Back to Journals » Advances in Medical Education and Practice » Volume 13
Teamwork in Pediatric Resuscitation: Training Medical Students on High-Fidelity Simulation
Authors Gonçalves BAR ![]() , Melo MCB
, Melo MCB ![]() , Ferri Liu PM, Valente BCHG, Ribeiro VP, Vilaça e Silva PH
, Ferri Liu PM, Valente BCHG, Ribeiro VP, Vilaça e Silva PH
Received 11 March 2022
Accepted for publication 29 June 2022
Published 11 July 2022 Volume 2022:13 Pages 697—708
DOI https://doi.org/10.2147/AMEP.S365976
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Beatriz Adriane Rodrigues Gonçalves,1 Maria do Carmo Barros de Melo,2 Priscila Menezes Ferri Liu,2 Beatriz Cristina Heitmann Gomes Valente,3 Vívian Paiva Ribeiro,4 Pedro Henrique Vilaça e Silva4
1Department of Pediatrics, Faculdade de Ciências Médicas de Minas Gerais, Belo Horizonte, Minas Gerais, Brazil; 2Department of Pediatrics, Medicine School, Federal University of Minas Gerais, Belo Horizonte, Minas Gerais, Brazil; 3Department of Pediatrics, Faculdade de Minas-BH, Belo Horizonte, Minas Gerais, Brazil; 4Faculdade de Minas-Belo Horizonte, Belo Horizonte, Minas Gerais, Brazil
Correspondence: Maria do Carmo Barros de Melo, Department of Pediatrics, Medicine School, Federal University of Minas Gerais, Avenida Professor Alfredo Balena, 190. Bairro Santa Efigênia, Belo Horizonte, Minas Gerais, CEP: 30.130-100, Brazil, Tel +55-31-9847-09444, Fax +55-31-3409-9745, Email [email protected]
Background: Simulation training and teamwork for medical students are essential to improve performance in pediatric cardiopulmonary resuscitation.
Purpose: To evaluate if a specific approach to teamwork improves technical and nontechnical performance.
Methods: We performed quasiexperimental, prospective, pre- and postinterventional, and nonrandomized research with 65 students in the fourth year of their medicine course. This was a case–control study in which teams used a customized TeamSTEPPS protocol (n=34) or not (n=31) for cardiopulmonary arrest training in children using high-fidelity simulation. All participants answered a sociodemographic and satisfaction questionnaire and underwent theory and practice pre- and posttesting. The survey data were collected in 2019 and analyzed using χ2, Mann–Whitney, κ, and Wilcoxon tests. p< 0.05 was considered significant.
Results: Intervention and control groups achieved better scores in theory posttesting (p< 0.001 and p=0.049), but there was no difference between them in pre- (p=0.291) and posttesting (p=0.397). In the checklist of the practice test, all groups obtained their best outcomes in posttesting and the intervention group achieved higher scores (p< 0.001). All groups increased the number of teamwork events and reduced the time span to perform resuscitation first steps (p< 0.001) in posttesting.
Conclusion: The use of teamwork training based on a customized TeamSTEPPS protocol improved performance in team behavior and group technical achievement. The evaluation of the students about the training was positive.
Keywords: cardiopulmonary resuscitation, medical education, patient-care team, patient safety, simulation training
Introduction
Associations among teamwork, quality of assistance, and patient safety are already widely proven in the literature.1–9 Important medical organizations like the American Heart Association (AHA) and the International Liaison Committee on Resuscitation support an increase on teamwork emphasis and suggest this training for members of a resuscitation team.10
The uniqueness of critical patient care, such as the need for fast decision-making, concurrently ongoing multiple complex processes, and an adverse environment enclosed by noise and disruption contribute to failures.11,12 In respect of pediatric patients, these features are enhanced by the childcare itself, particularly when medication doses must be calculated and devices based on weight or age chosen.13
Team Strategies and Tools to Enhance Performance and Patient Safety (TeamSTEPPS) is a specialist approach to training health professionals in teamwork. This strategy is based on scientific evidence, and was developed by the Patient Safety Program of the Department of Defense of the US in partnership with the Agency for Healthcare Research and Quality (AHRQ).14 TeamSTEPPS has been tested in several pediatric services,8,15–19,21,22 obtaining excellent results.8,15–21 This methodology has also been used in a variety of clinical contexts, apart from pediatrics,12,23,24 and is part of the practices of great American hospital associations.25 The program determines leadership, situation management, mutual support, and communication as the main skills to be trained, and also highlights tools and strategies to reinforce these skills.14
The active methodology comprises an interactive system where students turn into leaders in the learning process, while teachers become their assistants.26 Bonini-Rocha et al27 reinforced the need for technology and innovation as supports in the development of new proposals to improve the educational process. According to Melo et al,28 basic or advanced simulations can enhance and improve skills. This process allows the participants to cope with emergencies in a safe environment where “errors are forgiven”, and enables education and training of health professionals.
Teams can be instructed to better decision-making, improve performance under stress, and increase their technical achievements.29 Practical training raises the impact of acquisition, execution, and maintenance of teamwork skills on health issues.30 Following those pieces of evidence, this research aimed to evaluate whether a specific approach to teamwork based on TeamSTEPPS training attached a cardiopulmonary resuscitation (CPR) and high-fidelity simulation training founded on AHA protocols would improve technical performance and teamwork.
Methods
Design and Setting
We performed an experimental, prospective, controlled, nonrandomized study on 65 students in their fourth year of medical school from a private faculty of Belo Horizonte (Figure 1). The research was conducted in the faculty‘s simulation facility using high-fidelity rooms with SimJunior’s mannequins from Laerdal. The participants were divided into three control groups and three intervention groups by convenience sampling. Each group attended a meeting for training and evaluation, with a total workload of 6 hours per participant. Both groups (control and intervention) received standard training with a theory class, the intervention, and received teamwork training based on the American protocol of TeamSTEPPS Essentials. After the training, the students underwent practice training using high-fidelity simulation.
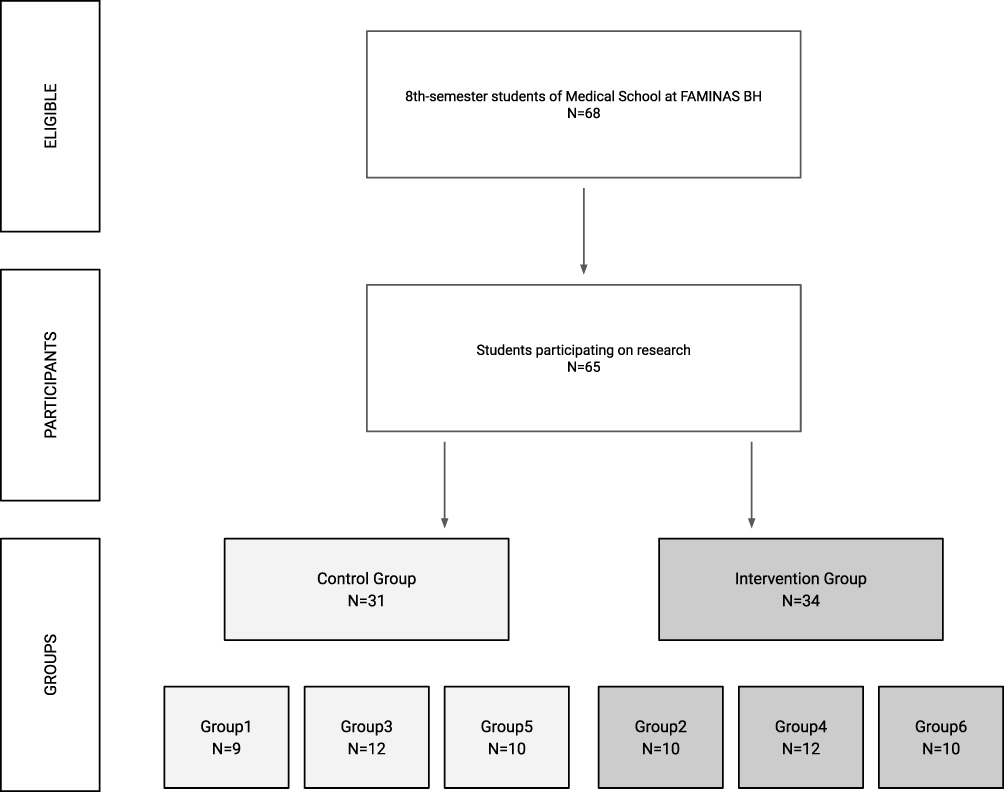 |
Figure 1 Sample-selection flowchart 64 medical students from FAMINAS-BH allocated to the control and intervention groups. |
Inclusion and Exclusion Criteria
Since the training was part of a curricular and mandatory subject, there were 68 undergraduate medical students who were eligible to participate. Three did not agree to participate, so they were excluded. The study included all students enrolled in the course and who agreed to participate.
Data-Collection Methods
Participants underwent theory pretesting with 20 multiple-choice questions filled within 30 minutes. For practice pretesting, each group was divided into two smaller groups with a maximum of six participants. In this test, all students acted as team leader in a simulated clinical case of cardiopulmonary arrest (CPA) or 3 minutes. While we assessed one team, the other one waited in a separate room, without contact.
Next, all students attended a 30-minute lecture about pediatric advanced life support (PALS) guidelines of CPR). After that, only the intervention group received additional training on teamwork using a customized TeamSTEPPS Essentials model approaching team building: occurrence and frequency of mistakes in clinical practice, discussion of the four essential abilities of effective teams (leadership, case management, mutual support, and communication), detection of barriers blocking the expected target exhibition of tools and strategies to improve teamwork, and patient safety. Then, in the practice training, each student acted as a leader in a simulated clinical case of CPA for 5 minutes, followed by a three-step debriefing. Half the students stayed in the simulation room, and the other half remained in the observation room watching the activity. When the procedure had finished, those students changed rooms. Subsequently, the students underwent theory and practice posttesting similarly to that for pretraining. Resuscitation teams remained the same in pre- and postpractice testing, only changing the leader. Ultimately, each participant filled a Likert scale satisfaction survey about the training, communication awareness, and teamwork. Figure 2 presents these study steps.
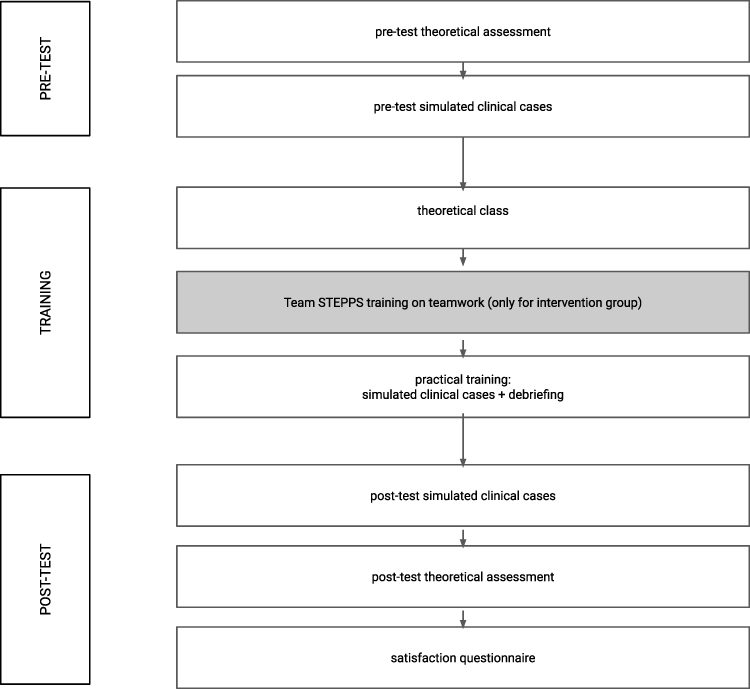 |
Figure 2 Data-collection stages: activities carried out for training and evaluation of study participants. |
We evaluated theory knowledge through pre- and posttraining testing, with maximum score of 20 points. The students’ performance on practice pre- and posttraining testing was measured using three tools. For the first, two blinded examiners analyzed the scenarios using checklists of expected acts, and likewise in PALS courses of AHA, and we obtained the percentage of hits in the checklist in relation to the maximum possible grade. To check agreement between examiners, we employed the κ index. Another evaluation was carried out separately by a teamwork-trained researcher who assessed the number of team-behavior events (use of nontechnical skills like leadership, situation management, mutual support, and communication) in each simulated clinical case, using absolute values. The third analysis was conducted using recorded material of practice pre- and posttesting, measuring in each scenario the time that the leader took to begin resuscitation: CPA recognition, first compressions, first adrenaline (nonshockable rhythms) or first shock (shockable rhythms), and the total time to progress from the first steps. Then, we compared the scores of the control and intervention groups on the three tools, both prior to and after training. Schematic presentation of the study design, protocol, and flow is presented in Figure 2.
Data Analysis
We analyzed data using the SPSS 23. Regardless of sociodemographic and academic sample features, we compared noncontinuous variables of control and intervention groups using the χ2 test. Descriptive statistics — median, minimum, and maximum — were evaluated for group performance. While we applied the Mann–Whitney test to compare the difference between control and intervention groups at the same time (between-group comparison), the Wilcoxon test contrasted pre- and posttesting in the same group at different time points (within-group comparison). To check agreement between examiners, we employed the κ index. Our standard of significance was p<0.05.
Ethics
Participation in the research was voluntary, and students could withdraw from the study at any moment without penalty. All participants signed the form for free and informed consent. All the documents (tests, checklists, surveys) were anonymous, and confidentiality criteria were followed. The study was approved by the Research Ethics Committee at the Federal University of Minas Gerais (CAAE: 10753419.2.0000.5149).
Results
The demographic data analyzed showed that there was no statistical difference between the control and intervention groups for any variables, as seen on Table 1. The results of pre- and posttraining theory and practice testing, number of teamwork-intervention events, and time to perform the first resuscitation steps are presented in Table 2. Figure 3 shows that there was no difference between the control and intervention groups on results of pre- and posttraining theory testing, though there was improvement in both groups on results of pre- and postpractice testing and number of teamwork-intervention events, with a more pronounced advance seen in the intervention group. Figure 4 shows the reduction in time in seconds for the recognition of CPA, initiation of CPR, and administration of epinephrine and/or shock according to the indication on the cases. Table 3 shows the results of the survey on satisfaction with the training divided according to a Likert scale into grades 1 and 2, and 4 and 5 (no answer 3).The scores given by examiners on the posttraining practice test checklist had few indices calculated, due to nonvariable answers. The examiners significantly agreed on the evaluation of the topics scored: 87% of topics on pretesting and 92% on posttesting.The satisfaction survey indicated very good participant opinions about the training (Table 3). We did not perform statistical analysis on these data, due to no variation in answers.
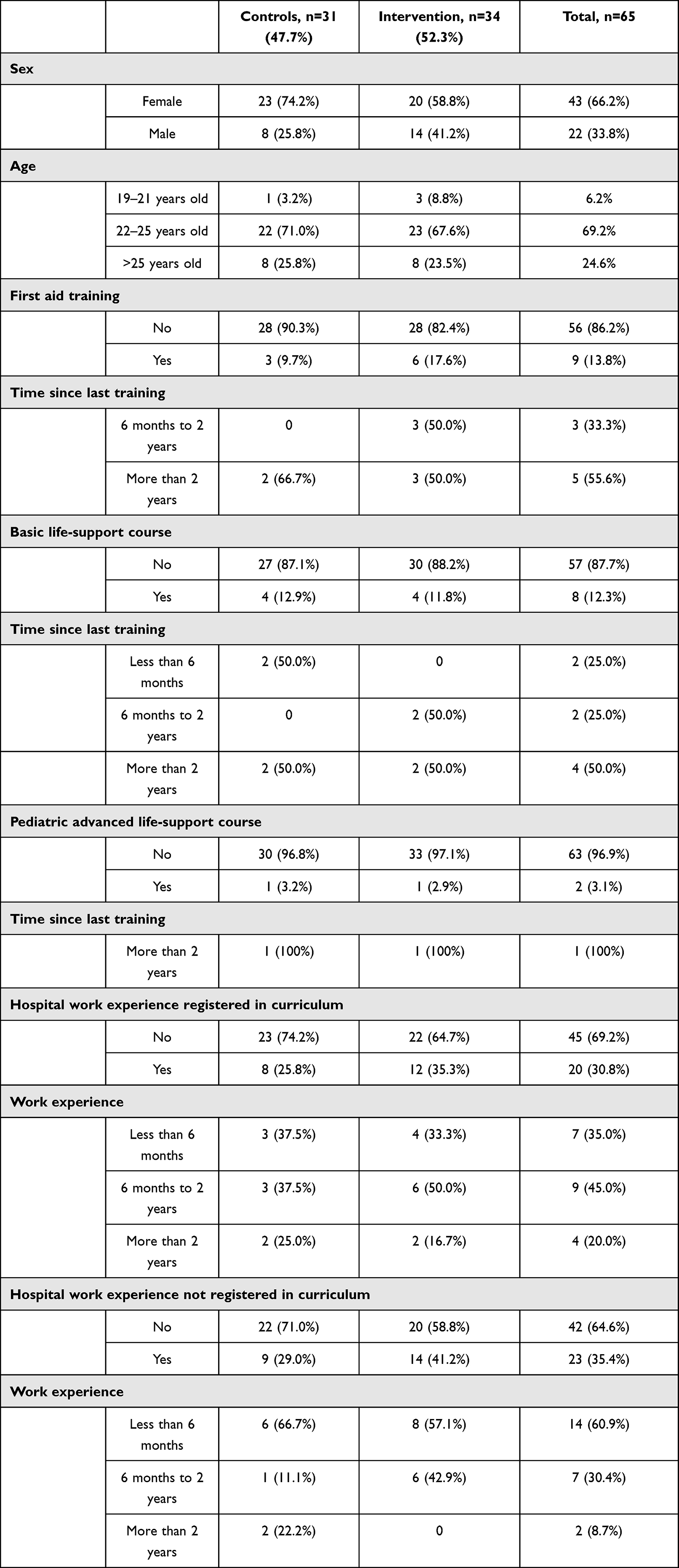 |
Table 1 Analyses of sociodemographic and academic profiles of students participating in the research |
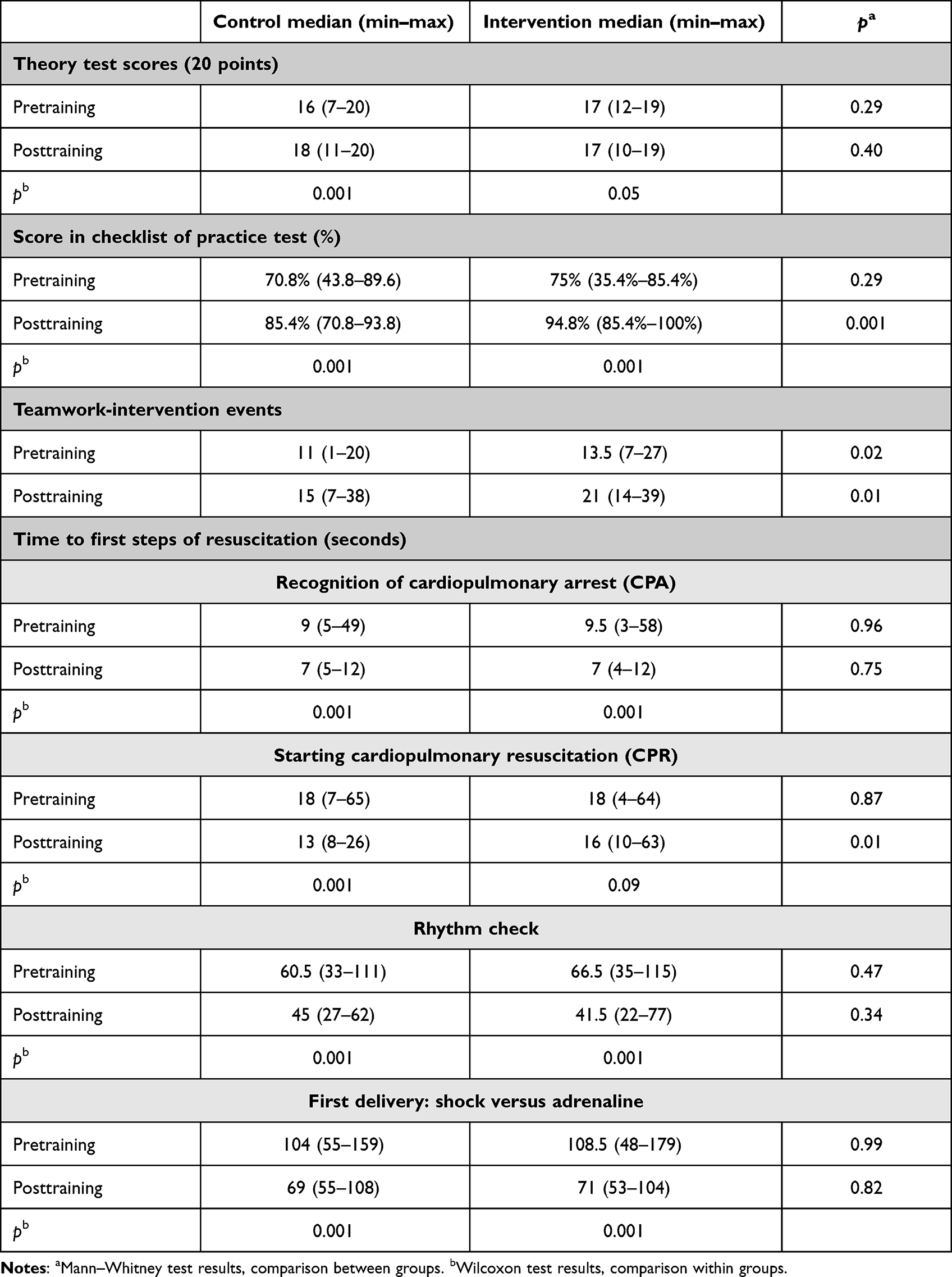 |
Table 2 Performance comparison of participants before and after training between and within control and intervention groups |
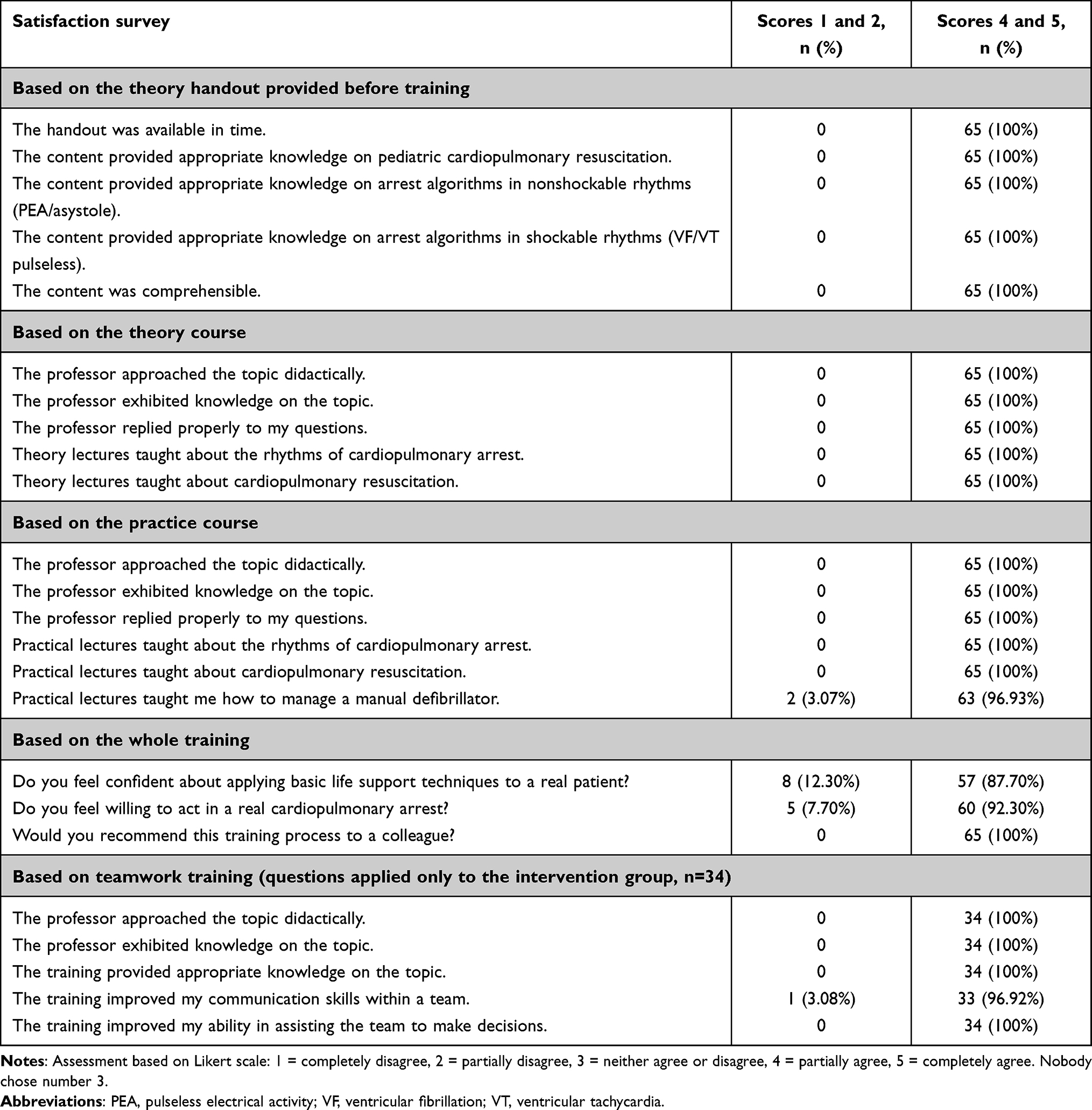 |
Table 3 Satisfaction and awareness of survey participants (n=65) based on five-point Likert scale |
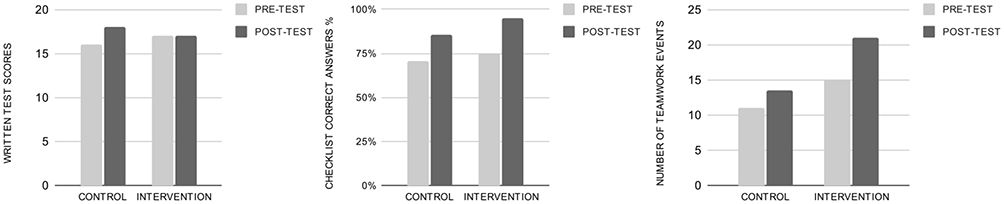 |
Figure 3 Results pre- and posttraining of theory testing, practice testing checklist, and number of team events per simulation. |
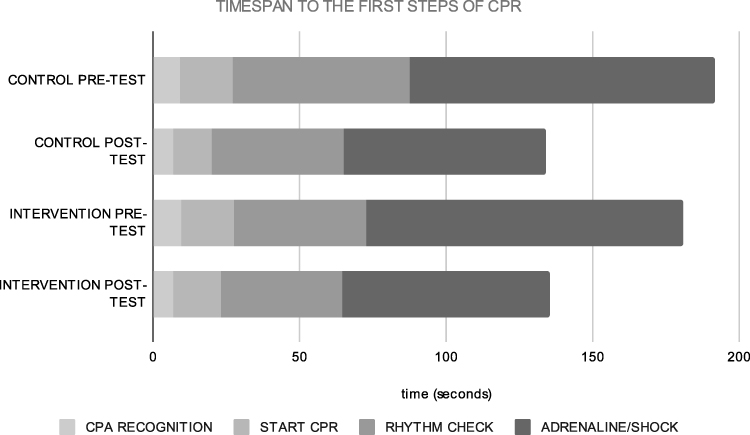 |
Figure 4 Results pre- and posttraining of time to perform the first steps of cardiopulmonary resuscitation. |
Discussion
The analyses of sociodemographic and academic medical profiles revealed a sample like other national and international research on the same topic.31–36 The results indicated that students’ experience on CPR was limited before the training. Theory testing demonstrated improvement in scores after training in both groups. Patterson et al obtained similar results in theory assessments prior to and after multidisciplinary training relying on simulation emphasizing teamwork and communication.25 The practice-test outcomes indicated better posttraining scores in both groups, corroborating the improvement in students’ performance. Canadian multicentric research37 employing 300 health professionals divided into 60 teams evaluated the effect of teamwork adopting simulation and PALS guidelines, but without a control group. The intervention group posttesting achieved a higher percentage of correct answers, proving that teamwork training enhanced their technical performance. There are few standard techniques to assess teamwork, and there is no agreement on which one should be applied for medical students. Some studies, such as the Clinical Teamwork Scale,37 Teamwork Evaluation of Non-Technical Skills,15 and TeamSTEPPS — Teamwork Attitudes Questionnaire, adopted scores that highlight key areas of teamwork using the Likert scale.21 Despite none of these studies being controlled, all of them showed better performance in the intervention group. In our research, the number of positive teamwork events increased in both groups. Despite the higher number of teamwork events in the intervention group before training, the addition of events before training was significantly higher than the control group. Similar research adopting control and randomized data evaluated medical internship students that underwent neonatal resuscitation training using simulation. These authors also concluded that the intervention group improved its performance as a team.20 In that research, they compared them only after training, limiting any evaluation on performance improvement.
We also checked the technical performance through the time span to the first steps of resuscitation. Both groups improved after training, reducing the time span basically in all steps considered, except the “start CPR” of the intervention group. The control group had a decrease of 33.6% in total time to the first steps, while the intervention group registered 34.2%. Those results reinforced that all students improved practice performance with the simulation training, despite receiving or not teamwork instructions. Analogously to our study, Gilfoyle et al37 found an increase in technical efficiency after teamwork training observed in the time-span decline for thoracic compression and defibrillation. Clinical results from another study revealed a reduction in time to set extracorporeal circulation during resuscitation after teamwork training of intensive unit care pediatric professionals.15 Although neither study was controlled, they suggest that teamwork training can successfully improve clinical performance. Furthermore, Thomas et al registered a reduction of around 30% of the total time spent on resuscitation comparing control and intervention groups.20 However, they did not obtain any difference between those groups, neither in each step nor in the total time to the first steps of CPR.
Facing the conflict between educational methodologies of traditional and active learning, understanding students’ opinions is essential to amend the educational processes at universities.26,38 Following our results, participants supported the quality of the theory handout, theory and practice classes, methodologies applied, and the possibility of acquiring knowledge on the topic. The students’ awareness of self-belief, which stands for the reliance on a successful task, positively assists them when they cope with life-support assistance in real patients. The section of the survey approaching teamwork training focused only on the intervention group and obtained full endorsement regarding quality and learning potential on the topic. Most research that has applied teamwork training in pediatric patients also evaluated the fulfillment and awareness of participants after instructions, recording positive feedback, mainly on reliance, knowledge, and skills to proceed with CPR.8,16–20,22,25,39,40 A controlled and randomized study assessed the effect of teamwork training on cooperation and coordination among professionals using the TeamSTEPPS Essentials model in the PALS course of AHA.41 This methodology is almost identical to ours and obtained significantly higher awareness of teamwork, cooperation, knowledge of the situation, and abilities to assist in teams’ decision-making.
It is needed to strengthen the team-leader component of the resuscitation skills lab and to identify students who may benefit from additional practice in the team-leader role and with other skills in which they lack confidence.42 The results of this study will help in the restructuring of cardiac resuscitation skills simulation involving students from other areas of health. Our outcomes follow the literature, indicating the efficiency of the TeamSTEPPS protocol as an educational source of teamwork to health professionals12,15,16,18,21,23–25,41 and also of the high-fidelity simulation as a teaching–learning methodology.7,25,43–49 Considering we could not find in Latin America experimental research on the teamwork of critical pediatric patients, our investigation added and opened new light into discussions of a relevant topic among Brazilian scientists.
Limitations
Some of the constraints registered are that we could not randomize students because of their class schedule, the relatively short time spent on teamwork training due to the time available in the simulation laboratory, and the absence of a standard tool to evaluate teamwork and measure its improvement. Despite these limitations, this study is innovative and pioneering in our country, as it provides important information about teamwork using a TeamSTEPPS-based model in CPR.
Recommendations
Scales to assess teamwork must be standardized to enhance results on this topic. The authors also suggest the development of other controlled and randomized studies and evaluation of memory retention.
Conclusion
Teamwork improved the performance of professionals coping with the assistance of critical pediatric patients. Additionally, we reinforce that simulation allows teams to safely practice technical and nontechnical skills, ensuring better performance and communication in a safe environment. Ultimately, teamwork training based on simulation should be practiced following undergraduate level and systematically sustained for all health professionals, especially those who assist critical pediatric patients.
Acknowledgments
The authors thank the coordinators and collaborators of the Simulation Laboratory at Faculdade de Minas (Faminas-BH), where the study was carried out.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Salas E, Diaz Granados D, Klein C, et al. Does team training improve team performance? A meta-analysis. Hum Factors. 2008;50(6):903–933. doi:10.1518/001872008X375009
2. Manser T. Teamwork and patient safety in dynamic domains of healthcare: a review of the literature. Acta Anaesthesiol Scand. 2009;53(2):143–151. doi:10.1111/j.1399-6576.2008.01717.x
3. Lerner S, Magrane D, Friedman E. Teaching teamwork in medical education. Mt Sinai J Med a J Transl Pers Med. 2009;76(4):318–329. doi:10.1002/msj.20129
4. Kilpatrick K, Paquette L, Jabbour M, et al. Systematic review of the characteristics of brief team interventions to clarify roles and improve functioning in healthcare teams. PLoS One. 2020;15(6):1–28. doi:10.1371/journal.pone.0234416
5. Schmutz J, Manser T. Do team processes really have an effect on clinical performance? A systematic literature review. Br J Anaesth. 2013;110(4):529–544. doi:10.1093/bja/aes513
6. Rosen MA, DiazGranados D, Dietz AS, et al. Teamwork in healthcare: key discoveries enabling safer, high-quality care. Am Psychol. 2018;73(4):433–450. doi:10.1037/amp0000298
7. Hunziker S, Johansson AC, Tschan F, et al. Teamwork and leadership in cardiopulmonary resuscitation. J Am Coll Cardiol. 2011;57(24):2381–2388. doi:10.1016/j.jacc.2011.03.017
8. Stocker M, Pilgrim SB, Burmester M, Allen ML, Gijselaers WH. Interprofessional team management in pediatric critical care: some challenges and possible solutions. J Multidiscip Healthc. 2016;9:47–58. doi:10.2147/JMDH.S76773
9. Buljac-Samardzic M, Doekhie KD, Van Wijngaarden JDH. Interventions to improve team effectiveness within health care: a systematic review of the past decade. Hum Resour Health. 2020;18(1):1–42. doi:10.1186/s12960-019-0441-x
10. Greif R, Bhanji F, Bigham BL, et al.; Education, Implementation, and Teams Collaborators. Education, implementation, and teams: 2020 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Circulation. 2020;142(16_suppl_1):S222–S283. doi:10.1161/CIR.0000000000000896
11. Murphy M, Curtis K, McCloughen A. What is the impact of multidisciplinary team simulation training on team performance and efficiency of patient care? An integrative review. Australas Emerg Nurs J. 2016;19(1):44–53. doi:10.1016/j.aenj.2015.10.001
12. Capella J, Smith S, Philp A, et al. Teamwork training improves the clinical care of trauma patients. J Surg Educ. 2010;67(6):439–443. doi:10.1016/j.jsurg.2010.06.006
13. Committee on Pediatric Emergency Medicine. Patient safety in the pediatric emergency care setting. Pediatrics. 2007;120(6):1367–1375. doi:10.1542/peds.2007-2902
14. King HB, Battles J, Baker DP, et al. TeamSTEPPSTM: team strategies and tools to enhance performance and patient safety heidi. In: Henriksen K, Battles JB, Keyes MA editors. Advances in Patient Safety: New Directions and Alternative Approaches. Rockville: Agency for Healthcare Research and Quality; 2008.
15. Mayer CM, Cluff L, Lin WT, et al. Evaluating efforts to optimize team STEPPS implementation in surgical and pediatric intensive care units. Jt Comm J Qual Patient Saf. 2011;37(8):365–374. doi:10.1016/s1553-7250(11)37047-x
16. Brodsky D, Gupta M, Quinn M, et al. Building collaborative teams in neonatal intensive care. BMJ Qual Saf. 2013;22(5):374–382. doi:10.1136/bmjqs-2012-000909
17. Allan CK, Thiagarajan RR, Beke D, et al. Simulation-based training delivered directly to the pediatric cardiac intensive care unit engenders preparedness, comfort, and decreased anxiety among multidisciplinary resuscitation teams. J Thorac Cardiovasc Surg. 2010;140(3):646–652. doi:10.1016/j.jtcvs.2010.04.027
18. Figueroa MI, Sepanski R, Goldberg SP, Shah S. Improving teamwork, confidence, and collaboration among members of a pediatric cardiovascular intensive care unit multidisciplinary team using simulation-based team training. Pediatr Cardiol. 2013;34(3):612–619. doi:10.1007/s00246-012-0506-2
19. Budin WC, Gennaro S, O’Connor C, Contratti F. Sustainability of improvements in perinatal teamwork and safety climate. J Nurs Care Qual. 2014;29(4):363–370. doi:10.1097/NCQ.0000000000000067
20. Thomas EJ, Williams AL, Reichman EF, Lasky RE, Crandell S, Taggart WR. Team training in the Neonatal Resuscitation Program for interns: teamwork and quality of resuscitations. Pediatrics. 2010;125(3):539–546. doi:10.1542/peds.2009-1635
21. Sawyer T, Laubach VA, Hudak J, Yamamura K, Pocrnich A. Improvements in teamwork during neonatal resuscitation after interprofessional TeamSTEPPS training. Neonatal Network. 2013;32(1):26–33. doi:10.1891/0730-0832.32.1.26
22. Bank I, Snell L, Bhanji F. Pediatric crisis resource management training improves emergency medicine trainees’ perceived ability to manage emergencies and ability to identify teamwork errors. Pediatr Emerg Care. 2014;30(12):879–883. doi:10.1097/PEC.0000000000000302
23. Reed T, Horsley TL, Muccino K, et al. Simulation using TeamSTEPPS to promote interprofessional education and collaborative practice. Nurse Educ. 2017;42(3):E1–5. doi:10.1097/NNE.0000000000000350
24. Amaya-Arias AC, Idarraga D, Giraldo V, Gómez LM. Effectiveness of a program for improving teamwork in operating rooms. Rev Colomb Anestesiol. 2015;43(1):68–75.
25. Patterson MD, Geis GL, LeMaster T, Wears RL. Impact of multidisciplinary simulation-based training on patient safety in a paediatric emergency department. BMJ Qual Saf. 2013;22(5):383–393. doi:10.1136/bmjqs-2012-000951
26. Christofoletti G, Fernandes JM, Martins AS, Oliveira Junior SA, Carregaro RL, Toledo AM. Degree of student satisfaction with the use of active learning methodology in a discipline of ethics in health. Rev Elet Educ. 2014;8(2):188–197.
27. Bonini-Rocha AC, Oliveira LF, Rosat RM, Ribeiro MFM. Satisfaction, perceived learning, and performance in video lesson and lecture. Cien Cogn. 2014;19(1):47–57.
28. Melo MCB, Silva NLC, Liu PMF, et al. E-Learning and simulation on a pré-hospital emergency course: a participant’s perspective. Rev Bras Educ Med. 2016;40(4):713–719. doi:10.1590/1981-52712015v40n4e02482014
29. Baker D, Gustafson S, Beaubien J, Salas E, Barach P. Medical Teamwork and Patient Safety: The Evidence-Based Relation. Rockville: Agency for Healthcare Research & Quality (AHRQ); 2005:59.
30. Salas E, Rosen MA. Building high reliability teams: progress and some reflections on teamwork training. BMJ Qual Saf. 2013;22(5):369–373. doi:10.1136/bmjqs-2013-002015
31. Barzansky B, Etzel SI. Educational programs in US medical schools, 2004–2005. JAMA. 2005;294(9):1068–1074. doi:10.1001/jama.294.9.1068
32. Veras RM, Fernandez CC, Feitosa CCM, Fernandes S. Career expectations of medical students of universidade Federal da Bahia. Rev Bras Educ Med. 2020;44(2):e056. doi:10.1590/1981-5271v44.2-20190208
33. Cardoso Filho FAB, Magalhães JF, Silva KML, Pereira D. Profile of medical students at the state University of Rio Grande do Norte (UERN), 2013. Rev Bras Educ Med. 2015;39(1):32–40. doi:10.1590/1981-52712015v39n1e01092014
34. Lamounier JA, Torga ALGF, Leite GLF. Characteristics and concepts of graduates of the UFMG medicine course. Pediatria São Paulo-SP. 2002;24(3/4):85–92.
35. Scheffer MC, Guilloux AGA, Dal Poz MR, Schraiber LB. Reasons for choosing the profession and profile of newly qualified physicians in Brazil. Rev Assoc Med Bras. 2016;62(9):853–861. doi:10.1590/1806-9282.62.09.853
36. Fiorotti KP, Rossoni RR, Miranda AE. Profile of medical students at the Federal University in Espírito Santo, Brazil, 2007. Rev Bras Educ Med. 2010;34(3):355–362. doi:10.1590/S0100-55022010000300004
37. Gilfoyle E, Koot DA, Annear JC, et al. Improved clinical performance and teamwork of pediatric interprofessional resuscitation teams with a simulation-based educational intervention. Pediatr Crit Care Med. 2017;18(2):e62–69. doi:10.1097/PCC.0000000000001025
38. Peixoto LF, Celeste LC, Silva EM, Da, Mangilli LD. Quality assessment/satisfaction of the learning of practical discipline of the speech, language, and hearing sciences course. Disturb Comun. 2017;29(4):625–635. doi:10.23925/2176-2724.2017v29i4p625-635
39. Thomson NM, Campbell DE, O’Leary FM. Teaching medical students to resuscitate children: an innovative two-part programme. Emerg Med Australas. 2011;23(6):741–747. doi:10.1111/j.1742-6723.2011.01477.x
40. Siems A, Cartron A, Watson A, McCarter R, Levin A. Improving pediatric rapid response team performance through crew resource management training of team leaders. Hosp Pediatr. 2017;7(2):88–95. doi:10.1542/hpeds.2016-0111
41. Fagan MJ, Connelly CD, Williams BS, Fisher ES. Integrating team training in the pediatric life support program: an effective and efficient approach? J Nurs Adm. 2018;48(5):279–284. doi:10.1097/NNA.0000000000000613
42. Luctkar-Flude M, Baker C, Pulling C, et al. Evaluating an undergraduate interprofessional simulation-based educational module: communication, teamwork, and confidence performing cardiac resuscitation skills. Adv Med Educ Pract. 2010;8(1):59–66. doi:10.2147/AMEP.S14100
43. Bender J, Kennally K, Shields R, Overly F. Does simulation booster impact retention of resuscitation procedural skills and teamwork? J Perinatol. 2014;34(9):664–668. doi:10.1038/jp.2014.72
44. Hunt EA, Walker AR, Shaffner DH, Miller MR, Pronovost PJ. Simulation of in-hospital pediatric medical emergencies and cardiopulmonary arrests: highlighting the importance of the first 5 minutes. Pediatrics. 2008;121(1):e34–e43. doi:10.1542/peds.2007-0029
45. Hunt EA, Vera K, Diener-West M, et al. Delays and errors in cardiopulmonary resuscitation and defibrillation by pediatric residents during simulated cardiopulmonary arrests. Resuscitation. 2009;80(7):819–825. doi:10.1016/j.resuscitation.2009.03.020
46. Prego J, Gerolami A, Más M, et al. Simulación de alta fidelidad en emergencia pediátrica: primera experiencia en la formación de posgrados y residentes de Pediatría. Rev Médica del Uruguay. 2014;30(4):247–254.
47. Semler MW, Keriwala RD, Clune JK, et al. A randomized trial comparing didactics, demonstration, and simulation for teaching teamwork to medical residents. Ann Am Thorac Soc. 2015;12(4):512–519. doi:10.1513/AnnalsATS.201501-030OC
48. Riskin A, Erez A, Foulk TA, et al. Rudeness and medical team performance. Pediatrics. 2017;139(2). doi:10.1542/peds.2016-2305
49. Sudikoff SN, Overly FL, Shapiro MJ. High-fidelity medical simulation as a technique to improve pediatric residents’ emergency airway management and teamwork: a pilot study. Pediatr Emerg Care. 2009;25(10):651–656. doi:10.1097/PEC.0b013e3181bd93ea
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge and Awareness of Non-Technical Skills Over the Course of an Educational Program in Nursing - A Repeated Cross-Sectional Study
Wevling A, Olsen BF, Nygaard AM, Heiberg T
Advances in Medical Education and Practice 2023, 14:31-41
Published Date: 10 January 2023
Mapping the Landscape: A Systematic Review of Technology Trends in Medical Education and Competency Development

Toofaninejad E, Mirzaei S, Mahdavi Shakib A, Gholipour Morad Dashtaki D, Raoufian H, Mirmoghtadaie Z, Sohrabi S
Advances in Medical Education and Practice 2025, 16:2369-2383
Published Date: 20 December 2025
Training without Harm: Rethinking Ethics, Simulation and the Evolving Future of Medical Education in West Africa
Dike NO, Kajjimu J, Amissah-Arthur MB
Advances in Medical Education and Practice 2026, 17:575929
Published Date: 20 February 2026