Back to Journals » OncoTargets and Therapy » Volume 19
A Novel Strategy for Treating Elderly Patients with Advanced Non-Small Cell Lung Cancer: Exploring the Efficacy and Safety of Anlotinib Combined with PD-1/PD-L1 Inhibitors
Received 4 November 2025
Accepted for publication 19 March 2026
Published 30 March 2026 Volume 2026:19 578933
DOI https://doi.org/10.2147/OTT.S578933
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Nagashree Seetharamu
Chuanzhen Chi,1,2 Li Li,1,2 Chunhua Xu1,2
1Department of Respiratory Medicine, Affiliated Nanjing Brain Hospital, Nanjing Medical University, Nanjing, People’s Republic of China; 2Clinical Center of Nanjing Respiratory Diseases an Imaging, Nanjing, People’s Republic of China
Correspondence: Li Li, Department of Respiratory Medicine, Affiliated Nanjing Brain Hospital, Nanjing Medical University, 215 Guangzhou Road, Nanjing, 210029, People’s Republic of China, Email [email protected] Chunhua Xu, Department of Respiratory Medicine, Affiliated Nanjing Brain Hospital, Nanjing Medical University, 215 Guangzhou Road, Nanjing, 210029, People’s Republic of China, Email [email protected]
Objective: This study aimed to explore whether the combination of anlotinib and immunotherapy is an effective and safe alternative to chemotherapy for clinical treatment. Provide a new treatment plan for elderly patients who are unwilling to undergo chemotherapy, intolerant to chemotherapy, or have poor ECOG PS scores.
Methods: This is a single-center retrospective investigation that collected clinical data of 58 elderly aNSCLC patients treated with anlotinib monotherapy or anlotinib plus PD-1/PD-L1 inhibitor combination therapy at Nanjing Chest Hospital during the period from January 1, 2020 to December 31, 2023, with the study being subject to a limited sample size.
Results: Fifty-eight elderly patients were evaluated after two cycles of anlotinib monotherapy and combined therapy. In the monotherapy group of 28 patients, the ORR and DCR were 25.0% (7/28) and 78.6% (22/28), respectively. Besides, the mPFS and the mOS reached up to 5.4 months (95% CI, 4.4– 6.4 months) and 11.2 months (95% CI, 7.2– 15.2 months), respectively. In the group with combination therapy of 30cases, the ORR for this group was calculated at 30.0% (9/30), the DCR was higher, at 86.7% (26/30), the mPFS and the mOS were determined to be 8.5 months (95% CI, 7.3– 9.7 months) and 17.8 months (95% CI, 13.2– 22.4 months), respectively. In multivariate COX analysis, brain metastasis and treatment methods were found to be independent risk factors for PFS alongside OS. Both groups had a comparable overall incidence of adverse events (AEs), at 70.0% and 64.3% respectively, with no statistically significant difference noted in the rate of grade 3 and above adverse events (23.3% versus 17.9%).
Conclusion: Anlotinib combined with immunotherapy demonstrated superior efficacy and better tolerability than anlotinib alone. The combination of anlotinib and immunotherapy may provide a “chemo-free” treatment mode for elderly patients with non-small cell lung cancer who refuse or cannot tolerate chemotherapy and have poor ECOG PS scores.
Keywords: anlotinib, immunotherapy, PD-1/PD-L1, non-small cell lung cancer, elderly patients, chemo-free
Introduction
Of all cancers worldwide, lung cancer (LC) represents the most prevalent form and accounts for the greatest number of fatalities, particularly in China.1,2 Non-small cell lung cancer (NSCLC) represents the most common form of lung malignancy, and most patients are diagnosed at an advanced stage, which contributes to unfavorable clinical outcomes and low overall survival.3,4 Over the past ten years, there have been considerable advancements in the management of advanced LC. In cases of NSCLC where driver gene mutations are identified, molecular targeted therapy constitutes the preferred initial therapeutic approach according to current clinical guidelines.5,6 Platinum-based dual-drug chemotherapy remains the primary treatment method for advanced NSCLC (aNSCLC) without driver gene mutations. With the emergence of immunotherapy, chemotherapy combined with immunotherapy has become a standard treatment that significantly improves patients’ quality of life and prolongs survival. In recent years, treatment options such as immunotherapy and anti-angiogenic therapy have emerged one after another. The growth and metastasis of tumors depends on the formation of tumor neovascularization; however, patients receiving anti angiogenic monotherapy did not show significant improvement in prognosis. Immune checkpoint inhibitors(ICIs) have led to a notable improvement in clinical outcomes for eligible lung cancer patients. However, immunotherapy alone is only suitable for patients with high PD-L1 expression.7 For patients with low or negative PD-L1 expression, immunotherapy alone yields limited benefit. As recommended by major guidelines, the standard first-line strategy is ICI-based combination therapy with chemotherapy or anti-angiogenic agents to improve clinical outcomes.8 Although the therapeutic benefits of immunotherapy combined with chemotherapy are not affected by PD-L1 expression, adverse reactions caused by chemotherapy are significant.9,10 In particular, elderly patients often have comorbidities and impaired organ function, resulting in lower tolerance and higher toxicity risk to platinum-based doublet chemotherapy. We are seeking an alternative to chemotherapy, a “chemo-free” strategy, particularly for elderly patients who are either unwilling to receive chemotherapy or unable to endure it and who also have low ECOG PS scores. Notably, most randomized controlled trials on anti-angiogenic combined immunotherapy have strict inclusion criteria, with elderly patients over 70 years old or those with ECOG PS score ≥2 often underrepresented or even excluded, leading to scarce real-world evidence and a lack of targeted treatment recommendations for this special population. This research gap directly results in clinical treatment dilemmas, which is the core motivation of our study.
PD-1/PD-L1 regulates the immune microenvironment and inhibits abnormal tumor angiogenesis. Upon activation, CD4+ T cells, CD8+ T cells, and Th1 cells can generate cytokines such as interferon-gamma (IFN-γ) and tumor necrosis factor (TNF), which have anti-tumor properties. These cytokines enhance the ability of the immune system to recognize tumor antigens and destroy tumor cells, thereby contributing to the normalization of blood vessels.11,12 Therapy with anti-angiogenic drugs can alter the tumor microenvironment to stimulate the immune system, thereby producing effective anti-tumor immune responses. Among anti-angiogenic agents, bevacizumab is often combined with chemotherapy or immunotherapy but has limited application in elderly poor-PS patients due to higher risks of bleeding and proteinuria; ramucirumab is mainly recommended for second-line or later treatment with modest single-agent efficacy. As a small-molecule drug, anlotinib functions as a multi-target tyrosine-kinase inhibitor and is capable of suppressing tumor angiogenesis as well as the proliferation of tumor cells. Compared with bevacizumab and ramucirumab, anlotinib has advantages of oral administration, mild adverse reactions, a broader anti-tumor spectrum, and better blood-brain barrier penetration, making it more suitable for elderly aNSCLC patients with poor PS scores. Although anlotinib shows significant efficacy in the initial treatment phase, some patients may develop resistance in the short term (usually within a few months), leading to limited treatment duration. Some studies have indicated that anlotinib can strengthen the key components of the tumor immune cycle. When combined with immunotherapy medications, it exhibits a synergistic effect that enhances anti-tumor efficacy. This synergistic boost can lead to a more enduring antitumor response from the ICIs.13 Additionally, cytoprotective autophagy is an important mechanism underlying primary and secondary resistance to PD-1/PD-L1 immunotherapy, as it promotes tumor cell survival under immune attack and reduces the killing effect of ICIs; PD-L1 can further aggravate this resistance by inducing autophagy via the MAPK signaling pathway. Notably, anlotinib can down-regulate tumor cell autophagy through inhibiting the MAPK/ERK pathway, thereby reversing autophagy-mediated resistance to PD-1/PD-L1 inhibitors, which further explains the synergistic anti-tumor mechanism of the combination therapy.14–16
This clinical investigation sought to conduct a retrospective assessment of the therapeutic efficacy and safety profile of anlotinib combined with PD-1/PD-L1 inhibitors for elderly aNSCLC patients. To provide a “chemo-free” treatment mode for aNSCLC patients who are elderly, refuse or cannot tolerate chemotherapy, and have poor ECOG PS scores, enabling them to achieve a favorable prognosis and better quality of life.
Patients and Methods
Patients
From January 1, 2020, to December 31, 2023, Nanjing Chest Hospital diagnosed approximately 845 cases of aNSCLC, of which 213 patients were aged 70 years and above. Among the elderly patients with aNSCLC who received anlotinib monotherapy and anlotinib combined with immunotherapy, there were 115 cases, including 50 patients who also received other anti-tumor medications and 7 patients who refused to disclose their condition and could not be followed up. Therefore, this study included 58 eligible patients, comprising 28 patients who received anlotinib monotherapy and 30 patients who received anlotinib combined with immunotherapy. A screening flowchart is shown in Figure 1. These included sex, ECOG PS score, smoking status, pathological type, distant metastatic organ, number of lines of previous treatment, gene mutation status, and the treatment plan. These patients were treated with at least one cycle of anlotinib monotherapy or anlotinib in combination with ICIs. Inclusion criteria: NSCLC confirmed by histology or cytology to have adenocarcinoma (ADC) or squamous cell carcinoma (SCC), stage III–IV, with measurable lesions, unwillingness to undergo chemotherapy, intolerance to chemotherapy (elderly, poor nutritional status, poor ECOG score), and estimated survival time exceeding 3 months. The exclusion Criteria: Small cell lung cancer, central squamous cell carcinoma, severe cardiovascular diseases, severe hepatic or renal insufficiency, autoimmune diseases requiring long-term immunosuppressive therapy, moderate to severe interstitial pneumonia, concurrent malignancies at other sites, active bleeding, or a high risk of major bleeding.
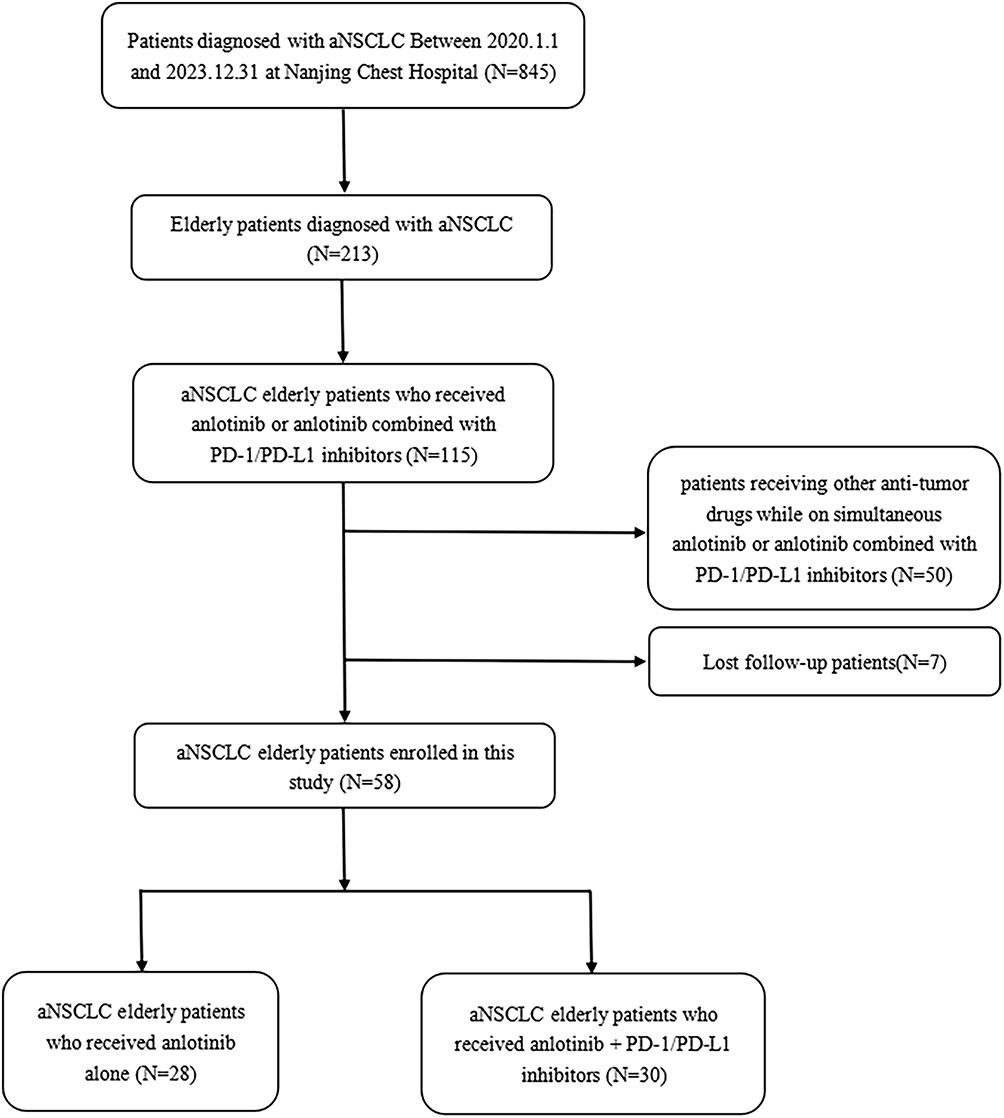 |
Figure 1 Flowchart of the screening procedure. |
Therapeutic Method
Anlotinib was administered at 12 mg/day for a continuous period of 14 days, followed by a 7-day break, which constituted a 21-day cycle. For PD-1 monoclonal antibody therapy, sintilimab (200 mg) or tislelizumab (200 mg) was chosen. In contrast, for PD-L1 monoclonal antibody therapy, either durvalumab (1000 mg) or atezolizumab (1200 mg) was administered every 21 days. Treatments were administered until disease progression, tolerable toxic AEs, or death occurred.
Efficacy and the Safety of Treatments
The clinical efficacy for treatments was assessed utilizing the RECIST 1.1 criteria for solid tumor response. Progression-free survival (PFS) was designated as the primary prognostic endpoint, and overall survival (OS), objective response rate (ORR), disease control rate (DCR), duration of response (DOR), and safety were regarded as secondary endpoints. AEs were recorded in compliance with the Common Terminology Criteria for Adverse Events (CTCAE) version 4.03.
Statistical Analysis
Statistical analysis was conducted using Prism8.0 (GraphPad software, La Hoya, USA) and SPSS (version 27.0; IBM, Armonk, New York, USA). Quantitative data are reported as the mean ± standard deviation, and intergroup differences were analyzed using the t-test or rank sum test. The chi-square test or Fisher’s exact test was applied to compare clinical characteristics and treatment efficacy across groups, and Kaplan-Meier analysis was used for survival curve assessment. Moreover, Cox proportional hazards regression was employed for univariate and multivariate examinations to assess factors associated with treatment response and survival outcomes. Differences were considered statistically significant at P values less than 0.05. It should be noted that this study is a retrospective exploratory analysis, and due to the limited sample size inherent to this study, formal power calculation was not performed during the study design, and the statistical power is insufficient to detect potential significant differences among subgroups.
Results
Baseline Characteristics of aNSCLC Patients
Fifty-eight elderly patients with aNSCLC were enrolled between January 2020 and December 2023. Baseline demographic and clinical characteristics of the study cohort are summarized in Table 1. Within this cohort, 28 patients (median age 75 years) received anlotinib monotherapy. This group comprised of 20 males and 8 females. Specifically, there were 18 ADC and 10 SCC cases. 21 patients had a smoking history, while seven had never smoked. Notably, 13 patients had an ECOG PS score of 0–1, whereas 15 had an ECOG PS score of ≥2. Furthermore, 17 cases exhibited fewer than 3 metastatic sites, whereas 11 cases had 3 or more sites, including 15 with brain metastasis and 8 with liver metastasis. In terms of treatment distribution, first-line and other-line treatments were administered in nine and 19 cases, respectively. Additionally, 5 patients had EGFR mutations, and 11 tested positive for PD-L1 expression.
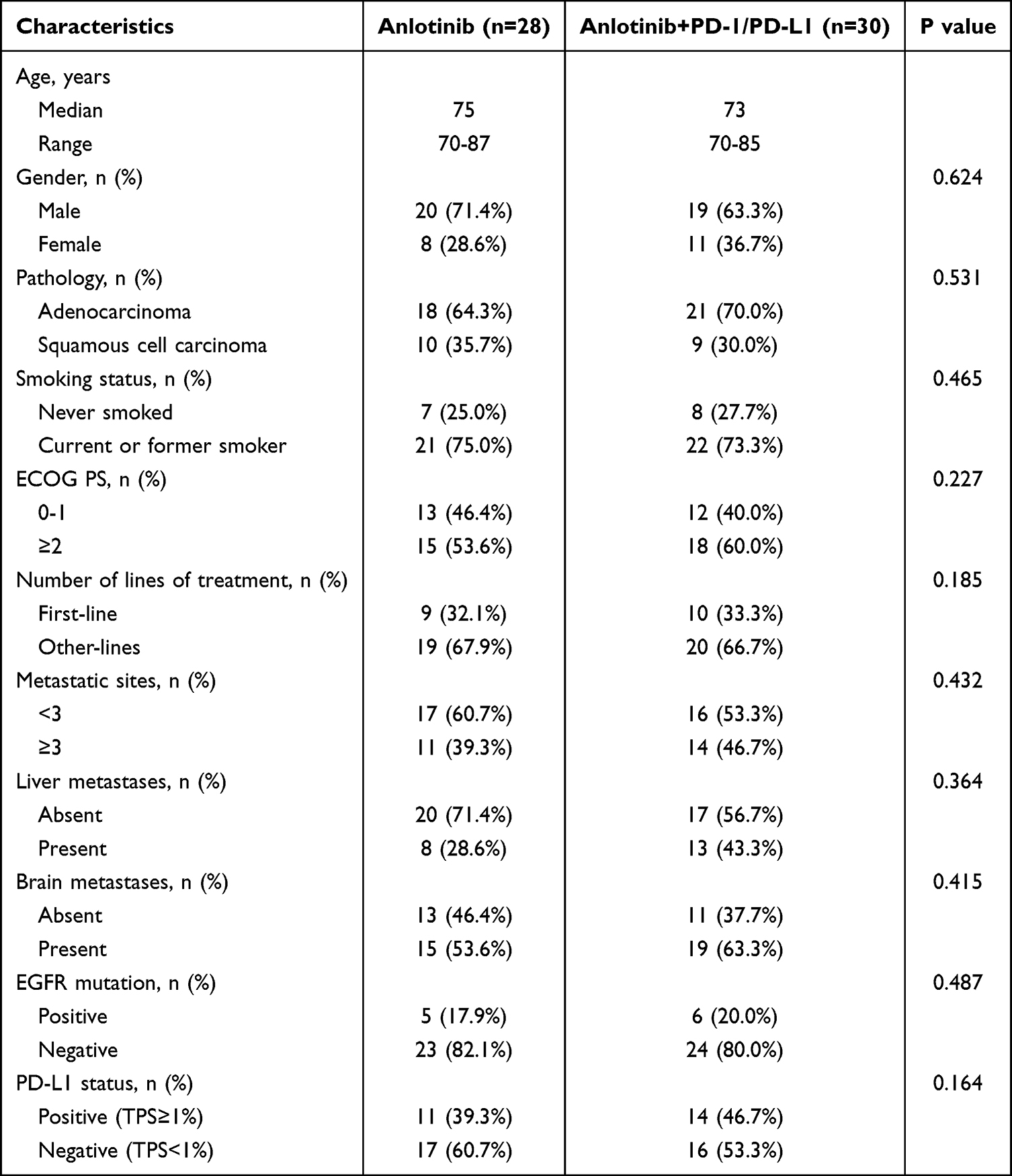 |
Table 1 Baseline Characteristics of Study Population |
There were 30 patients receiving combination therapy, the median age at baseline was 73 years, including 19 males as well as 11 females. This group consisted of 21 patients with ADC and nine patients with SCC, with 22 patients being ever smokers and eight patients with no smoking history. Regarding the ECOG PS scores,12 patients scored 0–1, while 18 patients scored ≥2. Furthermore, 16 cases had fewer than three metastatic sites and 14 cases had three or more sites, including 19 cases with brain metastasis and 13 cases with liver metastasis. First-line and other-line treatments were administered to 10 and 20 patients, respectively. Additionally, there were 6 cases of EGFR mutations and 14 cases of PD-L1 positivity in this group. Notably, all EGFR-positive patients received EGFR-TKI treatment.
Efficacy Evaluation
Fifty-eight patients were evaluated for efficacy after completing 2 cycles of treatment with either anlotinib monotherapy or combination therapy. In the anlotinib monotherapy group, the median follow-up time were 7.7 months. The shorter follow-up time in the monotherapy group was due to early death and disease progression. PR, SD, and PD were observed in seven, 15, and six patients, respectively. The ORR was 25.0% (7/28), DCR was 78.6% (22/28), and the median DOR was 7.6months (95% CI, 5.7–9.8 months). The maximum percent change from baseline in target lesion dimensions was −50% (Figure 2A). However, the median follow-up duration in the combination therapy group was 18.6 months. Nine patients achieved PR, 17 exhibited SD, and four experienced PD, resulting in an ORR of 30.0% (9/30) and a DCR of 86.7% (26/30), and the median DOR was 12.3months (95% CI, 9.1–14.4 months). The greatest percentage change observed in the target lesion size from baseline was −90% (Figure 2B). Median progression-free survival (mPFS) and median overall survival (mOS) in the anlotinib monotherapy cohort were 5.4 months (95% CI, 4.4–6.4 months) and 11.2 months (95% CI, 7.2–15.2 months), respectively (Figure 3A). For the combination therapy group, the corresponding mPFS and mOS were 8.5 months (95% CI, 7.3–9.7 months) and 17.8 months (95% CI, 13.2–22.4 months), respectively (Figure 3B).
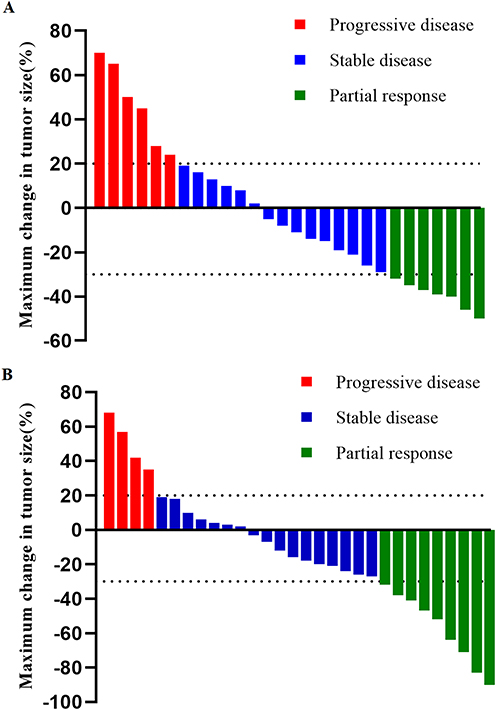 |
Figure 2 Waterfall plot of maximum change in tumor size in anlotinib (A) and anlotinib plus PD-1/PD-L1 (B). Abbreviations: PD, progressive disease; SD, stable disease; PR, partial response. |
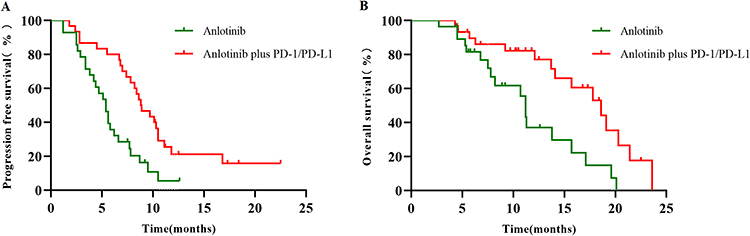 |
Figure 3 Kaplan-Meier survival curve of progression free survival (A) as well as overall survival (B) in the groups with anlotinib and anlotinib plus PD-1/PD-L1. Abbreviations: PFS, progression-free survival; OS, over survival. |
In univariate COX analysis, treatment lines (P=0.031), site of metastasis (P=0.024), brain metastasis (P=0.007), and treatment method (P=0.014) were associated with PFS (Table 2). In addition, ECOG PS score (P=0.027), metastatic sites (P=0.025), brain metastasis (P=0.003), and treatment plan (P=0.006) were correlated with OS (Table 3). However, histological type, clinical stage, liver metastasis, EGFR positivity, and PD-L1 positivity were not significantly associated with the survival outcomes. In the multivariate COX analysis, it was found that brain metastasis and treatment methods were independent prognostic factors for predicting PFS and OS (Tables 2 and 3). Log rank tests were performed to compare PFS and OS rates across different treatment methods and between groups with and without brain metastasis, and the differences were statistically significant (Figures 2 and 3).
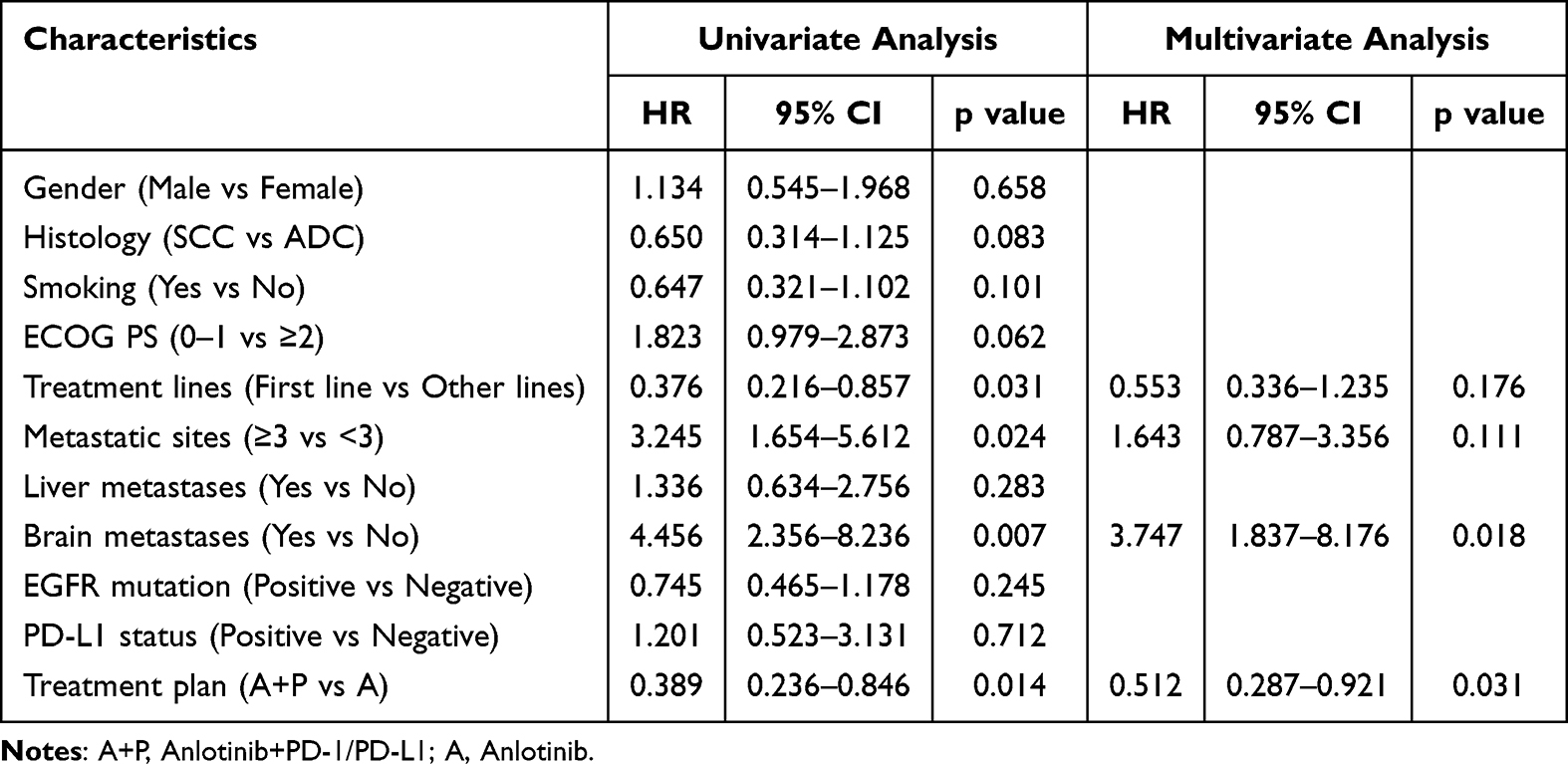 |
Table 2 Univariate and Multivariate Cox Regression Analysis of Factors Associated with PFS |
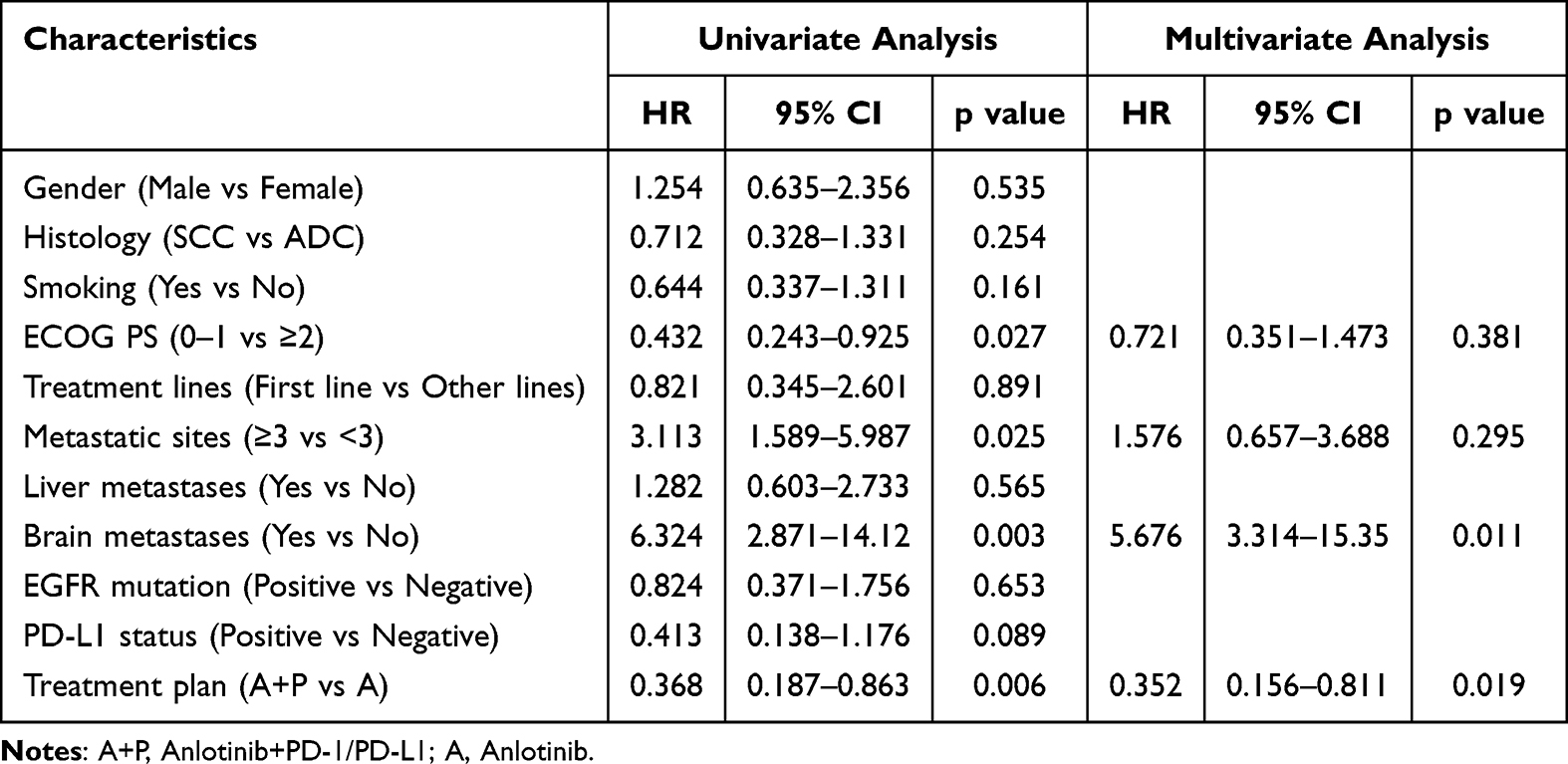 |
Table 3 Univariate and Multivariate Cox Regression Analysis of Factors Associated with OS |
Safety
In the combination therapy group, 21 patients (70.0%) experienced AEs, including fatigue (12/30,40.0%), hypertension (13/30,43.3%), decreased appetite (11/30,36.7%), diarrhea (10/30,33.3%), neutropenia (7/30,23.3%), proteinuria (7/30,23.3%), hypothyroidism (5/30,16.7%), and nausea (4/30,13.3%). In the anlotinib monotherapy group, 18 patients (64.3%) experienced AEs, with the most common being decreased appetite (13/28,46.4%), hypertension (11/28,39.3%), fatigue (10/28,35.7%), diarrhea (9/28,32.1%), proteinuria (7/28,25.0%), neutropenia (5/28,17.9%), hepatic function abnormalities (4/28,14.3%), thrombocytopenia (5/28,17.9%), and hand–foot syndrome (3/28,10.7%). The overall incidence of AE was similar among the two groups (P>0.05;Table 4). In the group with combination therapy, there were seven cases (23.3%) of grade 3 AEs, similar to five cases (17.9%) in the group with anlotinib monotherapy (P > 0.05) (Table 4). No fatal AEs occurred in either of the groups.
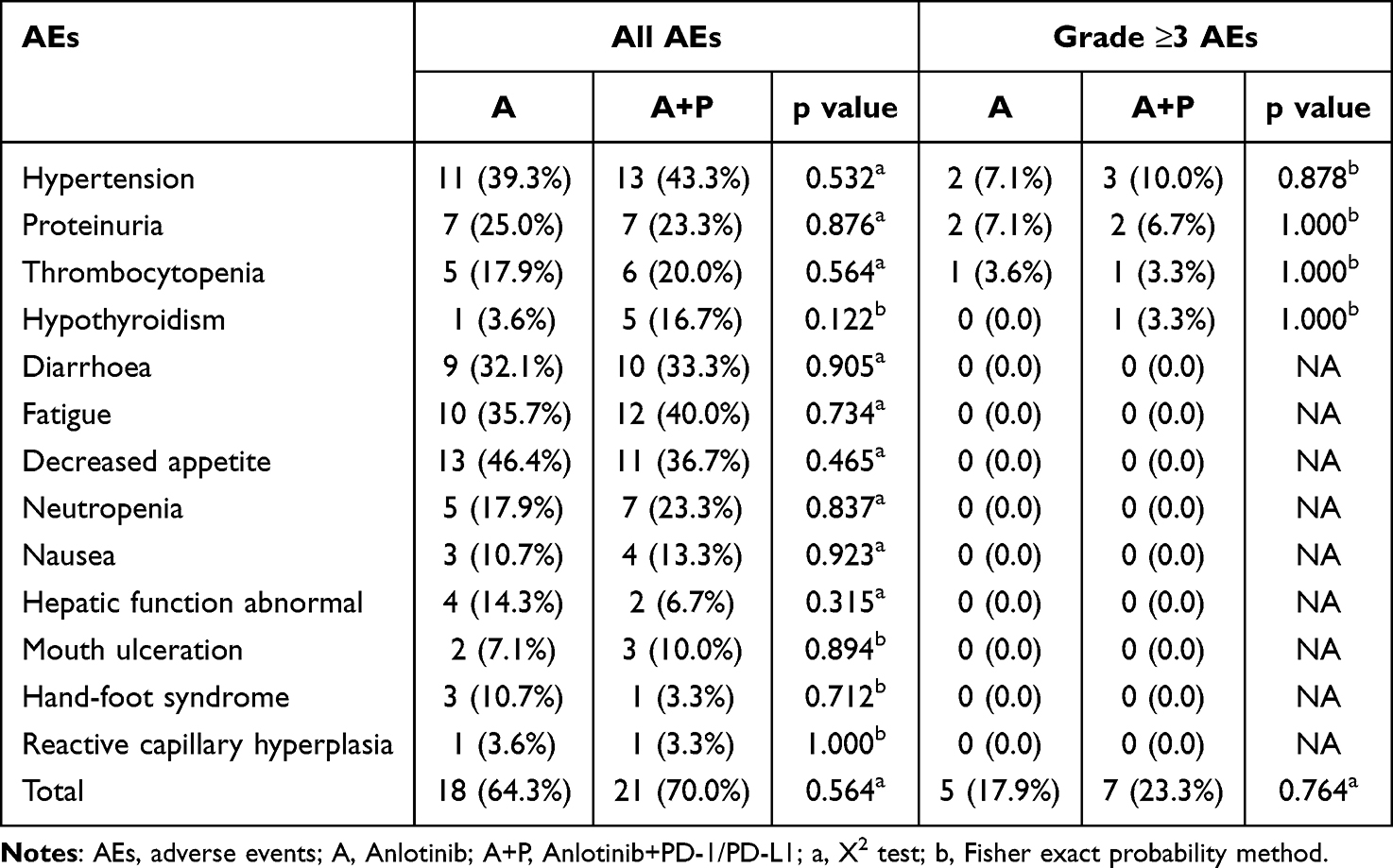 |
Table 4 Comparison of Adverse Events Between Groups |
Discussion
Elderly patients often have multiple underlying diseases, such as decreased liver and kidney function, weakened drug metabolism and excretion ability, poor PS score, high risk of chemotherapy, and poor tolerance. Therefore, these patients are more inclined to undergo chemotherapy and targeted therapy is the preferred option. However, not all patients exhibit drug-sensitive mutations. Anlotinib is a good choice for elderly patients without sensitive mutations. Studies have shown that using anlotinib monotherapy as third line treatment, the mPFS and the mOS have been reported to be 5.4 months and 9.6 months, respectively.17 However, monotherapy with anlotinib often has a short resistance time and cannot achieve longer survival benefits, whereas PD-1/PD-L1 inhibitors enhance their killing effect on tumor cells by activating the patient’s own immune system. The combination of the two may produce a synergistic effect and enhance antitumor activity. In Phase 3 clinical studies on NSCLC, the mOS of nivolumab was used as a second-line treatment was 9.2 months for cases with advanced SCC and 12.2 months for those with non-SCC.18 In our study, for aNSCLC patients with anlotinib monotherapy, the mPFS and mOS was 5.4 months and 11.2 months, respectively; In contrast, for those with anlotinib plus PD-1/PD-L1, the values were 8.5 months and 17.8 months, respectively. Therefore, by integrating this study with existing literature data, the combination of anlotinib and immunotherapy may have a greater survival advantage in aNSCLC than anlotinib alone.
In this study, multivariate COX analysis revealed that brain metastasis was a risk factor for predicting survival, whereas immunotherapy combined with anlotinib was a protective factor. We hypothesize that the protective effect of the combined therapy may stem from the synergistic mechanism between anlotinib and ICIs, anlotinib is capable of inhibiting tumor angiogenesis and attenuating the immunosuppressive microenvironment, thereby strengthening the anti-tumor activity of ICIs and further reduces the risk of brain metastasis. This observation is in line with the conclusions of previous researches, which have demonstrated that TKIs and ICIs exert a synergistic anti-tumor effect in cancer treatment.19 In terms of blood-brain barrier permeability, anlotinib has a lower molecular weight and higher lipid solubility than other TKIs like sorafenib and regorafenib, enabling it to cross the blood-brain barrier more effectively and exert anti-tumor effects within the central nervous system. This could be one of the key reasons why the combined therapy achieves superior efficacy in patients with brain metastasis, and this conclusion supported by studies on anlotinib plus EGFR-TKIs for the management of advanced EGFR-mutant NSCLC, where patients with brain metastasis gained more significant PFS benefits from the combined regimen.20 Furthermore, relevant studies have indicated that targeted drugs with excellent blood-brain barrier penetration capacity can effectively improve the therapeutic outcome of brain metastasis, which further validates our hypothesis.21 There are studies showing that immunity and anti-angiogenic drugs can mutually promote the anti-cancer mechanism. The mechanism may involve anti-angiogenic drugs reversing the immunosuppressive microenvironment, facilitating the restoration of normal function in tumor blood vessels, enhancing the function of immune cells, reversing immune escape, activating effector T cells, and upregulating IFN-γ. The secretion of anti-tumor cytokines, such as TNF, and the combined action of silver on blood vessels, normalization of the tumor vascular system, and promotion of the action of various anti-cancer drugs, including anti angiogenic drugs, there is a positive feedback effect between the two.22–24
Clinical studies have demonstrated that ICIs, together with anti-vascular survival drugs, substantially enhance the prognosis of patients with diverse malignant tumors. The IMbrave150 study investigated the response to immune combined anti vascular therapy in first-line hepatocellular carcinoma treatment. Atezolizumab combined with bevacizumab showed better efficacy than Sorafenib alone, with an mPFS of 5.7 months vs 3.2 months, and safe and controllable adverse reactions.25 KEYNOTE-426 is a randomized controlled study that evaluated first-line treatment of advanced renal cell using ICIs and axitinib. Compared to the use of axitinib alone, the combination of pembrolizumab and axitinib showed better efficacy in treating advanced renal cell carcinoma, with an ORR of 59.3% versus 35.7%, and a mPFS of 15.1 months versus 11.1 months, respectively.26
For patients with metastatic non-squamous NSCLC, supplementing the bevacizumab plus chemotherapy regimen with atezolizumab yielded statistically significant improvements in PFS and OS, irrespective of PD-L1 expression or EGFR/ALK genetic modification status.27 Research on anti-angiogenesis and immunotherapy in NSCLC is currently underway, and a randomized Phase 2 study showed that the combination of anti-angiogenesis ramucirumab and pembrolizumab showed significant survival benefits in patients with NSCLC who had previously received ICIs treatment.28 These findings suggest that the combination of immunotherapy and anti-angiogenic agents holds the potential to achieve therapeutic benefits in various malignancies. An exploratory study on the first-line treatment of aNSCLC using anlotinib plus sintilimab published at the 2019 World Congress on LC demonstrated an mPFS of 15 months.29 In addition, a retrospective study using anlotinib plus anti-PD-1 antibody as third-line therapy among 101 patients with aNSCLC reported an mPFS of 6.7 months as well as a DCR of 79.2%.30
The toxic AEs associated with the combination therapy were mostly tolerable. Similar to prior clinical trials and real-world investigations, fatigue, hypertension, decreased appetite, hypothyroidism, hand-foot syndrome, and oral mucosal inflammation have emerged as the most prevalent AEs.31–34 In the current study, the spectrum of toxic AEs was comparable between the combination therapy and anlotinib monotherapy groups. Regarding the overall incidence of AEs, the combination of anlotinib and immunotherapy showed a similar rate to anlotinib single-agent treatment (70.0% vs. 64.3%). The incidence of fatigue, decreased appetite, hypertension, diarrhea, neutropenia, proteinuria, and hypothyroidism was relatively high, and most AEs were grade 1–2; however, no obvious difference in ≥ grade 3 AEs was found in contrast with the anlotinib monotherapy group (23.3% vs. 17.9%), with most AEs detected in a timely manner and alleviated after active symptomatic treatment. In summary, combination therapy involving anlotinib and PD-1/PD-L1 demonstrated favorable safety profiles.
In summary, anlotinib combined with PD-1/PD-L1 immunotherapy exhibited a favorable overall therapeutic outcome and demonstrated good tolerability in the management of elderly patients with aNSCLC. Compared with monotherapy with anlotinib, patients exhibited significant advantages in both PFS and OS without experiencing a significant increase in toxicity. Brain metastasis could independently influenced PFS and OS in these patients. This study provides a possibility of “chemo-free” treatment for NSCLC patients who are elderly, have poor ECOG PS scores, refuse or cannot tolerate chemotherapy, and do not have sensitive drug mutations, but this needs to be further validated through prospective studies with larger sample sizes. Potential heterogeneity was introduced by the administration of multiple distinct PD-1/PD-L1 inhibitors. Despite overlapping immunological targets, variations in drug properties, dosage regimens, and clinical indications may have contributed to variability in treatment response and survival outcomes in this retrospective analysis.
However, this research has a number of limitations to acknowledge. Firstly, it represents a single-center retrospective analysis based on a relatively small sample size, we cannot completely rule out selection bias.The findings of this study are exploratory, and their further validation necessitates larger-scale prospective studies; secondly, the sample size of this study was limited, precluding subgroup analysis. Therefore, expanding the sample size of cases with first-line and other-line treatments and extending the follow-up duration is necessary to obtain more accurate data. However, in clinical practice, some problems still need to be solved, such as determining the optimal dosage and treatment timing to maximize the therapeutic effect, which will be one of the future research directions of our team.
Conclusions
This study confirms that anlotinib in combination with PD-1/PD-L1 inhibitors affords significant improvements in survival outcomes compared to monotherapy with anlotinib in elderly patients with aNSCLC, with no significant increase in therapeutic toxicity. Multivariate analysis showed that brain metastasis is an independent negative prognostic factor, whereas combination therapy is a protective predictor, which is consistent with the known synergistic mechanism of anti-angiogenic and immunotherapy drugs. It may become a new “chemotherapy-free” treatment model, providing a potential treatment option for elderly patients who are unwilling or intolerant to chemotherapy. Prospective studies should be conducted in the future to validate the efficacy, optimize dosing regimens, and explore biomarkers for patient screening.
Ethical Approval
All procedures in this retrospective study were performed in accordance with the Declaration of Helsinki. As the research was based on completely anonymized clinical data without any prospective patient involvement, the institutional ethics committee granted a formal waiver of written informed consent. This study was approved by the Institutional Review Board of Nanjing Brain Hospital Medical Ethics Committee (approval number: 2024-KY070-01).
Acknowledgments
The investigators gratefully acknowledge the contributions of all study participants were utilized in this retrospective investigation.
Funding
This work was supported in part by a grant from the Medical Scientific Research Project of Jiangsu Provincial Commission Health and Family Planning (H2017048).
Disclosure
The authors declare that there are no financial conflicts of interest or personal relationships that may affect the research presented in this study.
References
1. Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–12. doi:10.3322/caac.21492
2. Planchard D, Popat S, Kerr K, et al. Metastatic non-small cell lung cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29(suppl_4):iv192–iv237. doi:10.1093/annonc/mdy275
3. Duma N, Santana-Davila R, Molina JR. Non-small cell lung cancer: epidemiology, screening, diagnosis, and treatment. Mayo Clin Proc. 2019;94(8):1623–1640. doi:10.1016/j.mayocp.2019.01.013
4. Alexander M, Kim SY, Cheng H. Update 2020: management of non-small cell lung cancer. Lung. 2020;198(6):897–907. doi:10.1007/s00408-020-00407-7
5. Hirsch FR, Scagliotti GV, Mulshine JL, et al. Lung cancer: current therapies and new targeted treatments. Lancet. 2017;389(10066):299–311. doi:10.1016/S0140-6736(16)30958-8
6. Ramalingam SS, Vansteenkiste J, Planchard D, et al. Overall survival with osimertinib in untreated, EGFR-mutated advanced NSCLC. N Engl J Med. 2020;382(1):41–50. doi:10.1056/NEJMoa1913662
7. Reck M, Rodríguez-Abreu D, Robinson AG, et al. Pembrolizumab versus chemotherapy for PD-L1-Positive Non-Small-Cell lung cancer. N Engl J Med. 2016;375(19):1823–1833. doi:10.1056/NEJMoa1606774
8. Gandhi L, Rodríguez-Abreu D, Gadgeel S, et al. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N Engl J Med. 2018;378(22):2078–2092. doi:10.1056/NEJMoa1801005
9. Herbst RS, Arkenau HT, Santana-Davila R, et al. Ramucirumab plus pembrolizumab in patients with previously treated advanced non-small-cell lung cancer, gastro-oesophageal cancer, or urothelial carcinomas (JVDF): a multicohort, non-randomised, open-label, phase 1a/b trial. Lancet Oncol. 2019;20(8):1109–1123. doi:10.1016/S1470-2045(19)30458-9
10. Taylor MH, Lee CH, Makker V, et al. Phase IB/II trial of lenvatinib plus pembrolizumab in patients with advanced renal cell carcinoma, endometrial cancer, and other selected advanced solid tumors. J Clin Oncol. 2020;38(11):1154–1163. doi:10.1200/JCO.19.01598
11. Tian L, Goldstein A, Wang H, et al. Mutual regulation of tumour vessel normalization and immunostimulatory reprogramming. Nature. 2017;544(7649):250–254. doi:10.1038/nature21724
12. Kammertoens T, Friese C, Arina A, et al. Tumour ischaemia by interferon-γ resembles physiological blood vessel regression. Nature. 2017;545(7652):98–102. doi:10.1038/nature22311
13. Robert L, Ribas A, Hu-Lieskovan S. Combining targeted therapy with immunotherapy. Can 1+1 equal more than 2? Semin Immunol. 2016;28(1):73–80. doi:10.1016/j.smim.2016.01.001
14. Tang H, You T, Ge H, et al. Autophagy inhibition improves the efficacy of anlotinib and PD-1 inhibitors in the treatment of NSCLC. J Immunother Cancer. 2025;13(9):e010812. doi:10.1136/jitc-2024-010812
15. Robainas M, Otano R, Bueno S, et al. Understanding the role of PD-L1/PD1 pathway blockade and autophagy in cancer therapy. Onco Targets Ther. 2017;10:1803–1807. doi:10.2147/OTT.S132508
16. Li N, Zuo R, He Y, et al. PD-L1 induces autophagy and primary resistance to EGFR-TKIs in EGFR-mutant lung adenocarcinoma via the MAPK signaling pathway. Cell Death Dis. 2024;15(8):555. doi:10.1038/s41419-024-06945-7
17. Han B, Li K, Wang Q, et al. Effect of anlotinib as a third-line or further treatment on overall survival of patients with advanced non-small cell lung cancer: the ALTER 0303 phase 3 randomized clinical trial. JAMA Oncol. 2018;4(11):1569–1575. doi:10.1001/jamaoncol.2018.3039
18. Horn L, Spigel DR, Vokes EE, et al. Nivolumab versus docetaxel in previously treated patients with advanced non-small-cell lung cancer: two-year outcomes from two randomized, open-label, phase III trials (CheckMate 017 and CheckMate 057). J Clin Oncol. 2017;35(35):3924–3933. doi:10.1200/JCO.2017.74.3062
19. Fu M, Zhao J, Zhang L, et al. Overcoming tyrosine kinase inhibitor resistance in lung cancer brain metastasis with CTLA4 blockade. Cancer Cell. 2024;42(11):1882–1897. doi:10.1016/j.ccell.2024.09.012
20. Zhou HQ, Zhang YX, Chen G, et al. Gefitinib (an EGFR tyrosine kinase inhibitor) plus anlotinib (an multikinase inhibitor) for untreated, EGFR-mutated, advanced non-small cell lung cancer (FL-ALTER): a multicenter phase III trial. Signal Transduct Target Ther. 2024;9(1):215. doi:10.1038/s41392-024-01927-9
21. Lu J, Shi Q. Zhang L, et al. Integrated transcriptome analysis reveals KLK5 and L1CAM predict response to anlotinib in NSCLC at 3rd line. Front Oncol. 2019;9:886. eCollection 2019. doi:10.3389/fonc.2019.00886
22. Pircher A, Wolf D, Heidenreich A, et al. Synergies of targeting tumor angiogenesis and immune checkpoints in non-small cell lung cancer and renal cell cancer: from basic concepts to clinical reality. Int J Mol Sci. 2017;18(11):2291. doi:10.3390/ijms18112291
23. Huang Y, Kim BYS, Chan CK, et al. Improving immune-vascular crosstalk for cancer immunotherapy. Nat Rev Immunol. 2018;18(3):195–203. doi:10.1038/nri.2017.136
24. Long J, Hu Z, Xue H, et al. Vascular endothelial growth factor (VEGF) impairs the motility and immune function of human mature dendritic cells through the VEGF receptor 2-RhoA-cofilin1 pathway. Cancer Sci. 2019;110(8):2357–2367. doi:10.1111/cas.14103
25. Qin S, Ren Z, Feng YH, et al. Atezolizumab plus bevacizumab versus sorafenib in the Chinese subpopulation with unresectable hepatocellular carcinoma: phase 3 randomized, open-label IMbrave150 study. Liver Cancer. 2021;10(4):296–308. doi:10.1159/000518271
26. Rini BI, Plimack ER, Stus V, et al. Pembrolizumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2019;380(12):1116–1127. doi:10.1056/NEJMoa1816714
27. Socinski MA, Jotte RM, Cappuzzo F, et al. Atezolizumab for first-line treatment of metastatic nonsquamous NSCLC. N Engl J Med. 2018;378(24):2288–2301. doi:10.1056/NEJMoa1716948
28. Reckamp KL, Redman MW, Dragnev KH, et al. Phase II randomized study of ramucirumab and pembrolizumab versus standard of care in advanced non-small-cell lung cancer previously treated with immunotherapy-Lung-MAP S1800A. J Clin Oncol. 2022;40(21):2295–2306. doi:10.1200/JCO.21.02502
29. Chu T, Zhong R, Zhong H, et al. Phase 1b study of sintilimab plus anlotinib as first-line therapy in patients with advanced NSCLC. J Thorac Oncol. 2021;16(4):643–652. doi:10.1016/j.jtho.2020.11.025
30. Yang S, Zhang W, Chen Q, et al. Clinical investigation of the efficacy and safety of anlotinib with immunotherapy in advanced non-small cell lung cancer as third-line therapy: a retrospective study. Cancer Manag Res. 2020;12:10333–10340. doi:10.2147/CMAR.S27799
31. Garon EB, Ciuleanu TE, Arrieta O, et al. Ramucirumab plus docetaxel versus placebo plus docetaxel for second-line treatment of stage IV non-small-cell lung cancer after disease progression on platinum-based therapy (REVEL): a multicentre, double-blind, randomised phase 3 trial. Lancet. 2014;384(9944):665–673. doi:10.1016/S0140-6736(14)60845-X
32. Reck M, Kaiser R, Mellemgaard A, et al. Docetaxel plus nintedanib versus docetaxel plus placebo in patients with previously treated non-small-cell lung cancer (LUME-Lung 1): a phase 3, double-blind, randomised controlled trial. Lancet Oncol. 2014;15(2):143–155. doi:10.1016/S1470-2045(13)70586-2
33. Hanna NH, Kaiser R, Sullivan RN, et al. Nintedanib plus pemetrexed versus placebo plus pemetrexed in patients with relapsed or refractory, advanced non-small cell lung cancer (LUME-Lung 2): a randomized, double-blind, phase III trial. Lung Cancer. 2016;102:65–73. doi:10.1016/j.lungcan.2016.10.007
34. Paz-Ares L, Hirsh V, Zhang L, et al. Monotherapy administration of sorafenib in patients with non-small cell lung cancer (MISSION) trial: a Phase III, multicenter, placebo-controlled trial of sorafenib in patients with relapsed or refractory predominantly nonsquamous non-small-cell lung cancer after 2 or 3 previous treatment regimens. J Thorac Oncol. 2015;10(12):1745–1753. doi:10.1097/JTO.0000000000000723
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Long-Term Efficacy and Safety of Anlotinib as a Monotherapy and Combined Therapy for Advanced Sarcoma
Yao W, Du X, Wang J, Wang X, Zhang P, Niu X
OncoTargets and Therapy 2022, 15:669-679
Published Date: 14 June 2022
The Efficacy and Safety of Anlotinib in Extensive-Stage Small Cell Lung Cancer: A Multicenter Real-World Study
Zheng HR, Jiang AM, Gao H, Liu N, Zheng XQ, Fu X, Zhang R, Ruan ZP, Tian T, Liang X, Yao Y
Cancer Management and Research 2022, 14:2273-2287
Published Date: 2 August 2022
Emerging Therapeutic Strategies of Different Immunotherapy Approaches Combined with PD-1/PD-L1 Blockade in Cervical Cancer
Ge Y, Zhang Y, Zhao KN, Zhu H
Drug Design, Development and Therapy 2022, 16:3055-3070
Published Date: 9 September 2022
Anlotinib Hydrochloride and PD-1 Blockade as a Salvage Second-Line Treatment in Patients with Progress of Local Advanced Non-Small Cell Lung Cancer in Half a Year After Standard Treatment
Yu C, Jiang L, Yang D, Dong X, Yu R, Yu H
OncoTargets and Therapy 2022, 15:1221-1228
Published Date: 17 October 2022
The Path to Personalized Treatment in KRAS-Mutant Non-Small Cell Lung Cancer: A Review of Targeted Therapies and Immunotherapy
Shu CL, Liu YL
Cancer Management and Research 2022, 14:3485-3492
Published Date: 16 December 2022