Back to Journals » Neuropsychiatric Disease and Treatment » Volume 22
A Machine Learning and Traditional Chinese Medicine Constitution–Based Prediction Model for Mild Cognitive Impairment in Community-Dwelling Older Adults
Authors Xu Q, Huang Z ![]() , Su W, Cai A, Chen Z, Zhou W, Li J, Chen X
, Su W, Cai A, Chen Z, Zhou W, Li J, Chen X
Received 12 March 2026
Accepted for publication 4 June 2026
Published 17 June 2026 Volume 2026:22 608660
DOI https://doi.org/10.2147/NDT.S608660
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Qixin Xu,1,2,* Zhijie Huang,2,3,* Weiyang Su,1 Aiwu Cai,1 Zhuzhang Chen,1 Wanfei Zhou,1 Junyong Li,1 Xiaomei Chen4
1Public Health Department, Shiqi Town Community Public Health Service Center, Guangzhou, Guangdong, People’s Republic of China; 2Faculty of Medicine, Macau University of Science and Technology, Macao SAR, People’s Republic of China; 3Public Health Department, Dashi Street Community Public Health Service Center, Guangzhou, Guangdong, People’s Republic of China; 4Administrative Office, Panyu District Community Health Service Management Center, Guangzhou, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaomei Chen, Administrative Office, Panyu District Community Health Service Management Center, Guangzhou, Guangdong, 511400, People’s Republic of China, Email [email protected]
Objective: To develop and validate a nomogram screening model for mild cognitive impairment (MCI) in community-dwelling older adults by integrating Traditional Chinese Medicine (TCM) constitution classification with machine learning–based feature selection, aiming to provide a practical tool for early identification in primary care.
Methods: A cross-sectional study was conducted among 1,503 older adults (aged ≥ 60 years) at a community health service center in Guangzhou, China. Data were prospectively collected during standardized community health examinations between January and December 2025. Participants were randomly divided into training (n = 1,052) and validation (n = 451) sets. Four machine learning algorithms—LASSO regression, random forest, decision tree, and XGBoost—were applied to identify stable predictors. Variables selected by all four methods were entered into multivariable logistic regression, and a nomogram was constructed. Model performance was assessed using the area under the receiver operating characteristic curve (AUC), calibration curves, and decision curve analysis (DCA).
Results: The prevalence of MCI, defined by education-adjusted Chinese Mini-Mental Status (CMMS) cutoffs based on Petersen criteria, was 24.1%. Seven independent correlates were identified: increasing age, female sex, Qi-deficiency constitution, Yin-deficiency constitution, elevated serum creatinine, regular physical exercise, and Balanced constitution. The nomogram achieved AUCs of 0.813 (training) and 0.747 (validation), with satisfactory calibration. Adding TCM constitution to a clinical reference model significantly improved predictive performance (NRI > 0, p < 0.05).
Conclusion: The nomogram incorporating TCM constitution types demonstrated good discrimination, calibration, and clinical utility for community-based MCI screening, providing a practical tool for early identification and risk stratification in primary care settings.
Keywords: mild cognitive impairment, machine learning, traditional Chinese medicine constitution, prediction model, nomogram, community-dwelling older adults
Introduction
Dementia is a neurodegenerative syndrome characterized by progressive cognitive decline that profoundly impairs daily functioning. The accelerating pace of global population aging has driven a marked increase in dementia incidence worldwide. Current estimates indicate that more than 55 million people are living with dementia globally, a figure projected to rise significantly by 2050.1 China bears a particularly severe burden, with approximately 10 million people living with dementia, accounting for roughly 20% of all cases worldwide.2 Mild cognitive impairment (MCI), defined as the transitional state between normal aging and dementia, represents a critical window for early intervention. Delaying the onset of dementia through effective identification at the MCI stage could substantially reduce the projected prevalence.3 Developing accurate and accessible tools for early MCI screening is therefore of considerable strategic importance for the primary prevention of dementia. In community-based screening, the Petersen criteria remain the widely accepted diagnostic gold standard, requiring subjective cognitive complaints, objective cognitive impairment, preserved independence in daily living, and the absence of dementia. To operationalize these criteria within the constraints of large-scale primary care settings, researchers increasingly rely on validated two-step screening protocols—combining brief dementia screening instruments (eg., the Eight-item Informant Interview to Differentiate Aging and Dementia [AD8]) with objective neuropsychological tests (eg., the Chinese Mini-Mental Status [CMMS] with education-adjusted cutoffs) to balance diagnostic accuracy with screening efficiency.4,5
The Traditional Chinese Medicine (TCM) concept of “preventive treatment of disease” holds important guiding significance in disease prevention. Central to this concept is the TCM constitution, which refers to the relatively stable, inherent characteristics of an individual’s morphological structure, physiological functions, and psychological state.6 According to the industry standard established by the China Association of Chinese Medicine (ZYYXH/T 157–2009), individuals are classified into one balanced constitution (normality) and eight unbalanced (pathological) constitutions, such as Qi-deficiency, Yin-deficiency, and Phlegm-dampness, which are systematically evaluated using standardized instruments like the Constitution in Chinese Medicine Questionnaire (CCMQ).6,7 Individual constitutional differences directly influence disease susceptibility and developmental tendencies.
Recent evidence provides a biological and clinical rationale linking specific TCM constitution types with cognitive impairment. For example, pathological constitutions such as Yang-deficiency, Phlegm-dampness, and Blood-stasis have been identified as independent risk factors for MCI, often accompanied by elevated serum homocysteine and markers of oxidative stress (eg., 8-iso-PGF2α), which contribute to vascular endothelial dysfunction and accelerated amyloid-beta (Aβ) formation.8 Furthermore, the Phlegm-dampness constitution is strongly associated with metabolic syndrome, dyslipidemia, and chronic inflammation—characterized by elevated pro-inflammatory cytokines (eg., IL-12) and altered lymphocyte profiles—which are critical culprits in cardiovascular diseases and subsequent cognitive decline.9 Collectively, TCM constitution types serve as macroscopic phenotypic markers reflecting underlying metabolic, immune, and neurovascular dysregulations.
Machine learning methods have demonstrated unique advantages in disease risk prediction. While previous studies have constructed MCI prediction models using various algorithms, they have predominantly focused on clinical specialty populations and restricted their predictive indicators to biological markers.10 This highlights a significant research gap: there is a lack of community-based models that integrate holistic TCM constitution assessments with modern machine learning techniques to predict MCI. Furthermore, cognitive decline is influenced by a complex interplay of demographic, lifestyle, and health-related factors.11 To improve the robustness of the study context, the selection of variables for predictive modeling must be comprehensive, incorporating not only routine laboratory parameters and TCM constitution types but also potential confounders such as education level, socioeconomic status, medication use, and comorbid neuropsychiatric conditions.5,11
Against this background, the present study recruited community-dwelling older adults from Panyu District, Guangzhou. While this represents a specific community population, it provides a representative sample of the rapidly aging urban demographic in southern China, enhancing the external validity of the findings for similar community settings. We innovatively incorporated TCM constitution classification into a machine learning–assisted MCI prediction framework. Four machine learning algorithms (LASSO regression, random forest, decision tree, and XGBoost) were applied in combination to identify stable MCI-associated features. Multivariable logistic regression was subsequently used to determine independent predictors, and a nomogram integrating TCM constitution was developed and validated. This study aims to provide a practical, robust, and evidence-based tool for early MCI screening and risk stratification in primary care.
Material and Methods
Study Population
This cross-sectional study collected data from residents who participated in free health examinations provided under the National Basic Public Health Service program at the Community Health Service Center of Shiqi Town, Panyu District, Guangzhou. All clinical, laboratory, and TCM constitution data were prospectively collected at a single time point during these scheduled health examinations. Therefore, the study design is inherently cross-sectional, capturing a snapshot of the participants’ health status. Inclusion criteria were: (1) community-dwelling older adults aged ≥60 years; and (2) provision of written informed consent and voluntary participation. Exclusion criteria were: (1) pre-existing diagnosis of dementia, severe psychiatric disorders (eg., schizophrenia, major depressive disorder), or major neurological diseases (eg., Parkinson’s disease, severe stroke) that could confound cognitive assessment; (2) severe hearing or visual impairment precluding completion of assessments; and (3) missing information on essential eligibility or cognitive-outcome variables that precluded MCI classification; participants with missing values in eligible continuous laboratory predictors were retained and handled by the prespecified imputation strategy described below. A total of 1,503 community-dwelling older adults were ultimately enrolled, comprising 610 men and 893 women, with ages ranging from 60 to 96 years and a median age of 71.00 (interquartile range [IQR]: 68.00–74.00) years.
Data Collection and Randomization
Participants were allocated to a training set (n = 1,052) and a validation set (n = 451) in a 7:3 ratio using stratified random sampling according to key baseline characteristics. The baseline characteristics of the training and validation sets are presented in Table 1. Within the training set, participants were further stratified by MCI status into an MCI group (n = 243) and a non-MCI group (n = 809). This study was approved by the Ethics Committee of the Community Health Service Center of Shiqi Town, Panyu District, Guangzhou (Approval No.: [2025] Ethics Approval No. 001), and all participants provided written informed consent.
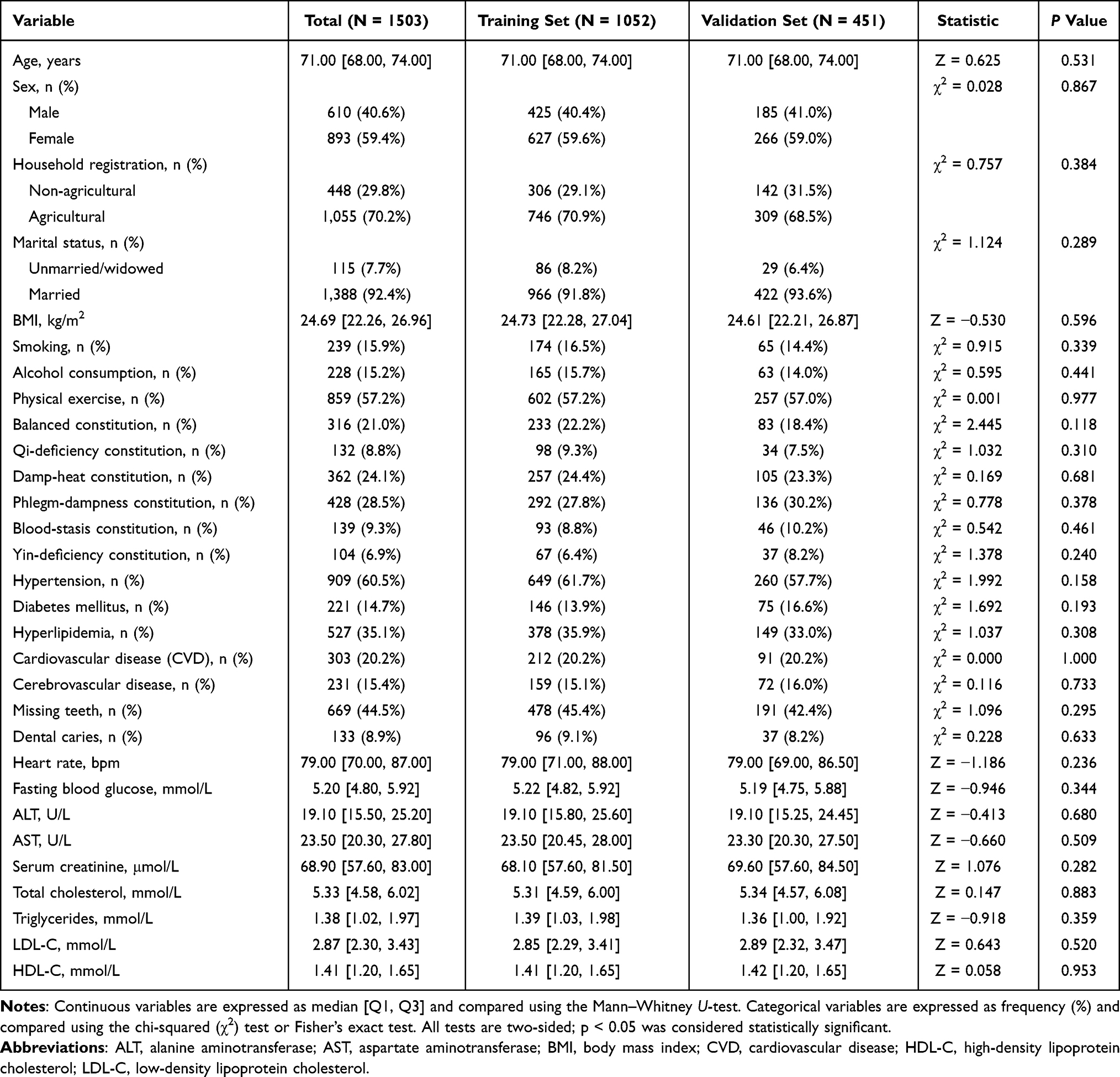 |
Table 1 Baseline Characteristics of the Training and Validation Sets (n = 1503) |
Multidimensional clinical data were collected through questionnaire interviews, physical examinations, laboratory testing, and TCM constitution assessment at the time of the community health examination. Data collection encompassed five domains: (1) demographic characteristics and lifestyle factors, including age, sex, household registration type (agricultural/non-agricultural), marital status, smoking history, alcohol consumption history, regular physical exercise, and body mass index (BMI); (2) TCM constitution types, nine types are defined by the Classification and Determination of TCM Constitutions standard (one Balanced and eight unbalanced types). The six most prevalent types in this sample—Balanced, Qi-deficiency, Damp-heat, Phlegm-dampness, Blood-stasis, and Yin-deficiency—were assessed by qualified TCM practitioners using the Constitution in Chinese Medicine Questionnaire (CCMQ) and coded as binary variables. The Balanced type is mutually exclusive with unbalanced types, whereas the latter may coexist. (3) comorbidities and oral health status, including hypertension, diabetes mellitus, hyperlipidemia, cardiovascular disease (CVD), cerebrovascular disease, missing teeth, and dental caries; (4) laboratory parameters, including heart rate, fasting blood glucose, white blood cell count, serum alanine aminotransferase (ALT), serum aspartate aminotransferase (AST), serum creatinine (Scr), blood urea nitrogen (BUN), total cholesterol (TC), triglycerides (TG), low-density lipoprotein cholesterol (LDL-C), and high-density lipoprotein cholesterol (HDL-C); and (5) cognitive function assessment, performed using a two-step screening protocol to operationalize the Petersen diagnostic criteria. Subjective cognitive complaints were first assessed using the AD8 administered directly to the participants, with a score of ≥2 indicating self-perceived cognitive decline. Objective cognitive impairment was subsequently evaluated using the Chinese Mini-Mental Status (CMMS). MCI was defined by meeting both criteria: (a) an AD8 score ≥2, and (b) a CMMS score below the education-adjusted cutoffs (<20 for illiterate individuals, <23 for those with primary school education, and <27 for those with middle school education or above.5,12 The requirements for preserved activities of daily living and absence of dementia were implicitly met, as all participants were capable of independently attending the community health center and completing the comprehensive health examination and assessments.
Statistical Analysis
All statistical analyses were performed using SPSS version 26.0 and R version 4.1.0. Continuous variables were confirmed to deviate from normality by the Shapiro–Wilk test and are expressed as median (IQR); between-group comparisons were performed using the Mann–Whitney U-test. Categorical variables are expressed as frequency and percentage (%), with between-group comparisons performed using the chi-squared (χ2) test or Fisher’s exact test. All tests were two-sided, and p <0.05 was considered statistically significant. Before model development, the extent and pattern of missing data were quantified for each candidate predictor. Missingness ranged from 0% to 59.88% across variables and was concentrated in selected laboratory parameters rather than in demographic characteristics, TCM constitution variables, comorbidities, lifestyle factors, or the MCI outcome. Because the missing laboratory values arose from routine community health-examination testing and recording procedures and were not part of the cognitive assessment process, the mechanism was considered plausibly missing at random. To reduce selection bias and avoid the loss of statistical power caused by complete case analysis, missing continuous laboratory values were imputed using mean imputation. After mean imputation, all 1,503 eligible participants were retained for model training and validation.
The prevalence of mild cognitive impairment (MCI) in our target population is 28.6%.13 denote this expected event proportion as p. To ensure model stability and mitigate overfitting, we adopted the events-per-variable (EPV) principle with a target EPV of 10, adapted for penalised logistic regression and feature selection. Using the formula N = (k × EPV) / p, and substituting k = 30, EPV = 10, and p = 0.286, we obtained N = 1049. Our study ultimately included 1503 participants, well above this requirement. The observed number of MCI events was 362, yielding an actual EPV of 362 / 30 = 12.1, which exceeds the prespecified threshold of 10. Therefore, the sample size provides adequate statistical power and scientific justification for both model development and internal validation.
Machine Learning Feature Selection
Four machine learning algorithms were applied to the training set to comprehensively identify candidate predictors of MCI. (1) LASSO regression was implemented using the R package glmnet, with the optimal penalty parameter λ determined by 10-fold cross-validation using the minimum cross-validation error criterion (lambda.min); variables whose regression coefficients were shrunk to zero were considered excluded. (2) Random forest was implemented using the randomForest package, with feature importance quantified by the mean decrease in Gini impurity. The random forest model was run under the package-default classification settings, and all unspecified parameters were kept at their default values to ensure reproducibility. (3) Decision tree was implemented using the CART algorithm via the rpart package, with feature importance assessed by Gini importance scores. The CART model was fitted using the default complexity-pruning settings of the rpart package, and all unspecified parameters were kept at their default values. (4) XGBoost was implemented using the xgboost package, with feature importance quantified by the Gain metric. For the XGBoost model, the main hyperparameters were set as follows: max_depth = 3, eta = 0.1, and nrounds = 100. Variables consistently selected by all four methods were considered robust candidate predictors and were entered into subsequent multivariable analyses. To enhance the interpretability of feature importance, SHAP (Shapley additive explanations) summary plots were further generated for the four machine-learning models to visualize both the relative contribution and the direction of feature effects.
Multivariable Logistic Regression and Nomogram Construction
All variables jointly identified by the four machine learning methods were simultaneously entered (forced-entry method) into a multivariable logistic regression model. The regression coefficient (β), odds ratio (OR), 95% confidence interval (CI), Wald χ2 statistic, and p-value were calculated for each variable. p <0.05 was considered statistically significant for identifying independent correlates associated with MCI. A nomogram was subsequently constructed using the R package rms, based on variables that achieved statistical significance in the multivariable model.
Model Validation
Model performance was evaluated across three dimensions. (1) Discrimination: receiver operating characteristic (ROC) curves were plotted and AUC values were calculated using the pROC package; the optimal cutoff value was determined by the Youden index (sensitivity + specificity − 1). (2) Calibration: calibration curves were plotted and the Hosmer–Lemeshow goodness-of-fit test was performed; p >0.05 indicated satisfactory calibration. (3) Clinical utility: decision curve analysis (DCA) was performed using the rmda package to evaluate the net clinical benefit of the nomogram relative to the “treat all” and “treat none” strategies. In addition, 10-fold cross-validation ROC analysis was performed in both the training and validation sets to further evaluate the stability and internal robustness of model discrimination.
Sensitivity Analysis
To quantify the incremental predictive value of TCM constitution types beyond traditional risk factors, a sensitivity analysis was performed by comparing two nested logistic regression models. The reference model included traditional risk factors only, namely age, sex, regular physical exercise, and serum creatinine. The full model further incorporated the TCM constitution variables retained in the final nomogram, namely Balanced constitution, Qi-deficiency constitution, and Yin-deficiency constitution. The added predictive value of the full model relative to the reference model was quantified using the total net reclassification improvement (NRI) and integrated discrimination improvement (IDI) in both the training and validation sets.
Results
Baseline Characteristics
A total of 1,503 participants were enrolled in this study, of whom 362 (24.1%) were diagnosed with MCI. Participants were randomly allocated to a training set (n = 1,052) and a validation set (n = 451) in a 7:3 ratio. As shown in Table 1, no statistically significant differences were observed between the training and validation sets with respect to age, sex, household registration type, marital status, BMI, smoking history, alcohol consumption history, exercise habits, TCM constitution types (Balanced, Qi-deficiency, Damp-heat, Phlegm-dampness, Blood-stasis, and Yin-deficiency), comorbidities (hypertension, diabetes mellitus, hyperlipidemia, CVD, and cerebrovascular disease), oral health status (missing teeth and dental caries), or laboratory parameters including heart rate, fasting blood glucose, liver function indices, renal function indices, and lipid profiles (all p > 0.05), indicating that the two sets were well-balanced with respect to baseline characteristics.
The missing-data pattern was further examined before imputation. No missing values were observed for the MCI outcome or for demographic, lifestyle, TCM constitution, comorbidity, oral-health, and most physical-examination variables. Missingness was mainly confined to laboratory indicators: fasting blood glucose had 13.31% missing values; serum alanine aminotransferase, serum aspartate aminotransferase, serum creatinine, blood urea nitrogen, total cholesterol, triglycerides, low-density lipoprotein cholesterol, and high-density lipoprotein cholesterol each had 53.23% missing values; and white blood cell count had 59.88% missing values. After mean imputation, all 1,503 eligible participants were retained for use in model training and validation.
Within the training set, participants were further stratified by MCI status into a non-MCI group (n = 809) and an MCI group (n = 243) (Table 2). Compared with the non-MCI group, the MCI group was significantly older (p < 0.001) and had a higher proportion of female participants and unmarried individuals (both p < 0.05). With regard to lifestyle factors, the MCI group had significantly lower proportions of current smokers, alcohol consumers, and participants engaging in regular physical exercise (all p < 0.05). The distribution of TCM constitution types differed markedly between groups: the proportion of Balanced constitution was significantly lower in the MCI group, whereas the proportions of Qi-deficiency and Yin-deficiency constitutions were significantly higher; the distribution of Phlegm-dampness constitution also differed significantly between groups (all p < 0.01). Regarding comorbidities, the MCI group had higher proportions of hyperlipidemia and cerebrovascular disease than the non-MCI group (p < 0.05), while the prevalences of hypertension, diabetes mellitus, and CVD did not differ significantly between groups (all p > 0.05). With respect to laboratory parameters, fasting blood glucose and serum creatinine levels were both significantly higher in the MCI group than in the non-MCI group (p < 0.05), whereas heart rate, liver function indices, and lipid-related parameters did not differ significantly between groups (all p > 0.05).
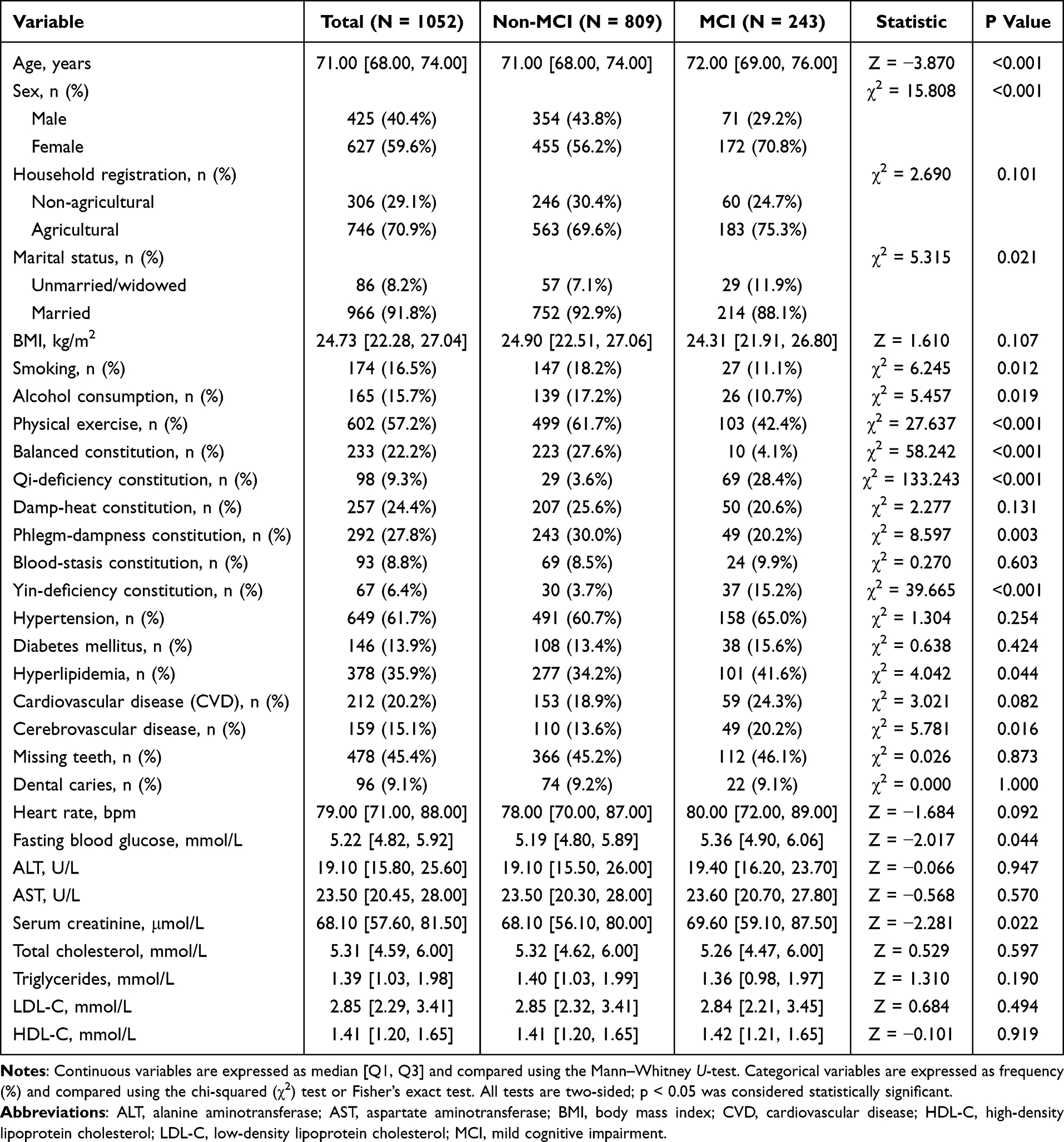 |
Table 2 Baseline Characteristics Stratified by MCI Status in the Training Set |
Machine Learning Feature Selection
In the training set, four machine learning methods—LASSO regression, random forest, decision tree, and XGBoost—were applied to screen clinical features associated with MCI. LASSO regression identified the optimal penalty parameter λ through 10-fold cross-validation; at the optimal λ value, the regression coefficients of several variables were shrunk to zero, retaining only those features most closely associated with MCI occurrence (Figure 1A and 1B). The random forest, decision tree, and XGBoost models ranked variables according to their respective feature importance weights, and while some variation in selected features was observed across methods, a number of consistently important variables were identified across multiple models (Table 3). To improve the visual interpretability of Table 3, SHAP analyses were performed and are presented after the model-validation figures to maintain sequential figure citation. Taking the intersection of variables selected by all four machine learning methods, 14 clinical features were found to recur across models (Figure 2): age, sex, agricultural household registration, marital status, regular exercise, Balanced constitution, Qi-deficiency constitution, Yin-deficiency constitution, heart rate, fasting blood glucose, serum creatinine, total cholesterol, HDL-C, and smoking history. This convergence indicates that these variables demonstrate robust and consistent predictive value for MCI. Based on these machine learning screening results, the overlapping variables were entered into subsequent multivariable logistic regression analysis to further clarify their independent associations with MCI.
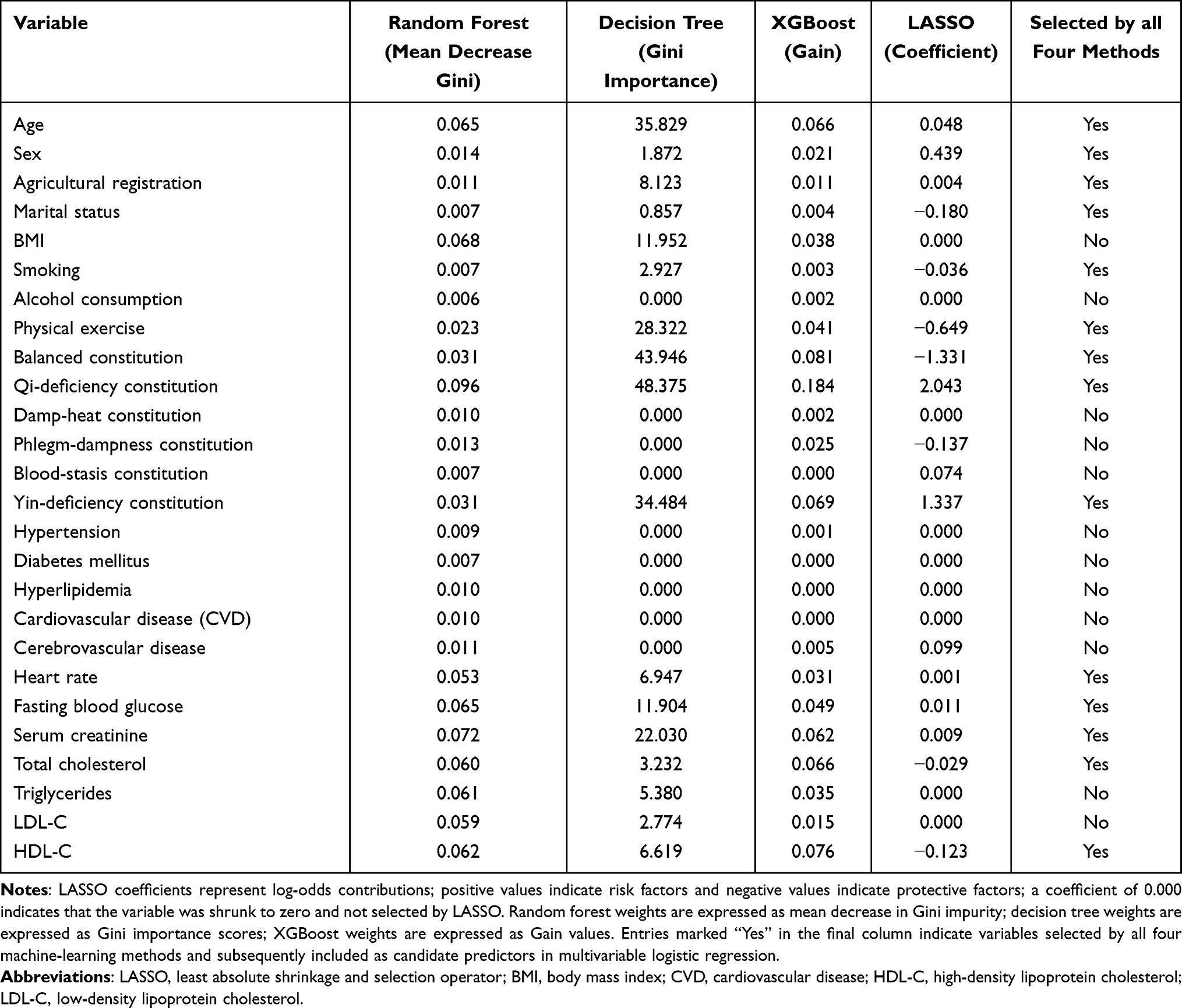 |
Table 3 Feature Importance Weights From Four Machine-Learning Methods |
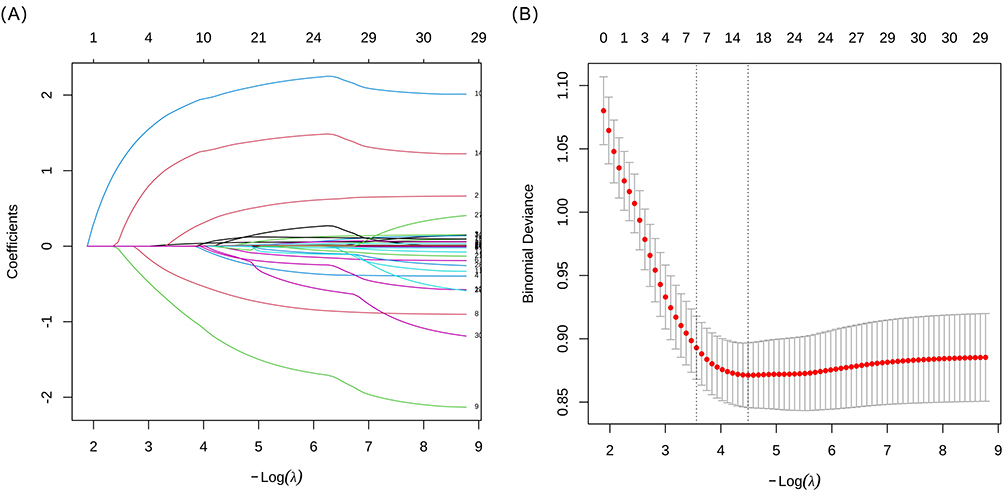 |
Figure 1 Feature selection using LASSO regression. (A) Coefficient trajectories of candidate variables across different values of log(λ). (B) Ten-fold cross-validation curve for selecting the optimal penalty parameter. The lower X-axis represents log(λ), whereas the upper axis indicates the number of non-zero coefficients retained at each λ value. The two vertical dotted lines indicate λmin, corresponding to the minimum cross-validation error, and λ1se, corresponding to the largest λ within one standard error of the minimum. |
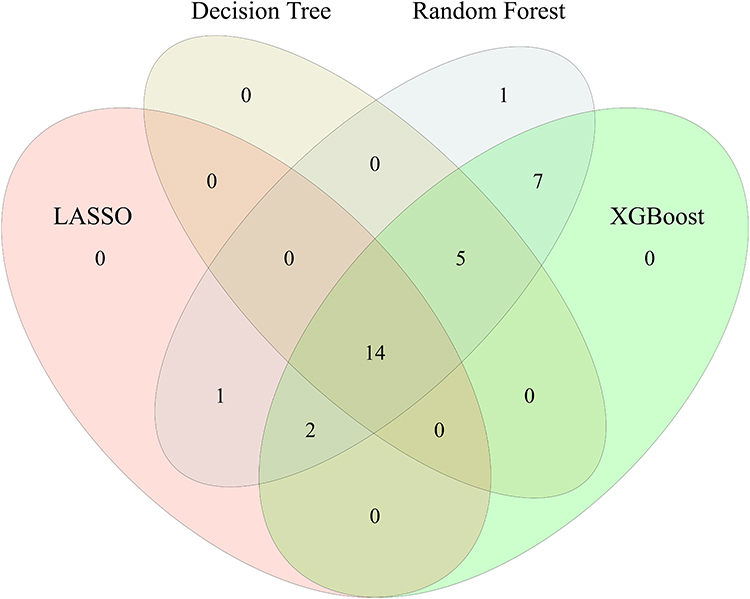 |
Figure 2 Venn diagram illustrating the overlap of features selected by four machine learning. |
Multivariable Logistic Regression Analysis for MCI in the Training Set
The overlapping variables identified by the four machine learning methods were entered into a multivariable logistic regression model in the training set (Table 4). The results demonstrated that increasing age (OR = 1.065, 95% CI: 1.018–1.114, p = 0.006), female sex (OR = 1.916, 95% CI: 1.213–3.029, p = 0.005), Qi-deficiency constitution (OR = 10.609, 95% CI: 6.378–17.647, p < 0.001), Yin-deficiency constitution (OR = 5.017, 95% CI: 2.882–8.733, p < 0.001), and elevated serum creatinine (OR = 1.015, 95% CI: 1.007–1.023, p < 0.001) were significantly associated with an increased risk of MCI. Conversely, regular physical exercise (OR = 0.418, 95% CI: 0.295–0.590, p < 0.001) and Balanced constitution (OR = 0.174, 95% CI: 0.088–0.344, p < 0.001) were identified as independent correlates inversely associated with MCI. In the multivariable model, agricultural household registration, marital status, smoking history, heart rate, fasting blood glucose, total cholesterol, and HDL-C were not significantly associated with MCI (all p > 0.05).
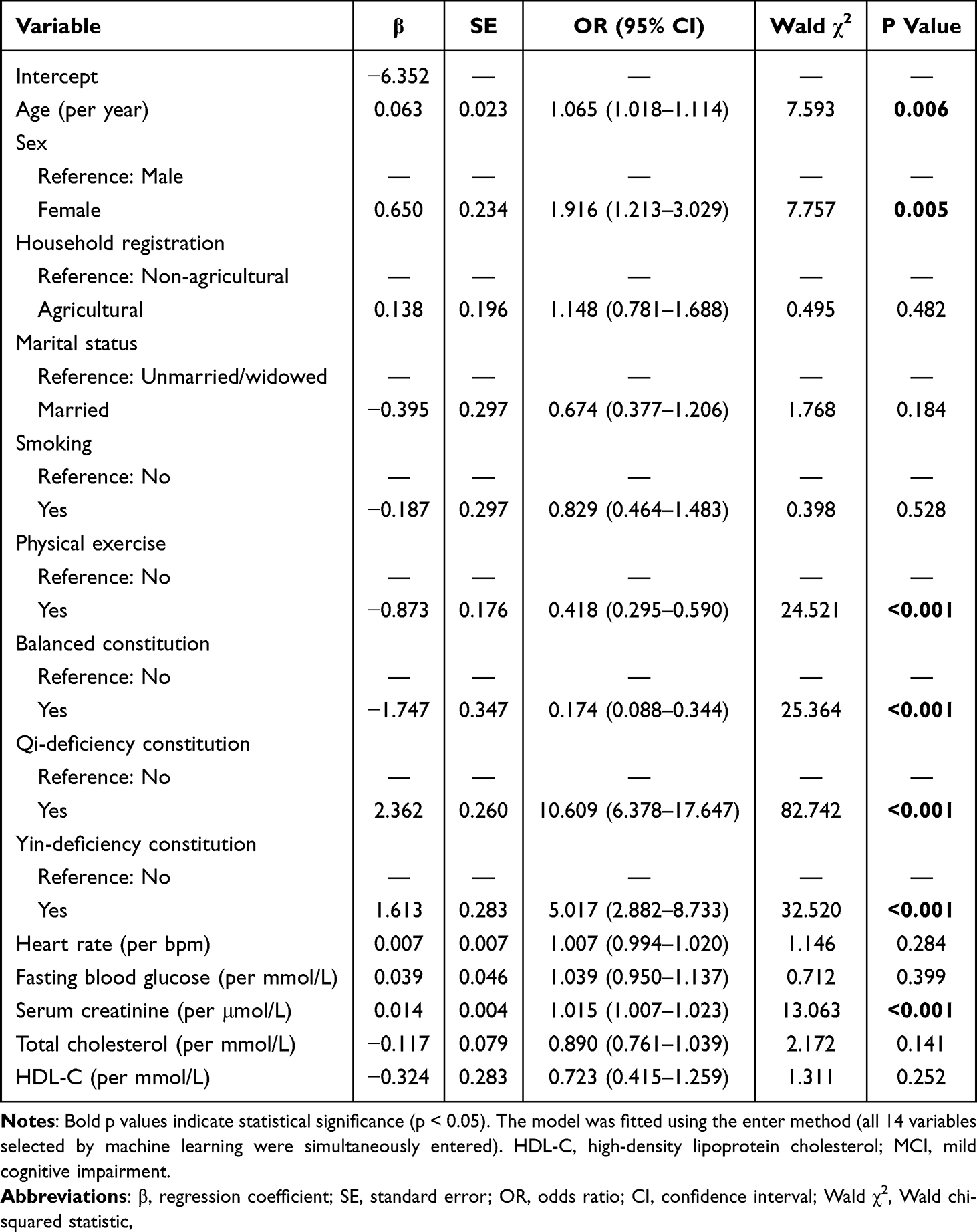 |
Table 4 Multivariable Logistic Regression Analysis for MCI in the Training Set |
Construction and Validation of the Nomogram Prediction Model
Based on the statistically significant variables identified in the multivariable logistic regression analysis—namely age, sex, regular exercise, Balanced constitution, Qi-deficiency constitution, Yin-deficiency constitution, and serum creatinine—a nomogram was constructed to estimate the individual risk of MCI in the training set (Figure 3). Individual MCI risk can be estimated by projecting each predictor value onto the corresponding scale axis, summing the resulting points to obtain a total score, and reading off the corresponding predicted probability; a higher total score corresponds to a greater predicted risk of MCI.
 |
Figure 3 Nomogram prediction model for mild cognitive impairment in the training set. |
The discrimination of the nomogram was evaluated using ROC curves (Figure 4). In the training set, the model achieved an AUC of 0.813 (95% CI: 0.781–0.844), with an optimal cutoff value of 0.270, corresponding to a sensitivity of 0.671 and a specificity of 0.842. In the validation set, the AUC was 0.747 (95% CI: 0.695–0.799), with an optimal cutoff value of 0.304, corresponding to a sensitivity of 0.611 and a specificity of 0.858, indicating satisfactory discriminative ability in both sets. To further assess the stability of discrimination, 10-fold cross-validation ROC analysis was additionally performed. The cross-validated AUCs were 0.806 (95% CI: 0.774–0.839) in the training set and 0.804 (95% CI: 0.773–0.836) in the validation set, indicating highly consistent model performance after cross-validation.
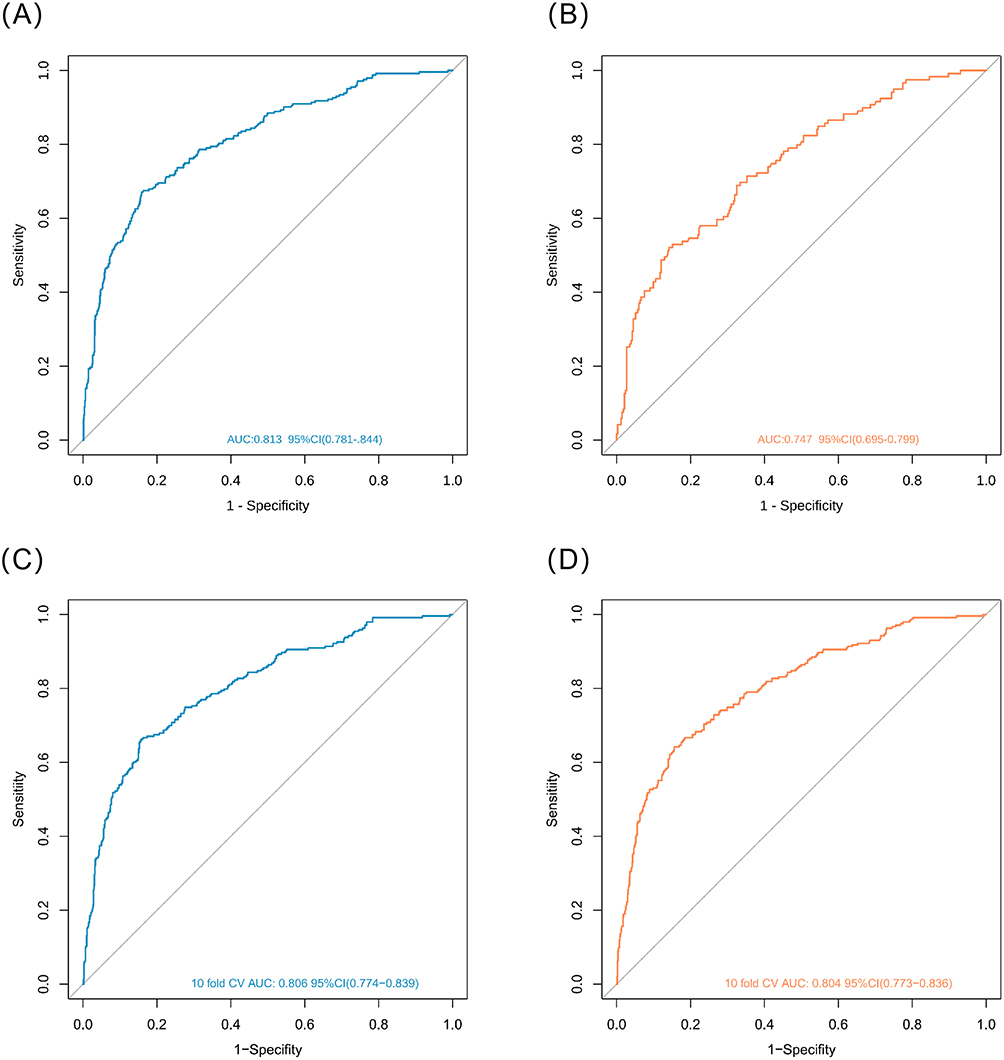 |
Figure 4 Receiver operating characteristic (ROC) curves of the nomogram prediction model for mild cognitive impairment: apparent ROC curves in the training set (A) and validation set (B), and 10-fold cross-validation ROC curves in the training set (C) and validation set (D). |
Calibration curves were used to assess the agreement between predicted probabilities and observed event rates (Figure 5). The Hosmer–Lemeshow goodness-of-fit test yielded χ2 = 8.606, df = 8, p = 0.377 in the training set, and χ2 = 3.888, df = 8, p = 0.867 in the validation set, with neither result indicating significant deviation from perfect calibration. The calibration curves closely approximated the ideal reference line, confirming the model’s satisfactory calibration performance.
 |
Figure 5 Calibration curves of the nomogram prediction model for mild cognitive impairment in the training set (A) and validation set (B). The diagonal dashed line represents perfect calibration; the solid line represents the observed calibration performance of the model. |
DCA was further applied to evaluate the clinical utility of the nomogram (Figure 6). Across both the training and validation sets, the nomogram yielded greater net benefit than either the “treat all” or “treat none” strategy across a wide range of risk threshold probabilities, indicating meaningful clinical utility in decision-making.
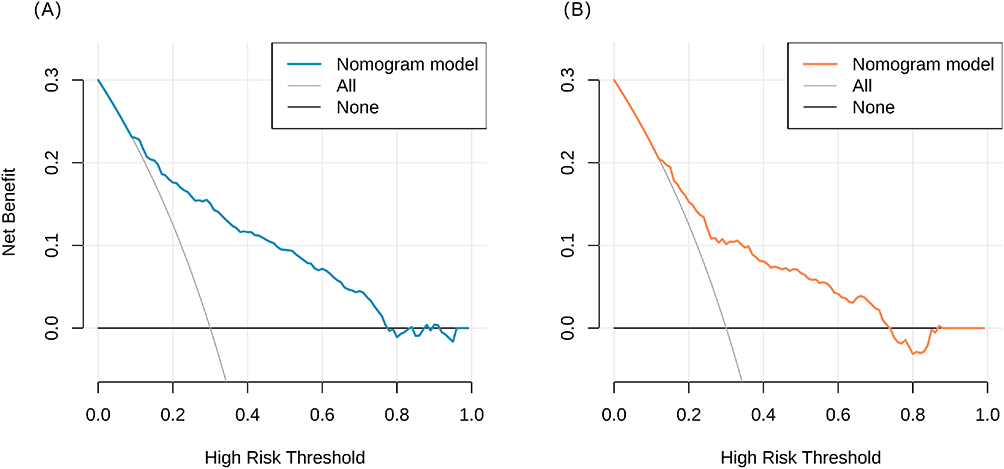 |
Figure 6 Decision curve analysis (DCA) of the nomogram prediction model for mild cognitive impairment in the training set (A) and validation set (B). |
To further support the interpretability of the machine-learning feature-selection results, SHAP summary plots were examined after the model validation analyses (Figure 7). The SHAP visualization showed that TCM constitution-related variables, particularly Qi-deficiency constitution, Balanced constitution, and Yin-deficiency constitution, together with physical exercise, age, sex, and serum creatinine, were among the most influential features across the four models, supporting the robustness and clinical interpretability of the feature-selection results.
 |
Figure 7 SHAP summary plots for feature importance interpretation across the four machine-learning models (XGBoost, random forest, decision tree, and LASSO). Each point represents one participant, the horizontal axis indicates the SHAP value, and the color gradient represents the original feature value from low to high. |
Sensitivity Analysis
To further evaluate whether TCM constitution types provided additional predictive information beyond traditional risk factors, a reference model including age, sex, regular physical exercise, and serum creatinine was compared with the full model additionally incorporating Balanced constitution, Qi-deficiency constitution, and Yin-deficiency constitution. The addition of TCM constitution variables significantly improved model performance in both datasets. In the training set, the total NRI was 0.3020 (95% CI: 0.2357–0.3732, p<0.001), and the total IDI was 0.1869 (95% CI: 0.1559–0.2180, p<0.001). In the validation set, the total NRI was 0.2412 (95% CI: 0.1539–0.3345, p<0.001), and the total IDI was 0.1378 (95% CI: 0.0959–0.1805, p<0.001). These findings indicate that incorporating TCM constitution types provided meaningful incremental predictive value beyond traditional risk factors.
Discussion
This study leveraged community health examination data from older adults and applied four machine learning methods—LASSO regression, random forest, decision tree, and XGBoost—to screen MCI-associated features. A nomogram prediction model integrating TCM constitution was subsequently developed and validated through multivariable logistic regression. The results demonstrated that increasing age (OR = 1.065), female sex (OR = 1.916), Qi-deficiency constitution (OR = 10.609), Yin-deficiency constitution (OR = 5.017), and elevated serum creatinine (OR = 1.015) were independently and positively associated with MCI, while regular physical exercise (OR = 0.418) and Balanced constitution (OR = 0.174) were independently and inversely associated with MCI. The model based on these seven variables achieved an AUC of 0.813 (95% CI: 0.781–0.844) in the training set and 0.747 (95% CI: 0.695–0.799) in the validation set; additional 10-fold cross-validation yielded similar AUCs in the training set (0.806, 95% CI: 0.774–0.839) and validation set (0.804, 95% CI: 0.773–0.836), supporting stable discriminative performance; calibration curves and DCA both confirmed satisfactory calibration and favorable net clinical benefit. Sensitivity analysis further demonstrated that adding TCM constitution variables to a traditional risk-factor model significantly improved reclassification and discrimination in both the training and validation sets. Given that all predictors can be obtained through routine community health examinations, this model is well-suited for implementation in community health service centers and provides a practical tool for early MCI screening and risk stratification among older adults.
Associations Between TCM Constitution Types and MCI Risk: Mechanisms and Implications
It is important to emphasize that TCM constitution types represent macroscopic phenotypic classifications based on clusters of somatic symptoms and functional states, rather than one-to-one equivalents of specific biomedical diagnoses. The association between TCM constitution types and MCI risk constitutes the central finding of this study. Qi-deficiency constitution (OR = 10.609) and Yin-deficiency constitution (OR = 5.017) emerged as the strongest independent correlates positively associated with MCI, while Balanced constitution (OR = 0.174) demonstrated a pronounced inverse association with MCI. These findings align with results from multiple prior studies. Deng et al8 examined 214 older adults from a hospital memory clinic and health examination center and found that Yang-deficiency, Phlegm-dampness, and Blood-stasis constitutions were independently associated with MCI. Qiao et al14 conducted a multicenter study spanning three regions of China and found that Qi-stagnation constitution (OR = 14.37) and Qi-deficiency constitution (OR = 4.48) were independently associated with cognitive frailty, with sleep quality partially mediating the association between Qi-stagnation constitution and cognitive frailty (mediation proportion: 22.7%). Zhang et al15 confirmed in a cohort of 313 older adults in Macao that Qi-stagnation constitution (β = −2.66) and Yin-deficiency constitution (β = −2.10) were negatively associated with neurocognitive function, primarily affecting visuospatial ability and naming performance. Sun et al16 further provided robust epidemiological evidence from a cohort of Chinese centenarians, demonstrating a significant association between Qi-stagnation constitution and age-related cognitive decline. Taken together, this body of cross-regional, cross-age evidence indicates that specific TCM constitution types—including Qi-deficiency, Yin-deficiency, Qi-stagnation, Yang-deficiency, Phlegm-dampness, and Blood-stasis—are consistently associated with cognitive impairment, whereas Balanced constitution shows an inverse association.
From a TCM theoretical perspective, the core pathomechanism of Qi-deficiency constitution is an insufficiency of primordial Qi (yuan qi) with consequent decline in organ function. The brain, as the “sea of marrow,” depends on the nourishment of Qi and blood; when Qi is deficient, clear Yang fails to ascend, the brain marrow is deprived of nourishment, and the spirit mechanism (shen ji) becomes dysfunctional, manifesting as forgetfulness, cognitive slowing, and other features of cognitive decline. Contemporary research has provided biological interpretations of this traditional pathomechanism: multiple studies suggest that Qi-deficiency constitution may be closely related to mitochondrial dysfunction and impaired energy metabolism. For instance, Tan et al17 noted in a review that the TCM active compound tanshinone I can maintain mitochondrial function by upregulating Nrf2 expression, while huperzine A can counteract Aβ-induced mitochondrial dysfunction, thereby exerting neuroprotective effects. These findings suggest that Qi-tonifying herbal medicines may delay cognitive decline by modulating mitochondrial function and improving energy metabolism, providing modern scientific support for Qi-supplementing therapeutic approaches in cognitive disorders such as Alzheimer’s disease. Yin-deficiency constitution is characterized by a depletion of Yin fluids and internal disturbance by deficiency-heat. The kidney stores essence, governs bone, and generates marrow that communicates with the brain; Yin deficiency of the kidney therefore leads to emptiness of the brain marrow. Moreover, Yin deficiency generates internal heat, and deficiency-heat disturbs the clear orifices, both of which contribute to cognitive impairment. Zhang et al’s study in older adults in Macao confirmed that Yin-deficiency constitution was significantly and negatively correlated with neurocognitive function, particularly visuospatial ability,15 corroborating the present findings. Balanced constitution, representing a state of harmonious Yin-Yang and Qi-blood balance, reflects optimal homeostasis and neurological reserve capacity. Both the present study and multiple prior investigations have confirmed its protective effect on cognitive function. In Deng et al’s study, Balanced constitution accounted for 64.5% of the cognitively normal control group but only 33.6% of the MCI group.8 Similarly, Zhang et al observed that older adults with Balanced constitution achieved significantly higher neurocognitive function scores than those with pathological constitutions.15 Collectively, this evidence indicates that maintaining or trending toward a Balanced constitution is inversely associated with cognitive decline. In community-based MCI prevention and control, TCM constitution assessment should be incorporated into routine screening, with targeted interventions directed at individuals with Qi-deficiency and Yin-deficiency constitutions; Qi-tonifying and Yin-nourishing approaches may potentially delay cognitive decline.
Association Between Serum Creatinine and MCI
Another important finding of this study was that elevated serum creatinine (OR = 1.015) was an independent correlate positively associated with MCI. Creatinine is one of the most commonly used clinical indicators of renal function. The recently proposed concept of the “kidney–brain axis” provides a novel framework for understanding this association. Gao et al18 found in patients with Parkinson’s disease and MCI that not only was serum creatinine an independent predictor, but the DTI-ALPS index—reflecting glymphatic clearance function in the brain—was also significantly reduced, suggesting that renal dysfunction may be associated with impaired clearance of metabolic waste products (such as α-synuclein) from the brain. Xiao et al19 similarly demonstrated in a large sample of older adults with diabetes in the United States that elevated serum creatinine (particularly Scr ≥ 300 μmol/L) was significantly associated with lower cognitive test scores. This cross-disease, cross-population evidence collectively suggests that renal impairment may influence cognition through several mechanisms: (1) accumulation of uremic toxins—reduced renal clearance allows toxins to accumulate systemically, cross the blood–brain barrier, and trigger neuroinflammation and oxidative stress in the central nervous system; (2) microvascular injury—both the kidney and the brain are organs with high blood flow and similar microvascular architecture, rendering them susceptible to vascular injury factors; declining renal function may therefore indirectly reflect subclinical cerebrovascular damage; and (3) glymphatic dysfunction—as demonstrated by Gao et al,18 renal dysfunction may be associated with impaired systemic and central nervous system glymphatic clearance, leading to the accumulation of neurotoxic proteins such as Aβ and tau in the brain. These findings underscore the importance of monitoring renal function indicators as early warning signals when assessing cognitive risk in older adults.
Traditional Associated Factors: Age, Sex, and Related Determinants
Increasing age is the strongest non-modifiable factor associated with cognitive decline. The present study found that each additional year of age was associated with a 6.5% increase in MCI risk, consistent with the conclusions of most prior studies20.A global meta-analysis by Bai et al,13 encompassing 66 studies and more than 240,000 community-dwelling older adults, further confirmed that MCI prevalence increases significantly with age, rising from 10.88% among those aged 50–59 years to 21.27% among those aged 80 years and older (p = 0.0185). With advancing age, the brain undergoes physiological atrophy, β-amyloid deposition, and neurotransmitter alterations, collectively leading to a decline in cognitive reserve. Female sex was associated with a significantly higher risk of MCI than male sex (OR = 1.916), which may be attributable to postmenopausal estrogen decline, women’s longer average lifespan, and differences in educational attainment. A large-scale survey by Wang et al21 among rural older adults in China similarly found that the MCI prevalence was higher in women (45.1%) than in men (40.0%), with the disparity becoming more pronounced after age 75 (62.7% vs. 45.4%). That study further revealed that educational attainment was inversely associated with cognitive impairment in women (OR = 0.352), indicating that illiterate women face substantially higher cognitive risk.
Inverse Association Between Physical Exercise and Cognitive Impairment
The present study identified regular physical exercise (OR = 0.418) as an independent correlate inversely associated with MCI, consistent with findings from prior research. Lim et al22 demonstrated in a cohort of 2,746 older adults in Korea that those meeting recommended physical activity levels (≥150 minutes of moderate-to-vigorous exercise per week) had significantly higher rates of normal cognitive function (OR = 1.35), and that physical activity level was positively correlated with cognitive function scores, suggesting a dose–response relationship. That study also found that older adults meeting recommended exercise levels had higher hemoglobin and creatinine levels and more favorable lipid profiles, suggesting that physical exercise may indirectly protect cognitive function by improving hematological and metabolic parameters.
Improvement in metabolic status may represent an important mediating pathway through which exercise protects cognition. Boccardi et al23 found in an Italian MCI population that individuals with dysglycemia performed significantly worse on memory and logical reasoning tasks, indicating a close relationship between impaired glucose metabolism and cognitive decline. Regular exercise has been shown to improve insulin sensitivity and reduce blood glucose levels, potentially delaying cognitive decline by correcting metabolic abnormalities. This mechanistic pathway provides a clear biological target for exercise-based interventions. The specific mechanisms through which exercise protects cognitive function may include: (1) increased expression of brain-derived neurotrophic factor (BDNF), promoting neuronal survival and synaptic plasticity; (2) improved cerebrovascular function and increased cerebral blood flow; (3) attenuation of neuroinflammation and oxidative stress; and (4) improved insulin sensitivity and metabolic homeostasis.22
Innovations and Clinical Significance
Compared with existing prediction models, the innovations and advantages of the present study are as follows. First, this study was conducted within a community health service center, leveraging the national basic public health service health examination platform for older adults. All predictors incorporated in the model—including age, sex, exercise habits, TCM constitution, and serum creatinine—are routinely collected during standard health examinations, ensuring low implementation costs and high accessibility. Second, this study innovatively incorporated TCM constitution into the prediction model, revealing the important role of constitutional factors in cognitive decline and embodying the organic integration of the “preventive treatment of disease” philosophy with modern predictive medicine. A recent systematic review by Zhang et al24 evaluated 72 MCI prediction models for older adults, reporting a pooled AUC of 0.83 but noting that most models suffer from high risk of bias and rely on expensive clinical biomarkers. The model developed by Wang et al20 using logistic regression achieved an AUC of 0.78, which is comparable to the validation set AUC of 0.747 achieved in the present study. However, compared to these existing tools, our present model highlights several unique strengths: it is entirely community-based, relies on low-cost, readily accessible routine health examination data without requiring expensive neuroimaging or cerebrospinal fluid biomarkers, and innovatively integrates TCM constitution information. This offers a broader predictor dimension and greater cultural and practical relevance for Chinese community populations, making it highly suitable for large-scale primary care screening. Third, the use of four machine learning methods for cross-validated variable selection is more robust than any single method, reducing the risk of overfitting and enhancing the generalizability of the model.
As an intuitive visualization tool, the nomogram translates complex regression equations into a straightforward scoring system that is readily interpretable by community physicians and older adults alike. Users can rapidly estimate an individual’s MCI risk based on age, sex, exercise habits, TCM constitution type, and serum creatinine level, enabling early identification and stratified management of high-risk individuals. Based on the modifiable associated factors identified by the model—including exercise habits and TCM constitution—targeted community interventions can be implemented: individuals with Qi-deficiency constitution may benefit from Qi-tonifying dietary therapies (eg., Astragalus [huangqi], Chinese yam [shanyao]) and gentle exercise regimens (eg., Baduanjin, Tai Chi);17 those with Yin-deficiency constitution may be advised to consume Yin-nourishing and moistening foods (eg., lily bulb [baihe], wolfberry [gouqi]) and to avoid staying up late;16 and all older adults should be encouraged to maintain regular physical exercise.22 This “constitution-based assessment plus precision intervention” model has the potential to enhance the effectiveness of community-level cognitive impairment prevention and control.14
Limitations and Future Directions
This study has several limitations. First, as all participants were recruited from a single community health center in Guangzhou through convenience sampling, selection bias may exist. Individuals with severe impairments or limited healthcare access may be underrepresented, potentially underestimating the true MCI prevalence. Since TCM constitution distribution varies across regions of China,14 and single-center prediction models often suffer from limited generalizability,25 extrapolation to other populations should be approached with caution, and multicenter external validation is required. Second, although machine learning methods were used for variable selection, the final model was constructed using logistic regression, which does not fully exploit the advantages of ensemble learning. Future research may explore multi-model fusion prediction systems to enhance performance. Third, due to community health examination data limitations, this study did not incorporate strong predictors such as APOE-ε4 genotype, neuroimaging biomarkers, or blood-based biomarkers (eg., Aβ, phosphorylated tau), potentially omitting important information. Fourth, the AUC in the validation set (0.747) was lower than that in the training set (0.813), suggesting a modest decrease in apparent discrimination in the validation set rather than severe overfitting. Moreover, the 10-fold cross-validation AUCs were highly consistent between the training set (AUC = 0.806, 95% CI: 0.774–0.839) and the validation set (AUC = 0.804, 95% CI: 0.773–0.836), supporting the stability of model discrimination. Nevertheless, further multicenter external validation remains warranted. Fifth, while our two-step diagnostic approach (AD8 combined with CMMS) operationalized the Petersen criteria, the self-administered AD8 may be subject to recall bias, and the CMMS has limited sensitivity for mild deficits compared with MoCA. Future studies should incorporate more comprehensive neuropsychological batteries. Sixth, the cross-sectional design, with data collected within a one-year timeframe, precludes the assessment of temporal relationships or causal pathways between predictors and MCI. To mitigate concerns regarding information leakage, the CCMQ primarily assesses stable somatic symptoms that are conceptually independent of the cognitive domains evaluated by the AD8 and CMMS,26 and longitudinal evidence supports the temporal precedence of TCM constitutional traits prior to clinical disease onset.27 Furthermore, this design does not permit evaluation of progression from MCI to dementia. A recent meta-analysis reported that the annual conversion rate from MCI to dementia is approximately 5.9% in community cohorts.28 Prospective longitudinal cohort studies are therefore essential to confirm the predictive validity of our model for dementia conversion.
Importantly, as this is a cross-sectional analysis, the developed nomogram is intended solely for risk screening and early identification in primary care, not for establishing definitive causality. Future research should prioritize multicenter, large-sample prospective cohort studies to externally validate the model and confirm causal relationships. As we transition these models toward clinical application, deployment should be guided by established frameworks for human-AI collaboration such as TRIAD,29 which emphasizes trustworthy governance, real-world clinical value, and integrated adaptive deployment. We also plan to explore multimodal data fusion incorporating wearable device data, speech analysis, and blood-based biomarkers, and to develop automated MCI risk assessment tools for dynamic cognitive monitoring in community-dwelling older adults.
Conclusions
This study, based on a large community sample of older adults, applied multiple machine learning methods for joint feature selection and developed and validated a nomogram prediction model for MCI risk that integrates TCM constitution. The principal conclusions are as follows. TCM constitution type is an important predictor of MCI: Qi-deficiency constitution (OR = 10.609) and Yin-deficiency constitution (OR = 5.017) are independent correlates positively associated with MCI, while Balanced constitution (OR = 0.174) is an independent correlate inversely associated with MCI; the effect sizes are substantial and robust, suggesting that TCM constitution assessment holds unique clinical value in community-level MCI risk stratification. Increasing age, female sex, and elevated serum creatinine are independent correlates positively associated with MCI, while regular physical exercise is an independent correlate inversely associated with MCI, consistent with the conclusions of prior research and further validating the applicability of these traditional associated factors in community-dwelling older adult populations. The nomogram model incorporating age, sex, regular exercise, Balanced constitution, Qi-deficiency constitution, Yin-deficiency constitution, and serum creatinine demonstrated good discrimination (training set AUC = 0.813; validation set AUC = 0.747), stable 10-fold cross-validation performance (training set AUC = 0.806; validation set AUC = 0.804), satisfactory calibration, and favorable clinical utility, providing a practical and scientifically grounded tool for early MCI screening and risk stratification in community settings. This study provides epidemiological evidence supporting the application of TCM constitutional theory in the early identification of cognitive impairment and offers a new perspective for the development of primary prevention strategies against dementia in the community.
Data Sharing Statement
All data generated during this study have been analyzed, and the results are included in this manuscript. The data supporting the findings of this study are available upon reasonable request from the corresponding author.
Ethics Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Shiqi Town Community Public Health Service Center, Panyu District, Guangzhou, Guangdong, China (Approval No.: [2025] Ethics Approval No. 001). All participants provided written informed consent prior to enrollment.
Acknowledgments
The authors would like to thank all participants who took part in this study and the staff of the Shiqi Town Community Public Health Service Center, Panyu District, Guangzhou, for their support in data collection. We also thank the anonymous reviewer for their careful reviewand helpful edits and comments on the manuscript.
Author Contributions
Qixin Xu and Zhijie Huang share first authorship. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Medical Science and Technology Research Foundation of Guangdong Province (B2026368); Guangzhou Health Technology General Funding Program (20261A011112); Guangzhou Health Technology Projects in New Technologies and New Programs (20261A040016); Panyu District Science and Technology Plan Medical and Health Project (2025-Z04-94).
Disclosure
All authors declare no conflicts of interest in this work.
References
1. Livingston G, Huntley J, Liu KY. et al. Dementia prevention, intervention, and care: 2024 report of the Lancet standing Commission. Lancet. 2024;404:572–19. doi:10.1016/S0140-6736(24)01296-0
2. Zhi N, Ren R, Qi J, et al. The China Alzheimer Report 2025. Gen Psychiatry. 2025;38:e102020. doi:10.1136/gpsych-2024-102020
3. Nantachai G, Vasupanrajit A, Tunvirachaisakul C, Solmi M, Maes M. Oxidative stress and antioxidant defenses in mild cognitive impairment: a systematic review and meta-analysis. Ageing Res Rev. 2022;79:101639. doi:10.1016/j.arr.2022.101639
4. Hessen E. Mild cognitive impairment and neuropsychological examination. Front Psychol. 2025;16:1662151. doi:10.3389/fpsyg.2025.1662151
5. Katzman R, Zhang MY, Ouang-Ya-Qu, et al. A Chinese version of the Mini-Mental State Examination; impact of illiteracy in a Shanghai dementia survey. J Clin Epidemiol. 1988;41(10):971–978. doi:10.1016/0895-4356(88)90034-0
6. Luo Y, Cheng X, Jiang L, et al. Exploration of influential factors about Qi-deficiency constitution of Traditional Chinese Medicine based on multi-methods. J Tradit Chin Med. 2025;45(3):693–701. doi:10.19852/j.cnki.jtcm.2025.03.020
7. Huang C, Chen Y, Li B, et al. Traditional Chinese Medicine Constitution Discrimination Model Based on Metabolomics and Random Forest Decision Tree Algorithm. Evid Based Complement Alternat Med. 2022;2022:3490130. doi:10.1155/2022/3490130
8. Deng X, Teng J, Nong X, et al. Characteristics of TCM Constitution and Related Biomarkers for Mild Cognitive Impairment. Neuropsychiatr Dis Treat. 2021;17:1115–1124. doi:10.2147/NDT.S290692
9. Huang Y, Guo S, Yang J, Tang Y, Zhu X, Ren S. An Objective Diagnosis Model with Integrated Metabolic and Immunity Parameters for Phlegm-Dampness Constitution. Evid Based Complement Alternat Med. 2022;2022:3353549. doi:10.1155/2022/3353549
10. Song Y, Yuan Q, Liu H, Gu K, Liu Y. Machine learning algorithms to predict mild cognitive impairment in older adults in China: a cross-sectional study. J Affect Disord. 2025;368:117–126. doi:10.1016/j.jad.2024.09.059
11. Cyy H, Zhou Z, Kan MMP, et al. Modifiable risk factors for mild cognitive impairment among cognitively normal community-dwelling older adults: a systematic review and meta-analysis. Ageing Res Rev. 2024;99:102350. doi:10.1016/j.arr.2024.102350
12. Wang ZY, Zhang MY. Application of the Chinese version of the Mini-Mental State Examination (MMSE). Shanghai Arch Psychiatry. 1989;7(3):108–111.
13. Bai W, Chen P, Cai H, et al. Worldwide prevalence of mild cognitive impairment among community dwellers aged 50 years and older: a meta-analysis and systematic review of epidemiology studies. Age Ageing. 2022;51(8):afac173. doi:10.1093/ageing/afac173
14. Qiao M, Yang S, Ma Y, et al. Traditional Chinese Medicine Constitution and Cognitive Frailty in Older Adults: prediction Models and Sleep-Quality Mediation Pathway from a Multicenter Study in China. Clin Interv Aging. 2025;20:2607–2625. doi:10.2147/CIA.S548401
15. Zhang Z, Chuang Y, Ke X, et al. The influence of TCM constitutions and neurocognitive function in elderly Macau individuals. Chin Med. 2021;16(1):32. doi:10.1186/s13020-021-00441-2
16. Sun Z, Ping P, Li Y, et al. Relationships Between Traditional Chinese Medicine Constitution and Age-Related Cognitive Decline in Chinese Centenarians. Front Aging Neurosci. 2022;14:870442. doi:10.3389/fnagi.2022.870442
17. Tan W, Qi L, Hu X, Tan Z. Research progress in traditional Chinese medicine in the treatment of Alzheimer’s disease and related dementias. Front Pharmacol. 2022;13:921794. doi:10.3389/fphar.2022.921794
18. Gao Y, Li Y, Ji N, et al. Predictive value of the combined DTI-Alps index and serum creatinine levels in mild cognitive impairment in Parkinson’s disease. Front Neurol. 2025;16:1628697. doi:10.3389/fneur.2025.1628697
19. Xiao Y, Devakumar V, Xu L, Liu L, Mo H, Hong X. Elevated serum creatinine levels and risk of cognitive impairment in older adults with diabetes: a NHANES study from 2011–2014. Front Endocrinol. 2023;14:1149084. doi:10.3389/fendo.2023.1149084
20. Wang B, Shen T, Mao L, Xie L, Fang QL, Wang XP. Establishment of a Risk Prediction Model for Mild Cognitive Impairment among Elderly Chinese. J Nutr Health Aging. 2020;24(3):255–261. doi:10.1007/s12603-020-1335-2
21. Wang J, Xiao LD, Wang K, Luo Y, Li X. Gender Differences in Cognitive Impairment among Rural Elderly in China. Int J Environ Res Public Health. 2020;17(10):3724. doi:10.3390/ijerph17103724
22. Lim ST, Jung YZ, Akama T, Lee E. Physical Activity Amount and Cognitive Impairment in Korean Elderly Population. Brain Sci. 2020;10(11):804. doi:10.3390/brainsci10110804
23. Boccardi V, Travaglini EG, Sciacca E, et al. Dysglycemia, gender, and cognitive performance in older persons living with mild cognitive impairment: findings from a cross-sectional, population-based study. Aging Clin Exp Res. 2024;36(1):145. doi:10.1007/s40520-024-02806-7
24. Zhang L, Tian J, Liu X, Wang L, Yang L. Prediction models for mild cognitive impairment in older adults: a systematic review and meta-analysis. Geriatr Nurs. 2025;65:103530. doi:10.1016/j.gerinurse.2025.103530
25. Vermeulen RJ, Andersson V, Banken J, et al. Limited generalizability and high risk of bias in multivariable models predicting conversion risk from mild cognitive impairment to dementia: a systematic review. Alzheimers Dement. 2025;21(4):e70069. doi:10.1002/alz.70069
26. Lai NS, Lu MC, Chang HH, et al. Association of Traditional Chinese Medicine Body Constitution and Health-Related Quality of Life in Female Patients with Systemic Lupus Erythematosus: a Cross-Sectional Study. Evid Based Complement Alternat Med. 2021;2021:5568219. doi:10.1155/2021/5568219
27. Lee CH, Tsai CI, Su YC, Lin SY, Lee IT, Li TC. Traditional Chinese medicine body constitution predicts new-onset diabetic albuminuria in patients with type 2 diabetes: taichung diabetic body constitution prospective cohort study. Medicine. 2022;101(50):e32342. doi:10.1097/MD.0000000000032342
28. Salemme S, Lombardo FL, Lacorte E, et al. The prognosis of mild cognitive impairment: a systematic review and meta-analysis. Alzheimers Dement. 2025;17(1):e70074. doi:10.1002/dad2.70074
29. LiJ, ZhouZC, WangZC, LvH. Prioritizing human-AI collaboration in healthcare: the TRIAD framework for trustworthy governance, real-world, and integrated adaptive deployment. Mil Med Res. 2026;12:97. doi:10.1186/s40779-026-00684-w
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Predicting the Risk of Unplanned Readmission at 30 Days After PCI: Development and Validation of a New Predictive Nomogram
Xu W, Tu H, Xiong X, Peng Y, Cheng T
Clinical Interventions in Aging 2022, 17:1013-1023
Published Date: 5 July 2022
Development and Validation of a Nomogram for Predicting 28-Day Mortality on Admission in Elderly Patients with Severe Community-Acquired Pneumonia
Song Y, Wang X, Lang K, Wei T, Luo J, Song Y, Yang D
Journal of Inflammation Research 2022, 15:4149-4158
Published Date: 21 July 2022
Using Machine Learning Algorithms to Predict High-Risk Factors for Postoperative Delirium in Elderly Patients
Liu Y, Shen W, Tian Z
Clinical Interventions in Aging 2023, 18:157-168
Published Date: 8 February 2023
Prediction of the Risk of Bone Mineral Density Decrease in Type 2 Diabetes Mellitus Patients Based on Traditional Multivariate Logistic Regression and Machine Learning: A Preliminary Study
Zhang J, Xu Z, Fu Y, Chen L
Diabetes, Metabolic Syndrome and Obesity 2023, 16:2885-2898
Published Date: 19 September 2023
Development and Validation of a Machine Learning–Based Clinical Model for Predicting Rupture in Ectopic Pregnancy: A Web-Based Nomogram Approach
Zhao X, Wu T, Zeng S, Yuan X, Liang X, Yang H, Ye L
Journal of Multidisciplinary Healthcare 2025, 18:5781-5799
Published Date: 13 September 2025