Back to Journals » Journal of Pain Research » Volume 19
Understanding Practitioner Comfort and Educational Priorities for Safe Opioid Prescribing: A Repeated Cross-Sectional Study
Authors Lai B ![]() , Cunningham J, Grimm JA, Olatoye D, Enke H
, Cunningham J, Grimm JA, Olatoye D, Enke H ![]()
Received 10 March 2026
Accepted for publication 19 June 2026
Published 26 June 2026 Volume 2026:19 606579
DOI https://doi.org/10.2147/JPR.S606579
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 1
Editor who approved publication: Professor Robert B. Raffa
Benjamin Lai,1 Julie Cunningham,2 Jessica A Grimm,3 Dare Olatoye,4 Halena Enke4
1Department of Family Medicine, Mayo Clinic, Rochester, MN, USA; 2Department of Pharmacy, Mayo Clinic, Rochester, MN, USA; 3Department of Quantitative Health Sciences, Mayo Clinic, Rochester, MN, USA; 4Division of Pain Medicine, Mayo Clinic, Rochester, MN, USA
Correspondence: Benjamin Lai, Department of Family Medicine Mayo Clinic, 200 First Street SW, Rochester, MN, 55905, USA, Tel +1 507 284 5300, Fax +1 507 284 5067, Email [email protected]
Background: The Centers for Disease Control and Prevention (CDC) released revised opioid prescribing guidelines in 2022 to address unintended harms associated with its original 2016 guidelines and to emphasize individualized care, shared decision-making, and appropriate screening for opioid use disorder. The extent to which clinicians are aware of and feel prepared to apply these revised recommendations remains unclear.
Methods: In a repeated cross-sectional study, we conducted an anonymized electronic survey of attendees to a nationally recognized annual opioid conference from 2022 to 2024 to assess familiarity with CDC opioid prescribing guidelines, perceived competence in chronic opioid management, and comfort with guideline application. Attendees included physicians, advanced practice providers (encompassing nurse practitioners and physician assistants), pharmacists, nurses, researchers and hospital/clinic administrators. Survey responses were compared across self-identified academic versus non-academic practice types, urban versus rural settings, and clinician roles.
Results: Across the three years, 72.3% of attendees completed the survey. No significant differences were observed between rural and urban clinicians in guideline familiarity or perceived competence. Academic clinicians were significantly more likely than non-academic clinicians to report the presence of institutional acute opioid prescribing guidelines. Clinicians with higher self-reported competence, particularly those in academic settings, had higher odds of perceiving that applying CDC guidelines and using opioid risk assessment tools require high levels of expertise. Differences by years of experience were not statistically significant.
Conclusion: These findings suggest meaningful variation in perceived competence between academic and non-academic clinicians and highlight potential educational opportunities needed to put prescribing guidelines into practice. Continued efforts to disseminate clear, practical guidance and provide targeted education may support safer, more confident opioid prescribing across diverse practice settings.
Keywords: CDC opioid prescribing guidelines, opioids, pain management, opioid prescribing, academic versus non-academic
Introduction
The Centers for Disease Control and Prevention (CDC) released opioid prescribing guidelines in 2016 to assist clinicians—particularly those in primary care—with initiating and managing opioid therapy for chronic non-cancer pain.1 Although intended to support best practices in response to the opioid epidemic, the guidelines led to several unintended consequences. These included rigid and inappropriate application, including use in populations explicitly excluded in the guidelines (such as patients with cancer-related pain or those in hospice). For example, shortly after the publication of the 2016 guidelines, several US States passed legislation to restrict the amount of opioids a patient was able to receive,2–4 with multiple national pharmacy chains adapting similar policies,5,6 which in some cases, delayed access of opioids for vulnerable patients, including those with end-of-life pain.4 Reports of abrupt opioid discontinuations, rapid tapers, and reports of patient abandonment were also published.3,4,7–9 An increasing number of studies have demonstrated the association between opioid tapering and increased risk of psychiatric destabilization,10,11 suicidality,12,13 and pain-related emergency department visits and hospitalizations.14,15 Meanwhile, opioid-involved overdose deaths continued to rise in the years following the 2016 publication.16,17
In response, the CDC issued revised guidelines in November 2022 emphasizing shared decision-making, individualizing care through clinical judgment, and cautioning against inflexible guideline implementation.18 The term “chronic pain” was removed from the guideline title, as the revised recommendations more precisely define and address acute, subacute and chronic pain. The update also underscored the importance of screening for opioid use disorder (OUD) and offering medications for OUD, such as buprenorphine.
The extent to which these guidelines influence prescribing practices remains uncertain. Opioid prescribing had already begun to decline before the 2016 guidelines,19 and it is unclear how widely or consistently the 2022 recommendations have been incorporated into routine practice. Further evaluation is needed to understand adoption patterns across clinical settings and their impact on patient care and opportunities for educational focus.
To this end, we conducted a repeated cross-sectional study whereby we deployed a confidential, anonymized electronic survey to multidisciplinary medical practitioners who attended a nationally recognized annual opioid conference hosted by our institution from 2022 to 2024 (3 cohorts) to assess awareness and knowledge of the 2022 revised CDC opioid prescribing guidelines, comfort applying these guidelines in clinical practice, and perceptions of the knowledge needed to use them effectively. We also compared responses between clinicians in academic settings (ie. those working in academic or university medical centers and usually involved in medical education and/or research) versus non-academic settings (ie. those working in private practice, independent clinics, community hospitals not affiliated with an academic medical center with limited to no formal teaching/research obligations). This is an important comparison as those in academic settings may be more aware of and to adapt latest guidelines given their responsibilities in education and research.
Materials and Methods
Study Setting
Our institution’s annual Opioid Conference, “Mayo Clinic Opioid Conference: Evidence, Clinical Considerations and Best Practice”, is a nationally recognized continuous medical education (CME) course spanning 3 days.20 The conference has been in existence since 2017 (not held in 2020 due to the COVID-19 pandemic) and offers CME credits for physicians, nurses and nurse practitioners, physician assistants, and pharmacists. Since 2021, the course has been offered in a hybrid format with attendees participating virtually and in-person. Topics of the conference range from interventional modalities, medications for opioid use disorder (MOUD), opioid prescribing guideline reviews, urine drug test result interpretations, and legal matters related to opioid prescribing. The conference took place between September 29-October 1, 2022 in Palm Springs, California; September 21-September 23, 2023 in Phoenix, Arizona; and September 19–21, 2024 in San Diego, California.
Survey Design
The survey was conducted electronically and contained 15 multiple-choice items. The first 6 items were related to demographics, which includes practice setting type. Items 7 and 8 inquired about the presence of acute opioid prescribing guidelines in the respondent’s institution, and whether opioid prescribing metrics are collected and made available for individual clinicians or department leadership to review, respectively (answer choices were yes, no, and unsure). Items 9 and 10 assess the respondent’s perceived level of competency related to opioid management, and the level of competency that respondents feel is necessary to manage patients using chronic opioids. These items were scored on a 5-point Likert scale ranging from None/No competency (1) to Expert competency (5). The remaining items assess respondents’ familiarity with the CDC opioid prescribing guidelines, comfort level in communicating with patients on chronic opioids, familiarity with opioid prescribing best practices and guidelines, ability to stay on time when seeing patients on chronic opioids and confidence level in screening those on chronic opioids for OUD (see Figures 1 and 2 for our questionnaire).
Figure 1 2022 Version of Survey. Figure 1 continued. Figure 2 2023 and 2024 Version of Survey. Figure 2 continued.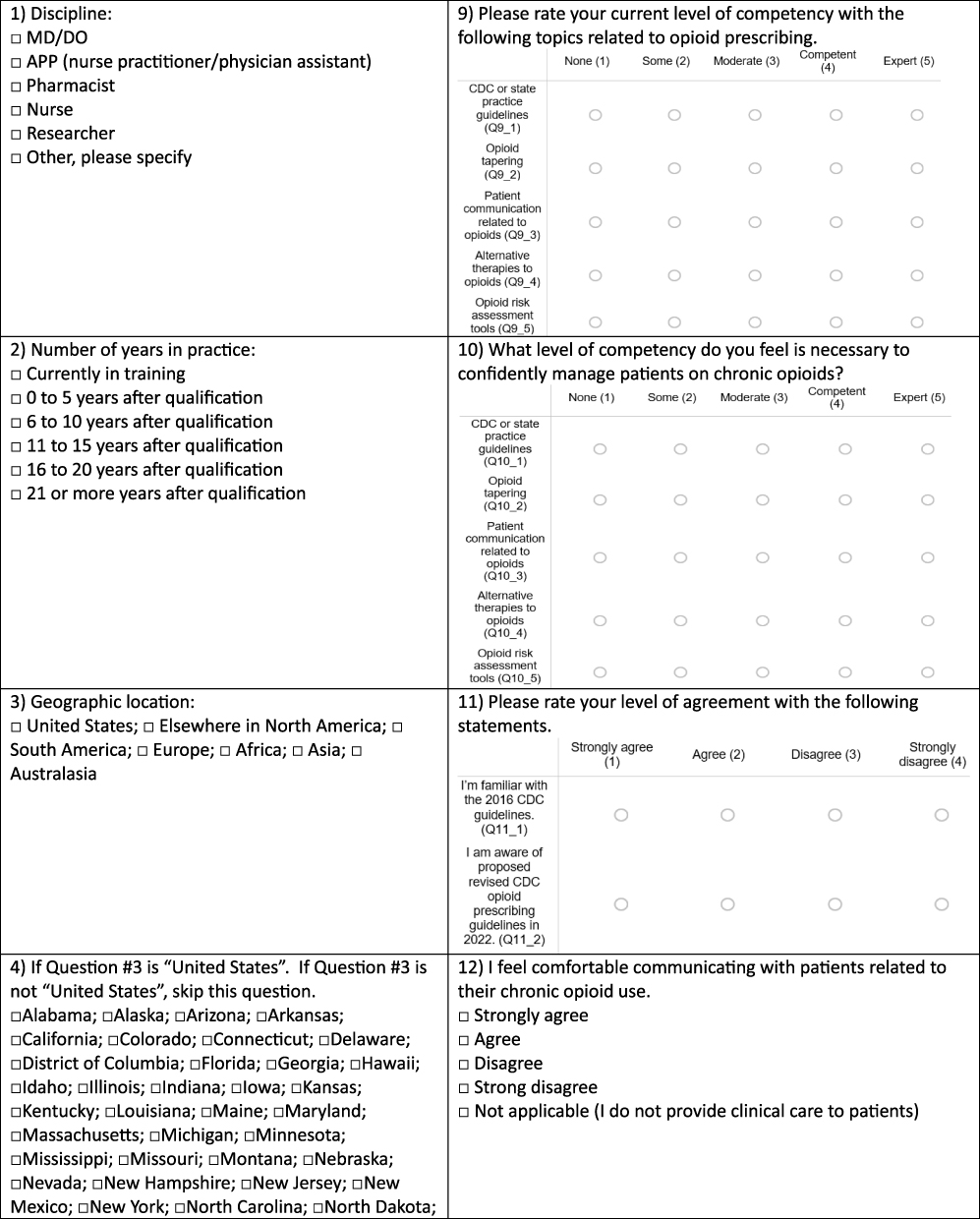
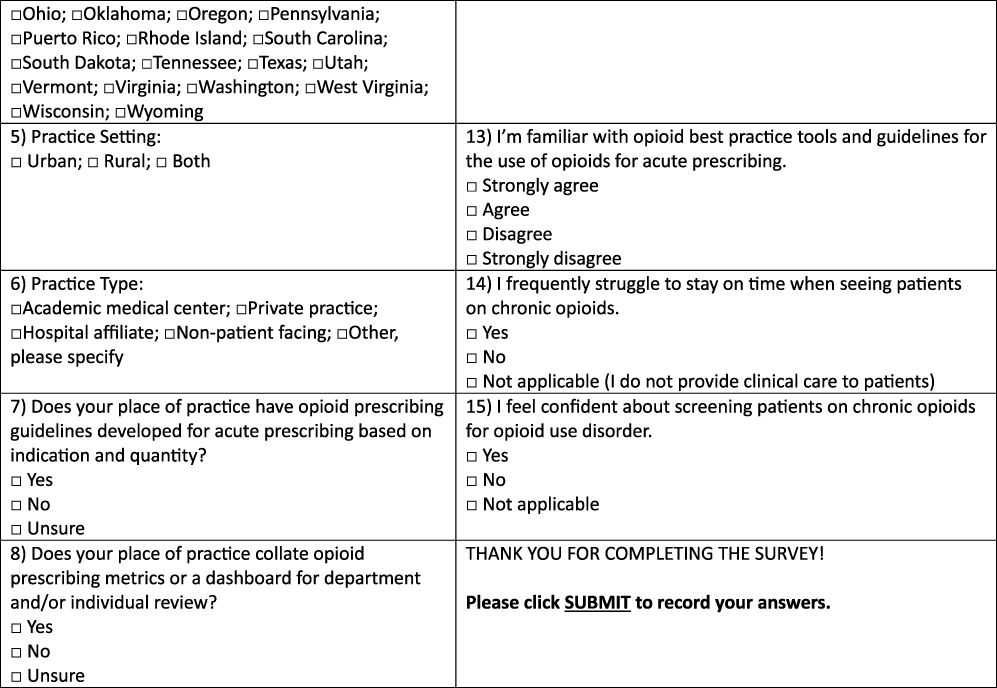
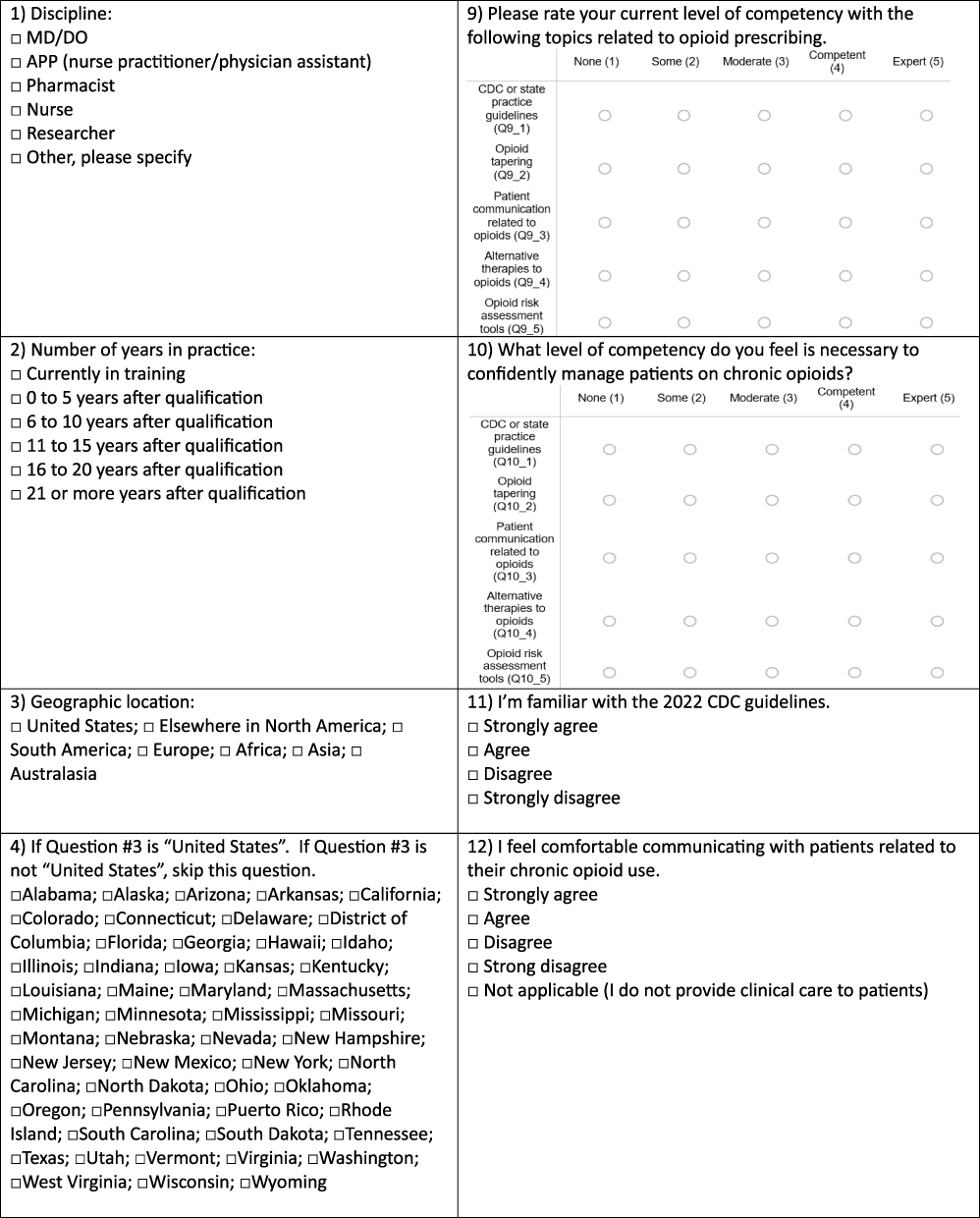
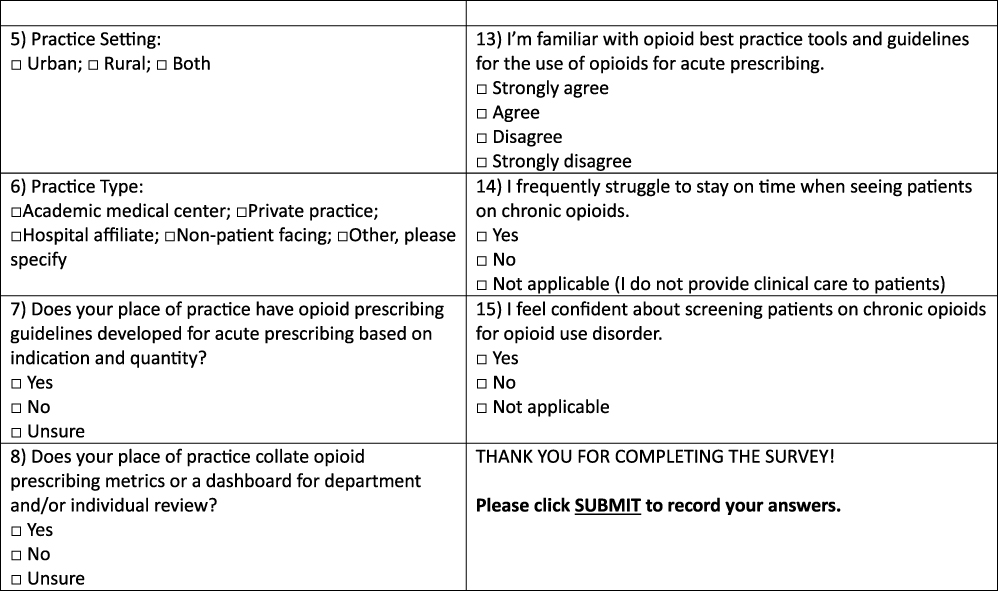
Item 11 in our 2022 survey differs from that of 2023 and 2024; this item assessed respondents’ familiarity with CDC opioid prescribing guidelines. When our 2022 survey was deployed, the revised 2022 CDC guidelines had not yet been published, although there was communication from the CDC about its upcoming publication. Therefore, in the 2022 version of the survey, respondents were asked about their familiarity with the 2016 CDC guidelines, and separately, about their awareness of the proposed revised CDC opioid prescribing guidelines in 2022 (Figure 1). In 2023 and 2024, Item 11 only assessed respondents’ familiarity with the 2022 CDC guidelines (Figure 2).
We sought assistance from our institution’s Research Survey Center to verify the language and clarity of our questions. Neither patients nor members of the public were involved in the conceptualization, design and conduct of the study as our primary focus was on clinicians’ familiarity with CDC guidelines. This study was reviewed by our Mayo Clinic’s Institution Review Board (IRB) and was determined to be exempt from ethical/IRB review under 45 CFR 46.102.
Survey Pilot Testing
Six participants (3 physicians, 1 nurse practitioner, 1 pharmacist, and 1 administrator) were asked to pilot-test the survey and provide feedback on the content, length, and language of the survey. All respondents took less than 10 minutes to complete the survey. This was not a validated survey.
Survey Deployment
All conference attendees were required to provide an Email address at the time of registration. Basic demographic information, such as region of practice and specialty, was collected as part of conference registration.
The confidential and anonymized electronic survey was deployed to all registered conference attendees 1 day prior to conference start date. The electronic survey was sent to the Email address that attendees used to register for the conference. A reminder Email was sent on each of the 3 conference days in 2022. In 2023 and 2024, in addition to the reminders in each of the conference days, we added a final reminder 2 days after the conference end date based on attendee feedback in 2022. The survey was open until 1 week after the last day of the conference. All conference attendees were eligible and were informed that completing the survey was entirely voluntary; no incentives or compensation were provided for participation. All participants provided informed consent.
Data Analysis
Demographic and characteristics of conference attendees are summarized. Categorical variables are reported as count and percentages.
Fisher’s Exact Test and trend test for ordinal variables were used to compare survey responses between practice setting (urban, rural, or both) and practice type (academic or non-academic). Wilcoxon Rank Sum Test was used to determine if there was a potential difference in the percentage of physicians compared to advanced practice providers (APPs), which include nurse practitioners and physician assistants, and years of experience.
Respondents were asked about their current level of competence on topics related to opioid prescribing and the level of competency needed in those topics to manage patients on chronic opioids. These topics included current competence with CDC/state practice guidelines, opioid tapering, patient communication related to opioids, alternative therapies, and opioid risk assessment tools. Ordinal logistic regression was used to assess the potential association between level of increasing current competence reported on these topics and the outcome of perceived necessary competence level, stratified by academic and non-academic and survey years. Competence level was multinomial with the following answer options: none, some, moderate, competent, and expert (see Figures 1 and 2 for our original survey). A p-value of <0.05 was considered statistically significant. Statistical analyses were performed using RStudio (version 4.5.1, Posit team (2025). RStudio: Integrated Development Environment for R. Posit Software, PBC, Boston, MA. URL http://www.posit.co/).
Results
Conference Attendee Demographics
From 2022 to 2024, 700 individuals attended the conference. Attendee demographics, including regions of practice, specialty of practice, and discipline (ie. physician, APPs, nurse, pharmacist, researcher) are summarized in Table 1. The majority of attendees practiced in Family or Internal Medicine, were physicians or APPs, and were from the Midwest and Western regions of the United States.21
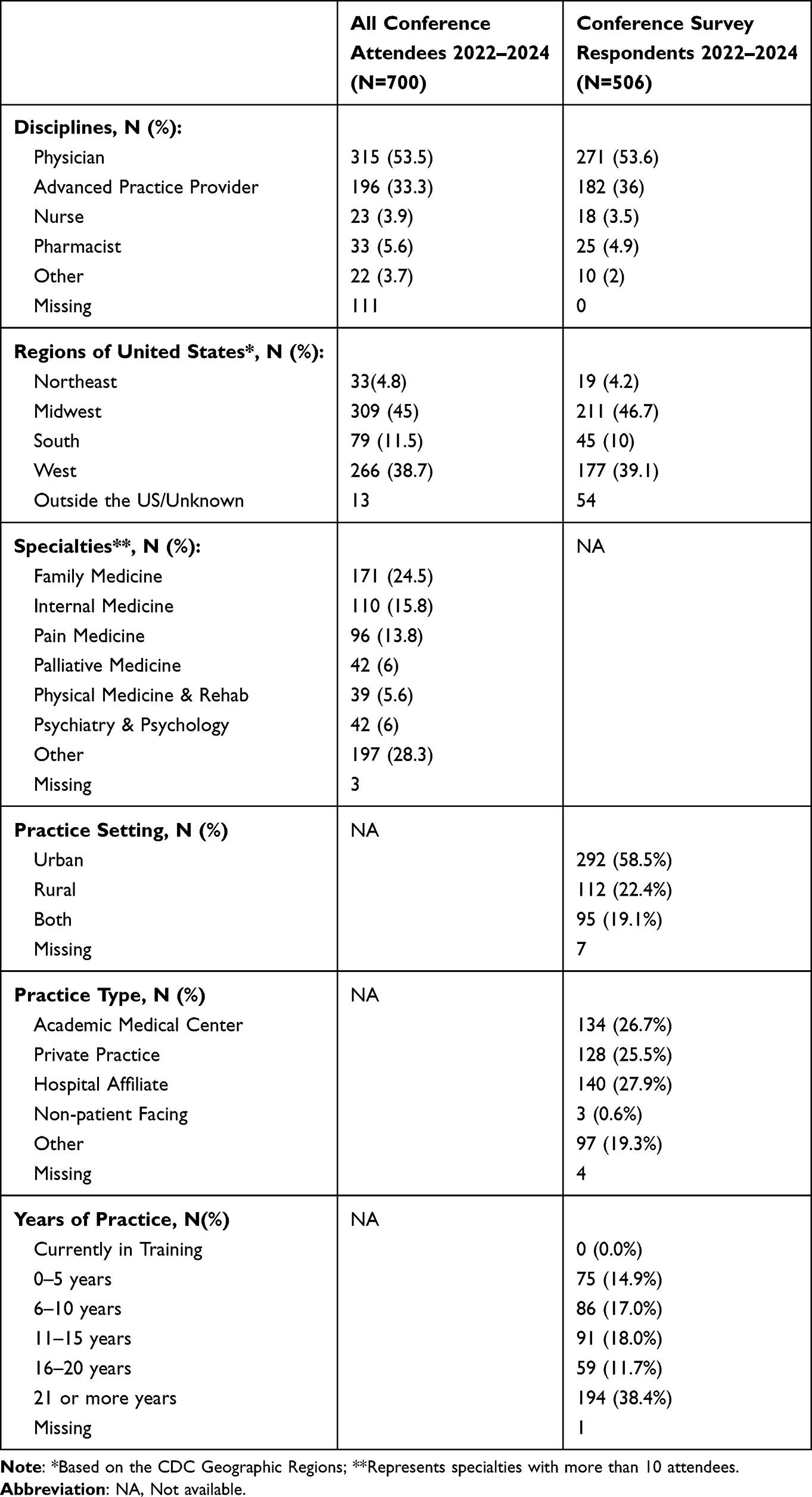 |
Table 1 Demographics |
Survey Response
Survey respondent demographics are summarized in Table 1. Across the 3 years (2022–2024), 72.3% attendees completed the survey (54.2% in 2022, 51.9% in 2023, and 83.6% in 2024). The survey respondents and the total conference attendee population discipline type and regional demographics were proportionally consistent.
Greater than half of respondents reported a discipline of physician (MD/DO; 53.6%), and 38.4% of respondents report 21 or more years of practice.
Rural versus Urban Comparison
We found no significant differences in the presence of institutional opioid prescribing guidelines and metrics available between rural and urban practitioners. There were no significant differences found in the level of familiarity with opioid prescribing guidelines between these groups. Similarly, no between-group differences were found in the perceived level of competence required to apply guidelines, opioid tapering, communicating with patients about opioids, use of alternate pain management therapies, and using the opioid risk assessment tools. In sum, there were no statistically significant differences found in any of our surveyed items between rural and urban practitioners.
Respondent Clinician Type and Years of Experience
There was a significant difference between clinician type (MD/DO vs APP) and years of experience, where MD/DOs (median of 6 years) have more years of experience after qualification compared to APPs (median of 3.5 years). Other disciplines were not compared due to small sample size. There were no statistical differences found in any of the surveyed item responses between clinician type and years of experience.
Academic versus Non-Academic Comparison
During all three survey years, there was a significant difference between academic and non-academic respondents in having opioid prescribing guidelines developed for acute prescribing/indications, with more academics reporting opioid prescribing guidelines during each survey year than non-academic respondents (p<0.05 for all, Table 2).
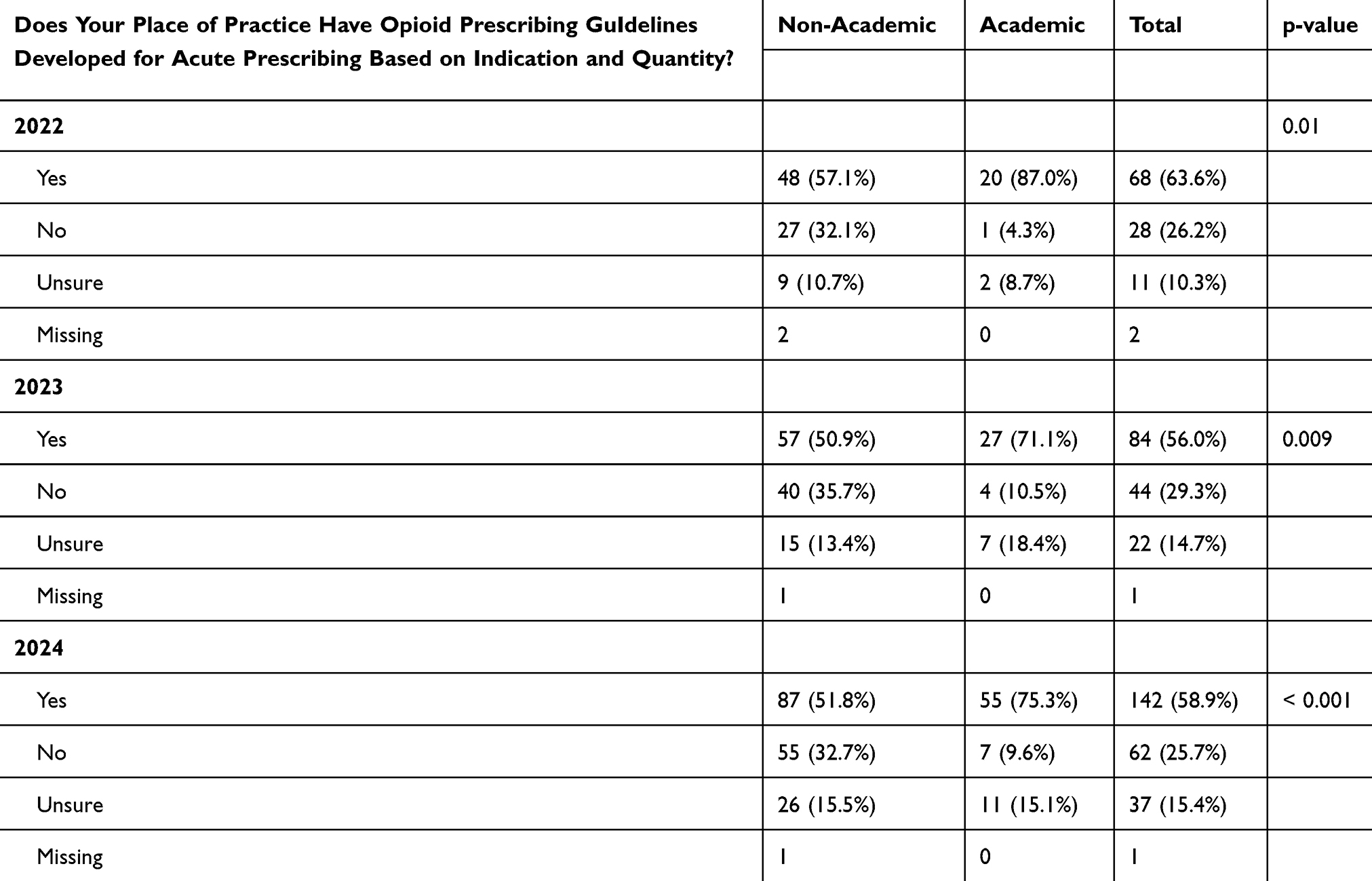 |
Table 2 Presence of Opioid Prescribing Guidelines for Acute Prescribing for Non-Academic versus Academic Survey Respondents |
Over time, for each increasing level of competence reported in academic respondents (versus non-academic respondents), there was an increased odds of respondents stating that greater competence is needed to apply CDC/state practice guidelines, opioid tapering, patient communication related to opioids, alternative therapies, and opioid risk assessment tools (see Table 3 for odds ratios and 95% confidence intervals across all 3 surveyed years). Interestingly, in 2022, academics had decreased odds (compared to non-academics) in reporting high competence in prescribing guidelines needed to manage patients on chronic opioids; the odds reversed by 2023. The same increased odds were seen for non-academics but to a lesser degree (Table 3).
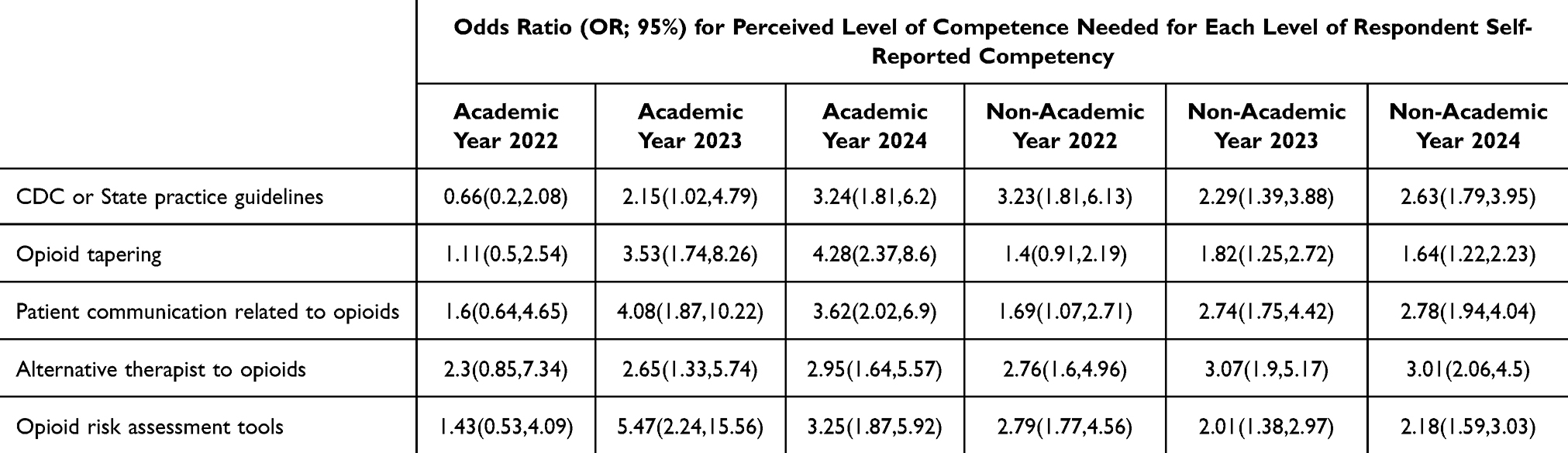 |
Table 3 Ordinal Logistic Regression for Outcomes of Opioid Topics and Perceived Necessary Competence Level, Stratified by Year and Practice Type |
Discussion
To our knowledge, this was the first multi-year survey study assessing familiarity with CDC opioid prescribing guidelines and respondent attitudes on competence levels needed to manage patients on opioids and implement guidelines in clinical practice.
We found a statistically significant difference between academic and non-academic respondents in the presence of opioid prescribing guidelines for acute pain indications in our sample. More academic respondents reported having acute prescribing guidelines in their institution than their non-academic peers. These findings may help explain prior research demonstrating higher pain assessment competence among academic clinicians.22 Although we found a significant difference between academic and non-academic respondents in collating or having access to opioid prescribing metrics in 2022, this difference no longer existed in 2023 and 2024. This may signal a more widespread institutional awareness of prescribing metrics and efforts to address opioid stewardship in the years following the publication of the revised CDC guidelines in 2022.
Our findings seem to suggest that clinicians working in academic settings and those who reported higher competence in opioid prescribing may be more likely than non-academic clinicians to believe that applying CDC’s guidelines in practice and appropriately using opioid risk assessment tools require greater expertise. While a similar pattern was seen among non-academic clinicians, highly competent clinicians in this group seemed less likely to say that high competence or expertise is required. This belief seems consistent with previous findings showing CDC guideline awareness was associated with enhanced confidence in treating patients with chronic non-cancer pain.23
The discrepancies between academic versus non-academic clinicians on perceived competence may be related to the heightened awareness of prescribing guidelines among those working in academic settings, and the fact that they are more likely to train learners on these guidelines. This is supported by a prior study indicating that a higher percentage of academic (versus non-academic) pain physicians have completed a pain medicine fellowship or training in neurology, admit patients to hospital for aggressive management for severe pain, and have an interdisciplinary practice within institutions that conduct research.24 Non-pain specialists in academic settings were also found to have greater access to pain specialist consultants compared to non-pain specialists in non-academic settings.22 Furthermore, previous studies demonstrated that managing chronic pain to be particularly stressful for trainees,25 which could further reinforce academic clinicians’ perception that a high level of competence is required to manage this patient population. Taken together, academic clinicians may need more in-depth knowledge of opioid prescribing guidelines in order to train learners, conduct research, and participate in interdisciplinary team practices.
Academic clinicians may also be more likely to encounter patients with higher medical complexity in tertiary referral centers and thus may feel the need for higher competence to manage patients with chronic pain. Studies to date, however, point to similar patient complexity between primary care and tertiary care,26 and in fact, patients with co-occurring mental health complexities are more likely to have their referrals declined for tertiary pain care.27
The interaction between years of experience and perceived level of competence needed to implement CDC guidelines was not statistically significant, which could suggest that perceived level of competence may be more related to prior training and level of exposure to guidelines rather than years of experience. However, we acknowledge that due to our relatively small sample size, we may lack adequate power to make this assertion. Future studies surveying a larger sample of academic and non-academic clinicians beyond our conference venues are being considered to determine whether this non-significant interaction persists in a larger sample.
This study has several important limitations. Survey respondents were all attendees of our institution’s annual opioid conference, which was held in the western region of the United States during all 3 years. We acknowledge that respondents are likely a self-selected group of practitioners with a vested interest in learning more about opioid prescribing and pain management; they are also more likely to work within institutions where Continuing Medical Education funds and time allowance are available. Practitioners working in other regions of the country, those who are unaware of our conference, and those who are aware but did not register may have different levels of comfort, attitudes and knowledge of the CDC guidelines. Moreover, conference attendees who did not respond to the survey may also have different characteristics, comfort levels, and attitudes regarding opioid prescribing guidelines and management. Therefore, selection bias likely played a role, and our results may not be entirely generalizable. As well, we were unable to differentiate between survey respondents who attended our conference virtually versus in-person; these 2 groups may differ in knowledge and perceptions. Future efforts to assess differences in response between virtual and in-person attendees are being considered.
Finally, we acknowledge that some practitioners may have concerns related to CDC guidelines, which could influence their survey responses. Concerns raised and published include the strength of supporting evidence underlying CDC’s recommendations and inter-individual variability in opioid responses,28,29 as well as the need for greater clarity around shared decision making in pain management – a concept emphasized in the revised guidelines.30
Conclusion
Across all 3 survey years of our study, we found that academic clinicians were more likely than non-academic clinicians to report having opioid prescribing guidelines for acute pain management in their workplace. Over time, academic clinicians who reported higher competence were also more likely to state that a high level of competence is needed to appropriately implement elements of CDC’s opioid prescribing guidelines into clinical practice.
These findings underscore the need for targeted educational support for non-academic clinicians to promote guideline-concordant pain management and improve familiarity with CDC guidelines in non-academic settings. The association between greater self-reported competence and higher perceived competency requirements also suggests that longitudinal opioid prescribing training may be more effective than one-time education efforts.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, BL, upon reasonable request.
Acknowledgments
The authors acknowledge and are deeply grateful for the assistance of Lisa Winter, MA, PMP of Mayo Clinic School of Continuous Professional Development for collating conference attendee demographic data and for her dedication in coordinating Mayo Clinic’s annual Opioid Conference.
Disclosure
Benjamin Lai, MB BCh BAO, receives financial support for research through Mayo Clinic’s Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery. All other authors declare they do not have any conflicts of interest in this work.
References
1. Dowell D, Haegerich TM, Chou R. CDC Guideline for Prescribing Opioids for Chronic Pain - United States, 2016. MMWR Recomm Rep. 2016;65(1):1–12. doi:10.15585/mmwr.rr6501e1
2. Buonora MJ, Hanna DB, Zhang C, et al. U.S. state policies on opioid prescribing during the peak of the prescription opioid crisis: associations with opioid overdose mortality. Int J Drug Policy. 2022;110:103888. doi:10.1016/j.drugpo.2022.103888
3. Dowell D, Haegerich T, Chou R. no shortcuts to safer opioid prescribing. N Engl J Med. 2019;380(24):2285–2287. doi:10.1056/NEJMp1904190
4. Kroenke K, Alford DP, Argoff C, et al. Challenges with implementing the centers for disease control and prevention opioid guideline: a consensus panel report. Pain Med. 2019;20(4):724–735. doi:10.1093/pm/pny307
5. Walmart introduces additional measures to help curb opioid abuse and misuse. Walmart. Available from: https://corporate.walmart.com/news/2018/05/07/walmart-introduces-additional-measures-to-help-curb-opioid-abuse-and-misuse.
6. CVS Caremark® Opioid Quantity Limits Pharmacy Reference Guide. CVS Caremark. Available from: https://www.caremark.com/content/dam/enterprise/caremark/pdfs/Opioid_Reference_Guide.pdf.
7. Fenton JJ, Agnoli AL, Xing G, et al. Trends and rapidity of dose tapering among patients prescribed long-term opioid therapy, 2008-2017. JAMA Netw Open. 2019;2(11):e1916271. doi:10.1001/jamanetworkopen.2019.16271
8. Henry SG, Paterniti DA, Feng B, et al. Patients’ experience with opioid tapering: a conceptual model with recommendations for clinicians. J Pain. 2019;20(2):181–191. doi:10.1016/j.jpain.2018.09.001
9. “Not Allowed to Be Compassionate”: chronic Pain, the Overdose Crisis, and Unintended Harms in the US. 2018. Available from: https://www.hrw.org/report/2018/12/18/not-allowed-be-compassionate/chronic-pain-overdose-crisis-and-unintended-harms-us.
10. Agnoli A, Xing G, Tancredi DJ, Magnan E, Jerant A, Fenton JJ. Association of dose tapering with overdose or mental health crisis among patients prescribed long-term opioids. JAMA. 2021;326(5):411–419. doi:10.1001/jama.2021.11013
11. Fenton JJ, Magnan E, Tseregounis IE, Xing G, Agnoli AL, Tancredi DJ. Long-term risk of overdose or mental health crisis after opioid dose tapering. JAMA Netw Open. 2022;5(6):e2216726. doi:10.1001/jamanetworkopen.2022.16726
12. Oliva EM, Bowe T, Manhapra A, et al. Associations between stopping prescriptions for opioids, length of opioid treatment, and overdose or suicide deaths in US veterans: observational evaluation. BMJ. 2020;368:m283. doi:10.1136/bmj.m283
13. Larochelle MR, Lodi S, Yan S, Clothier BA, Goldsmith ES, Bohnert ASB. Comparative effectiveness of opioid tapering or abrupt discontinuation vs no dosage change for opioid overdose or suicide for patients receiving stable long-term opioid therapy. JAMA Netw Open. 5(8):e2226523. doi:10.1001/jamanetworkopen.2022.26523
14. Mark TL, Parish W. Opioid medication discontinuation and risk of adverse opioid-related health care events. J Subst Abuse Treat. 2019;103:58–63. doi:10.1016/j.jsat.2019.05.001
15. Magnan E, Tancredi DJ, Xing G, Agnoli A, Tseregounis IE, Fenton JJ. Association of opioid tapering with pain-related emergency department visits, hospitalizations, and primary care visits: a retrospective cohort study. Pain Med. 2025;26(4):199–206. doi:10.1093/pm/pnae121
16. James JR, Scott JM, Klein JW, et al. Mortality after discontinuation of primary care-based chronic opioid therapy for pain: a retrospective cohort study. J Gen Intern Med. 2019;34(12):2749–2755. doi:10.1007/s11606-019-05301-2
17. Dowell D, Nataraj N, Rikard M, Park J, Zhang K, Baldwin GT. Why have overdose deaths decreased? Widespread fentanyl saturation and decreased drug use among key drivers. Lancet Reg Health Am. 2025;51(101226):101226. doi:10.1016/j.lana.2025.101226
18. Dowell D, Ragan KR, Jones CM, Baldwin GT, Chou R. CDC Clinical Practice Guideline for Prescribing Opioids for Pain - United States, 2022. MMWR Recomm Rep. 2022;71(3):1–95. doi:10.15585/mmwr.rr7103a1
19. Guy GP Jr, Zhang K, Bohm MK, et al. Vital Signs: changes in Opioid Prescribing in the United States 2006-2015. MMWR Morb Mortal Wkly Rep. 2017;66(26):697–704. doi:10.15585/mmwr.mm6626a4
20. Mayo Clinic Opioid Conference. Evidence, clinical considerations and best practice 2026. mayo clinic school of continuous professional development. Available from: https://ce.mayo.edu/emergency-medicine/content/mayo-clinic-opioid-conference-evidence-clinical-considerations-and-best-practice-2026.
21. Health. United States: geographic division or region. National Center for Health Statistics, The Centers for Disease Control and Prevention. Available from:
22. Dale CM, Cioffi I, Novak CB, et al. Continuing professional development needs in pain management for Canadian health care professionals: a cross sectional survey. Can J Pain. 2023;7(1):2150156. doi:10.1080/24740527.2022.2150156
23. Ebbert JO, Philpot LM, Clements CM, et al. Attitudes, beliefs, practices, and concerns among clinicians prescribing opioids in a large academic institution. Pain Med. 2018;19(9):1790–1798. doi:10.1093/pm/pnx140
24. Breuer B, Pappagallo M, Tai JY, Portenoy RK. U.S. board-certified pain physician practices: uniformity and census data of their locations. J Pain. 2007;8(3):244–250. doi:10.1016/j.jpain.2006.08.009
25. Webster F, Bremner S, Oosenbrug E, Durant S, McCartney CJ, Katz J. From opiophobia to overprescribing: a critical scoping review of medical education training for chronic pain. Pain Med. 2017;18(8):1467–1475. doi:10.1093/pm/pnw352
26. Fink-Miller EL, Long DM, Gross RT. Comparing chronic pain treatment seekers in primary care versus tertiary care settings. J Am Board Fam Med. 2014;27(5):594–601. doi:10.3122/jabfm.2014.05.130311
27. Bosma R, Rosenbloom BN, Burke E, et al. An examination of referrals declined for chronic pain care: there is increasing mental health complexity within care-seeking patients with chronic pain over time. Can J Pain. 2024;8(1):2337074. doi:10.1080/24740527.2024.2337074
28. Nadeau SE, Lawhern RA. Use of opioids for chronic noncancer pain. a recapitulation of the science. letters to editor. Eur Soc Med Med Res Arch. 2025;13(3).
29. Lawhern RA. Doctors diagnosing addiction - are the blind leading the blind? Eur Society Med Med Res Arch. 2023;11(11). doi:10.18103/mra.v11i1.3135
30. Warner NS, Buonora MJ, Lai B, et al. Purposeful shared decision-making in caring for and with patients with chronic pain receiving opioid therapy. J Gen Intern Med. 2025;40(13):3232–3240. doi:10.1007/s11606-025-09535-1
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Utilizing Pharmacogenomics Results to Determine Opioid Appropriateness and Improve Pain Management in a Patient with Osteoarthritis
Pizzolato K, Thacker D, Del Toro-Pagán NM, Amin NS, Hanna A, Turgeon J, Michaud V
Pharmacogenomics and Personalized Medicine 2022, 15:943-950
Published Date: 7 November 2022
Evaluating the Effect of COVID-19 on Outpatient Opioid Utilization Among Health First Colorado Members and a National Non-Medicaid Cohort: An Interrupted Time Series Analysis
Anderson HD, Patterson VP, Wright G, Rawlings JE, Moore GD, Leonard J, Page RL II
Therapeutics and Clinical Risk Management 2023, 19:745-753
Published Date: 18 September 2023
Exploring Pain Clinical Specialists’ Perspectives on Opioid Optimization for Chronic Non-Malignant Pain in England
Alenezi A, Paudyal V, Yahyouche A
Journal of Pain Research 2025, 18:4037-4051
Published Date: 13 August 2025
The Role of the Multidisciplinary Team for Opioid Stewardship: A Scoping Review
Pg Abdul Haris DNNB, Sze Hui A, Islam N, Goh HP, Kifli N, Hall AD, Alrasheedy AA, KC B
Journal of Multidisciplinary Healthcare 2025, 18:7797-7810
Published Date: 2 December 2025