Back to Journals » Journal of Inflammation Research » Volume 18
A Novel NPR48-Based Model for Early Prediction of Severe Acute Pancreatitis: Development and Multicenter Validation in Comparison with Traditional Clinical Scores
Received 2 June 2025
Accepted for publication 30 September 2025
Published 15 October 2025 Volume 2025:18 Pages 14307—14324
DOI https://doi.org/10.2147/JIR.S544209
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Tara Strutt
Kaier Gu,1 Lianmin Ye2
1Department of Internal Medicine, Shaoxing Maternity and Child Health Care Hospital, Shaoxing, Zhejiang, People’s Republic of China; 2Department of Intensive Care Unit, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China
Correspondence: Lianmin Ye, Department of Intensive Care Unit, The First Affiliated Hospital of Wenzhou Medical University, Nanbaixiang Street, Luchen Qu, Wenzhou, 325000, People’s Republic of China, Email [email protected]
Background: Acute pancreatitis (AP) is associated with significant morbidity and mortality when progressing to severe acute pancreatitis (SAP). Timely and accurate prediction of SAP remains challenging due to the limitations of existing clinical scoring systems in terms of sensitivity, specificity, and operational practicality. Inflammatory indices derived from routine blood tests have emerged as promising alternatives, though dynamic monitoring beyond admission remains underexplored.
Purpose: This study aimed to evaluate dynamic changes in inflammatory indices at admission and 48 hours post-admission in AP patients, investigate their predictive capacity for SAP development, and establish a novel predictive model.
Patients and Methods: A retrospective analysis was conducted on 343 AP patients, including 76 SAP and 267 non-SAP cases. Blood routine parameters were collected at admission and 48 hours thereafter. The roles of the neutrophil-to-lymphocyte ratio (NLR), neutrophil-to-platelet ratio (NPR), systemic inflammation response index (SIRI), and other inflammatory indices in AP were analyzed and compared with six traditional clinical scores. Feature selection was performed using LASSO regression, followed by the construction of a multivariate logistic regression model. The model was evaluated via receiver operating characteristic curves, calibration curves, and decision curve analysis.
Results: The SAP group showed significant elevations in NLR0, NLR48, NPR0, NPR48, NPR48/NPR0, SIRI48, and SIRI48/SIRI0. Among these, NPR48 exhibited the highest predictive performance for SAP, comparable to the Ranson score. The NPR48-based nomogram achieved an AUC of 0.905, with 86.8% sensitivity and 82.4% specificity, significantly outperforming all clinical scores.
Conclusion: Dynamic monitoring of NPR, particularly its value at 48 hours post-admission (NPR48), significantly improves early SAP detection. Through LASSO regression for feature selection, we developed and validated a novel NPR48-based nomogram that combines NPR48 with other relevant clinical variables. This tool is efficient, cost-effective, and readily applicable in clinical settings for warning of SAP.
Keywords: acute pancreatitis, severe acute pancreatitis, inflammatory indices, prediction model, NPR48
Introduction
Acute pancreatitis (AP) is a clinical syndrome characterized by acute inflammation of the pancreas and associated systemic pathological responses, with an estimated annual global incidence of approximately 34 cases per 100,000 individuals.1 The predominant etiological factors contributing to AP include gallstones, chronic alcohol abuse, and hyperlipidemia.2 Based on the revised Atlanta classification system, AP can be categorized into mild acute pancreatitis (MAP), moderately severe acute pancreatitis, and severe acute pancreatitis (SAP), each exhibiting distinct prognostic profiles. Notably, approximately 70%–80% of patients present with MAP, which typically follows a self-limiting course and is associated with a mortality rate of less than 1%. Conversely, 15%–20% of patients progress to SAP, often accompanied by persistent organ dysfunction or infectious complications, resulting in mortality rates ranging from 20% to 40%.3,4 Consequently, the timely identification of high-risk patients for SAP is critical for predicting disease development trends and adjusting therapeutic strategies.5
Currently, the severity assessment of AP primarily relies on clinical scoring systems, including the Ranson, Systemic Inflammatory Response Syndrome (SIRS), Bedside Index for Severity in Acute Pancreatitis (BISAP), Modified Marshall Score, Acute Physiology And Chronic Health Evaluation II (APACHE II), and Sequential Organ Failure Assessment (SOFA).6,7 Nevertheless, these systems exhibit notable limitations in clinical application. The Ranson score requires data collected at admission and 48 hours later. Its complex process and low early sensitivity limit its usefulness for early detection. The SIRS score is quick to apply but lacks specificity, often leading to overestimation of severity. BISAP is simple and uses data from the first 24 hours, but it is not sensitive enough for identifying SAP. The Modified Marshall Score assesses organ dysfunction and helps monitor disease progression. However, it requires multiple complex measurements, making it difficult to apply consistently. APACHE II provides comprehensive evaluation for critically ill patients but is impractical due to its complexity and data demands. SOFA tracks organ function changes during hospitalization and was designed for sepsis; it is less effective in early AP prediction. In summary, these scoring systems have shortcomings in early sensitivity, specificity, or ease of use. This highlights the need to investigate more efficient predictive indicators.8
In recent years, numerous studies have suggested the application of laboratory-based markers to assess the severity of AP.9–11 Notably, inflammatory indices derived from routine blood tests, characterized by their rapidity and cost-effectiveness, have emerged as a research focus.12,13 The progression of SAP involves the release of numerous inflammatory mediators, which trigger a cascade of inflammatory responses, resulting in bacterial translocation and secondary damage to distant organs. Consequently, utilizing inflammation-related indicators to predict the likelihood of SAP development appears justified.
The neutrophil-to-lymphocyte ratio (NLR) has been consistently recognized as a reliable marker for predicting both inflammatory progression and pancreatitis severity, and it is recommended as an early predictor of AP.14–16 Beyond NLR, other inflammatory indices include the systemic immune-inflammation index (SII), platelet-to-lymphocyte ratio (PLR), lymphocyte-to-monocyte ratio (LMR), neutrophil-to-platelet ratio (NPR), and systemic inflammation response index (SIRI).
The majority of existing studies concentrate on the blood profile at admission, whereas there is a paucity of research focusing on dynamic monitoring of the blood profile post-admission.13 Nevertheless, inflammatory indices at admission may still be in their early ascending phase, and a single measurement might underestimate the actual risk while overlooking critical trends.17 A dynamic evaluation conducted at two distinct time points can more precisely reflect the characteristics of inflammatory kinetics, thereby providing a robust basis for risk stratification. Furthermore, calculating the ratio between the blood profiles at admission and post-admission could theoretically mitigate the impact of individual variability.
The severity of AP generally does not become fully apparent at the time of admission. Instead, it is a dynamically evolving process. During the early phase of the disease (0–24 hours), it is primarily characterized by the initiation of local inflammatory responses, and systemic symptoms remain inconspicuous. Subsequently, a significant quantity of inflammatory mediators is released into the bloodstream, which triggers the SIRS and organ dysfunction. The peak of this pathological process typically occurs between 24 and 72 hours. Consequently, the 48-hour time point serves as a crucial transition window from local inflammation to systemic damage. Clinical parameters obtained at this time point can more precisely reflect the severity of the disease and the prognosis trends compared to evaluations conducted at earlier stages (such as within 12–24 hours). Moreover, the 48-hour time point coincides with the critical decision-making time recommended in current major clinical guidelines for re-evaluating the severity of AP and adjusting treatment strategies.18,19
This study aims to systematically assess the dynamic changes in inflammatory factors at two specific time points (at admission and 48 hours thereafter) among patients with acute pancreatitis, as well as to elucidate their association with the progression of SAP. Additionally, this study investigates whether integrating inflammatory indices into predictive models enhances the specificity of SAP identification. The results of this study are anticipated to offer clinicians an objective decision-making foundation based on dynamic blood testing, enabling timely recognition of inflammation signals and adjusting treatment strategies, ultimately improving patient outcomes.
Materials and Methods
Study Population
The study retrospectively reviewed the electronic medical records of patients from the Department of Gastroenterology at the First Affiliated Hospital of Wenzhou Medical University.
Inclusion Criteria: Patients diagnosed with AP between January 2016 and December 2023 were included in the study. Exclusion Criteria: 1. Ages below 18 years or above 80 years; 2. Time from symptom onset to hospital admission exceeding 72 hours; 3. Other possible causes of pancreatic disease (eg, chronic pancreatitis, trauma, pregnancy-related pancreatitis, or pancreatic cancer); a history of previous pancreatic surgery; 4. A history of severe cardiovascular, pulmonary, hepatic, or renal diseases; 5. A history of immune or hematological disorders; 6. A history of malignancies, chemotherapy, or radiation therapy; 7. Hospital stays shorter than 48 hours; 8. Insufficient clinical documentation or incomplete medical records. Ultimately, a total of 343 AP patients met the inclusion criteria and were included in the study (Figure 1).
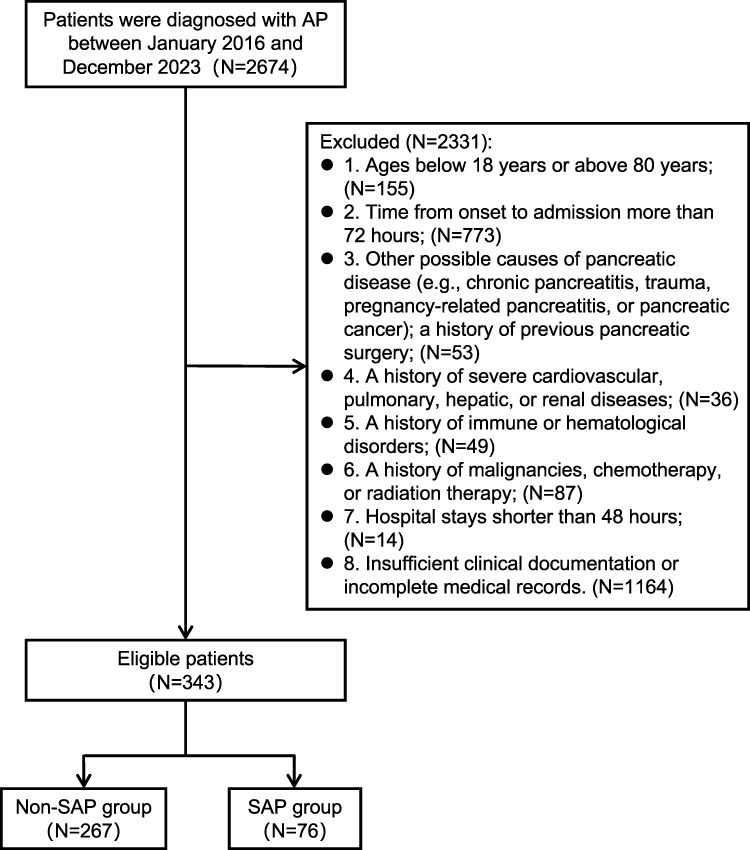 |
Figure 1 Flow chart of study inclusions and exclusions. Abbreviations: AP, acute pancreatitis; SAP, severe acute pancreatitis. |
Data Collection
The electronic medical records of patients from the First Affiliated Hospital of Wenzhou Medical University were retrospectively reviewed. Based on existing literature and prior clinical experience, we collected patient data at admission, including demographic information (age, gender, BMI, medical history), laboratory test results upon admission, and blood counts within 48 hours post-admission.
The SII, NLR, PLR, LMR, NPR, and SIRI were calculated based on the medical records.12 SII was calculated as the neutrophil counts multiplied by the platelet counts and divided by the lymphocyte counts. NLR was calculated as the neutrophil counts divided by the lymphocyte counts. PLR was calculated as the platelet counts divided by the lymphocyte counts. LMR was calculated as the lymphocyte counts divided by the monocyte counts. NPR was calculated as the neutrophil counts multiplied by 1000 and divided by the platelet counts. SIRI was calculated as the neutrophil counts multiplied by the monocyte counts and divided by the lymphocyte counts. All cell counts are expressed in 109/L.
Commonly used clinical scores for predicting the severity of AP were also calculated using the medical records, including the Ranson, SIRS, BISAP, Modified Marshall Score, APACHE II, and SOFA.
The primary outcome measure was the incidence of SAP. The secondary outcome measure was the length of hospital stay.
Definition and Diagnostic Criteria
Two or more of the following three requirements must be met in order to diagnose AP, under the 2012 revisions to the Atlanta criteria:20 (a) Persistent upper abdominal pain; (b) Characteristic imaging findings of AP; (c) Serum amylase and/or lipase levels were elevated to at least three times the upper limit of normal.
The severity of AP is classified as follows: (a) Mild acute pancreatitis, which is characterized by the absence of both local complications and organ failure; (b) Moderate-severity acute pancreatitis, defined by the presence of transient organ failure (<48 hours) and/or local complications; (c) Severe acute pancreatitis, characterized by persistent organ failure (≥48 hours), with or without associated local complications.
Organ failure was determined using the Modified Marshall Score System, which evaluates the respiratory, renal, and cardiovascular functions. Organ failure is identified when the Modified Marshall Score reaches or exceeds two for any of these three systems. Local complications encompass acute peripancreatic fluid accumulation, acute necrotic collections, pancreatic pseudocysts, encapsulated necrosis, and infected pancreatic necrosis.
Etiological Classification
The etiological diagnostic criteria for AP are as follows: 1. Biliary acute pancreatitis (BAP) can be diagnosed if any of the following criteria are met:21 (a) Imaging examinations (eg, abdominal ultrasonography, computed tomography, magnetic resonance imaging, or magnetic resonance cholangiopancreatography) detect cholelithiasis, common bile duct stones, or cholestasis. (b) Alanine aminotransferase > 100 U/L and total bilirubin > 2.3 mg/dL in the absence of any other definitive explanation. 2. Hyperlipidemic acute pancreatitis (HLAP) can be diagnosed when either of the following conditions is met, and other definite etiologies are excluded:22 (a) Serum triglyceride levels are ≥11.3 mmol/L. (b) Serum triglyceride levels are 5.65–11.3 mmol/L and the serum appears chylous. 3. Alcoholic acute pancreatitis (AAP) can be diagnosed if there is a history of long-term and heavy alcohol consumption prior to the onset of the disease (for men >40–80 g/d; for women >40–60 g/d, either for over 5 years or with substantial intake over a shorter period), and other definite etiologies are ruled out.23 4. Other etiologies AP can be diagnosed in cases that do not fall into the above classifications. Through detailed history-taking, other definite causes are identified (eg, chronic pancreatitis, trauma, pregnancy-related pancreatitis, pancreatic cancer). 5. Idiopathic AP can be diagnosed if no definitive etiology can be identified from the aforementioned categories following a comprehensive initial assessment, which includes evaluation of medical history, laboratory tests, and imaging studies.
Exclusion of Other Etiologies AP
To minimize the interference of potential confounding factors to the greatest extent, other etiologies AP cases were excluded. The specific diagnostic process is as follows: For patients with a long-term history of abdominal pain, chronic pancreatitis can be diagnosed by integrating characteristic imaging findings (eg, pancreatic calcification and irregular dilation of the pancreatic duct). For patients with a clear history of abdominal trauma, traumatic pancreatic injury can be diagnosed by combining the imaging signs of pancreatic contusion or laceration. For all female AP patients of childbearing age, sexual history was routinely inquired about, and serum β-hCG detection was performed to diagnose whether pregnancy was complicated. For patients with pancreatic space-occupying lesions, initial evaluation was first carried out through computed tomography or magnetic resonance imaging. For highly suspicious cases, further endoscopic ultrasound-guided biopsy was performed to clarify the pathology, enabling the diagnosis of pancreatic cancer.
In conclusion, this study identified and excluded other conditions through a detailed systematic review and thorough examination of medical histories.
Treatment Protocol
All AP patients were managed according to the latest Chinese guidelines for AP.24,25 Core treatments included early fluid resuscitation, pain management, nutritional support, and treatment of complications. Intensive care unit (ICU) admission criteria were based on guideline recommendations and included persistent organ failure (respiratory, circulatory, or renal), the need for organ support (eg, invasive mechanical ventilation or blood purification), sepsis or septic shock, and other severe complications (eg, abdominal compartment syndrome).
Study Groups
In this study, all AP patients (N = 343) were categorized into two groups according to the occurrence of SAP: the Non-SAP group (N = 267) and the SAP group (N = 76). They were also categorized into three groups according to etiology: BAP group (N = 163), HLAP group (N = 102), and the combined group of AAP and idiopathic AP (N = 78).
Data Processing
The sample size of this study was estimated based on the incidence of SAP (15–20%) reported in previous literature.3 Setting α = 0.05 and β = 0.20 (statistical power of 80%), the minimum sample size required was calculated to be 300 cases. In this study, 343 patients were enrolled ultimately. This sample size meets the requirements of statistical test power, ensuring the robustness of the model and the reliability of the research findings.
Variables with a missing rate exceeding 25% were excluded from the analysis. For variables with a missing rate between 5% and 25%, multiple imputation was employed to replace missing values. For variables with a missing rate below 5%, single imputation (mode or median) was utilized to address missing data (Table S1). To assess the influence of imputation on the NPR48-based model, the model was retrained using a complete-case dataset, which was generated by excluding all instances with missing values. The results showed an area under the curve (AUC) of 0.903, differing by less than 0.03 from the original result, with the significance direction and effect size of all key variables remaining unchanged (Table S2). This indicates that the imputation process did not alter the underlying data relationships, confirming the robustness of the primary findings.
Construction and Evaluation of the Model
This study evaluated a total of 34 clinical and inflammatory indices, including NPR48, as potential predictive variables. Given the high dimensionality of the dataset, Least Absolute Shrinkage and Selection Operator (LASSO) regression was employed to perform variable selection. This approach applies an L1 penalty to the regression coefficients, thereby enabling model regularization and the identification of key predictors. Compared to conventional stepwise regression methods, LASSO demonstrates improved stability in handling high-dimensional data and helps prevent overfitting while enhancing model generalizability. The variables selected by LASSO were incorporated into a multivariate logistic regression model to construct the predictive model.
The discriminatory ability of different inflammatory indices, clinical scores, and the predictive model was evaluated using the receiver operating characteristic (ROC) curve, AUC, and confusion matrices. The optimal cutoff value for the predictive model was determined using the Youden index. Model calibration was evaluated via calibration curves and the Hosmer–Lemeshow test, while clinical utility was assessed using decision curve analysis (DCA).
Statistical Analysis
The normality of continuous variables was assessed using the Kolmogorov–Smirnov test. For normally distributed variables, differences between groups were evaluated using the independent samples T-test; for non-normally distributed variables, the Mann–Whitney U-test was applied. Normally distributed variables were presented as mean ± standard deviation, while non-normally distributed variables were expressed as median (interquartile range). Categorical variables were analyzed using the chi-square test or Fisher’s exact test, as appropriate, and reported as frequency (percentage).
All statistical analyses and data visualizations were performed using R (version 4.4.2). A P-value less than 0.05 was regarded as statistically substantive.
Results
Baseline Characteristics of Patients
Based on the inclusion and exclusion criteria, a total of 343 patients were included in this study, with 76 (22.2%) classified into the SAP group and 267 (77.8%) into the Non-SAP group. The baseline characteristics of the patients are presented in Table 1. In the overall cohort, the mean age was 47 years, with males comprising 69.7% of the population, and the average BMI was 25.34 kg/m2.
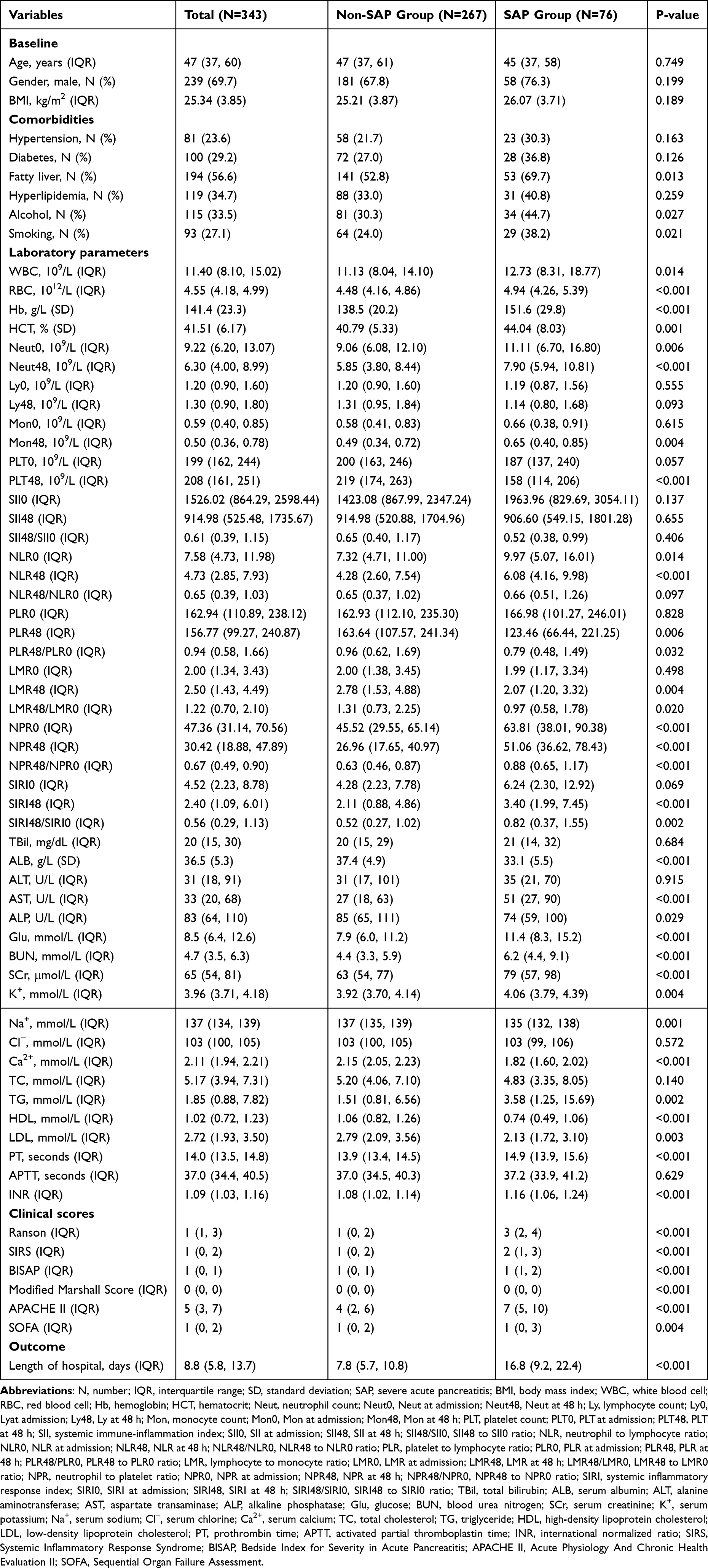 |
Table 1 Characteristics of Patients Between Non-SAP Group and SAP Group |
Intergroup comparisons between the SAP and Non-SAP groups revealed that the SAP group had significantly higher proportions of alcohol consumption (44.7% vs 30.3%, P = 0.027), smoking (38.2% vs 24.0%, P = 0.021), and fatty liver disease (69.7% vs 52.8%, P = 0.013). Laboratory findings indicated that the SAP group exhibited more pronounced inflammatory responses (white blood cell, P < 0.05), blood concentration (increased red blood cell, hemoglobin, and hematocrit, all P < 0.01), metabolic disturbances (elevated glucose, blood urea nitrogen, and TG, and reduced high-density lipoprotein cholesterol, all P < 0.01), and organ dysfunction (increased aspartate transaminase and serum creatinine, and decreased serum albumin, all P < 0.001). Coagulation parameters (prothrombin time, international normalized ratio) and electrolyte levels (serum potassium, serum sodium, serum calcium) were also significantly altered in the SAP group (all P < 0.01). Furthermore, the hospital stay for the SAP group was nearly twice as long compared to the Non-SAP group (16.8 days vs 7.8 days, P < 0.001). These findings indicate that SAP patients experience more severe systemic inflammation, metabolic abnormalities, and multi-organ dysfunction.
Comparison of Inflammatory Indices and Clinical Scores Between Groups
This study systematically analyzed and compared the differences in inflammatory indices and clinical scores between the Non-SAP group and the SAP group (Table 1). The findings demonstrated that the severity of AP was significantly associated with most inflammatory indices and all clinical scores.
Regarding inflammatory indices, the NLR0 and NLR48 values in the SAP group were higher than those in the Non-SAP group (P < 0.05). Furthermore, the NPR0 and NPR48 levels in the SAP group were markedly elevated compared to the Non-SAP group (P < 0.001). The SIRI48 value in the SAP group was significantly increased (P < 0.001), whereas PLR48 and LMR48 were notably reduced (P < 0.01). Dynamic analysis indicated that the ratios of NPR48/NPR0 and SIRI48/SIRI0 in the SAP group were significantly higher than those in the Non-SAP group (P < 0.005), suggesting a more persistent inflammatory response in SAP patients. Notably, NPR was the sole marker that exhibited significant increases both at admission and 48 hours post-admission in the SAP group, with a pronounced difference in its dynamic ratio.
In terms of clinical scoring, all clinical scores revealed that the SAP group had significantly higher scores than the Non-SAP group (P < 0.005). Among these, the Ranson and APACHE II showed particularly significant differences (all P < 0.001), indicating more severe systemic inflammation and organ dysfunction in SAP patients.
In conclusion, SAP patients displayed a stronger systemic inflammatory response (eg, elevated NLR, NPR, and SIRI) and an imbalance in immune regulation (eg, decreased PLR48 and LMR48). These results suggest that inflammatory indices may serve as potential predictors of AP severity. Moreover, traditional clinical scores (eg, Ranson and APACHE II) effectively differentiate disease severity. Combining dynamic monitoring of inflammatory indices with classical clinical scores could provide a foundation for the timely identification of severe pancreatitis and optimization of intervention strategies.
Performance Evaluation of Inflammatory Indices in Predicting the Severity of AP
To evaluate the effectiveness of inflammatory indices in predicting the severity of AP, this study calculated the AUC values for various inflammatory indices and clinical scores (Table 2) and generated the ROC curve (Figure 2). Through comprehensive analysis of multiple indicators, superior parameters were identified from among the inflammatory indices and clinical scores.
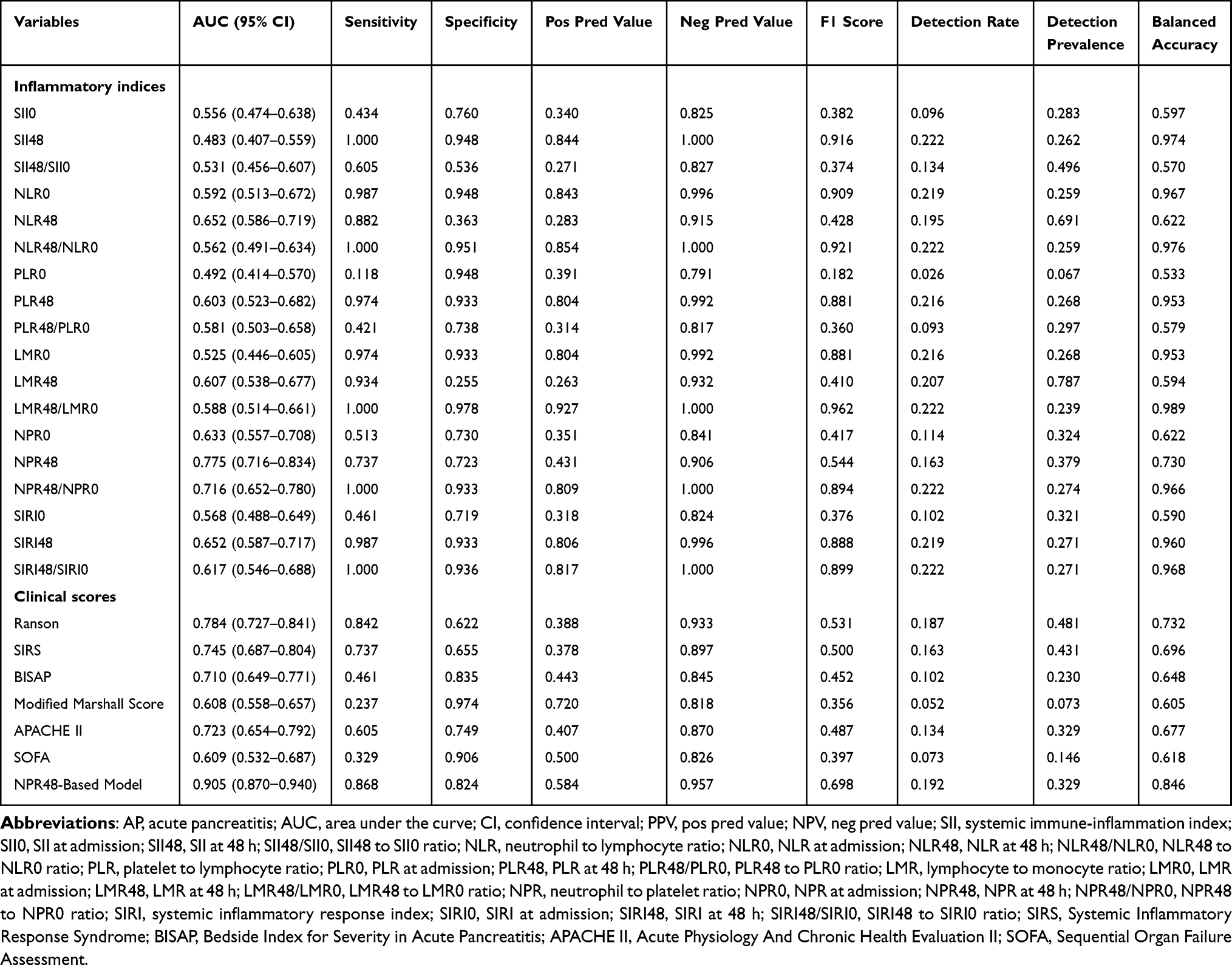 |
Table 2 Comparison of Diagnostic Performance for Predicting Different Severities of AP Between Inflammatory Indices and Scoring Systems |
 |
Figure 2 Comparison of ROC curve analyses for NPRs and clinical scores. (A) ROC curves for NPRs. (B) ROC curves for clinical scores. Abbreviations: ROC, receiver operating characteristic; AUC, area under the curve; NPR, neutrophil to platelet ratio; NPR0, NPR at admission; NPR48, NPR at 48 h; NPR48/NPR0, NPR48 to NPR0 ratio; SIRS, Systemic Inflammatory Response Syndrome; BISAP, Bedside Index for Severity in Acute Pancreatitis; APACHE II, Acute Physiology And Chronic Health Evaluation II; SOFA, Sequential Organ Failure Assessment. |
Among the inflammatory indices, NPR48 demonstrated the highest AUC value [0.775; 95% confidence Interval (CI): 0.716–0.834] compared to all other indicators. Its sensitivity (73.7%) and specificity (72.3%) were well-balanced, with a balanced accuracy of 0.730 and a neg pred value (NPV) of 0.906, indicating its potential for continuous monitoring, particularly for early-stage risk stratification. However, its pos pred value (PPV) (0.431) and F1 score (0.544) suggest that positive results should be interpreted in conjunction with clinical context. The AUC of NPR48/NPR0 was 0.716 (95% CI: 0.652–0.780), also showing excellent predictive performance. Its sensitivity (1.00), specificity (0.933), F1 score (0.894), and balanced accuracy (0.966) were all at high levels, highlighting its ability to identify SAP patients with both high sensitivity and specificity. Despite its high specificity, which makes it suitable for scenarios requiring strict exclusion of non-SAP patients, its clinical utility may be limited in practice if false negatives are masked by high sensitivity, potentially leading to missed diagnoses of severe cases. Notably, the detection rate was only 0.222, which may restrict its applicability in early screening. Additionally, the detection prevalence of 0.274 suggests that its high sensitivity might result from sample bias or overfitting. Furthermore, as NPR48/NPR0 requires two measurements, it may delay decision-making in emergency settings and increase medical costs. Therefore, although NPR48/NPR0 performs well in terms of sensitivity and specificity, its limitations in AUC, reliance on baseline values, and operational complexity reduce its suitability as a core indicator. In contrast, NPR48’s high AUC, single-test convenience, and balanced sensitivity and specificity make it more appropriate for emergency settings, initial screening, and resource-limited environments. The AUC of SIRI48 was relatively low (0.652; 95% CI: 0.587–0.717), but its specificity (0.933), F1 score (0.888), PPV (0.806), and NPV (0.996) were all at high levels. This apparent contradiction may stem from data distribution bias or model overfitting to specific features, warranting further validation in multi-center studies. Similar observations were made for SIRI48/SIRI0. The AUC of NLR48 (0.652; 95% CI: 0.586–0.719) was relatively low, with a specificity of only 36.3% and a high false-positive rate (63.7%), severely limiting its independent application value. Similarly, the AUC values of NLR0 and NLR48/NLR0 were also low, indicating limited overall discrimination ability.
Among traditional clinical scores, the Ranson exhibited the highest AUC (0.784; 95% CI: 0.727–0.841). It excelled in sensitivity (0.842), effectively identifying high-risk patients with severe pancreatitis. However, its relatively low specificity (0.622) may lead to an elevated false-positive rate. Despite limitations in its F1 score (0.531) and PPV (0.388), it maintained stable balanced accuracy (0.732). Given its extensive clinical validation and ease of use, the Ranson remains a valuable reference for basic screening. The SIRS (AUC 0.745) offered the advantage of operational simplicity but suffered from insufficient specificity (0.655), making it less suitable as a primary tool. The APACHE II (AUC 0.723), with a sensitivity of 0.605 and specificity of 0.749, performed well in comprehensive assessments but was less practical due to its complexity.
In summary, among multiple inflammatory indices, NPR48 demonstrated the best predictive performance, comparable to the Ranson and superior to several other clinical scores. Moreover, NPR48 offers unparalleled advantages in terms of operational convenience, making it suitable as an initial screening indicator for SAP prediction.
Inflammatory Indices Predict the Severity of AP Across Different Etiologies
Further evaluation demonstrated that NPR48 exhibited superior performance compared to other inflammatory indices in predicting the risk of SAP among AP patients of varying etiologies (Table 3).
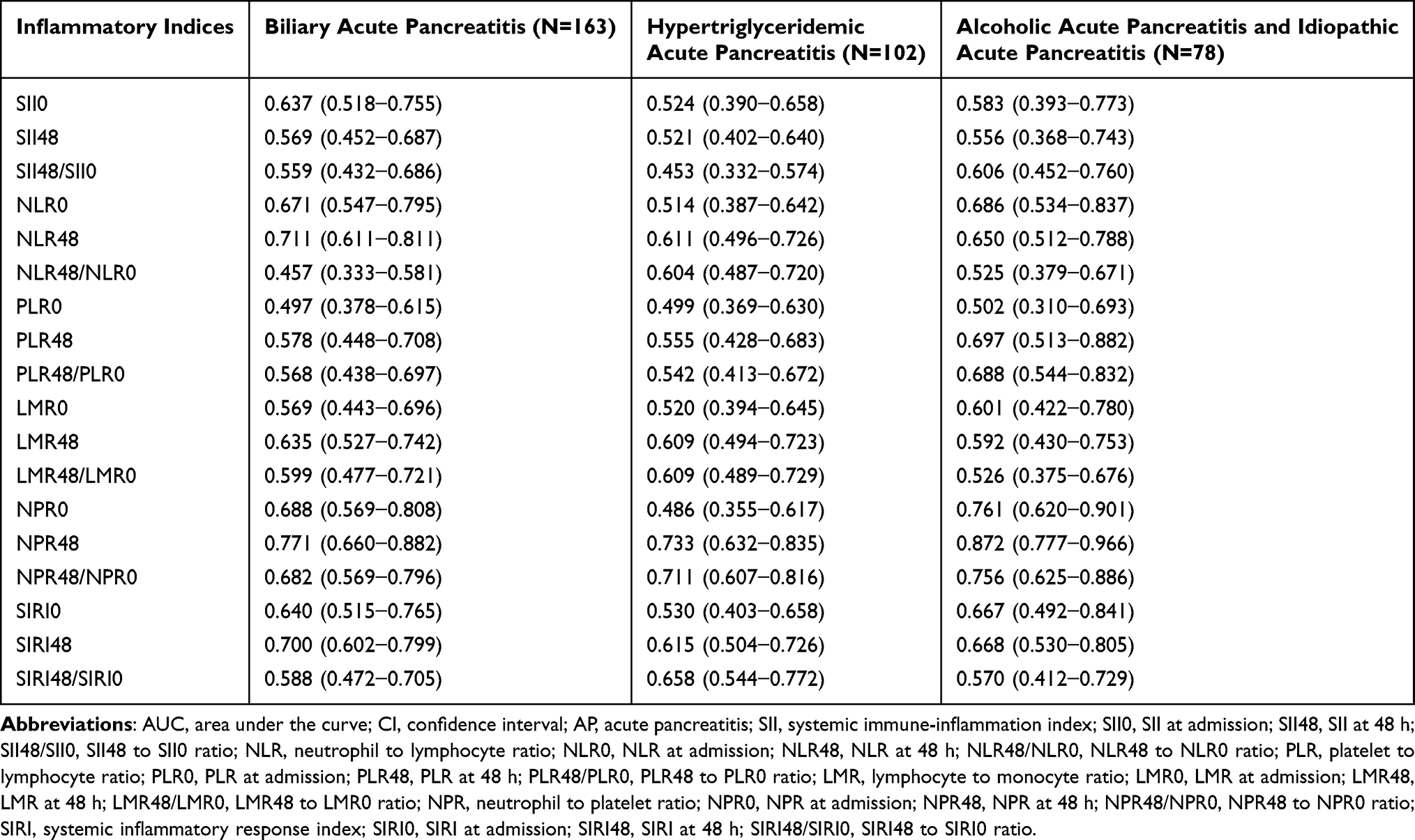 |
Table 3 Predictive Performance of Inflammatory Indices for SAP Risk Across Different Etiologies of AP |
Specifically, in the BAP group and the HLAP group, the AUC values of NPR48 were 0.771 and 0.733, respectively, indicating its excellent discriminatory ability. In the combined group of AAP and idiopathic AP, the AUC of NPR48 reached 0.872, showcasing particularly outstanding predictive performance. Notably, across all etiology groups, the AUC of NPR48 was consistently higher than its baseline value (NPR0) and dynamic change ratio (NPR48/NPR0), suggesting that the standalone assessment of NPR at 48 hours holds greater clinical significance. Furthermore, compared to other indicators, NPR48 exhibited a narrower CI range, providing additional support for the stability and reliability of its predictive results.
In conclusion, the AUC of NPR48 across all etiology groups was significantly higher than that of other indicators, such as SII48 and NLR48. These findings indicate that NPR48 demonstrates exceptional accuracy in stratifying SAP risk among AP patients with different etiologies and may serve as an important auxiliary predictive tool in clinical practice.
Construction of the NPR48-Based Model
Given the correlations among inflammatory indices, only NPR48 was selected for further investigation in conjunction with other common clinical indicators. The LASSO regression method was employed to include thirty-four clinical parameters for variable selection. The coefficients and corresponding log(λ) values are presented in Figure 3. When λ was set to 0.01225379, the minimum cross-validation error was identified, resulting in sixteen parameters with non-zero coefficients (age, body mass index, alcohol consumption, smoking history, fatty liver, red blood cell, platelet counts, serum albumin, aspartate transaminase, blood urea nitrogen, serum calcium, triglyceride, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, prothrombin time, NPR48). When λ was set to 0.04946878, the minimum cross-validation error within one standard error was identified, yielding five parameters with non-zero coefficients (hemoglobin, blood urea nitrogen, serum calcium, prothrombin time, NPR48).
 |
Figure 3 Variable selection using the LASSO regression approach. (A) Coefficient values of 34 variables plotted against log(λ). (B) The left vertical dashed line indicates the point with the lowest cross-validation error, while the right vertical dashed line represents the position corresponding to the minimum error plus one standard deviation. Abbreviation: LASSO, Least Absolute Shrinkage and Selection Operator. |
Using these five parameters with non-zero coefficients, a multi-factor logistic regression algorithm was applied to construct an NPR48-based model for predicting the severity of AP (Table 4).
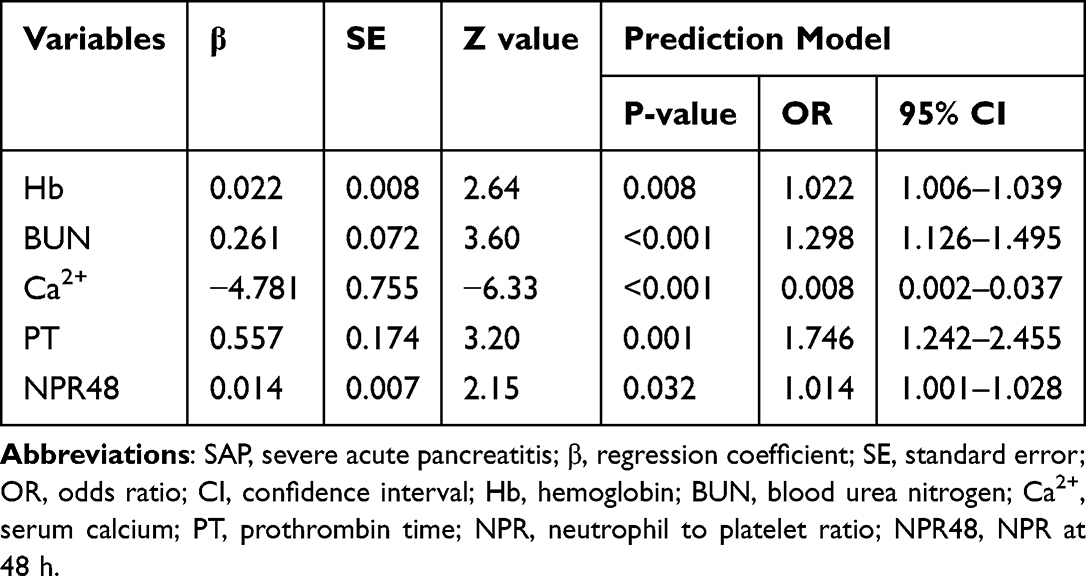 |
Table 4 Multivariate Logistic Regression Analysis of the Predictors of SAP |
Figure 4 presents the static and dynamic nomograms of the NPR48-based model (https://npr48.shinyapps.io/DynNomapp/), respectively. The total score is calculated by summing up the scores of each variable in the nomogram. The total score is computed by summing up the scores of each variable within the nomogram. The probability corresponding to this total score represents the probability of patients with AP will progress to SAP.
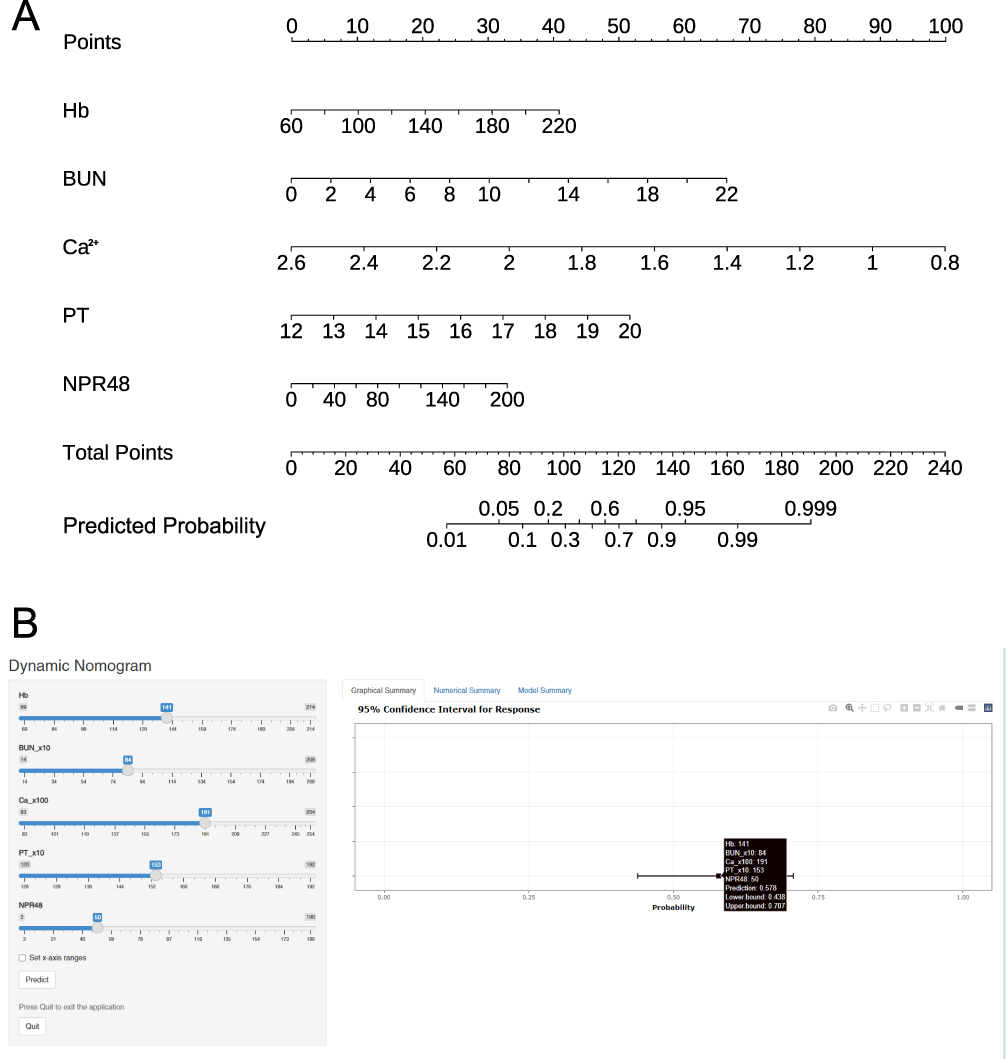 |
Figure 4 Nomograms for predicting the incidence of severe acute pancreatitis rate in acute pancreatitis patients. (A) A static nomogram. (B) A dynamic online nomogram. Abbreviations: Hb, hemoglobin; BUN, blood urea nitrogen; Ca2+, serum calcium; PT, prothrombin time; NPR, neutrophil to platelet ratio; NPR48, NPR at 48 h. |
Evaluation of the NPR48-Based Model’s Performance
As presented in Figure 5, the predictive performance of the NPR48-based model was appraised from three dimensions: discriminative ability, calibration, and clinical utility.
 |
Figure 5 Assessment of prediction accuracy and clinical applicability of the NPR48-based model. (A) ROC curve. (B) Calibration plot. (C) DCA curve. Abbreviations: NPR, neutrophil to platelet ratio; NPR48, NPR at 48 h; ROC, receiver operating characteristic; DCA, decision curve analysis; AUC, area under the curve. |
The AUC of the model was 0.905 (95% CI: 0.870–0.940), the sensitivity was 0.868, and the specificity was 0.824. Across multiple evaluation metrics, the model significantly outperformed single inflammatory indices or traditional clinical scores (Table 2), demonstrating exceptional discriminatory ability.
The calibration performance was satisfactory (Hosmer–Lemeshow test: χ² = 5.18, df = 8, p = 0.74), indicating good agreement between predicted and observed outcomes. The calibration curve confirmed this alignment visually.
DCA indicated that the predictive model could yield a relatively high net benefit rate across a broad range of threshold probabilities, highlighting its notable clinical utility.
Collectively, the NPR48-based model exhibited robust discriminative ability, substantial calibration performance, and favorable clinical utility.
The NPR48-based model demonstrates significantly superior performance compared to traditional clinical scores across multiple metrics for predicting AP severity, particularly in overall discrimination ability and the exclusion of non-severe cases.
In the ROC curve analysis of the NPR48-based model, 0.191 was identified as the optimal cut-off value. The corresponding sensitivity and specificity were 0.868 and 0.824, respectively. Based on the nomogram established with this model, the score corresponding to this cut-off value was 63. Accordingly, in this study, patients with a score of less than 63 were categorized into the low-risk group, while those with a score of 63 or above were grouped into the high-risk group. Figure S1 presents the probabilities of the incidence of SAP in patients from different risk groups, further validating the superiority of the NPR48-based model in predicting the severity of AP.
Discussion
Currently, the clinical scores used in clinical practice for predicting the risk of SAP each have certain limitations. The Ranson requires two evaluations—at admission and 48 hours later—and involves 11 parameters, which limits its practicality.26 The SIRS does not directly assess organ failure but only reflects systemic inflammatory status, resulting in low specificity and a high false-positive rate for SAP. The BISAP can be completed within 24 hours and requires only five parameters, offering high specificity but limited sensitivity.27
The Modified Marshall Score and SOFA include complex parameters such as blood gas analysis, requiring repeated testing and increasing clinical application costs and time consumption. The APACHE II is comprehensive but involves more than ten parameters and is computationally intensive.28 Therefore, identifying more efficient and convenient predictive indicators remains an urgent priority.
This study reveals that the predictive efficiency of NPR for SAP is significantly better than that of clinical scores and other inflammatory indices. The mechanism can be elucidated from the dynamic interaction between neutrophils and platelets in inflammation.
Neutrophils are the earliest immune cells to respond to inflammation and are typically considered as a signal of systemic inflammation.29 As the core effector cells of innate immunity, they directly engage in pathogen elimination through phagocytosis, the release of Neutrophil Extracellular Traps, and the secretion of inflammatory mediators. During the course of AP, neutrophils are excessively activated, releasing copious pro-inflammatory factors and proteolytic enzymes, which aggravate the self-digestion of the gland and the systemic inflammatory response.30
Platelets play a crucial role in the pathogenesis of inflammation-induced coagulation activation.31 Inflammation can directly activate platelets, resulting in platelet aggregation, adhesion to endothelial cells, and the release of inflammatory mediators, as well as facilitating further coagulation activation. Apart from regulating hemostasis, activated platelets are involved in microthrombosis formation and inflammation amplification by secreting mediators such as PF4 and P-selectin.32 Furthermore, activated platelets also participate in neutrophil accumulation and the increase of vascular permeability. Hence, systemic inflammation is often accompanied by a reduction in platelet quantity.33 In the course of AP, especially when it progresses to the SAP stage, platelets undergo progressive reduction due to excessive consumption and bone marrow suppression, and the contents released after their apoptosis further exacerbate tissue damage.
As a novel inflammatory index, NPR is capable of concurrently reflecting the subtle equilibrium between acute inflammatory responses and chronic inflammatory conditions. An elevation in neutrophils indicates the severity of acute inflammation, while a reduction in platelets might suggest previous chronic inflammation consumption or microcirculation issues in the body. When neutrophils are overly active, they stimulate platelet activation, form microthrombi and release more inflammatory substances, further aggravating the condition; conversely, a decrease in platelets would weaken the body’s capacity to control inflammation, creating a vicious cycle.34,35 Hence, NPR, as a marker of the dynamic interaction between neutrophils and platelets, integrates the “wax and wane” changes of both, not only avoiding the one-sidedness of a single indicator but also providing an earlier indication of the risk of disease deterioration. Some studies have pointed out that NPR is an effective index for assessing systemic inflammation in infective endocarditis.36 Moreover, NPR demonstrates excellent performance in detecting the disease activity of ulcerative colitis.37
Nevertheless, at present, there are scarce studies on whether NPR can predict the severity of AP. Li et al noted that SAP is correlated with higher levels of NPR.12 Based on the findings of our study, dynamic monitoring of NPR values up to 48 hours (NPR48) demonstrates significant advantages in predicting the severity of AP (AUC 0.775, 95% CI: 0.716–0.834), with balanced sensitivity (73.7%) and specificity (72.3%), outperforming NLR48 (AUC 0.652, 95% CI: 0.586–0.719). Compared to traditional clinical scores, NPR48 also shows significant superiority. Its accuracy in predicting the severity of AP surpasses both the SIRS (AUC 0.745, 95% CI: 0.687–0.804) and the BISAP (AUC 0.710, 95% CI: 0.649–0.771), while being comparable to the Ranson (AUC 0.784, 95% CI: 0.727–0.841).
This study, through etiological stratification analysis, found that NPR48 demonstrated excellent accuracy in predicting the severity of AP risk across different etiologies of AP. NPR48 exhibited the highest predictive value in the combined group of AAP and idiopathic AP, whose performance was superior to that in the BAP and HLAP groups. This phenomenon may be related to the distinct inflammatory driving mechanisms of AP with different etiologies. In AAP, ethanol metabolites (eg, acetaldehyde) directly activate neutrophils and induce oxidative stress, intensifying neutrophil activation and platelet consumption simultaneously. BAP is primarily characterized by secondary bacterial translocation due to bile duct obstruction, with higher neutrophil infiltration but relatively delayed thrombocytopenia due to slower local microthrombosis formation.38 In HLAP, the systemic inflammatory response is mainly mediated by lipotoxicity, where thrombocytopenia may result more from fat embolism than immune consumption. Additionally, HLAP patients often exhibit metabolic syndrome (eg, insulin resistance), which may interfere with NPR48 interpretation by affecting thrombopoietin levels.39 Notably, due to the small number of AAP cases in this study, these were combined with idiopathic AP, totaling 78 cases. The small sample size likely significantly impacts model predictive ability. Future studies should increase the sample size of AAP and explore multi-parameter models incorporating triglyceride levels (eg, dynamic monitoring of triglyceride values at 48 hours) or lipoprotein phenotypes to enhance predictive accuracy for this subgroup.
The core value of the NPR48-based model established in this study lies in its accurate prediction of the disease severity at the 48-hour mark after admission, a critical time window during which AP progresses from local inflammation to systemic injury. This model captures dynamic inflammatory changes and aligns with the recommended timing in clinical guidelines for re-evaluating patients and adjusting treatment strategies. Although the NPR48-based model does not predict SAP at initial admission, it provides timely and precise prognostic information 48 hours post-admission, facilitating clinical intervention. Compared with traditional clinical scores, the NPR48-based model not only delivers comparable predictive performance but also offers greater operational convenience by eliminating complex calculations. Relying solely on routine blood test parameters, it is feasible for implementation across various healthcare settings, including resource-limited regions. Its practicality and ease of use make it particularly suitable for emergency departments and primary care hospitals, where it can serve as an efficient complement to existing scoring systems.
This study has several limitations. Firstly, as a single-center retrospective study, it is subject to selection bias; strict inclusion and exclusion criteria led to a limited sample size, and the final cohort may not represent the entire population of AP patients, which also restricts the application of other machine learning algorithms. Secondly, the retrospective data did not distinguish between mild and moderate among non-SAP patients, nor did it establish a separate moderate group, limiting the grouping methodology. Thirdly, due to data acquisition constraints, this study did not include other key dynamic indicators (eg, C-reactive protein, procalcitonin), thus failing to construct a multi-dimensional early warning system. Additionally, to avoid interfering with the analysis results, patients discharged within 48 hours were excluded, which might introduce survivor bias. Moreover, due to restrictions in accessing mortality data and a relatively small number of ICU referral cases, the correlation between the model and mortality or ICU transfer rate could not be deeply analyzed. Finally, the model has a certain risk of overfitting, with a low positive predictive value in the high-risk group, and the calibration and discrimination performance still need to be optimized. The universality and the extrapolation of the conclusions need to be verified through larger-scale, multi-center prospective studies.
Although the NPR48-based model constructed in this study demonstrated good predictive performance, its applicability in clinical practice still needs further validation and optimization. In future research, we will enhance the robustness and generalization ability of the model from the following aspects: Firstly, we will collaborate with multiple medical institutions to conduct external validation in new and heterogeneous patient groups. Secondly, we will introduce a stricter k-fold cross-validation method to more accurately assess the model’s performance and reduce the risk of overfitting. Additionally, we will try various machine learning algorithms and compare them with the logistic regression model used in this study to select the model with better predictive performance. Finally, we will further optimize the selection of feature variables in combination with clinical significance to avoid introducing unnecessary noise from redundant variables.
Conclusion
Among various inflammatory indices, SAP was significantly associated with elevated NPR. Among the dynamic NPR indicators measured after admission, NPR48 (measured 48 hours post-admission) exhibited the best performance in predicting the severity of AP, surpassing both the SIRS and BISAP, and demonstrating a diagnostic accuracy comparable to the Ranson. In this study, an NPR48-based model was developed for the timely identification of SAP, incorporating five parameters: hemoglobin, blood urea nitrogen, serum calcium, prothrombin time, and NPR48. The model demonstrated excellent diagnostic capability. Future multicenter studies are warranted to further validate these findings.
Abbreviations
AP, acute pancreatitis; MAP, mild acute pancreatitis; SAP, severe acute pancreatitis; SIRS, Systemic Inflammatory Response Syndrome; BISAP, Bedside Index for Severity in Acute Pancreatitis; APACHE II, Acute Physiology And Chronic Health Evaluation II; SOFA, Sequential Organ Failure Assessment; NLR, neutrophil-to-lymphocyte ratio; SII, systemic immune-inflammation index; PLR, platelet-to-lymphocyte ratio; LMR, lymphocyte-to-monocyte ratio; NPR, neutrophil-to-platelet ratio; SIRI, systemic inflammation response index; BAP, biliary acute pancreatitis; HLAP, hyperlipidemic acute pancreatitis; AAP, alcoholic acute pancreatitis; ICU, intensive care unit; AUC, area under the curve; LASSO, Least Absolute Shrinkage and Selection Operator; ROC, receiver operating characteristic; DCA, decision curve analysis; CI, confidence Interval; NPV, neg pred value; PPV, pos pred value.
Data Sharing Statement
The data examined in this research were governed by the following licenses/restrictions: the datasets utilized and examined during the present study can be obtained from the corresponding author upon reasonable request. Inquiries regarding access to these datasets should be addressed to LY, [email protected].
Ethics Approval and Informed Consent
This retrospective study was conducted in accordance with the principles of the Declaration of Helsinki and received ethical approval from the Ethics Committee of the First Affiliated Hospital of Wenzhou Medical University. Since patient data were deidentified and aggregated before analysis, the Ethics Committee waived the requirement for informed consent.
Acknowledgments
The authors would like to express gratitude to all the patients and investigators who participated in this study.
Funding
The authors declare that no financial support was received for the research, authorship, and/or publication of this article.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Xiao AY, Tan ML, Wu LM, et al. Global incidence and mortality of pancreatic diseases: a systematic review, meta-analysis, and meta-regression of population-based cohort studies. Lancet Gastroenterol Hepatol. 2016;1(1):45–55. doi:10.1016/S2468-1253(16)30004-8
2. Roberts SE, Morrison-Rees S, John A, et al. The incidence and aetiology of acute pancreatitis across Europe. Pancreatology. 2017;17(2):155–165. doi:10.1016/j.pan.2017.01.005
3. Boxhoorn L, Voermans RP, Bouwense SA, et al. Acute pancreatitis. Lancet. 2020;396(10252):726–734. doi:10.1016/S0140-6736(20)31310-6
4. Van Santvoort HC, Bakker OJ, Bollen TL, et al. A conservative and minimally invasive approach to necrotizing pancreatitis improves outcome. Gastroenterology. 2011;141(4):1254–1263. doi:10.1053/j.gastro.2011.06.073
5. Mederos MA, Reber HA, Girgis MD. Acute pancreatitis: a review. JAMA. 2021;325(4):382–390. doi:10.1001/jama.2020.20317
6. Mounzer R, Langmead CJ, Wu BU, et al. Comparison of existing clinical scoring systems to predict persistent organ failure in patients with acute pancreatitis. Gastroenterology. 2012;142(7):1476–e16. doi:10.1053/j.gastro.2012.03.005
7. Capurso G, Ponz De Leon Pisani R, Lauri G, et al. Clinical usefulness of scoring systems to predict severe acute pancreatitis: a systematic review and meta-analysis with pre and post-test probability assessment. United Eur Gastroenterol J. 2023;11(9):825–836. doi:10.1002/ueg2.12464
8. Lee DW, Cho CM. Predicting severity of acute pancreatitis. Medicina. 2022;58(6):787.
9. Li S, Zhang Y, Li M, et al. Serum albumin, a good indicator of persistent organ failure in acute pancreatitis. BMC Gastroenterol. 2017;17(1):59. doi:10.1186/s12876-017-0615-8
10. Kumaravel A, Stevens T, Papachristou GI, et al. A model to predict the severity of acute pancreatitis based on serum level of amylase and body mass index. Clin Gastroenterol Hepatol. 2015;13(8):1496–1501. doi:10.1016/j.cgh.2015.03.018
11. Gong F, Zhou Q, Gui C, et al. Association of estimated glomerular filtration rate and all-cause mortality in acute pancreatitis: a retrospective analysis. BMC Anesthesiol. 2023;23(1):121. doi:10.1186/s12871-023-02074-4
12. Li X, Zhang Y, Wang W, et al. An inflammation-based model for identifying severe acute pancreatitis: a single-center retrospective study. BMC Gastroenterol. 2024;24(1):63. doi:10.1186/s12876-024-03148-4
13. Cazacu SM, Parscoveanu M, Cartu D, et al. NLR48 is better than CRP, and mCTSI, and similar to BISAP and SOFA scores for mortality prediction in acute pancreatitis: a comparison of 6 scores. J Inflamm Res. 2023;16:4793–4804. doi:10.2147/JIR.S432408
14. Azab B, Jaglall N, Atallah JP, et al. Neutrophil-lymphocyte ratio as a predictor of adverse outcomes of acute pancreatitis. Pancreatology. 2011;11(4):445–452. doi:10.1159/000331494
15. Han C, Zeng J, Lin R, et al. The utility of neutrophil to lymphocyte ratio and fluid sequestration as an early predictor of severe acute pancreatitis. Sci Rep. 2017;7(1):10704. doi:10.1038/s41598-017-10516-6
16. Wang Y, Fuentes HE, Attar BM, et al. Evaluation of the prognostic value of neutrophil to lymphocyte ratio in patients with hypertriglyceridemia-induced acute pancreatitis. Pancreatology. 2017;17(6):893–897. doi:10.1016/j.pan.2017.10.001
17. Mofidi R, Duff MD, Wigmore SJ, et al. Association between early systemic inflammatory response, severity of multiorgan dysfunction and death in acute pancreatitis. Br J Surg. 2006;93(6):738–744. doi:10.1002/bjs.5290
18. Ranson JH, Rifkind KM, Roses DF, et al. Prognostic signs and the role of operative management in acute pancreatitis. Surg Gynecol Obstet. 1974;139(1):69–81.
19. IAP WG, Guidelines AA. IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology. 2013;13(4 Suppl 2):e1–15. doi:10.1016/j.pan.2013.07.063
20. Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62(1):102–111. doi:10.1136/gutjnl-2012-302779
21. Van Geenen EJ, Van Der Peet DL, Bhagirath P, et al. Etiology and diagnosis of acute biliary pancreatitis. Nat Rev Gastroenterol Hepatol. 2010;7(9):495–502. doi:10.1038/nrgastro.2010.114
22. Scherer J, Singh VP, Pitchumoni CS, et al. Issues in hypertriglyceridemic pancreatitis: an update. J Clin Gastroenterol. 2014;48(3):195–203. doi:10.1097/01.mcg.0000436438.60145.5a
23. Yadav D, Whitcomb DC. The role of alcohol and smoking in pancreatitis. Nat Rev Gastroenterol Hepatol. 2010;7(3):131–145. doi:10.1038/nrgastro.2010.6
24. Chinese Pancreatic Surgery Association, Chinese Medical Association. Guidelines for diagnosis and treatment of acute pancreatitis in China (2021). Zhonghua Wai Ke Za Zhi. 2021;59(7):578–587. doi:10.3760/cma.j.cn112139-20210416-00172
25. Li J, Chen J, Tang W. The consensus of integrative diagnosis and treatment of acute pancreatitis-2017. J Evid Based Med. 2019;12(1):76–88. doi:10.1111/jebm.12342
26. Ong Y, Shelat VG. Ranson score to stratify severity in acute pancreatitis remains valid - Old is gold. Expert Rev Gastroenterol Hepatol. 2021;15(8):865–877. doi:10.1080/17474124.2021.1924058
27. Gao W, Yang HX, Ma CE. The value of BISAP score for predicting mortality and severity in acute pancreatitis: a systematic review and meta-analysis. PLoS One. 2015;10(6):e0130412. doi:10.1371/journal.pone.0130412
28. Papachristou GI, Muddana V, Yadav D, et al. Comparison of BISAP, Ranson’s, APACHE-II, and CTSI scores in predicting organ failure, complications, and mortality in acute pancreatitis. Am J Gastroenterol. 2010;105(2):435–442. doi:10.1038/ajg.2009.622
29. Irwin MR, Miller AH. Depressive disorders and immunity: 20 years of progress and discovery. Brain Behav Immun. 2007;21(4):374–383. doi:10.1016/j.bbi.2007.01.010
30. Segal AW. How neutrophils kill microbes. Annu Rev Immunol. 2005;23(1):197–223. doi:10.1146/annurev.immunol.23.021704.115653
31. García-Culebras A, Durán-Laforet V, Peña-Martínez C, et al. Myeloid cells as therapeutic targets in neuroinflammation after stroke: specific roles of neutrophils and neutrophil-platelet interactions. J Cereb Blood Flow Metab. 2018;38(12):2150–2164. doi:10.1177/0271678X18795789
32. Ho-Tin-Noé B, Demers M, Wagner DD. How platelets safeguard vascular integrity. J Thromb Haemost. 2011;9 Suppl 1(Suppl 1):56–65. doi:10.1111/j.1538-7836.2011.04317.x
33. Rossaint J, Margraf A, Zarbock A. Role of platelets in leukocyte recruitment and resolution of inflammation. Front Immunol. 2018;9:2712. doi:10.3389/fimmu.2018.02712
34. Zarbock A, Polanowska-Grabowska RK, Ley K. Platelet-neutrophil-interactions: linking hemostasis and inflammation. Blood Rev. 2007;21(2):99–111. doi:10.1016/j.blre.2006.06.001
35. Von Brühl ML, Stark K, Steinhart A, et al. Monocytes, neutrophils, and platelets cooperate to initiate and propagate venous thrombosis in mice in vivo. J Exp Med. 2012;209(4):819–835. doi:10.1084/jem.20112322
36. Wei XB, Liu YH, He PC, et al. The impact of admission neutrophil-to-platelet ratio on in-hospital and long-term mortality in patients with infective endocarditis. Clin Chem Lab Med. 2017;55(6):899–906. doi:10.1515/cclm-2016-0527
37. Warpechowski M, Warpechowski J, Pieńkowska A, et al. Neutrophil-to-platelet ratio in patients with ulcerative colitis treated with infliximab or vedolizumab: a retrospective, single-center study in Poland. Med Sci Monit. 2023;29:e938827. doi:10.12659/MSM.938827
38. Wan J, Ren Y, Yang X, et al. The role of neutrophils and neutrophil extracellular traps in acute pancreatitis. Front Cell Dev Biol. 2020;8:565758. doi:10.3389/fcell.2020.565758
39. Qiu M, Zhou X, Zippi M, et al. Comprehensive review on the pathogenesis of hypertriglyceridaemia-associated acute pancreatitis. Ann Med. 2023;55(2):2265939. doi:10.1080/07853890.2023.2265939
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Prediction Score for Early Diagnosis of Acute Pancreatitis in Emergency Departments
Liengswangwong W, Preechakul P, Yuksen C, Jenpanitpong C, Tienpratarn W, Watcharakitpaisan S
Open Access Emergency Medicine 2022, 14:355-366
Published Date: 26 July 2022
Establishment and Validation of a Nomogram Prediction Model for the Severe Acute Pancreatitis
Li B, Wu W, Liu A, Feng L, Li B, Mei Y, Tan L, Zhang C, Tian Y
Journal of Inflammation Research 2023, 16:2831-2843
Published Date: 8 July 2023
NLR48 is Better Than CRP, and mCTSI, and Similar to BISAP and SOFA Scores for Mortality Prediction in Acute Pancreatitis: A Comparison of 6 Scores
Cazacu SM, Parscoveanu M, Cartu D, Moraru E, Rogoveanu I, Ungureanu BS, Iordache S, Florescu DN, Iovanescu VF, Dragomir MI
Journal of Inflammation Research 2023, 16:4793-4804
Published Date: 20 October 2023