Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Which Remote Exercise Interventions are Most Effective in Improving Physical Activity and Quality of Life in Patients with Chronic Obstructive Pulmonary Disease? A Systematic Review and Network Meta-Analysis
Authors Tang H, Shen H, Chen G, Luo X, Wu Q, Liu Y
Received 17 July 2025
Accepted for publication 28 October 2025
Published 8 November 2025 Volume 2025:20 Pages 3607—3629
DOI https://doi.org/10.2147/COPD.S552283
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Huan Tang,* Huapeng Shen,* Guihua Chen, Xiaoqing Luo, Qian Wu, Yiqun Liu
Department of Respiratory and Critical Care Medicine, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, 400010, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guihua Chen; Xiaoqing Luo, Department of Respiratory and Critical Care Medicine, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, 400010, People’s Republic of China, Email [email protected]; [email protected]
Background: Remote technology is recommended for exercise management in chronic obstructive pulmonary disease (COPD) patients to enhance health and exercise function. Despite numerous studies, the optimal combination of remote technologies and auxiliary interventions remains unclear.
Objective: Evaluate which remote exercise interventions and their additional behavioral support measures are most effective in improving exercise function, exercise behavior, and healthy quality of life in COPD patients.
Methods: A systematic review using a network meta-analysis (NMA) of randomized controlled trials (RCTs). We searched PubMed, the Cochrane Central Register of Controlled Trials, Web of Science, EMBASE, CINAHL, and Medline from their inception to December 31, 2024. RCTs evaluating remote exercise interventions were included. The NMA was performed using STATA software.
Results: Twenty-nine RCTs were included (3,234 participants). Remote device & Exercise was superior in improving 6-minute walking distance (6MWD, SMD 0.51, 95% CI 0.10− 0.93, SUCRA 81.8%) compared to usual care, traditional face-to-face rehabilitation, and other remote exercise intervention types; Online self-management & Exercise was superior in facilitating daily activity time (SMD 0.48, 95% CI 0.08− 0.88, SUCRA 90.1%); Application & Exercise significantly improved healthy quality of life (Negative scale, SMD -0.67, 95%CI-1.05−-0.29, SUCRA 81.1%); increased behavioral aids had an integrative effect with the remote exercise intervention, Motivation & Feedback + Health education significantly improved exercise function and quality of life; Motivational interviewing + Goal setting + Activity monitor/Pedometer + Health education significantly promoted exercise behavior. On average, the quality of evidence ranged from low to very low.
Conclusion: This review found evidence that remote exercise series of interventions is superior in improving outcomes such as exercise function, promoting exercise behavior and enhancing healthy quality of life in patients with COPD. Additional behavioral aids had an integrative effect on outcome improvement.
Plain Language Summary: Clinical guidelines recommend remote technology for home-based COPD exercise rehabilitation to overcome constraints, yet evidence supporting specific remote exercise interventions remains limited. This review found:Remote device & Exercise was the most effective remote-exercise intervention to improve exercise function.Online self-management & Exercise, Application & Exercise and Telephone & Exercise were the most effective in improving exercise behaviour and quality of life, respectively.The effectiveness of the remote-exercise interventions utilised a limited range of behaviour change interventions.
Keywords: chronic obstructive pulmonary disease, remote exercise, physical activity, network meta-analysis
Background
Chronic obstructive pulmonary disease (COPD) affects individuals worldwide. It causes patients to experience breathlessness, reduced physical function, diminished social engagement, places a significant burden on healthcare systems, and is a key predictor of years lived with disability.1 In the future, the disease and economic burden of COPD is likely to continue increasing due to ongoing exposure to risk factors.2 Clinical guidelines recommend exercise intervention as a vital non-pharmacological treatment to improve clinical symptoms and functional outcomes in COPD patients, provided that exercise translates into genuine physical activity.3 Compared to inactive patients, those engaging in exercise experience a 34% reduction in the risk of readmission within 30 days of discharge and a 47% decrease in mortality risk within 12 months.4 However, it is well established that exercise and activity levels among COPD patients fall far short of guideline targets (achievement rates approximately 23.0–34.3%) due to various complex factors.5–7 Their daily step counts cluster between 4064 and 6000 steps,8,9 with 6,000 steps being the current step target recommended by the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines.10 The 4,064-step range equates to approximately 70% of the average daily step count for older adults within the same national context.8 Among these complex factors, the most severe is the limited capacity of rehabilitation centers11 and staff, making it difficult to disseminate health knowledge and conduct effective supervision. Remote exercise may help address these challenges.
Remote-exercise intervention12 refers to the use of remote technologies such as telephone or internet-based platforms (eg, videoconferencing) to deliver exercise training. Recent systematic reviews13–15 have reiterated the multiple benefits of remote exercise for COPD patients, including improved exercise capacity, enhanced quality of life, and alleviation of breathlessness. However, these reviews reported limited outcome measures, failing to consider exercise behavior and thus unable to address whether remote exercise facilitates behavioral improvement. Furthermore, their meta-analysis methodology permitted comparisons only between two groups, without distinguishing between different components of the implemented interventions. Consequently, they could not answer crucial questions regarding which remote exercise technology yields superior or optimal therapeutic outcomes. Network meta-analysis builds upon traditional meta-analysis techniques by incorporating weighted synthesis, enabling simultaneous comparison of three or more treatment approaches while accounting for additional sources of heterogeneity. This facilitates better determination of optimal remote exercise management for COPD patients. To date, no network meta-analyses closely related to this topic have been identified. Therefore, the objective of this systematic review is to determine through network meta-analysis:
Which remote exercise intervention technologies and their adjunctive behavioral interventions are most effective in improving exercise function, exercise behavior, and health-related quality of life in patients with chronic obstructive pulmonary disease (COPD)?
Methods
This study is reported according to the Network Meta-Analysis extension of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA-NMA) reporting guidelines16 and was registered in PROSPERO database (CRD420251001560).17 The PRISMA-NMA checklist is listed in Supplementary Material 1 of eAddenda.
Identification and Selection of Studies
The Cochrane Central Register of Controlled Trials, PubMed, Web of Science, EMBASE, CINAHL, and Medline were searched from indexing to 31 December 2024. The search strategy used appropriate thesaurus and free text terms with free words containing three key concepts: Pulmonary Disease, Chronic Obstructive, Remote, Exercise (for the full search strategy, see Supplementary Material 2 on eAddenda). The search strategy was peer reviewed using the PRESS checklist.18
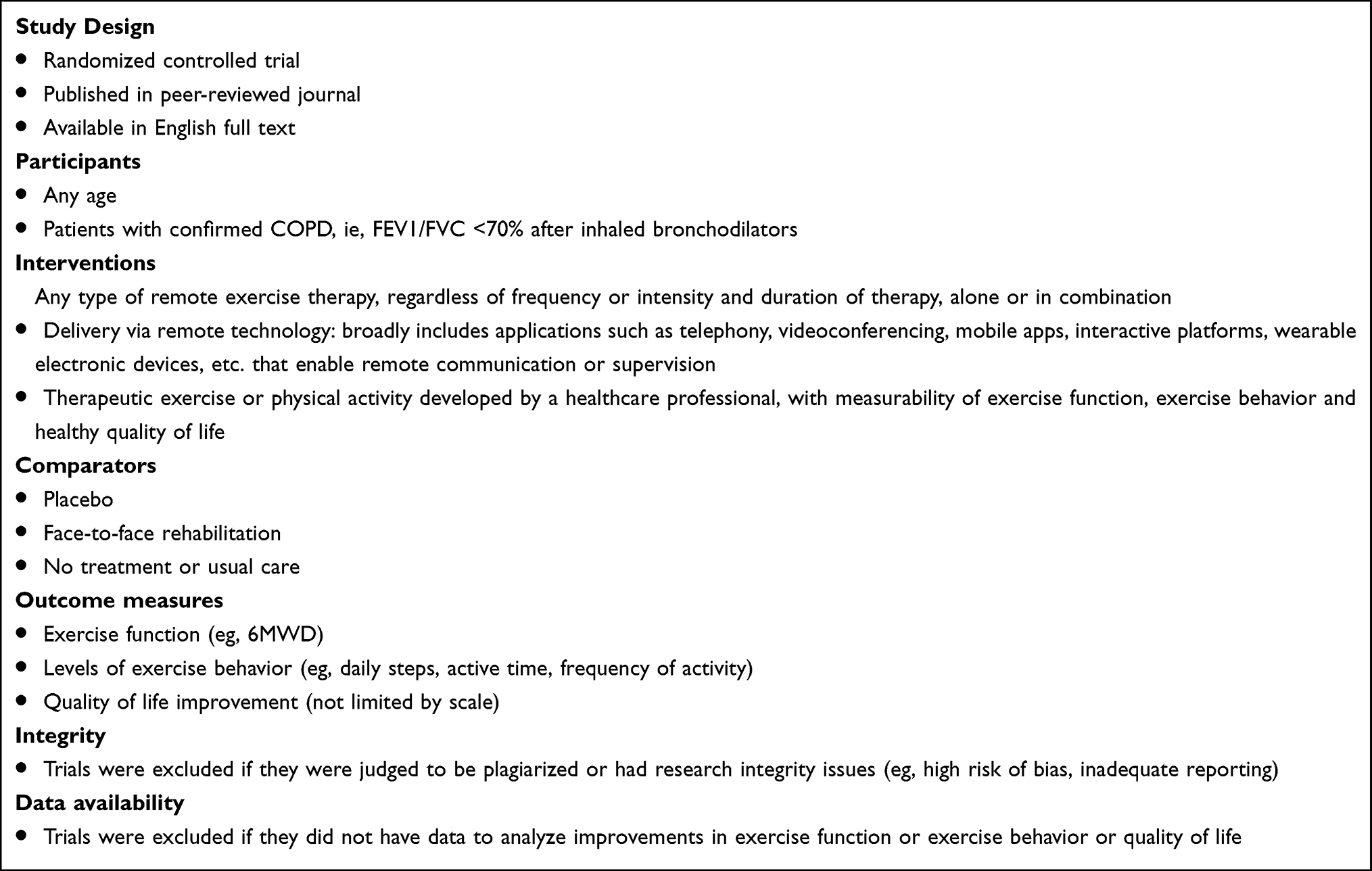 |
Box 1 Systematic Review Selection Criteria, and Additional Criteria for Inclusion and Exclusion in This Network Meta-Analysis |
The inclusion criteria are listed in Box 1, describing the study design, population, intervention, comparator, and outcome characteristics. Studies were eligible for inclusion if the trial intervention involved therapeutic exercise or physical activity prescribed by healthcare professionals and delivered via remote technology, and if outcomes measuring exercise function, exercise behavior, and health-related quality of life were measurable. Studies conducted in English were eligible.
Based on the predetermined criteria, two reviewers (TH, SHP) independently read each title and abstract to initially screen the relevant literature using Endnote 20 software, and then read the full text of the initial screened literature for inclusion and assessed the quality of the literature, respectively. If there was a conflict at any of the above stages, the third or fourth (LXQ) reviewer would join in and discuss and eventually reach a consensus agreement based on the inclusion criteria. The authors of the articles will be contacted by Email if the full-text manuscript is not available or if clarification of aspects of the study is required.
Data Extraction and Risk of Bias Assessment
Two researchers (TH and SHP) independently extracted data from eligible publications, using Excel spreadsheets to extract and store the information. Any missing information was recorded as unclear or not described. Data extracted from each study included the following characteristics: first author’s name, year of publication, country/region, number of participants, male-to-female ratio, mean age (standard deviation), characteristics of the intervention/control measures (including remote technology used, type of exercise program, and behavioral support measures involved), and outcome measures. Five evaluation items using The Cochrane Risk of Bias 2 tool for randomized trials: generation of random sequences; allocation concealment; blinding; completeness of outcome data; and selective reporting and other potential biases. Each domain featured three risk categories: “high risk”, “low risk”, and “unclear”. Studies with all five items rated “low risk” present minimal potential for bias. Studies with some items rated “low risk” present moderate potential for bias. Studies failing to meet any “low risk” criteria present higher potential for bias. Risk of bias plots were generated using RevMan 5.4.1 software.
Data Analysis
Descriptive Analysis
Overall, key study and patient characteristics were summarized using descriptive synthesis and risk of bias assessment. Narrative summaries were provided for studies for which outcome data allowing for NMA were not available (eg, data expressed as median due to skewed distribution, p values, unreported time points).
Network Meta-Analysis
We employed STATA software to conduct the network meta-analysis and constructed a network evidence association diagram to evaluate the impact of interventions on improving outcomes related to exercise function, exercise behavior, and quality of life. The network evidence map assessed both direct (ie, pairwise comparisons) and indirect evidence for each primary outcome. Continuous data variables (mean±standard deviation) were represented as effect sizes using standardized mean differences (SMDs) with their 95% confidence interval (95% CI).
Inconsistency Test
We assessed inconsistencies across all outcome networks (ie, the consistency between direct and indirect evidence). When both direct and indirect comparisons coexist for all interventions, this constitutes a closed loop. Where closed loops exist in the network diagram, we first employed the Design-by-treatment interaction model for global inconsistency testing. If P≥0.05 or I2≤50%, indicating relatively consistent results between direct and indirect comparisons, we analyzed using the consistency model. Conversely, the inconsistency model is applied, supplemented by sensitivity analyses. Secondly, node splitting is employed for local inconsistency testing. Finally, loop inconsistency tests evaluate consistency within closed loops for each outcome measure. A 95% confidence interval for the loop inconsistency factor encompassing zero indicates good consistency between direct and indirect evidence.
Assessment of Cumulative Ranking
We used the area under the Cumulative Ranking probability map (Surface Under the Cumulative Ranking, SUCRA) to rank to present the likelihood of each rehabilitation intervention being the best intervention. Where 0%≤SUCRA≤100%, the larger the SUCRA value, the more effective the intervention.
Sensitivity Analysis
Sensitivity analysis was performed using a deletion-by-deletion method to exclude studies with high risk of bias and missing information. Funnel plots were also drawn to assess small sample effects and possible publication bias.
Results
Research Options
This review conducted a systematic search of various databases to obtain 1155 potentially eligible papers, excluded 977 papers that did not fulfil the study criteria based on the title and abstract, and subsequently read the full text of 178 papers. Of these, 149 articles were excluded for the following reasons: 85 had only study protocols, 26 were conference abstracts or full text was unavailable, 13 did not have relevant outcome metrics, 11 were unable to extract the required data, 9 were repetitively published studies, 4 had comparisons that were not relevant to the topic, and 1 was withdrawn. Finally, a total of 29 literatures were included. The literature screening process is shown in Figure 1.
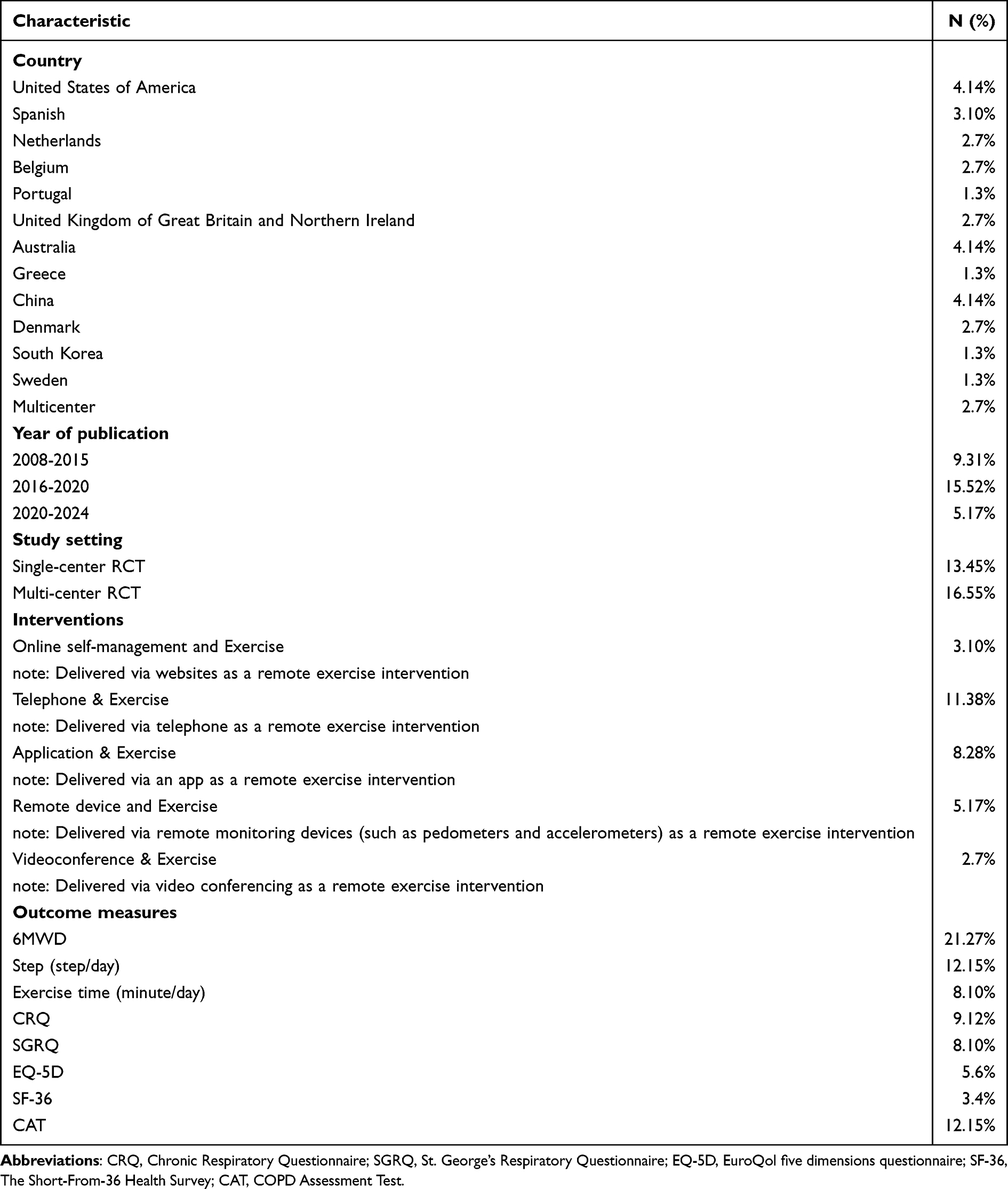 |
Table 1 Summary Characteristics of Included Studies |
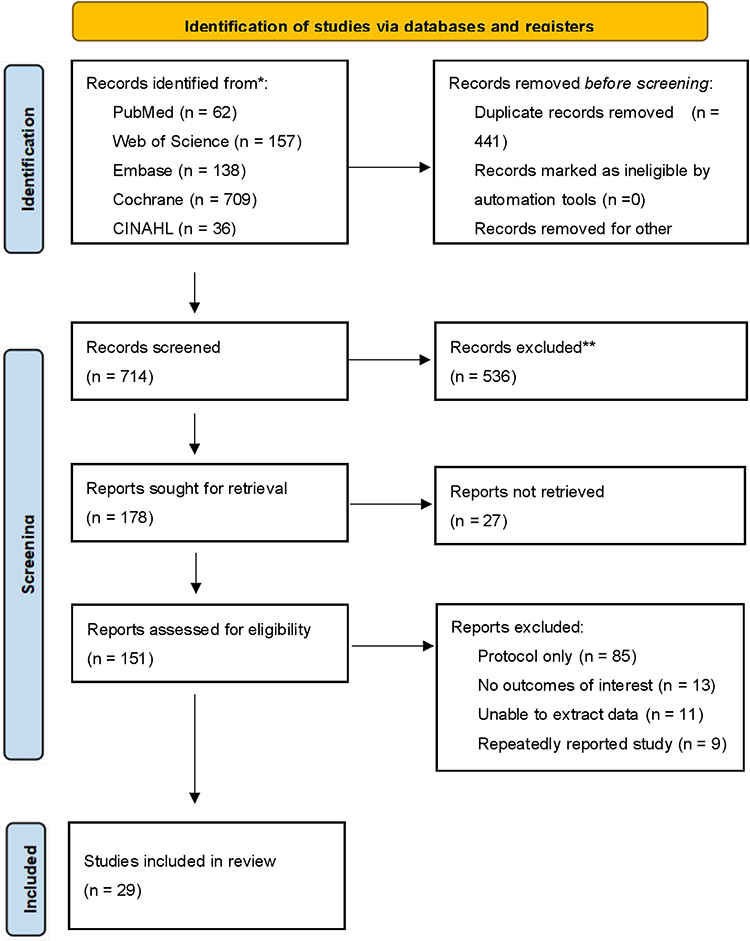 |
Figure 1 Flow of trials through the review. |
Description of Included Trials
Table 1 describes the summary characteristics of the included trials, which were published between 2008 and 2024 and included a total of 3234 participants. Fifteen countries were involved, with the largest number of studies (n=4, 13.8%) conducted in Australia. Overall, there was a predominance of male subjects. The trials included did not incorporate hybrid interventions (remote intervention + face-to-face or two or more remote interventions). Five types of remote exercise interventions were employed: Telephone & Exercise (n=11, 38%), Application & Exercise (n=8, 28%), Remote device and Exercise (n=5, 17%), Online self-management and Exercise (n=3, 10%), and Videoconference & Exercise (n=2, 7%); effect evaluation metrics were categorized into one exercise function (6MWD), two exercise behavioral (steps, exercise time), and five healthy quality of life outcomes (CRQ, SGRQ, EQ-5D, SF-36, and CAT). The summary characteristics of the studies included are presented in Table 2. In addition, we found that all included trials used behavioral aids including: Motivational interviewing, Goal setting, Activity monitor/Pedometer, Motivation & Feedback and Health education, as shown in Table 3.
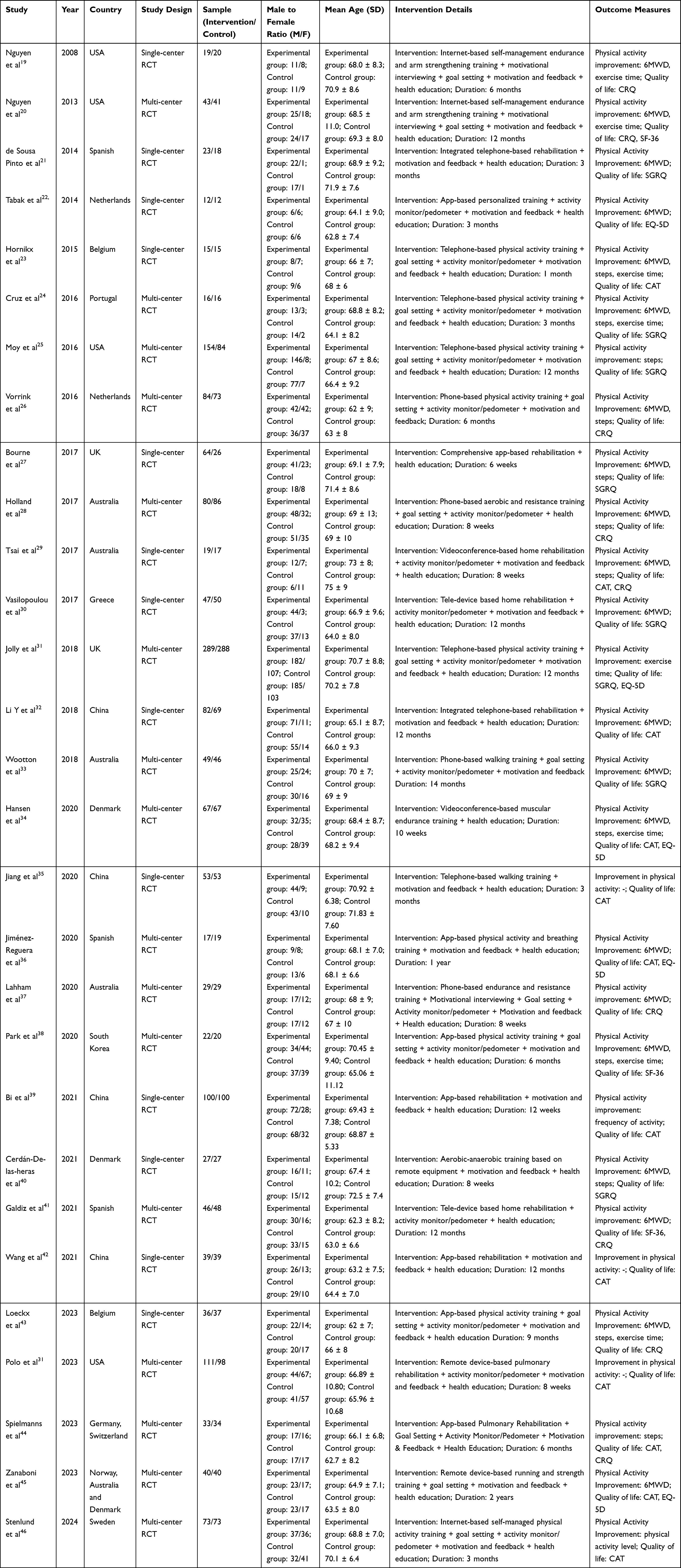 |
Table 2 Basic Characteristics of the Included Studies (n = 29) |
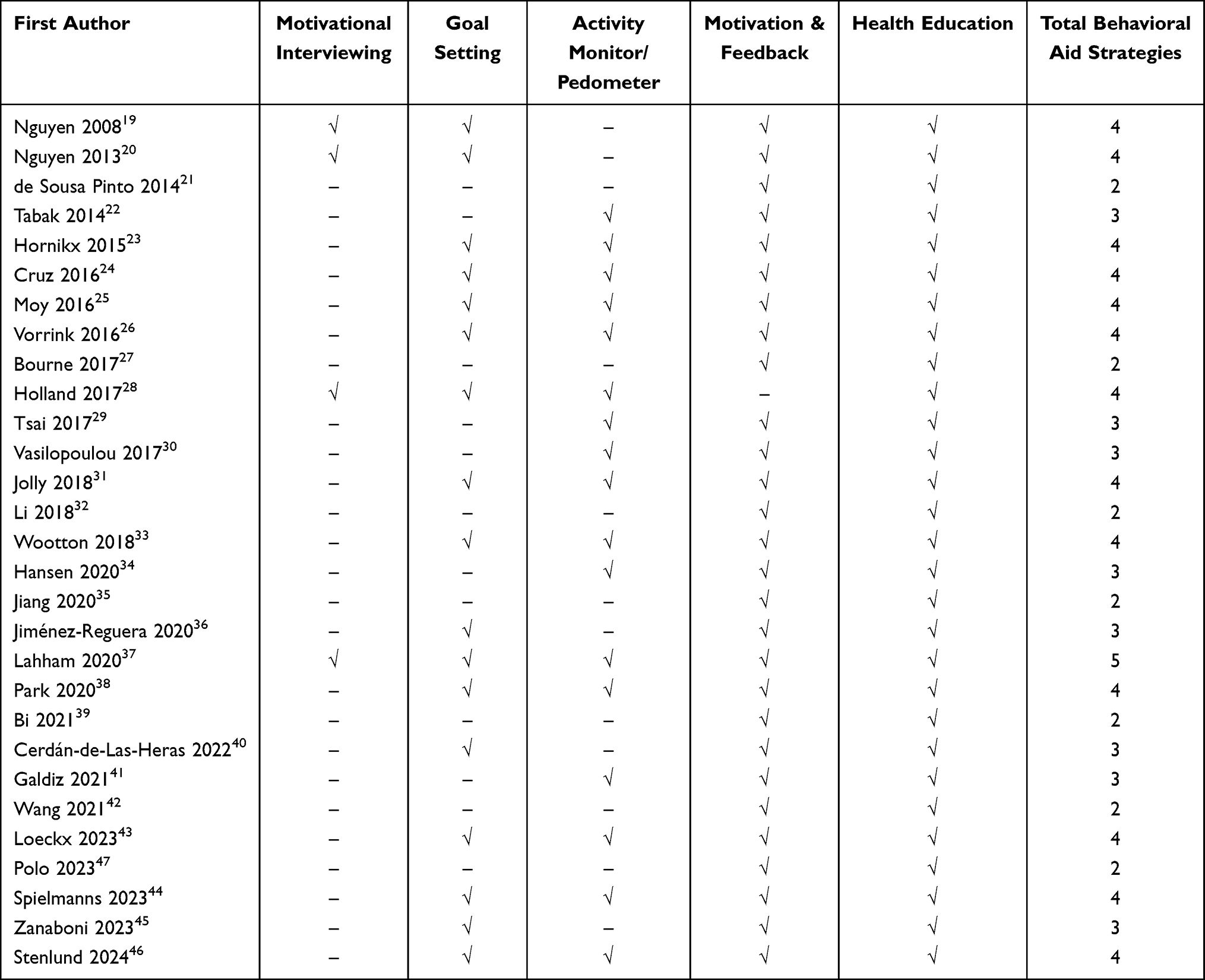 |
Table 3 Behavioral Aids for Telematic Interventions (n = 29) |
Risk of Bias
Of the 29 included trials, 24 reported random sequence generation (random number tables, computers),19,21,22,24,26–31,33–42,44–47 13 reported specific allocation concealment methods (sealed envelopes, blank folders),19,22,24,27,28,31,33,34,36,37,41,42,46 12 blinded outcome assessors,19,26–29,33,34,36,37,40,42,45 and 19 had complete data.20,21,23–25,27–31,34,35,38,40,42,43,45–47 None of the studies reported selectivity, and none mentioned other sources of bias. The results of the risk of bias evaluation are shown in Figures 2 and 3.
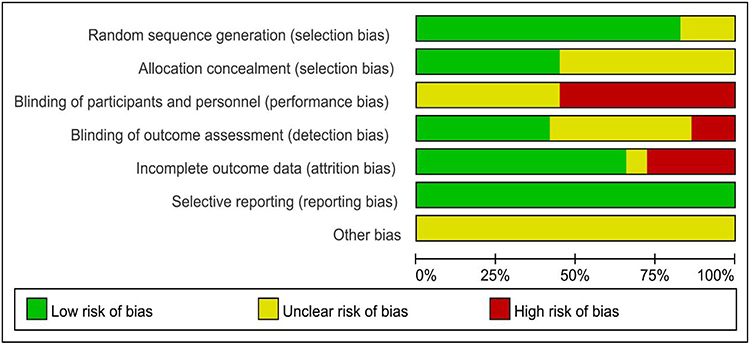 |
Figure 2 Risk of bias of the included studies. |
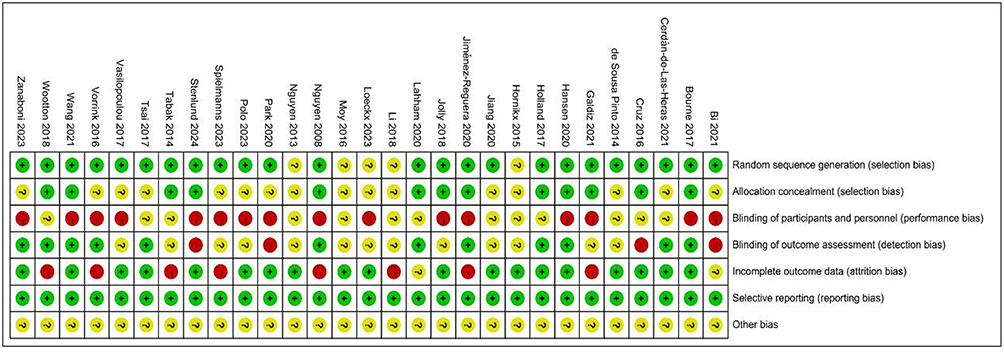 |
Figure 3 Summary of risk of bias of the included studies. Notes: “−” is high risk; “?” is risk unclear; “+” is low risk. |
Network Evidence Map
Network evidence maps are constructed based on different outcome measures. Circles in the diagram represent distinct remote-rehabilitation interventions, with circle size proportional to the study sample size. Connecting lines between circles denote the number of studies comparing these interventions, with thicker lines indicating a greater number of comparative studies. A total of 21 studies19–21,22–24,26–30,32–34,36–38,40,41,43,45 reported exercise function metrics (6MWD), 16 studies19,20,23–26,27–29,31,34,37,38,40,43,44 reported behavioral metrics (steps, exercise time). Nineteen studies21,24,25,27,29–36,39,40,42,44–46,47 reported quality of life outcomes using negative vector scales and 11 studies19,20,22,29,31,34,36,37,43–45 reported quality of life outcomes using positive vector scales, respectively. In the network diagram of 6WMD outcome measures, the circles representing conventional care and telephone intervention are the largest, indicating the highest sample sizes. The thickest line connecting these two groups signifies the greatest number of comparative studies between them. For more details, see Supplementary Figure 1.
Comparative Effectiveness of Types of Remote-Exercise Interventions
Exercise Function (6MWD)
The exercise function indicators included in the study were analyzed, and the nodal analysis model showed P= 0.8920 for the 6MWD indicator; the inconsistency test was also carried out using the node splitting method, and the results showed good consistency (all P-values > 0.05), which indicated that the results of the direct and indirect comparisons were consistent, and therefore the consistency model was used for the analysis. Direct results indicate that in terms of exercise function, encompassing 21 studies and 1,382 participants, Remote device and Exercise (SMD 0.51, 95% CI: 0.10–0.93) demonstrated a significant improvement in exercise function compared with Usual care (P < 0.05), and the two-by-two comparisons of the remaining exercise interventions were not significant (P > 0.05).
Exercise Behavior
For the exercise behavior indicators, the nodal analysis model showed P= 0.5059 for the daily steps indicator and P= 0.4351 for the daily activity time indicator; the inconsistency test was also conducted using the node splitting method and the results showed good agreement (P value > 0.05 for both), which indicated that the results of the direct and indirect comparisons were consistent, and therefore the consistency model was used for the analysis. Direct results indicate that, encompassing 10 studies and 527 participants, Online self-management & Exercise (SMD 0.48, 95% CI: 0.08–0.88) demonstrated a statistically significant improvement in daily step count compared with usual care (P < 0.05), and the two-by-two comparisons for the remaining exercise interventions were not significant (P > 0.05).
Quality of Life
Quality of Healthy Life (symptoms/problems) was analyzed and the nodal analysis model showed a P= 0.6351 for the Quality of Healthy Life indicator; inconsistency test was also conducted using the node splitting method and the results showed good agreement (all P-values > 0.05), which indicates that the results of the direct and indirect comparisons are consistent, so a consistency model was used for the analysis. Direct results indicate that on negative symptom scales, encompassing 19 studies and 2,072 participants, Application & Exercise (SMD −0.67, 95% CI: −1.05 - −0.29) and Telephone & Exercise (SMD −0.57, 95% CI: −0.94 - −0.21) demonstrated greater efficacy than Usual Care in improving patients’ quality of life (P < 0.05). No significant differences were observed in pairwise comparisons between the remaining exercise interventions (P > 0.05).
Quality of life (function/health) was analyzed, and the nodal analysis model showed a quality of life indicator of P = 0.8912; the inconsistency test was also performed using the node splitting method, and the results showed good consistency (all P values > 0.05), which indicated that the results of the direct and indirect comparisons were consistent, and so the consistency model was used for the analysis. Direct results indicate that, in terms of positive scales encompassing 11 studies and 1,084 participants, no exercise intervention demonstrated a statistically significant improvement in quality of life compared with usual care (P > 0.05). Furthermore, pairwise comparisons between the remaining exercise interventions revealed no statistically significant differences (P > 0.05). As shown in Figure 4.
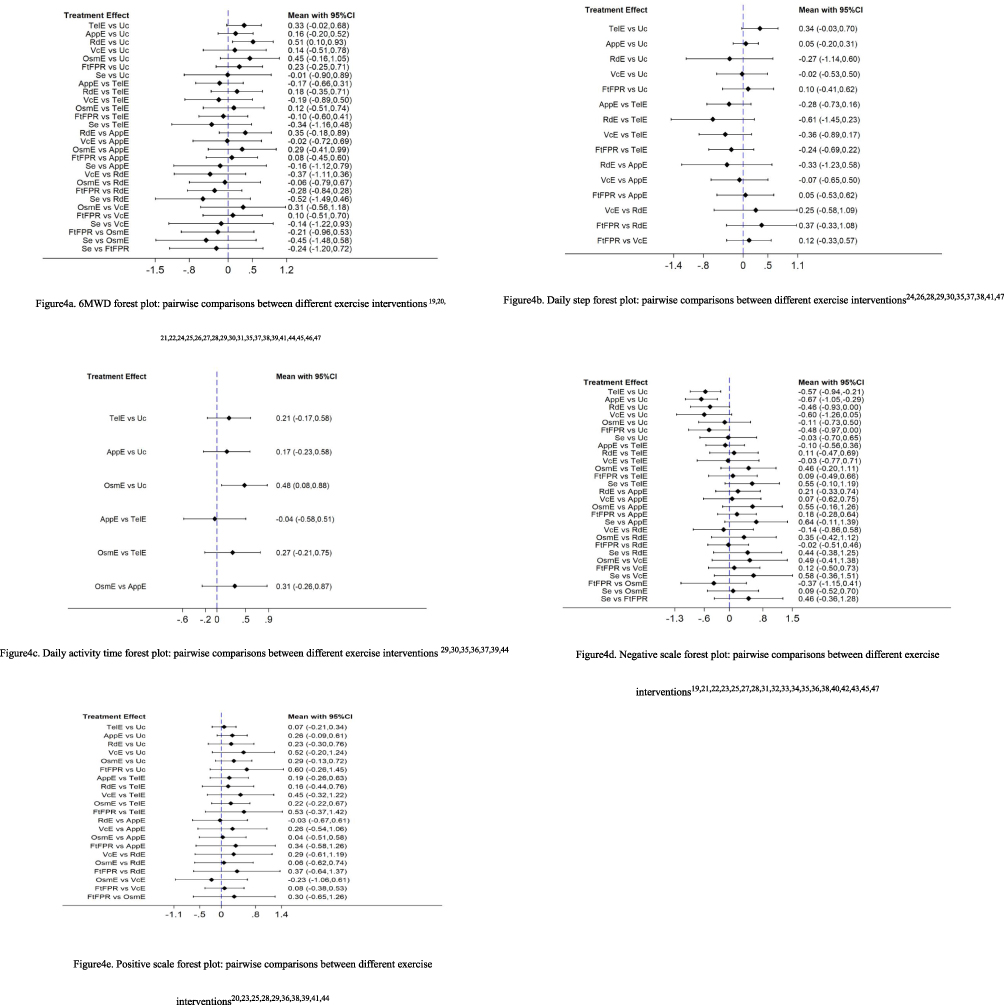 |
Figure 4 Forest plot of direct meta-analysis for various outcome indicators of different exercise interventions. Notes: The horizontal coordinates represent 95% CI and the blue dashed line is the null line; if a short line parallel to the horizontal coordinates in the figure intersects the null line, it means that the result is not significant. |
SUCRA Probability Ranking Results
The SUCRA metric is used to rank the efficacy of each remote-exercise intervention, and the numbers in the graph represent the area under the SUCRA curve, with a larger area indicating a more effective one for that exercise type.
The results showed that the cumulative probability of improvement in exercise function was ranked in order: Remote device and Exercise (81.8%) > Online self-management and Exercise (72.7%) > Telephone & Exercise (63.8%) > Face-to-Face Pulmonary Rehabilitation (51.5%) > Application & Exercise (41.2%) > Videoconference & Exercise (40.1%) > Usual care (18.9%).
The cumulative probability of an increase in exercise behavior (daily step) was ranked in order: Telephone & Exercise (90.7%) > Face-to-Face Pulmonary Rehabilitation (58.4%) > Application & Exercise (51.3%) > Videoconference & Exercise (40.3%) > Usual care (39.1%) > Remote device and Exercise (20.2%); The cumulative probability of an increase in physical activity (daily activity time) was ranked in order: Online self-management and Exercise (90.1%) > Telephone & Exercise (51.1%) > Application & Exercise (47.2%) > Usual care (11.5%).
The cumulative probability of improvement in quality of life (symptoms/problems) was ranked in order: Application & Exercise (81.1%) > Videoconference & Exercise (71.2%) > Telephone & Exercise (70.6%) > Face-to-Face Pulmonary Rehabilitation (58.9%) > Remote device and Exercise (57.4%) > Online self-management and Exercise (27.1%) > Usual care (13.1%); The cumulative probability of improvement in quality of life (functioning/health) is ranked in order: Face-to-Face Pulmonary Rehabilitation (78.0%) > Videoconference & Exercise (72.1%) > Online self-management and Exercise (57.9%) > Application & Exercise (53.5%) > Remote device and Exercise (47.7%) > Telephone & Exercise (26.9%) > Usual care (13.9%). As shown in Figure 5.
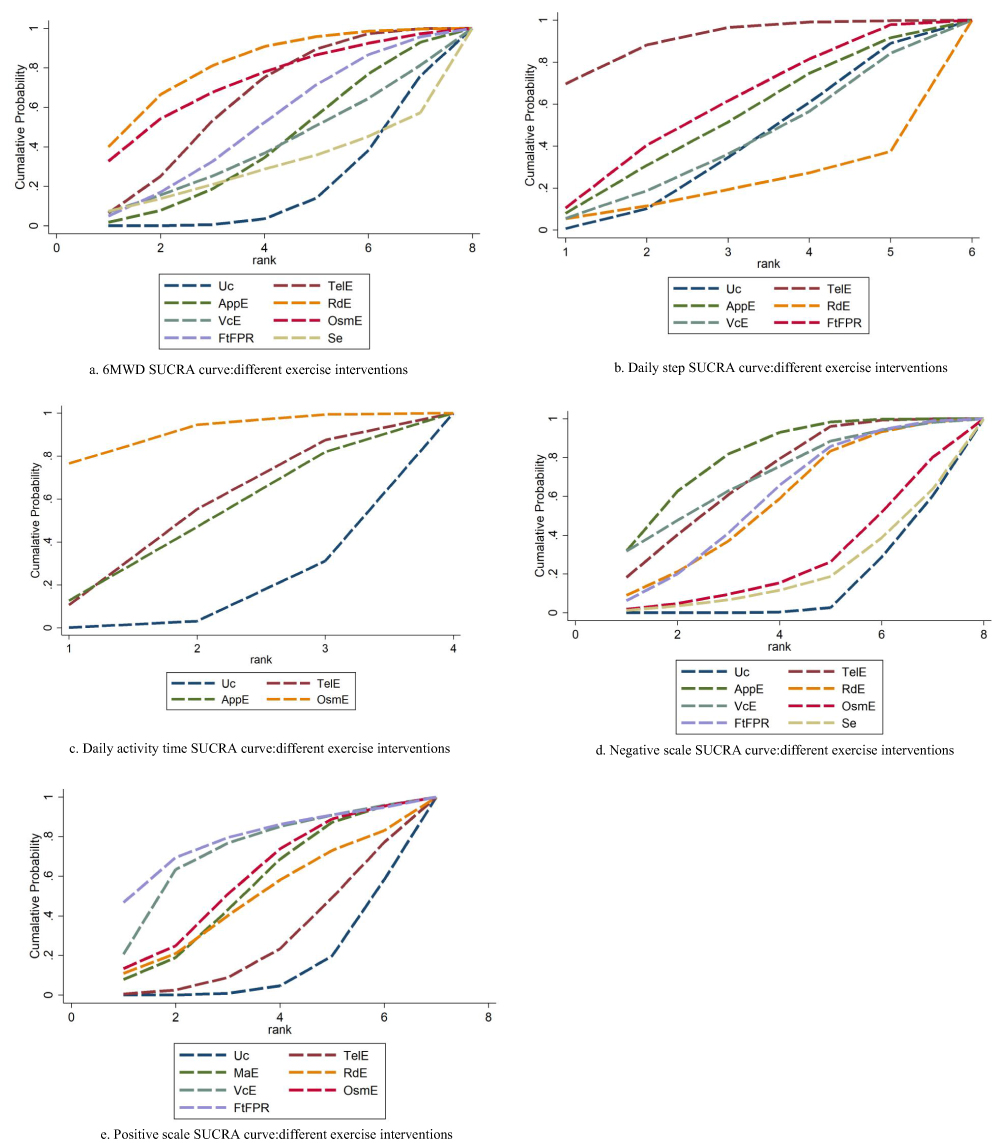 |
Figure 5 Cumulative probability rank of different exercise interventions. Abbreviations: Uc, Usual care; TelE, Telephone & Exercise; AppE, Application & Exercise; RdE, Remote device & Exercise; VcE, Videoconference & Exercise; OsmE, Online self-management & Exercise; FtFPR, Face-to-Face Pulmonary Rehabilitation; Se, Self-exercise. Notes: The area under the fold line represents the level of efficacy of the exercise intervention. The horizontal coordinate is the value of the random variable and the vertical coordinate is the corresponding cumulative probability (%). |
Ring Inconsistency Test Results
The existence of both direct and indirect comparisons for all exercise types is known as 1 closed loop. For exercise function, a total of 7 closed loops were formed in the studies we included, with insufficient factor (IF) ranging from 0.103 to 0.608; for exercise behavior, 1 closed loop was formed for the number of steps per day and the duration of activity, with IF of 0.337 and 0.267, respectively; a total of 5 closed loops were formed for the evaluation of negative quality of life, with IF ranging from 0.079 to 0.722; and 1 closed loop was formed for the evaluation of positive quality of life, with IF of 0.062. The confidence intervals of the above closed loops all contained 0, suggesting that there was no significant inconsistency among the indicators. Results of the inconsistency test for different remote exercise interventions are provided in the Supplementary Table 1.
Meta-Analysis Results of Different Behavioral Aids
Behavioral aids were used in all the included studies. Therefore, Meta-analysis of different behavioral aids was conducted to find effective behavioral aids. The network evidence maps showed that for each outcome indicator, the sample with Goal setting + Activity monitor/Pedometer + Motivation & Feedback + Health education (GAPMFH), Motivation & Feedback + Health education (MFH) in direct comparison with usual care, for more details, see Supplementary Figure 2; overall, local and ring inconsistency tests (except for the absence of a closed ring revealed no significant inconsistencies between indicators, details are provided in the Supplementary Table 2. Meta-analysis results indicate that compared with usual care, Motivation & Feedback + Health education (MFH) demonstrated significant superiority in improving 6-week mean difference (WMD) (20 studies, 1,343 participants) (SMD 0.63, 95% CI: 0.13–1.13) Motivational Interviewing + Goal Setting + Activity Monitor/Pedometer + Health Education (MiGAPH) demonstrated significant superiority in increasing patients’ daily activity duration (10 studies, 527 participants) (SMD 0.59, 95% CI: 0.15–1.02). Motivation & Feedback + Health education (MFH) effectively improved patients’ negative quality of life scores (SMD−0.66, 95% CI: −1.08-−0.25) (16 studies, 1,713 participants). However, none of the behavioral intervention types significantly improved patients’ daily step count or positive quality of life scores, see Figure 6. The SUCRA probability ranking results showed that the behavioral aid with the highest cumulative probability of improving exercise function was Motivation & Feedback + Health education (MFH, 88.3%); the behavioral aids with the highest cumulative probability of increasing the number of steps per day and the duration of activity were both Motivational interviewing + Goal setting + Activity monitor/Pedometer + Health education (MiGAPH), 86.9% and 97.6%, respectively; in terms of quality of life, the behavioral aids with the highest cumulative probability of improvement in both negative and positive scores were Motivation & Feedback + Health education (MFH, 88.3%). Behavioral aids were Motivation & Feedback + Health education (MFH, 87.0%) and Goal setting + Motivation & Feedback + Health education (GMFH, 71.6%) for quality of life, respectively, as shown in Figure 7.
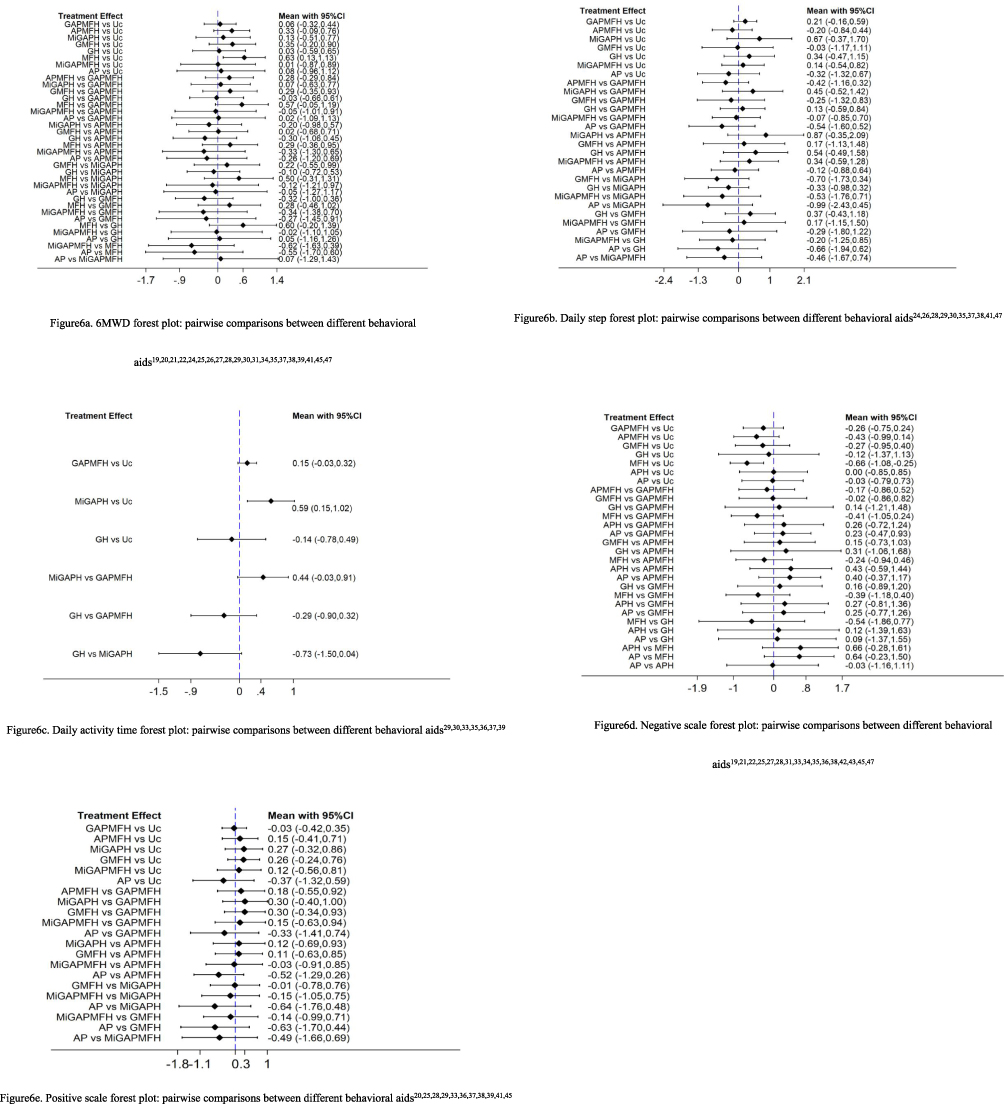 |
Figure 6 Forest plot of direct meta-analysis for various outcome indicators of different behavioral assistance measures. Abbreviations: Uc, Usual care; GAPMFH, Goal setting + Activity monitor/Pedometer + Motivation & Feedback + Health education; APMFH, Activity monitor/Pedometer + Motivation & Feedback + Health education; MiGAPH, Motivational interviewing + Goal setting + Activity monitor/Pedometer + Health education; GMFH, Goal setting + Motivation & Feedback + Health education; GH, Goal setting + Health education; MFH, Motivation & Feedback + Health education; MiGAPMFH, Motivational interviewing + Goal setting + Activity monitor/Pedometer + Motivation & Feedback + Health education; APH, Activity monitor/Pedometer + Health education; AP, Activity monitor/Pedometer. |
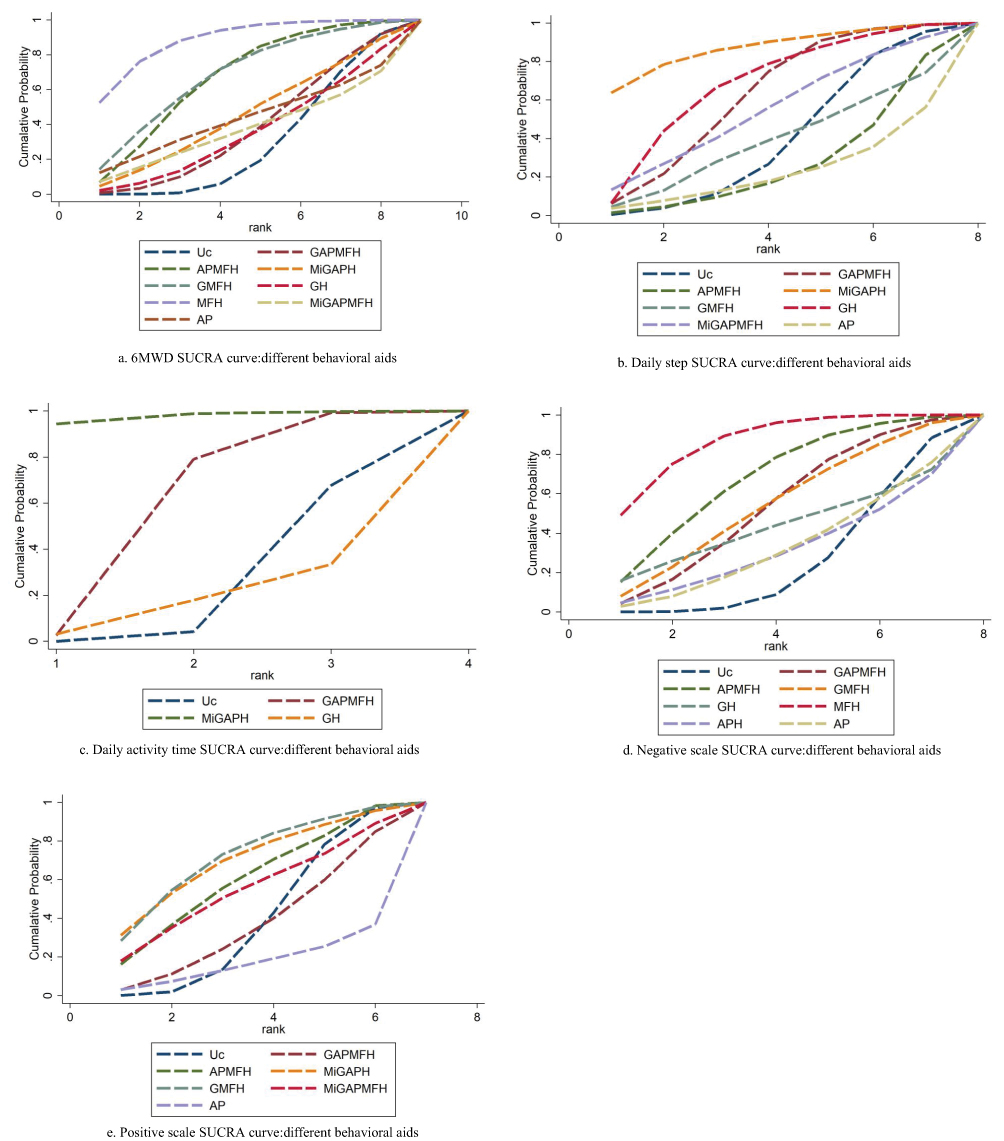 |
Figure 7 Cumulative probability rank of different behavioral aids. Abbreviations: Uc, Usual care; GAPMFH, Goal setting + Activity monitor/Pedometer + Motivation & Feedback + Health education; APMFH, Activity monitor/Pedometer + Motivation & Feedback + Health education; MiGAPH, Motivational interviewing + Goal setting + Activity monitor/Pedometer + Health education; GMFH, Goal setting + Motivation & Feedback + Health education; GH, Goal setting + Health education; MFH, Motivation & Feedback + Health education; MiGAPMFH, Motivational interviewing + Goal setting + Activity monitor/Pedometer + Motivation & Feedback + Health education; APH, Activity monitor/Pedometer + Health education; AP, Activity monitor/Pedometer. Notes: The area under the fold line represents the level of efficacy of behavioral aids. The horizontal coordinate is the value of the random variable and the vertical coordinate is the corresponding cumulative probability (%). |
Publishing Biased Evaluation
Based on the different outcome indicators, we plotted separate funnel plots to detect the presence of publication bias. Among the different remote exercise measures, it can be seen from the funnel plots that the distribution of scattered points within the ranges of exercise function, exercise behavior and quality of life (positive scale) is basically symmetrical, suggesting that there is a small possibility of publication bias and small sample effect in the literature; the funnel plots of quality of life (negative scale) have poor symmetry on both sides and some points are scattered, suggesting that there may be publication bias and small sample effect. See Supplementary Figure 3.
Among the different behavioral aids, the distribution of scattered points within the range of exercise behavior and quality of life (positive scale) was basically symmetrical, suggesting that the literature is less likely to have a publication bias and a small sample effect; the funnel plots of exercise functioning and quality of life (negative scale) had poor symmetry on both sides of the funnel graphs and some scattered points, suggesting that there may be a publication bias and a small sample effect. See Supplementary Figure 4. In addition, we conducted a sensitivity analysis using a stepwise exclusion method for the 29 included studies based on different outcome measures. The results demonstrated that the network meta-analysis findings for the primary outcome (6WMD) and the cumulative ranking results remained largely unchanged after sequentially excluding included studies, indicating a degree of robustness in the results.
Discussion
Different Remote Exercise Interventions
This is believed to be the first systematic review and network meta-analysis to analyze the comparative effectiveness of different remote-exercise interventions for patients with COPD. Overall, all types of remote-exercise interventions demonstrated comparable or more effective outcomes than face-to-face traditional rehabilitation in improving exercise function, exercise behavior levels and quality of life in COPD patients. However, our findings suggest that the magnitude of intervention effect on outcomes varies by outcome indicator. Remote device and Exercise was more effective than other control treatments and other exercise intervention types in improving exercise function. Telephone & Exercise and Online self-management and Exercise were more effective in improving the exercise behavior levels, while Application & Exercise was more helpful in improving quality of life. In addition, our study found that almost all remote-exercise interventions incorporated health education as a behavioral adjunct. Therefore, we considered the impact of behavioral adjuncts on outcomes. The results suggest that the effectiveness of remote-exercise interventions is not only dependent on the choice of technical means but also closely related to the degree of integration of behavioral adjuncts. Motivation and feedback combined with health education was effective in improving exercise capacity and quality of life, whereas the combination of motivational interviewing, goal setting, activity monitors and health education (MiGAPH) performed optimally in exercise behavior promotion. However, the limited number of studies included and potential risks of bias may have reduced our statistical power and test effectiveness.
In contrast to previous systematic review studies15,48 that pooled all telemobility interventions together or included only one teletechnique, our study integrates all available randomized evidence on the effectiveness of telemobility interventions on exercise function, behavior, and quality of life, building on and expanding the current understanding of the effectiveness of telemobility interventions. Integrating direct and indirect comparisons allows us to clarify comparisons between different interventions and rank the effectiveness of different treatments according to their individual outcome components, which provides more useful information for patient and practitioner decision-making.
The main findings support the recommended interventions reported in the most recently published guidelines, which suggest home-based rehabilitation mediated by remote-technology for patients with COPD in order to improve patients’ function and healthy quality of life. Nonetheless, this review provides some guidance on which interventions may be most effective, especially when focusing on different outcome metrics. The 6-minute walk distance is an important metric for assessing exercise function in patients with COPD and is one of the most commonly used outcome evaluation metrics for studies in the category of exercise interventions for patients with COPD.49 Remote device-based exercise interventions had the most significant effect on exercise function improvement in our study, demonstrating the beneficial effect of real-time monitoring. However, most previous studies have only incorporated 6MWD as an indicator of effect evaluation in the motor domain, ignoring the fact that the benefits of motor interventions are predicated on the production of real behaviors. A recent omnibus review50 reported that remote-exercise interventions helped to improve exercise function in patients with COPD but were not significant for improvements in objective physical activity. Our study may explain, in part, that different teletechniques lead to heterogeneity in outcome effects. From the results of our study, Telephone & Exercise and Online self-management and Exercise were optimal in terms of daily steps and daily activity time, respectively.
In addition, the included studies all used a variety of behavioral interventions, including Motivational interviewing, Goal setting, Activity monitor/Pedometer, Motivation & Feedback, and Health education, which we refer to as behavioral adjuncts to distinguish the primary role of the tele-intervention. Each study used at least two or more behavioral adjuncts, which may be one of the reasons for the heterogeneity in the effects of the remote-exercise intervention. Similar to the Paixão et al study,51 our study did not assess the quality of implementation of behavior change interventions, but only their presence or absence. The results of the meta-analysis showed that the addition of behavioral adjuncts was significant in improving outcomes compared with usual care, in particular, the combined behavioral intervention of motivational interviewing combined with goal setting, activity monitoring and health education (MiGAPH) had a high cumulative probability of improvement in daily steps and activity time of 86.9% and 97.6%. However, this is in contrast to the findings of Hanrahan et al52 that behavioral interventions do not improve physical activity in patients with COPD, which did not incorporate remote-technology. The heterogeneity of the two results suggests some synergy between remote technology and behavioral intervention strategies, as the latter did not include consideration of the effects of remote technology.
Clinical Application Guidelines
Clinicians may use the results of our meta-analysis to improve access to digital healthcare for COPD patients. Remote device and Exercise, Telephone & Exercise, Online self-management and Exercise, and Application & Exercise were found to be more effective than other types of tele-exercise in improving exercise function, exercise behavior, and healthy quality of life, respectively. Behavioral aids intervention may have an integrative effect. These two points are critical, especially as evidence grows that tele-digital health is cost-effective and improves access to care.53 Firstly, exercise management teams can use remote device interventions (eg, wearable monitoring devices combined with personalized exercise programs) as the preferred option for COPD patients to improve their exercise capacity, tracking daily exercise and 6WMD in real time and adjusting the intensity of training through remote monitoring systems. Secondly, the design of exercise management programs should be combined with behavioral interventions, such as the development of an official COPD management app that integrates goal-setting, pedometer feedback and health education, or the addition of motivational interviews and goal-setting for patients with poor behavioral levels. In addition, telephone interventions can be a low-cost and efficient alternative for areas where healthcare resources are scarce, eg, rehabilitation staff guiding patients through breathing exercises and walking programmes through regular telephone follow-ups.
Advantages and Limitations
Some of the strengths of this review include a comprehensive systematic review approach that follows the Cochrane Handbook and PRISMA-NMA reporting guidelines.16,54 It used comprehensive searches, robust selection criteria and a detailed data extraction process. The large number of included trials increased generalizability and provided a dense, well-connected network for analysis; differences between protocols and reviews were transparently reported, as well as an assessment of the transferability of all grids, with some value as a guide to clinical practice. However, our findings are constrained by limitations in the quality of included evidence and sample sizes. Due to the risk of bias within studies and the absence of blinding, no trials demonstrated an overall low risk of bias. Furthermore, publication bias may exist for certain outcome measures, such as quality of life (negative scale), thereby reducing the credibility of the available evidence. Secondly, despite exploring different intervention characteristics, unexplained heterogeneity persists due to inadequate descriptions of intervention components (eg, frequency, dosage, duration, and intensity) and the specific definition of remote rehabilitation. Incomplete data precluded comparative analysis of minimum clinically important differences (MCIDs). Future studies should standardize outcome measures to conduct MCID effect analyses, thereby clarifying clinically significant practice effects. It should also be noted that there appears to be an invisible risk of population bias, with most of the included studies coming from high-income countries, and that our results may be confounded with other factors associated with the higher socioeconomic status of these patient groups (eg, healthcare access), potentially affecting the interpretability and generalizability of our results. Future studies should adhere to rigorous reporting guidelines, especially as telemedicine or remote interventions become increasingly important. Standardized methods should be used in describing intervention components for better clarity and replicability.
Conclusions
Our analysis confirms that different types of remote exercise rehabilitation yield varying optimal effects on distinct outcomes such as exercise function, exercise behavior, and quality of life in COPD patients. Furthermore, incorporating behavioral support strategies demonstrates a supplementary effect in improving these outcomes. These findings reaffirm the necessity of personalized rehabilitation Programs. It is recommended that clinicians select remote exercise modalities and behavioral support strategies based on individual characteristics, establish personalized rehabilitation goals, and provide patients with long-term, effective home-based exercise. However, the optimal combination of these two interventions requires further development and validation in future research. It is recommended that subsequent high-quality, multicenter, large-sample RCTs be conducted to verify these findings. Finally, due to limitations in the number of included studies, risk of bias, heterogeneity in intervention combinations, and indirect evidence comparisons, the conclusions of this study should be interpreted and applied with caution.
Abbreviations
COPD, Chronic Obstructive Pulmonary Disease; 6MWD, 6-minute walk test; CRQ, Chronic Respiratory Questionnaire; SGRQ, St. George’s Respiratory Questionnaire; EQ-5D, EuroQol five dimensions questionnaire; SF-36, The Short-From-36 Health Survey; CAT, COPD Assessment Test.
Data Sharing Statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Acknowledgments
The authors extend their gratitude to individuals who have participated in this research. This gratitude is also extended to the Second Affiliated Hospital of Chongqing Medical University, for their unwavering assistance in ensuring the accomplishment of this written work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Development Center for Medical Science & Technology, National Health Commission of the People’s Republic of China (WKZX2023HK0102) and the Chongqing medical scientific research project (Joint project of Chongqing Health Commission and Science and Technology Bureau) (2025ZDXM010). The funder of this study had no role in study design, data collection, data analysis, data interpretation, or writing of the report. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jo YS. Long-term outcome of chronic obstructive pulmonary disease: a review. Tuberc Respir Dis. 2022;85(4):289–301. doi:10.4046/trd.2022.0074
2. Khakban A, Sin DD, FitzGerald JM, et al. The projected epidemic of chronic obstructive pulmonary disease hospitalizations over the next 15 years. A population-based perspective. Am J Respir Crit Care Med. 2017;195(3):287–291. doi:10.1164/rccm.201606-1162PP
3. GOLD. Global Strategy for Prevention, Diagnosis and Management of COPD. 2025. Available from: https://goldcopd.org/2025-gold-report/.
4. Shu CC, Lee JH, Tsai MK, Su TC, Wen CP. The ability of physical activity in reducing mortality risks and cardiovascular loading and in extending life expectancy in patients with COPD. Sci Rep. 2021;11(1):21674. doi:10.1038/s41598-021-00728-2
5. Orme MW, Steiner MC, Morgan MD, et al. 24-hour accelerometry in COPD: exploring physical activity, sedentary behavior, sleep and clinical characteristics. Int J Chron Obstruct Pulmon Dis. 2019;14:419–430. doi:10.2147/COPD.S183029
6. Geidl W, Carl J, Cassar S, et al. Physical activity and sedentary behaviour patterns in 326 persons with COPD before starting a pulmonary rehabilitation: a cluster analysis. J Clin Med. 2019;8(9). doi:10.3390/jcm8091346
7. De Bontridder S, Corhay JL, Haenebalcke C, Fievet F, Etienne I, Vanderhelst E. Correlation of symptoms and physical activity level in chronic obstructive pulmonary disease patients: results from the observational SPACE study. ACTA CLINICA BELGICA. 2022;77(3):671–678. doi:10.1080/17843286.2021.1950419
8. Ichinose M, Yoshiaki M, Takashi M, et al. A non-interventional, cross-sectional study to evaluate factors relating to daily step counts and physical activity in japanese patients with chronic obstructive pulmonary disease: STEP COPD. Int J Chronic Obstr. 2020;15:3385–3396. doi:10.2147/COPD.S277782
9. Pimenta S, Silva CG, Flora S, et al. What motivates patients with COPD to be physically active? A cross-sectional study. J Clin Med. 2021;10(23). doi:10.3390/jcm10235631
10. Global Initiative for Chronic Obstructuive Pulmonary Disease (GOLD). Global Strategy for Diagnosis, Management Prevention of COPD, 2022. Available from: https://goldcopd.org/2022-gold-reports/.
11. Martins SM, Adams R, Rodrigues EM, et al. Living with COPD and its psychological effects on participating in community-based physical activity in Brazil: a qualitative study. Findings from the breathe well group. Npj Primary Care Respiratory Medicine. 2024;34(1):1–10. doi:10.1038/s41533-024-00386-7
12. Ayala-Chauvin M, Chicaiza FA, Acosta-Vargas P, et al. Web-based pulmonary telehabilitation: a systematic review. npj Prim Care Respir Med. 2024;34(1):1–12. doi:10.1038/s41533-024-00396-5
13. Zhuang M, Hassan II, Ahmad WMAW, et al. Effectiveness of digital health interventions for chronic obstructive pulmonary disease: systematic review and meta-analysis. J Medical Internet Re. 2025;27(1):e76323. doi:10.2196/76323
14. Martínez-pozas O, Corbellini C, Cuenca-zaldívar JN, Meléndez-Oliva É, Sinatti P, Sánchez ROMERO. Effectiveness of telerehabilitation versus face-to-face pulmonary rehabilitation on physical function and quality of life in people with post COVID-19 condition: a systematic review and network meta-analysis. Eur J Phys Rehabil Med. 2024;60(5):868–877. doi:10.23736/S1973-9087.24.08540-X
15. Bonnevie T, Smondack P, Elkins M, et al. Advanced telehealth technology improves home-based exercise therapy for people with stable chronic obstructive pulmonary disease: a systematic review. Journal of Physiotherapy. 2021;67(1):27–40. doi:10.1016/j.jphys.2020.12.006
16. Hutton B, Salanti G, Caldwell DM, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. 2015;162(11):777–784. doi:10.7326/M14-2385
17. Prospero. International prospective register of systematic reviews. Available from: https://www.crd.york.ac.uk/PROSPERO/view/CRD420251001560.
18. McGowan J, Sampson M, Lefebvre C. An evidence based checklist for the peer review of electronic search strategies (PRESS EBC). EBLIP. 2010;5(1):149–154. doi:10.18438/B8SG8R
19. Nguyen HQ, Donesky-Cuenco D, Wolpin S, et al. Randomized controlled trial of an internet-based versus face-to-face dyspnea self-management program for patients with chronic obstructive pulmonary disease: pilot study. J Med Internet Res. 2008;10(2):e9. doi:10.2196/jmir.990
20. Nguyen HQ, Donesky D, Reinke LF, et al. Internet-based dyspnea self-management support for patients with chronic obstructive pulmonary disease. J Pain Sympt Manage. 2013;46(1):43–55. doi:10.1016/j.jpainsymman.2012.06.015
21. de Sousa Pinto JM, Martín-Nogueras AM, Calvo-Arenillas JI, Ramos-González J. Clinical benefits of home-based pulmonary rehabilitation in patients with chronic obstructive pulmonary disease. J Cardiopulmonary Rehab Prevent. 2014;34(5):355–359. doi:10.1097/HCR.0000000000000061
22. Tabak M, VanderValk P, Hermens H, Vollenbroek-Hutten M, Brusse-Keizer M. A telehealth program for self-management of COPD exacerbations and promotion of an active lifestyle: a pilot randomized controlled trial. COPD. 2014:935. doi:10.2147/COPD.S60179
23. Hornikx M, Demeyer H, Camillo CA, Janssens W, Troosters T. The effects of a physical activity counseling program after an exacerbation in patients with chronic obstructive pulmonary disease: a randomized controlled pilot study. BMC Pulm Med. 2015;15(1):136. doi:10.1186/s12890-015-0126-8
24. Cruz J, Brooks D, Marques A. Walk2Bactive: a randomised controlled trial of a physical activity-focused behavioural intervention beyond pulmonary rehabilitation in chronic obstructive pulmonary disease. Chron Respir Dis. 2016;13(1):57–66. doi:10.1177/1479972315619574
25. Moy ML, Martinez CH, Kadri R, et al. Long-term effects of an internet-mediated pedometer-based walking program for chronic obstructive pulmonary disease: randomized controlled trial. J Med Internet Res. 2016;18(8):e215. doi:10.2196/jmir.5622
26. Vorrink SNW, Kort HSM, Troosters T, Zanen P, Lammers JWJ. Efficacy of an mHealth intervention to stimulate physical activity in COPD patients after pulmonary rehabilitation. Eur Respir J. 2016;48(4):1019–1029. doi:10.1183/13993003.00083-2016
27. Bourne S, Devos R, North M, et al. Online versus face-to-face pulmonary rehabilitation for patients with chronic obstructive pulmonary disease: randomised controlled trial. BMJ Open. 2017;7(7). doi:10.1136/bmjopen-2016-014580
28. Holland AE, Mahal A, Hill CJ, et al. Home-based rehabilitation for COPD using minimal resources: a randomised, controlled equivalence trial. Thorax. 2017;72(1):
29. Tsai LLY, McNamara RJ, Moddel C, Alison JA, McKenzie DK, McKeough ZJ. Home-based telerehabilitation via real-time videoconferencing improves endurance exercise capacity in patients with COPD: the randomized controlled TeleR study. Respirology. 2017;22(4):699–707. doi:10.1111/resp.12966
30. Vasilopoulou M, Papaioannou AI, Kaltsakas G, et al. Home-based maintenance tele-rehabilitation reduces the risk for acute exacerbations of COPD, hospitalisations and emergency department visits. Eur Respir J. 2017;49(5):1602129. doi:10.1183/13993003.02129-2016
31. Jolly K, Sidhu MS, Hewitt CA, et al. Self management of patients with mild COPD in primary care: randomised controlled trial. BMJ. 2018:
32. Li Y, Feng J, Li Y, Jia W, Qian H. A new pulmonary rehabilitation maintenance strategy through home-visiting and phone contact in COPD. Patient Preference Adherence. 2018;12:
33. Wootton SL, McKeough Z, Clw N, et al. Effect on health-related quality of life of ongoing feedback during a 12-month maintenance walking programme in patients with COPD: a randomized controlled trial. Respirology. 2018;23(1):
34. Hansen H, Bieler T, Beyer N, et al. Supervised pulmonary tele-rehabilitation versus pulmonary rehabilitation in severe COPD: a randomised multicentre trial. Thorax. 2020;75(5):
35. Jiang Y, Liu F, Guo J, et al. Evaluating an intervention program using WeChat for patients with chronic obstructive pulmonary disease: randomized controlled trial. J Medical Internet Res. 2020;22(4):e17089. doi:10.2196/17089
36. Jiménez-Reguera B, Maroto López E, Fitch S, et al. Development and preliminary evaluation of the effects of an mHealth web-based platform (HappyAir) on adherence to a maintenance program after pulmonary rehabilitation in patients with chronic obstructive pulmonary disease: randomized controlled trial. JMIR mHealth and uHealth. 2020;8(7):e18465. doi:10.2196/18465
37. Lahham A, McDonald CF, Moore R, et al. The impact of home-based pulmonary rehabilitation on people with mild chronic obstructive pulmonary disease: a randomised controlled trial. Clin Respiratory J. 2020;14(4):335–344. doi:10.1111/crj.13138
38. Park SK, Bang CH, Lee SH. Evaluating the effect of a smartphone app-based self-management program for people with COPD: a randomized controlled trial. Appl Nurs Res. 2020;52:1. doi:10.1016/j.apnr.2020.151231
39. Bi J, Yang W, Hao P, et al. WeChat as a platform for baduanjin intervention in patients with stable chronic obstructive pulmonary disease in China: retrospective randomized controlled trial. JMIR mHealth and uHealth. 2021;9(2):e23548. doi:10.2196/23548
40. Cerdán-de-las-heras J, Balbino F, Løkke A, Catalán-Matamoros D, Hilberg O, Bendstrup E. Effect of a new tele-rehabilitation program versus standard rehabilitation in patients with chronic obstructive pulmonary disease. J Clin Med. 2022;11(1). doi:10.3390/jcm11010011
41. Galdiz JB, Gómez A, Rodriguez D, et al. Telerehabilitation programme as a maintenance strategy for COPD patients: a 12-month randomized clinical trial. Archivos Bronconeumologia. 2021;57(3):
42. Wang L, Guo Y, Wang M, Zhao Y. A mobile health application to support self-management in patients with chronic obstructive pulmonary disease: a randomised controlled trial. Clin rehabilitat. 2021;35(1):90–101. doi:10.1177/0269215520946931
43. Loeckx M, Rodrigues FM, Blondeel A, et al. Sustaining training effects through physical activity coaching (STEP): a randomized controlled trial. Int J Behav Nutr Phys Act. 2023;20(1):1–11. doi:10.1186/s12966-023-01519-w
44. Spielmanns M, Gloeckl R, Jarosch I, et al. Using a smartphone application maintains physical activity following pulmonary rehabilitation in patients with COPD: a randomised controlled trial. Thorax. 2023;78(5):442–450. doi:10.1136/thoraxjnl-2021-218338
45. Zanaboni P, Dinesen B, Hoaas H, et al. Long-term telerehabilitation or unsupervised training at home for patients with chronic obstructive pulmonary disease a randomized controlled trial. Am J Respir Crit Care Med. 2023;207(7):865–875. doi:10.1164/rccm.202204-0643OC
46. Stenlund T, Karlsson Å, Liv P, Nyberg A, Wadell K. Short-term effects on physical activity level with web-based self-management support in people with COPD: a randomised controlled trial. npj Prim Care Respir Med. 2024;34(1):32. doi:10.1038/s41533-024-00394-7
47. Polo J, Basile MJ, Zhang M, et al. Application of the RE-AIM framework to evaluate the implementation of telehealth pulmonary rehabilitation in a randomized controlled trial among african-American and hispanic patients with advanced stage chronic obstructive pulmonary disease. BMC Health Serv Res. 2023;23(1):515. doi:10.1186/s12913-023-09492-7
48. Zhang Y, Zhao Y, Jiang X, et al. Telehealth approaches for improving depression and anxiety among patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. General Hospital Psychiatry. 2025;92:28–35. doi:10.1016/j.genhosppsych.2024.12.009
49. Cox NS, McDonald C, Burge AT, Hill CJ, Bondarenko J, Holland AE. Comparison of Clinically Meaningful Improvements After Center-Based and Home-Based Telerehabilitation in People With COPD. CHEST. 2025;167(4):1003–1011. doi:10.1016/j.chest.2024.11.001
50. Koh JH, Chong LCY, Koh GCH, Tyagi S. Telemedical interventions for chronic obstructive pulmonary disease management: umbrella review. J Medical Internet Re. 2023;25(1):e33185. doi:10.2196/33185
51. Paixão C, Rocha V, Brooks D, Marques A. Unsupervised physical activity interventions for people with COPD: a systematic review and meta-analysis. Pulmonology. 2024;30(1):53–67. doi:10.1016/j.pulmoe.2022.01.007
52. Hanrahan C, Broderick J, O’Connor TM, McVeigh JG. Behaviour change interventions for physical activity in adults with chronic obstructive pulmonary disease; A systematic review and meta-analysis. Respiratory Medicine and Research. 2024;85:101068. doi:10.1016/j.resmer.2023.101068
53. Russo JE, McCool RR, Davies L. VA telemedicine: an analysis of cost and time savings. Telemed E-Health. 2016;22(3):209–215. doi:10.1089/tmj.2015.0055
54. Shuster JJ. Review: cochrane handbook for systematic reviews for interventions, version 5.1.0, published 3/2011. In: Julian PT, Sally G, editors. Research Synthesis Methods. 2011;Vol. 2:126–130. doi:10.1002/jrsm.38
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Exercise Interventions on Health-Related Quality of Life in Patients with Fibromyalgia Syndrome: A Systematic Review and Network Meta-Analysis
Zhang KD, Wang LY, Zhang ZH, Zhang DX, Lin XW, Meng T, Qi F
Journal of Pain Research 2022, 15:3639-3656
Published Date: 22 November 2022
Effects of Music, Massage, Exercise, or Acupuncture in the Treatment of Depression Among College Students: A Network Meta-Analysis
Li FB, Lu P, Wu HT, Wang MH, Wang JD
Neuropsychiatric Disease and Treatment 2023, 19:1725-1739
Published Date: 1 August 2023
Effects of Home-Based Training with Internet Telehealth Guidance in COPD Patients Entering Pulmonary Rehabilitation: A Systematic Review
Hartman M, Mináriková J, Batalik L, Pepera G, Su JJ, Formiga MF, Cahalin L, Dosbaba F
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2305-2319
Published Date: 19 October 2023
Addressing Barriers to Chronic Obstructive Pulmonary Disease (COPD) Care: Three Innovative Evidence-Based Approaches: A Review
Siu DCH, Gafni-Lachter L
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:331-341
Published Date: 1 February 2024
Comparative Efficacy of Nutritional Supplements in Modulating Lung Function and Exercise Capacity in COPD Patients: A Network Meta-Analysis
Zeng Y, He T, Ma X, Guo Q, Zhang J
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1525-1541
Published Date: 17 May 2025