Back to Journals » Advances in Medical Education and Practice » Volume 17
Ultrasound-Guided Vascular Access Simulation-Based Educational Training Improves Skills and Confidence in Preclinical Medical Students: A Pilot Study
Authors Johns Z, Bellala V ![]() , Bi L
, Bi L ![]() , Warzecha H, Yeh J
, Warzecha H, Yeh J ![]() , Asher SR
, Asher SR ![]()
Received 3 March 2026
Accepted for publication 29 April 2026
Published 14 May 2026 Volume 2026:17 604095
DOI https://doi.org/10.2147/AMEP.S604095
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Sateesh Arja
Zachary Johns, Venkatsai Bellala, Lulu Bi, Haley Warzecha, Jasper Yeh, Shyamal R Asher
Department of Anesthesiology, The Warren Alpert Medical School of Brown University, Providence, Rhode Island, USA
Correspondence: Shyamal R Asher, Department of Anesthesiology, The Warren Alpert Medical School of Brown University, 593 Eddy Street, Davol #129, Providence, RI, 02903, USA, Email [email protected]
Purpose: Early development of the ultrasound skills relevant to a career in anesthesiology, like ultrasound-guided IV placement, is often overlooked in nationwide preclinical curricula. This single center, pilot study aims to compare the performance of preclinical medical students on their ultrasound guided vascular access skills before and after their participation in an ultrasound workshop.
Methods: Participants were administered a clinical simulation scenario for ultrasound-guided vascular access prior to undergoing an interactive educational ultrasound workshop. Students were randomized into a medical student teacher cohort or an attending physician teacher cohort. Two weeks later, the clinical scenario was re-administered. The clinical scenario involved simulation of attaining “vascular” access by cannulating an IV on a balloon within a tofu model. The clinical scenario was scored in accordance with the P-UGVA rating score; a composite score developed through a Delphi consensus study that evaluates eight elements of proficiency in ultrasound guided vascular access skills.
Results: Post-workshop performance scores from twelve medical students demonstrated increases from baseline across all eight P-UGVA domains (n=12, p< 0.005) for all students. There were no statistically significant differences in post-test performance between the medical student peer-teaching cohort and the attending physician teaching cohort across any category. Following the workshop, participants reported a greater degree of confidence using ultrasound, teaching another student basic ultrasound skills and a better understanding of peripheral vasculature anatomy.
Conclusion: The educational intervention of an ultrasound workshop was effective in improving preclinical student participants’ procedural efficiency and confidence in attaining ultrasound-guided vascular access on a tofu model. Medical students may be effective teachers of their peers for procedural skills. The small sample size limits the generalizability of this study.
Keywords: POCUS, ultrasound-guided IV placement, medical education, simulation training
Introduction
The incorporation of point-of-care ultrasound (POCUS) into modern clinical practice has transformed the diagnostic and interventional capabilities of numerous medical specialties. As a result, early exposure to ultrasound techniques in preclinical medical education has become more widespread, yielding a heightened understanding of anatomy, pathology, physical exam skills and clinical knowledge.1 Ultrasound has been demonstrated as a useful tool to bridge the basic and clinical science curricula of organ-based systems at medical schools and its incorporation into the preclinical curriculum has increased student confidence in using POCUS to detect pathology and make clinical decisions.2 Longitudinal ultrasound curriculum has been shown to improve preclinical exam performance in cardiovascular anatomy3 and improve OSCE performance among preclinical students.4
As early adopters of POCUS for nerve blocks and vascular access, anesthesiologists are at the forefront of wielding ultrasound techniques to augment clinical practice.5 Ultrasound education is a common feature of anesthesiology residency training and it is highly effective.6 While POCUS has been further incorporated into medical preclinical curricula nationwide, early development of the procedural ultrasound skills relevant to a career in anesthesiology, like ultrasound-guided IV placement, is often overlooked. In particular, most existing preclinical programs focus on image acquisition and interpretation, leaving less emphasis on the coordination, hand-eye skills, and needle guidance techniques required for real-time ultrasound-guided procedures.7 This represents a distinct educational gap for students who will later perform these procedures in high-acuity settings, including the operating room and emergency department.
Despite growing interest in the specialty, medical students have limited exposure to anesthesiology in the preclinical curriculum. However, preclinical elective courses on the basics of anesthesiology have been shown to augment student understanding of airway management, anesthetic pharmacology, basics of ultrasound and vascular access.8 Anesthesia-based simulation training has demonstrated improved basic induction skills and response to hemodynamic changes.9 No study has examined the effectiveness of ultrasound-guided vascular access simulation training in the context of the preclinical medical curriculum, despite being a high-yield procedural skill that builds foundational ultrasound competencies like probe handling, image acquisition, needle visualization and procedural ergonomics.
The main objective of this study is to compare participants’ procedural acumen of ultrasound-guided IV cannulation before and after an educational ultrasound workshop led by anesthesiology attending and medical students using a tofu model. Current approaches to teaching ultrasound-guided vascular access are limited by restricted access to human models and concerns regarding patient safety during novice skill acquisition. To address these challenges, this study utilizes a low-cost, tofu-based simulation model that provides a safe, reproducible environment for preclinical students to develop technical skills prior to clinical application.
Additionally, the study will compare student performance between the attending-teacher group and the student-teacher group. We hypothesized that participants would demonstrate significantly improved overall performance following the intervention with no difference between the attending-teacher group and student-teacher group. Performance was evaluated using the composite P-UGVA rating score. The P-UGVA score is a composite score developed through a Delphi consensus study and subsequently validated.10,11 It evaluates eight elements of proficiency in ultrasound guided vascular access skills; preparation of utensils, ergonomics, preparation of the ultrasound device, identification of blood vessels, anatomy, hygiene, coordination of the needle, and completion of the procedure.
Materials and Methods
Study Population
The study participants consisted of 9 first year and 3 second year medical students at the Warren Alpert Medical School of Brown University. Participants voluntarily signed up to participate in the workshop and the study. Participation in the study was not required and had no impact on participating in the rest of the workshop.
Ethics Statement
This study was reviewed by the Brown University Institutional Review Board and the study protocol was determined to be Exempt under review Category (2) (ii) regarding the inclusion of human participants in research in accordance with 45 CFR 46.104 and does not require consent documentation. (IRB ID# STUDY00000944). Participants received an introduction letter describing the study and their completion of the study indicated willingness to participate in the study.
Randomization
Participants were randomly split into two groups of six for the educational ultrasound workshop. Our approach entailed a stratified randomization based on class year (MS1 and MS2). Within each stratum, participants were assigned to study groups using a computer-generated random number generator. Random numbers were generated using Excel and were assigned to participant codes to ensure researcher blindness. Odd numbers were assigned to the attending physician teacher cohort. Even numbers were assigned to the medical student teacher cohort.
Ultrasound Workshop
This study took place in the context of a workshop series sponsored by the medical school’s Anesthesiology Student Interest Group. The workshop series was designed by the Student Interest Group to offer a longitudinal curriculum in anesthesiology to preclinical students. The entire first- and second-year student body was invited to participate and twenty students became regular participants. The workshop series included procedural workshops for skills like intubation, central line placement and TEE, as well as panel discussions regarding anesthesia basics, subspecialties of anesthesiology, research opportunities in the field. The peripheral ultrasound-guided IV placement portion of the workshop was led in two stations; one station with an attending anesthesiologist and one station with a second-year medical student, who had completed the same workshop series the prior year and trained in ultrasound-guided IV placement by the attending anesthesiologist in one 30-minute simulation session. To enhance reproducibility and ensure consistency across training sessions, the workshop was delivered using a standardized format. All participants underwent the same sequence of instruction, consisting of a brief didactic session introducing the principles of peripheral ultrasound-guided vascular access, a live demonstration of probe handling, vessel identification, and needle guidance, and a hands-on practice session using the tofu-based simulation model. The total workshop length was fixed across all sessions to minimize variability in exposure.
Instructors followed a uniform curriculum that outlined key teaching points, including hygiene, probe positioning, image optimization, identification of structures, and needle visualization. The same equipment, ultrasound settings, and tofu simulation materials were used for all participants. Additionally, instructor-to-participant ratios were kept consistent to ensure comparable levels of feedback. This approach minimized inter-instructor variability and ensured that all participants received equivalent training.
This educational intervention was rooted in the established pedagogy of deliberate practice. Deliberate practice emphasizes repeated performance of a skill with immediate feedback and opportunities for refinement. This is crucial for procedural skill acquisition. The workshop was therefore designed to provide iterative, hands-on practice with real-time instructor feedback.
Intervention
The intervention includes two arms: 1) a clinical simulation scenario and its effect on students’ skills, and 2) a tutorial of the scenario led by an attending physician or medical students. All participants were individually administered the clinical scenario immediately before attending the ultrasound tutorial. After this initial assessment, one group was instructed on how to complete the scenario by an attending physician while the second group was simultaneously taught the same in a separate room by two medical students, who had been instructed by the same attending. Two weeks later, participants were individually readministered the same clinical simulation and evaluated for their improvement.
Tofu Model
The tofu model included one block of firm tofu, red dye-filled long balloon, gloves, alcohol wipes, saline flush, tourniquet, transparent dressing, IV catheter, cannula leash, sterile ultrasound gel, and ultrasound machine. This model has been used in prior studies.12,13 To simulate venous access of the human forearm, the balloon was inserted length-wise into the tofu (Figure 1). The firm tofu provided resistance similar to subcutaneous tissue, while the dye-filled balloon approximated a compressible vein that could be visualized under ultrasound and yielded flash upon successful placement of the needle tip. The depth of the balloon within the tofu was mimicked typical forearm vein depth, allowing participants to practice needle angle, probe positioning, and hand-eye coordination during ultrasound-guided access. For each participant, a new model was set up to minimize damage or influence from access by previous participants. The tofu model is a necessary work-around of the practical limitations surrounding the use of cadaveric models, and safety concerns for novice procedural attempts on patients.
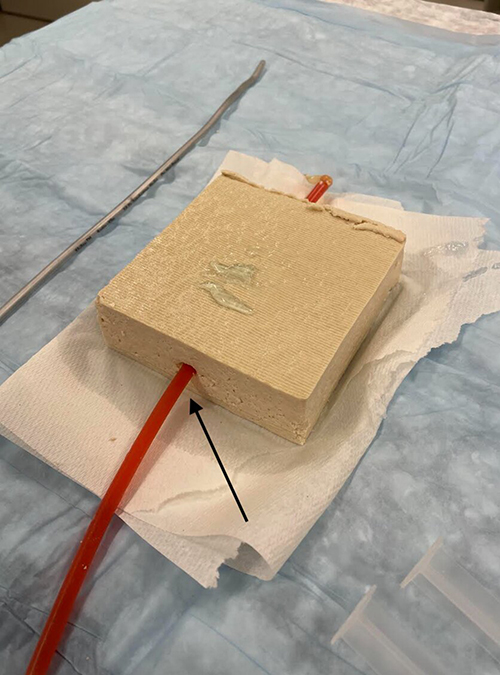 |
Figure 1 A picture depicting the Tofu-based simulation model for ultrasound guided peripheral vascular access. A red dye filed long balloon (black arrow) is inserted length wise into a block of firm tofu. |
Performance Assessment
Prior to the pre-assessment, participants completed a survey regarding their familiarity with ultrasound and IV cannulation (Appendix 1); they were administered another survey at the completion of the study regarding their confidence in completing such tasks (Appendix 2). Both pre- and post-assessments for participant completion of the simulation graded students using the P-UGVA rating score, a validated global rating scale for competence assessment of Peripheral Ultrasound-Guided Vascular Access (Appendix 3). The two evaluators were second-year medical students who were trained by an attending anesthesiologist on how to assess procedural acumen in ultrasound-guided IV skills using the P-UGVA rating score. Education in the P-UGVA rating score and evaluation of ultrasound acumen was provided by an attending anesthesiologist in a 30-minute didactic session. Evaluators were blinded to whether each participant was trained in the medical student or attending anesthesiologist cohort. Our assessment of two categories within the rating score, such as “Anatomy”, and “Identification of Blood Vessels” were altered due to the utilization of the tofu model rather than the human forearm. In lieu of assessing for identification of arteries and veins, students were asked how they would use ultrasound to differentiate between the two on a human forearm. Acceptable responses include evaluating vessel compressibility or doppler flow color technique. Each participant received one score from each evaluator for both pre- and post-assessments.
Statistical Analysis
All data were de-identified and analyzed to compare pre- and post-workshop outcomes. Descriptive statistics, including means and standard deviations, were calculated for demographic data and performance scores. The Shapiro–Wilk test assessed normality for all continuous variables. Primary outcomes (P-UGVA composite scores) were treated as continuous variables to facilitate parametric analysis and compared using paired t-tests for normally distributed data and Wilcoxon signed-rank tests for non-normally distributed data. To account for the increased risk of Type I error associated with testing multiple P-UGVA domains, p-values were adjusted using the Benjamini-Hochberg procedure. Practical significance for all pre- and post-workshop comparisons was evaluated by calculating effect sizes: Cohen’s d for parametric data and the rank-biserial correlation (r) for non-parametric data.
Secondary survey outcomes were summarized using descriptive statistics (means and standard deviations) and compared between pre- and post-workshop responses using the Wilcoxon signed-rank test. To evaluate the efficacy of peer versus attending physician teaching, post-test performance scores were compared using the Mann–Whitney U-test with associated rank-biserial correlation effect sizes due to small sample sizes (n=6 per group). Categorical survey items, such as probe selection, were analyzed using McNemar’s test. A p-value of p < 0.05 was considered statistically significant. All analyses were performed using R statistical software (Version 4.5.2).
Results
Twelve medical students (nine MS1, three MS2) participated in this simulation study, all completing the baseline simulation prior to an ultrasound-guided IV teaching workshop. Participants were randomized into two equal groups for the teaching intervention: a medical student peer-teaching group (n=6) and an attending physician teaching group (n=6).
Performance scores, calculated as the average of ratings from two independent evaluators, are presented in Figure 2a and b and Table 1. Normality testing via the Shapiro–Wilk test indicated normal distribution for all variables (p > 0.05) except “Hygiene” (W=0.834, p=0.024). Consequently, a Wilcoxon signed-rank test was utilized for “Hygiene” (n=12), while paired t-tests (df=11) were used for all other categories. As depicted in Figure 2 and Table 1 post-workshop performance scores demonstrated statistically significant increases from baseline across all eight P-UGVA domains (p < 0.005). The 95% confidence intervals (CI) for these improvements remained entirely above the threshold of zero. The educational impact was characterized by exceptionally large effect sizes. The most substantial improvements were observed in Ergonomics (d = 4.905), Preparation of Ultrasound Device (d = 3.755), and Anatomy Identification (d = 3.752). Even in domains requiring complex motor skills, such as Needle Coordination (d = 2.574) and Procedure Completion (d = 2.264), the intervention yielded large practical significance. In the non-parametric Hygiene domain, students achieved a perfect improvement score (Rank-Biserial r = 1.000, p = 0.002).
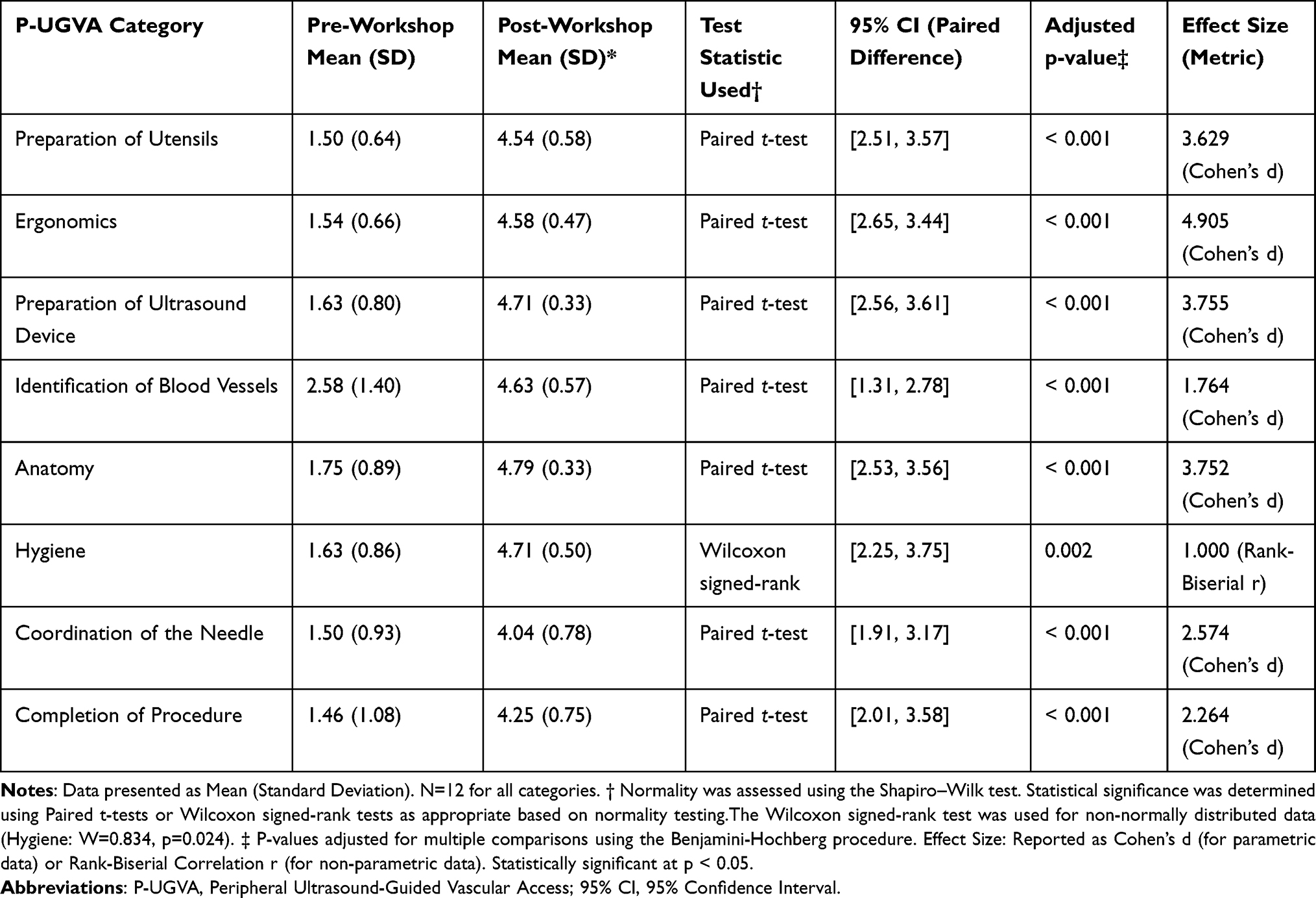 |
Table 1 Pre- and Post-Workshop P-UGVA Performance Score |
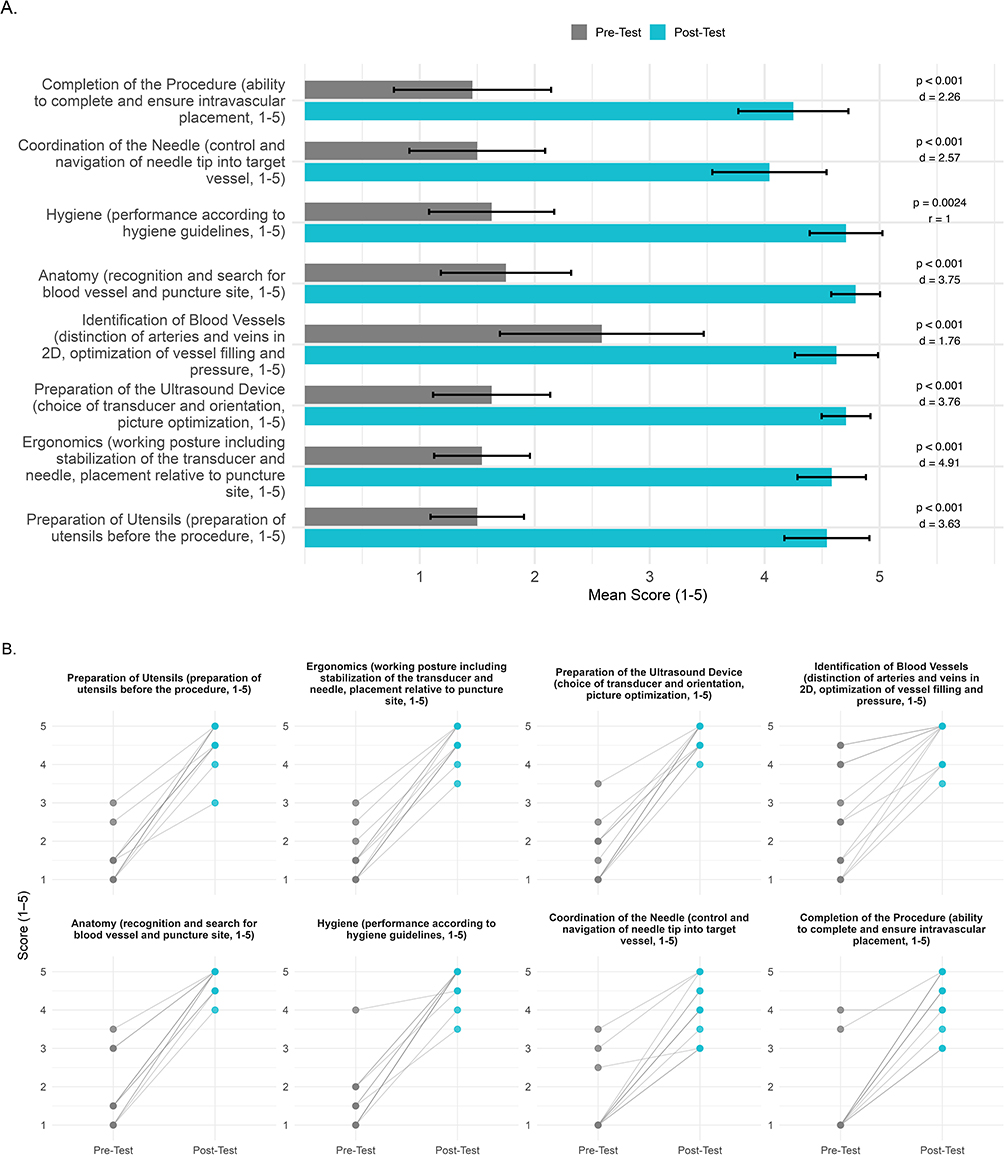 |
Figure 2 (A) Proficiency Assessment Using the P-UGVA Score. The P-UGVA score is a composite score evaluating eight elements of proficiency: preparation of utensils, ergonomics, preparation of the ultrasound device, identification of blood vessels, anatomy, hygiene, coordination of the needle, and completion of the procedure. Bars represent the mean ± 95% confidence intervals. P-values and effect sizes (Cohen’s d or Rank-Biserial r) for Pre-Test vs Post-Test comparisons (N=12) are shown for each P-UGVA domain. All p-values were adjusted for multiple comparisons using the Benjamini-Hochberg procedure. All variables were normally distributed (Shapiro–Wilk, p > 0.05) except Hygiene; comparisons used paired t-tests, except Hygiene (Wilcoxon signed-rank). (B) Individual Workshop Scores by P-UGVA Domain. Individual lines show Pre- and Post-Test scores for each participant across P-UGVA domains (n = 12). |
Post-test performance stratified by teaching group is displayed in Figure 3 and Table 2. A Mann–Whitney U-test compared outcomes between participants taught by peers versus those taught by an attending physician. No statistically significant differences were observed between the two groups across any P-UGVA category (all p > 0.118; Table 2). Analysis of practical significance using rank-biserial correlation revealed negligible to small effect sizes (r values ranging from −0.286 to 0.486). The largest observed difference was in “Identification of Blood Vessels” (r=0.486, p=0.118), which did not reach statistical significance and represented a moderate effect that favored the attending physician group. However, in all other technical domains, including “Anatomy” (r=0.057, p=0.802) and “Preparation of Ultrasound Device” (r=0.086, p=0.922), effect sizes were negligible.
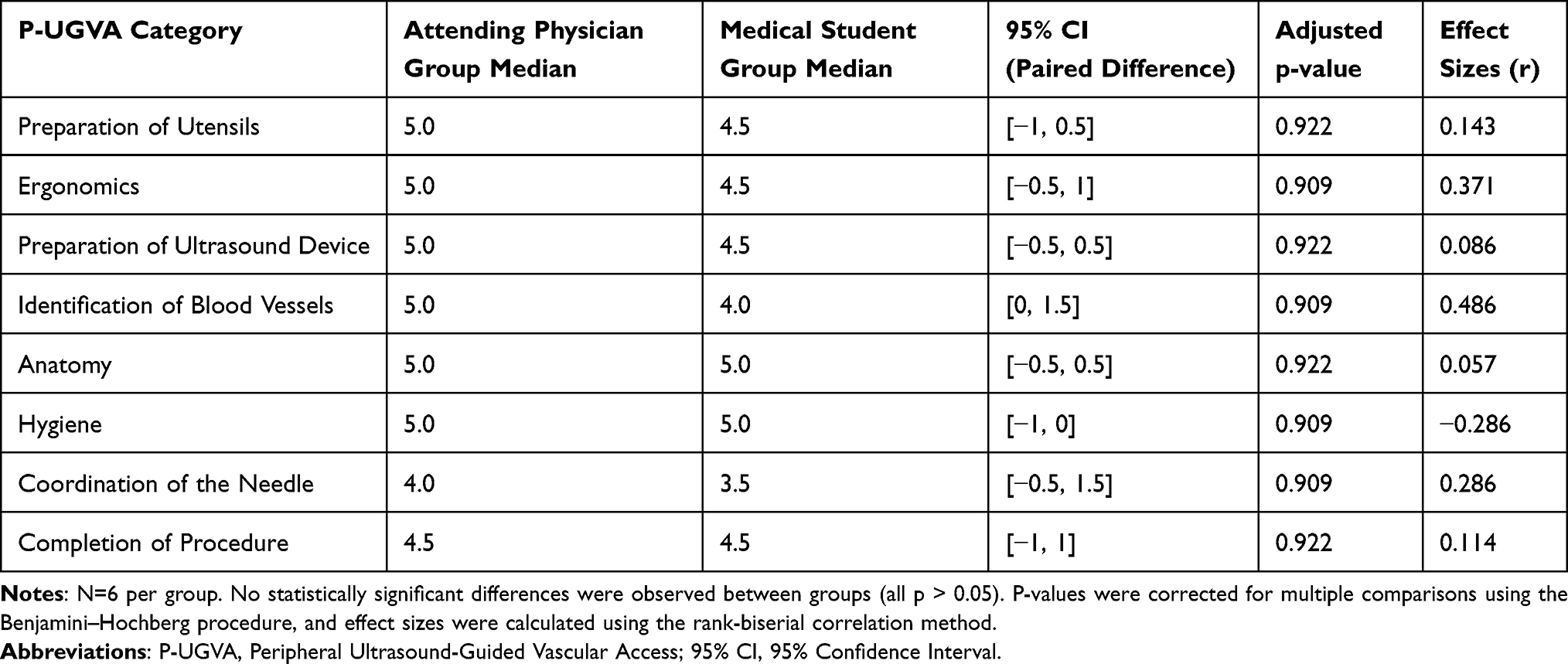 |
Table 2 Post-Workshop Performance Comparison by Teaching Modality (Mann–Whitney U-Test) |
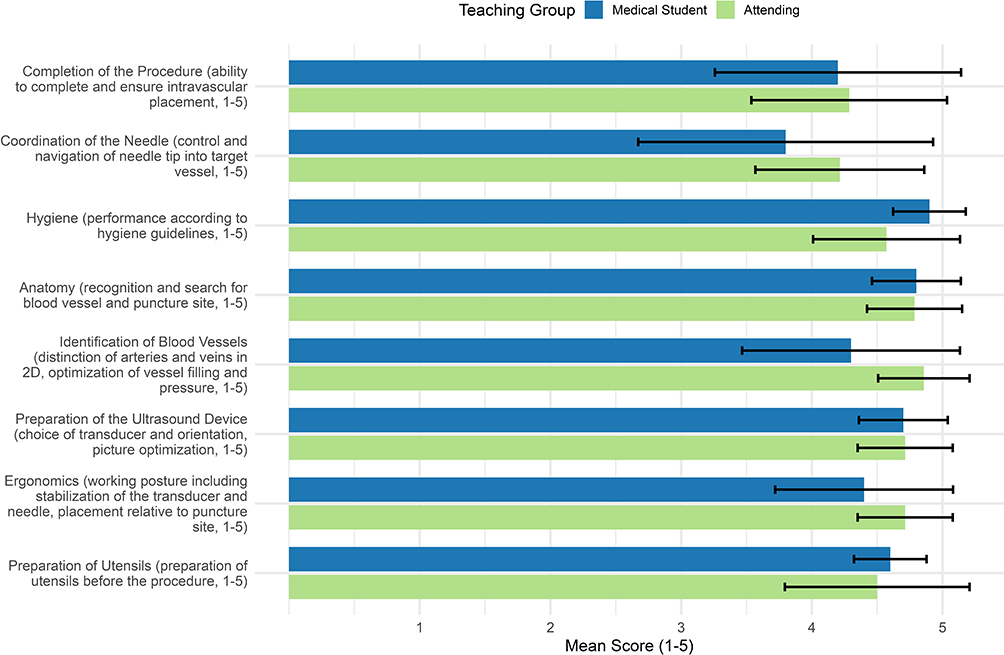 |
Figure 3 Difference in Post-Workshop Scores between Attending Physician Teacher and Medical Student Teacher. The P-UGVA score is a composite score evaluating eight elements of proficiency: preparation of utensils, ergonomics, preparation of the ultrasound device, identification of blood vessels, anatomy, hygiene, coordination of the needle, and completion of the procedure. Post-test P-UGVA scores for Peer (n = 6) and Attending Physician (n = 6) groups. Error bars indicate 95% confidence intervals. Mann–Whitney U-tests showed no statistically significant differences between groups across domains (all p > 0.118), although moderate effect sizes were observed in select domains (e.g., vessel identification, ergonomics). |
Survey responses comparing pre-workshop familiarity (Appendix 1) and post-workshop confidence (Appendix 2) on a 5-point Likert scale (1 = Strongly Disagree, 5 = Strongly Agree) are summarized in Figure 4 and Table 3. Participants reported increased comfort and confidence across all assessed domains following the workshop. Notable improvements in mean ratings were observed for vasculature identification (Pre: 2.08 vs. Post: 4.17, p < 0.005), differentiating arteries from veins (Pre: 2.33 vs. Post: 4.67, p < 0.005), operating the ultrasound machine (Pre: 1.75 vs. Post: 3.50, p < 0.005), and teaching basic skills to peers (Pre: 1.25 vs. Post: 3.58, p < 0.005).
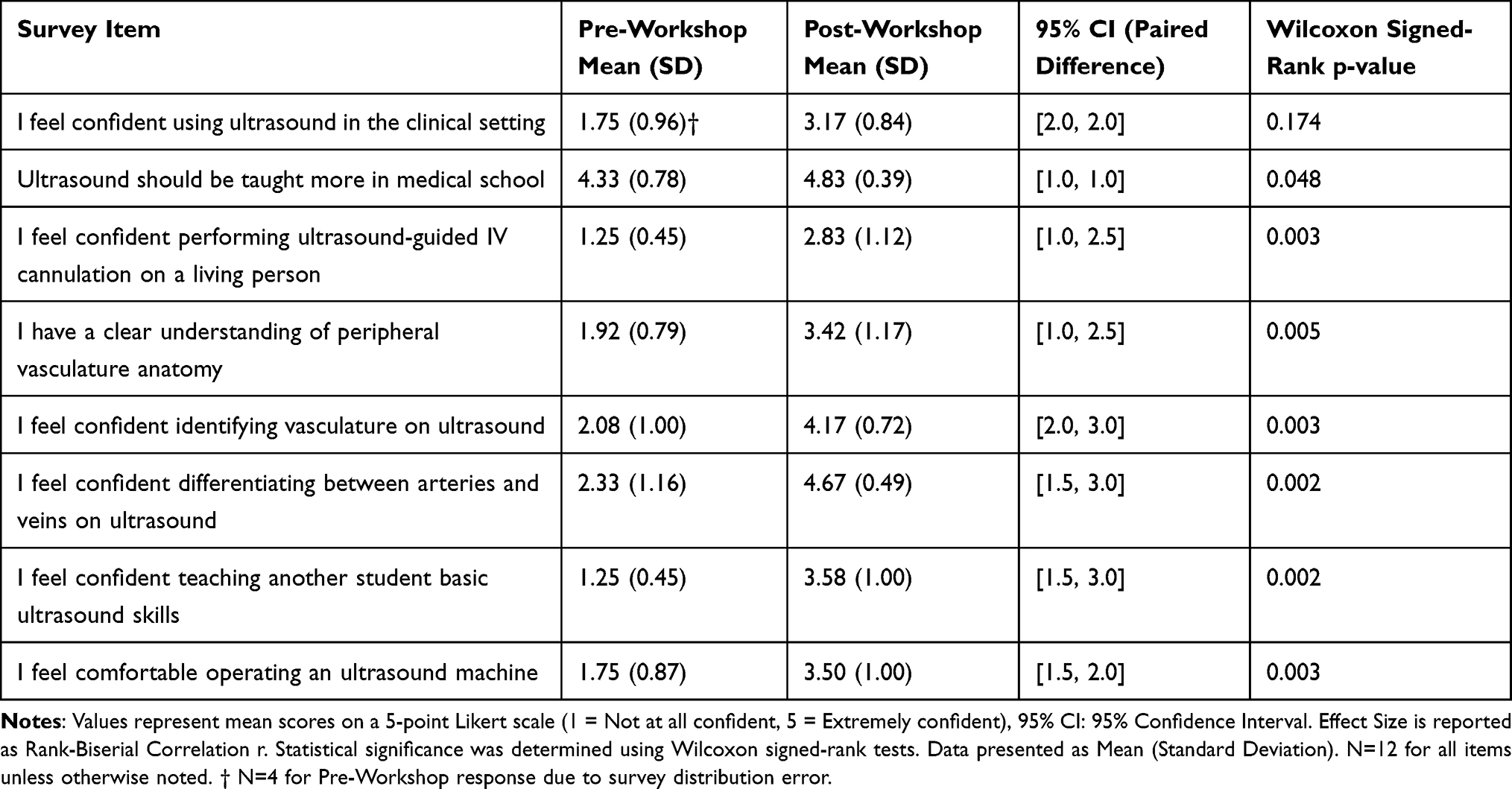 |
Table 3 Pre- and Post-Workshop Survey Responses (Likert Scale 1–5) |
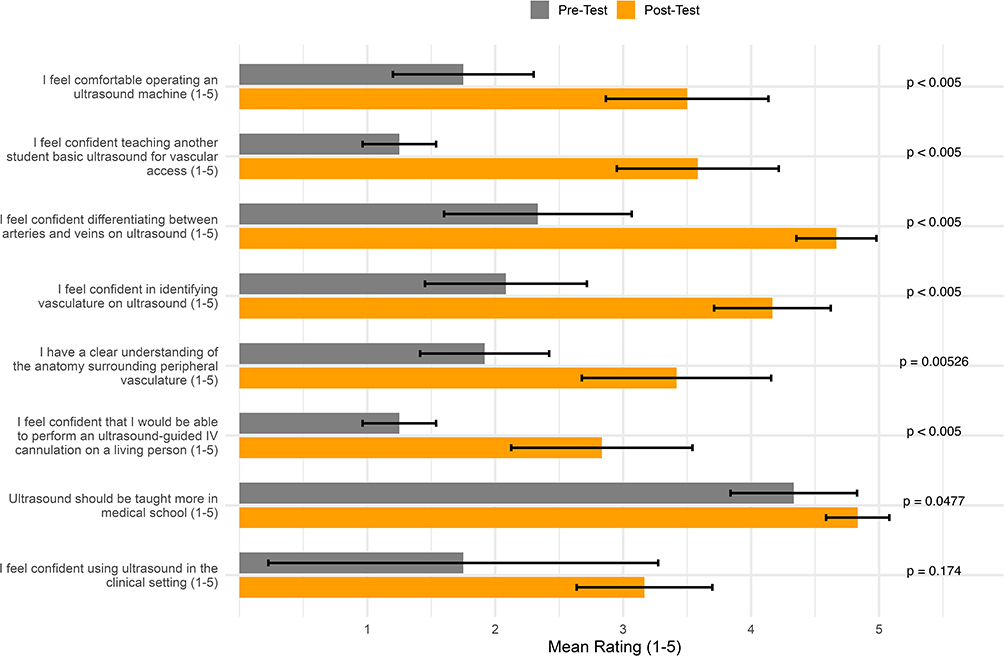 |
Figure 4 Effect of Workshop on Self-Reported Familiarity and Confidence. Pre-workshop familiarity and post-workshop confidence on a 5-point Likert scale (1 = Strongly Disagree, 5 = Strongly Agree). Data are mean ± 95% CI; differences assessed with Wilcoxon signed-rank test. Pre-workshop general clinical ultrasound confidence was limited (n = 4); all other items n = 12. |
Mean ratings for confidence in performing ultrasound-guided IV cannulation on a living person also increased (Pre: 1.25 vs. Post: 2.83, p < 0.005). Data for the item regarding general clinical ultrasound confidence was limited in the pre-workshop survey (n=4) due to a distribution error; however, available mean ratings (Pre: 1.75) were lower than the complete post-workshop dataset (Post: 3.17, n=12), consistent with trends in other domains (p = 0.174). Participants also expressed a stronger preference for increased ultrasound education in the medical school curriculum (Mean: 4.83).
In addition to confidence ratings, participants were assessed on their ability to select the correct ultrasound probe (Linear, Curvilinear, or Phased Array) for ultrasound-guided IV cannulation. A McNemar’s test was conducted to evaluate changes in probe selection accuracy pre- and post-intervention. While three students corrected their probe selection to the linear probe post-intervention, the overall change was not statistically significant (χ2 = 1.33, p = 0.25).
Discussion
In this study, preclinical medical students demonstrated higher P-UGVA scores, as a proxy for ultrasound-guided IV skills, following the educational intervention of a hands-on IV cannulation educational workshop. Whether participants were taught by trained medical students or an attending physician during the workshop did not have a statistically significant impact on P-UGVA score outcomes. Additionally, survey respondents demonstrated that the workshop yielded higher degrees of comfort, confidence, ability to teach and understanding of peripheral vascular anatomy. Providing early simulation of ultrasound-guided IV skills for preclinical students may improve clinical procedural skills and confidence as students prepare to enter the clinical setting, ultimately leading to more effective, efficient and skillful IV placement, augmenting the patient experience at academic hospitals.
Performance of ultrasound guided IV placement is innately challenging, as operators must combine their anatomical knowledge of 3D structures with their visuospatial and psychomotor skills. Simultaneous use of both hands is required to navigate needle placement and maintain visualization of anatomical strictures with the ultrasound probe. The marriage of these various skills can be assessed using the internationally validated P-UGVA scoring system. Operators can improve their skills by developing their understanding of peripheral vascular anatomy - a domain in which our participants reported significantly increased confidence - and increasing their repetitions of the procedure through practice. In this study, the authors conclude that markedly improved performance between pre- and post-test scores can be attributed to first year medical students’ novel understanding and limited exposure to ultrasound prior to the study and limited knowledge of peripheral vasculature.
Previous studies have shown that psychomotor and visuospatial skills improve with procedural competence.14,15 For preclinical medical students, exposure to ultrasound technique is not robustly embedded into the curriculum. It is unlikely that participants in our study have adequately developed their psychomotor and visuospatial skills from repetitive ultrasound use. This is further supported by participants’ relatively low pre-test scores prior to the intervention.
Notably, this simulation study showed no difference in performance across any procedural or technical category between participants who were taught by an attending physician and students who were taught by peer instructors trained in ultrasound-guided IV access from an anesthesiology attending physician. This result implies that future hands-on ultrasound skill workshops may be effectively spearheaded by trained medical students. This finding is synergistic with Cohen et al’s guiding principles for “Student-as-Teacher” curricula, which advocates for increased medical student teaching skills training. They propose curricular accommodations for authentic opportunities for medical students to teach their peers in a longitudinal and progressive manner.16 Another study from Cash et al, showed that “near-peer” simulation training (ie., simulations taught by students one year ahead in their clinical training) showed statistically significant improvement of learners’ self-reported confidence in history-taking, assessment and clinical management.17
Other medical specialties have adopted near-peer teaching curricula at the residency level with success. This was illustrated by Oldan et al, whose radiology department adopted didactic symposia by which radiology residents taught a radiology basics course for medical students, demonstrating a positive outcome on medical student satisfaction.18 Resident satisfaction is also augmented by near-peer teaching responsibilities, as a general surgery resident-as-teacher curriculum showed statistically significant improvement in residents’ teaching confidence and helped them transition into a teaching role.19 Our study demonstrates that medical students too may be highly effective teachers of anesthesiology-relevant procedural skills. As shown in the literature, adding a procedural student teaching component to medical curricula may be beneficial for the student-teacher’s learning and student learners alike.
The objective technical parity observed between groups suggests that for introductory procedural skills, “cognitive congruence” - the shared conceptual framework between peers - may be as effective as expert instruction. Furthermore, the high degree of curricular standardization likely minimized the impact of instructor seniority on initial skill acquisition. These results indicate that a structured, simulation-based curriculum can effectively bridge the expertise gap in novice learners, making student-led instruction a viable, resource-efficient model.20
Limitations
Several limitations to this study should be noted. First, the sample size was small (N=12), which may limit the generalizability of the findings and the statistical power to detect smaller differences between teaching cohorts. However, the exceptionally large effect sizes observed in the primary performance outcomes suggest that the educational impact was robust despite the small cohort.
Second, potential participants were primarily recruited from a single institution’s Anesthesiology Interest Group (AIG), which introduces a degree of selection bias, and the absence of a control group limits causal attribution of observed improvements to the intervention. These students likely possessed higher baseline motivation for procedural learning than the general medical student population. Third, while the post-workshop assessment demonstrated immediate skill acquisition within a two-week follow-up timeframe, this study did not evaluate long-term skill retention or the transferability of these skills to clinical practice on live patients. Additionally, the tofu model, while a practical, low-cost option for simulation, does not robustly replicate the physiologic properties of peripheral vasculature like compressibility and pulsatility, and may not reflect the realism of pressure, resistance and tactile feedback during IV cannulation. Although two trained, blinded student evaluators were used, formal inter-rater reliability (IRR) was not assessed, which may limit confidence in scoring consistency across evaluators.
Finally, while the Benjamini-Hochberg procedure was used to control for multiple comparisons, the pilot nature of this study means that these results should be interpreted as foundational. Future multi-center studies with larger, randomized cohorts from entire preclinical classes are necessary to further validate the equivalence of near-peer teaching in ultrasound-guided vascular access training.
Conclusion
The educational intervention of an ultrasound workshop was effective in improving preclinical student participants’ procedural acumen in a non-clinical simulation of ultrasound-guided vascular access. Through the result of increased P-UGVA scores, our study suggests that early preclinical exposure of ultrasound-guided procedural techniques may improve procedural performance, student confidence and understanding of peripheral vascular anatomy. Medical students may be effective teachers of procedural ultrasound skills. However, further research with larger sample sizes is needed to validate these findings and assess their generalizability to clinical performance.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Draper R, Ellinger D, Trottier M, Armstrong K, Ma W. Ultrasound education in an elective course in the undergraduate medical curriculum improves students’ subjective learning and clinical rotation and residency preparedness. Med Sci Educ. 2023;33(3):737–12. PMID: 37501805; PMCID: PMC10368609. doi:10.1007/s40670-023-01800-4
2. Alerhand S, Choi A, Ostrovsky I, et al. Integrating basic and clinical sciences using point-of-care renal ultrasound for preclerkship education. MedEdPORTAL. 2020;16:11037. PMID: 33324747; PMCID: PMC7732135. doi:10.15766/mep_2374-8265.11037
3. Haidar DA, Kessler R, Khanna NK, et al. Association of a longitudinal, preclinical ultrasound curriculum with medical student performance. BMC Med Educ. 2022;22(1):50. PMID: 35062942; PMCID: PMC8780388. doi:10.1186/s12909-022-03108-0
4. Dinh VA, Dukes WS, Prigge J, Avila M. Ultrasound integration in undergraduate medical education: comparison of ultrasound proficiency between trained and untrained medical students. J Ultrasound Med. 2015;34(10):1819–1824. PMID: 26333569.5. doi:10.7863/ultra.14.12045
5. Li L, Yong RJ, Kaye AD, Urman RD. Perioperative point of care ultrasound (POCUS) for anesthesiologists: an overview. Curr Pain Headache Rep. 2020;24(5):20. PMID: 32200432. doi:10.1007/s11916-020-0847-0
6. Lee SC, Yang EC, Navarro JC, Minard CG, Huang X, Deng Y. An introductory point-of-care ultrasound curriculum for an anesthesiology residency program. MedEdPORTAL. 2022;18:11291. PMID: 36654982; PMCID: PMC9780414. doi:10.15766/mep_2374-8265.11291
7. Troianos CA, Hartman GS, Glas KE, et al. Guidelines for performing ultrasound guided vascular cannulation: recommendations of the American society of echocardiography and the society of cardiovascular anesthesiologists. J Am Soc Echocardiography. 2011;24(12):1291–1318. doi:10.1016/j.echo.2011.09.021
8. Walsh KL, Yadav A, Cradeur M, et al. Impact of a preclinical medical student anesthesiology elective on the attitudes and perceptions of medical students regarding anesthesiology. Adv Med Educ Pract. 2023;14:1347–1355. PMID: 38050578; PMCID: PMC10693776. doi:10.2147/AMEP.S427974
9. Sawka DM, Kendall MC, Diorio MS, et al. Impact of a preclinical elective on medical student performance on an anesthesiology simulation scenario. Adv Med Educ Pract. 2025;16:1229–1238. PMID: 40708762; PMCID: PMC12288752. doi:10.2147/AMEP.S516942
10. Primdahl SC, Todsen T, Clemmesen L, Knudsen L, Weile J. Rating scale for the assessment of competence in ultrasound-guided peripheral vascular access – a delphi consensus study. J Vascular Access. 2016;17(5):440–445. PMID: 27516142. doi:10.5301/jva.5000581
11. Primdahl SC, Weile J, Clemmesen L, et al. Validation of the peripheral ultrasound-guided vascular access rating scale. Medicine. 2018;97(2):e9576. PMID: 29480851; PMCID: PMC5943877. doi:10.1097/MD.0000000000009576
12. Hayward G, Huang H, Regan BR, Bellomo M-C, Kendall MC. Comparing static versus dynamic ultrasound techniques: a randomized pilot trial of novice and advanced users. J Vascular Access. 2026;27(1):136–143. PMID: 39989188. doi:10.1177/11297298251315237
13. Parker C, Foster T. Realistic Tofu-based phantom model for ultrasound-guided femoral nerve blocks. Visual J Emerge Med. 2020;18(18):100678. doi:10.1016/j.visj.2019.100678
14. Mulder TA, Van De Velde T, Dokter E, et al. Unravelling the skillset of point-of-care ultrasound: a systematic review. Ultrasound J. 2023;15(1):19. doi:10.1186/s13089-023-00319-4
15. Jalolova M, Jankovic D, Sasaki K, Tanaka R, Kato Y. Simulation-based bypass training and learning curves—resident experience. Asian J Neurosurg. 2023;18(4):773–776. doi:10.1055/s-0043-1775859
16. Cohen A, Steinert Y, Ruano Cea E. Teaching medical students to teach: a narrative review and literature-informed recommendations for student-as-teacher curricula. Acad Med. 2022;97(6):909–922. PMID: 35108235. doi:10.1097/ACM.0000000000004608
17. Cash T, Brand E, Wong E, Richardson J, Athorn S, Chowdhury F. Near-peer medical student simulation training. Clin Teach. 2017;14(3):175–179. PMID: 27488259. doi:10.1111/tct.12558
18. Oldan JD, Jordan SG, Wallace J, Campbell J, Fordham LA, Beck Dallaghan GL. Near-peer teaching in radiology symposia: a success story in residents as teachers. J Med Educ Curric Dev. 2023;10:23821205231162459. PMID: 36911752; PMCID: PMC9996712. doi:10.1177/23821205231162459
19. Kobritz M, Demyan L, Hoffman H, Bolognese A, Kalyon B, Patel V. “Residents as teachers” workshops designed by surgery residents for surgery residents. J Surg Res. 2022;270:187–194. PMID: 34688990. doi:10.1016/j.jss.2021.09.003
20. Loda T, Erschens R, Loenneker H, et al. Cognitive and social congruence in peer-assisted learning – a scoping review. PLoS One. 2019;14(9):e0222224. PMID: 31498826; PMCID: PMC6733464. doi:10.1371/journal.pone.0222224
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Teamwork in Pediatric Resuscitation: Training Medical Students on High-Fidelity Simulation
Gonçalves BAR, Melo MCB, Ferri Liu PM, Valente BCHG, Ribeiro VP, Vilaça e Silva PH
Advances in Medical Education and Practice 2022, 13:697-708
Published Date: 11 July 2022
Mapping the Landscape: A Systematic Review of Technology Trends in Medical Education and Competency Development

Toofaninejad E, Mirzaei S, Mahdavi Shakib A, Gholipour Morad Dashtaki D, Raoufian H, Mirmoghtadaie Z, Sohrabi S
Advances in Medical Education and Practice 2025, 16:2369-2383
Published Date: 20 December 2025
Clinician Led Point of Care Ultrasound Workshops for Anatomy Instruction: A Pilot Study
Ledbetter D, Mumber JT, Strong LB, Cawley D, Nickols J, Edison J, Douthit NT
Advances in Medical Education and Practice 2026, 17:598393
Published Date: 22 May 2026