Back to Journals » Advances in Medical Education and Practice » Volume 8
What millennial medical students say about flipped learning
Authors Pettit RK ![]() , McCoy L
, McCoy L ![]() , Kinney M
, Kinney M ![]()
Received 13 April 2017
Accepted for publication 26 May 2017
Published 20 July 2017 Volume 2017:8 Pages 487—497
DOI https://doi.org/10.2147/AMEP.S139569
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Robin K Pettit, Lise McCoy, Marjorie Kinney
School of Osteopathic Medicine in Arizona, A. T. Still University, Mesa, AZ, USA
Abstract: Flipped instruction is gaining popularity in medical schools, but there are unanswered questions such as the optimum amount of the curriculum to flip and whether flipped sessions should be mandatory. We were in a unique position to evaluate feedback from first-year medical students who had experienced both flipped and lecture-based courses during their first semester of medical school. A key finding was that the students preferred a variety of different learning formats over an “all or nothing” learning format. Learning format preferences did not necessarily align with perceptions of which format led to better course exam performance. Nearly 70% of respondents wanted to make their own decisions regarding attendance. Candid responses to open-ended survey prompts reflected millennial preferences for choice, flexibility, efficiency, and the ability to control the pace of their learning, providing insight to guide curricular improvements.
Keywords: flipped classroom, mandatory attendance, medical education, lecture-based, variety
A Letter to the Editor has been received and published for this article.
A Letter to the Editor has been received and published for this article.
Introduction
Most of today’s medical students are millennial or Generation Y learners.1 Millennials expect choice, flexibility, speed, and efficiency.2 They are usually attentive learners if the format is on their own terms,3 and they can control the pace, sequence, and content.4 Millennials are technology savvy and often prefer to learn by trial and error5 and by doing,4 both major components of the flipped classroom.6
In a flipped classroom, typical lecture and homework elements are reversed; recorded lectures, vodcasts (video podcasts), or readings are viewed by students prior to class, while in-class time is devoted to more student-centered activities.6 Various medical schools have reported their experiences in flipping courses, disciplines, and even entire curricula.7–13 While other medical schools have compared student satisfaction with flipped instruction to cohorts from previous years who experienced traditional instruction,7,11 we had the ideal environment to obtain input regarding both strategies from a single cohort. This cohort experienced a pilot flipped course followed by four traditional courses in their first semester of medical school.
Evaluation of instructional methods should address learner beliefs and preferences.14,15 With this in mind, the aim of this study was to identify stakeholder preferences prior to curricular changes, with the goal of increasing opportunities for student learning. The following research questions were posed: Do first-year medical students (MS1s) prefer flipped or lecture-based formats or a combination of approaches? Which format do they think helps them learn better? What are students’ obstacles to mandatory attendance for flipped activities? Are there additional teaching strategies that would aid their learning styles?
Methods
Participants and setting
The first course of the year for the class of 2019 (MS1s) was a pilot 3-week anatomy course, Basic Structural Foundations, in which 75% of the content was flipped and the other 25% was lecture-based with embedded activities. For flipped sessions, students viewed vodcasts containing interactive quizzes prior to coming to class for non-mandatory practice activities. The next four courses were lecture-based, ~70% of these with built-in activities, and a small percent (5%) flipped with vodcasts. Activities for flipped sessions and lecture-based sessions varied widely, from drawing anatomical structures to games to case presentations (McCoy et al, manuscript in preparation).
Development of the survey instrument
An original, four-item, interactive, electronic Qualtrics™ survey (Figure S1) was used to gather student feedback on flipped learning. Two questions at the beginning of the survey addressed age range and gender.
Data collection
MS1s were surveyed in January 2016 after completing the five courses described earlier. Survey data collection involved an email solicitation containing a clickable link to the online survey. Survey participation was voluntary and anonymous, and there were no rewards offered for completing the survey. Completion of the survey was deemed consent. The A. T. Still University Institutional Review Board (IRB) deemed the study exempt from IRB reporting requirements for human subjects research because no collected data associated directly through identifiers linked to participants and was conducted via anonymous surveys.
Data analysis
We used open- and axial coding16 to analyze students’ responses to open-ended survey prompts.
Results
Survey response rate and demographics
A total of 104 students (91.0% response rate) participated in the survey. There were 54 male and 50 female respondents (65 aged 23–25 years, 31 aged 26–30 years, 7 aged 31–35 years, and 1 aged 37 years).
Do MS1s prefer flipped, lecture-based formats or a combination of approaches?
A major unanswered question for educators implementing the flipped method is the optimum amount of the curriculum to flip. We probed this topic with the following interactive survey question: “Slide the scale to indicate your preferred large group format”. The preferred large group format for 18% of respondents (n=94) was 50% flipped/50% lecture based (Figure 1). There was tremendous variation in preferred pedagogical approach for the rest of the students. Indeed, the histogram in Figure 1 shows a peak at 50% flipped/50% lecture based, with the remaining responses distributed almost equally on either side.
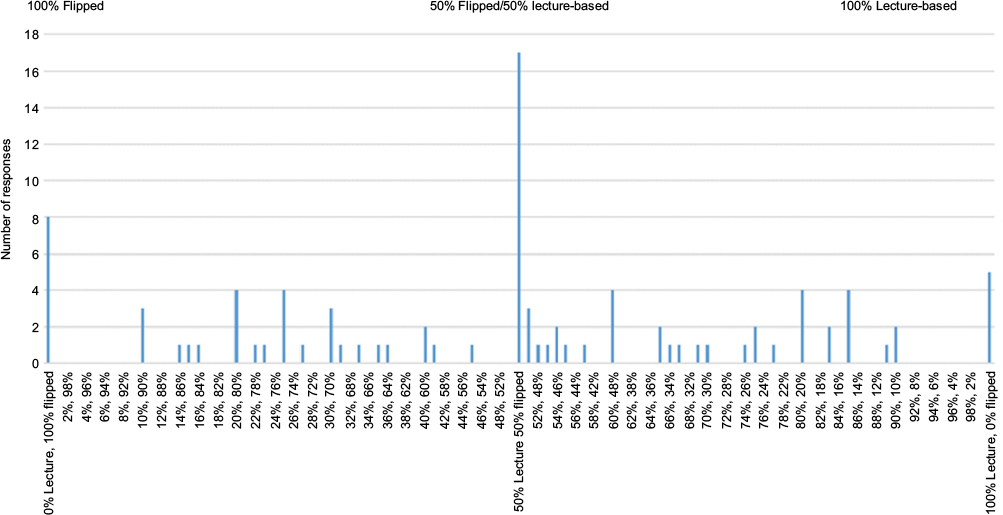 | Figure 1 Summary of student responses to the prompt, “Slide the scale to indicate your preferred large group format. Slide the dial to any % flipped, from 0% to 100%.” Notes: Flipped = typical lecture and homework elements of a course are reversed; video lectures are viewed by students at home before the class session, while in-class time is devoted to exercises, projects, or discussions (Association of American Medical Colleges, 2013). Lecture-based = lectures with activities built into some presentations. |
Twenty students provided optional comments regarding their preferred large group format. When these comments were categorized using open and axial coding,16 six key themes emerged: Pace, Organization, Discipline-specific, Schedule/Echo360™ (lecture capture technology), Suggestions to enhance lecture-based with activities, and Independent study (Table 1). Some comments reflected perceived drawbacks to the flipped method in terms of Pace and Organization. For example, one comment exemplified the millennial desire to control the pace of their learning: “People work at different paces, and flipped classrooms encourage rushed learning, especially when people blurt out answers, it makes you feel behind and inadequate” (theme Pace). Comments that are coded with Discipline-specific and Schedule/Echo360 provided suggestions for selective use of the flipped method and illustrate the millennial preference to control the content and sequence of their learning, including “This really depends on the subject matter. For me, I like flipped for anatomy and micro courses as there is simply a bunch to memorize and the podcasts/vodcasts do a good job of this tedious stuff and then in class activities for what we learned. However, courses like physiology, biochemistry, genetics, I prefer regular lectures given in class” (theme Discipline-specific) and “Enjoy flipped classroom, however would prefer if they occur earlier in the week so there is enough time over the weekend to prepare for those classes” (theme Schedule/Echo360). Three comments that are coded with the theme Suggestions to enhance lecture-based with activities were supportive of preview videos (short vodcasts on basic concepts), which were provided in advance of some biochemistry and genetics lectures. A few students indicated their preference for other methods of receiving information (theme Independent study), including reading.
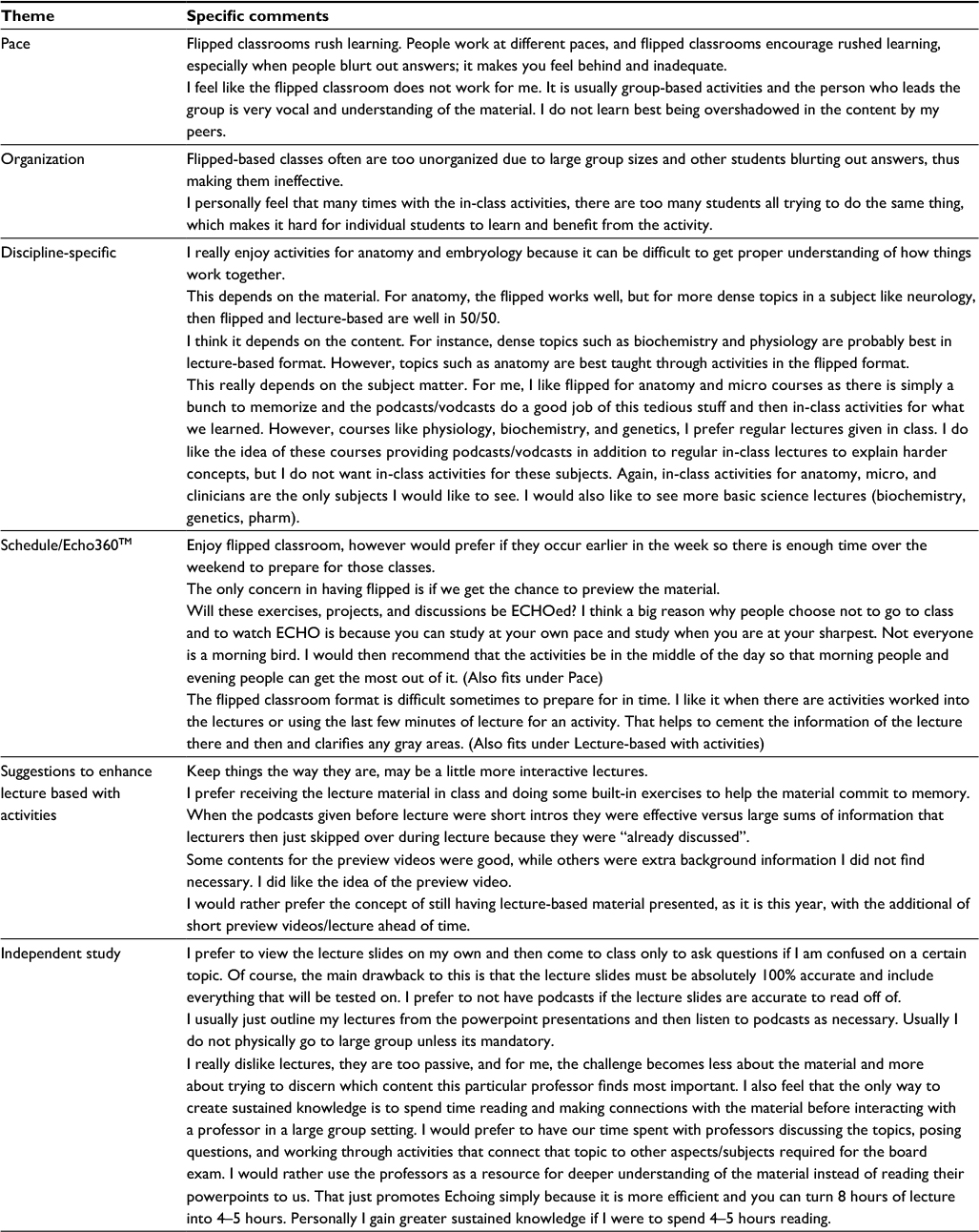 | Table 1 Summary of student responses to optional comments regarding preferred large group format Note: Echo refers to Echo360TM lecture capture technology. |
Which pedagogical format do MS1s think helps them learn better?
The follow-up survey prompt was “Best learning format. Disregarding your preferred large group format above, which of these methods leads to better course exam performance for you?” Of the 17 students who selected 50% lecture/50% flipped as their preferred large group format, six thought that flipped formats led to better course exam performance, five thought that lecture led to better course exam performance, and six selected “other”, explaining that either a combination or some alternate method (eg, study groups) worked best. For the remaining students, ie, those who selected a combination other than 50% lecture/50% flipped, 75.9% perceived that their selected method led to better exam performance, 19% perceived that the opposite of their preferred modality led to better exam performance, and 5.1% chose “other”, explaining that either a combination or some alternate method led to better exam performance.
What are MS1 obstacles to mandatory attendance for flipped activities?
Another unanswered question regarding flipped learning is whether in-class activities should be mandatory. When the preclinical curriculum was flipped at one medical school, student attendance and engagement were lower than expected,13 which was partially attributed to non-mandatory attendance.17 Our medical school does not currently require attendance for lecture-based and flipped sessions, but lectures are recorded via lecture capture.
In this study, 68.7% of respondents thought that in-class practice activities for flipped sessions should be non-mandatory. Their responses to the follow-up prompt, “Please explain your choice” coded into seven key themes: Learning style, Attitude/Preferred learning conditions, Not efficient, Choice, Lack of preparation/time, Situation-dependent, and Pace (Table 2). Many of these themes and associated comments aligned with millennial expectations for choice, flexibility, efficiency, and the ability to control the pace of their learning.2 For example, the millennial desire for choice was exemplified by the comment “People should have the choice if they want to use in-class activities or their own activities to strengthen their understanding of material” (theme Choice). The millennial desire to control the pace of their learning was exemplified by the comment “I like practice activities but I do sometimes feel like I take a backseat in group work. Other people come up with answers and I feel like I do not have as much time to work through problems on my own” (theme Pace). Two enlightening comments under the theme Attitude/Preferred learning conditions were “When people are required to attend but do not actually want to be there, it ruins it for those of us who do want to attend” and “I like when it is less crowded.”
 | Table 2 Summary of student responses to the open-ended prompt, “Please explain your choice”, that followed “For flipped sessions, should in-class practice activities be mandatory?” Notes: aThese comments were from students who selected non-mandatory. Echo refers to Echo360TM lecture capture technology. Parentheses refer to the number of additional similar comments obtained from respondents. |
Nearly one-third of respondents (31.3%) indicated that flipped learning sessions should be mandatory. Their responses to the follow-up prompt “Please explain your choice” coded into six key themes: Motivation to attend, Motivation to stay on top of material, Application of knowledge, Promotes learning, Activity enhanced with increased participation, and Situation-dependent (Table 3). Motivation to attend, Motivation to stay on top of material, and Situation-dependent were the most common themes. An unexpected comment that was coded with Motivation to attend was “Non-mandatory makes the material feel unnecessary.” Other valuable perspectives included “For many activities having more participants makes the activity more enriching (such as competitive games)” (theme Activity enhanced with increased participation). Well-structured activities, a critical component of a successful flipped class, were important to both group of students, those who supported non-mandatory attendance (Table 2, theme Situation-dependent) and those who supported mandatory attendance (Table 3, theme Situation-dependent).
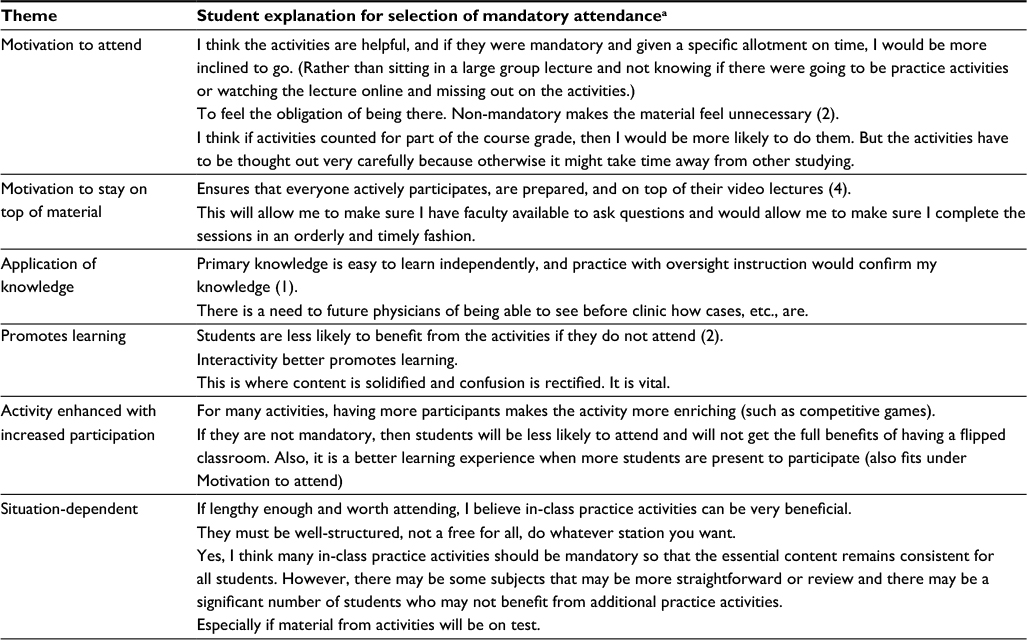 | Table 3 Summary of student responses to the open-ended prompt, “Please explain your choice”, that followed “For flipped sessions, should in-class practice activities be mandatory?” Notes: aThese comments were from students who selected mandatory. Parentheses refer to the number of additional similar comments obtained from respondents. |
Are there additional teaching strategies that would aid their learning styles?
In response to the prompt, “Are there additional teaching and learning strategies that would aid your learning style?”, 11 categories emerged: Incorporation of more practice questions, including clicker questions (16% of respondents); Larger formative quizzes (12% of respondents); Review sessions (4% of respondents); Cumulative exams (2% of respondents); Independent study (6% of respondents); Group study (2% of respondents); Vodcast transcripts (4% of respondents); Board preparation including professors “referencing First Aid pages” (4% of respondents); Inclusion of external vodcast sources (4% of respondents); Mandatory individual small group preparation so that students “can rip through as many cases as we can in the time given” (2% of respondents); and Large group strategies including “organized PowerPoints”, “tons of examples”, “games”, “more models”, “connecting lecture material”, “small groups where we draw physiologic processes with peers to demonstrate our understanding”, and “presentations that touch on a variety of learning styles” (44% of respondents).
Discussion
While student preference does not necessarily equate to what approach is best for student learning, millennials are more likely to be attentive learners if the format is on their own terms.3 In addition, health science student engagement has been shown to positively influence academic achievement.18 As such, stakeholder feedback regarding the two most implemented pedagogical approaches (flipped or lecture-based), including student suggestions for optimizing them, will be considered during curricular improvements.
One of the most surprising results was the relatively large number of students who preferred >50% lecture-based classes. This finding was unexpected for several reasons: the high ratings MS1s gave the pilot flipped course, and millennial preferences for collaborative learning1 and learning by doing.4 These student preferences may have been influenced by the fact that most lectures had some active learning component or that lecture was perceived to be more efficient than the flipped method.19 A small percent of the respondents wanted 100% lecture, a finding that other medical schools have reported.7,11 In addition to the insights provided by our students, possible explanations for lecture preference include undergraduate experience, rock concert “event-ness” making the material memorable,20 the auditory-dominant learning mode of high-risk medical students,21 and students’ perceived misalignments between active learning and national board exams.19 Methods to engage students with a preference for lecture should be investigated, including those suggested by our students under Large group strategies (“Results” section).
Another unexpected result was that large group learning format preference did not always align with perceptions of which format led to better course exam performance. Rigorous studies are needed to determine if discrepancies between preferred learning format and actual outcomes are significant.
Student attendance requirements are the subject of ongoing debate in the medical education community. The availability of lecture capture technology has increased the number of students who choose not to attend class. For students in this study, obstacles to mandatory attendance were largely focused on choice, flexibility, speed, efficiency, and control of the format and pace of their learning; all well-known millennial expectations.2–4 While our faculty discuss the merits and drawbacks of particular attendance policies, we are incorporating MS1 suggestions to make flipped sessions efficient, high yield, and of broad appeal, and are providing enough time in the curriculum for students to prepare for these sessions. The hope is that these efforts will motivate students to attend and potentially increase their learning.
Moffett22 suggested that a flipped learning approach does not have to be “all or nothing,” and only a minority of our students preferred all or nothing. In fact, the range of individual preferences for pedagogical approach was striking. Millennials were raised in an entertainment-focused, multimedia environment; as a result, they have a low tolerance for boredom.23 Lack of pedagogical variety has the potential to cause boredom and to negatively impact students who do not perceive that they learn with the pedagogical method being implemented. In this study, the need for faculty to accommodate varied learning styles was evident throughout survey responses, lending further support to the important role of variety in the medical school curriculum.10,24,25
A recent study provided evidence that the benefits of the flipped model are simply due to the active learning component.26 As such, our results may have been influenced by the fact that ~70% of our lecture-based large group presentations have an active learning component.
Limitations
This research is limited by the institutional and cultural contexts in which it was conducted. Surveys were collected anonymously to reduce the likelihood of response bias. We were not able to characterize non-responders, who may or may not have had different perceptions of pedagogical approach. These students were in their first year of medical school, which may have influenced perceptions. The results of this study might not be generalizable to other educational programs or cultures. In an attempt to apply these methods and findings in a different context, investigators should consider the specific constraints, type of learning, outcome measures used, and the natural environment of the study setting.
Disclosure
The authors report no conflicts of interest in this work.
References
Evans KH, Ozdalga E, Ahuja N. The medical education of generation Y. Acad Psychiatry. 2016;40(2):382–385. | ||
Western Michigan University [webpage on the Internet]. How Are Millennial Students (and Faculty) Different from Previous Generations? Available from: http://www.med.wmich.edu/how-are-millennial-students-and-faculty-different-previous-generations. Accessed December 19, 2016. | ||
Borges NJ, Manuel RS, Elam CL, Jones BJ. Differences in motives between Millennial and Generation X medical students. Med Educ. 2010;44(6):570–576. | ||
Twenge JM. Generational changes and their impact in the classroom: teaching generation me. Med Educ. 2009;43:398–405. | ||
Mangold K. Educating a new generation teaching baby boomer faculty about millennial students. Nurse Educ. 2007;32:21–23. | ||
EDUCAUSE. 7 Things You Should Know About…Flipped Classrooms. Available from: https://net.educause.edu/ir/library/pdf/eli7081.pdf. Accessed November 2, 2016. | ||
Evans KH, Thompson AC, O’Brien C, et al. An innovative blended preclinical curriculum in clinical epidemiology and biostatistics: impact on student satisfaction and performance. Acad Med. 2016;91(5):696–700. | ||
Hernandez M, Brown J, Foster J. A flipped-classroom model that integrates basic and clinical sciences in a new medical school: the first 2 years at the Alabama College of Osteopathic Medicine. Med Sci Educ. 2016;26:181–184. | ||
Morton DA, Colbert-Getz JM. Measuring the impact of the flipped anatomy classroom: the importance of categorizing an assessment by Bloom’s taxonomy. Anat Sci Educ. 2017;10(2):170–175. | ||
Sharma N, Lau CS, Doherty I, Harbutt D. How we flipped the medical classroom. Med Teach. 2015;37(4):327–330. | ||
Street SE, Gilliland KO, McNeil C. The flipped classroom improved medical student performance and satisfaction in a pre-clinical physiology course. Med Sci Educ. 2015;25:35–43. | ||
Szarek JL, Boardman JM, White M, Holt JT. Integrated and flipped: 5 years’ experience of integrating active learning in an integrated course. Med Sci Educ. 2016;26:159–167. | ||
White C, Bradley E, Martindale J, et al. Why are medical students ‘checking out’ of active learning in a new curriculum? Med Educ. 2014;48(3):315–324. | ||
Vermetten YJ, Vermunt JD, Lodewijks HG. Powerful learning environments? How university students differ in their response to instructional measures. Learn Instr. 2002;12:263–284. | ||
Roberts DH, Newman LR, Schwartzstein M. Twelve tips for facilitating Millennials’ learning. Med Teach. 2012;34:274–278. | ||
Corbin J, Strauss A. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory. Thousand Oaks, CA: Sage Publications; 2010. | ||
White C, McCollum M, Bradley E, et al. Challenges to engaging medical students in a flipped classroom model. Med Sci Educ. 2015;25:219–222. | ||
Casuso-Holgado MJ, Cuesta-Vargas AI, Moreno-Morales N, Labajos-Manzanares MT, Barón-López FJ, Vega-Cuesta M. The association between academic engagement and achievement in health sciences students. BMC Med Educ. 2013;13:33. | ||
Walling A, Istas K, Bonaminio GA, et al. Medical student perspectives of active learning: a focus group. Teach Learn Med. 2017;29(2):173–180. | ||
Rysavy M, Christine P, Lenoch S, Pizzimenti MA. Student and faculty perspectives on the use of lectures in the medical school curriculum. Med Sci Educ. 2015;25:431–437. | ||
Johnson M. Evaluation of learning style for first year medical students. Intl J Scholarship Teach Learn. 2009; Vol 3. | ||
Moffett J. Twelve tips for “flipping’ the classroom. Med Teach. 2015;37:331–336. | ||
Roehling PV, Vander Kooi TL, Dykema S, Quisenberry B, Vandlen C. Engaging the millennial generation in class discussions. Coll Teach. 2011;59:1–6. | ||
Lujan HL, DiCarlo SE. First-year medical students prefer multiple learning styles. Adv Physiol Educ. 2006;30(1):13–16. | ||
Pettit RK, McCoy L, Kinney M, Schwartz FN. Student perceptions of gamified audience response system interactions in large group lectures and via lecture capture technology. BMC Med Educ. 2015;15:92. doi: 10.1186/s12909-015-0373-7. | ||
Jensen JL, Kummer TA, d M Godoy PD. Improvements from a flipped classroom may simply be the fruits of active learning. CBE Life Sci Educ. 2015;14(1):1–12. |
Supplementary material
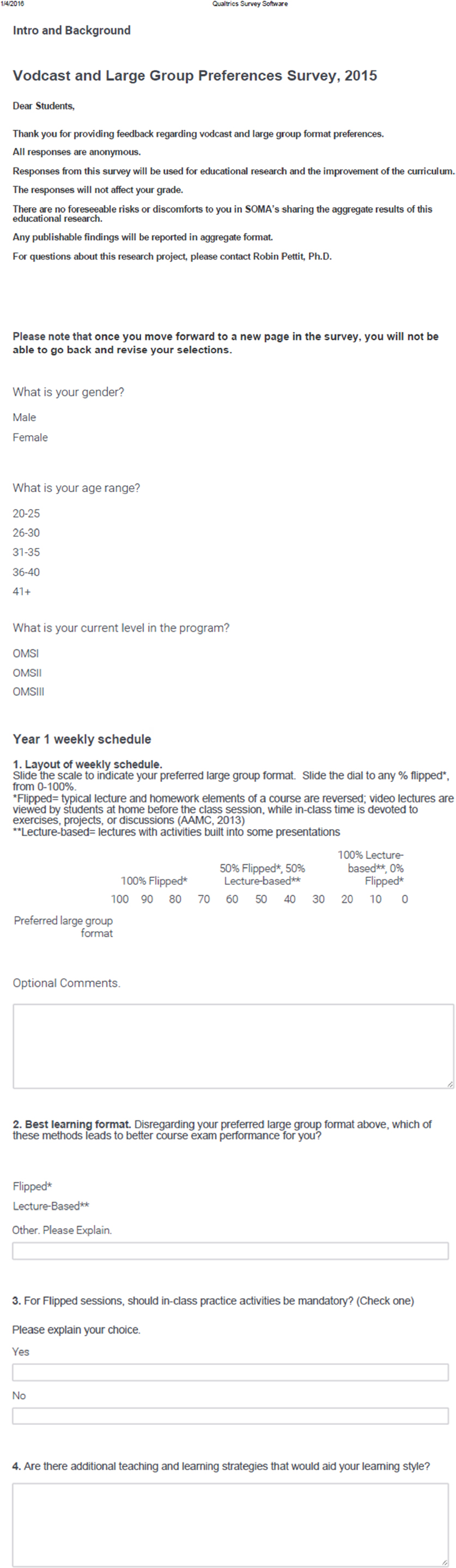 | Figure S1 Flipped Preferences Survey Abbreviations: AAMC, Association of American Medical College; SOMA, School of Osteopathic Medicine in Arizona. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.