrospectively study the clinical factors of children with severe RSV infection and, on this basis, develop and verify the nomogram model to identify independent risk factors for early prediction of children with severe RSV infection.
Methods: This study retrospectively analyzed the clinical characteristics of children diagnosed with respiratory syncytial virus infection and divided the children into a severe group and a non-severe group. Based on five multiply imputed datasets, variable selection was performed using Elastic Net regression combined with clinical knowledge, and a multivariable logistic regression model was constructed. Internal validation was conducted using 500 bootstrap resamples to obtain optimism-corrected AUC and calibration slope, which was subsequently applied as a shrinkage factor to adjust regression coefficients for overfitting.
Results: Of the 2595 children, 160 were in the severe group and 2435 were in the non-severe group. Five predictors were retained in the final model: Neutrophil-to-Lymphocyte Ratio (NLR), age, winter onset, hypoxemia, and preterm. The pooled area under the ROC curve was 0.847 (95% CI: 0.833– 0.860), and the optimism-corrected AUC after bootstrap validation was 0.843. The calibration slope was 0.975, indicating low overfitting risk after shrinkage correction.
Conclusion: A nomogram incorporating five predictors (NLR, age, winter onset, hypoxemia, and preterm) was developed to predict severe RSV infection in children. Bootstrap internal validation showed good discrimination and indicated low overfitting. This tool can assist clinicians in timely identifying high-risk patients for early intervention.
Keywords: respiratory syncytial virus, children, risk factors, nomogram, predicting
Introduction
Background and Clinical Burden
Respiratory syncytial virus (RSV) is the leading cause of acute lower respiratory tract infections and hospitalizations in children under 18 years of age worldwide, especially in infants.1,2 RSV is an enveloped virus possessing a non-segmented, single-stranded, negative-sense RNA genome, which places it taxonomically within the Pneumoviridae family. Its surface fusion protein (F protein) and adhesion protein (G protein) are the core antigens that mediate the virus’s invasion of host cells. RSV is categorized into two primary subtypes, A and B, based on genetic and antigenic disparities, which can be prevalent at the same time. Infections caused by subtype A often result in more severe clinical manifestations.3 According to relevant epidemiological data, RSV infections exhibit distinct patterns in terms of age of onset and seasonal distribution. Most children experience at least one RSV infection before the age of two,4 this virus is also one of the leading causes of child mortality worldwide. Studies indicate that at least one in every 28 deaths among infants aged 0 to 6 months is associated with RSV infection.5,6 The manifestations of RSV infection are highly variable, with significant heterogeneity in disease severity observed across different patient populations, particularly between infants and older adults. Most children initially present with cold-like symptoms, including nasal congestion, runny nose, cough, fever, and sore throat. Some children, especially infants and young children who are infected with the RSV virus for the first time, are characterized by wheezing, shortness of breath, nasal flaring, and three concave signs. In severe cases, they are also accompanied by cyanosis, hypoxia, and respiratory failure, which can easily lead to bronchiolitis and pneumonia.
RSV infection is a self-limiting process, and healthy full-term infants without underlying diseases usually recover on their own within 1–2 weeks. However, for some high-risk groups, such as premature infants and children with congenital heart disease, bronchopulmonary dysplasia, immune deficiency, or neurological diseases, the condition is more serious, and they even need to enter the pediatric intensive care unit (PICU) for respiratory support treatment.7 A large number of evidence-based medical studies have shown that severe RSV bronchiolitis in infancy is an independent risk factor for subsequent recurrent wheezing and childhood asthma.8,9 Therefore, early identification and intervention of children with severe RSV infection are important for decreasing the mortality rate and complications and raising the prognosis of children.
Current Assessment and Predictive Tools
To scientifically assess pediatric patients’ conditions and enable group comparisons, this study employs the internationally validated Wang’s Score (Wang’s Bronchiolitis Severity Score) as its core quantitative tool.10 The scoring system provides an objective and quantitative assessment of disease severity through four key dimensions: respiratory rate, wheezing characteristics, chest wall retractions, and general condition (specific grading and scoring criteria are detailed in Table 1, with a higher total score indicating greater severity). Based on the total score, patients were categorized into three severity groups: mild (0–3 points), moderate (4–8 points), and severe (9–12 points).11 For this study, patients with a score ≥ 9, classified as “severe”, constituted the case group for severe RSV infection. Currently, although the Wang’s Score is used for disease assessment, no studies have developed a risk prediction model for severe RSV infection in children based on this scoring system. Therefore, this study aims to retrospectively analyze the clinical characteristics of children with severe RSV infection and, based on this analysis, develop and validate a nomogram prediction model. This approach seeks to enable early risk identification, guide intervention, ultimately improve patient outcomes, and reduce the incidence of complications.
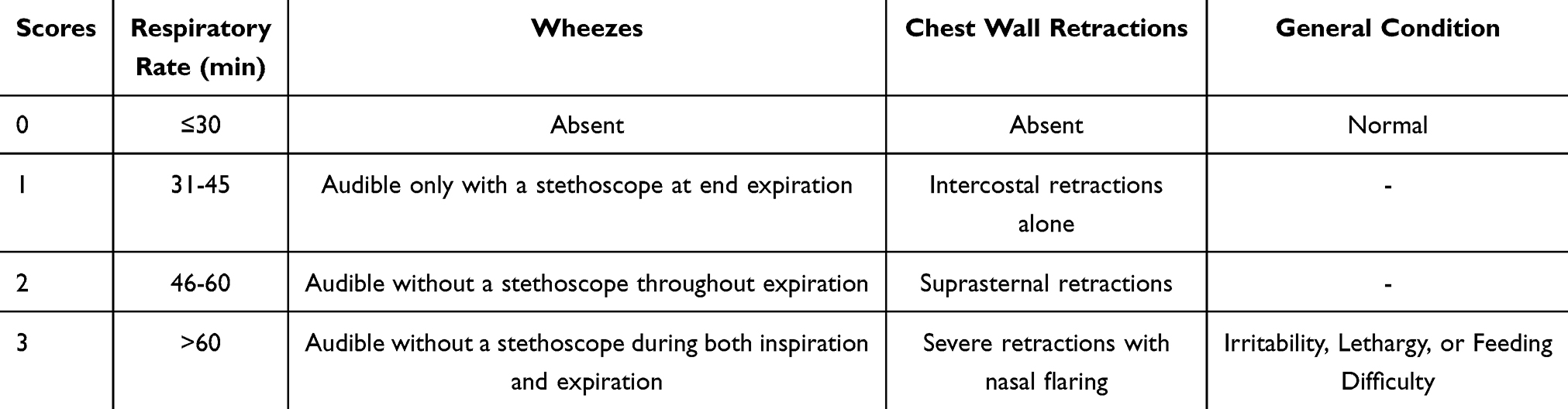 |
Table 1 Wang’s Severity Score (Clinical Severity Score for Bronchiolitis) |
Objective of the Study
This study aimed to develop and internally validate a nomogram prediction model for severe RSV infection in children, as defined by Wang’s Score. To overcome the overfitting inherent in traditional methods when applied to retrospective data, we employed high-dimensional data analysis techniques, including Elastic Net regression on multiply imputed datasets, to identify stable predictors from a large pool of clinical candidate variables. Our ultimate goal was to create a statistically robust and clinically interpretable tool to facilitate the early identification of children at high risk for severe RSV infection.
Methods
Data Source and Study Participants
This study adopted a single-center retrospective study design, and included children with RSV infection who were hospitalized in Tianjin Children’s Hospital (Children’s Hospital of Tianjin University) from January 1, 2022 to August 10, 2024 as the research objects. The clinical data of the children were collected comprehensively thru the electronic medical record system of Tianjin Children’s Hospital, including: (1). Basic demographic characteristics of children: name, gender, age, season of admission, whether premature, birth weight, feeding method, total course of disease, length of stay; (2). Clinical manifestations at admission: days of fever, wheezing, cough, three concave signs, cyanosis, hypoxemia, combined with other infections; (3). Assessment of the severity of the disease: The severity of illness at admission was objectively graded using the internationally validated Wang’s Score. This scoring system assesses four clinical domains: respiratory rate, characteristics of wheezing, chest wall retractions, and general condition. The detailed scoring criteria for each domain are presented in Table 1. The scores from each domain are summed to yield a total score ranging from 0 to 12, with a higher score indicating greater severity. To ensure consistency and objectivity in the assessment, two investigators who received unified training independently reviewed each patient’s admission records (including clinical notes and findings from the initial physical examination) and assigned scores according to the criteria in Table 1. Any discrepancy between the two assessors was resolved through discussion and joint re-evaluation of the case materials. If consensus could not be reached, a third senior clinical researcher was consulted for arbitration to determine the final score. Based on the finalized total score, patients were categorized into three groups: mild (0–3 points), moderate (4–8 points), and severe (9–12 points). For this study, patients in the severe group (Wang Score ≥ 9) were defined as having severe RSV infection and constituted the case group for predictive model development; (4). Laboratory tests: White Blood Cell (WBC), Neutrophil Percentage (N%), Lymphocyte Percentage (L%), Neutrophil-to-Lymphocyte Ratio (NLR), Hemoglobin (Hb), Platelet (PLT), C-Reactive Protein (CRP), Erythrocyte Sedimentation Rate (ESR), Ferritin (FER), Procalcitonin (PCT), Interleukin-6 (IL-6), Alanine Aminotransferase (ALT), Alkaline Phosphatase (ALP), Aspartate Aminotransferase (AST), Gamma-Glutamyl Transferase (γ-GT), Total Protein (TP), Albumin (ALB), Globulin (GLO), Lactic Acid (La), Glucose (GLU), Total Bilirubin (TBil), Direct Bilirubin (DBil), Indirect Bilirubin (IBil), Lactate Dehydrogenase (LDH), Creatine Kinase (CK), Creatine Kinase-Myocardial Band (CK-MB), Serum Creatinine (Cr), Blood Urea Nitrogen (BUN), Immunoglobulin G (IgG), Immunoglobulin A (IgA), Immunoglobulin M (IgM), Immunoglobulin E (IgE), Potential of Hydrogen (PH), Arterial Oxygen Partial Pressure (PaO2), Arterial Carbon Dioxide Partial Pressure (PaCO2), Arterial Oxygen Saturation (SaO2), Bicarbonate (HCO3-), Total Carbon Dioxide Content (TCO2). All predictor variables (including laboratory measures) were based on specimens collected or clinical assessments performed on the day of admission (Day 1).
Inclusion criteria: (1). Age less than 18 years; (2). Diagnosed with RSV infection, the etiological basis meets the RSV positive and/or nucleic acid positive confirmed by nasopharyngeal swab specimen detection; (3). The patient’s clinical medical record data is complete and available for inspection; Exclusion criteria: (1). Patients having key clinical variables with >20% missing values; (2). Patients with major underlying diseases that seriously affect respiratory function, such as severe congenital heart disease, bronchopulmonary dysplasia, congenital airway malformation, severe neurological diseases, and immunodeficiency diseases.
The laboratory data for this study were all extracted from the hospital information system. Since this is a retrospective study, some specific technical details of the tests (such as the brand of specific kits, the type of sample collection tubes, etc.) could not be fully traced in the original records. To ensure data reliability, we conducted strict quality control: a) all data came from the laboratory of the same center, following standardized operating procedures; b) only records with clear test results and reference ranges were included; c) abnormal results were re-checked.
Statistical Analysis
In this study, statistical software such as SPSS (version 25.0) were used to statistically analyze the research data. The clinical data of the children were classified into categorical variables and continuous variables. Categorical variables were described using frequency (percentage), and the chi-square test was used for comparison between groups. Prior to parametric testing, the distribution of continuous variables was evaluated for normality with the Kolmogorov–Smirnov test. Following a normal distribution, continuous variables were described as mean ± standard deviation (SD) and independent sample t-tests were used for intergroup comparisons; variables that did not follow a normal distribution were expressed as median (interquartile range), and intergroup differences were assessed using the Mann–Whitney U-test. All continuous predictor variables in this study, including LDH (U/L), CK (U/L), and ESR (mm/hr), were included in the analysis using their clinically reported original measurement units and original scales.
Missing Value Treatment
This study used the multiple chained equations imputation method to handle missing values in the baseline data.12 Using the MICE Data module from the statsmodels library (version 0.14.3) in Python (version 3.9), five complete datasets were generated. During the imputation process, 10 burn-in iterations and 5 iterations between groups were set, and k-nearest neighbors predictive mean matching was used for the imputation. This method effectively preserved the data distribution characteristics of the original variables.
Variable Selection
To identify stable predictors from high-dimensional clinical indicators, this study implemented variable selection based on multiple interpolated datasets. First, Elastic Net Regression with 5-fold cross-validation was run on each interpolated dataset. Parameter settings included: l1_ratios = [0.5, 0.7, 0.9, 0.95, 0.99] to enhance sparse solution search; regularization parameter C was grid-searched within the range 10−4 to 100.5. Subsequently, the frequency of each variable being selected across the five interpolation models was calculated. Only variables with the highest selection frequency were retained for the candidate list (see Appendix for variable occurrence frequencies). Among the variables with the highest frequency rankings, we combined clinical a priori knowledge with validated indicators from prior literature to ultimately select five highly clinically interpretable predictors: NLR, Age, Winter Onset, Hypoxemia, Preterm Infant. Additionally, multicollinearity tests were performed on each of the five datasets. Subsequently, a final predictive model was constructed using conventional logistic regression. To ensure numerical stability and convergence of the algorithm, all continuous variables underwent standardization prior to entering the model. The results from the five interpolated models were combined according to Rubin’s Rules to comprehensively account for both intra- and inter-dataset variability. This process yielded the combined regression coefficients (β), odds ratios (OR), and their 95% confidence intervals (CI). Both variable selection and final modeling were performed using the scikit-learn library (version 1.5.1).
Model Performance Assessment
This study comprehensively assesses model performance in terms of both discrimination and calibration. Discrimination is quantified using the area under the receiver operating characteristic curve (AUC). Calibration is evaluated using calibration curves and the Brier score. To test the model’s generalizability and correct for overfitting, internal validation is performed using the bootstrap method. By performing 500 bootstrap resamples with replacement, the differences in model performance between the original sample and the bootstrap validation samples are calculated, and the optimism-corrected AUC is computed to obtain a bias-corrected performance estimate. To further enhance the clinical applicability and robustness of the model, this study applied heuristic shrinkage estimation to adjust the model coefficients. Specifically, the average calibration slope obtained from the previously mentioned bootstrap validation was used as the shrinkage factor to perform global shrinkage on the coefficients of the initial logistic regression model. Subsequently, the shrunken standardized coefficients were transformed back to the original clinical scale to preserve the direct interpretability of the variables. Finally, a clinical nomogram was constructed based on the adjusted coefficients, enabling individualized and visualized prediction of the risk of severe respiratory syncytial virus infection in children by integrating the weighted scores of each predictive variable.
This study is reported in accordance with the RECORD (REporting of studies Conducted using Observational Routinely-collected health Data) guidelines.
Results
After selection based on inclusion and exclusion criteria, a total of 2595 inpatients were included in this single-center study. After two researchers independently evaluated the condition of the admitted patients, with any discrepancies resolved through discussion, 2435 patients were evaluated as having a mild- moderate infection, and 160 patients were evaluated as having a severe infection. The demographic and clinical characteristics of patients were collected on the day of admission and analyzed for differences. The detailed results Therefore, this study aims to retrospectively analyze the clinical characteristics of children with severe RSV are shown in Table 2. In the mild- moderate group, there were 1396 males and 1039 females, with a median age of 12 months; in the severe group, there were 97 males and 63 females, with a median age of 3 months. There was no statistically significant difference in gender, birth weight, and cough between the two groups (p>0.05). There was a statistically significant difference in age, season of admission, premature infant, feeding pattern, length of hospital stay, duration of illness, duration of fever, wheezing, retractions, cyanosis, hypoxemia, and combined bacterial infection between the two groups (p<0.05).
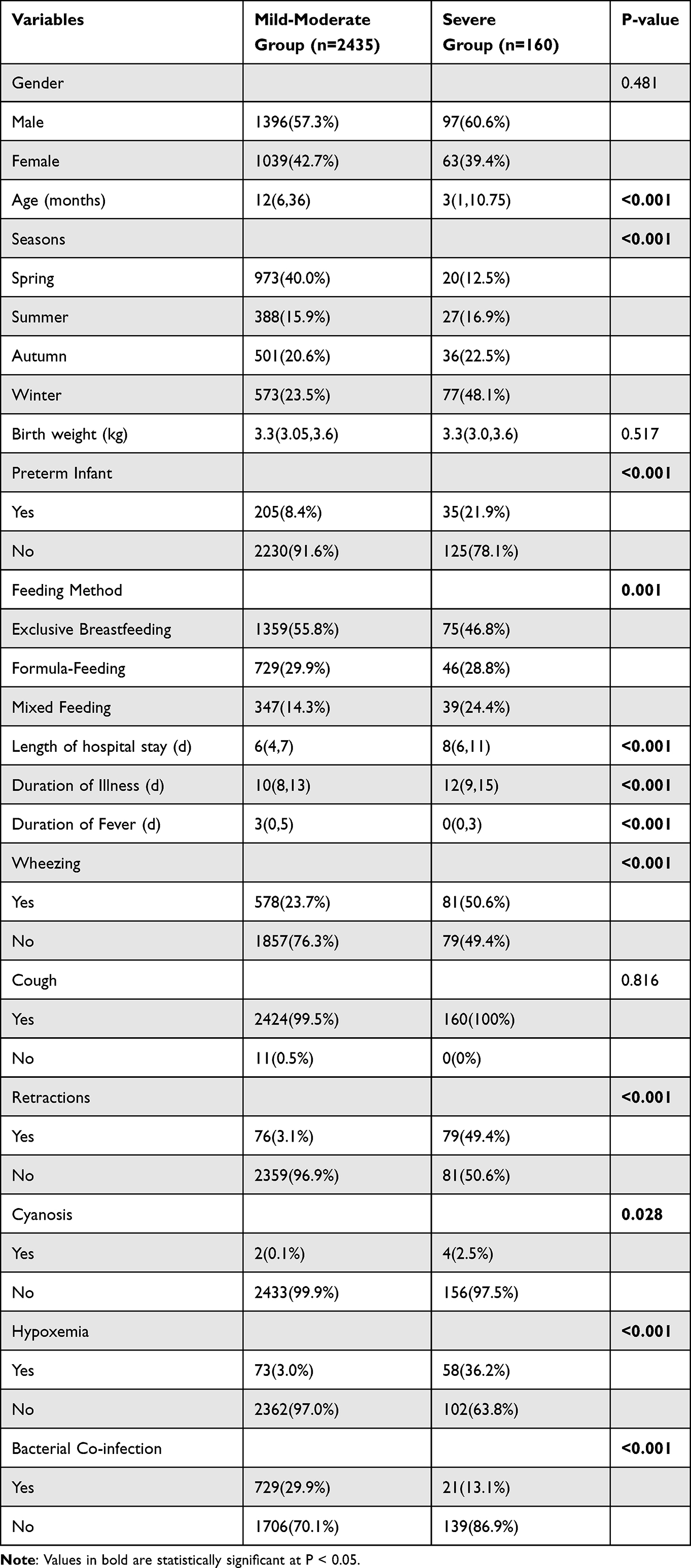 |
Table 2 Characteristics of Demographic and Clinical Presentation on Admission in Children with RSV Infection |
According to the clinical indicators of patients on the day of admission collected by the electronic medical record system of Tianjin, after excluding the samples with a large amount of missing data, the samples with a small amount of missing data were cleaned and the blanks were supplemented by multiple imputation method,13 and then statistical analysis was carried out. The specific results are shown in Table 3. In the comparison of various laboratory indicators, the difference in WBC, N%, L%, NLR, Hb, PLT, CRP, ESR, FER, PCT, ALT, ALP, γ-GT, ALB, GLO, GLU, TBil, DBil, IBil, LDH, CK, CK-MB, Cr, BUN, IgG, IgA, IgM, IgE, PH, PaO2, PaCO2, SaO2, HCO3-and TCO2 levels differed significantly between the severe and mild-moderate groups (p < 0.05). In contrast, the levels of IL-6, AST, TP, and La showed no significant differences between the two groups (p > 0.05).
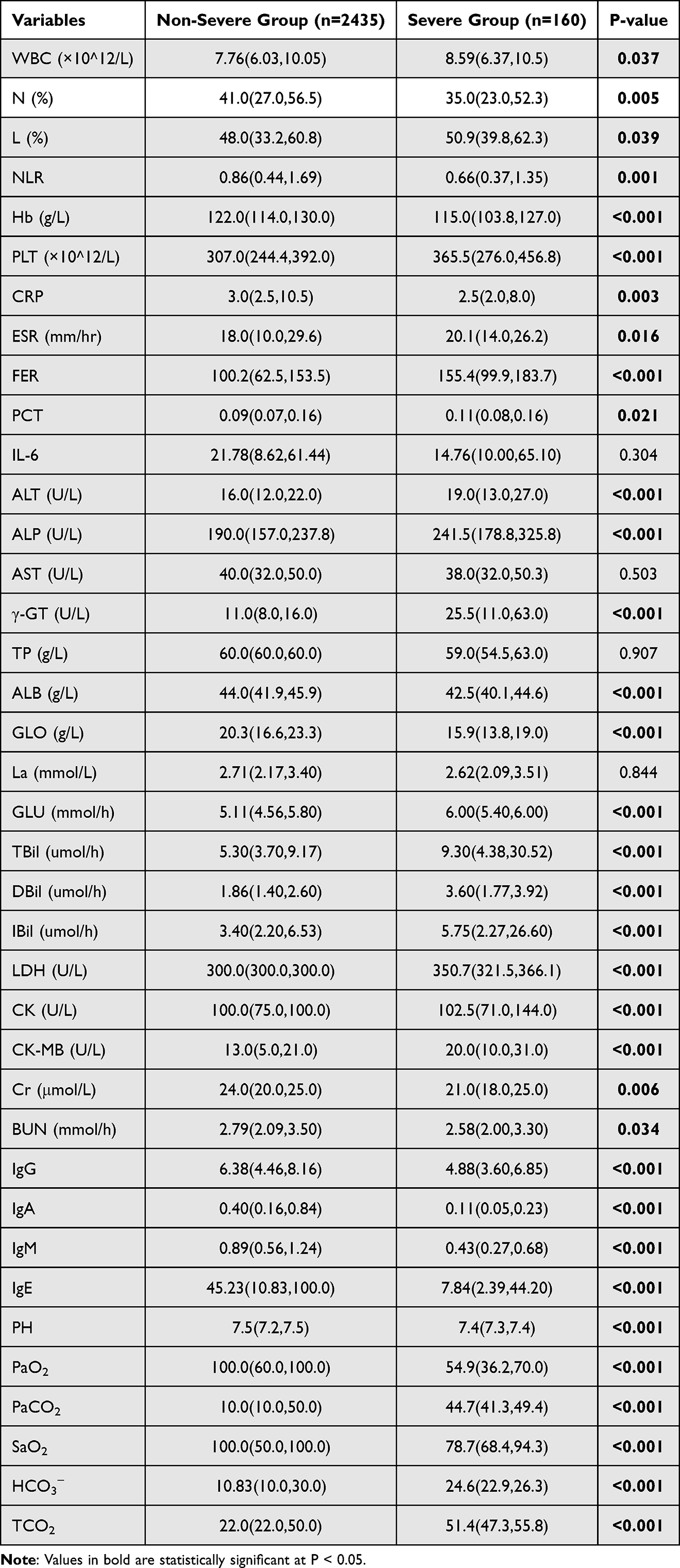 |
Table 3 Comparison of Laboratory Parameters in Children with RSV Infection |
This study conducted multicollinearity tests based on five multiple imputed datasets. The average variance inflation factor (VIF) of each predictor variable across all datasets was calculated, and the results showed that they were all within an acceptable range, indicating no severe multicollinearity (see the supplementary table 1 of additional file for details). The study first preliminarily screened candidate features associated with severe RSV infection in children through elastic net regression, along with their frequency across the five datasets (see the supplementary table 2 of additional file). Ultimately, the model incorporated six predictor variables: NLR, Duration of Illness, Age, Winter Onset, Hypoxemia, and Preterm Infant. Based on these variables, we constructed a nomogram for assessing the severity of pediatric RSV infection, as shown in Figure 1.
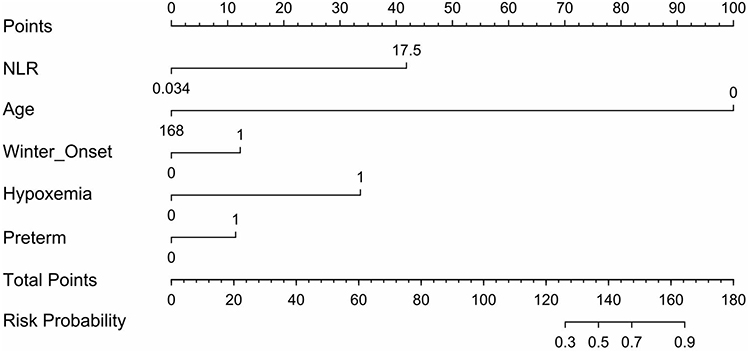 |
Figure 1 Nomogram model for predicting severe RSV infection. |
The overall significance of the combined model was evaluated using the Wald test, and the results indicated that the model was statistically significant (Wald χ 2 = 232.273, P < 0.01). The model demonstrated good discriminative ability, with the pooled area under the receiver operating characteristic curve (AUC) of 0.847 (95% CI: 0.833–0.860) (as shown in Figure 2). To assess internal model stability, we performed 500 Bootstrap samples across five interpolated datasets, yielding an optimism-corrected AUC mean of 0.843, indicating robust predictive performance in novel samples. Furthermore, the Bootstrap-derived mean calibration slope was 0.975. We applied this value as a global shrinkage factor to adjust regression coefficients, thereby mitigating overfitting risk. The calibrated curve is depicted in Figure 3. The final parameters after shrinkage correction are summarized in Table 4.
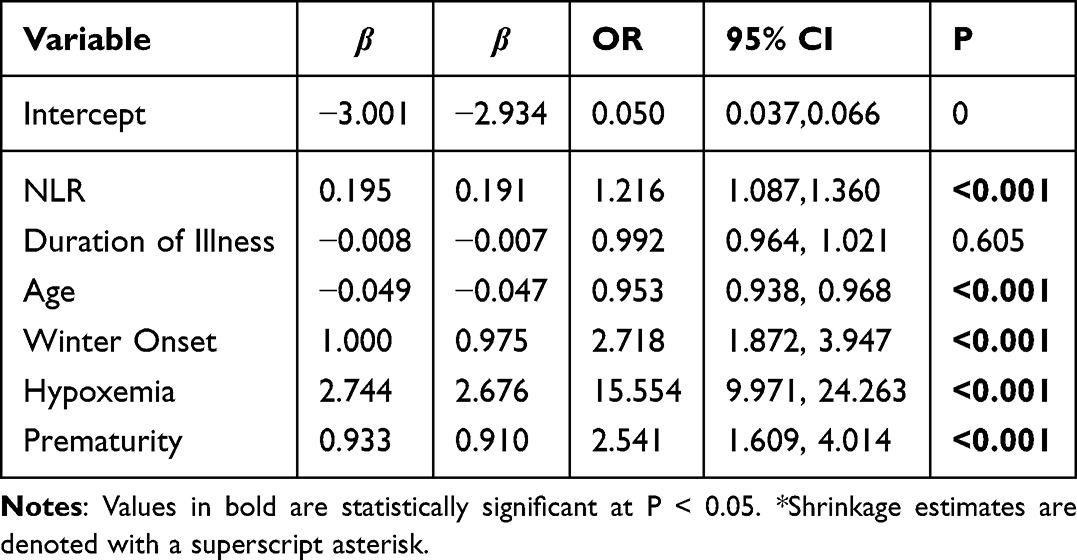 |
Table 4 Final Predictive Model Parameters After Bootstrap Internal Validation and Calibration Shrinkage |
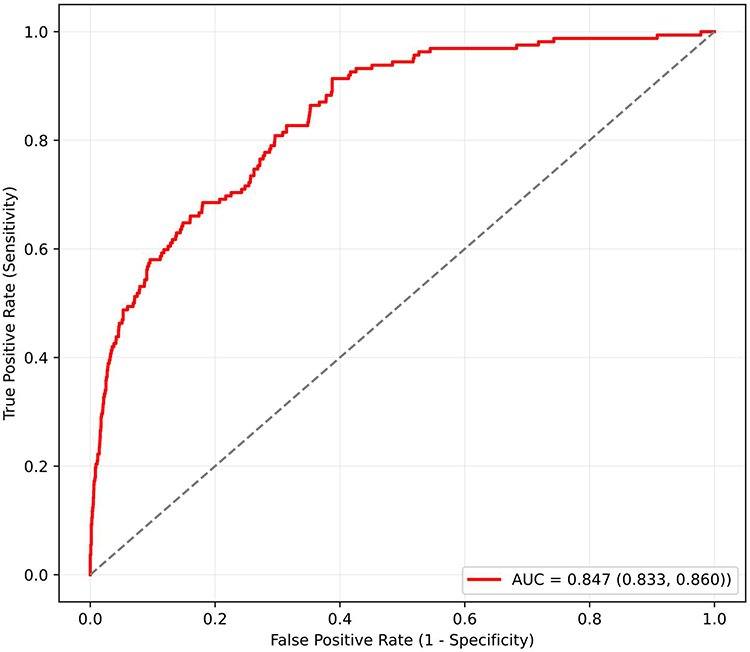 |
Figure 2 ROC curve of the nomogram model. The area under the ROC curve for the independent risk factors was 0.847 (95% CI: 0.833–0.860). |
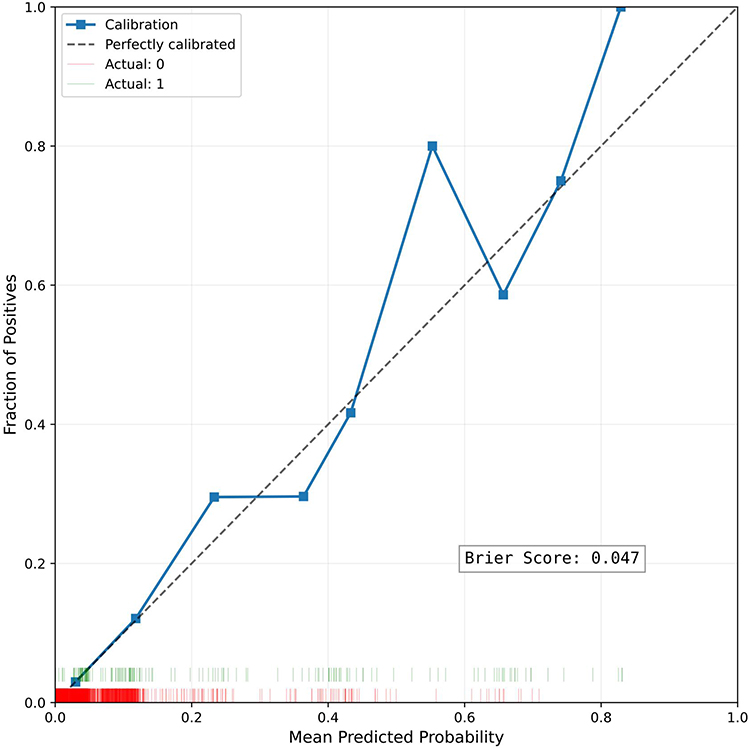 |
Figure 3 Calibration curve of the nomogram model. The horizontal axis represents the risk of severe RSV predicted by the nomogram; the vertical axis represents the risk of severe RSV actually observed. |
Discussion
Recently, the epidemiological characteristics of respiratory infections in children have undergone significant evolution. Following the novel coronavirus pandemic, the predominant viral spectrum has shifted: respiratory syncytial virus (RSV) now dominates among children under 5 years old, while influenza A virus predominates among children aged 5–10 years. Both viruses exhibit pronounced seasonal fluctuations.14,15 Annually, RSV infection accounts for an estimated 58,000 to 80,000 hospitalizations among children under 5 years of age in the United States.16 As non-pharmaceutical interventions are gradually lifted, RSV epidemic patterns have become increasingly complex, including phenomena such as seasonal shifts and delays.17 Against this backdrop, the disease burden of RSV as a primary pathogen causing acute lower respiratory infections and hospitalizations in infants and young children has become increasingly prominent. The clinical significance of severe RSV infection extends beyond the acute respiratory damage it causes in children. It also stems from the potential for RSV infection to trigger a series of complications, significantly increasing the risk of mortality and the likelihood of long-term sequelae in affected children.18 Therefore, this study aims to construct a predictive model based on early, readily accessible clinical indicators, providing clinicians with an intuitive and practical decision-making tool to address the new challenges posed by current epidemiological shifts in RSV. Based on data from Tianjin Children’s Hospital, a predictive nomogram for severe RSV infection was constructed and validated using data from a single-center retrospective cohort. Through multivariate analysis, we identified several clinical characteristics independently associated with the risk of severe RSV infection, including NLR, Age, Winter Onset, Hypoxemia, Preterm Infant.
In recent years, in-depth investigations into independent risk factors for RSV infection in children and the development of corresponding predictive models have provided a crucial foundation for improving patient outcomes and enabling early intervention for complications. RSV infection can affect multiple systems and trigger a series of complications, posing a serious threat to children’s healthy development. First, in terms of the respiratory system, the most common complications include respiratory failure and acute distress syndrome (ARDS).19 The mechanism is mainly that a large number of virus replications triggers a severe inflammatory response, leading to extensive alveolar epithelial damage, pulmonary edema, and host immune response disorders, forming an “inflammatory waterfall” effect. Secondly, RSV infection is prone to secondary bacterial pneumonia,20 causing pulmonary consolidation. The pathological basis is that the virus damages the airway mucosal barrier function and promotes bacterial colonization and invasion, thus making the condition more complex and critical. Cardiovascular complications should not be ignored, such as myocardial damage, tachycardia, and even heart failure, which are mostly related to the direct inhibition of myocardial hypoxia, inflammatory factor storm, and the increased cardiac load caused by pulmonary hypertension.21,22 In addition, children often have difficulty feeding due to respiratory distress and are complicated by dehydration and electrolyte disturbances. In severe cases, they may progress to acute respiratory acidosis and even have neurological manifestations such as drowsiness and convulsions.23 More importantly, a large amount of evidence-based medical evidence shows that severe RSV infection in infancy is an independent risk factor for recurrent wheezing and childhood asthma in the later period.24,25 Given this clinical context, the predictive model developed in this study holds significant practical value: its objective is to identify infants at high risk for complications early. By providing early warning for high-risk groups, clinicians can implement closer monitoring, more active respiratory support, and more comprehensive organ function protection strategies, thereby blocking the progression of the disease to the above-mentioned serious complications and ultimately improving the long-term prognosis of children.
Previous studies have identified independent risk factors associated with RSV infection, such as young age, preterm birth, various congenital disorders, and household and environmental factors.22,26,27 These findings are highly consistent with the results of this study. Among the many risk factors, young age (especially less than 6 months) is a well-established risk factor for severe RSV infection.28 The limitations in its physiological structure constitute the fundamental reason: the airway diameter of infants and young children is small, the resistance is high, the respiratory muscle development is not mature and it is easy to fatigue, the chest wall compliance is high, and it is difficult to effectively maintain the ventilation function. The immature development of the immune system is the key internal factor. The innate immunity and adaptive immune response of newborns and infants are not perfect. This immune deficiency state promotes a large number of virus replications and spreads to the lower respiratory tract.29 Furthermore, although full-term newborns carry maternal RSV neutralizing antibodies transmitted transplacentally at birth, their levels exhibit significant individual variation and rapidly decline postnatally. By six months of age, these antibodies have diminished to levels insufficient to provide effective immune protection. Extensive epidemiological data provide compelling evidence for this: The burden of RSV-associated ALRI is highest in early infancy, showing a sharp, age-dependent decrease after the first few months.30 Therefore, in this predictive model, age serves as a highly accessible and objective indicator. Its robust predictive power is grounded not only in extensive clinical observations but also deeply rooted in the aforementioned profound pathophysiological and immunological mechanisms.
Prematurity (usually defined as gestational age <37 weeks) is a definite high-risk factor for severe RSV infection. The mechanism is partially overlapped with that of the aforementioned young children, mainly involving immature lung structure development and immune dysfunction. The key reason is that the synthesis and secretion of pulmonary surfactant (PS) in premature infants are insufficient. The lack of PS not only leads to the decline of alveolar stability and compliance, which is prone to alveolar collapse and causes neonatal respiratory distress syndrome (NRDS), but also weakens the ability of alveolar macrophages to phagocytose and clear pathogens, thus creating favorable conditions for RSV colonization and diffusion in the lower respiratory tract. In terms of acquired immunity, preterm infants miss out on the active, substantial transfer of maternal antibodies through the placenta during late pregnancy, resulting in significantly lower levels of RSV-specific IgG at birth compared to full-term infants. Extensive clinical epidemiological evidence consistently confirms this high-risk factor. Retrospective studies and meta-analyses uniformly indicate that prematurity—particularly extreme prematurity (<32 weeks)—is a strong predictor of RSV-related hospitalization and intensive care unit admission.31 In summary, preterm infants constitute an independent high-risk group for severe RSV infection due to dual vulnerabilities in anatomical structure and immune defense. In clinical practice, heightened vigilance and proactive early intervention for these patients are fully supported by pathophysiological and evidence-based medical principles.
This study confirmed through multivariate regression analysis that both the NLR and hypoxemia are independent risk factors for severe RSV infection in children. These two indicators provide complementary pathophysiological evidence for early identification of severe risk from the perspectives of immune-inflammatory imbalance and physiological dysfunction: an elevated NLR reflects excessive neutrophil-driven inflammation and a relative deficiency in lymphocyte response, suggesting that systemic immune dysregulation may drive disease progression;32 meanwhile, hypoxemia directly indicates severe impairment of gas exchange function, marking that the condition is approaching respiratory failure, a critical clinical turning point.33 In clinical practice, the combined use of easily accessible NLR (revealing underlying immunopathological mechanisms) and real-time blood oxygen monitoring (objectively reflecting the degree of physiological decompensation) can achieve earlier and more comprehensive risk stratification, aiding in the timely implementation of targeted interventions for high-risk children, such as enhanced oxygen therapy, close monitoring, and even immunomodulatory treatment, thereby preventing disease progression and improving prognosis.
This study also found that winter onset is an independent risk factor for severe RSV infection in children, this finding is highly consistent with the results of numerous high-quality studies both domestically and internationally.34,35 From the perspective of exposure biology, the predictive value of winter onset for severe disease risk is far from a simple seasonal label; rather, it reflects a high convergence of multiple pathogenic mechanisms over time. Low-temperature and low-humidity environments can enhance the stability of RSV in aerosols and on surfaces, prolonging the virus’s survival time; meanwhile, increased indoor gatherings during the cold season significantly raise the contact frequency and infectious dose per unit time. The identification of this risk factor has clear clinical translational value. Unlike some laboratory indicators that can only be obtained after admission, “winter onset” is prospective information that can be obtained at the moment the child is seen. This feature makes it an ideal variable for primary triage and early warning systems.
Scope of Research and Clinical Applicability
Notwithstanding the promising performance of the developed and internally validated prediction model, several limitations must be acknowledged. First, a primary limitation is that this was a retrospective analysis conducted at a single center, and all data came from Tianjin Children’s Hospital, which may introduce selection bias and limit the external validity of the results. This design itself is inevitably affected by selection bias and information bias. Second, although we included several important clinical indicators for analysis, there are still several potential risk factors known to be related to the severity of RSV infection that have not been included, such as the specific nutritional status of the children, the duration of exclusive breastfeeding, the exposure to tobacco smoke in the family environment, and detailed viral load data. The absence of these factors may have limited the model’s comprehensiveness and predictive accuracy to some extent. Third, model validation is currently limited to internal validation (using the Bootstrap method). While internal validation demonstrates good discrimination and calibration, the model’s generalizability to novel, independent pediatric cohorts require further validation. Its ultimate applicability in clinical practice must be confirmed through multicenter, prospective, large-scale external validation studies.
This study excluded children with serious underlying conditions such as congenital heart disease (CHD) and bronchopulmonary dysplasia (BPD) from its design. Our decision to establish this exclusion criterion is primarily based on the following two key considerations: First of all, the pathophysiological mechanisms underlying severe RSV infection in such children are often closely related to their inherently low cardiopulmonary reserve and abnormal immune regulation, as well as other chronic conditions, which are fundamentally different from the deterioration seen in previously healthy children due to acute infections. Combining these two mechanistically distinct groups in analyses risks confounding key predictor identification, making it difficult to distinguish whether findings indicate acute infection severity or the inherent vulnerability of underlying conditions. Second, this study aims to develop a specialized prediction tool tailored for children with previously healthy physical conditions. Including children with high-risk comorbidities would diminish the model’s specificity and practical value for this primary target population. Therefore, this model is designed to serve a specific yet large clinical cohort—children hospitalized with acute RSV infection who lack significant chronic comorbidities. For this group of patients, our model provides a clear early risk stratification tool. We acknowledge that this is indeed a significant limitation of the model, meaning that the Benno nomogram is not directly applicable to children with severe pre-existing chronic cardiopulmonary diseases. This also points to a future research direction: developing independent predictive models for specific high-risk populations, such as those with CHD or BPD, within multicenter cohorts.
Conclusion
A nomogram incorporating five predictors (NLR, age, winter onset, hypoxemia, and preterm) was developed to predict severe RSV infection in children. Bootstrap internal validation showed good discrimination and indicated low overfitting. This tool can assist clinicians in timely identifying high-risk patients for early intervention.
Abbreviations
RSV, Respiratory syncytial virus; WBC, White Blood Cell; N, Neutrophil; L, Lymphocyte; NLR, Neutrophil-to-Lymphocyte Ratio; Hb, Hemoglobin; PLT, Platelet; CRP, C-Reactive Protein; ESR, Erythrocyte Sedimentation Rate; FER, Ferritin; PCT, Procalcitonin; IL-6, Interleukin-6; ALT, Alanine Aminotransferase; ALP, Alkaline Phosphatase; AST, Aspartate Aminotransferase; γ-GT, Gamma-Glutamyl Transferase; TP, Total Protein; ALB, Albumin; GLO, Globulin; La, Lactic Acid; GLU, Glucose; TBil, Total Bilirubin; DBil, Direct Bilirubin; IBil, Indirect Bilirubin; LDH, Lactate Dehydrogenase; CK, Creatine Kinase; CK-MB, Creatine Kinase-Myocardial Band; Cr, Serum Creatinine; BUN, Blood Urea Nitrogen; Ig, Immunoglobulin; PH, Potential of Hydrogen; PaO2, Arterial Oxygen Partial Pressure; PaCO2, Arterial Carbon Dioxide Partial Pressure; SaO2, Arterial Oxygen Saturation; HCO3-, Bicarbonate; TCO2, Total Carbon Dioxide Content.
Data Sharing Statement
The raw data included in this study are available in the article. For further inquiries, please contact the first author of this article at [email protected].
Ethical Statement
This study was approved by the Ethic Committee of the Tianjin Children’s Hospital (KY2020-19). This study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Ethics Committee, with written informed consent provided by all participants and their legal guardians.
Acknowledgments
We thank all participants and staff of this study and the physicians at the Tianjin Children’s Hospital (Children’s Hospital of Tianjin University).
Author Contributions
WL: Writing – original draft, Formal analysis. SW: Writing – original draft. XW: Writing – original draft. XN: Formal analysis. YG: Formal analysis, Supervision, Conceptualization, Writing – review & editing. YZ: Supervision, Conceptualization, Writing – review & editing. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Tianjin Key Medical Discipline Construction Project (No. TJYXZDXK-016B) and the Major Project of Tianjin Natural Science Foundation (20JCZDJC00630).
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Bourdeau M, Vadlamudi NK, Bastien N, et al. Pediatric RSV-associated hospitalizations before and during the COVID-19 pandemic. JAMA Network Open. 2023;6(10):e2336863. doi:10.1001/jamanetworkopen.2023.36863
2. Shi T, McAllister DA, O’Brien KL, et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: a systematic review and modelling study. Lancet. 2017;390(10098):946–14. doi:10.1016/s0140-6736(17)30938-8
3. Eshaghi A, Duvvuri VR, Lai R, et al. Genetic variability of human respiratory syncytial virus A strains circulating in Ontario: a novel genotype with a 72 nucleotide G gene duplication. PLoS One. 2012;7(3):e32807. doi:10.1371/journal.pone.0032807
4. Borchers AT, Chang C, Gershwin ME, Gershwin LJ. Respiratory syncytial virus--a comprehensive review. Clin Rev Allergy Immunol. 2013;45(3):331–379. doi:10.1007/s12016-013-8368-9
5. Thampi N, Knight BD, Thavorn K, et al. Health care costs of hospitalization of young children for respiratory syncytial virus infections: a population-based matched cohort study. CMAJ Open. 2021;9(4):E948–e956. doi:10.9778/cmajo.20200219
6. Li Y, Wang X, Blau DM, et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: a systematic analysis. Lancet. 2022;399(10340):2047–2064. doi:10.1016/s0140-6736(22)00478-0
7. Maglione M, Pierri L, Savoia F, et al. The path of bronchiolitis towards intensive care: risk factor analysis in a large italian cohort. J Clin Med. 2025;14(15). doi:10.3390/jcm14155420
8. Baraldi E, Bonadies L, Manzoni P. Evidence on the link between respiratory syncytial virus infection in early life and chronic obstructive lung diseases. Am J Perinatol. 2020;37(S 02):S26–s30. doi:10.1055/s-0040-1714345
9. Buttarelli L, Caselli E, Gerevini S, et al. Predictive factors and clinical markers of recurrent wheezing and asthma after RSV infection. Viruses. 2025;17(8). doi:10.3390/v17081073
10. Postiaux G, Zwaenepoel B, Louis J. Chest physical therapy in acute viral bronchiolitis: an updated review. Respir Care. 2013;58(9):1541–1545. doi:10.4187/respcare.01890
11. Sheikh Z, Potter E, Li Y, et al. Validity of clinical severity scores for respiratory syncytial virus: a systematic review. J Infect Dis. 2024;229(Supplement_1):S8–s17. doi:10.1093/infdis/jiad436
12. Jiang Y, Wang Y, Xia R, et al. Clinical features and risk factors of adenovirus-related plastic bronchitis in children. Ital J Pediatr. 2025;51(1):128. doi:10.1186/s13052-025-01968-y
13. Jiang Y, Wang X, Li L, Wang Y, Wang X, Zou Y. Predicting and interpreting key features of refractory Mycoplasma pneumoniae pneumonia using multiple machine learning methods. Sci Rep. 2025;15(1):18029. doi:10.1038/s41598-025-02962-4
14. Duan Y, He J, Cui Y, Li W, Jiang Y. Characteristics and forecasting of respiratory viral epidemics among children in west China. Medicine. 2021;100(16):e25498. doi:10.1097/md.0000000000025498
15. Dallmeyer LK, Schüz ML, Fragkou PC, et al. Epidemiology of respiratory viruses among children during the SARS-CoV-2 pandemic: a systematic review and meta-analysis. Int J Infect Dis. 2024;138:10–18. doi:10.1016/j.ijid.2023.10.023
16. Robinson RF. Impact of respiratory syncytial virus in the United States. Am J Health Syst Pharm. 2008;65(23 Suppl 8):S3–6. doi:10.2146/ajhp080438
17. Olsen SJ, Winn AK, Budd AP, et al. Changes in influenza and other respiratory virus activity during the COVID-19 pandemic-United States, 2020-2021. Am J Transplant. 2021;21(10):3481–3486. doi:10.1111/ajt.16049
18. Khanal S, Khanal B, Chou FS, Moon-Grady AJ, Ghimire LV. Comparison of mortality and cardiovascular complications due to COVID-19, RSV, and influenza in hospitalized children and young adults. BMC Cardiovasc Disord. 2024;24(1):686. doi:10.1186/s12872-024-04366-0
19. Ghazaly MMH, Abu Faddan NH, Raafat DM, Mohammed NA, Nadel S. Acute viral bronchiolitis as a cause of pediatric acute respiratory distress syndrome. Eur J Pediatr. 2021;180(4):1229–1234. doi:10.1007/s00431-020-03852-9
20. Lin HC, Liu YC, Hsing TY, et al. RSV pneumonia with or without bacterial co-infection among healthy children. J Formos Med Assoc. 2022;121(3):687–693. doi:10.1016/j.jfma.2021.08.012
21. Gavotto A, Ousselin A, Pidoux O, et al. Respiratory syncytial virus-associated mortality in a healthy 3-year-old child: a case report. BMC Pediatr. 2019;19(1):462. doi:10.1186/s12887-019-1847-2
22. Erdoğan S, Yakut K, Kalın S. Acute encephalitis and myocarditis associated with respiratory syncytial virus infections. Turk J Anaesthesiol Reanim. 2019;47(4):348–351. doi:10.5152/tjar.2019.52028
23. Saravanos GL, King CL, Deng L, et al. Respiratory syncytial virus-associated neurologic complications in children: a systematic review and aggregated case series. J Pediatr. 2021;239:39–49.e9. doi:10.1016/j.jpeds.2021.06.045
24. Kneyber MCJ, Steyerberg EW, de Groot R, Moll HA. Long-term effects of respiratory syncytial virus (RSV) bronchiolitis in infants and young children: a quantitative review. Acta Paediatr. 2000;89(6):654–660. doi:10.1080/080352500750043945
25. Hon KL, Leung AKC, Wong AHC, Dudi A, Leung KKY. Respiratory syncytial virus is the most common causative agent of viral bronchiolitis in young children: an updated review. Curr Pediatr Rev. 2023;19(2):139–149. doi:10.2174/1573396318666220810161945
26. Cai W, Buda S, Schuler E, Hirve S, Zhang W, Haas W. Risk factors for hospitalized respiratory syncytial virus disease and its severe outcomes. Influenza Respir Virus. 2020;14(6):658–670. doi:10.1111/irv.12729
27. Deng S, Cong B, Edgoose M, De Wit F, Nair H, Li Y. Risk factors for respiratory syncytial virus-associated acute lower respiratory infection in children under 5 years: an updated systematic review and meta-analysis. Int J Infect Dis. 2024;146:107125. doi:10.1016/j.ijid.2024.107125
28. Hall CB, Weinberg GA, Blumkin AK, et al. Respiratory syncytial virus-associated hospitalizations among children less than 24 months of age. Pediatrics. 2013;132(2):e341–8. doi:10.1542/peds.2013-0303
29. Lambert L, Sagfors AM, Openshaw PJ, Culley FJ. Immunity to RSV in Early-Life. Front Immunol. 2014;5:466. doi:10.3389/fimmu.2014.00466
30. Wang X, Li Y, Shi T, et al. Global disease burden of and risk factors for acute lower respiratory infections caused by respiratory syncytial virus in preterm infants and young children in 2019: a systematic review and meta-analysis of aggregated and individual participant data. Lancet. 2024;403(10433):1241–1253. doi:10.1016/s0140-6736(24)00138-7
31. Sarna M, Gebremedhin A, Richmond P, Levy A, Glass K, Moore HC. Determining the true incidence of seasonal respiratory syncytial virus-confirmed hospitalizations in preterm and term infants in Western Australia. Vaccine. 2023;41(36):5216–5220. doi:10.1016/j.vaccine.2023.07.014
32. Burrack N, Adar A, Goldbart A, et al. Monocyte and neutrophil to lymphocyte ratios in hospitalized children with RSV bronchiolitis. Pediatr Pulmonol. 2023;58(12):3530–3541. doi:10.1002/ppul.26687
33. Wetzke M, Lange M, Koerner-Rettberg C, et al. RSV is the main cause of severe respiratory infections in infants and young children in Germany - data from the prospective, multicenter PAPI study 2021-2023. Infection. 2025;53(5):1715–1723. doi:10.1007/s15010-025-02484-1
34. Rave N, de Bruijne MEM, Stellato RK, et al. Normalization of seasonality and age distribution of pediatric RSV infection following the pandemic disruption in the Netherlands. Open Forum Infect Dis. 2026;13(1):ofaf759. eCollection 2026 Jan. doi:10.1093/ofid/ofaf759
35. Dallagiacoma G, Lundholm C, Smew AI, et al. Risk factors for severe outcomes of respiratory syncytial virus infection in children: a nationwide cohort study in Sweden. Lancet Reg Health Eur. 2025;58:101447. doi:10.1016/j.lanepe.2025.101447
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Model That Predicts the Risk of Diabetic Nephropathy in Type 2 Diabetes Mellitus Patients: A Cross-Sectional Study
Yang J, Jiang S
International Journal of General Medicine 2022, 15:5089-5101
Published Date: 20 May 2022
Paraspinal Muscle Degeneration: A Potential Risk Factor for New Vertebral Compression Fractures After Percutaneous Kyphoplasty
Si F, Yuan S, Zang L, Fan N, Wu Q, Wang T, Wang A
Clinical Interventions in Aging 2022, 17:1237-1248
Published Date: 13 August 2022
Tracking Epidemiological Characteristics and Risk Factors of Multi-Drug Resistant Bacteria in Intensive Care Units
Wu C, Lu J, Ruan L, Yao J
Infection and Drug Resistance 2023, 16:1499-1509
Published Date: 15 March 2023
Construction and Validation of a Novel Nomogram for Predicting the Recurrence of Diffuse Large B Cell Lymphoma Treated with R-CHOP
Gong Y, Yan H, Yang Y, Zhai B, Huang Z, Zhang Z
Pharmacogenomics and Personalized Medicine 2023, 16:291-301
Published Date: 1 April 2023
Development and Validation of a Nomogram for Predicting Bronchiolitis Obliterans in Children with Severe Adenovirus Pneumonia: Identification of Key Risk Factors
Xiao J, Zhang L, Su L, Ali K, Wu S, Zhao M
Pediatric Health, Medicine and Therapeutics 2025, 16:267-277
Published Date: 16 September 2025