Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
A Clinical-Imaging Nomogram for Predicting Early Recurrence in Patients with Solitary Hepatocellular Carcinoma After Postoperative Adjuvant TACE
Authors Liu J, Ding X, Zhang Y ![]() , Li H
, Li H
Received 1 June 2025
Accepted for publication 8 August 2025
Published 19 August 2025 Volume 2025:12 Pages 1835—1847
DOI https://doi.org/10.2147/JHC.S544127
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Mohamed Shaker
Jiachen Liu,1 Xiurong Ding,2 Yanyan Zhang,1 Hongjun Li1
1Radiology Department, Beijing Youan Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Clinical Laboratory, Beijing Youan Hospital, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Hongjun Li, Email [email protected]
Objective: This study aimed to identify independent predictors of early recurrence (ER) and to establish a clinically applicable, individualized nomogram for patients with solitary hepatocellular carcinoma (HCC) who underwent postoperative adjuvant transarterial chemoembolization (PA-TACE).
Methods: A total of 165 patients with solitary HCC treated with PA-TACE between January 2018 and December 2022 were retrospectively analyzed. Among these patients, 71 experienced ER, while 94 remained recurrence-free for over 24 months. Independent prognostic variables were identified through univariate and multivariate Cox regression analyses. These factors were integrated into a nomogram model, and its performance was evaluated using internal validation and calibration curves.
Results: Multivariate analysis revealed that AFP-L3% > 10% (p = 0.009), presence of satellite lesions (p = 0.026), GLR > 20 (p = 0.020), microvascular invasion (MVI) (p = 0.008), and Ki-67 expression > 50% (p < 0.001) were independently associated with ER. These five variables were used to establish the nomogram, which had a C-index of 0.763 (95% CI: 0.736− 0.870).
Conclusion: A nomogram incorporating AFP-L3, satellite lesions, GLR, MVI, and Ki-67 for predicting ER in patients with solitary HCC following PA-TACE was developed and validated. This model exhibits high predictive accuracy and provides a valuable tool for identifying patients who may benefit from PA-TACE.
Keywords: hepatocellular carcinoma, postoperative adjuvant transarterial chemoembolization, early recurrence, nomogram
Introduction
Liver cancer remains the third leading cause of cancer-related deaths worldwide, with hepatocellular carcinoma (HCC) accounting for approximately 75–85% of all primary liver malignancies.1 Surgical resection continues to be the primary curative treatment modality for patients with favorable physical status. Nonetheless, the consistently high rates of tumor recurrence and metastasis, which can reach up to 75–100% within five years following surgery, represent a substantial challenge to improving long-term survival outcomes.2 Transarterial chemoembolization (TACE) is a locoregional treatment that involves delivering chemotherapeutic agents and embolic materials into the hepatic artery, thereby blocking the tumor’s blood supply and increasing drug concentration within the tumor. Although TACE has been firmly established as the standard treatment for intermediate-stage HCC, there is growing interest in its application as a postoperative adjuvant therapy (PA-TACE) in patients undergoing curative liver resection.3 Several clinical studies4–6 have indicated that the early administration of PA-TACE—typically within 1 to 3 months postoperatively, can significantly reduce recurrence rates and improve disease-free survival (DFS), with some reports demonstrating a 2-year DFS of up to 82%. Conversely, conflicting evidence also exists, revealing limited survival benefits in certain patient populations and even a potential risk of early recurrence (ER) in specific subgroups.7,8 Notably, PA-TACE has demonstrated limited efficacy in patients with tumors smaller than 5 cm, solitary tumors, or no microvascular invasion (MVI), indicating that not all patients are suitable candidates for this intervention.9,10
Magnetic resonance imaging (MRI), a crucial clinical tool, plays a central role in the preoperative assessment of HCC. Its imaging characteristics are intricately linked to the biological properties of the tumor and are therefore extensively utilized for evaluating and predicting the recurrence risk of HCC.11,12 However, the existing research on the role of MRI imaging features in predicting ER following PA-TACE remains relatively limited. Therefore, the present study aimed to identify preoperative MRI features associated with ER (≤24 months) in patients with solitary HCC after PA-TACE and to establish a clinically applicable prediction model by integrating these features with clinical and pathological factors.
Materials and Methods
Study Population
This retrospective study adhered to the ethical principles of the Declaration of Helsinki and was approved by the Ethics Committee of Beijing You’an Hospital. Given the anonymized and non-interventional nature of the research, the need for written informed consent was waived.
Between January 2018 and December 2022, a total of 165 patients diagnosed with HCC who underwent R0 surgical resection followed by PA-TACE at Beijing You’an Hospital (Beijing Liver Disease Research Center) were retrospectively reviewed.
Inclusion criteria comprised: (1) preoperative MRI completed within 30 days prior to surgery and meeting diagnostic standards for HCC; (2) histologically confirmed solitary HCC without intrahepatic metastases or multicentric involvement; (3) complete (R0) tumor resection, defined as the absence of macroscopic residual disease and negative surgical margins; (4) availability of full pathological data post-resection; and (5) receipt of a single PA-TACE treatment approximately four weeks post-surgery.
Exclusion criteria included: (1) prior anti-tumor therapies before surgery or TACE; (2) multifocal tumors or a single lesion exceeding 10 cm in diameter; (3) coexistence of other malignancies or distant metastasis; (4) incomplete clinical, radiological, or pathological data; and (5) early follow-up termination due to comorbid conditions or insufficient data. After applying these criteria, 165 eligible solitary HCC cases were selected. Based on 24-month disease-free survival (DFS), patients were categorized into an early recurrence (ER, ≤24 months) group and a Non-early recurrence (Non-ER, disease-free >24 months) group. The enrollment and selection process is illustrated in Figure 1.
 |
Figure 1 Flowchart of patient selection and exclusion criteria. |
MRI Acquisition
MRI examinations were performed using a Siemens 3.0 T Magnetom Trio Tim scanner equipped with an 8-channel phased-array body coil. Patients were positioned in the supine position, and the liver was scanned from the diaphragm to its inferior margin. Dynamic contrast-enhanced imaging was acquired in four phases using a 3D breath-hold volume sequence (TR = 3.5 ms, TE = 1.28 ms, slice thickness = 3.0 mm, interslice gap = 0.6 mm). The contrast agent gadobenate dimeglumine (provided by Shanghai Boleke XinYi Pharmaceutical Co., Ltd.) was administered intravenously at a dose of 0.1 mmol/kg and an injection rate of 2.0 mL/s. Sequential imaging was initiated at 20, 30, 65, and 240 seconds post-injection to capture the early arterial, late arterial, portal venous, and delayed phases, respectively.
Image Analysis
MRI scans were independently reviewed by two board-certified abdominal radiologists with extensive experience in liver imaging. The reviewers were blinded to patient-specific lesion characteristics but were aware of the overall HCC risk. Discrepancies were resolved through consensus. Tumors were evaluated according to LI-RADS version 2018, including major features (eg, tumor diameter, non-rim arterial phase hyperenhancement [APHE], washout appearance, and enhancing capsule), ancillary features (eg, restricted diffusion, corona enhancement, hepatobiliary phase [HBP] hypointensity, mild-to-moderate T2 hyperintensity, mosaic architecture, hemorrhage, and fat content), and additional non-LI-RADS findings such as satellite lesions, necrosis, and irregular tumor margins. Each lesion was assigned a LI-RADS category (LR-4, LR-5, or LR-M). Specific feature definitions are shown in Supplementary Table 1. The differentiation of satellite lesions from metastatic or multicentric lesions is detailed in Supplementary Table 2. Representative MRI images demonstrating satellite lesions and their imaging characteristics are illustrated in Figure 2.
 |
Figure 2 (A) Schematic illustration of the treatment sequence from initial HCC diagnosis through surgical resection, adjuvant transarterial chemoembolization (PA-TACE), to potential tumor recurrence. (B) Representative gadoxetate-disodium enhanced MRI images from a 55-year-old male patient with hepatocellular carcinoma (HCC). (1) Arterial-phase image on preoperative imaging, showing a large hypervascular lesion in segment VI (asterisk), representing the primary tumor. (2) A satellite nodule (yellow arrow) adjacent to the main lesion is visualized, with an enlarged view shown in the inset. (3) On follow-up imaging, a new enhancing lesion (red arrow) appeared in segment III, consistent with intrahepatic recurrence. The inset highlights the recurrent focus. (4) Another arterial-phase slice showing no residual lesion in the surgical region. |
Clinical Laboratory and Clinico-Pathological Variables
Baseline demographic and clinical data included gender, age, hepatitis infection status, cirrhosis, and Child-Pugh score. Preoperative laboratory values, obtained within one week before surgery, comprised liver function tests [alanine aminotransferase (ALT), aspartate transaminase (AST), gamma-glutamyl transferase (GGT), alkaline phosphatase (ALP)], platelet count, alpha-fetoprotein (AFP), lens culinaris agglutinin-reactive fraction ofalpha-fetoprotein (AFP-L3)%, and inflammation-based markers such as neutrophil-to-lymphocyte ratio (NLR), gamma-glutamyl transferase-to-lymphocyte ratio (GLR), aspartate aminotransferase-to-lymphocyte ratio (ALRI), and systemic immune-inflammation index (SII). These were calculated as follows: NLR = neutrophil count / lymphocyte count; GLR = GGT / lymphocyte count; ALRI = AST / lymphocyte count; SII = platelet count × neutrophil count / lymphocyte count. Receiver operating characteristic (ROC) analysis determined optimal cut-off values for dichotomization of inflammatory markers. Histopathological indicators included MVI, Edmondson-Steiner grading, and Ki-67 expression. Ki-67 positivity >50% was categorized as high expression.13
Postoperative PA-TACE Procedure
TACE was performed approximately one month after hepatectomy using the Seldinger technique. A catheter was inserted via the femoral artery to selectively access tumor-feeding hepatic arteries. Chemotherapeutic agents (hydroxycamptothecin, oxaliplatin, pirarubicin, and 5-fluorouracil) were emulsified with a non-ionic contrast medium at a 1:1 ratio. Subsequently, embolization was carried out using gelatin sponge particles or polyvinyl alcohol (PVA) microspheres. Treatment regimens were tailored based on physician discretion and therapeutic objectives.
Follow-Up and End-Points
Patients were followed up every 1–2 months in the first postoperative year, then at 3-month intervals, either by phone or in outpatient clinics. Follow-up consisted of AFP testing and imaging (CT or MRI) performed every 3–6 months. Tumor recurrence was confirmed based on imaging findings, elevated AFP levels, or both. ER was defined as tumor reappearance within 24 months after PA-TACE. The final follow-up date was December 31, 2024, ensuring a minimum follow-up duration of 24 months for all patients. Recurrence-free survival (RFS) was defined as the interval from the date of PA-TACE to the documentation of tumor recurrence.
Statistical Analysis
Statistical analysis was performed using SPSS (version 24.0; IBM Corp., Armonk, NY, USA) and R software (version 4.1.1), utilizing packages such as “MatchIt”, “survival”, and “rms”. Continuous variables were compared using Student’s t-test or Mann–Whitney U-test based on distribution. Categorical variables were assessed with chi-square or Fisher’s exact test as appropriate. ROC curve analysis identified optimal cut-off points for inflammatory markers and Ki67. Variables with p < 0.05 in univariate Cox regression were included in multivariate analysis to identify independent predictors of early recurrence. A nomogram was constructed from significant predictors using the “rms” package. Model performance was evaluated using the C-index, ROC curves, calibration plots, and decision curve analysis (DCA). RFS differences were assessed using Kaplan–Meier analysis with Log rank testing. All p-values were two-tailed, with statistical significance defined as p < 0.05.
Results
Baseline Clinical and Pathological Characteristics
Table 1 summarizes the demographic and clinicopathological characteristics of the 165 patients included in the study. Among these patients, 130 were male (78.8%), and the mean age was 56.0 ± 9.4 years (range: 30–74 years). Hepatitis B virus (HBV) infection was the predominant etiology, identified in 90.3% of the patients, while cirrhosis was present in 58.8%. A total of 71 patients (43.0%) experienced ER within 24 months postoperatively, with a mean time to recurrence of 13.0 ± 7.3 months. The remaining 94 patients were classified into the Non-ER group, exhibiting a median follow-up of 29.0 months (IQR: 26.0–38.0; range: 25–73 months). Comparative analysis revealed that the ER group had significantly higher proportions of patients with AFP-L3% >10% (53.5% vs 21.3%, p < 0.001), GLR >20 (69.0% vs 46.8%, p = 0.004), and ALRI >12 (87.3% vs 71.3%, p = 0.013). In terms of pathological features, MVI and Ki-67 overexpression (>50%) were markedly more prevalent in the ER group compared to the non-ER group (all p <0.05).
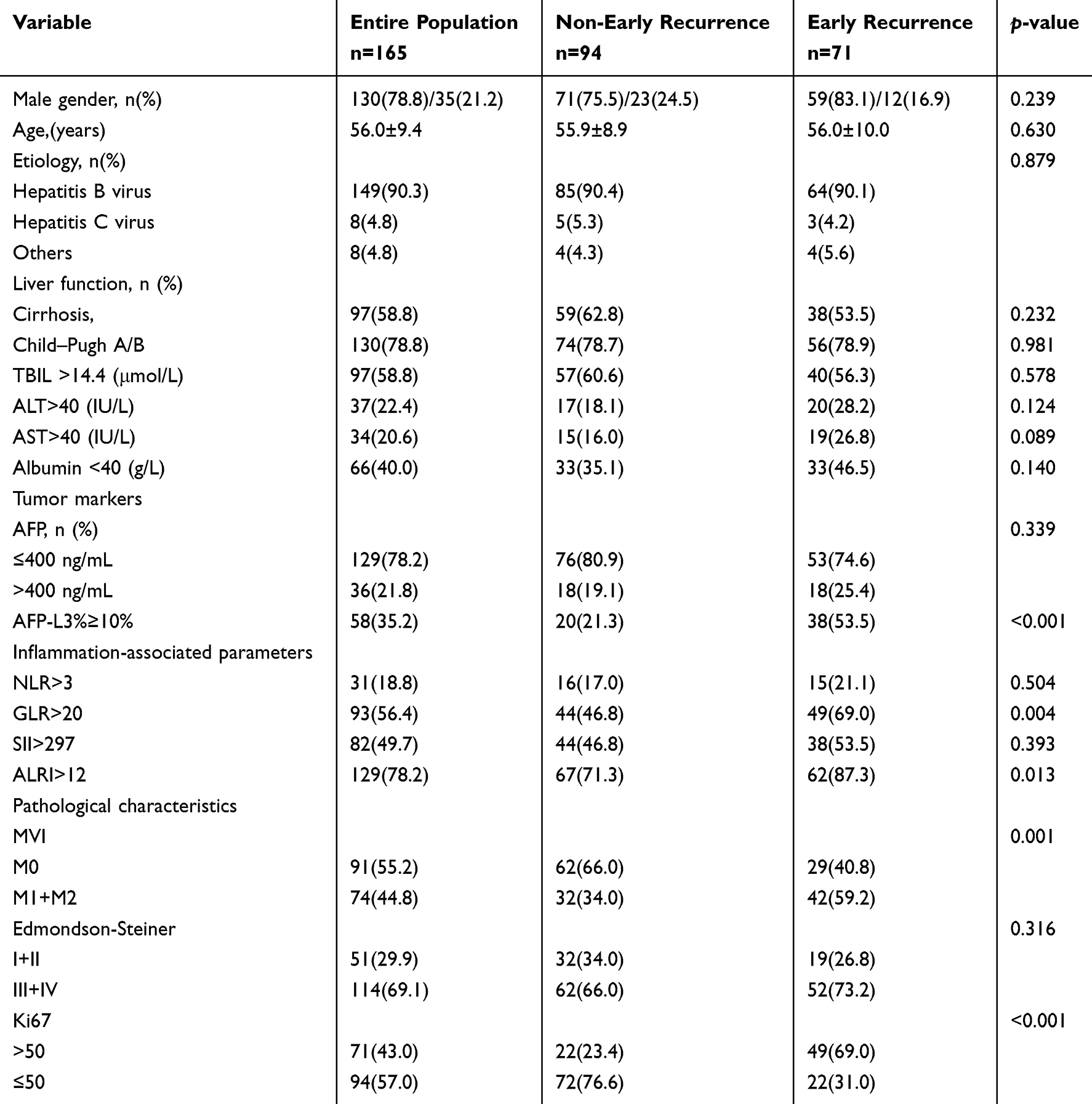 |
Table 1 Baseline Characteristics of HCC Patients Undergoing PA-TACE |
MR Imaging Features
Table 2 provides a comparison of imaging characteristics between the two groups. Among LI-RADS-defined features, tumor size showed statistically significant differences between groups (tumors>3cm, 64.8% in ER group vs 40.4% in Non-ER group, p = 0.002). With respect to non-LI-RADS features, satellite lesions and irregular margins were significantly more prevalent in the ER group (29.5% vs 8.5%, p < 0.001; 35.2% vs 19.1%, p = 0.020). Other imaging traits, including APHE, washout, corona enhancement, and HBP hypointensity, showed no statistically significant differences between the two groups.
 |
Table 2 Imaging Characteristics of HCC Patients Receiving PA-TACE Treatment |
Prognostic Factors for ER
The results of Cox regression analyses are detailed in Table 3. Univariate analysis identified nine variables significantly associated with ER: AFP-L3>10% (p < 0.001), GRL > 20 (p = 0.005), ALRI>12 (p = 0.011), tumor size (p = 0.004), satellite lesions (p =0.001), irregular margins (p = 0.003), MVI (p = 0.002), and Ki-67 expression > 50% (p <0.001). Subsequently, multivariate Cox regression revealed five independent predictors of ER: AFP-L3% >10% (HR: 1.922; 95% CI: 1.177–3.138; p = 0.009), GLR >20 (HR: 1.840; 95% CI: 1.103–3.069; p = 0.020), Satellite lesions (HR: 1.828; 95% CI: 1.077–3.103; p = 0.026), MVI (HR: 1.951; 95% CI: 1.189–3.201; p = 0.008) and Ki-67 >50% (HR: 2.842; 95% CI: 1.755–4.603; p < 0.001).
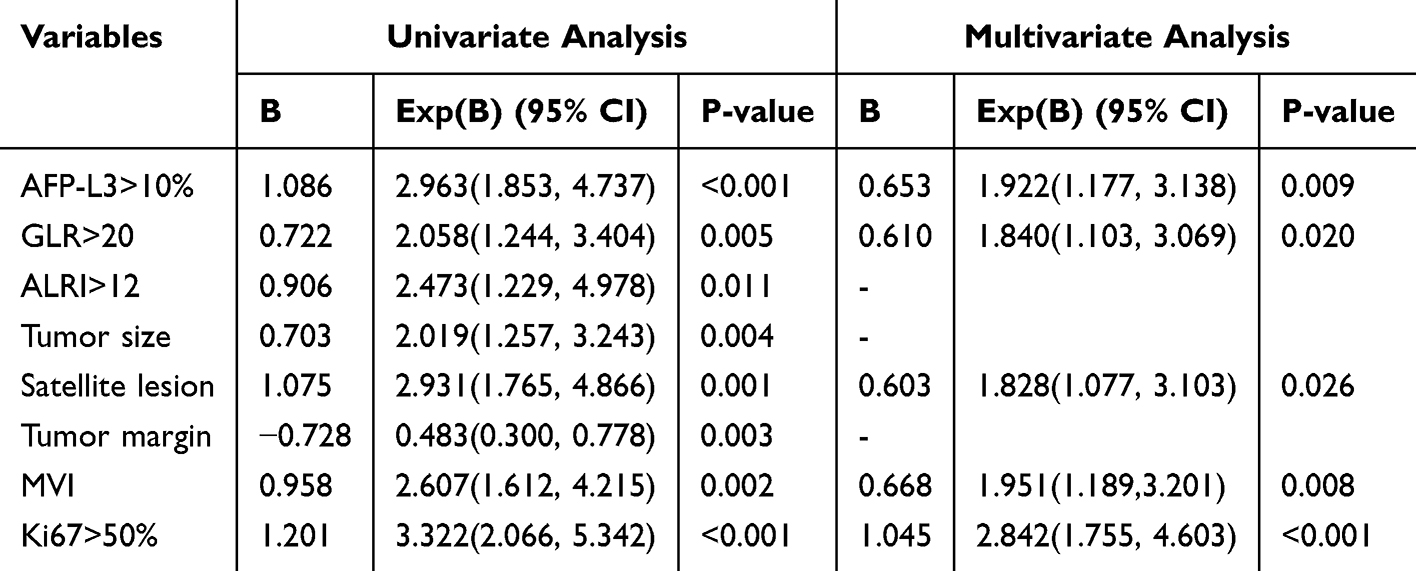 |
Table 3 Cox Regression Analyses Identify Independent Prognostic Factors for ER |
Predictive Performance of Risk Indicators and Integrated Model
Table 4 shows the predictive accuracy of individual risk factors and the combined model in forecasting ER. Among the single predictors, satellite lesions demonstrated the highest specificity (94.7%) but the lowest sensitivity (26.8%). In contrast, Ki-67 expression >50% exhibited a more balanced performance, achieving 69.0% sensitivity and 76.6% specificity. When the five independent risk factors were integrated into a single model, the resulting prediction model achieved a sensitivity of 70.4%, specificity of 80.9%, and overall accuracy of 76.4%, outperforming any single indicator.
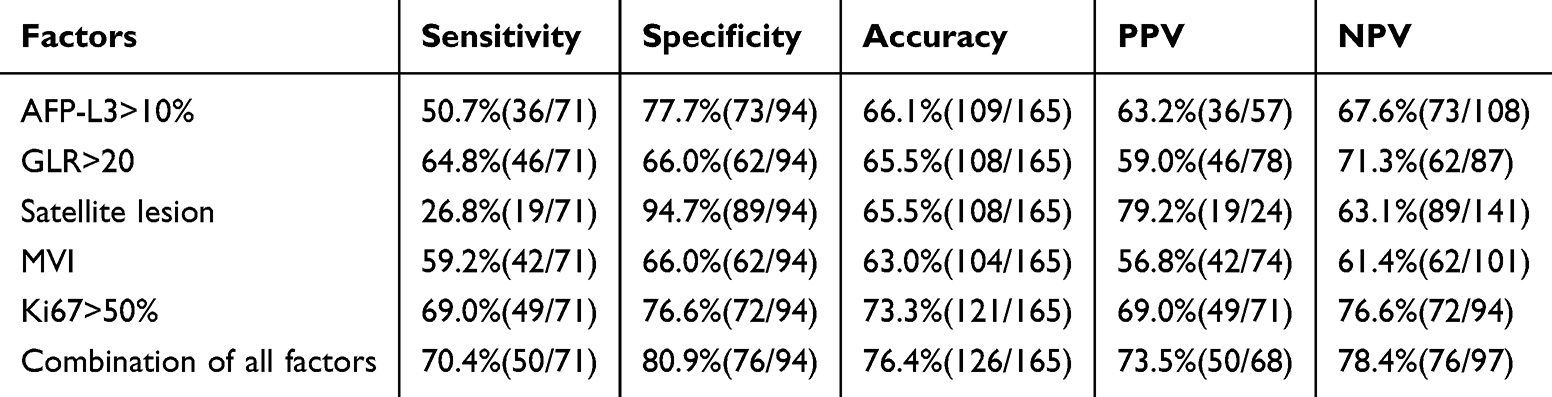 |
Table 4 Performance of Individual Predictors and Combined Model for the ER of HCC Treatment with PA-TACE |
Nomogram Construction and Validation
A nomogram was constructed based on the five independent predictors of ER. As illustrated in Figure 3, this model provides individualized estimates of recurrence risk for each patient. The discriminative performance of the nomogram, as assessed by the C-index (0.763; 95% CI: 0.736–0.870) and AUC (0.803), demonstrated strong predictive capacity (Figure 4A). The calibration curve revealed close agreement between the predicted and actual recurrence probabilities (Figure 4B), thereby confirming the reliability of the model. Decision curve analysis (DCA) further validated its clinical utility (Figure 4C). Kaplan–Meier survival analysis indicated significantly poorer recurrence-free survival in the high-risk group compared with the low-risk group (p < 0.0001), as shown in Figure 4D.
 |
Figure 3 Nomogram for predicting ER after PA-TACE in HCC patients. |
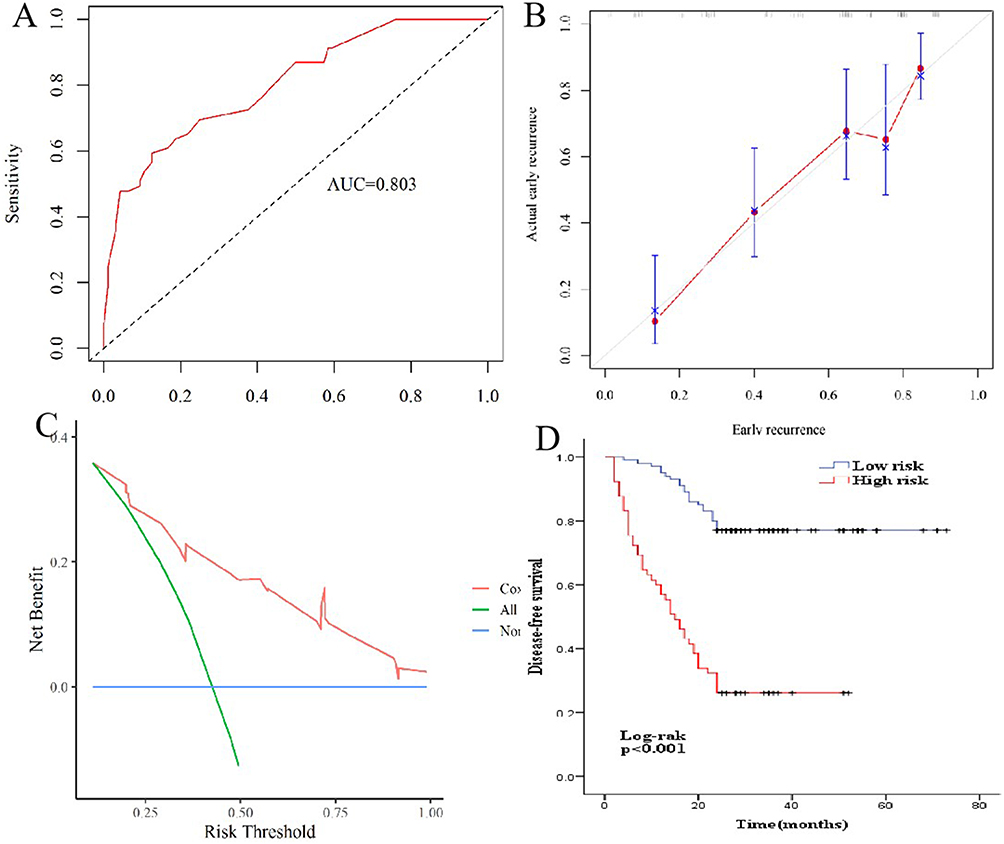 |
Figure 4 (A) The area under ROC curve (AUC) for the nomogram predicting ER; (B) Calibration curves of the nomogram showing agreement between actual and predicted probabilities; (C) Decision curve analysis for evaluating the clinical utility of the nomogram in ER prediction; (D) Kaplan-Meier curves illustrate the RFS. |
Discussion
In China, TACE has become the most commonly used postoperative adjuvant therapy following liver resection for HCC, largely due to its relatively brief treatment duration and favorable safety profile.4,14 Nonetheless, the heterogeneity in patient populations and tumor biology has resulted in inconsistent findings across clinical studies regarding its efficacy. Several studies7,8 have demonstrated that PA-TACE does not consistently improve long-term survival or delay recurrence across all HCC patients. In this study, a significant proportion of solitary HCC patients (43.0%) experienced ER (within 24 months) following PA-TACE, highlighting the critical need for improved patient stratification before treatment. This further emphasizes the critical clinical need for a reliable preoperative tool to predict ER. To address this, we developed a multiparametric nomogram that integrates accessible clinical, pathological, and imaging variables. The final model incorporated five independent predictors: MVI, satellite lesions, Ki-67 expression >50%, AFP-L3% >10%, and GLR >20. The nomogram demonstrated excellent discriminative performance and calibration ability.
Among these, MVI is widely recognized as a critical indicator reflecting the high invasiveness and metastatic potential of tumors and serves as an essential pathological basis for assessing the recurrence risk of HCC and guiding treatment strategies.15–17 Previous studies18–21 have shown that PA-TACE reduces recurrence and improves survival outcomes in patients with MVI, whereas no significant effect has been observed in patients without MVI. For instance, Wang et al22 proposed a scoring system for HCC patients based on AFP, cirrhosis status, tumor count, tumor diameter, number of MVI foci, and the distance between MVI and HCC. This system categorized MVI-positive patients into three subtypes (type A, type B, and type C). The findings indicated that only type C patients derive significant benefit from adjuvant TACE, while the therapeutic benefits for type A and type B patients remain to be further elucidated. In this study, MVI emerged as an independent risk factor for ER, reaffirming the importance of its consideration in therapeutic planning. Therefore, for patients with positive MVI, the decision for adjuvant TACE treatment should be individually tailored and based on each patient’s clinical characteristics and prognostic factors.
Accumulating evidence indicates that ER (≤2 years) following hepatectomy is primarily attributed to residual micrometastatic foci.23 Satellite lesions, defined as daughter nodules located within 2 cm of the dominant tumor mass, are considered to arise from micrometastatic spread and indicate aggressive tumor behavior. Research24 has established that satellite lesions are frequently associated with significant tumor-related vascular alterations and frequent vascular invasion, thereby facilitating the formation of circulating tumor cells and ultimately contributing to distant metastases. Several studies25–27 have confirmed the close association between satellite lesions and the recurrence of liver cancer. Notably, in liver transplant settings, satellite lesions have been identified as the sole independent predictor of early post-transplant recurrence.28 Currently, models based on imaging features have gradually gained attention for predicting the prognosis of patients undergoing PA-TACE.29,30 In this study, univariable analyses revealed that ER was significantly associated with several imaging features, such as tumor size, satellite lesions, and irregular margins. Notably, satellite lesions were the sole imaging feature independently associated with ER following PA-TACE. In the context of PA-TACE, despite their low sensitivity, the high specificity of satellite lesions indicates they may serve as a reliable marker for identifying patients who are less likely to benefit from adjuvant therapy.
The Ki-67 protein, which is expressed during the active phases of the cell cycle, serves as a well-established marker for cellular proliferation. Elevated Ki-67 levels have been consistently associated with more aggressive tumor phenotypes and poorer prognoses across various malignancies.31,32 A meta-analysis33 of 54 cohorts (N=4996) demonstrated that high Ki-67 expression was significantly associated with several key factors in HCC patients, including histologic grade progression, tumor enlargement, multinodular disease, metastasis, cirrhosis, and vascular invasion. Moreover, elevated Ki-67 expression correlates with worse survival outcomes, including reduced disease-free, recurrence-free, and overall survival in HCC patients. This establishes Ki-67 as a reliable biomarker for prognostication and therapeutic stratification. In this study, Ki-67-high expression was significantly more prevalent in the ER group (69.0% vs 23.4%), thereby corroborating Xu et al’s34 findings that high Ki-67 independently predicts ER risk following PA-TACE and reinforcing its prognostic significance in the context of PA-TACE.
AFP-L3, an isoform of alpha-fetoprotein with specific glycosylation patterns, is recognized as a complementary tumor biomarker to AFP and PIVKA-II.35,36 In prognostic studies related to PA-TACE, AFP has traditionally been considered a risk factor for poor prognosis; however, this study demonstrates that AFP-L3% is more strongly correlated with ER after PA-TACE than total AFP. Given the current state of research, investigations into AFP-L3% remain relatively limited and require further validation through large-scale multicenter studies. Nonetheless, existing evidence underscores the significant clinical value of AFP-L3% in predicting postoperative recurrence following HCC resection and ER after liver transplantation.37,38
Pro-tumorigenic inflammation drives oncogenesis through epigenetic remodeling, proliferative augmentation, angiogenic activation, and invasion facilitation, enabling malignant conversion and vascular infiltration.39 Lymphocytes are central to immune surveillance, and a reduction in their number may indicate impaired immune function; GGT, as a key enzyme involved in glutathione metabolism, reflects the oxidative stress status in the body.40 GLR, a composite biomarker derived from GGT and lymphocyte count, reflects both tumor-related oxidative stress and host immune competence, demonstrating superior predictive capacity compared to conventional markers. Existing studies41,42 have demonstrated that GLR is closely linked to the prognosis of HCC patients and serves as an effective predictor of ER following hepatectomy. Consistent with earlier studies,30 our results showed that a higher GLR was significantly associated with an increased risk of ER after PA-TACE. Including GLR in the nomogram enhanced both its predictive accuracy and clinical utility.
The limitations of this study are as follows: First, the retrospective study design may have introduced selection bias. Second, the cohort was restricted to solitary tumors ≤10 cm in size, which limits the generalizability of the findings to patients with multinodular or large HCC. Third, the study was conducted at a single institution in an HBV-endemic region, and lacked external validation. Future prospective, multicenter studies involving more diverse populations will be essential to to confirm these findings.
In conclusion, we developed and validated a clinically practical nomogram that incorporates imaging and laboratory indicators to predict ER in solitary HCC patients treated with PA-TACE. By incorporating five independent predictors—MVI, Ki-67, satellite lesions, AFP-L3%, and GLR, the model exhibited high accuracy and strong clinical utility. This tool could aid clinicians in identifying patients who are more likely to derive benefit from PA-TACE, thereby facilitating individualized treatment decisions.
Data Sharing Statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics Statement
This retrospective study was approved by the Ethics Committee of Beijing Youan Hospital, Capital Medical University. Given the anonymized and retrospective nature of the data, the requirement for written informed consent was waived.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that no financial support was received for the research and/or publication of this article.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. European Association for the Study of the Liver. EASL clinical practice guidelines on the management of hepatocellular carcinoma. J Hepatol. 2025;82(2):315–374. doi:10.1016/j.jhep.2024.08.028
2. Ding Z, Wang L, Sun J, Zheng L, Tang Y, Tang H. Hepatocellular carcinoma: pathogenesis, molecular mechanisms, and treatment advances. Front Oncol. 2025;15:1526206. doi:10.3389/fonc.2025.1526206
3. Hwang SY, Danpanichkul P, Agopian V, et al. Hepatocellular carcinoma: updates on epidemiology, surveillance, diagnosis and treatment. Clin Mol Hepatol. 2025;31(Suppl):S228–S254. doi:10.3350/cmh.2024.0824
4. Chen W, Ma T, Zhang J, et al. A systematic review and meta-analysis of adjuvant transarterial chemoembolization after curative resection for patients with hepatocellular carcinoma. HPB. 2020;22(6):795–808. doi:10.1016/j.hpb.2019.12.013
5. Chen ZH, Zhang XP, Zhou TF, et al. Adjuvant transarterial chemoembolization improves survival outcomes in hepatocellular carcinoma with microvascular invasion: a systematic review and meta-analysis. Eur J Surg Oncol. 2019;45(11):2188–2196. doi:10.1016/j.ejso.2019.06.031
6. Shen A, Liu M, Zheng D, Chen Q, Wu Z. Adjuvant transarterial chemoembolization after curative hepatectomy for hepatocellular carcinoma with microvascular invasion: a systematic review and meta-analysis. Clin Res Hepatol Gastroenterol. 2020;44(2):142–154. doi:10.1016/j.clinre.2019.06.012
7. Wang Z, Ren Z, Chen Y, et al. Adjuvant transarterial chemoembolization for HBV-related hepatocellular carcinoma after resection: a randomized controlled study. Clin Cancer Res. 2018;24(9):2074–2081. doi:10.1158/1078-0432.CCR-17-2899
8. He Y, Qian J, Zhu G, et al. Development and validation of nomograms to evaluate the survival outcome of HCC patients undergoing selective postoperative adjuvant TACE. Radiol Med. 2024;129(4):653–664. doi:10.1007/s11547-024-01792-0
9. Qian J, Shen Y, Cui L, et al. Survival effects of postoperative adjuvant TACE in early-HCC patients with microvascular invasion: a multicenter propensity score matching. J Cancer. 2024;15(1):68–78. doi:10.7150/jca.87435
10. Wang H, Du PC, Wu MC, Cong WM. Postoperative adjuvant transarterial chemoembolization for multinodular hepatocellular carcinoma within the Barcelona clinic liver cancer early stage and microvascular invasion. Hepatobiliary Surg Nutr. 2018;7(6):418–428. doi:10.21037/hbsn.2018.09.05
11. Zhao QY, Liu SS, Fan MX. Prediction of early recurrence of hepatocellular carcinoma after resection based on Gd-EOB-DTPA enhanced magnetic resonance imaging: a preliminary study. J Gastrointest Oncol. 2022;13(2):792–801. doi:10.21037/jgo-22-224
12. Wei Y, Pei W, Qin Y, Su D, Liao H. Preoperative MR imaging for predicting early recurrence of solitary hepatocellular carcinoma without microvascular invasion. Eur J Radiol. 2021;138:109663. doi:10.1016/j.ejrad.2021.109663
13. Yang X, Ni H, Lu Z, et al. Mesenchymal circulating tumor cells and Ki67: their mutual correlation and prognostic implications in hepatocellular carcinoma. BMC Cancer. 2023;23(1):10. doi:10.1186/s12885-023-10503-3
14. Liao M, Zhu Z, Wang H, Huang J. Adjuvant transarterial chemoembolization for patients after curative resection of hepatocellular carcinoma: a meta-analysis. Scand J Gastroenterol. 2017;52(6–7):624–634. doi:10.1080/00365521.2017.1292365
15. Feng LH, Dong H, Lau WY, et al. Novel microvascular invasion-based prognostic nomograms to predict survival outcomes in patients after R0 resection for hepatocellular carcinoma. J Cancer Res Clin Oncol. 2017;143(2):293–303. doi:10.1007/s00432-016-2286-1
16. Shindoh J, Kobayashi Y, Kawamura Y, et al. Microvascular invasion and a size cutoff value of 2 cm predict long-term oncological outcome in multiple hepatocellular carcinoma: reappraisal of the American joint committee on cancer staging system and validation using the surveillance, epidemiology, and end-results database. Liver Cancer. 2020;9(2):156–166. doi:10.1159/000504193
17. Luo L, Shan R, Cui L, et al. Postoperative adjuvant transarterial chemoembolisation improves survival of hepatocellular carcinoma patients with microvascular invasion: a multicenter retrospective cohort. United Eur Gastroenterol J. 2023;11(2):228–241. doi:10.1002/ueg2.12365
18. Wang L, Ke Q, Lin N, Zeng Y, Liu J. Does postoperative adjuvant transarterial chemoembolization benefit for all patients with hepatocellular carcinoma combined with microvascular invasion: a meta-analysis. Scand J Gastroenterol. 2019;54(5):528–537. doi:10.1080/00365521.2019.1610794
19. Chen ZH, Zhang XP, Feng JK, et al. Actual long-term survival in hepatocellular carcinoma patients with microvascular invasion: a multicenter study from China. Hepatol Int. 2021;15(3):642–650. doi:10.1007/s12072-021-10174-x
20. Mo A, Lin B, Chen D. Efficacy of sequential TACE on primary hepatocellular carcinoma with microvascular invasion after radical resection: a systematic review and meta-analysis. World J Surg Oncol. 2023;21(1):277. doi:10.1186/s12957-023-03160-0
21. Ye JZ, Chen JZ, Li ZH, et al. Efficacy of postoperative adjuvant transcatheter arterial chemoembolization in hepatocellular carcinoma patients with microvascular invasion. World J Gastroenterol. 2017;23(41):7415–7424. doi:10.3748/wjg.v23.i41.7415
22. Wang K, Xiang YJ, Yu HM, et al. A novel classification in predicting prognosis and guiding postoperative management after R0 liver resection for patients with hepatocellular carcinoma and microvascular invasion. Eur J Surg Oncol. 2022;48(6):1348–1355. doi:10.1016/j.ejso.2021.12.466
23. European Association for the Study of the Liver. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236. doi:10.1016/j.jhep.2018.03.019
24. Xing H, Zhang WG, Cescon M, et al. Defining and predicting early recurrence after liver resection of hepatocellular carcinoma: a multi-institutional study. HPB. 2020;22(5):677–689. doi:10.1016/j.hpb.2019.09.006
25. Wang X, Yu Y, Tao Y, et al. Clinical-radiological characteristic for predicting ultra-early recurrence after liver resection in solitary hepatocellular carcinoma patients. J Hepatocell Carcinoma. 2023;10:2323–2335. doi:10.2147/JHC.S434955
26. Tung-Ping Poon R, Fan ST, Wong J. Risk factors, prevention, and management of postoperative recurrence after resection of hepatocellular carcinoma. Ann Surg. 2000;232(1):10–24. doi:10.1097/00000658-200007000-00003
27. Masuda Y, Yeo MHX, Burdio F, et al. Factors affecting overall survival and disease-free survival after surgery for hepatocellular carcinoma: a nomogram-based prognostic model-a Western European multicenter study. Updates Surg. 2024;76(1):57–69. doi:10.1007/s13304-023-01656-8
28. Plessier A, Codes L, Consigny Y, et al. Underestimation of the influence of satellite nodules as a risk factor for post-transplantation recurrence in patients with small hepatocellular carcinoma. Liver Transpl. 2004;10(2 Suppl 1):S86–90. doi:10.1002/lt.20039
29. Chen C, Liu J, Gu Z, et al. Integration of multimodal computed tomography radiomic features of primary tumors and the spleen to predict early recurrence in patients with postoperative adjuvant transarterial chemoembolization. J Hepatocell Carcinoma. 2023;10:1295–1308. doi:10.2147/JHC.S423129
30. Zhao H, Liu X, Xu R, Guo X, Shen A. Predictive value of and relationship between the gamma-glutamyl transpeptidase to lymphocyte ratio and CT features in hepatocellular carcinoma patients with postoperative adjuvant TACE. J BUON. 2021;26(4):1346–1354.
31. Karabulut E, Akbulut S, Samdanci ET, et al. Are Ki-67 and procalcitonin expression levels useful in predicting the biological behavior of hepatocellular carcinoma after liver transplantation? J Clin Med. 2024;14(1):144. doi:10.3390/jcm14010144
32. Liu J, Yan C, Liu C, et al. Predicting Ki-67 expression levels in breast cancer using radiomics-based approaches on digital breast tomosynthesis and ultrasound. Front Oncol. 2024;14:1403522. doi:10.3389/fonc.2024.1403522
33. Luo Y, Ren F, Liu Y, et al. Clinicopathological and prognostic significance of high Ki-67 labeling index in hepatocellular carcinoma patients: a meta-analysis. Int J Clin Exp Med. 2015;8(7):10235–10247.
34. Xu JX, Qin SL, Wei HW, Chen YY, Peng YC, Qi LN. Prognostic factors and an innovative nomogram model for patients with hepatocellular carcinoma treated with postoperative adjuvant transarterial chemoembolization. Ann Med. 2023;55(1):2199219. doi:10.1080/07853890.2023.2199219
35. Force M, Park G, Chalikonda D, et al. Alpha-Fetoprotein (AFP) and AFP-L3 is most useful in detection of recurrence of hepatocellular carcinoma in patients after tumor ablation and with low AFP level. Viruses. 2022;14(4):775. doi:10.3390/v14040775
36. Yi X, Yu S, Bao Y. Alpha-fetoprotein-L3 in hepatocellular carcinoma: a meta-analysis. Clin Chim Acta. 2013;425:212–220. doi:10.1016/j.cca.2013.08.005
37. Norman JS, Li PJ, Kotwani P, Shui AM, Yao F, Mehta N. AFP-L3 and DCP strongly predict early hepatocellular carcinoma recurrence after liver transplantation. J Hepatol. 2023;79(6):1469–1477. doi:10.1016/j.jhep.2023.08.020
38. Tong JS, Lu CD, Lu CJ, Zheng S, Mao SQ. Longitudinal surveillance of three biomarkers to predict recurrence of hepatocellular carcinoma after radical resection. Eur J Gastroenterol Hepatol. 2023;35(10):1178–1185. doi:10.1097/MEG.0000000000002610
39. Deng Z, Lu L, Li B, Shi X, Jin H, Hu W. The roles of inflammasomes in cancer. Front Immunol. 2023;14:1195572. doi:10.3389/fimmu.2023.1195572
40. Zhang T, Yao C, Zhou X, et al. Glutathione‑degrading enzymes in the complex landscape of tumors (Review). Int J Oncol. 2024;65(1):72. doi:10.3892/ijo.2024.5660
41. Wang Y, Zhou CW, Zhu GQ, et al. A multidimensional nomogram combining imaging features and clinical factors to predict the invasiveness and metastasis of combined hepatocellular cholangiocarcinoma. Ann Transl Med. 2021;9(20):1518. doi:10.21037/atm-21-2500
42. Zhou PC, Huang R, Wang HT, et al. Gamma-glutamyl transferase-to-lymphocyte ratio as a prognostic marker in patients with hepatocellular carcinoma undergoing hepatectomy. World J Gastrointest Surg. 2025;17(2):98578. doi:10.4240/wjgs.v17.i2.98578
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Construction and Validation of a Novel Nomogram for Predicting the Recurrence of Diffuse Large B Cell Lymphoma Treated with R-CHOP
Gong Y, Yan H, Yang Y, Zhai B, Huang Z, Zhang Z
Pharmacogenomics and Personalized Medicine 2023, 16:291-301
Published Date: 1 April 2023
Increased Platelet Distribution Width Predicts 3-Year Recurrence in Patients with Hepatocellular Carcinoma After Surgical Resection
Li H, Liu J, Yan S, Rao C, Wang L
Cancer Management and Research 2023, 15:501-509
Published Date: 14 June 2023
Clinical-Radiological Characteristic for Predicting Ultra-Early Recurrence After Liver Resection in Solitary Hepatocellular Carcinoma Patients
Wang X, Yu Y, Tao Y, Wang Y, Zhang C, Cui Y, Zhou Y
Journal of Hepatocellular Carcinoma 2023, 10:2323-2335
Published Date: 21 December 2023
Establishment and Significance of a Nomogram Prediction Model for the Risk of Hepatocellular Carcinoma in Budd-Chiari Syndrome
Gao ZK, Wu ZC, Xu H
Journal of Hepatocellular Carcinoma 2025, 12:2795-2809
Published Date: 17 December 2025
Construction and Validation of a Predictive Model for Post-TACE Recurrence Risk in Hepatocellular Carcinoma: A Retrospective Cohort Study
Zhao J, Meng Y, Jiang Z, Li Z, Li Y, Liu Y, Zeng Y, Dai S, Du Z, Liu L
Journal of Hepatocellular Carcinoma 2026, 13:584698
Published Date: 18 March 2026