Back to Journals » Journal of Pain Research » Volume 16
Effects of a Mind-Body Program for Chronic Pain in Older versus Younger Adults
Authors LaRowe LR, Bakhshaie J, Vranceanu AM ![]() , Greenberg J
, Greenberg J ![]()
Received 8 September 2023
Accepted for publication 10 November 2023
Published 15 November 2023 Volume 2023:16 Pages 3917—3924
DOI https://doi.org/10.2147/JPR.S435639
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Michael Schatman
Lisa R LaRowe,1,2 Jafar Bakhshaie,3,4 Ana-Maria Vranceanu,3,4 Jonathan Greenberg3,4
1Mongan Institute Center for Aging and Serious Illness, Division of Palliative Care and Geriatric Medicine, Massachusetts General Hospital, Boston, MA, USA; 2Department of Medicine, Harvard Medical School, Boston, MA, USA; 3Center for Health Outcomes and Interdisciplinary Research, Department of Psychiatry, Massachusetts General Hospital, Boston, MA, USA; 4Department of Psychiatry, Harvard Medical School, Boston, MA, USA
Correspondence: Ana-Maria Vranceanu, Center for Health Outcomes and Interdisciplinary Research, Department of Psychiatry, Massachusetts General Hospital, Boston, MA, USA, Email [email protected]
Purpose: Improving physical function is key to decreasing the burden of chronic pain across the lifespan. Although mind-body interventions show promise in increasing physical function in chronic pain, very little is known about whether older and younger adults derive similar benefit. Indeed, older adults experience higher rates of chronic pain and greater impacts of pain on physical function compared to younger adults. Therefore, additional work is needed to determine the extent of benefit older versus younger adults receive from a mind-body intervention. Here, we examined age differences in the effects of two mind-body and walking programs on pain and multimodal physical function.
Participants and Methods: Participants were 82 individuals with heterogenous chronic musculoskeletal pain (66% female, 57% aged ≥ 50 years) who participated in a feasibility randomized controlled trial of two mind-body interventions. They completed self-reported (WHODAS 2.0), performance-based (6-minute walk test), and objective (accelerometer-measured step count) measures of physical function, as well as self-report measures of pain intensity, before and after the intervention.
Results: Results indicated that adults aged ≥ 50 (vs adults aged < 50) demonstrated greater improvements in performance-based physical function (6-minute walk test) and reductions in pain during activity. No age differences in the effects of the intervention on self-reported or objectively measured physical function were observed.
Conclusion: Collectively, these findings suggest that older adults can achieve equivalent or greater benefits from mind-body programs for chronic pain, despite facing unique challenges to chronic pain management (eg, multimorbidity, greater sedentary behavior).
Keywords: older adults, physical function, pain, disability, mindfulness
Introduction
Chronic pain affects over one in five US adults.1 The prevalence of chronic pain increases with age,1 and the negative impact of pain is often greater among older (vs younger) adults.2 Given the ubiquity and detrimental effects of chronic pain, developing interventions that reduce the burden of pain across the lifespan is a major public health priority.3–5 Improving physical function is key to decreasing such burden, as it shows promise in reducing the impact of pain on daily activities and improving emotional function.6,7
We developed the first mind-body activity intervention to increase multimodal physical function among individuals with heterogenous chronic pain.8 The intervention includes mind-body skills such as mindfulness, commonly defined as the ability to pay attention, on purpose, in the present moment and in a non-judgmental manner, given evidence this skill can improve pain outcomes including physical function in this population.9,10 The program additionally included other evidence-based skills, such as pain-specific cognitive behavioral skills (eg, challenging pain-related thoughts) and physical restoration skills (eg, setting walking goals).11 We tested the program in a two-armed RCT, with each arm offering an identical program either with (GetActive-Fitbit) or without (GetActive) a Fitbit device (Greenberg et al, 2020). Consistent with IMMPACT recommendations for comprehensive assessment of physical function, we examined the effects of the program on self-reported, performance-based, and objective physical function.6 Results indicated that participation in this group-based program led to significant improvements in self-reported and performance-based (ie, 6-minute walk test) physical function, regardless of whether the program was offered with or without a Fitbit device.
Given that there are several key differences between older and younger adults that may influence intervention effects,2,12–14 an important next step is to determine whether older and younger adults derive similar benefit from the program. Indeed, older adults differ from younger adults in psychological mechanisms that influence pain-related functioning,12 which may result in differential treatment effects. For example, older (versus younger) adults tend to experience lower levels of pain catastrophizing and higher levels of pain acceptance and pain self-efficacy, suggesting a potential need for age-tailored interventions.12 Moreover, adults aged ≥50 report high levels of pain during activity, which may lead to greater sedentary behavior and lower levels of physical activity.15,16 Older adults also experience unique barriers to pain management, such as high rates of multimorbidity,2,13,14 which may further impact the extent of benefit they receive from a mind-body intervention. Alternatively, given that older adults tend to be more sedentary,17,18 they may have a greater potential (compared to younger adults) for improvement in physical activity and may derive greater benefit from reducing sedentary behavior. Such potential differential treatment effects may bear important implications for optimizing the target population (and potentially choosing a more clinically relevant subsample of individuals with chronic pain) for mind-body interventions aimed at improving physical function for chronic pain and tailoring specific program content for different age groups. However, the comparative utility of mind-body pain management interventions in older versus younger adults remains unknown.
The current study is the first to examine whether there are age differences in the effects of a mind-body program on pain during activity and multimodal physical function. Specifically, we conducted secondary data analysis to test whether older (age ≥50) versus younger (age <50) adults reported greater improvements in pain during activity and self-reported, performance-based, and objectively measured physical function from pre- to post-treatment. We also examined age differences in longer-term effects of the intervention on pain and self-reported physical function at a 3-month follow-up assessment.
Methods
Transparency and Openness
This study was pre-registered on ClinicalTrials.gov (NCT03412916). We report how we determined our sample size, and describe all data exclusions, manipulations, and all measures in the primary outcomes paper of the parent trial (Greenberg et al, 2020). Study materials, deidentified data, and analytic code are available upon reasonable request to the corresponding author.
Participants
Participants were 82 individuals with heterogeneous chronic musculoskeletal pain who participated in feasibility randomized controlled trial of two mind-body interventions designed to increase multimodal physical function and other measures (PROs).19 Participants were recruited from July 2018 to September 2019 via direct referrals from the Massachusetts General Hospital Pain Clinic, hospital-wide email lists, and flyers, and were screened for eligibility via phone. To be included in the trial, participants had to be at least 18 years-old, report nonmalignant chronic pain for >3 months, be able to walk unassisted for at least 6 minutes, have access to a mobile device with Bluetooth version 4.0, report no changes in psychotropic or pain medications in the past 3 months, and be cleared for participation by a physician. Participants were excluded if they reported a medical illness expected to worsen in the next 6 months, serious and untreated psychiatric illness or active suicidality, or current untreated substance use disorder. In addition, participants who reported that they practiced meditation/yoga or relaxation response skills for >45 minutes a week, used a Fitbit device, or engaged in regular physical exercise for >30 minutes daily in the past 6 months were also excluded from the study. Additional information regarding our sample – including how sample size was determined – is provided in Greenberg et al, 2020.
Procedure and Intervention
We recruited patients with heterogenous musculoskeletal pain (self-reported nonmalignant chronic pain for >3 months), who were at least 18 years old, able to walk unassisted for at least 6 minutes, had access to a mobile device with Bluetooth version 4.0, had no change in psychotropic or pain medications for the past 3 months, and were cleared for participation by a physician. Patients who reported a medical illness expected to worsen in the next 6 months, serious and untreated psychiatric illness or active suicidality, current untreated substance use disorder, regular practice of meditation/yoga or relaxation response skills, use of a Fitbit device in the past month, or engagement in regular physical exercise were excluded. Eligible participants were randomly assigned to one of two 10-week 90-minute groups focused on increasing walking using time-based goals (GetActive, n = 41) or step-count reinforced via Fitbit (GetActive-Fitbit, n = 41). The two programs are identical, with the exception of the inclusion of the Fitbit device in GetActive-Fitbit. The programs were adapted from the Relaxation Response Resiliency Program (3RP),20 and included core skills of 3RP (eg, relaxation strategies, mindfulness skills) in addition to pain-specific skills (eg, pain-specific cognitive behavioral skills, physical restoration skills). Participants completed assessments, which included self-report, objectively measured, and performance-based assessments of physical function (see Measures section), one week prior to beginning the intervention (baseline) and again approximately one week following completion of the program (post-treatment). Participants also completed a 3-month follow-up assessment which included self-report (but not objective or performance-based) measures of physical function. This study was approved by the Massachusetts General Hospital Institutional Review Board under protocol number 2017P000628 (“Integrating Mind-Body Skills with Physical Activity to Improve Physical and Emotional Outcomes in Patients with Chronic Pain”). All participants provided written informed consent prior to participating in this study and all procedures were conducted in accordance with the Declaration of Helsinki. Additional details about the procedure and intervention conditions can be found in Greenberg et al.19
Measures
Pain Intensity During Activity
We used a numerical rating scale (NRS) ranging from 0 (no pain) to 10 (worst pain ever) to assess pain intensity with activity at baseline, post-treatment, and 3-month follow-up.21,22
Physical Functioning
In accordance with the IMMPACT criteria6,23 and the International Classification of Functioning, disability and Health (ICF) guidelines,24 we assessed self-reported, objectively measured, and performance-based physical function.
Self-Reported Physical Function
We used the World Health Organization Disability Assessment Schedule 2.0 (WHODAS)25 to measure self-reported physical function. The WHODAS is a 36-item questionnaire that assesses difficulties in 6 domains of function: cognition (understanding and communication), mobility (moving and getting around), self-care (hygiene, dressing, eating, and staying alone), getting along with others (interacting with other people), life activities (domestic responsibilities, leisure, and work), and participation (joining community activities). The WHODAS was administered at baseline, post-treatment, and 3-month follow-up.
Objectively Measured Physical Function
We used average daily step count, as measured by a wGT3X-BT ActiGraph accelerometer device,26 to objectively assess physical function. We asked participants to wear the device during all waking hours for 7 days before (baseline) and after (post-treatment) the programs. As described in our prior work,8,19 we used ActiLife software (ActLife LLC) to store, clean, and analyze the data. A staff member verified that each participant had valid wear time (≥7 hours per day) and ensured that each participant’s recorded activity was consistent with self-reported wear times logged in activity diaries. Step count was assessed at baseline and immediately post-treatment.
Performance-Based Physical Function
We used a 6-minute walk test to measure performance-based physical function.27 Specifically, we measured and recorded the distance (meters) that each participant covered by walking on a flat surface for 6 minutes. Participants completed the 6-minute walk test at baseline and immediately post-treatment.
Sociodemographic Characteristics
We asked participants to report sociodemographic information, including age, gender, race/ethnicity, and marital status at baseline. For these secondary analyses, we dichotomized age to reflect younger (<50 years) versus older (≥50 years) adults. We elected to use this age cut-off because a more progressive decline in physical activity is seen after age 50.28 Moreover, this is the most commonly-used cut-off in prior studies on mind-body interventions for older adults with chronic pain.29
Analytic Plan
We used SAS 9.4 for analyses. We used a linear mixed model with completely unstructured covariance and autoregressive random visit-specific effects to examine the impact of time in interaction with age on outcomes. We merged the data from both treatment groups as the parent paper did not indicate any significant differences in outcomes between the treatment conditions. We conducted a series of contrasts (baseline to post-treatment, and baseline to 3-month follow-ups) to test the specific hypotheses regarding the within-group and between-group differences in the outcome variables at different time points. The model took into account all available data. The estimated covariance across repeated measurements implicitly imputes missing data and produces unbiased estimates, under the missing-at-random assumption.
Age-dependent differences in changes from baseline to post-treatment (for all outcome variables) and baseline to 3-month follow-up (for pain during activity and WHODAS disability) were evaluated using least-squares linear contrasts and provided as point estimates with 95% CIs. We controlled for the baseline levels of the outcome variables which were significantly different between the younger and older adults. We employed a False Discovery Rate (FDR) approach to control for Type I error given the multiple hypotheses testing, as outlined by Benjamini & Hochberg.30 We calculated the model-based effect size (ES) estimate by dividing the model-derived mean difference estimates by the pooled within-individual variations of each outcome at baseline, a method equivalent to Cohen’s d in RCTs.31–33
Results
Participant Characteristics
About two-thirds of participants (65.9%) were female and slightly more than half (57.3%) were aged 50 and older. Among younger adults (age <50 years), age ranged from 21 to 49 (M = 37.7, SD =7.4), whereas, among older adults (age ≥50 years), age ranged from 50 to 79 (M = 62.3, SD = 8.2). The majority of participants (80.5%) were White, and half (54.8%) completed at least a 4-year college degree. Other than age, no significant differences in sociodemographic characteristics were observed between older versus younger adults. Baseline levels of the hypothesized dependent variables were not significantly different as a function of age, except for pain during activity, which was significantly higher in older adults (Mdiff = −1.01; t = −2.22; p = 0.029).
Age Differences in Treatment Effects
For baseline to post-treatment assessment, the time by age interaction was significantly associated with the distance walked during the 6-minute walk test (B = 17.77, SE = 6.69, p = 0.03; ES = 0.19; Table 1). Simple slope analysis indicated that the effect of time on change in distance was significant for both groups but was greater for the 50 years of age or older participants (Mdiff = 53.02, SE = 8.20, p < 0.001; ES = 0.63) compared to younger participants (Mdiff = 36.12, SE = 10.47, p = 0.002; ES = 0.40; Figure 1). The time by age interaction was not significant for other outcome variables (ps > 0.05; Table 1).
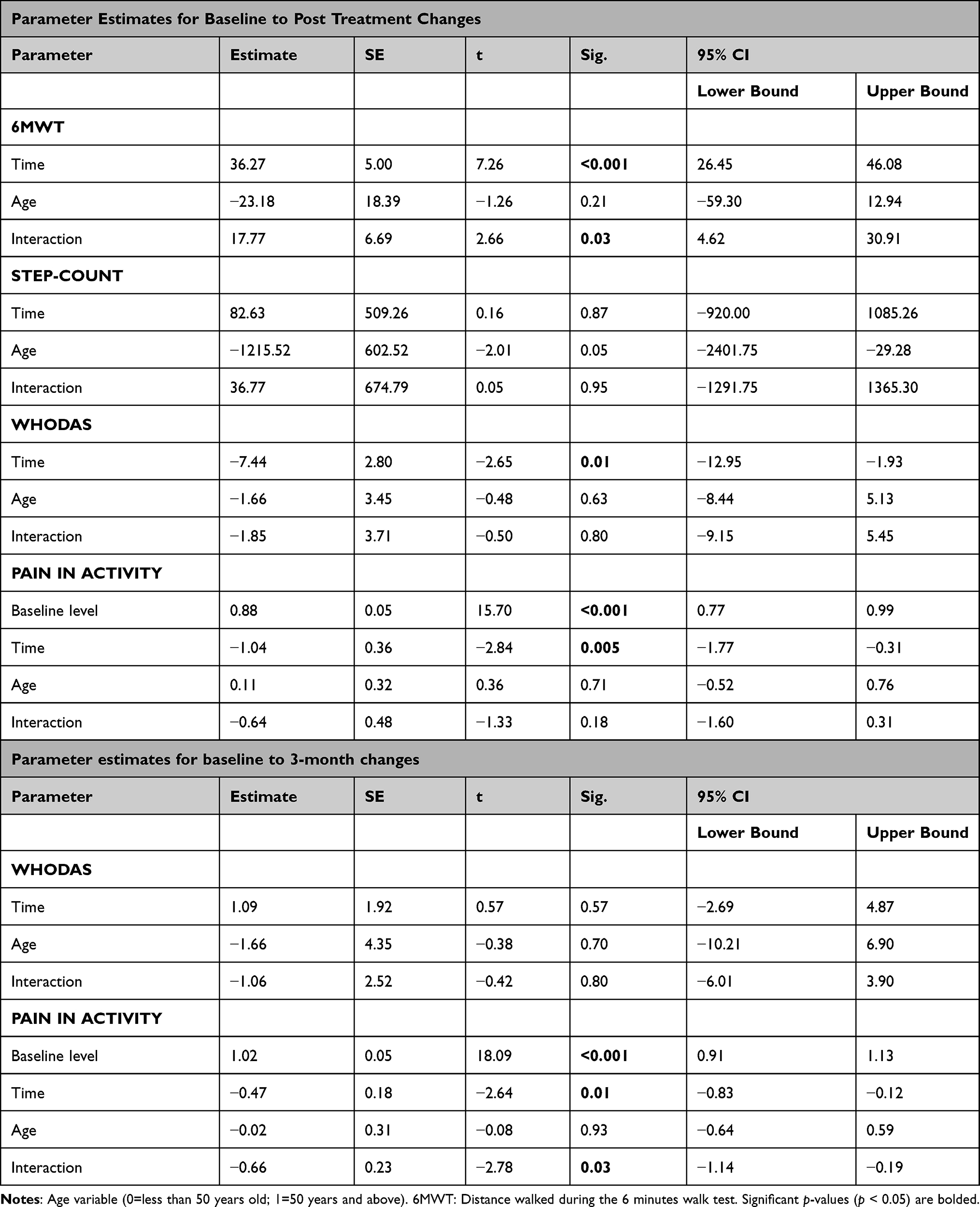 |
Table 1 Parameter Estimates |
For the baseline to the 3-month follow-up assessment, the time by age interaction was significantly associated with pain during activity (B = −0.66, SE = 0.23, p = 0.03; ES = 0.28; Table 1). Simple slope analysis indicated that while the effect of time on the intensity of pain during activity was significant for both age groups, participants 50 years of age or older (Mdiff = 2.30, SE = 0.37, p < 0.001; ES = 1.09) had greater improvement in pain during activity compared to the younger participants (Mdiff = 0.96, SE = 0.42, p = 0.03; ES = 0.46; Figure 1). The time by age interaction was not significant for WHODAS (p = 0.80; Table 1).
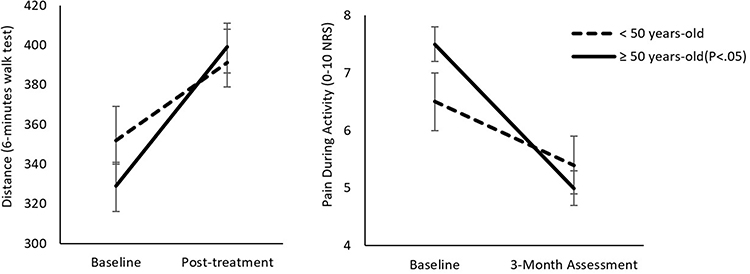 |
Figure 1 Simple slope of change in the 6-min walk test and pain during activity for both age groups. |
Discussion
Despite well-established age differences in the prevalence and impact of chronic pain and underlying psychological mechanisms, the comparative utility of mind-body interventions for pain management and improvement in multimodal physical function in older relative to younger adults is not known. Here, we tested whether there were age differences in the effects of a recently developed mind-body intervention designed to improve physical function among individuals with chronic pain on pain during activity and multimodal physical function. Results indicated that adults aged 50 and older demonstrated greater improvements in performance-based physical function, as measured by the 6-minute walk test, when compared to their younger counterparts. Moreover, older (vs younger) adults reported greater decreases in pain intensity during activity from baseline to 3-month follow-up assessment. No age differences in the effects of the intervention on self-reported or objectively measured physical function were observed. Taken together, these findings indicate that older adults achieve equivalent or greater benefits from a mind-body intervention program for chronic pain.
These findings are consistent with evidence supporting the effectiveness of mind-body interventions for chronic pain in older adults,29 and extend prior studies by comparing older and younger adults when examining intervention effects. Although both age groups benefited from the programs, our findings suggest that older adults may derive even greater benefit from a mind-body intervention. These findings are in line with prior evidence indicating that older adults may respond more positively to interventions that focus on improving functioning versus pain reduction.34 Given that older adults may have experienced a greater number of unsuccessful attempts to reduce their pain in the past, this population (compared to younger adults) may have higher levels of motivation to engage in an intervention that focuses on living well with pain instead of pain reduction.34 Moreover, older adults face numerous uncontrollable stressors (eg declining health), and, thus, may more readily adopt pain acceptance during mindfulness-based pain interventions.35 Future work is needed to elucidate the mechanisms underlying the current findings and to determine whether pain acceptance contributes to the observed age differences in intervention effects.
One important clinical implication of this study is that mind-body interventions may offer benefit for chronic pain management across the lifespan. Although older adults often face significant barriers to chronic pain management, such as high rates of sedentary behavior and multimorbidity,2,13,14,36 it is still possible for older adults to achieve meaningful benefit from a mind-body intervention. Moreover, given these unique challenges, older adults may have even more room for improvement in physical activity and function-related outcomes than their younger counterparts, and thus may derive even greater benefit from mind-body intervention programs. Indeed, although these results underscore the importance of physical activity promotion among all individuals with chronic pain, it may be especially important to promote physical activity among older adults with chronic pain.
This study has several strengths, including the utilization of multimodal physical function assessment and inclusion of a 3-month follow-up time point which permitted examination of maintenance of intervention effects over time for self-reported measures. However, several limitations are also worth noting. The sample was relatively small (N = 82), primarily white, and the older adults who participated were on the younger spectrum of older adulthood (age range: 50–79). Although our decision to include adults aged 50 and older in the “older adult” group was based on prior work and evidence of a more progressive decline in physical activity after age 50,28,29 additional work is needed to extend these findings to larger samples that include a wider range of older adults, including those aged 80 and older. Moreover, future research should include a control group to establish causality in observed treatment effects.
Conclusion
The results of this study advance our understanding of the role of age in chronic pain treatment effects. Collectively, our findings provide the first evidence that older (versus younger) adults with chronic pain derive equivalent benefits – and perhaps even greater benefits in pain and performance-based physical function – from a mind-body program designed to increase multimodal physical function among individuals with chronic pain.
Data Sharing Statement
Data and associated study documents are available from the corresponding author upon request.
Funding
This work was supported by the National Center for Complementary and Integrative Health (1K23AT012364-01 to JB; IR34AT00935601A1 and 1K24AT011760-01 to AMV; 1K23AT010653-01A1 to JG).
Disclosure
Ana-Maria Vranceanu and Jonathan Greenberg are co-senior authors for this study. The authors report no conflicts of interest in this work.
References
1. Zelaya CE, Dahlhamer JM, Lucas JW, Connor EM. Chronic pain and high-impact chronic pain among US adults, 2019. NCHS Data Brief; 2020:390.
2. Schofield P. Pain in older adults: epidemiology, impact and barriers to management. Rev Pain. 2007;1(1):12–14. doi:10.1177/204946370700100104
3. Goldberg DS, McGee SJ. Pain as a global public health priority. BMC Public Health. 2011;11(1):1–5. doi:10.1186/1471-2458-11-770
4. Bonezzi C, Fornasari D, Cricelli C, Magni A, Ventriglia G. Pharmacological management of adults with chronic non-cancer pain in general practice. Pain Ther. 2020;9(Suppl 1):17–28. doi:10.1007/s40122-020-00218-9
5. Office of Disease Prevention and Health Promotion. Health People: Chronic Pain; 2030. Available from: https://health.gov/healthypeople/objectives-and-data/browse-objectives/chronic-pain.
6. Taylor AM, Phillips K, Patel KV, et al. Assessment of physical function and participation in chronic pain clinical trials: IMMPACT/OMERACT Recommendations. Pain. 2016;157(9):1836–1850. doi:10.1097/j.pain.0000000000000577
7. Turk DC, Dworkin RH, Revicki D, et al. Identifying important outcome domains for chronic pain clinical trials: an IMMPACT survey of people with pain. Pain. 2008;137(2):276–285. doi:10.1016/j.pain.2007.09.002
8. Greenberg J, Lin A, Zale EL, et al. Development and early feasibility testing of a mind-body physical activity program for patients with heterogeneous chronic pain; the getactive study. J Pain Res. 2019;12:3279–3297. doi:10.2147/JPR.S222448
9. Hilton L, Hempel S, Ewing BA, et al. Mindfulness Meditation for Chronic Pain: systematic Review and Meta-analysis. Ann Behav Med. 2016;51(2):199–213.
10. Soundararajan K, Prem V, Kishen TJ. The effectiveness of mindfulness-based stress reduction intervention on physical function in individuals with chronic low back pain: systematic review and meta-analysis of randomized controlled trials. Complement Ther Clin Pract. 2022;49:101623. doi:10.1016/j.ctcp.2022.101623
11. Greenberg J, Mace RA, Bannon SM, Kulich RJ, Vranceanu A-M. Mind-body activity program for chronic pain: exploring mechanisms of improvement in patient-reported, performance-based and ambulatory physical function. J Pain Res. 2021;14:359–368. doi:10.2147/JPR.S298212
12. Murray CB, Patel KV, Twiddy H, Sturgeon JA, Palermo TM. Age differences in cognitive–affective processes in adults with chronic pain. Eur J Pain. 2021;25(5):1041–1052. doi:10.1002/ejp.1725
13. Nakad L, Booker S, Gilbertson-White S, Shaw C, Chi N-C, Herr K. Pain and multimorbidity in late life. Curr Epidemiol Rep. 2020;7(1):1–8. doi:10.1007/s40471-020-00225-6
14. Salive ME. Multimorbidity in older adults. Epidemiol Rev. 2013;35(1):75–83. doi:10.1093/epirev/mxs009
15. LaRowe LR, Williams DM. Activity-induced pain as a predictor of sedentary behavior among midlife adults with chronic pain. Res Q Exerc Sport. 2023;19:1–7. doi:10.1080/02701367.2023.2222783
16. LaRowe LR, Williams DM . Activity-induced pain as a predictor of physical activity behavior among individuals with chronic pain: the role of physical activity enjoyment. J Behav Med. 2022;1–11. doi:10.1007/s10865-021-00246-6
17. Suorsa K, Pulakka A, Leskinen T, Pentti J, Vahtera J, Stenholm S. Changes in prolonged sedentary behaviour across the transition to retirement. Occup Environ Med. 2021;78(6):409–412. doi:10.1136/oemed-2020-106532
18. Bernaards CM, Hildebrandt VH, Hendriksen IJ. Correlates of sedentary time in different age groups: results from a large cross sectional Dutch survey. BMC Public Health. 2016;16(1):1–12. doi:10.1186/s12889-016-3769-3
19. Greenberg J, Popok PJ, Lin A, et al. A mind-body physical activity program for chronic pain with or without a digital monitoring device: proof-of-concept feasibility randomized controlled trial. JMIR Form Res. 2020;4(6):e18703. doi:10.2196/18703
20. Park ER, Traeger L, Vranceanu A-M, et al. The development of a patient-centered program based on the relaxation response: the Relaxation Response Resiliency Program (3RP). Psychosomatics. 2013;54(2):165–174. doi:10.1016/j.psym.2012.09.001
21. Rodriguez CS. Pain measurement in the elderly: a review. Pain Manag Nurs. 2001;2(2):38–46. doi:10.1053/jpmn.2001.23746
22. Farrar JT, Young JP Jr, LaMoreaux L, Werth JL, Poole RM. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2001;94(2):149–158. doi:10.1016/S0304-3959(01)00349-9
23. Gewandter JS, Dworkin RH, Turk DC, et al. Improving study conduct and data quality in clinical trials of chronic pain treatments: IMMPACT recommendations. J Pain. 2020;21(9–10):931–942. doi:10.1016/j.jpain.2019.12.003
24. World Health Organization. World Health Organization: International Classification of Functioning, Disability and Health: ICF. Geneva: World Health Organization; 2001.
25. Üstün TB, Kostanjsek N, Chatterji S, Rehm J. Measuring Health and Disability: Manual for WHO Disability Assessment Schedule WHODAS 2.0. World Health Organization; 2010.
26. Cain KL, Conway TL, Adams MA, Husak LE, Sallis JF. Comparison of older and newer generations of ActiGraph accelerometers with the normal filter and the low frequency extension. Int J Behav Nutr Phys Act. 2013;10(1):1–6. doi:10.1186/1479-5868-10-51
27. Redelmeier DA, Bayoumi AM, Goldstein RS, Guyatt GH. Interpreting small differences in functional status: the Six Minute Walk test in chronic lung disease patients. Am J Respir Crit Care Med. 1997;155(4):1278–1282. doi:10.1164/ajrccm.155.4.9105067
28. Luke A, Dugas LR, Durazo-Arvizu RA, Cao G, Cooper RS. Assessing physical activity and its relationship to cardiovascular risk factors: NHANES 2003–2006. BMC Public Health. 2011;11(1):387. doi:10.1186/1471-2458-11-387
29. Morone NE, Greco CM. Mind–body interventions for chronic pain in older adults: a structured review. Pain Med. 2007;8(4):359–375. doi:10.1111/j.1526-4637.2007.00312.x
30. Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J R Stat Soc B: Stat Methodol. 1995;57(1):289–300.
31. Feingold A. New approaches for estimation of effect sizes and their confidence intervals for treatment effects from randomized controlled trials. Quant Meth Psych. 2019;15(2):96–111. doi:10.20982/tqmp.15.2.p096
32. Feingold A. A regression framework for effect size assessments in longitudinal modeling of group differences. Rev Gen Psychol. 2013;17(1):111–121. doi:10.1037/a0030048
33. Feingold A. Effect sizes for growth-modeling analysis for controlled clinical trials in the same metric as for classical analysis. Psychol Methods. 2009;14(1):43–53. doi:10.1037/a0014699
34. Wetherell JL, Petkus AJ, Alonso‐Fernandez M, Bower ES, Steiner AR, Afari N. Age moderates response to acceptance and commitment therapy vs. cognitive behavioral therapy for chronic pain. Int J Geriatr Psychiatry. 2016;31(3):302–308. doi:10.1002/gps.4330
35. Fishbein JN, Tynan M, Truong L, Wetherell JL, Herbert MS. Age differences in acceptance and commitment therapy for chronic pain. J Contextual Behav Sci. 2023;30:106–111. doi:10.1016/j.jcbs.2023.09.006
36. Harvey JA, Chastin SF, Skelton DA. Prevalence of sedentary behavior in older adults: a systematic review. Int J Environ Res Public Health. 2013;10(12):6645–6661. doi:10.3390/ijerph10126645
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Use of QR Codes for Promoting a Home-Based Therapeutic Exercise in Patients with Lumbar Disc Herniation and Lumbar Spinal Stenosis: A Prospective Randomized Study
Chang MC, Park D, Choo YJ
Journal of Pain Research 2022, 15:4065-4073
Published Date: 23 December 2022
Association Between Timed Up-and-Go Test and Future Changes in the Frailty Status in a Longitudinal Study of Japanese Community-Dwelling Older Adults
Wada Y, Shojima K, Tamaki K, Mori T, Kusunoki H, Onishi M, Tsuji S, Matsuzawa R, Nagai K, Sano K, Hashimoto K, Goto M, Nagasawa Y, Shinmura K
Clinical Interventions in Aging 2023, 18:1191-1200
Published Date: 28 July 2023
A Study of the Effect of Treatment On the Clinical Profile, Pain, and Disability in Migraine Patients Seen in a Tertiary Hospital
Kandasamy G, Almaghaslah D, Almanasef M, Almeleebia TM, Orayj K, Siddiqua A, Shorog E, Alshahrani AM, Prabahar K, Veeramani VP, Amirthalingam P, Alqifari S, Alshahrani N, AlSaedi AH, A Alsaab A, Aljohani F, Begum MY, Atiya A
Journal of Multidisciplinary Healthcare 2024, 17:3525-3534
Published Date: 22 July 2024
Disability in Older Adults with COPD: Prevalence, Assessment, and Influencing Factors — A Scoping Review
Huang X, Li H, Yao H, Ma P, Chen H, Zhang Y, Duan W, Yan X
Clinical Interventions in Aging 2026, 21:610177
Published Date: 22 June 2026