Back to Journals » Infection and Drug Resistance » Volume 19
A Nomogram Predictive Model for Drug-Resistant Tuberculosis Detection by GeneXpert MTB/RIF Assay in Paediatric Patients
Authors Wang L, Ma W, Wei N, Guo W, Zhao D, Zhou N, Guo X, Han M, Zhang F, Guo C, Li S
Received 12 June 2025
Accepted for publication 21 January 2026
Published 13 February 2026 Volume 2026:19 542863
DOI https://doi.org/10.2147/IDR.S542863
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Lingchao Wang,1,* Weiwei Ma,1,* Na Wei,1 Weijie Guo,2 Dean Zhao,1 Nan Zhou,1 Xiaonan Guo,1 Meigui Han,1 Fangmin Zhang,1 Can Guo,2 Shujun Li1
1Department of Pediatric, The First Affiliated Hospital of Henan Medical University (formerly The First Affiliated Hospital of Xinxiang Medical University), Weihui, 453100, People’s Republic of China; 2Department of Tuberculosis, The First Affiliated Hospital of Henan Medical University (formerly The First Affiliated Hospital of Xinxiang Medical University), Weihui, 453100, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shujun Li, Department of Pediatric, The First Affiliated Hospital of Henan Medical University (formerly The First Affiliated Hospital of Xinxiang Medical University), No. 88 of Jiankang Road, Weihui, Henan, 453100, People’s Republic of China, Tel +86 13781905766, Fax +86 0373-4402573, Email [email protected] Dean Zhao, Department of Pediatric, The First Affiliated Hospital of Henan Medical University (formerly The First Affiliated Hospital of Xinxiang Medical University), No. 88 of Jiankang Road, Weihui, Henan, 453100, People’s Republic of China, Tel +86 13781905766, Fax +86 0373-4402573, Email [email protected]
Objective: To develop and validate a clinical-imaging integrated nomogram predictive model for DR-TB risk in pediatric patients (≤ 18 years), and to evaluate the diagnostic performance of the GeneXpert MTB/RIF assay in this context.
Methods: This retrospective study included 223 patients with TB aged ≤ 18 years hospitalised between 1 July 2018 and 31 December 2023. Drug resistance profiles were analysed, and the clinical/imaging features of DR-TB were compared with those of drug-susceptible TB (DS-TB). Multivariate logistic regression was used to identify DR-TB risk factors.
Results: Of the 223 patients, 73.5% had DS-TB and 26.5% had DR-TB (including 13.5% with multidrug-resistant TB). Resistance rates to first-line drugs were as follows: isoniazid 22.4%, rifampicin 16.1%, streptomycin 8.1% and ethambutol 3.6%. Independent DR-TB risk factors were retreatment (odds ratio [OR] = 5.303, 95% confidence interval [CI]: 1.378– 20.414), smoking history (OR = 4.129, 95% CI: 1.233– 13.825), right middle lobe involvement (OR = 3.004, 95% CI: 1.148– 7.863) and cavity formation (OR = 2.950, 95% CI: 1.325– 6.567) (all P < 0.05). A nomogram model was developed, with an area under the curve of 0.776, showing effective predictive performance and clinical utility. The GeneXpert MTB/RIF assay had 87.5% sensitivity and 90.48% specificity for detecting rifampicin resistance, with good agreement with drug susceptibility testing (kappa 0.751) (P < 0.001). No significant differences in T-lymphocyte subsets were found between the DR-TB and DS-TB groups.
Conclusion: In children and adolescents, TB is more common in older individuals and consists primarily of new cases. The nomogram model has good predictive value for DR-TB risk. Key predictors include retreatment, smoking, right middle lobe involvement and cavity formation. The GeneXpert MTB/RIF assay is a potential early screening tool for DR-TB. Further validation with larger samples is needed.
Keywords: drug-resistant tuberculosis, GeneXpert MTB/RIF, Mycobacterium tuberculosis, nomogram predictive model, paediatric tuberculosis
Introduction
Tuberculosis (TB), caused by Mycobacterium tuberculosis (MTB), remains a major global public health threat. According to the World Health Organization (WHO) Global Tuberculosis Report 2023, approximately 10.6 million new TB cases were reported worldwide in 2022, of which 12% occurred in children and adolescents. Paediatric patients account for 16% of TB-related deaths, highlighting their higher risk of severe disease progression. 1 As one of the high TB burden countries, China ranks third globally in TB incidence (accounting for 7.1% of the global total). The growing prevalence of drug-resistant tuberculosis (DR-TB) has further complicated disease control efforts. Each year, an estimated 25,000–32,000 children worldwide develop multidrug-resistant tuberculosis (MDR-TB), defined as resistance to at least both isoniazid (INH) and rifampicin (RIF), comprising approximately 3% of all children and adolescents infected with TB.1,2 However, the diagnosis and treatment of paediatric DR-TB, particularly RIF-resistant TB (RR-TB), pose numerous challenges, such as nonspecific clinical manifestations, low bacterial load and difficulties in specimen collection, often leading to delayed diagnosis and treatment failure. Therefore, there is an urgent need to develop early warning tools based on clinical and imaging features to overcome the limitations of microbiological testing.
Most predictive studies on DR-TB have focused on adult populations. However, children and adolescents differ substantially from adults in epidemiological characteristics, mechanisms of drug resistance and immune responses. Previous studies have identified associations between DR-TB and factors such as history of retreatment, smoking, malnutrition and specific imaging features (eg multiple cavities, thick-walled cavities and extensive pulmonary involvement).3–5 Nevertheless, existing predictive models are often based on a single dimension, either clinical or imaging data, and population heterogeneity (eg geographic and age-related differences) limits the generalisability of these models. For instance, Sun3 identified smoking and retreatment as risk factors for DR-TB but did not develop a visual prediction tool. Cheng et al4 reported an association between thick-walled cavities and DR-TB, and Jiang et al6 constructed a radiomics–clinical nomogram model for drug-resistant pulmonary tuberculosis (DR-PTB). However, these studies were all conducted in adult cohorts and lack validation in paediatric populations. Developing a specific, multimodal (clinical and imaging based) predictive model tailored to paediatric patients is essential for optimising early screening strategies.
Research indicates that T-lymphocyte-mediated cellular immunity plays a central role in the clearance of MTB.7 However, the relationship between cellular immune dysfunction and DR-TB remains debatable Some studies have reported that patients with DR-TB exhibit significantly higher counts of CD4⁺ and CD8⁺ T cells and an elevated CD4/CD8 ratio compared with those with drug-susceptible TB (DS-TB).8 By contrast, other studies9 have found lower levels of CD3/HLA-DR and CD4⁺ T cells in patients with MDR-TB than in those with DS-TB. These conflicting findings may stem from differences in study populations, age or the complexity of resistance mechanisms, highlighting the need for independent research in paediatric cohorts. Current studies involving children and adolescents remain limited, and the immature immune systems of paediatric patients further complicate our understanding of T-cell subset dynamics in DR-TB, thereby constraining the development of targeted immunotherapeutic strategies.
Treatment of paediatric DR-TB is complex,1 and accurate diagnosis is a prerequisite for effective treatment. Although drug susceptibility testing (DST) based on bacterial culture remains the “gold standard” for detecting drug resistance, it is time-consuming, technically demanding and often impractical in paediatric settings due to difficulties in specimen collection and low detection rates in paediatric patients.10,11 GeneXpert® MTB/RIF (Cepheid, Sunnyvale, CA, USA) represents a major innovation in TB diagnostics. It is a semi-nested real-time polymerase chain reaction (PCR) assay that simultaneously identifies MTB complex DNA and mutations within the rpoB gene (Rv0664) that are associated with RIF resistance, providing results within approximately 2 hours.1,12 This rapid, integrated detection of both the pathogen and a key marker of drug resistance has positioned it as a pivotal tool for early suspicion of MDR/RR-TB. Although other molecular techniques, such as conventional PCR, multiplex PCR (M-PCR) and loop-mediated isothermal amplification (LAMP), are valuable for detecting MTB in various sample types and may have lower costs, they often present limitations in the context of paediatric DR-TB diagnosis. These limitations can include the inability to simultaneously detect resistance mutations (requiring separate assays for drug susceptibility), generally lower sensitivity in paucibacillary paediatric samples and a need for more complex laboratory infrastructure and skilled personnel, which may not be uniformly available in clinical settings. Therefore, the GeneXpert platform was selected for this study due to its established integration into our hospital’s clinical diagnostic pathway for suspected DR-TB, its endorsement by the WHO for use in paediatric populations12 and its unique capability to provide a rapid, integrated result that directly informs the need for a DR-TB treatment regimen despite its higher cost. The WHO recommendation of GeneXpert MTB/RIF for the detection of DR-TB (specifically RR-TB/MDR-TB) in paediatric populations was formalised in a 2013 policy update, which extended its use from adults (initially recommended in 2010) to include the initial screening of suspected TB or MDR-TB in children and adolescents.12 However, the sensitivity and specificity of GeneXpert MTB/RIF in paediatric populations still require validation through large-scale studies, especially considering the potential variability in diagnostic performance across different regions and resistance profiles.
Despite these advances, a substantial gap remains in the early clinical risk stratification of paediatric DR-TB. Existing predictive tools are often derived from adult populations or rely on single dimensions of data (either clinical or radiographic), limiting their applicability and accuracy in children and adolescents.13 A comprehensive, easy-to-use tool that integrates readily available clinical and imaging features to quantify individual risk prior to or alongside confirmatory microbiological testing could be of considerable assistance in the case of early suspicion and for timely management. The nomogram, a visual predictive model that translates multivariate analysis into a practical scoring system, offers a potential solution to this gap by providing clinicians with an intuitive method to estimate patient-specific probability of DR-TB, thereby optimising resource allocation for further diagnostic testing and guiding early therapeutic decisions.
In China, the drug resistance characteristics of paediatric TB show notable regional heterogeneity. For instance, the proportion of MDR-TB among children in Shenyang is as high as 12.9%,3 whereas it is only 5.4% in Chengdu, Sichuan Province.14 These disparities may be attributed to differences in healthcare infrastructure, circulating strains of MTB and the implementation strength of local TB control measures. Therefore, it is crucial to systematically analyse the epidemiological characteristics of DR-TB in paediatric patients; construct multimodal prediction models integrating clinical, imaging and immunological data; evaluate the diagnostic consistency of novel tools such as GeneXpert MTB/RIF; and explore the role of T-lymphocyte subsets in DR-TB. All these are essential for improving early identification and guiding treatment strategies for DR-TB in children and adolescents.
Materials And Methods
Study Population and Data Collection
This was a retrospective observational cohort study. Using the electronic medical record system, we retrospectively included paediatric patients (≤18 years) who were hospitalised with a clinical diagnosis of TB at the First Affiliated Hospital of Xinxiang Medical University/Henan Provincial Chest Hospital between 1 July 2018 and 31 December 2023. Eligible patients were selected based on predefined inclusion and exclusion criteria. Demographic and clinical data were collected and recorded, including age, sex, height, weight, place of residence, Bacillus Calmette–Guérin (BCG) vaccination history, history of TB exposure, smoking history, routine examinations, human immunodeficiency virus (HIV) status, site of disease involvement, smear results, MTB culture and DST results, GeneXpert MTB/RIF findings, symptom duration prior to effective treatment, treatment details, imaging findings and lymphocyte subset profiles.
The inclusion criteria were patients who were (1) aged ≤18 years and (2) clinically diagnosed with TB.
The exclusion criteria were as follows: (1) all specimens negative for Mycobacterium culture, (2) positive Mycobacterium culture but identified as non-MTB upon species identification, (3) no available first-line anti-TB DST results, (4) duplicate hospital admissions or incomplete clinical records and/or (5) the presence of co-infection with other pathogens.
All chest computed tomography (CT) images were independently reviewed in a blinded manner by two attending radiologists. A consensus was reached regarding the interpretation principles, lesion characteristics and extent of involvement. In cases of disagreement, the final diagnosis was determined with reference to the opinion of a senior radiologist.
All Mycobacterium and MTB culture results were obtained from the hospital’s electronic medical record system. For cases with positive Mycobacterium culture, species identification was further performed using thiophene-2-carboxylic acid hydrazide and p-nitrobenzoic acid tests. The BACTEC MGIT 960 system was used for MTB culture, and DST was subsequently performed. This study collected DST results for first-line anti-TB drugs, including INH, RIF, ethambutol (EMB) and streptomycin (STR). GeneXpert MTB/RIF was introduced at our hospital in 2022 and is used for TB diagnosis and the detection of RIF resistance.
Patients were categorised into DS-TB and DR-TB groups based on their DST results. Clinical and imaging data were compared between the two groups to identify risk factors associated with DR-TB, and a predictive model was developed accordingly.
Definitions
Clinically diagnosed TB in children and adolescents are patients presenting with clinical symptoms consistent with TB, radiological findings compatible with TB and meeting at least one of the following criteria: a positive tuberculin skin test, a positive interferon-gamma release assay or a clear history of contact with a patient with TB.
Diagnosis of TB and DR-TB in children and adolescents was made according to the Chinese standards for TB diagnosis, WS 288–2017 Diagnostic Criteria for Pulmonary Tuberculosis and WS 196–2017 Classification of Tuberculosis.15,16
Pulmonary tuberculosis refers to TB lesions occurring in the lungs, trachea, bronchi or pleura.
Extrapulmonary tuberculosis (EPTB) refers to TB lesions affecting organs or sites outside the lungs, such as lymph nodes (except for intrathoracic lymph nodes), bones, joints, the genitourinary system, the gastrointestinal tract and the central nervous system, and is classified based on the affected organ or site.
Newly treated TB refers to one of the following: a) patients who have never received anti-TB drug treatment, b) patients who are undergoing a standardised treatment regimen but have not yet completed the full course and c) patients who have received irregular anti-TB treatment for <1 month.
Retreated TB refers to one of the following: a) patients who have received inappropriate or irregular anti-TB treatment for ≥1 month, or b) patients who experienced treatment failure or relapse after initial therapy.
Drug-susceptible TB is defined in this study as TB caused by strains sensitive to all four first-line anti-TB drugs.
Mono-resistant TB is defined as resistance to only one of the first-line anti-TB drugs.
Rifampicin-resistant TB is defined as TB resistant only to RIF.
Drug-resistant TB is defined as resistance to at least one first-line anti-TB drug.
Multidrug-resistant TB is defined as resistance to at least INH and RIF, with or without resistance to other first-line anti-TB drugs.
Effective treatment refers to treatment with at least three anti-TB drugs to which the isolate is susceptible, as determined by phenotypic DST.17
Severe TB refers to disease with any uncontrolled, disseminated or complex clinical syndromes, including cavitary PTB, PTB with empyema, tuberculous pericarditis, abdominal TB (primarily intestinal TB, TB of solid abdominal organs and tuberculous peritonitis), tuberculous arthritis, tuberculous synovitis, skeletal TB, tuberculous meningitis, genitourinary TB and miliary TB.1,18
Malnutrition is defined using the WHO-recommended Z-score system, with a Z-score < −2 considered indicative of malnutrition.19
Anaemia is defined by age-specific and sex-specific haemoglobin thresholds: a) 6–59 months: <110 g/L, b) 5–11 years: <115 g/L, c) 12–14 years: <120 g/L, d) ≥15 years: <120 g/L for girls and <130 g/L for boys.20
History of smoking is defined as smoking 10 or more cigarettes per month.21
Statistical Analysis
Statistical analysis was performed using SPSS25. The Shapiro–Wilk test was used to assess the distribution of measurement data. Normally distributed data were expressed as means ± standard deviations or frequencies and percentages (n[%]), and between-group comparisons were made using the chi-square test. Non-normally distributed data were represented by medians with interquartile ranges and compared between groups using the Mann–Whitney U-test. For variables with less than 5% missing data, median imputation was used for continuous variables and mode imputation for categorical variables. Variables with more than 5% missingness were excluded from the subsequent multivariate logistic regression analysis to ensure the robustness of the predictive model. Given the exploratory nature of the univariate analysis aimed at variable screening for the subsequent multivariate model and to avoid over-conservatism that might exclude clinically relevant predictors, adjustment for multiple comparisons (eg Bonferroni, FDR) was not applied at this stage. The primary statistical inference was based on the final multivariate logistic regression model. A multivariate logistic regression model was applied to identify factors independently associated with DR-TB, which was used as the dependent variable. No formal subgroup or stratified analyses (eg by specific age groups or treatment status) were performed in this study, as the primary aim was to develop a unified predictive model for the entire paediatric cohort. Variables with P < 0.1 in univariate analysis were included in the model. Stepwise regression (entry criterion P < 0.05; removal criterion P > 0.10) was used to select independent risk factors. The variance inflation factor (VIF) was calculated using the regression model, and variables with a VIF-value >5 were considered to exhibit significant collinearity and were excluded or adjusted to optimise the model. Forest and violin plots for group comparisons were generated using GraphPad Prism 8 (GraphPad Software, San Diego, CA, USA).22 A nomogram predictive model for DR-TB was constructed using the rms package in R 4.4.3.23 The model’s discrimination was evaluated using receiver operating characteristic (ROC) curves generated with the ROCR and rms packages, and its calibration was assessed using calibration plots.24 Clinical utility was evaluated using decision curve analysis (DCA).25 The consistency between phenotypic DST and GeneXpert MTB/RIF in detecting RIF resistance was assessed using Cohen’s kappa statistic. A P-value <0.05 was considered statistically significant.
Results
General Characteristics and Drug Resistance Profile of Tuberculosis in Paediatric Patients
During the study period, a total of 1,876 paediatric patients clinically diagnosed with TB were reviewed, and 223 were rendered eligible using the inclusion and exclusion criteria (Figure 1). All patients had received the BCG vaccination at birth and tested negative for HIV. The study cohort comprised 112 boys and 111 girls, with a male-to-female ratio of approximately 1:1. The patients ranged in age from 2 to 18 years, with a median age of 16.0 years. Adolescents (aged 13–18 years) accounted for 78.5% of the sample. Newly treated TB cases constituted 90.13% of cases (201/223), whereas retreated TB cases accounted for 9.87% (22/223). Moreover, PTB was diagnosed in 87.89% of patients (196/223), PTB and EPTB in 10.76% (24/223) and EPTB alone in 1.35% (3/223) (Table 1).
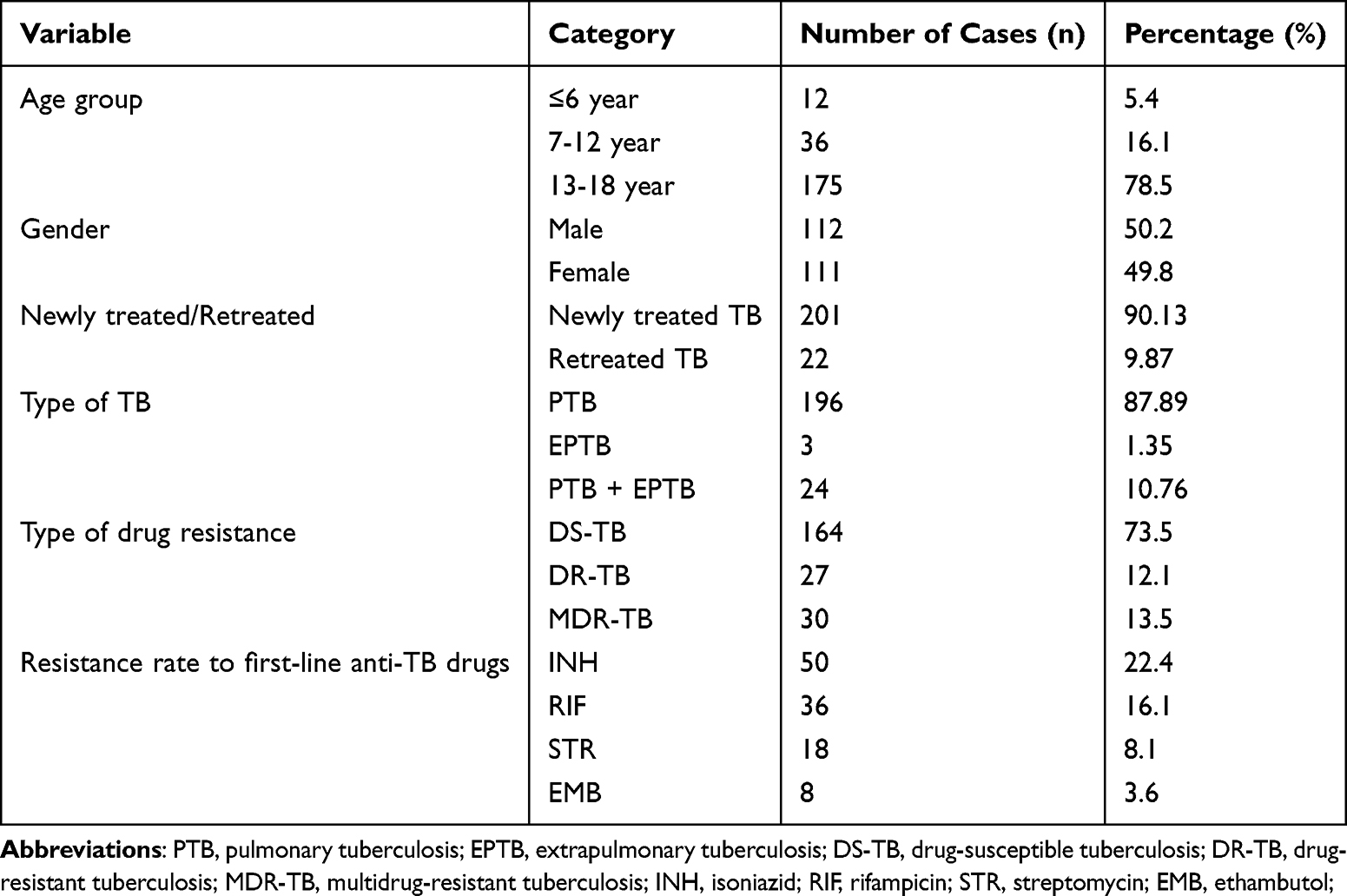 |
Table 1 Demographic Characteristics and Drug Resistance Distribution in Pediatric Patients with TB (n = 223) |
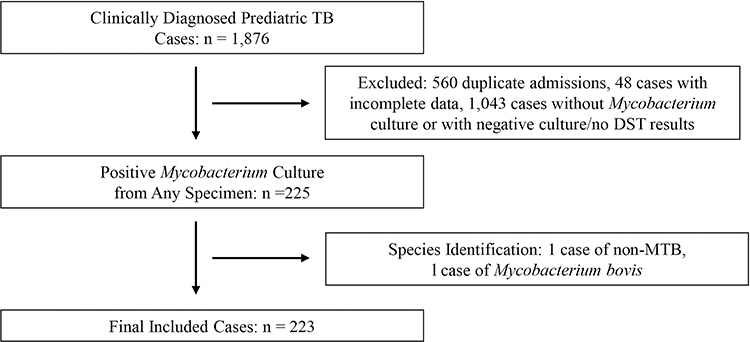 |
Figure 1 Flowchart of study population A total of 223 pediatric TB cases were included in this study. |
Specimen sources were as follows: sputum (n = 116), bronchoalveolar lavage fluid (BALF; n = 83), pleural effusion (n = 15), tissue samples (n = 3), synovial fluid (n = 2), peritoneal effusion (n = 1), aspirate from chest wall mass (n = 1), cerebrospinal fluid (n = 1) and perianal abscess drainage (n = 1). Each specimen was collected from a unique patient.
According to the DST results, the overall drug resistance rate was 26.5% (59/223), with MDR-TB accounting for 50.8% (30/59) of all DR-TB cases. The resistance rates for individual first-line anti-TB drugs were as follows: INH 22.4% (50/223), RIF 16.1% (36/223), STR 8.1% (18/223) and EMB 3.6% (8/223) (Table 1). The drug resistance patterns among the 59 patients with DST-confirmed resistance were as follows: resistance to INH alone (n = 18); resistance to both INH and RIF (n = 16); resistance to INH, RIF, EMB and STR (n = 7); resistance to INH, RIF and STR (n = 6); resistance to RIF alone (n = 6); resistance to STR alone (n = 3); resistance to INH and STR (n = 2); and resistance to INH, RIF and EMB (n = 1) (Figure 2).
 |
Figure 2 Drug resistance profile of 59 pediatric cases. |
Comparison of Demographic and Clinical Characteristics Between Drug-Resistant Tuberculosis and Drug-Susceptible Tuberculosis in 223 Paediatric Patients
Significant differences were observed between DR-TB and DS-TB cases in treatment history, adherence to medication, smoking history, duration of symptoms before effective treatment and site of infection (all P < 0.05) (Table 2).
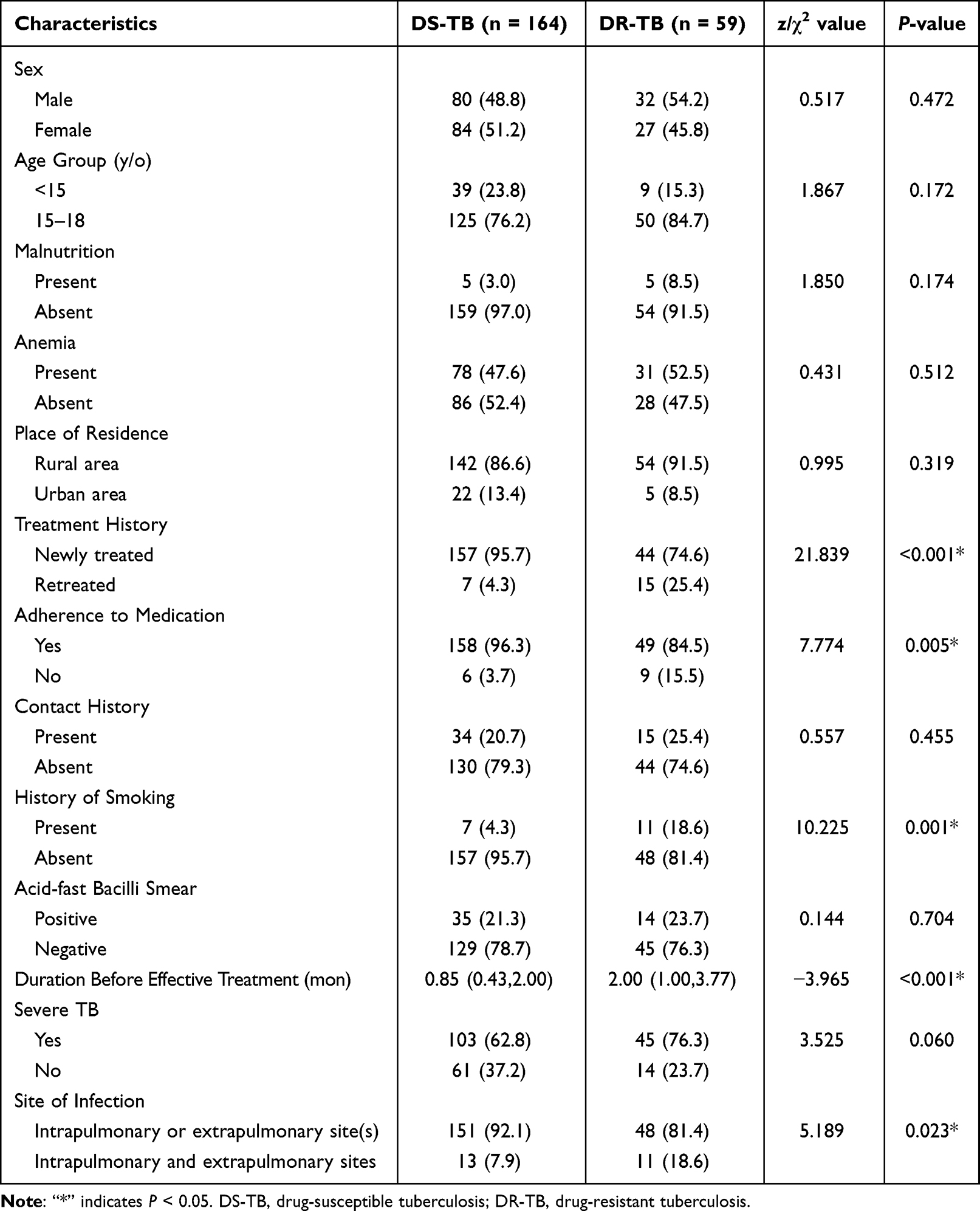 |
Table 2 Comparison of Demographic and Clinical Characteristics Between DS-TB and DR-TB in Pediatric Patients (n[%] or M[P25,P75]) |
Comparison of Imaging Findings Between Drug-Resistant Tuberculosis and Drug-Susceptible Tuberculosis in 220 Paediatric Patients
Three cases with isolated EPTB were excluded, leaving 220 paediatric TB cases for imaging analysis – 162 with DS-TB and 58 with DR-TB. A comparison of chest CT findings between the two groups revealed that patients with DR-TB had significantly higher rates of lesions involving the left lower lobe, right middle lobe and three or more pulmonary lobes than those with DS-TB (P < 0.05). In addition, chest CT findings, including the tree-in-bud sign, cavitation, pleural thickening and mediastinal lymphadenopathy or calcification, were significantly more common in patients with DR-TB than in those with DS-TB (P < 0.05; Table 3).
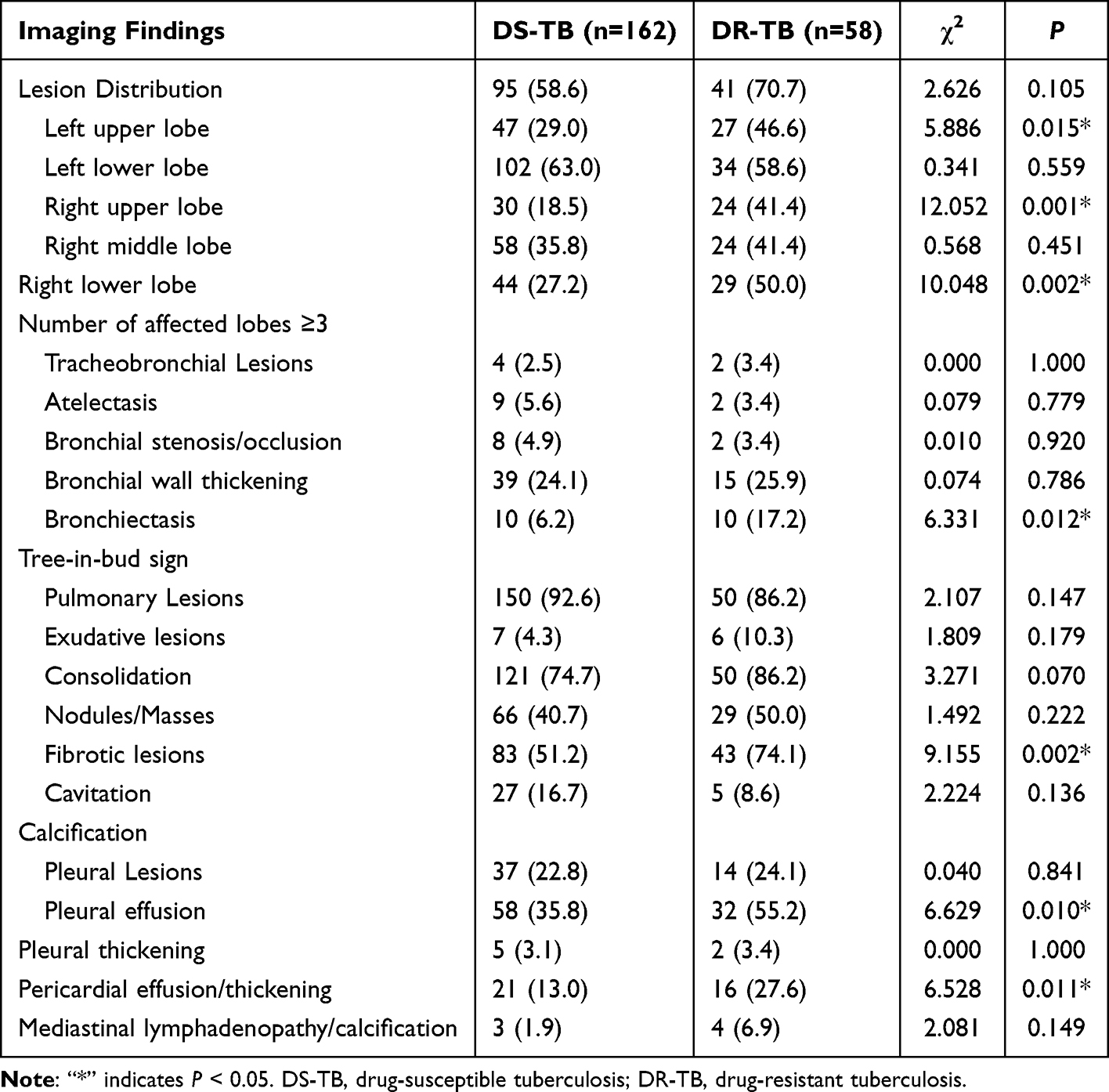 |
Table 3 Comparison of Imaging Findings Between DR-TB and DS-TB in Pediatric Patients (n[%]) |
Analysis of Risk Factors Associated with Drug-Resistant Tuberculosis in 220 Paediatric Patients
A multivariate logistic regression analysis was performed using paediatric DR-TB as the dependent variable and variables with statistical significance (all P < 0.05) from Tables 1–3 as independent variables, including site of infection, treatment history, adherence to medication, duration of symptoms before effective treatment, smoking history, involvement of the right middle lobe and left lower lobe, total number of affected pulmonary lobes, tree-in-bud sign, cavitation, pleural thickening and mediastinal lymphadenopathy or calcification. The results identified the following as independent risk factors for the occurrence of DR-TB in paediatric patients: treatment history, smoking history, right middle lobe involvement and the presence of cavitation (all P < 0.05; Figure 3).
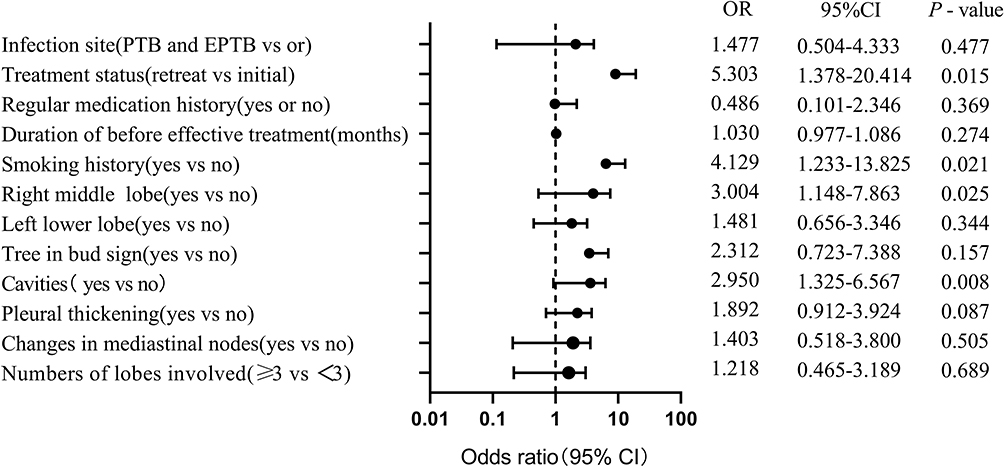 |
Figure 3 Forest plot of multivariate logistic regression analysis for risk factors of DR-TB in pediatric patients. |
Construction and Validation of a Nomogram Predictive Model for Paediatric Drug-Resistant Tuberculosis
Based on the significant factors obtained from the multivariate logistic regression analysis, a nomogram model was constructed to quantitatively predict the risk of DR-TB in paediatric patients. The model allows individualised risk assessment for each patient. For example, a total score of 222 on the nomogram corresponds to a predicted probability of 0.897 for developing DR-TB (Figure 4). Model validation included the following assessments: (1) discrimination – ROC curve analysis showed that the area under the curve (AUC) was 0.776 (95% confidence interval [CI]: 0.710–0.841), indicating good predictive performance of the model (Figure 5); (2) calibration – internal validation using bootstrapping (1,000 resamplings from the original dataset) demonstrated that the calibration curve closely followed the ideal diagonal line, suggesting acceptable model fit and good agreement between predicted and observed outcomes (Figure 6); (3) clinical utility – DCA revealed that the model had a net clinical benefit when the threshold probability ranged from 8% to 98%, indicating good practical applicability of the nomogram in predicting paediatric DR-TB in a clinical setting (Figure 7).
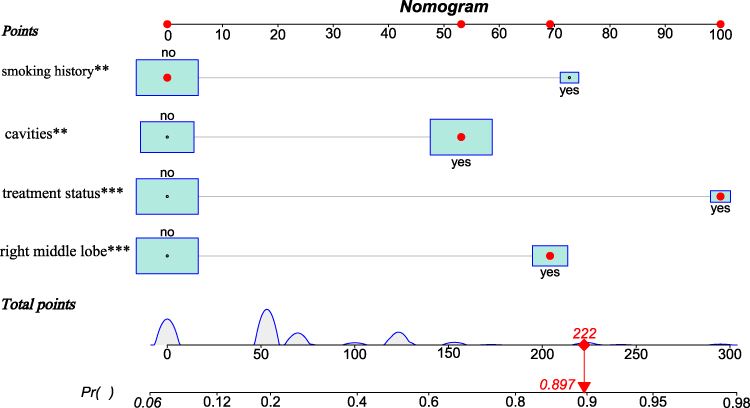 |
Figure 4 Nomogram predictive model for pediatric DR-TB. Note: “**”P<0.01;*** P<0.001; ① Points score indicator; ② Variables in the predictive model: (from top to bottom: smoking history, cavity, treatment status, lesion in the right middle lobe);③ Total points: Assuming no smoking history, the corresponding score is 0 points; presence of a cavity corresponds to 52 points; retreatment corresponds to 100 points; presence of a lesion in the right middle lobe corresponds to 70 points. Thus, the total score is 0 + 52 + 100 + 70 = 222 points; ④ Probability of developing DR-TB: If the total score is 222 points, the probability of developing DR-TB is 0.897. |
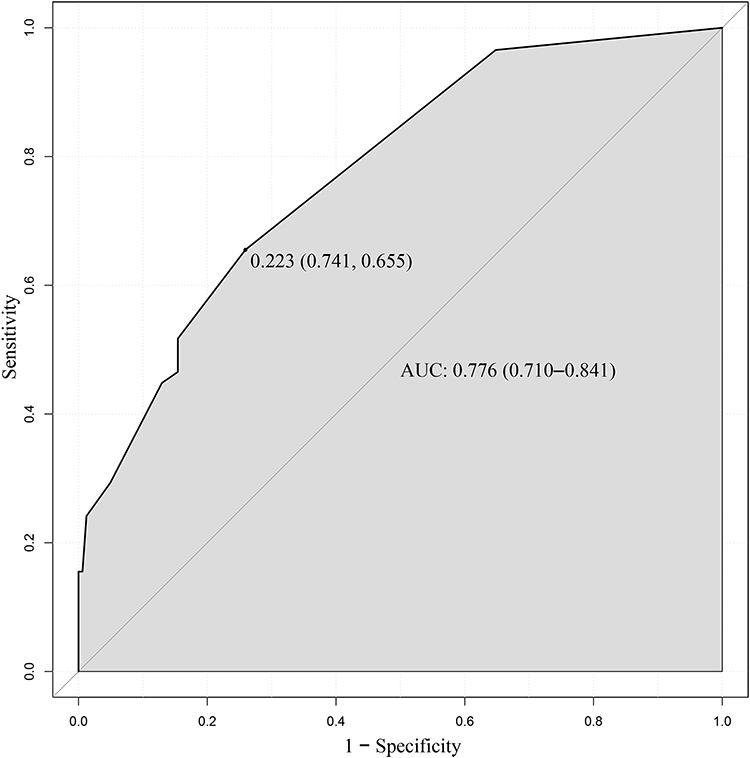 |
Figure 5 ROC curve for the nomogram predictive model for pediatric DR-TB. |
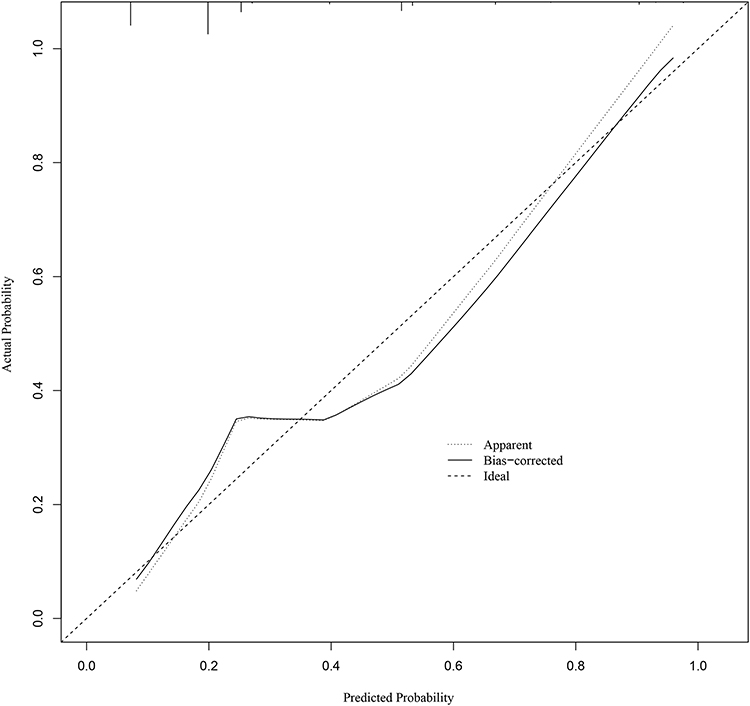 |
Figure 6 Calibration curve of the nomogram predictive model for pediatric DR-TB. |
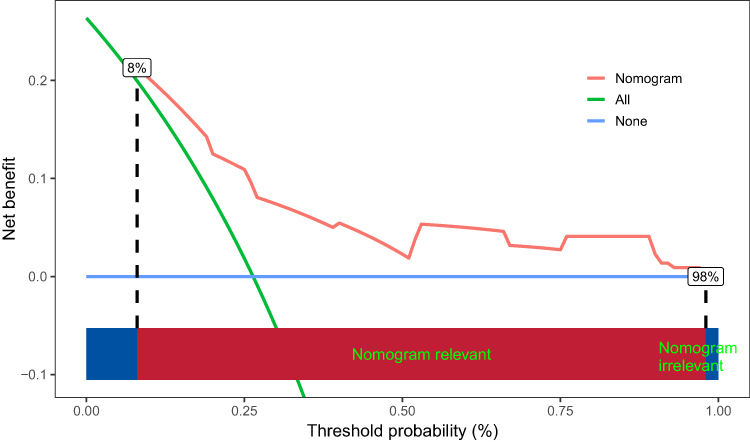 |
Figure 7 DCA of the nomogram predictive model for pediatric DR-TB. |
Comparison of T-Lymphocyte Subsets Between Drug-Resistant Tuberculosis and Drug-Susceptible Tuberculosis in 56 Paediatric Patients
Among the enrolled paediatric patients with TB, 56 underwent testing for T-lymphocyte subsets. All selected patients had no known immunodeficiency disorders, autoimmune diseases or prior treatment with immunosuppressive agents. Of these, 12 were diagnosed with DR-TB and 44 with DS-TB. Baseline characteristics were balanced between the two groups, and no statistically significant differences were found in any T-cell subset parameters (all P > 0.05; Table 4 and Figure 8).
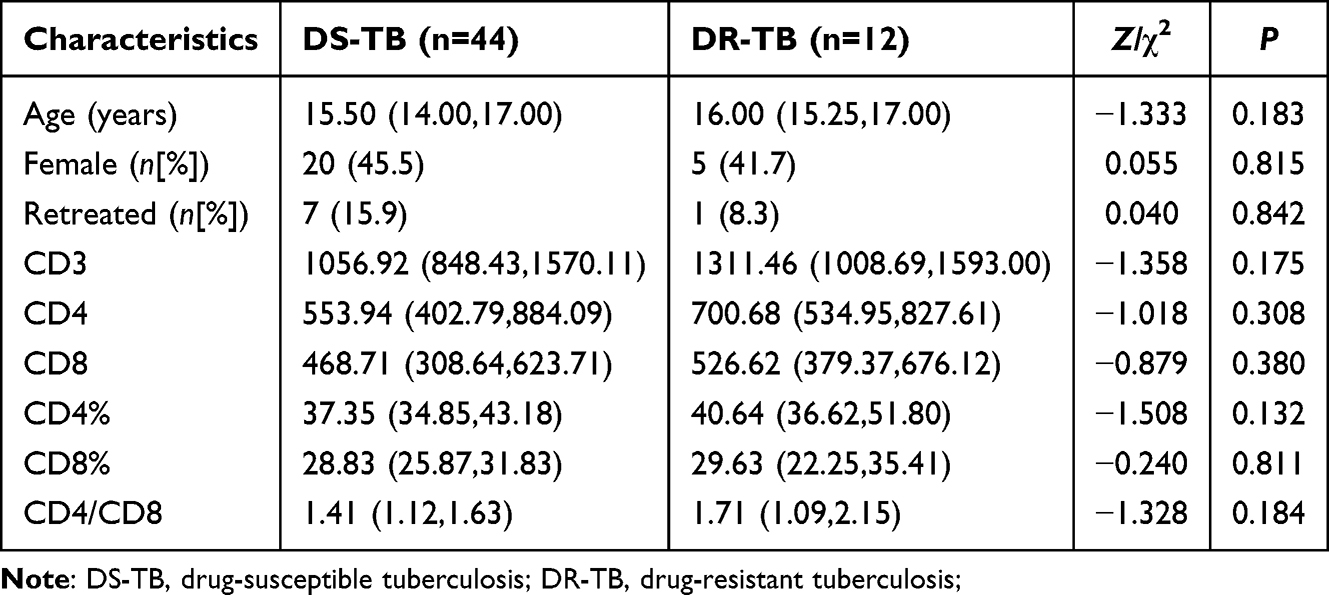 |
Table 4 Comparison of Baseline Characteristics and T Lymphocyte Subsets Between Pediatric Patients with DR-TB and DS-TB |
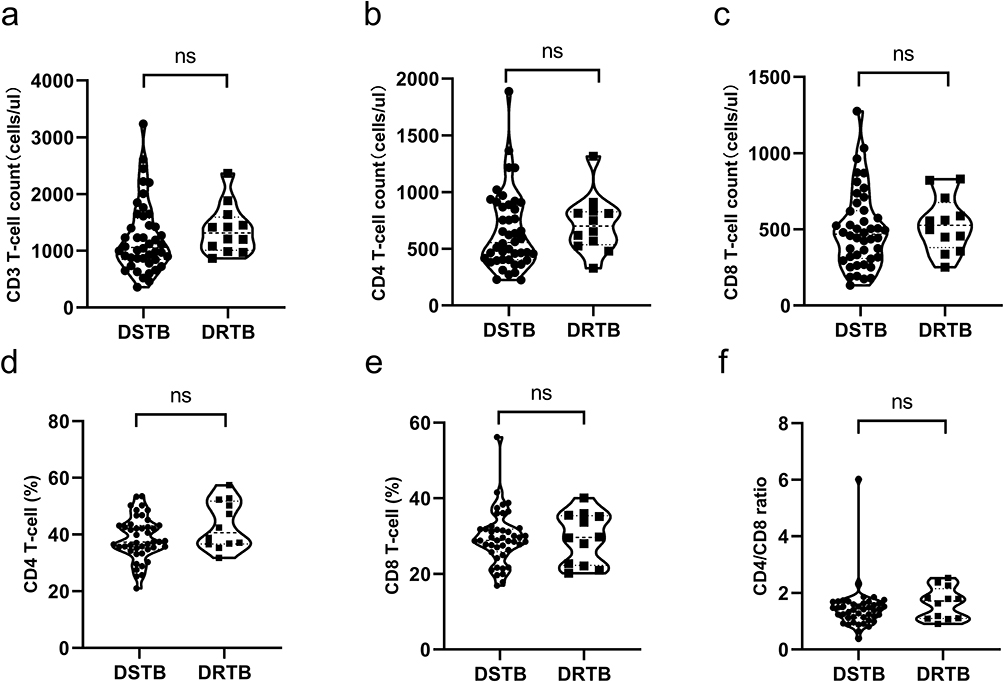 |
Figure 8 Comparison of T lymphocyte subsets between DR-TB and DS-TB in pediatric patients. Notes: Group comparisons were performed using the Mann–Whitney U-test; ns: P > 0.05. (a) Violin plot of CD3⁺ T cell count (cells/μL) (b) Violin plot of CD4⁺ T cell count (cells/μL) (c) Violin plot of CD8⁺ T cell count (cells/μL) (d) Violin plot of CD4⁺ T cell percentage (%) (e) Violin plot of CD8⁺ T cell percentage (%) (f) Violin plot of CD4/CD8 ratio; ns: an abbreviation for “not significant,” indicating that the difference between groups is not statistically significant (P > 0.05). |
Consistency Between Drug Susceptibility Testing and GeneXpert MTB/RIF in Detecting Rifampicin Resistance
Among the 58 paediatric TB cases with MTB-positive results from both the MGIT 960 culture and GeneXpert MTB/RIF, the phenotypic DST results obtained from the MGIT 960 system were used as the reference standard. Based on this reference, 37 cases were classified as DS-TB and 21 as DR-TB. In the DS-TB group (n = 37), two cases tested positive for RIF-resistance-associated gene mutations using GeneXpert MTB/RIF but were RIF sensitive in the DST. In the DR-TB group (n = 21), 16 patients tested positive for RIF resistance using GeneXpert MTB/RIF, of whom 14 were confirmed as RR-TB through DST and 2 were not. Among the five GeneXpert RIF-negative DR-TB cases, three were classified as RIF susceptible through DST (two resistant only to INH, one only to STR) and two tested positive for RR-TB in the DST.
Using DST as the reference, GeneXpert MTB/RIF demonstrated a sensitivity of 87.50% (14/16) and specificity of 90.48% (38/42) in detecting RR-TB. A total of 6.90% (4/58) of cases were identified as RR-TB by GeneXpert MTB/RIF but not by DST (Table 5). McNemar’s test yielded a P-value of 0.687, and the kappa coefficient was 0.751 (P < 0.001), indicating good agreement between DST and GeneXpert MTB/RIF for detecting RIF resistance.
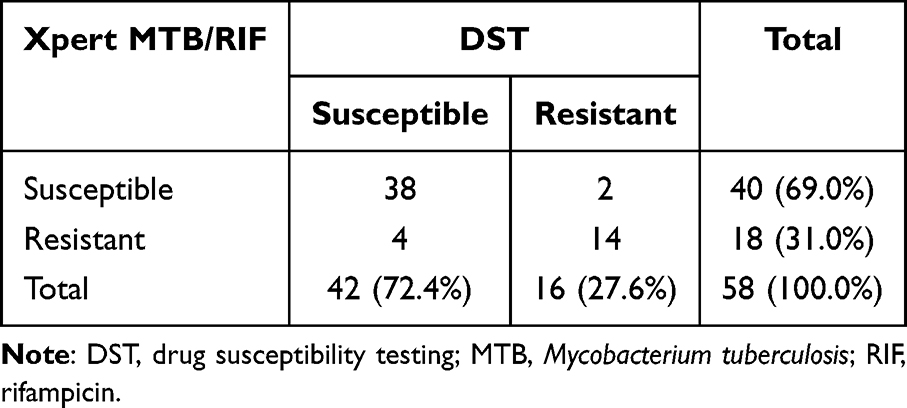 |
Table 5 Diagnostic Performance of Xpert MTB/RIF for Detecting Rifampicin Resistance in Pediatric Tuberculosis Patients, with Phenotypic Drug Susceptibility Testing as the Reference Standard |
Discussion
Drug-resistant TB in children and adolescents poses a serious public health challenge, particularly in countries with high TB prevalence. This underlines the value of understanding the epidemiological and drug resistance patterns in paediatric patients and identifying factors influencing drug resistance to achieve early diagnosis and timely intervention. To date, relevant studies remain limited. In this study, we analysed data from paediatric patients with TB admitted to our hospital between July 2018 and December 2023. Aiming to deepen the understanding of DR-TB in paediatric patients, this study investigated the epidemiological and resistance characteristics of the condition, constructed a nomogram predictive model for DR-TB, examined the expression of T-lymphocyte subsets and evaluated the consistency between GeneXpert MTB/RIF and conventional DST regarding RIF resistance detection.
General Characteristics and Drug Resistance Patterns in Children and Adolescents with Tuberculosis
In our cohort, the majority of paediatric patients with TB were aged ≥15 years, accounting for 78.48% of cases, which aligns with findings from previous studies.3 All patients in this study had received the BCG vaccination, supporting prior research from India indicating that the protective effect of BCG declines substantially after the age of 12.5 years.26 Additionally, older adolescents typically have broader social interactions and a higher risk of exposure to TB, which may also contribute to this age distribution. Notably, 90.13% of the patients were new TB cases, and among the DR-TB cases, 74.6% (44/59) were newly diagnosed. This suggests a pronounced trend of primary DR-TB infection among paediatric patients, possibly due to the direct transmission of drug-resistant strains from adults, highlighting the need for rigorous screening of close contacts in children and adolescents.27 Moreover, PTB was the predominant form of TB in our study cohort, with EPTB accounting for only 12.11% of cases. This is lower than the 24.6% reported by Li et al28 and the 17% global estimate reported by the WHO in 2022.1 These discrepancies may be attributed to differences in population demographics, sample sizes or geographic regions. Clinicians should remain vigilant for asymptomatic or atypical forms of EPTB to avoid missed diagnoses, which could increase the risk of DR-TB transmission.
In terms of drug resistance characteristics, in China, the prevalence of drug resistance among children and adolescents with TB remains high. In this study, the overall DR-TB rate was 26.5%, with MDR-TB accounting for 13.5%. These figures are consistent with regional data from Shenyang (28.78% for DR-TB, 12.90% for MDR-TB) and Chengdu, Sichuan Province (24.3% and 5.4%, respectively).3,14 However, they are markedly higher than the results of a meta-analysis by Song et al,29 which reported DR-TB and MDR-TB rates of 13.59% and 3.72%, respectively. This discrepancy highlights the critical and urgent situation of DR-TB prevalence in China and underscores the necessity of the present study, as well as the imperative need to strengthen TB control and prevention strategies. Our drug resistance profile revealed that INH (22.4%) and RIF (16.1%) had the highest resistance rates, consistent with resistance patterns reported domestically and internationally, although the levels observed in this study were notably higher.15,28 This may be attributed to the widespread use of these two first-line anti-TB drugs for treating active TB and as preventive therapy for close contacts, including children and adolescents. Although Song et al29 reported STR resistance as the most prevalent (10.82%), its resistance rate was relatively low in our study. This discrepancy may be due to the implementation of WHO guideline-based standardised treatment protocols and regional prescription control measures, suggesting the effectiveness of precise prevention and control strategies. Additionally, the reduced use of STR as a result of a shift towards second-line therapies may have indirectly suppressed resistance development to this drug.
Although extensive research has been conducted on DR-TB in adults, predictive studies specifically tailored to the paediatric population remain limited. Our study distinguishes itself by constructing and validating a clinical-imaging-based nomogram predictive model exclusively for paediatric patients. Although factors such as retreatment history and cavity formation have been reported as DR-TB risks in adults, our model uniquely identifies and incorporates imaging features such as right middle lobe involvement within a paediatric cohort, which has been less frequently highlighted in adult-centric studies. Furthermore, by integrating these variables into a visual, point-based scoring tool, we provide a practical instrument for clinicians to quantify individual risk at the bedside, an approach not previously well established for children and adolescents.
Comparison of Clinical and Imaging Features Between Drug-Susceptible Tuberculosis and Drug-Resistant Tuberculosis
Previous studies on risk factors for DR-TB have shown considerable variability due to differences in ethnicity, population characteristics, geographic regions and study designs. In the present study, multivariate logistic regression analysis identified retreatment history, smoking history, right middle lobe involvement and cavity formation as independent risk factors for DR-TB in children and adolescents.
Compared with DS-TB, retreatment was significantly more frequent among patients with DR-TB (odds ratio [OR] = 5.303, 95% CI: 1.378–20.414, P = 0.015). This may be related to prolonged treatment durations, irregular medication adherence, incomplete treatment or an initially incomplete drug susceptibility profile in retreated cases. All these contribute to the development of resistance-associated genetic mutations in MTB, thereby promoting the spread of DR-TB among previously treated patients and increasing both treatment difficulty and transmission risk. These findings are consistent with those reported by Sun et al3 and Li et al.30
Smoking introduces harmful substances that increase oxidative stress and inflammation, impair bronchial mucosal barriers and weaken immune responses, thereby raising susceptibility to TB infection.31 In this study, smoking was found to have a significant impact on DR-TB (OR = 4.129, 95% CI: 1.233–13.825, P = 0.021), suggesting that smoking may increase the risk of infection with DR-TB strains. Potential mechanisms include smoking-induced impairment of drug absorption, alterations in pharmacokinetics, immune suppression and poor treatment adherence. Furthermore, smoking may interfere with culture conversion and prolong treatment duration, thus contributing to the emergence and persistence of DR-TB strains.32 These findings are in line with those reported by Tao,5 reinforcing the conclusion that smoking cessation is a critical preventive measure against TB, particularly DR-TB.
This study, through analysis of chest CT imaging, revealed significant differences in lesion distribution and characteristics between DR-TB and DS-TB. The data showed that the proportion of cases involving multiple lung lobes (≥3 lobes) was significantly higher in the DR-TB group than in the DS-TB group (P < 0.05). This finding is consistent with the conclusion of Cheng et al4 regarding diffuse pulmonary involvement and aligns with previous studies describing the multilobar distribution pattern of DR-TB lesions.33 However, no significant difference was observed between the two groups in multivariate analysis, which may be attributed to sample size limitations or the influence of confounding factors. Notably, this study found that lesions in the right middle lobe (P = 0.001) and left lower lobe (P = 0.015) were more characteristic of DR-TB. Multivariate analysis further identified right middle lobe involvement as an independent risk factor (OR = 3.004, 95% CI: 1.148–7.863, P = 0.025). This result differs from most prior studies,4,34 potentially due to variations in age stratification, lesion classification criteria or regional differences in the circulating MTB strains. These findings highlight the need for further validation through multicentre studies.
In this study, cavity formation was verified as an independent risk factor for DR-TB. The incidence of cavities was significantly higher in the DR-TB group than in the DS-TB group (74.1% vs 51.2%, P = 0.002). Multivariate analysis further indicated that cavity formation was more characteristic of DR-TB (OR = 2.950, 95% CI: 1.325–6.567, P = 0.008), consistent with findings from previous studies.4,35 This observation is well supported by molecular biological mechanisms. The fibrous deposition and sparse vascularisation of cavity walls hinder drug penetration and create a microenvironment conducive to persistent infection, promoting the selection and amplification of drug-resistant mutant strains. In particular, the overexpression of matrix metalloproteinases (MMPs), especially MMP-9, accelerates cavity formation by degrading the extracellular matrix.36–39 Moreover, previous studies have reported that chest CT images in children with DR-PTB often show multiple, multilobar, thick-walled cavities, whereas thin-walled cavities are more commonly seen in DS-TB. This suggests that quantitative metrics related to cavity features may serve as key parameters in assessing the risk of drug resistance. These findings provide new perspectives for further analysis of cavity characteristics and molecular-level research.
The discriminatory performance of the predictive model was evaluated using ROC curve analysis. The results demonstrated that retreatment history, smoking history, right middle lobe involvement and cavity formation significantly contributed to the DR-TB risk score, yielding an AUC of 0.776 (95% CI: 0.710–0.841). This indicates that the model allows for effective differentiation between DR-TB and DS-TB cases. Model calibration was further assessed using a calibration curve, which showed that the fitted curve closely aligned with the ideal diagonal line (Figure 6), suggesting good agreement between predicted and observed risk probabilities. The clinical utility of the model was evaluated via DCA, which indicated that when the threshold probability ranged from 8% to 98%, the model provided a positive net benefit (Figure 7), demonstrating its potential value in guiding clinical decision-making. Although the AUC and calibration curves assess the model’s discriminatory power and calibration accuracy, respectively, the DCA curve directly reflects its clinical utility. By integrating these three validation methods, this study comprehensively verified both the scientific robustness and practical utility of the nomogram predictive model. It is important to note that the validation performed in this study was internal, using bootstrapping on the original dataset. Although this provides an estimate of model performance and helps mitigate overfitting, external validation on independent, prospective paediatric cohorts from different geographic or clinical settings is essential to verify the generalisability and robustness of our nomogram before broad clinical implementation.
Added Value and Clinical Purpose of the Predictive Model
The independent risk factors identified in our model – retreatment history, smoking, right middle lobe involvement and cavity formation – are consistent with some previous reports in adult or mixed populations. The primary innovation and added value of this study, therefore, lie not in the discovery of novel risk factors per se but in the development and validation of a paediatric-specific, quantitative risk stratification tool that integrates these established predictors into a single, clinically actionable framework. Although individual factors are known, clinicians lack a method to easily combine and evaluate them to estimate an individual child’s probability of having DR-TB. Our nomogram addresses this gap by translating multivariate analysis into a visual scoring system. Its purpose is to enable early, individualised risk estimation at the point of care, guiding decisions about prioritising rapid molecular testing (eg GeneXpert MTB/RIF) or escalating diagnostic efforts before conventional drug susceptibility results are available. This is particularly crucial in paediatric TB, for which diagnostic delays are common. Thus, the model aims to improve early identification and risk stratification beyond what is achievable by considering these factors in isolation, ultimately supporting more targeted and timely intervention in high-risk paediatric patients.
Future Validation, Generalisability and Clinical Application of the Predictive Model
The nomogram developed in this study represents a preliminary step towards individualised risk assessment for paediatric DR-TB. To transition this tool from a research construct to a clinically useful instrument, several key steps are required. First and foremost, external validation in independent paediatric cohorts from diverse geographic and epidemiological settings is essential. Such validation would rigorously test the model’s generalisability and calibrate its performance for local use, addressing potential spectrum bias from our single-centre, retrospective sample. Furthermore, the model’s practical application should be explored. It could be integrated into clinical decision-support systems to help prioritise children at high risk of DR-TB for expedited molecular testing (eg GeneXpert MTB/RIF) or more intensive diagnostic workups, especially in resource-limited settings where universal rapid DST is not feasible. The nomogram’s simple, visual format is amenable to implementation as a bedside scoring sheet or a digital calculator. Future research should also focus on defining clinically actionable risk thresholds, evaluating the model’s impact on diagnostic timelines and treatment outcomes, and potentially refining it by incorporating a broader range of predictors, including social determinants of health (eg household crowding, socioeconomic status) and treatment-related factors (eg detailed medication adherence history, pharmacokinetic data), alongside emerging biomarkers. This would move the model closer to a truly holistic risk assessment tool. By framing our model as a foundation for future validation and implementation research, we aim to strengthen its potential relevance and utility for improving the early identification of DR-TB in children globally.
Comparison of T-Lymphocyte Subsets
As markers of total T lymphocytes, CD3⁺ T cells play a central role in cellular immune activation. Moreover, CD4⁺ T cells secrete cytokines upon antigen stimulation, activating macrophages to kill MTB, whereas CD8⁺ T cells exert cytotoxic effects by clearing inactivated target cells and inducing apoptosis. They also enhance phagocytic function in a synergistic manner, contributing to a specific anti-TB immune response.8 The balance between CD4⁺ and CD8⁺ T cells is critical for mediating protective immunity. Our previous research40 indicated that cellular immune defences are impaired in children with TB infection, with more pronounced deficits observed in severe cases. In this study, we further investigated the differences in T-lymphocyte subsets between patients with DR-TB and those with DS-TB. The results showed that the levels of T-cell subsets in the DR-TB group were slightly higher than those in the DS-TB group; however, the differences lacked statistical significance (all P > 0.05). This finding differs from several studies in adult populations that have reported significant alterations in T-cell subsets (eg CD4⁺, CD8⁺ counts or CD4/CD8 ratio) associated with DR-TB,8,9,41 and several possible explanations are considered: (1) a small sample size, which may have introduced statistical bias; (2) a higher proportion of retreated cases in the DS-TB group, in which prolonged therapy may have led to increased T-cell depletion; (3) differences in immune maturity, as most previous studies were conducted in adults, whereas the immune system in children and adolescents is still developing, making T-cell subsets more susceptible to confounding factors; and (4) the complex mechanisms of drug resistance, which may not primarily involve immune dysregulation. Given the retrospective design and limitations of this study, further prospective, multicentre studies with larger sample sizes are needed to validate these findings.
Consistency Between Drug Susceptibility Testing and GeneXpert MTB/RIF in Detecting Rifampicin Resistance
Current clinical guidelines recommend managing patients with MDR-TB or RR-TB using MDR-TB-specific treatment regimens. GeneXpert MTB/RIF is a semi-nested PCR assay based on molecular beacon technology that enables the rapid detection of MTB and its resistance to RIF. Since its endorsement by the WHO in 2013 for the auxiliary diagnosis of suspected PTB in children and adolescents, MDR-TB, TB-HIV co-infection and tuberculous meningitis, GeneXpert MTB/RIF has become an increasingly important tool in identifying RR-TB.
In this study, DST was used as the gold standard to evaluate the diagnostic consistency of GeneXpert MTB/RIF for paediatric RR-TB. The results showed a sensitivity of 87.50% and a specificity of 90.48%, with a kappa coefficient of 0.751, indicating good agreement between the two methods in detecting RIF resistance. These performance metrics, derived from a well-defined paediatric cohort in China, are consistent with the high sensitivity and specificity reported in other paediatric and adult studies, contributing valuable, contemporary evidence specific to a high TB burden regional setting. Notably, four cases (6.90%) of RR-TB were identified exclusively by GeneXpert MTB/RIF, demonstrating its supplementary value in early detection. These findings are supported by studies conducted by Lavu et al42 and Sun et al.3
This study presents several novel contributions to the field of paediatric TB. First, it is among the few studies to develop and validate a clinical-imaging-based nomogram predictive model specifically for DR-TB risk in paediatric patients. Unlike previous models primarily designed for adults, our model integrates readily accessible clinical (retreatment history, smoking) and imaging (right middle lobe involvement, cavity formation) variables into a practical, visual tool for clinicians. Second, we provide contemporary, clinic-based evidence on the diagnostic performance of the GeneXpert MTB/RIF assay for detecting RR-TB in a well-defined paediatric cohort in China, contributing to the ongoing validation of this tool in varied settings. Third, we explored the profile of T-lymphocyte subsets in paediatric DR-TB, an area with scarce and conflicting data in children, adding to the understanding of the immunological context in this age group. Collectively, our work shifts the focus towards integrated risk prediction and rapid molecular diagnosis tailored to the paediatric population, addressing critical gaps in the early identification and management of DR-TB in children and adolescents.
Limitations
This study has several limitations. First, the low culture-positive rate in paediatric patients may have introduced selection bias, potentially underestimating the burden of DR-TB among younger children. By contrast, older children, whose clinical and radiological features may more closely resemble those of adults, were overrepresented. Second, resistance to second-line anti-TB drugs was not assessed. Third, considering the analysis of T-lymphocyte subsets was limited to cases with available test results, the differences in disease stage, the small sample size and the lack of post-treatment comparison, this retrospective study may fail to accurately reflect the true immune status in DS-TB compared with DR-TB. Fourth, the predictive nomogram model was validated internally using bootstrap resampling but has not undergone external validation in an independent paediatric cohort. Although internal validation mitigates overfitting and provides performance estimates, external validation is essential to confirm the model’s generalisability and robustness across different settings before it can be recommended for clinical use. Fifth, GeneXpert MTB/RIF was only introduced at our centre within the past 2 years, resulting in a small number of included cases and possible bias in the consistency analysis between DST and GeneXpert MTB/RIF in detecting RIF resistance. Sixth, the diagnostic performance of GeneXpert MTB/RIF could not be reliably evaluated in EPTB due to the limited number of such cases and the even smaller subset with both positive GeneXpert and DST results. This precludes meaningful conclusions about its sensitivity and specificity in paediatric EPTB specimens, which are often paucibacillary and pose a known challenge for nucleic acid amplification tests. Seventh, our diagnostic evaluation was confined to specimens routinely collected in clinical practice (eg sputum, BALF, pleural fluid). Non-invasive samples such as urine, which could be used for novel immunological assays, were not systematically collected or analysed. Although such approaches represent a promising future direction for child-friendly diagnostics, they were beyond the scope of this retrospective assessment of established clinical and laboratory tools.
Conclusion
In conclusion, TB in children and adolescents predominantly affects older individuals and is primarily characterised by newly diagnosed cases. The nomogram model developed in this study effectively predicts the risk of DR-TB in paediatric patients, with an AUC of 0.776. Key predictive factors include a retreatment history, smoking history, right middle lobe involvement and cavity formation. The GeneXpert MTB/RIF assay demonstrated a sensitivity of 87.5% for detecting RIF resistance and showed good concordance with DST, supporting its role as an early screening tool for DR-TB in paediatric patients. No significant changes were observed in T-lymphocyte subsets in DR-TB cases, in contrast to findings from adult studies, underscoring the need for further validation with larger sample sizes.
Abbreviations
AFB, acid-fast bacilli; AUC, area under the curve; BCG, Bacillus Calmette–Guérin; CI, confidence interval; DCA, decision curve analysis; DR-TB, drug-resistant tuberculosis; DS-TB, drug-susceptible tuberculosis; DST, drug susceptibility testing; EMB, ethambutol; EPTB, extrapulmonary tuberculosis; HIV, human immunodeficiency virus; INH, isoniazid; MDR-TB, multidrug-resistant tuberculosis; MTB, Mycobacterium tuberculosis; OR, odds ratio; PTB, pulmonary tuberculosis; RIF, rifampicin; ROC, receiver operating characteristic; RR-TB, rifampicin-resistant tuberculosis; STR, streptomycin; TB, tuberculosis; WHO, World Health Organization; LAMP: loop-mediated isothermal amplification.
Ethics Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Research Ethics Committee of The First Affiliated Hospital of Henan Medical University (formerly The First Affiliated Hospital of Xinxiang Medical University). Due to the nature of retrospective study and anonymized patien’s information, informed consent is waived with the approval of Ethics Committee of The First Affiliated Hospital of Xinxiang Medical University. All methods were carried out in accordance with relevant guidelines and regulations.
Funding
Open Project of tuberculosis Research Institute of Xinxiang Medical University (NO.XYJHB202105); Medical Science and Technology Research Joint Venture Project Foundation of Henan Province (No. LHGJ20220614, Wang Lingchao).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Organization W H. Global tuberculosis report 2023 [M]. 2023.
2. Guidance for National Tuberculosis Programmes on the Management of Tuberculosis in Children. Geneva; 2014.
3. Sun J, Fan L, Zhao Y, et al. Analysis of drug-resistant tuberculosis in children in shenyang, China, 2017-2021. Infect Drug Resist. 2023;16(6983–98.
4. Cheng N, Wu S, Luo X, et al. A comparative study of chest computed tomography findings: 1030 cases of drug-sensitive tuberculosis versus 516 cases of drug-resistant tuberculosis. Infect Drug Resist. 2021;14:1115–18. doi:10.2147/IDR.S300754
5. Tao NN, Li YF, Song WM, et al. Risk factors for drug-resistant tuberculosis, the association between comorbidity status and drug-resistant patterns: a retrospective study of previously treated pulmonary tuberculosis in Shandong, China, during 2004-2019. BMJ Open. 2021;11(6):e044349. doi:10.1136/bmjopen-2020-044349
6. Jiang F, Xu C, Wang Y, et al. A CT-based radiomics analyses for differentiating drug‑resistant and drug-sensitive pulmonary tuberculosis. BMC Med Imaging. 2024;24(1):307. doi:10.1186/s12880-024-01481-4
7. Khan N, Vidyarthi A, Amir M, et al. T-cell exhaustion in tuberculosis: pitfalls and prospects. Crit Rev Microbiol. 2017;43(2):133–141. doi:10.1080/1040841X.2016.1185603
8. Song T, Li LJ, Liu JL, et al. Study on the relationship between changes of immune cells and TNF-alpha in peripheral blood of patients with multidrug-resistant and extensively drug-resistant tuberculosis. Eur Rev Med Pharmacol Sci. 2018;22(4):1061–1065. doi:10.26355/eurrev_201802_14389
9. Kiran B, Cagatay T, Clark P, et al. Can immune parameters be used as predictors to distinguish between pulmonary multidrug-resistant and drug-sensitive tuberculosis? Arch Med Sci. 2010;6(1):77–82. doi:10.5114/aoms.2010.13511
10. Dunn JJ, Starke JR, Revell PA. Laboratory diagnosis of Mycobacterium tuberculosis infection and disease in children. J Clin Microbiol. 2016;54(6):1434–1441. doi:10.1128/JCM.03043-15
11. Yang R, Liu M, Jiang H, et al. The epidemiology of pulmonary tuberculosis in children in Mainland China, 2009-2015. Arch Dis Child. 2020;105(4):319–325. doi:10.1136/archdischild-2019-317635
12. Automated Real-Time Nucleic Acid Amplification Technology for Rapid and Simultaneous Detection of Tuberculosis and Rifampicin Resistance: Xpert MTB/RIF Assay for the Diagnosis of Pulmonary and Extrapulmonary TB in Adults and Children: Policy Update. Geneva; 2013.
13. Khan A, Khan N, Singh R. Tuberculosis diagnosis versus GeneXpert®MTB/RIF formats. Bioanalysis. 2024(16(16):843–848.
14. Xu Y, Li Q, Zhu M, et al. The epidemiological characteristics and profile of drug-resistant tuberculosis among children with tuberculosis in Sichuan, China, 2015-2018: a retrospective study. Medicine. 2020;99(43):e22608. doi:10.1097/MD.0000000000022608
15. WS 288-2017 Diagnosis of pulmonary tuberculosis. Int J Tuberc Lung Dis. 2024;5(04):376–378.
16. WS 196-2017 Tuberculosis Classification. Int J Tuberc Lung Dis. 2024;5(04):379–380.
17. Zhang Y, Zhao R, Zhang Z, et al. Analysis of factors influencing multidrug-resistant tuberculosis and validation of whole-genome sequencing in children with drug-resistant tuberculosis. Infect Drug Resist. 2021;14:4375–4393. doi:10.2147/IDR.S331890
18. Wiseman CA, Gie RP, Starke JR, et al. A proposed comprehensive classification of tuberculosis disease severity in children. Pediatr Infect Dis J. 2012;31(4):347–352. doi:10.1097/INF.0b013e318243e27b
19. Onis MD, Garza C, Onyango AW, et al. WHO child growth standards based on length/height, weight and age. Acta Paediatr Suppl. 2006;450:76–85. doi:10.1111/j.1651-2227.2006.tb02378.x
20. H OW. Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. 2017: M.
21. B CB, Zhang Y, Zou H, et al. Survival analysis of patients with tuberculosis and risk factors for multidrug-resistant tuberculosis in Monrovia, Liberia. PLoS One. 2021;16(4):e0249474. doi:10.1371/journal.pone.0249474
22. Peng T, Wonganan O, Zhang Z, et al. A 2-benzylmalonate derivative as stat3 inhibitor suppresses tumor growth in hepatocellular carcinoma by upregulating β-TrCPE3Ubiquitin ligase. Int J Mol Sci. 2021;22(7):3354. doi:10.3390/ijms22073354
23. Efthimiou O, Hoogland J, Debray TPA, et al. Measuring the performance of prediction models to personalize treatment choice. Stat Med. 2023;42(8):1188–1206. doi:10.1002/sim.9665
24. Sing T, Sander O, Beerenwinkel N, et al. ROCR: visualizing classifier performance in R. Bioinformatics. 2005;21(20)):3940–3941. doi:10.1093/bioinformatics/bti623
25. Vickers AJ, van Calster, Steyerberg EW, van Calster B. A simple, step-by-step guide to interpreting decision curve analysis. Diagn Progn Res. 2019;3:18. doi:10.1186/s41512-019-0064-7
26. Hart PD, Sutherland IA. BCG and vole bacillus vaccines in the prevention of tuberculosis in adolescence and early adult life. Br Med J. 1977;2(6082):293–295. doi:10.1136/bmj.2.6082.293
27. Dheda K, Chang KC, Guglielmetti L, et al. Clinical management of adults and children with multidrug-resistant and extensively drug-resistant tuberculosis. Clin Microbiol Infect. 2017;23(3):131–140. doi:10.1016/j.cmi.2016.10.008
28. Li T, Yan X, Du X, et al. Extrapulmonary tuberculosis in China: a national survey. Int J Infect Dis. 2023;128:69–77. doi:10.1016/j.ijid.2022.12.005
29. Song WM, Li YF, Liu YX, et al. Drug-resistant tuberculosis among children: a systematic review and meta-analysis. Front Public Health. 2021;9(721817). doi:10.3389/fpubh.2021.721817.
30. Li M, Deng B, Huang Y, et al. Trends and risk factors for drug-resistant tuberculosis among children in Sichuan, China: a 10-year retrospective analysis, 2013-2022. Medicine. 2024;103(15):e37643. doi:10.1097/MD.0000000000037643
31. Altet N, Latorre I, A J-FM, et al. Tobacco Smoking and Second-Hand Smoke Exposure Impact on Tuberculosis in Children. J Clin Med. 2022;11(7):2000. doi:10.3390/jcm11072000
32. Ali S, R RN, Ashraf, et al. Comparative analysis of culture and sputum smear conversion timelines and their associated factors in smokers versus non-smokers with drug-resistant tuberculosis. Cureus. 2025;17(3):e80704. doi:10.7759/cureus.80704
33. CHuchottaworn C, Thanachartwet V, Sangsayunh P, et al. Risk factors for multidrug-resistant tuberculosis among patients with pulmonary tuberculosis at the central chest institute of Thailand. PLoS One. 2015;10(10):e0139986. doi:10.1371/journal.pone.0139986
34. Wong KS, Huang YC, Lai SH, et al. Validity of symptoms and radiographic features in predicting positive AFB smears in adolescents with tuberculosis. Int J Tuberc Lung Dis. 2010;14(2):155–159.
35. Yang F, Yu H, Kantipudi K, et al. Differentiating between drug-sensitive and drug-resistant tuberculosis with machine learning for clinical and radiological features. Quant Imaging Med Surg. 2022;12(1):675–687. doi:10.21037/qims-21-290
36. Ihms EA, Urbanowski ME, Bishai WR. Diverse cavity types and evidence that mechanical action on the necrotic granuloma drives tuberculous cavitation. Am J Pathol. 2018;188(7):1666–1675. doi:10.1016/j.ajpath.2018.04.006
37. Wang YXJ, Chung MJ, Skrahin A, et al. Radiological signs associated with pulmonary multi-drug resistant tuberculosis: an analysis of published evidences. Quant Imaging Med Surg. 2018;8(2):161–173. doi:10.21037/qims.2018.03.06
38. Li D, He W, Chen B, et al. Primary multidrug-resistant tuberculosis versus drug-sensitive tuberculosis in non-HIV-infected patients: comparisons of CT findings. PLoS One. 2017;12(6):e0176354. doi:10.1371/journal.pone.0176354
39. Walker NF, Stek C, Wasserman S, et al. The tuberculosis-associated immune reconstitution inflammatory syndrome: recent advances in clinical and pathogenesis research. Curr Opin HIV AIDS. 2018;13(6):512–521. doi:10.1097/COH.0000000000000502
40. Ma W, Wang LC, Zhao DA, et al. Analysis of T-lymphocyte subsets and risk factors in children with tuberculosis. Tuberculosis. 2024;146:102496. doi:10.1016/j.tube.2024.102496
41. Li K, Ran R, JIang Z, et al. Changes in T-lymphocyte subsets and risk factors in human immunodeficiency virus-negative patients with active tuberculosis. Infection. 2020;48(4):585–595. doi:10.1007/s15010-020-01451-2
42. Lavu EK, Johnson K, Banamu J, et al. Drug-resistant tuberculosis diagnosis since Xpert((R)) MTB/RIF introduction in Papua New Guinea, 2012-2017. Public Health Action. 2019;9(Suppl 1):S12–S8. doi:10.5588/pha.19.0005
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Risk Factors and Predictive Model for Dermatomyositis Associated with Rapidly Progressive Interstitial Lung Disease
Wang K, Tian Y, Liu S, Zhang Z, Shen L, Meng D, Li J
Pharmacogenomics and Personalized Medicine 2022, 15:775-783
Published Date: 1 September 2022
Development and Validation of Machine Learning Models for Prediction of Fracture Risk in Patients with Elderly-Onset Rheumatoid Arthritis
Chen R, Huang Q, Chen L
International Journal of General Medicine 2022, 15:7817-7829
Published Date: 14 October 2022
The Incidence, Risk Factors, and Predictive Model of Obstructive Disease in Post-Tuberculosis Patients
Chang W, Li Z, Liang Q, Zhao W, Li F
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:2457-2466
Published Date: 19 November 2024
A QuantiFERON®-TB Gold Plus-Based Model for Predicting Latent Tuberculosis Infection in Patients with Diabetes
Zhou J, Lin X, Yu Y, Zhang Y, Qiu L, Lin Z, Jiang X, Shi J
Infection and Drug Resistance 2026, 19:581374
Published Date: 29 May 2026