Back to Journals » Patient Preference and Adherence » Volume 16
Why Does COVID-19 Vaccine Acceptance Rate Remain Low Among Patients with Chronic Diseases? Evidences from Public Hospitals of Ethiopia
Authors Daba C ![]() , Asefa L
, Asefa L ![]() , Lemma H, Atamo A
, Lemma H, Atamo A ![]() , Kebede E
, Kebede E ![]() , Gebrehiwot M
, Gebrehiwot M ![]()
Received 11 February 2022
Accepted for publication 24 May 2022
Published 27 May 2022 Volume 2022:16 Pages 1371—1380
DOI https://doi.org/10.2147/PPA.S362131
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Chala Daba,1,* Lechisa Asefa,2 Hailu Lemma,2 Amanuel Atamo,1 Edosa Kebede,3 Mesfin Gebrehiwot1,*
1Department of Environmental Health, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia; 2Department of Environmental Health, Institute of Health, Bule Hora University, Bule Hora, Ethiopia; 3Department of Medical Laboratory, College of Medicine and Health Sciences, Ambo University, Ambo, Ethiopia
*These authors contributed equally to this work
Correspondence: Chala Daba, Email [email protected]
Background: Elders and patients with chronic diseases are more vulnerable to coronavirus disease 2019 (COVID-19) infection. In Ethiopia, these groups of people are given vaccination priorities amongst others. However, there is limited information on the acceptance of COVID-19 vaccine among patients with chronic diseases. Therefore, this study aimed to assess the acceptance of COVID-19 vaccine and associated factors among patients with chronic diseases visiting public hospitals in West Guji zone (Ethiopia).
Methods and Materials: Facility-based cross-sectional study was employed among 408 chronic disease patients visiting two public hospitals in Ethiopia from September to October 2021. Data was collected using structured questionnaire. Multivariable logistic regression was computed to identify factors associated with acceptance of COVID-19 vaccine. Independent variables with p-value less than 0.05 were considered statistically significantly associated with the acceptance of COVID-19 vaccine.
Results: The acceptance of COVID-19 vaccine among patients with chronic diseases was 39.5% (95% CI: 35– 44). Factors positively associated with the acceptance of COVID-19 vaccine were age ≥ 40 years (AOR = 2.84; 95% CI: 1.53– 5.28), urban residence (AOR = 0.6; 95% CI: 0.38– 0.95), having upper respiratory tract infection (AOR = 1.32; 95% CI: 1.03– 2.8), previous COVID-19 infection (AOR = 2.1; 95% CI: 1.22– 3.47), having health insurance (AOR = 2.55; 95% CI: 1.23– 5.28), those not drinking alcohol (AOR = 1.95; 95% CI: 1.24– 3.06), those not chewing Khat (AOR = 2.01; 95% CI: 1.27– 3.2), and having good knowledge (AOR = 1.55; 95% CI: 1.03– 2.87) and positive attitude (AOR = 2.05; 95% CI: 1.26– 3.33) towards the vaccine.
Conclusion: The overall proportion of COVID-19 vaccine acceptance is low among patients with chronic diseases. Therefore, to improve the acceptance of COVID-19 vaccine, the government and health professionals should provide continuous health education.
Keywords: COVID-19, vaccine acceptance, chronic disease, Ethiopia
Introduction
Coronavirus disease 2019 (COVID-19) is one of the viral diseases affecting human respiratory system.1–3 It is transmitted mainly through respiratory droplets that are released from an infected person while sneezing, coughing, and talking.4 As of 8 February 2022, it affected more than 398 million people and caused 5.7 million deaths globally.5 In Africa, over 10.9 million cases and 241,723 deaths were reported as of 8 February, 2022. Similarly, till this period, there were 466,677 confirmed cases and 7373 deaths in Ethiopia.6
Although the virus is infecting all age groups, elders and patients living with chronic diseases, such as hypertension, tuberculosis, cardiac disease, lung disease, cancer, and diabetes, are almost five times more likely to develop severe COVID-19 illnesses and deaths.7,8 To curb the transmission of this pandemic, different prevention and control measures, including social distancing, wearing face masks, proper hand washing with soap, and staying at home, are being applied.8,9 In spite of the implementation of different prevention and control methods, the transmission is not decreasing substantially.10 Hence, development of other effective control method, particularly vaccination, is becoming a significant protective measure against COVID-19 transmission.10–12 Accordingly, as of 28 September 2021, approximately 104 vaccines have been tested in human clinical trials, of which 46 in phase II and 35 in phase III clinical trials.13
However, the acceptance of these vaccines varied from place to place. For instance, a study conducted in northeast Ethiopia by Berihun et al has reported about 59.4% acceptance of COVID-19 vaccine among patients with chronic diseases.14 Other studies performed in northwest Ethiopia, Arab world, and France also reported an acceptance rate of 54.8%17, 62.4%,9 and 65.6%,15 respectively. Higher acceptance rates were also indicated in China (91.3%)19 and Indonesia (93.3%).25 Age, gender, educational level, income, and knowledge were found to be associated with vaccine acceptance.9,14,16–18,24
In Ethiopia, the government has given vaccination priority for the elders and patients with chronic diseases. However, the acceptance of COVID-19 vaccine is reported to be low among patients with chronic diseases,14 which could lead to the loss of many lives since they are more vulnerable to COVID-19 infection. Except for few studies, there is limited evidence that shows the level of acceptance of COVID-19 vaccine and its determinant factors in Ethiopia. Therefore, this study aimed to assess the acceptance of COVID-19 vaccine and associated factors among patients with chronic diseases visiting public hospitals in West Guji zone (Ethiopia). The findings of this study could help suggest priorities of intervention so as to reduce the spread of COVID-19 in Ethiopia and other similar developing countries.
Methods and Materials
Study Design, Period, and Setting
Facility-based cross-sectional study design was employed among 408 patients with chronic diseases who were visiting public hospitals in southern Ethiopia from September to October 2021. The study was conducted on two public hospitals located in West Guji zone, namely Bule Hora teaching hospital and Malka Soda hospital. In West Guji zone, there are three public hospitals which serve more than three million people.
Source and Study Population
All patients with chronic diseases who were visiting the public hospital of West Guji zone were the source population, whereas all patients with chronic diseases who were visiting the randomly selected public hospitals during the data collection time were the study population.
Inclusion and Exclusion Criteria
All patients with chronic diseases who were attending the public hospitals in West Guji zone were included, whereas those who were seriously ill, not volunteer to participate, and under 18 years old were excluded from the study.
Sample Size Determination
The sample size was computed using a single population proportion formula21
Where, “Zα/2” = 1.96, “p” = 59.4%, and “d” -margin of error = 5.0%. “p” is the proportion of COVID-19 vaccine acceptance among patients with chronic diseases which was taken from a study done in Amhara region.14 Accordingly, the calculated sample size becomes 371 and by adding a 10% of non-response rate, the final sample size becomes 408.
Sampling Techniques and Procedure
From the three public hospitals in West Guji zone, two public hospitals (Bule Hora teaching hospital and Malka Soda hospital) were randomly selected by using a lottery method. According to the reports obtained from registration records, about 1457 chronic disease patients of different cases were registered for follow-up in the selected hospitals at the time of the study. Of the total 1457 patients, 569 were scheduled to be present between 1st September, 2021 and 30th October, 2021 for care or pharmacy pick-ups, and hence fulfilled the inclusion criteria. Proportional allocation was then made considering the number of patients in each hospital. Accordingly, 217 patients with chronic diseases from Bule Hora teaching hospital and 191 patients from Malka Soda hospital were interviewed. A simple random sampling technique was used to select the study participants.
Operational Definitions
The dependent variable, acceptance of COVID-19 vaccine, was measured using “Yes” or “No” questions. Comprehensive knowledge towards COVID-19 vaccine was computed considering seven knowledge-related questions. The correct answer for each item was scored “1” and the incorrect answer was scored “0.” Accordingly, patients who scored above the mean value (4.1) were taken as having good knowledge, while those who scored below the mean value (4.1) were considered as having poor knowledge. Similarly, the attitude of the respondents towards COVID-19 vaccine was computed using six attitude-related questions. The correct answer for each item was scored “1” and the incorrect answer was scored “0.” Accordingly, respondents who scored above the mean value (3.2) were considered as having positive attitude and vice versa.
Data Collection Method and Quality Control
The data was collected using a structured questionnaire which was adapted from different published articles.9,14,20,22–25 The questionnaire was prepared in English, translated to local language, and then translated back to English. The internal consistency of the questionnaire was checked using Cronbach’s alpha coefficient and was found to be 0.85. Pre-test was conducted in Karca public hospital (n = 21) and amendment was made before the actual data collection. Face-to-face interview was used as a means of data collection. Three nurses and two supervisors (health officers) were recruited for data collection. The completeness and consistency of the data was checked daily by the supervisors. In addition, to ensure accuracy, 5% of the data was double-entered.
Data Management and Statistical Analysis
The collected data was checked, coded, and entered into EpiData version 3.1 and exported to SPSS version 25.0 for data cleaning and analysis. Logistic regression analyses (bivariate and multivariable logistic regression) were carried out to analyze the data. In the bivariate analysis, variables with p-value ≤0.25 were retained for the multivariable logistic regression analysis. Multivariable logistic regression was computed to identify significant factors associated with the acceptance of COVID-19 vaccine. Variables with p-value <0.05 were considered to be significantly associated with the acceptance of COVID-19 vaccine. Hosmer Lemeshow test26 with a p-value of 0.157 indicated that the model was fit.
Ethical Considerations
The study complies with the declaration of Helsinki. All procedures, including ethical approval and research permission, were performed in accordance with national standards, guaranteeing the anonymity of the respondents. Ethical approval (BHU/IH 3015/2/2013) was obtained from the Ethical Review Committee of the Institute of Health, Bule Hora University. Besides, written consent was obtained from the heads of the selected hospitals. In addition, respondents were informed about the purpose of the study, and their informed consent was obtained. The respondents’ right to refuse or withdraw from the study was fully maintained, and the information provided by each respondent was kept strictly confidential.
Results
Socio-Demographic Characteristics
A total of 408 respondents have participated, giving a response rate of 100%. More than one-third (42.6%) of the respondents were within the age group of 30–39 years, and the slight majority of the study participants were male (n = 210, 51.5%). More than three-fourths (77.2%) of the study participants had no previous COVID-19 infection and 99.5% of the patients with chronic diseases had no family death due to COVID-19. Again, more than three-fourths (85.8%) of the patients had health insurance. Regarding the types of chronic diseases, majority (121, 29.7%) of the study participants had TB diseases followed by HIV (110, 27%) (Table 1).
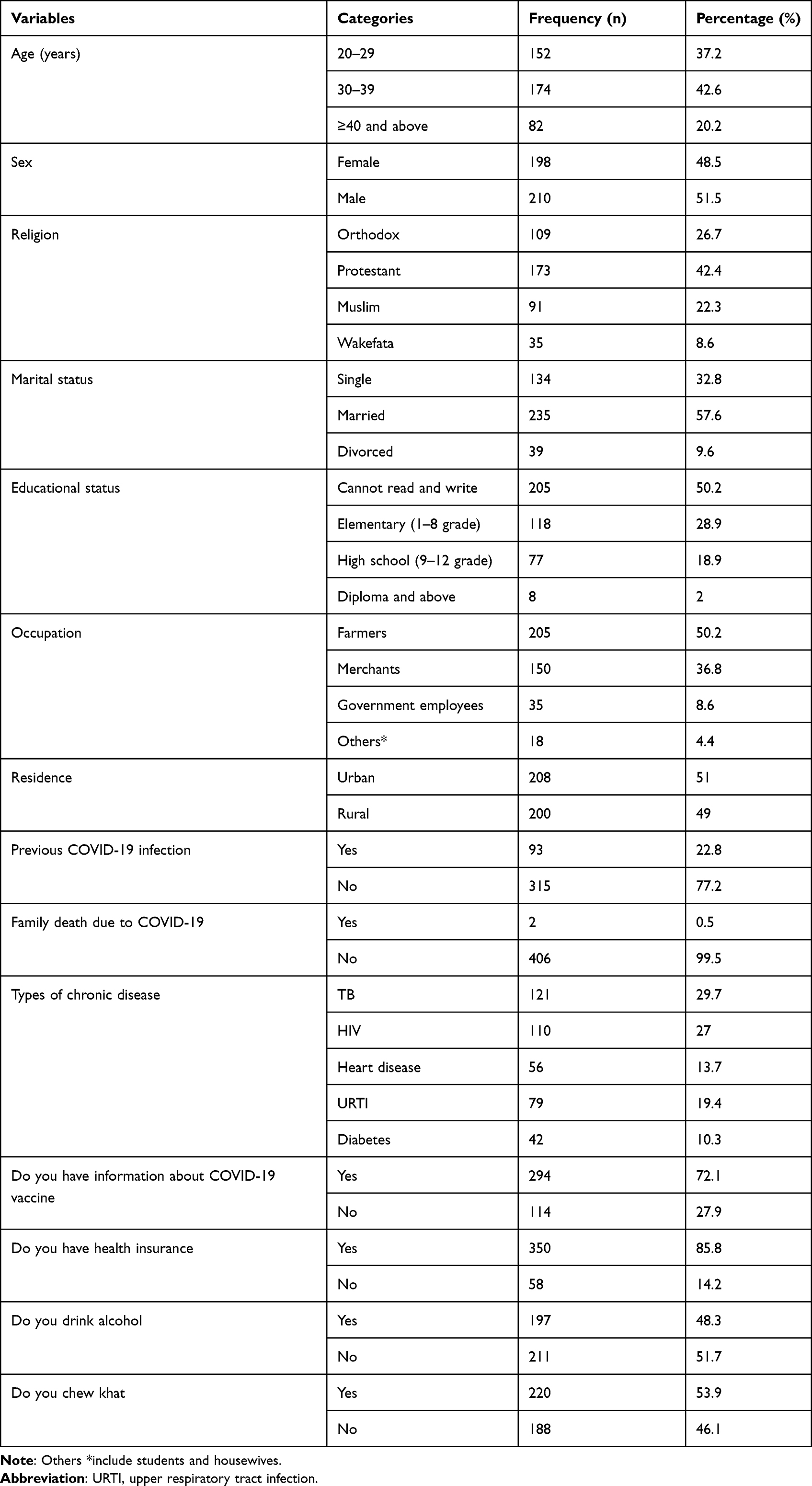 |
Table 1 Socio-Demographic Characteristics of Patients with Chronic Disease (September to October, 2021) |
Willingness to Accept COVID-19 Vaccine
In the current study, only 161 (39.5%, 95% CI: 35–44) of the patients with chronic diseases were willing to accept COVID-19 vaccination.
Knowledge of the Study Participants Towards COVID-19 Vaccine
More than one-third (161, 39.6%) of the study patients with chronic diseases had good knowledge about COVID-19 vaccine. Two-thirds (270, 66.2%) of the respondents knew COVID-19 vaccine could reduce the risk of virus infection and less than two-thirds (237, 58.1%) of patients knew COVID-19 vaccination has started in Ethiopia (Table 2).
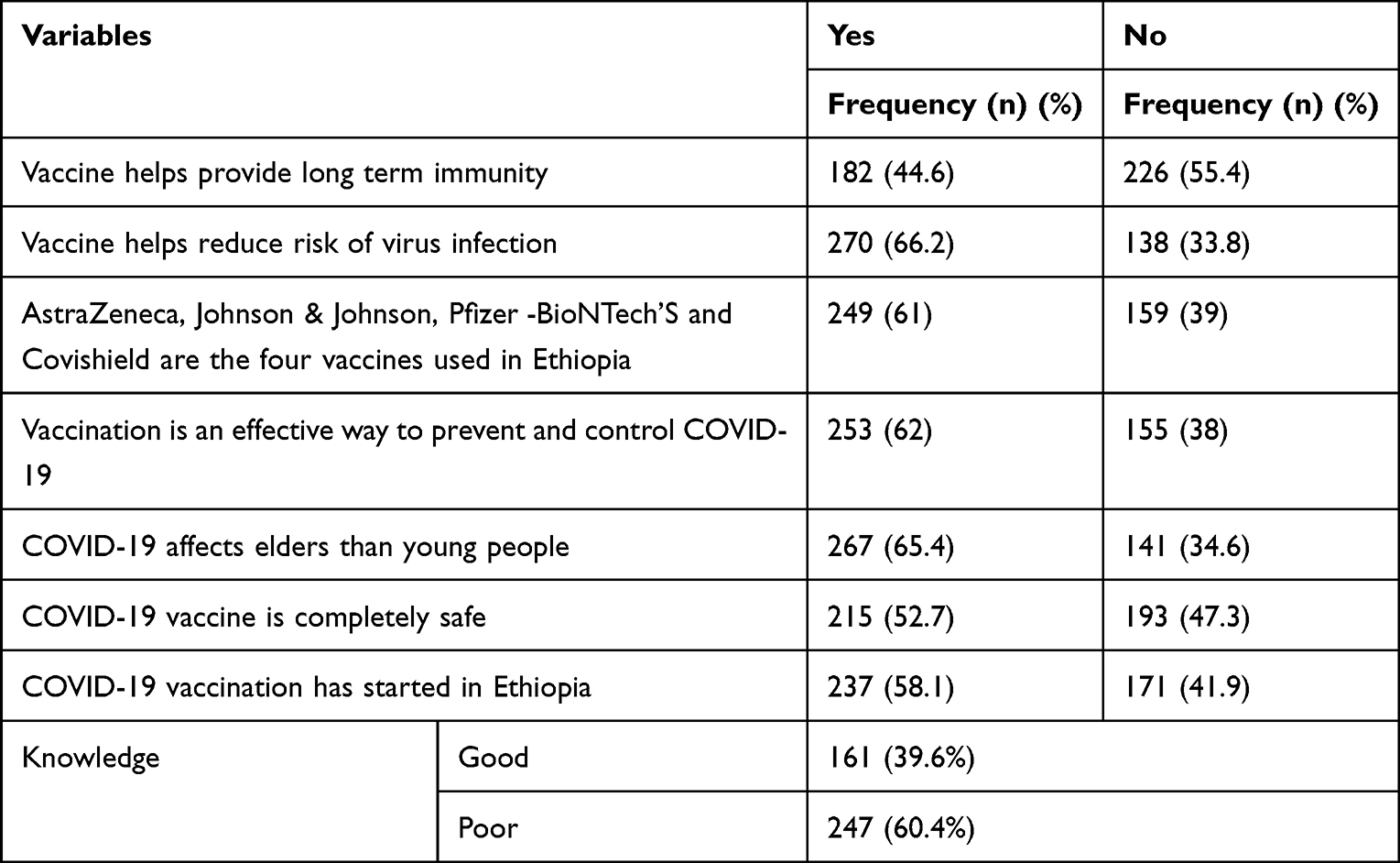 |
Table 2 Knowledge of Respondents Towards COVID-19 Vaccine (September to October, 2021) |
Attitude of the Study Participants Towards COVID-19 Vaccine
Only about one-third (144, 35.3%) of the participants had positive attitude towards COVID-19 vaccine. On top of that, more than half (229, 56.1%) of the respondents believed COVID-19 vaccine had side effects. Despite this, 217 (53.2%) of the respondents believed they are susceptible to COVID-19 (Table 3).
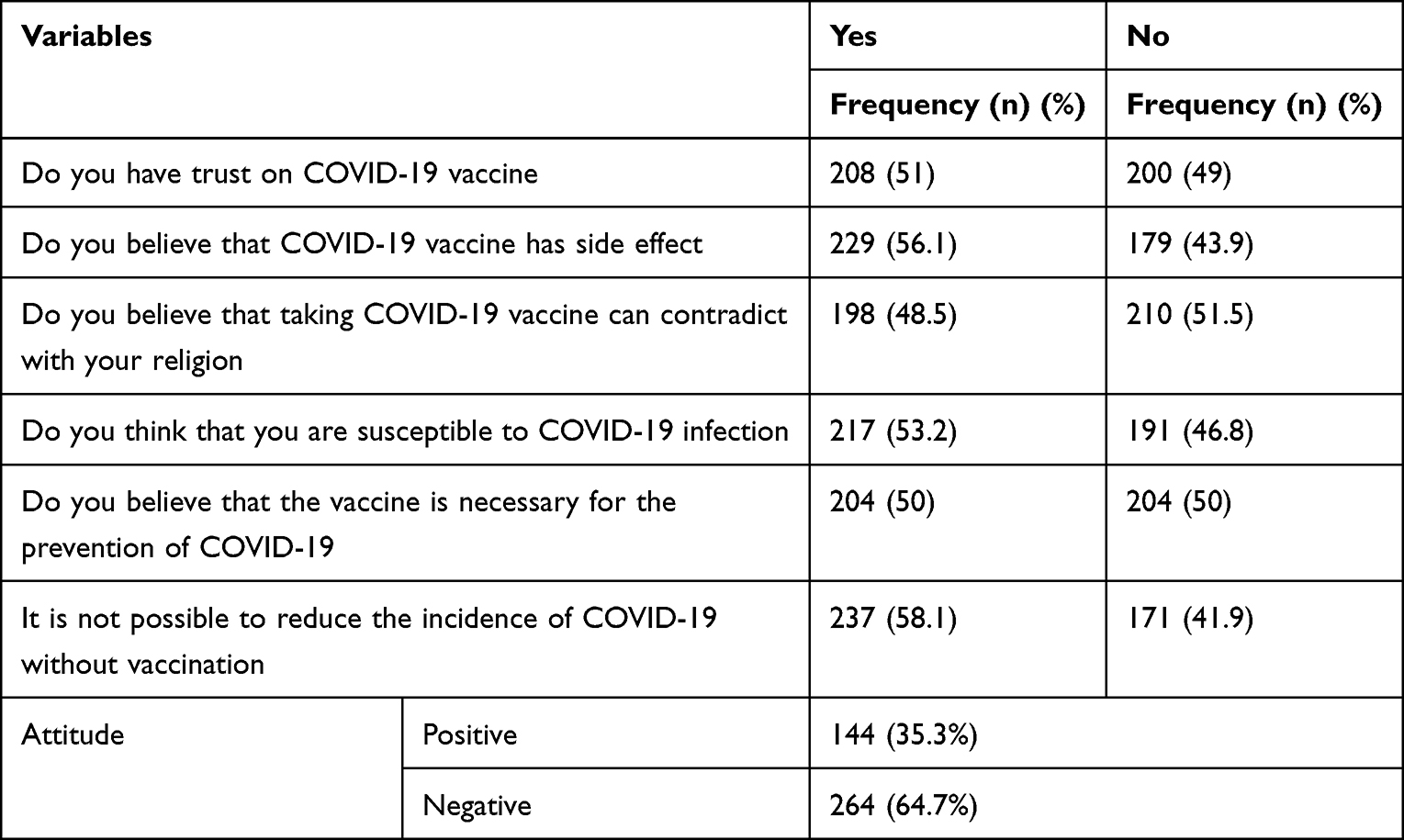 |
Table 3 Attitude of Respondents Towards COVID-19 Vaccine (September to October, 2021) |
Factors Associated with the Willingness to Accept COVID-19 Vaccine
In the multivariable logistic regression analysis, the factors knowledge and attitude towards COVID-19 vaccine, age, residence, health insurance, previous COVID-19 infection, chewing Khat, alcohol use, and types of chronic diseases were significantly associated with the acceptance of COVID-19 vaccine. To indicate some, patients who had upper respiratory tract infection (URTI) were 1.32 times more likely to accept COVID-19 vaccine than patients with other types of chronic diseases (AOR = 1.32, 95% CI: 1.03–2.80). Patients older than 40 years were also likely to accept COVID-19 vaccine (AOR = 2.84, 95% CI: 1.53–5.28).
The odds of COVID-19 vaccine acceptance were 1.95 times higher among non-alcohol user patients than others (AOR = 1.95, 95% CI: 1.24–3.06). Patients who did not chew Khat were two times more likely to accept COVID-19 vaccine than those who did chew (AOR = 2.01, 95% CI: 1.27–3.2). Once more, participants who had good knowledge about COVID-19 vaccine were 1.55 times more likely to accept COVID-19 vaccine than these with poor knowledge (AOR = 1.55, 95% CI: 1.03–2.87). In the same way, the odds of COVID-19 vaccine acceptance were two times higher among patients who had positive attitude towards COVID-19 vaccine (AOR = 2.05, 95% CI: 1.26–3.33) (Table 4).
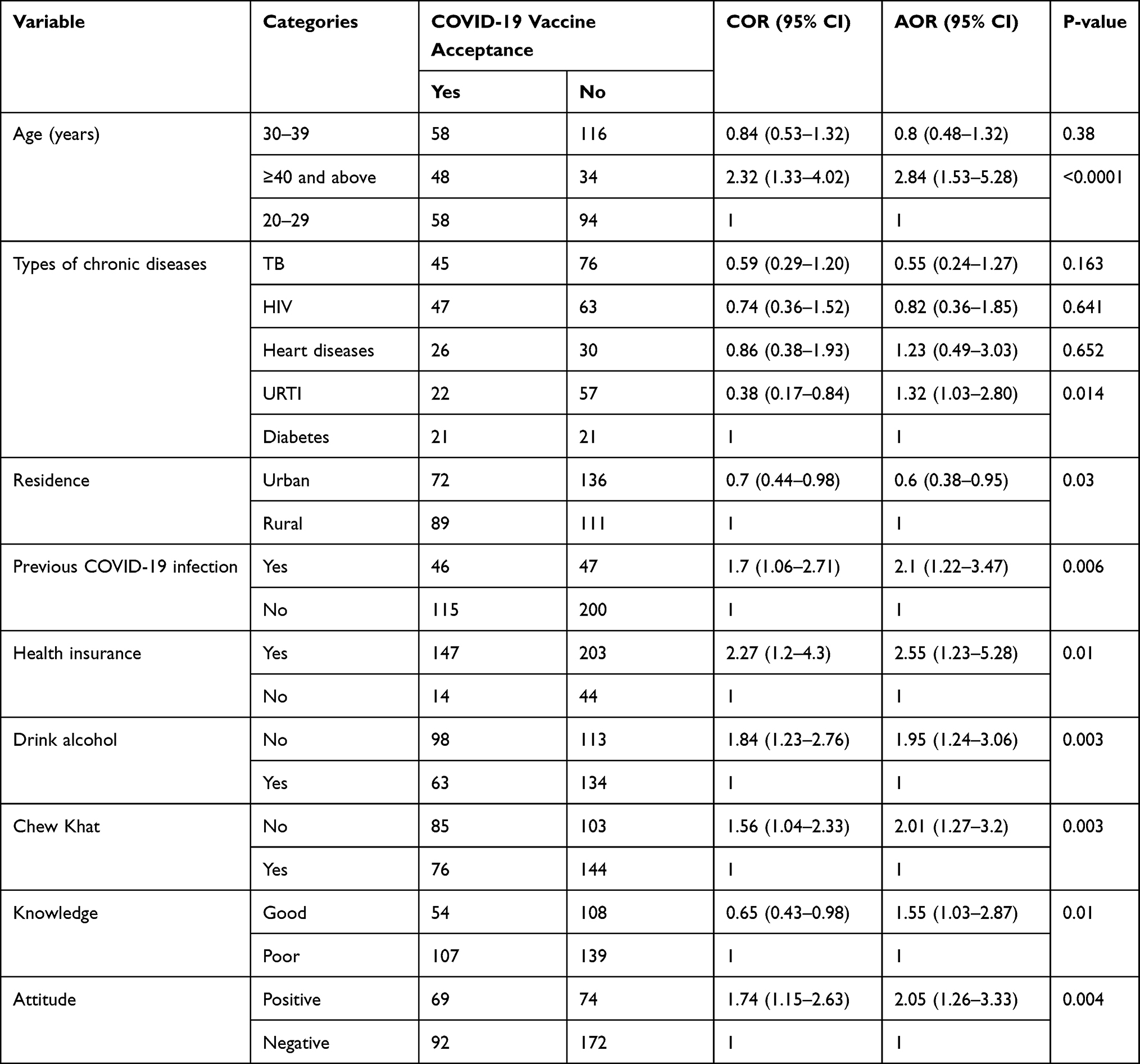 |
Table 4 Factors Associated with the Acceptance of COVID-19 Vaccine Among Patients with Chronic Diseases (September to October, 2021) |
Discussion
The aim of this study was to assess the acceptance of COVID-19 vaccine among patients with chronic diseases, who visited public hospitals in West Guji (Ethiopia). The study showed that the acceptance rate of COVID-19 vaccine among patients with chronic diseases was only 39.5% (95% CI: 35–44) which is lower than the findings in Chile (49%),37 Northern Ethiopia (59.4%),14 Arab world (62.4%),9 Southern Ethiopia (62.6%),24 the Netherlands (73%),27 Australia (77.3%),29 Denmark (80%),27 China (91.3%),19 Indonesia (93.3%),25 and Malaysia (94.3%).28 On the other hand, our finding is consistent with a study done in the USA,30 where vaccine acceptance was 36%. The generally low COVID-19 vaccine acceptance in this study might be due to perceived benefits, action signals, susceptibility, and severity of COVID-19.37 Difference in vaccine acceptance among different countries might also be associated with variations in socio-demographic characteristics of the participants, time of the study period, and availability of health facility.
The present study revealed that knowledge and attitude towards COVID-19 vaccine, age, residence, health insurance, previous COVID-19 infection, khat chewing, habit of drinking alcohol, and type of chronic disease were significant factors associated with the acceptance of COVID-19 vaccine. COVID-19 vaccine was three times more likely to be accepted by patients with age greater than 40 years old as compared to patients with age group between 20 and 29 years old. This finding is consistent with the finding in other parts of Ethiopia24 and Arab world.9
In this study, more than one-third (39.6%) of the study patients had good knowledge about COVID-19 vaccine. The finding of this study was in line with the reports from West India (35.5%).35 This figure was, however, lower than that reported in South Ethiopia (74%),24 Bangladesh (62.1%),33 Southeast Ethiopia (62.7%),14 France (81.2%),15 and southwest Ethiopia (87%).34 This disparities may be due to dissemination of information about COVID-19 vaccine to the risk group, variations of the study period, and accessibility of health facility. Patients who had good knowledge towards COVID-19 vaccine were almost one and half times more likely to accept the vaccine as compared to those who had poor knowledge. The finding of this study corroborates other previous reports from northeastern Ethiopia, Southern Gondar, Pakistan, and the USA.14,24,31,32 Similarly, the present study revealed that only 35.3% of the participants had positive attitude towards COVID-19 vaccine which was lower than the findings in China (70.1%),36 Ethiopia (44%),24 and Bangladesh (78%).33 This difference might be due to the variation of the target population, study design, and variation in risk perception towards COVID-19.
The odds of COVID-19 vaccine acceptance were two times higher among patients who had health insurance than those who had no health insurance. This is in agreement with studies done in Southeastern Ethiopia,14 USA,30 and China.22 We also found that the likelihood of vaccine acceptance was two times higher among patients who had previous COVID-19 infection than those who had no previous COVID-19 infection. As more than two-thirds (77.2%) of the participants were not previously infected by COVID-19, the low acceptance rate of the vaccine is alarming. Indeed, our finding is in agreement with that found in the Arab world.9
Furthermore, participants who did not consume alcohol and who did not chew khat were likely to accept COVID-19 vaccine as compared to their counterparts. This is possibly associated with addiction-related negligence and carelessness to avoid COVID-19.
Conclusions
In this study, we found the proportion of COVID-19 vaccine acceptance among patients with chronic diseases to be low. This low acceptance of COVID-19 vaccine would have a significant adverse effect. The main factors that were positively associated with COVID-19 vaccine acceptance were age greater than forty years, being resident in urban area, having upper respiratory tract infection, previous COVID-19 infection, having health insurance, those not drinking alcohol, those not chewing khat, and positive attitude and good knowledge towards COVID-19 vaccine. Therefore, we recommend that interventions, such as continuous health education and awareness creation about the risks of the pandemic, and benefit, safety, and efficacy of the vaccine should be delivered to patients with chronic diseases. These factors influencing the acceptance/rejection of vaccine should also be considered in developing promotional mechanisms and formulating public health policies towards controlling COVID-19.
Limitation of the Study
This cross-sectional study was based on self-reported vaccine acceptance, and hence the results were possibly liable to social desirability and recall biases. The study also did not consider those people who were hesitant to get vaccinated.
Abbreviations
AOR, adjusted odds ratio; CI, confidence interval; COR, crude odds ratio; COVID-19, coronavirus disease 2019; Ref, reference.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethical Approval
The study complies with the declaration of Helsinki. All procedures, including ethical approval and research permission, were performed in accordance with national standards, guaranteeing the anonymity of the respondents. Ethical approval (BHU/IH 3015/2/2013) was obtained from the Ethical Review Committee of the Institute of Health, Bule Hora University. Besides, written consent was obtained from the heads of the selected hospitals. In addition, respondents were informed about the purpose of the study, and their informed consent was obtained. The respondents’ right to refuse or withdraw from the study was fully maintained, and the information provided by each respondent was kept strictly confidential.
Acknowledgments
We would like to forward our heartfelt thanks to Bule Hora University, Institute of Health, for providing ethical clearance for this study. The authors also want to extend their pleasure to the heads of the hospitals for their permission to conduct this study. Besides, we acknowledge the data collectors, supervisors, and study participants for their commitment, efforts, and willingness to participate in this study.
Funding
There is no funding to report.
Disclosure
The authors declare that there are no competing interests in this study.
References
1. Zhu N, Zhang D, Wang W, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020;382(8):727–733. doi:10.1056/NEJMoa2001017
2. Saqlain M, Munir MM, Rehman SU, et al. Knowledge, attitude, practice and perceived barriers among healthcare workers regarding COVID-19: a cross-sectional survey from Pakistan. J Hosp Infect. 2020;105(3):419–423. doi:10.1016/j.jhin.2020.05.007
3. Elhadi M, Msherghi A, Alkeelani M, et al. Assessment of healthcare workers’ levels of preparedness and awareness regarding Covid-19 infection in low-resource settings. Am J Trop Med Hyg. 2020;103(2):828–833. doi:10.4269/ajtmh.20-0330
4. Kumar J, Katto MS, Siddiqui AA, et al. Knowledge, attitude, and practices of healthcare workers regarding the use of face mask to limit the spread of the new coronavirus disease (COVID-19). Cureus. 2020;12(4):e7737.
5. Worldometers report COVID-19 case in the world; 2022 Available from: https://www.worldometers.info/coronavirus/.
6. Worldometer report COVID-19 cases in Ethiopia; 2022. Avaliable from: https://www.worldometers.info/coronavirus/country/ethiopia.
7. Kebede Y, Yitayih Y, Birhanu Z, Mekonen S, Ambelu A. Knowledge, perceptions and preventive practices towards COVID-19 early in the outbreak among Jimma University Medical Center visitors, Southwest Ethiopia. PLoS One. 2020;15(5):1–15. doi:10.1371/journal.pone.0233744
8. Hoque AM, Hoque M, Hoque ME, Van Hal G. Estimates and determinants of psychological problems of pregnant women during COVID-19 epidemic in South Africa. Eur J Med Heal Sci. 2021;3(1):143–149.
9. Kaadan MI, Abdulkarim J, Chaar M, Zayegh O, Keblawi MA. Determinants of COVID-19 vaccine acceptance in the Arab world: a cross-sectional study. Glob Heal Res Policy. 2021;6(1):1–7.
10. Tran VD, Pak TV, Gribkova EI, et al. Determinants of covid-19 vaccine acceptance in a high infection-rate country: a cross-sectional study in Russia. Pharm Pract. 2021;19(1):1–9.
11. The New York Times. Coronavirus vaccine tracker. Available from: https://www.nytimes.com/interactive/2020/science/coronavirus-vaccine-tracker.html.
12. A phase 2a, randomized, observer-blind, placebo controlled, dose-confirmation study to evaluate the safety, reactogenicity, and immunogenicity of mRNA-1273 SARS-COV-2 vaccine in adults aged 18 years and older. Avalialble from: https://clinicaltrials.gov/ct2/show/NCT04405076.
13. Adaptive phase IB-II randomized clinical trial of preventive vaccine consisting of autologous dendritic cells loaded with antigens from severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), with or without GM-CSF, in subjects negative for COVID-19. Available from: https://clinicaltrials.gov/ct2/show/NCT04386252.
14. Berihun G, Walle Z, Berhanu L, Teshome D. Acceptance of covid-19 vaccine and determinant factors among patients with chronic disease visiting Dessie comprehensive specialized hospital, northeastern Ethiopia. Patient Prefer Adherence. 2021;15:1795–1805. doi:10.2147/PPA.S324564
15. Verger P, Scronias D, Dauby N, et al. Attitudes of healthcare workers towards COVID-19 vaccination: a survey in France and French-speaking parts of Belgium and Canada, 2020. Eurosurveillance. 2021;26(3):1–8. doi:10.2807/1560-7917.ES.2021.26.3.2002047
16. Famuyiro TB, Ogunwale A, Des Bordes J, Raji M. COVID-19: perceived infection risk and barriers to uptake of Pfizer-BioNTech and moderna vaccines among community healthcare workers. J Racial Ethn Heal Disparities. 2021;15:7–12.
17. Handebo S, Wolde M, Shitu K, Kassie A. Determinant of intention to receive COVID-19 vaccine among school teachers in Gondar City, Northwest Ethiopia. PLoS One. 2021;16(6 June):1–11. doi:10.1371/journal.pone.0253499
18. Paul E, Steptoe A, Fancourt D. Attitudes towards vaccines and intention to vaccinate against COVID-19: implications for public health communications. Lancet Reg Heal - Eur. 2021;1:100012.
19. Lin Y, Hu Z, Zhao Q, Alias H, Danaee M, Wong LP. Understanding COVID-19 vaccine demand and hesitancy: a nationwide online survey in China. PLoS Negl Trop Dis. 2020;14(12):e0008961. doi:10.1371/journal.pntd.0008961
20. Wang J, Jing R, Lai X, et al. Acceptance of covid-19 vaccination during the covid-19 pandemic in China. Vaccines. 2020;8(3):1–14. doi:10.3390/vaccines8030482
21. Kelsey JL, Whittemore AS, Evans ASTW. Methods in Observational Epidemiology: Monographs in Epidemiology and Biostatistics. New York, Oxford: Oxford University Press; 1996:2245–2252.
22. Liu R, Zhang Y, Nicholas S, Leng A, Maitland E, Wang J. COVID-19 vaccination willingness among Chinese adults under the free vaccination policy. Vaccines. 2021;9(3):1–10. doi:10.3390/vaccines9030292
23. Ademas A, Adane M, Keleb A, et al. Covid-19 prevention practices and associated factors among diabetes and HIV/AIDS clients in south-wollo zone, Ethiopia: a health facility-based cross-sectional study. J Multidiscip Healthc. 2021;14(August):2079–2086. doi:10.2147/JMDH.S325207
24. Abebe H, Shitu S, Mose A. Understanding of COVID-19 vaccine knowledge, attitude, acceptance, and determinates of COVID-19 vaccine acceptance among adult population in Ethiopia. Infect Drug Resist. 2021;14:2015–2025. doi:10.2147/IDR.S312116
25. Harapan H, Wagner AL, Yufika A, et al. Acceptance of a COVID-19 vaccine in Southeast Asia: a cross-sectional study in Indonesia. Front Public Heal. 2020;8(July):1–8.
26. Hosmer J, Lemeshow SSR. Applied Logistic Regression.
27. Neumann-Böhme S, Varghese NE, Sabat I, et al. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur J Heal Econ. 2020;21(7):977–982. doi:10.1007/s10198-020-01208-6
28. Wong LP, Alias H, Wong PF, Lee HY, AbuBakar S. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Hum Vaccines Immunother. 2020;16(9):2204–2214. doi:10.1080/21645515.2020.1790279
29. Rhodes A, Hoq M, Measey MADM. Intention to vaccinate against COVID-19 in Australia. Lancet Infect Dis. 2020;21(January):2020–2021.
30. Shekhar R, Sheikh AB, Upadhyay S, Singh M, Kottewar S. COVID-19 vaccine acceptance among health care workers in the United States. Vaccine. 2021;9:1–15.
31. Guidry JPD, Laestadius LI, Vraga EK, et al. Willingness to get the COVID-19 vaccine with and without emergency use authorization. Am J Infect Control. 2021;49(1):137–142. doi:10.1016/j.ajic.2020.11.018
32. Maraqa B, Nazzal Z, Rabi R, Sarhan N, Al-Shakhrah K, Al-Kaila M. COVID-19 vaccine hesitancy among health care workers in Palestine: a call for action. Prev Med. 2021;149(January):106618. doi:10.1016/j.ypmed.2021.106618
33. Saiful Islam M, Siddique AB, Akter R, et al. Knowledge, attitudes and perceptions towards COVID-19 vaccinations: a cross-sectional community survey in Bangladesh. medRxiv. 2021;2021. doi:10.1101/2021.02.16.21251802
34. Mose A, Yeshaneh A. COVID-19 vaccine acceptance and its associated factors among pregnant women attending antenatal care clinic in southwest Ethiopia: institutional-based cross-sectional study. Int J Gen Med. 2021;14(June):2385–2395. doi:10.2147/IJGM.S314346
35. Bhartiya S, Kumar N, Singh T, Murugan S, Rajavel SWM. Knowledge, attitude and practice towards COVID-19 vaccination acceptance in West India. Int J Community Med Public Heal. 2021;8(3). doi:10.18203/2394-6040.ijcmph2021048
36. Jiang N, Wei B, Lin H, Wang Y, Chai S, Liu W. Nursing students’ attitudes, knowledge and willingness of to receive the coronavirus disease vaccine: a cross-sectional study. Nurse Educ Pract. 2021;55(May):103148. doi:10.1016/j.nepr.2021.103148
37. Cerda AA, García LY. Hesitation and refusal factors in individuals ’ decision-making processes regarding a coronavirus disease 2019 vaccination. Front Public Heal. 2021;9(April). doi:10.3389/fpubh.2021.626852
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Willingness to receive the COVID-19 vaccine and associated factors among residents of Southwestern Ethiopia: A cross-sectional study
Jabessa D, Bekele F
Patient Preference and Adherence 2022, 16:1177-1185
Published Date: 3 May 2022
Baseline Thrombocytopenia and Disease Severity Among COVID-19 Patients, Tibebe Ghion Specialized Hospital COVID-19 Treatment Center, Northwest Ethiopia
Asrie F, Tekle E, Gelaw Y, Dagnew M, Gelaw A, Negash M, Kassa E, Bizuneh S, Wudineh D
Journal of Blood Medicine 2022, 13:315-325
Published Date: 10 June 2022
Determinant Factors of COVID-19 Vaccine Hesitancy Among Adult and Elderly Population in Central Java, Indonesia
Utami A, Margawati A, Pramono D, Nugraheni A, Pramudo SG
Patient Preference and Adherence 2022, 16:1559-1570
Published Date: 28 June 2022
COVID-19 Case Fatality Rate and Factors Contributing to Mortality in Ethiopia: A Systematic Review of Current Evidence
Girma D, Dejene H, Adugna L, Tesema M, Awol M
Infection and Drug Resistance 2022, 15:3491-3501
Published Date: 4 July 2022
New Onset of Severe Plaque Psoriasis Following COVID-19 Vaccination: A Case Report
Hu YQ, Zhang JZ, Zhao Y
Clinical, Cosmetic and Investigational Dermatology 2022, 15:1485-1487
Published Date: 2 August 2022