Back to Journals » Journal of Pain Research » Volume 15
Use of QR Codes for Promoting a Home-Based Therapeutic Exercise in Patients with Lumbar Disc Herniation and Lumbar Spinal Stenosis: A Prospective Randomized Study
Authors Chang MC ![]() , Park D
, Park D ![]() , Choo YJ
, Choo YJ ![]()
Received 5 October 2022
Accepted for publication 14 December 2022
Published 23 December 2022 Volume 2022:15 Pages 4065—4073
DOI https://doi.org/10.2147/JPR.S391735
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Alaa Abd-Elsayed
Min Cheol Chang,1,* Donghwi Park,2,* Yoo Jin Choo3
1Department of Rehabilitation Medicine, Yeungnam University Hospital, Daegu, Republic of Korea; 2Department of Physical Medicine and Rehabilitation, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Republic of Korea; 3Medical Interdisciplinary Team, Medical Device Development Center, Daegu-Gyeongbuk Medical Innovation Foundation, Daegu, 41061, Republic of Korea
*These authors contributed equally to this work
Correspondence: Yoo Jin Choo, Medical Interdisciplinary Team, Medical Device Development Center, Daegu-Gyeongbuk Medical Innovation Foundation, 80, Cheombok-ro, Dong-gu, Daegu, 41061, Republic of Korea, Tel +82 10 7344 7841, Email [email protected]
Purpose: In the current study, we investigated the usefulness of the quick response (QR) code linked to the source of a video of home-based therapeutic exercise to promote home-based therapeutic exercise in patients with LDH and LSS.
Patients and Methods: Forty patients with LDH and LSS were included in this study. The patients were randomly assigned to one of two groups: QR codes or control groups (20 patients per group). The QR code group received QR code stickers linked with a video that includes a demonstration on how to exercise for the back muscles. We instructed the patients to perform home-based therapeutic exercises three or more days a week. Patients in the control group were asked to perform the therapeutic exercise without providing a QR code to them. The primary outcome was the number of exercises per week. The scores of the numeric rating scale (NRS) and Oswestry disability index (ODI) were investigated as secondary outcomes.
Results: The patients in the QR code group exercised for the lower back muscles on average about two times a week, and 40% of the patients in the QR code group performed the exercise three or more days a week. However, almost no patients in the control group performed therapeutic exercises. Patients in the QR code group showed significantly lower ODI scores at the 1-month and 2-month follow-ups compared with the control group. In addition, the patients who exercised ≥ 3 times per week showed more improvement in the disability than those who exercised < 3 times per week. The NRS scores for lower back pain and radicular leg pain were not significantly different between the QR code and control groups.
Conclusion: We found that QR codes can be useful for encouraging patients with LDH or LSS to perform home-based therapeutic exercises.
Keywords: lumbar disc herniation, lumbar spinal stenosis, quick response code, exercise, pain, disability
Introduction
Lumbar disc herniation (LDH) and lumbar spinal stenosis (LSS) are the most common spinal degenerative disorders which can lead to low back pain (LBP) and radicular leg pain.1,2 These disorders can result in the absence of work and decreased activities of daily living.3 In clinical practice, pain from LDH and LSS is one of the most frequent complaints of patients visiting a clinic. The prevalence of chronic LBP is reported to be approximately 15% in the general population,4 and the prevalence of radicular pain ranges from 16–55% in patients with chronic LBP.5
For controlling pain from LDH or LSS, oral medications and procedures are used.6–8 In addition, these disorders can reduce muscle strength, endurance, flexibility, and balance ability of the lower back muscles, which can accelerate degenerative changes in the lumbar spine and aggravate pain from degenerative spinal disorders.9–11 Therefore, in treating LDH and LSS, exercise to increase the strength, endurance, flexibility, and balance ability of the lower back muscles is essential.12–15 However, repetitive exercise is limited because patients lack the motivation to exercise continuously.16 If the methods of exercise for the lower back muscles are verbally explained, patients frequently cannot understand them sufficiently. Even though clinicians should demonstrate how to perform the exercise in patients, it is not easy in real practice owing to time and space constraints.
Recently, digital technology has been greatly advanced and is actively applied in various medical fields.17–19 Quick response (QR) codes can contain a large amount of data or information while keeping the code size small.20,21 Additionally, it has the advantage of being easily recognizable through a smartphone and has a fast recognition speed.20,21 In addition, by converting video uniform resource locators (URLs) to QR codes, people can easily access and view videos. We linked a video demonstrating how a patient with LDH and LSS should perform a therapeutic exercise to the QR code and made it a sticker for an easy supply to patients.
In the current study, we investigated the usefulness of QR codes linked to the source of the video of home-based therapeutic exercise for promoting home-based therapeutic exercise in patients with LDH and LSS.
Materials and Methods
Subjects
This study was conducted prospectively. Of 134 consecutive patients who visited the spine center of our university hospital from March 2022 to April 2022, 40 patients met the inclusion criteria and participated in this study. Patients were recruited by one of our researchers (Y.J.C.) according to the following criteria: 1) age between 20 and 79 years; 2) ≥6-month history of chronic LBP and radicular leg pain; 3) no psychological disorders or cognitive deficits (we excluded patients with psychological disorders or cognitive deficits by directly asking the patients about their diagnostic history, and included patients who have no problems in communicating and acting according to instructions); 4) no exercise for the lower back muscles; 5) endurable pain (numeric rating scale [NRS; 0 {no pain} to 10 {worst pain imaginable}]22 <4) that does not require epidural steroid injection or surgery, and 6) imaging findings (magnetic resonance imaging and/or computed tomography) compatible with patients’ pain. The Institutional Review Board of Yeungnam University Hospital approved this study, and all patients signed an informed consent form. Our study conformed to the Declaration of Helsinki.
The included patients were randomly assigned to one of two groups (QR code and control groups). A total of 20 patients were allocated to each group. Randomization was performed by an independent data manager using a simple method that employed a random number table. The patients were allocated in a 1:1 ratio into either QR code or control groups using a sealed envelope to ensure concealment of the allocation sequence. An independent study nurse assigned the patients into both groups.
Quick Response (QR) Code
We created two videos for patients with LDH or LSS and the videos were uploaded on YouTube (https://www.youtube.com). The video URLs were linked to QR codes. Two QR codes are created as stickers. QR code stickers attached to stiff paper were provided to patients. We thoroughly educated the patients of QR code group on how to view the video using a smartphone (Figure 1). We told the patients to perform home-based therapeutic exercises three or more days a week. The main purpose of the exercise was to strengthen the lower back muscles.
 |
Figure 1 The process for the patients of quick response (QR) code group. |
The exercise program for LDH consisted of the following steps: 1. placed on the floor in the supine position, 2. rolling up the pelvis (posterior tilting of the pelvis) in the supine position, 3. hip lifting from the supine position, 4. sitting up in the supine position, 5. maintaining a quadrupedal position with the stomach tight, 6. raising the opposite arm and leg from the quadrupedal position, 7. lying on one side and raise the legs, 8. maintaining the side plank position, 9. standing up from a sitting position, and 10. from the supine position, lying on one`s side, lowering legs under the bed, and getting up. The exercise program for the LSS consisted of the following: 1. pulling both knees to the chest, 2. placing back on the floor in the supine position, 3. lifting one leg with the knee bent in the supine position, 4. Raising legs with the knee straight in the supine position, 5. cross-lifting of the opposite arm and leg in the supine position, 6. maintaining a quadruped position, and 7. leaning forward in a sitting position. Each exercise step was conducted with 3 sets of 10 repetition a day.
We explained the importance of lower back muscle exercise to the 20 patients in the control group and instructed the patients to find the exercise method on the internet and perform the exercise following it. We did not provide QR codes to the patients in the control group, and no information was given about specific internet sources. Also, any practice for the exercise was not conducted for the patients of control group. The patients were asked to perform home-based exercises for at least three days a week.
During the follow-up period of this study, no injection procedure was conducted, and oral medication for reducing pain did not change in any of the 40 patients.
Outcome Measurements
The assessments during the pretreatment and follow-up periods were performed by one investigator (physiatrist) who was blinded to the patient grouping. The measurements were conducted before initiating the study (initial) and at 1 and 2 months after initiating the study.
The primary outcome was the number of exercises per week. The scores of the NRS and Oswestry disability index (ODI) were investigated as secondary outcomes.22,23 The NRS was used to measure LBP and radicular leg pain. The ODI consists of 10 questions and is used to evaluate functional disabilities caused by LBP.23 Each variable was rated on a 0–5 points scale and the total score ranged from 0 to 50. A high ODI score indicates a more severe functional disability related to pain. We also evaluated the number of times each patient performed a therapeutic exercise for the lower back muscles per week on average during the last month before each 1- and 2-month follow-ups. Additionally, we investigated whether the QR code helped the patient perform the exercise. The NRS was investigated orally, and other outcomes were investigated using a paper-based form.
Statistical Analysis
Data were analyzed using the Statistical Package for Social Science (SPSS, v. 25.0, IBM Corporation, Armonk, NY). Demographic data and outcomes were compared between the QR code and control groups using the Mann–Whitney U and chi-square tests. We divided the patients in the QR code group into the regular exercise group (average ≥3 exercise per week during the follow-up period of 2 months) and non-regular exercise group (average <3 exercise per week during the follow-up period of 2 months). The intragroup comparison between outcomes at the initial and each follow-up was evaluated using the Wilcoxon signed-rank test. Demographic data and outcomes of the regular exercise and non-regular exercise groups were compared using the Mann–Whitney U-test and chi-square test. The level of statistical significance was set at P < 0.05.
Results
Comparison of Demographic and Baseline Data
No dropouts occurred during the study period. Figure 2 presents a CONSORT flow diagram. Sex, age, and initial NRS and ODI scores were not significantly different between the QR code and control groups (age, p = 0.616; sex, p = 0.752; initial NRS of LBP, p = 0.968; initial NRS of radicular leg pain, p = 0.776; initial ODI, p = 0.103) (Table 1).
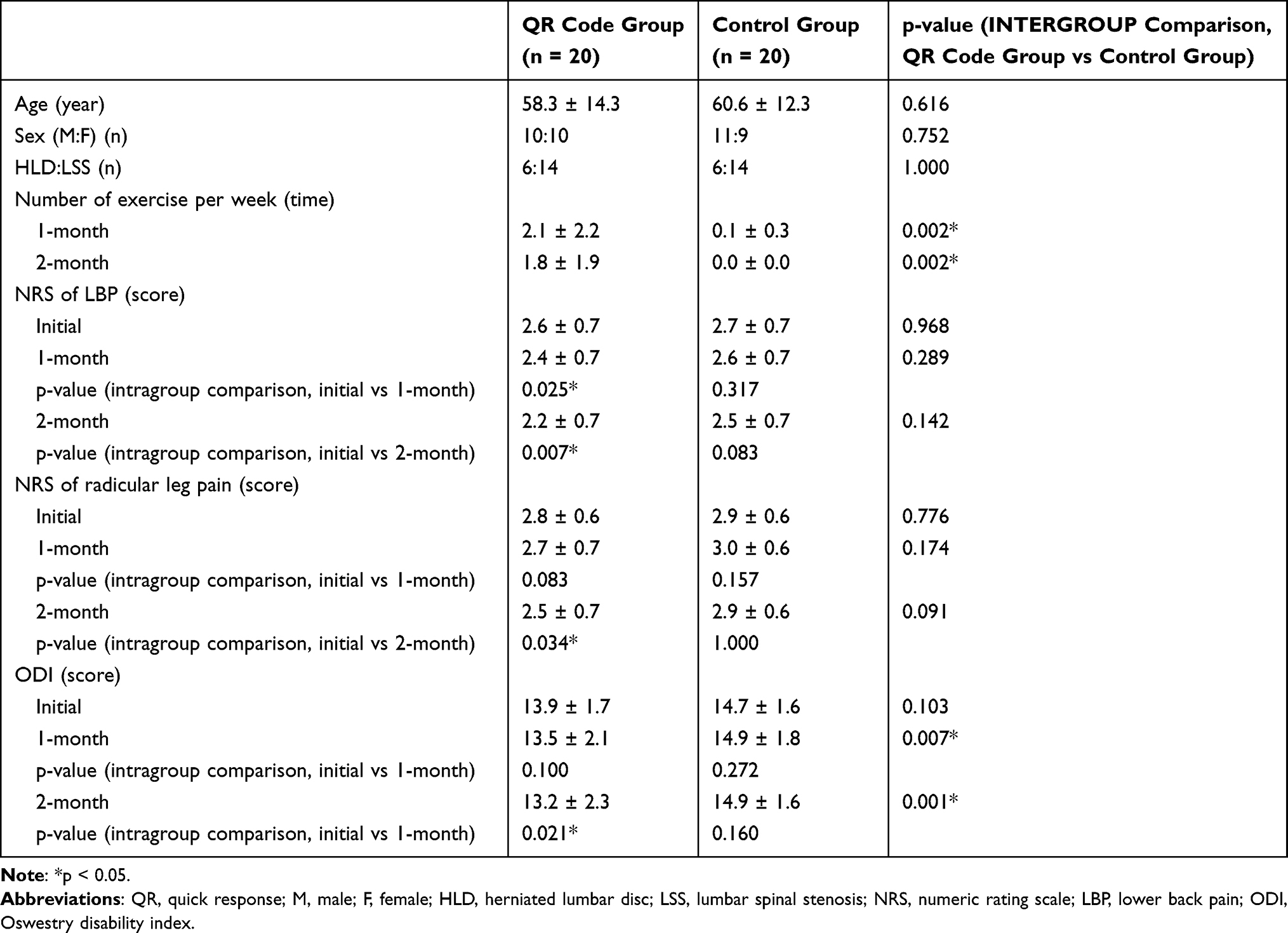 |
Table 1 Demographic Data and Findings at Follow-Ups of the Patients in quick response (QR) Code and Control Groups |
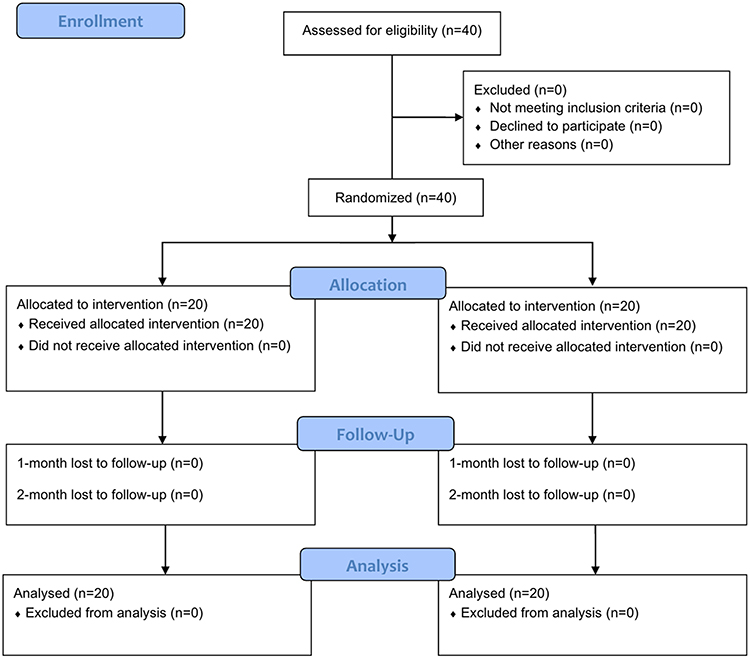 |
Figure 2 CONSORT flow diagram of participant flow through the trial. |
Intragroup Comparison
In the QR code group, NRS for LBP was significantly reduced at the 1- and 2-month follow-ups compared with the initial score (NRS of LBP: 1-month, p = 0.025; 2-month, p = 0.007) (Table 1). In addition, compared with the initial NRS of radicular leg pain and ODI, the scores at the 1-month follow-up were not significantly changed, however, the scores at the 2-month follow-up were significantly reduced (NRS of radicular leg pain: 1-month, p = 0.083, 2-month, p = 0.034; ODI:1-month, p = 0.100, 2-month, p = 0.021) (Table 1). While statistically significant, these NRS reductions may not be clinically relevant because NRS only slightly decreased by 0.3 to 0.4 points.
In contrast, in the control group, the NRS and ODI scores at each follow-up were not significantly different from the initial scores (NRS of LBP: 1-month, p = 0.317, 2-month, p = 0.083; NRS of radicular leg pain: 1-month, p = 0.157, 2-month, p = 1.000; ODI: p = 0.272, 2-month, p = 0.160) (Table 1).
Intergroup Comparison (QR Code Group vs Control Group)
In the intergroup comparison, at the 1- and 2-month follow-ups, the patients in the QR code group exercised more frequently (1-month, p = 0.002; 2-month, p = 0.002), and ODI scores were lower in the patients in the QR code group (1-month, p = 0.007; 2-month, p = 0.001) than in the control group (Table 1). However, the NRS scores for LBP and radicular leg pain were not significantly different between the QR code and control groups (LPB: 1-month, p =0.289, 2-month, p = 0.142; radicular leg pain: 1-month, p =0.174, 2-month, p = 0.091) (Table 1).
Intergroup Comparison (Regular Exercise Group vs Non-Regular Exercise Group)
In the QR code group, eight patients exercised ≥3 times per week on average during the follow-up period and were allocated to the regular exercise group. The other 12 patients performed the exercise on an average of <3 times per week or did not perform the exercise during the follow-up period and were allocated to the non-regular exercise group. Sex, age, and initial NRS and ODI scores were not significantly different between the regular exercise and non-regular exercise groups (age, p = 0.115; sex, p = 1.000; initial NRS of LBP, p = 0.238; initial NRS of radicular leg pain, p = 0.624; initial ODI, p = 0.851) (Table 2). The eight patients in the regular exercise group showed a significant reduction in NRS of LBP and ODI at 1- and 2-month follow-ups, compared with the initial scores (NRS of LBP: 1-month, p = 0.046, 2-month, p = 0.020; ODI: 1-month, p = 0.024, 2-month, p = 0.014) (Table 2). The NRS of radicular leg pain was reduced at the 2-month follow-up, but not at the 1-month follow-up (NRS of radicular leg pain: 1-month, p = 0.083, 2-month, p = 0.014) (Table 2). Among the 12 patients in the non-regular exercise group, NRS and ODI scores at each follow-up were not significantly different from the initial scores (NRS of LBP: 1-month, p = 0.317, 2-month, p = 0.157; NRS of radicular leg pain: 1-month, p = 1.000, 2-month, p = 1.000; ODI: p = 0.317, 2-month, p = 0.317) (Table 2).
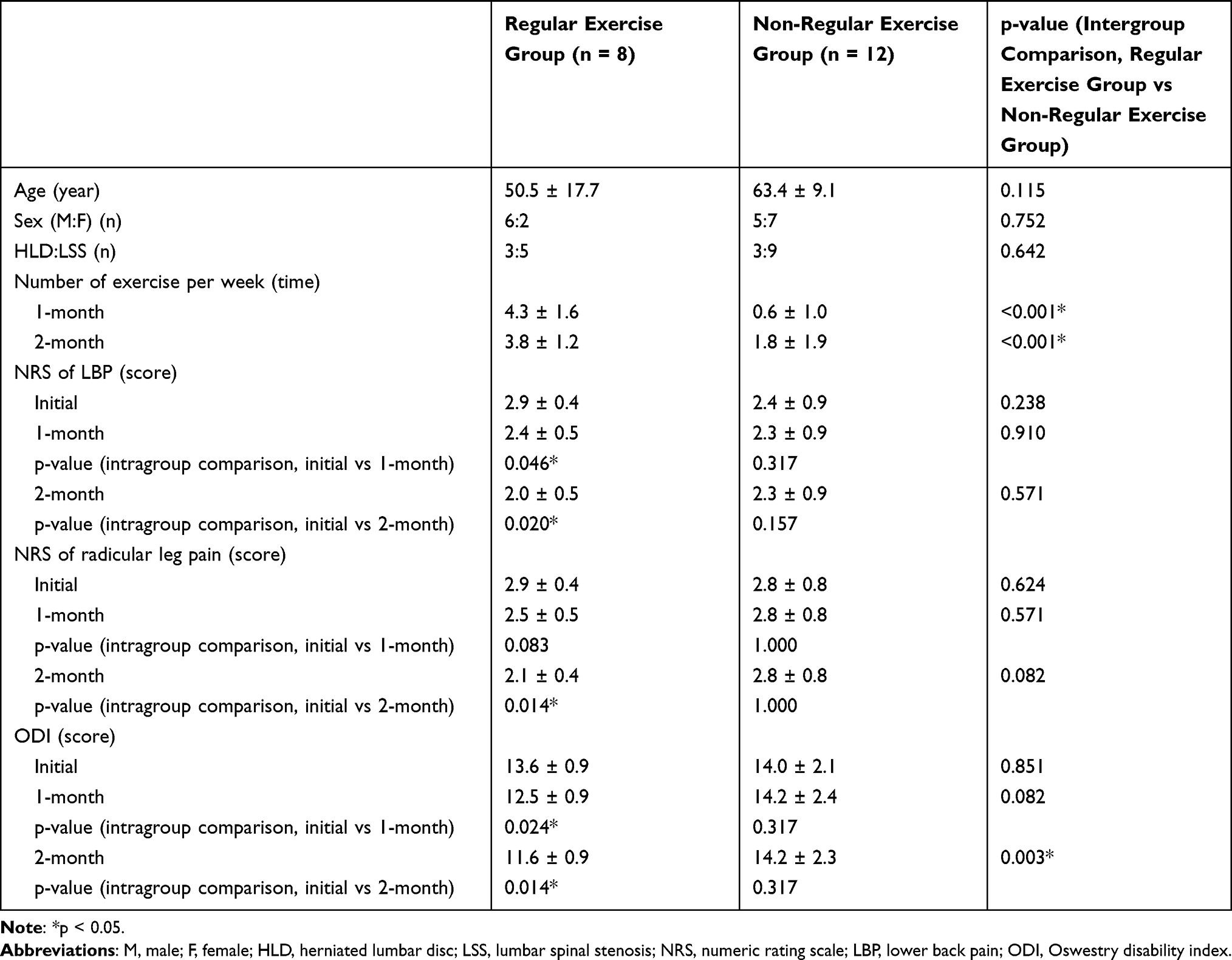 |
Table 2 Demographic Data and Findings at Follow-Ups of the Patients in Good Response and Poor Response Groups |
In the comparison between regular and non-regular exercise groups, at 1- and 2- month follow-ups, the patients in the regular exercise group did exercise more frequently (1-month, p < 0.001; 2-month, p < 0.001), and at 2-month follow-up, ODI scores were lower in the patients in the regular exercise group, compared with the patients in the non-regular exercise group (p = 0.003) (Table 2). However, at the 1-month follow-up, the ODI scores were not significantly different between the regular exercise and non-regular exercise groups (p = 0.082) (Table 2). In addition, the NRS scores of LBP and radicular leg pain were not significantly different between the regular and non-regular exercise groups (LBP: 1-month, p =0.910, 2-month, p = 0.571; radicular leg pain: 1-month, p =0.571, 2-month, p = 0.082) (Table 2).
Discussion
We applied QR codes to patients with LDH or LSS to encourage home-based therapeutic exercise for the lower back muscles and evaluated its effectiveness compared with the control group.
In clinical practice, clinicians emphasize that therapeutic exercise is essential for the treatment of pain and prevention of aggravation of lumbar spine pathologies, and most patients with degenerative spinal disorders usually do not perform the therapeutic exercise. Therefore, encouraging patients to perform therapeutic exercises for the lower back muscles is important for clinicians. In our study, when we asked patients to perform the therapeutic exercise without providing any information on exercise, nearly no patients performed therapeutic exercise. On the other hand, the patients in the QR code group exercise the lower back muscles, on average, about two times a week. We asked the patients to perform home-based exercise three or more days a week, and 40% of the patients in the QR code group performed the exercise three or more days per week. This result suggests that providing the QR code linked to the video of an exercise for the lower back muscles is an effective method to encourage patients with LDH or LSS to perform a home-based therapeutic exercise.
In addition, in the patients who received the QR code, LBP, radicular leg pain, and disability related to LBP, measured with the ODI, were significantly reduced in follow-up evaluations. Moreover, compared with the control group, significantly less disability related to LBP was observed at the 1-month and 2-month follow-ups. However, despite statistically significance, the degrees of improvement of NRS and ODI scores were minimal. Therefore, we cannot confirm that pain and disability of patients in the QR code group were actually improved clinically.
In addition, patients who performed the exercise ≥3 times per week showed reduced LBP, radicular leg pain, and disability. However, patients who exercised <3 times per week showed no significant improvement in LBP, radicular leg pain, and disability. The patients who exercised ≥3 times per week showed less disability related to LBP at the 2-month follow-up than those who exercised <3 times per week. Our results indicate that home-based therapeutic exercise for the lower back muscles is effective for controlling pain related to LDH or LSS and reducing disability related to LBP. In particular, home-based therapeutic exercise has positive clinical effectiveness in improving disability. However, its positive therapeutic effect was only observed when a patient exercised regularly, ≥3 times per week.
In our results, in the comparison between the QR code and control groups, although the ODI score in the QR code group was significantly reduced compared to the control group, the NRS score was not significantly reduced. The NRS score in the QR code group tended to be lower than that in the control group, but the difference was not statistically significant. While the ODI score ranged from 0 to 50, the NRS score ranged from 0 to 10.18,19 Therefore, we think that the ODI score is more likely to change to a larger degree than the NRS. If the number of included subjects was larger in our study, a significant intragroup difference in NRS score would have also been shown.
Recently, QR codes have been used in various fields such as finance, payments, authentication, and transportation.24–26 QR codes have the advantage of being able to contain a lot of information in a small space, and even if some part of the code is damaged, the code can be read to some extent.20,21 Therefore, QR codes containing useful information can be easily provided to patients, and patients can conveniently store and use them. In addition, the rapid speed of reading the information in the QR code can be attributed to its practical and wide use. We applied the QR code to inform how to do the home-based therapeutic exercise for patients with LDH and LSS, and our study is the first to demonstrate its usefulness in clinical practice. However, our study had some limitations. First, only a small number of patients were included in the study. Second, we did not compare the clinical effects of home-based exercise in the QR code group with those of hospital- or center-based exercises. Third, The detail information of exercise compliance of each patient (exercise sets and repetitions per a day) was not investigated. Fourth, sample size could not be calculated before the study given the absence of available comparable data in literature. The primary endpoint of our study was the number of exercises per week. Post-hoc analysis of the power for the primary endpoint between the QR code and control groups showed a high power of 0.98. Fifth, the information on the exercise was not provided enough to the patients of control group. Lastly, our study was non-blinded, therefore there is likely a placebo effect favoring the intervention group. Further studies are warranted to address these limitations.
Conclusion
In conclusion, we found that QR codes can be useful for encouraging patients with LDH or LSS to perform home-based therapeutic exercises. We believe that the QR code can be applied in various musculoskeletal disorders, such as adhesive capsulitis, supraspinatus tendinopathy, epicondylitis, herniation of the cervical disc, and cervical spinal stenosis.
Funding
The present study was supported by a National Research Foundation of Korea grant funded by the Korean government (grant no. NRF-2019M3E5D1A02069399 and NRF2021R1A2C1013073).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lee DG, Cho YW, Ahn SH, et al. The effect of bipolar pulsed radiofrequency treatment on chronic lumbosacral radicular pain refractory to monopolar pulsed radiofrequency treatment. Pain Physician. 2018;21:E97–E103.
2. Van Boxem K, Cheng J, Patijn J, et al. 11. Lumbosacral radicular pain. Pain Pract. 2010;10:339–358. doi:10.1111/j.1533-2500.2010.00370.x
3. Bowman SJ, Wedderburn L, Whaley A, et al. Outcome assessment after epidural corticosteroid injection for low back pain and sciatica. Spine. 1993;18:1345–1350. doi:10.1097/00007632-199308000-00014
4. Iizuka Y, Iizuka H, Mieda T, et al. Prevalence of chronic nonspecific low back pain and its associated factors among middle-aged and elderly people: an analysis based on data from a musculoskeletal examination in Japan. Asian Spine J. 2017;11:989–997. doi:10.4184/asj.2017.11.6.989
5. Fishbain DA, Cole B, Lewis JE, et al. What is the evidence that neuropathic pain is present in chronic low back pain and soft tissue syndromes? An evidence-based structured review. Pain Med. 2014;15:4–15. doi:10.1111/pme.12229
6. Chang MC. The blind spot and challenges in pain management. J Yeungnam Med Sci. 2022;39:179–180. doi:10.12701/jyms.2022.00339
7. Park D, Chang MC. The mechanism of action of pulsed radiofrequency in reducing pain: a narrative review. J Yeungnam Med Sci. 2022;39:200–205. doi:10.12701/jyms.2022.00101
8. Chang MC, Lee DG. Outcome of transforaminal epidural steroid injection according to the severity of lumbar foraminal spinal stenosis. Pain Physician. 2018;21:67–72. doi:10.36076/ppj.1.2018.67
9. Clael S, Campos LF, Correia KL, et al. Exercise interventions can improve muscle strength, endurance, and electrical activity of lumbar extensors in individuals with non-specific low back pain: a systematic review with meta-analysis. Sci Rep. 2021;11:16842. doi:10.1038/s41598-021-96403-7
10. Nowotny AH, Calderon MG, de Souza PA, et al. Lumbar stabilisation exercises versus back endurance-resistance exercise training in athletes with chronic low back pain: protocol of a randomised controlled trial. BMJ Open Sport Exerc Med. 2018;4:e000452. doi:10.1136/bmjsem-2018-000452
11. Ozcan Kahraman B, Salik Sengul Y, Kahraman T, et al. Developing a reliable core stability assessment battery for patients with nonspecific low back pain. Spine. 2016;41:E844–E850. doi:10.1097/BRS.0000000000001403
12. Ammendolia C, Hofkirchner C, Plener J, et al. Non-operative treatment for lumbar spinal stenosis with neurogenic claudication: an updated systematic review. BMJ Open. 2022;12:e057724. doi:10.1136/bmjopen-2021-057724
13. Bussières A, Cancelliere C, Ammendolia C, et al. Non-surgical interventions for lumbar spinal stenosis leading to neurogenic claudication: a clinical practice guideline. J Pain. 2021;22:1015–1039. doi:10.1016/j.jpain.2021.03.147
14. Rousing R, Jensen RK, Fruensgaard S, et al. Danish national clinical guidelines for surgical and nonsurgical treatment of patients with lumbar spinal stenosis. Eur Spine J. 2019;28:1386–1396. doi:10.1007/s00586-019-05987-2
15. Zaina F, Tomkins-Lane C, Carragee E, et al. Surgical versus non-surgical treatment for lumbar spinal stenosis. Cochrane Database Syst Rev. 2016;2016:CD010264. doi:10.1002/14651858.CD010264.pub2
16. Boutevillain L, Dupeyron A, Rouch C, et al. Facilitators and barriers to physical activity in people with chronic low back pain: a qualitative study. PLoS One. 2017;12:e0179826. doi:10.1371/journal.pone.0179826
17. Chang MC. Storing information of stroke rehabilitation patients using blockchain technology: a software study. J Yeungnam Med Sci. 2022;39:98–107. doi:10.12701/yujm.2021.01368
18. Cordeiro JV. Digital technologies and data science as health enablers: an outline of appealing promises and compelling ethical, legal, and social challenges. Front Med. 2021;8:647897. doi:10.3389/fmed.2021.647897
19. Wang Q, Su M, Zhang M, et al. Integrating digital technologies and public health to fight covid-19 pandemic: key technologies, applications, challenges and outlook of digital healthcare. Int J Environ Res Public Health. 2021;18:6053. doi:10.3390/ijerph18116053
20. Pandya KH, Galiyawala HJ. A survey on QR codes: in context of research and application. Int J Emerg Technol Adv Eng. 2014;4:258–262.
21. Victor N. Enhancing the data capacity of QR codes by compressing the data before generation. Int J Comput Appl. 2012;60:17–21. doi:10.5120/9663-1104
22. Haefeli M, Elfering A. Pain assessment. Eur Spine J. 2006;15 Suppl 1:S17–24. doi:10.1007/s00586-005-1044-x
23. Fairbank J, Couper J, Davies JB, et al. The Oswestry low back pain disability questionnaire. Physiotherapy. 1980;66:271–273.
24. Hayes WC. Using QR Codes to Connect Patients to Health Information. Ann Fam Med. 2017;15:275. doi:10.1370/afm.2067
25. Hur J, Chang MC. Usefulness of an online preliminary questionnaire under the COVID-19 pandemic. J Med Syst. 2020;44:116. doi:10.1007/s10916-020-01586-7
26. Karmawan GM, Fernandoand Y, Gui A. QR code payment in Indonesia and its application on mobile banking. KnE Soc Sci. 2019;3:551–568. doi:10.18502/kss.v3i22.5073
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Sex Differences in the Mediating Effect of Kinesiophobia on Chronic Pain, Dysesthesia, and Health-Related Quality of Life in Japanese Individuals Aged 65 Years Old and Older Treated with Surgery for Lumbar Spinal Stenosis
Higuchi D, Kondo Y, Watanabe Y, Miki T
Journal of Pain Research 2022, 15:1845-1854
Published Date: 30 June 2022
Effects of a Mind-Body Program for Chronic Pain in Older versus Younger Adults
LaRowe LR, Bakhshaie J, Vranceanu AM, Greenberg J
Journal of Pain Research 2023, 16:3917-3924
Published Date: 15 November 2023
A Study of the Effect of Treatment On the Clinical Profile, Pain, and Disability in Migraine Patients Seen in a Tertiary Hospital
Kandasamy G, Almaghaslah D, Almanasef M, Almeleebia TM, Orayj K, Siddiqua A, Shorog E, Alshahrani AM, Prabahar K, Veeramani VP, Amirthalingam P, Alqifari S, Alshahrani N, AlSaedi AH, A Alsaab A, Aljohani F, Begum MY, Atiya A
Journal of Multidisciplinary Healthcare 2024, 17:3525-3534
Published Date: 22 July 2024
Minimally Invasive Lumbar Decompression (MILD) in Patients with Lumbar Spinal Stenosis: A Systematic Review of Randomized and Prospective Trials
Orhurhu V, Brancolini S, Zheng D, Snyder S, Jevotovsky DS, Chopra H, Sahni S, Li N, D’Souza RS, Evankovich M, Lynch B, Farrell ME, Alter BJ, Emerick T
Journal of Pain Research 2025, 18:3527-3540
Published Date: 11 July 2025
Effect of Exercise Interventions for Rheumatoid Arthritis: A Systematic Review and Network Meta-Analysis of Randomised Controlled Trials
Zhang Y, He Z, Yin Z, Wang J, Gao W, Jie L
Journal of Pain Research 2025, 18:5109-5126
Published Date: 30 September 2025