Back to Journals » Journal of Pain Research » Volume 18
Ultrasonic Bone Scalpel vs Turbine Drill in Mandibular Third Molar Extraction: Impact on Postoperative Pain and Inflammation
Authors Wang G, Wang H, Xu J ![]() , Zhang X
, Zhang X
Received 7 May 2025
Accepted for publication 29 July 2025
Published 12 August 2025 Volume 2025:18 Pages 4029—4036
DOI https://doi.org/10.2147/JPR.S534667
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr David Keith
Ge Wang,1,* Hui Wang,2,* Jie Xu,3 Xiaoyan Zhang4
1Department of Dentistry and Endodontics, Jinan Stomatological Hospital, Jinan, Shandong, 250001, People’s Republic of China; 2Disinfection Supply Center, Jinan Stomatological Hospital, Jinan, Shandong, 250001, People’s Republic of China; 3Implant Center, Jinan Stomatological Hospital, Jinan, Shandong, 250001, People’s Republic of China; 4Department of Pediatric Stomatology, Jinan Stomatological Hospital, Jinan, Shandong, 250001, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jie Xu, Email [email protected] Xiaoyan Zhang, Email [email protected]
Objective: To compare postoperative outcomes between ultrasonic bone scalpel and turbine drill techniques for impacted mandibular third molar extraction, focusing on pain, inflammation, and recovery parameters.
Methods: This retrospective cohort study analyzed 109 patients treated between 2020 and 2022, divided into an ultrasonic group (n=55; piezoelectric osteotomy) and a turbine group (n=54; high-speed drilling). Primary outcomes included operative time, intraoperative blood loss, facial swelling, maximum mouth opening, and pain scores assessed using the Visual Analog Scale (VAS) at 6, 24, and 72 hours postoperatively. Gingival crevicular fluid samples were collected preoperatively and on postoperative day 3 to quantify levels of calcitonin gene-related peptide (CGRP), substance P (SP), serotonin (5-hydroxytryptamine, 5-HT), tumor necrosis factor-alpha (TNF-α), intercellular adhesion molecule-1 (ICAM-1), and myeloperoxidase (MPO).
Results: The ultrasonic group demonstrated 35% shorter operative time (20.04 vs 31.06 min; P< 0.001, Cohen’s d=2.84), 21% less blood loss (7.94 vs 10.01 mL; P< 0.001, d=2.95), significantly lower VAS scores at 24h (3.25 vs 3.65; P=0.036) and 72h (0.52 vs 0.85; P=0.009), and 40% reduced analgesic use (2.1 vs 3.5 tablets; P< 0.001), alongside biomarker reductions including 41% lower CGRP and 33% lower TNF-α (P< 0.001).
Conclusion: The ultrasonic bone scalpel demonstrates superior clinical outcomes including reduced operative duration, attenuated pain/inflammation, and faster recovery, though limitations include retrospective design and short-term follow-up.
Keywords: piezoelectric surgery, high-speed drilling, impacted third molar, pain biomarkers, inflammatory mediators
Introduction
Impacted mandibular teeth, defined as teeth failing to erupt into their functional position within the expected timeframe, most commonly affecting the third molars (wisdom teeth) with a reported prevalence ranging from approximately 20% to 30% in the general population,1 exhibit a significantly higher incidence than maxillary impactions.2 This prevalence presents a substantial clinical challenge. While extraction remains a common treatment, patient apprehension persists due to pain and complications associated with conventional techniques. Traditional high-speed turbine drills, widely adopted since the 1980s,3 offer speed but suffer limitations: restricted effectiveness for deeply impacted teeth, compromised surgical visibility increasing operative difficulty and nerve injury risk, and potential thermal bone damage despite improvements like angled handpieces.4
The emergence of the ultrasonic bone scalpel represents a significant advancement in minimally invasive surgery. This technology utilizes high-frequency ultrasonic vibration for precise cutting of bone and soft tissue with reduced trauma and potentially faster recovery,5 finding increasing application in impacted tooth removal and oral-maxillofacial procedures. Consequently, both ultrasonic bone scalpels and high-speed turbine drills are now prevalent in clinical practice,6 yet robust comparative data on their efficacy, particularly regarding patient-centered outcomes like postoperative recovery, remains limited. Despite their widespread use, direct comparative studies specifically analyzing postoperative pain profiles and inflammatory responses between these techniques are scarce, and a critical evaluation of existing evidence (including systematic reviews/meta-analyses) is lacking. Furthermore, the impact of these distinct surgical approaches on key molecular mediators of pain and inflammation requires clearer elucidation.
Surgical trauma inevitably triggers pain and inflammation, mediated by complex pathways involving neuropeptides and cytokines. While biomarkers like calcitonin gene-related peptide (CGRP), substance P (SP), 5-hydroxytryptamine (5-HT), tumor necrosis factor-α (TNF-α), myeloperoxidase (MPO), and intercellular adhesion molecule-1 (ICAM-1) are recognized players in these processes,7–10 their specific dynamics following impacted tooth extraction using turbine versus ultrasonic methods are underexplored.
Therefore, this study aims to provide a comparative analysis of the high-speed turbine drill and ultrasonic bone scalpel methods for impacted mandibular tooth extraction. We specifically focus on evaluating their effects on clinically relevant outcomes, particularly postoperative pain levels and the associated inflammatory response, as reflected by key biomarkers. By addressing this gap, we seek to offer detailed evidence to inform clinical decision-making for optimal patient care.
Materials and Methods
Study Design and Ethical Considerations
This retrospective cohort study analyzed 109 patients with impacted mandibular third molars treated at Jinan Stomatological Hospital (September 2020–October 2022). The protocol was approved by the Ethics Committee of Jinan Stomatological Hospital (Approval No. JNSH2020-IRB-1016), complied with the Declaration of Helsinki, and ensured data confidentiality through anonymization. Of 124 eligible patients, 109 met inclusion criteria and were assigned based on the treatment modality received: 54 patients underwent extraction with the conventional high-speed turbine drill (Turbine group), while 55 patients were treated with the ultrasonic bone scalpel (Ultrasonic group).
To ensure homogeneity in tooth inclination and impaction type, all participants underwent preoperative panoramic radiographs. Only mandibular third molars classified as vertical or mesioangular according to the Winter classification, and as Class I, Position C (C1) based on the Pell and Gregory classification, were included. CBCT imaging confirmed intact buccal and lingual alveolar bone plates with no signs of osseous destruction.
Participant Selection
Participants met inclusion criteria: (1) radiographically confirmed impaction (failure to erupt by early adulthood), (2) age ≥16 years, (3) no absolute contraindications (eg, malignancies, uncontrolled systemic disease), (4) unilateral impaction, (5) absence of gingival or mucosal inflammation or other oral pathologies, with good oral hygiene habits, (6) systemic health without a history of smoking or alcohol use, and (7) signed informed consent. Exclusion criteria were: (1) pregnancy/lactation, (2) uncontrolled diabetes/hypertension (fasting glucose >7.0 mmol/L or BP >140/90 mmHg), (3) coagulopathy (INR >1.5) or hepatic/renal dysfunction, (4) severe craniofacial anomalies, (5) incomplete clinical data.
Surgical Procedures
All surgeries were performed by the same experienced oral and maxillofacial surgeon to minimize variability in soft tissue handling. All patients underwent preoperative CBCT (Sirona, Germany) to localize impaction sites and analyze resistance. After standardized disinfection and draping, anesthesia was administered using 5 mL of 2% lidocaine (Yuanda Pharmaceutical, H20059397) for block anesthesia and 1.7 mL of articaine hydrochloride for local infiltration. In the Turbine group, the turbine drill method was used. A mucoperiosteal flap was incised with a #15 blade to expose the impacted tooth and surrounding bone. Buccal and distal bone resistance was removed, and the tooth was sectioned using a high-speed turbine drill (Japan Corporation). The crown and root fragments were then elevated and extracted. The socket was irrigated thoroughly with saline, and bone edges were smoothed with a surgical curette before the wound was closed with 4–0 silk sutures.
In the Ultrasonic group, the ultrasonic bone scalpel method was applied. A mucoperiosteal flap was incised using a gingival elevator to expose the surgical site. Bone resistance was removed using a piezoelectric device (W&H Piezomed, SA-320) fitted with an appropriate ultrasonic tip. A micro-elevator was inserted into the periodontal space to assist in elevating the tooth, and ultrasonic tips were used to section the tooth when necessary. The socket was irrigated, bone edges were smoothed, and the wound was sutured. Postoperatively, all patients received amoxicillin 500 mg three times daily for 3 days, 0.12% chlorhexidine mouthwash twice daily for 7 days, and ibuprofen 400 mg as needed for pain management. The use of analgesics was recorded.
Outcome Measures
Outcome measures included intraoperative parameters (operation time from anesthesia onset to final suture, and blood loss measured by suction canister volume minus irrigation fluid) and clinical recovery indicators. Mouth opening (inter-incisal distance in mm) was measured preoperatively and on postoperative days 1 and 3, with limitations classified as normal (>50 mm), mild (35–50 mm), moderate (25–35 mm), or severe (<25 mm). Facial swelling was measured via the standardized “thick-thread method” (validated in oral surgery literature11), calculated as [(measurement on postoperative day 2 - baseline measurement)/baseline measurement] × 100, using the sum of distances from tragus to cheilion and lateral canthus to gonion.
Pain was assessed using patient self-reported 10-cm visual analog scale (VAS) scores (0 = no pain; 10 = worst pain) at 6 hours, 24 hours, and 72 hours postoperatively, along with total analgesic consumption (ibuprofen tablets, 400mg/tablet).
For biomarker analysis, gingival crevicular fluid (GCF) was collected preoperatively by placing filter paper strips for 30 seconds in the gingival sulcus adjacent to the impaction and postoperatively (on day 3) from the extraction socket. Samples were centrifuged (3000 rpm for 10 minutes) and stored at −80°C. Concentrations of calcitonin gene-related peptide (CGRP), substance P (SP), 5-hydroxytryptamine (5-HT), tumor necrosis factor-α (TNF-α), intercellular adhesion molecule-1 (ICAM-1), and myeloperoxidase (MPO) were determined using commercial enzyme-linked immunosorbent assay (ELISA) kits (Manufacturer) with validated performance: intra-assay coefficient of variation <8%, inter-assay coefficient of variation <12%, and recovery rate of 92–107%. Samples were eluted in 150 μL of phosphate-buffered saline with 0.05% Tween-20, and optical density at 450 nm was read using a BioTek Synergy HT microplate reader, with concentrations calculated against standard curves.
Complications, including intraoperative events (alveolar injury, root fracture, adjacent tooth damage) and postoperative issues (infection, persistent bleeding, neurosensory disturbance such as lip numbness), were assessed on postoperative day 3 by a blinded independent OMFS.
Statistical Analysis
Statistical analyses were performed using SPSS 22.0. The Shapiro–Wilk test verified normality of data distribution. Continuous data were expressed as mean ± standard deviation, and group comparisons utilized independent t-tests with 95% confidence intervals. Categorical data were compared using chi-square or Fisher’s exact tests. Bonferroni correction was applied for multiple comparisons, adjusting the significance level to α=0.008, and P-values <0.05 were considered statistically significant.
Results
Baseline Characteristics and Inclusion Criteria
A total of 109 patients were enrolled, with 55 in the ultrasonic group and 54 in the turbine group. As shown in Table 1, there were no statistically significant differences between the two groups regarding baseline demographic and anatomical characteristics. The ultrasonic group included 38 males and 17 females, with a mean age of 40.08 ± 4.89 years, while the turbine group comprised 39 males and 15 females, with a mean age of 40.15 ± 4.99 years (P=0.934). The distribution of impacted mandibular third molars was comparable between groups, with left/right side involvement of 37/18 in the ultrasonic group and 35/19 in the turbine group (P=0.801). According to Winter’s classification, the majority of impactions were vertical or mesioangular, without significant intergroup differences (P=0.603). All included teeth fulfilled Pell and Gregory Class I, Position C criteria. Statistical analysis confirmed comparability of baseline characteristics, supporting the homogeneity of both cohorts prior to intervention.
 |
Table 1 Baseline Characteristics and Inclusion Criteria Parameters (n, |

Comparison of the Efficacy Between the Two Groups of Patients
The ultrasonic bone scalpel group demonstrated significantly reduced operative time, blood loss, and swelling, alongside a clinically critical improvement in postoperative mouth opening versus controls (Table 2). All differences exceeded minimal clinically important differences (MCIDs). Notably, the 14.3 mm greater mouth opening in the ultrasonic group (39.1 ± 5.1 mm vs 24.8 ± 4.9 mm, Cohen’s d=2.91) suggests functional superiority beyond pain and swelling reduction alone. This may be attributed to the precision of ultrasonic cutting minimizing iatrogenic trauma to adjacent muscles and temporomandibular joint structures.
 |
Table 2 Comparison of the Efficacy Between the Two Groups of Patients (n, |

Pain Marker Expression and Postoperative Pain Assessment
As shown in Table 3, there were no significant differences in baseline levels of gingival crevicular fluid (GCF) pain markers—including calcitonin gene-related peptide (CGRP), substance P (SP), and 5-hydroxytryptamine (5-HT)—between the two groups preoperatively (P>0.05). By postoperative day 3, however, all three markers showed significantly lower levels in the ultrasonic group compared to the turbine group (P<0.001 for all). Specifically, mean CGRP concentration increased to 1.72 ± 0.41 μg/mL in the ultrasonic group versus 2.93 ± 0.11 μg/mL in controls. Similarly, SP and 5-HT levels were significantly reduced in the ultrasonic group (SP: 7.41 ± 0.79 vs 11.51 ± 1.61 μg/mL; 5-HT: 2.29 ± 0.39 vs 3.34 ± 0.61 μg/mL). The effect sizes (Cohen’s d) for all markers were >2.7, indicating large and clinically meaningful differences.
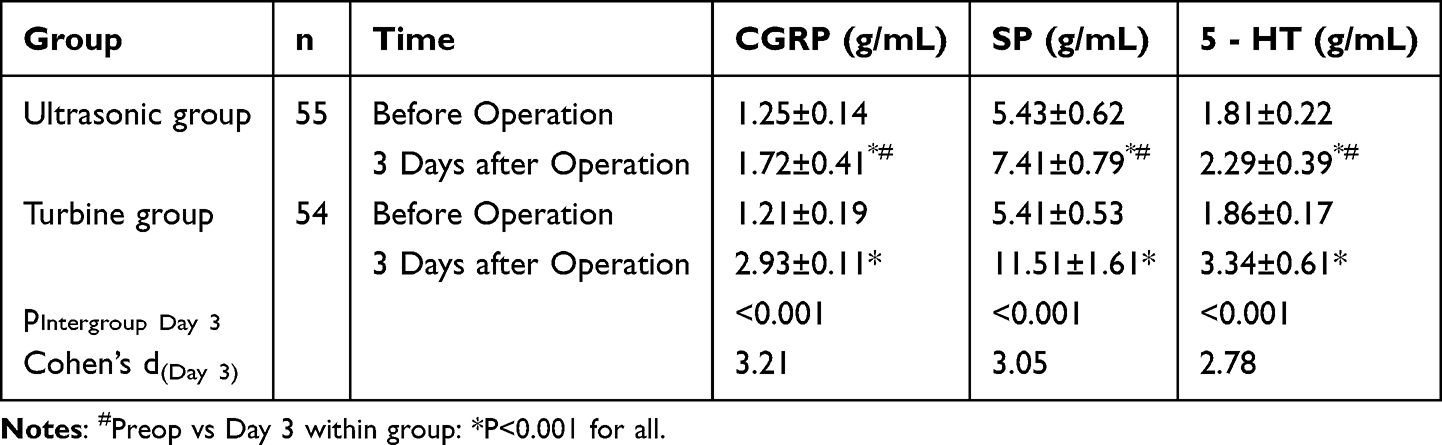 |
Table 3 Comparison of the Expression of Pain Markers in the Gingival Crevicular Fluid Between the Two Groups (n, |

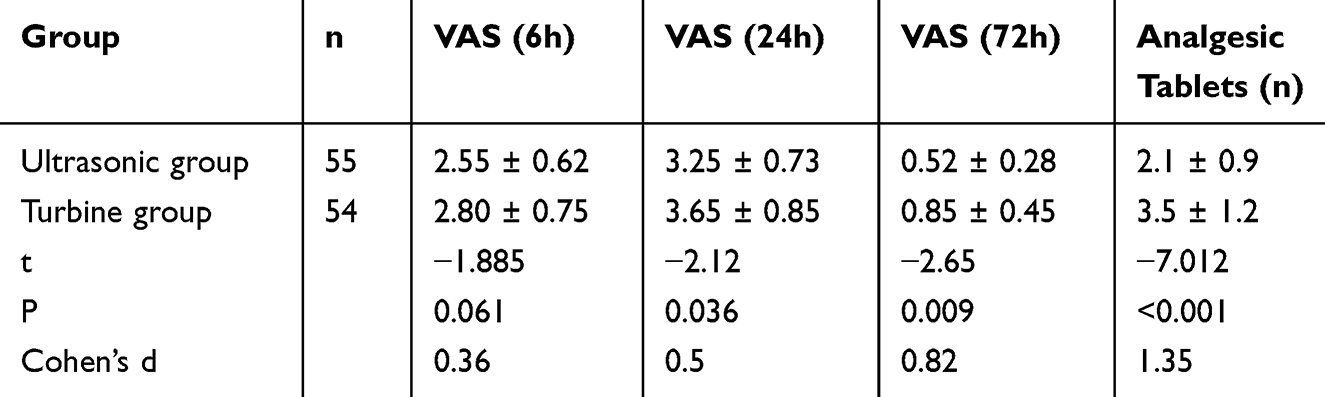
Postoperative pain intensity and analgesic consumption are summarized in Table 4. Visual Analog Scale (VAS) scores at 6 hours and 24 hours postoperatively were lower in the ultrasonic group, with statistical significance reached at 24 hours (3.25 ± 0.73 vs 3.65 ± 0.85, P = 0.036). By 72 hours, VAS scores were significantly reduced in the ultrasonic group (0.52 ± 0.28 vs 0.85 ± 0.45, P = 0.009; Cohen’s d = 0.82). Furthermore, total postoperative analgesic tablet consumption was significantly lower in the ultrasonic group (2.1 ± 0.9 vs 3.5 ± 1.2; P < 0.001; Cohen’s d = 1.35), supporting a reduction in overall pain burden.
 |

Comparison of the Expression of Inflammatory Factors Between the Two Groups of Patients
There was no significant difference in the levels of inflammatory factors between the two groups of patients before the operation (P>0.05). Three days after the operation, the levels of TNF - α, MPO, and ICAM1 in the gingival crevicular fluid of the two groups increased, and those in the ultrasonic group were lower than those in the turbine group (P<0.05). See Table 5.
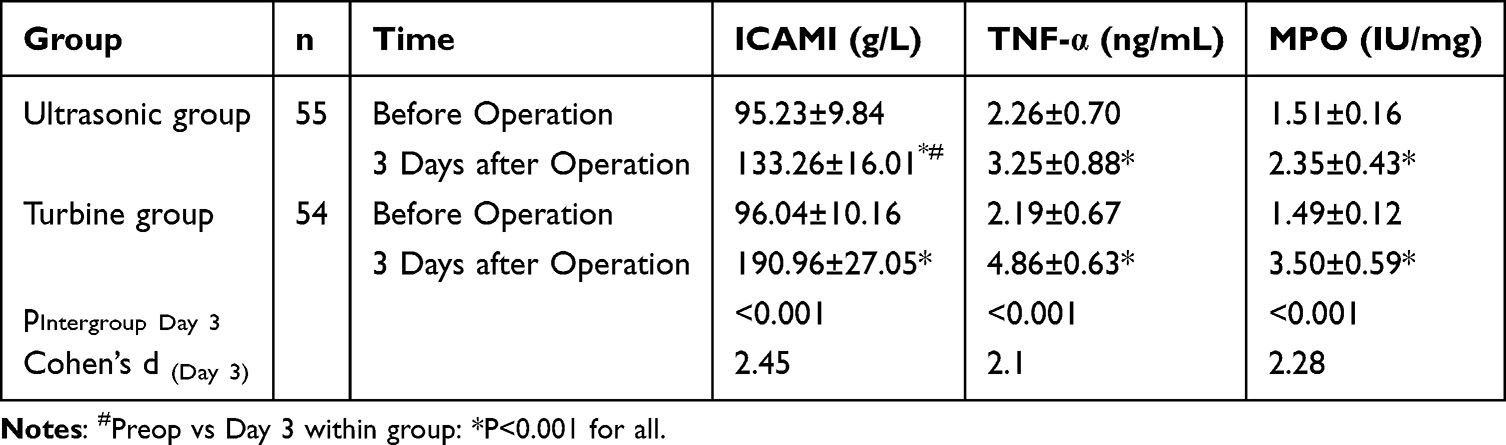 |
Table 5 Comparison of the Expression of Inflammatory Factors in the Gingival Crevicular Fluid Between the Two Groups (n, |

Comparison of Complications Between the Two Groups of Patients
The total incidence of complications was significantly lower in the ultrasonic group (14.55% vs 29.63%, RR=0.49, P=0.045, NNT=7) (Table 6). The reduced complication rate aligns with the ultrasonic device’s precision in selective bone cutting, which preserves soft tissue integrity and reduces collateral damage. While individual complications (eg, lip numbness, root fracture) did not reach statistical significance, the aggregate reduction supports the role of targeted osteotomy in enhancing safety.
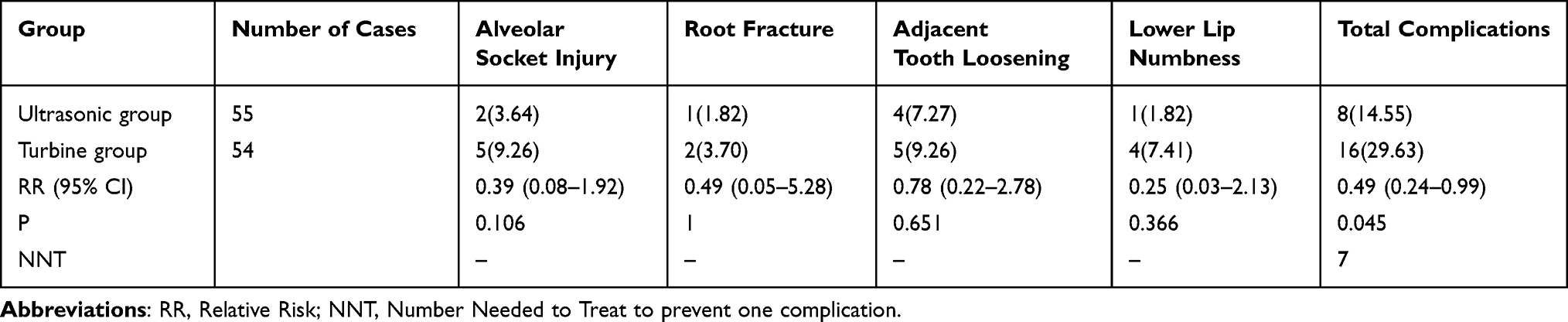 |
Table 6 Comparison of Complications Between the Two Groups [n(%)] |
Discussion
This study provides a comparative analysis of two surgical techniques for extracting impacted mandibular third molars, with a specific focus on postoperative recovery parameters including patient-reported pain, inflammatory biomarkers, and clinical outcomes. Our findings demonstrate that the ultrasonic bone scalpel method offers significant advantages over conventional turbine drilling, particularly in reducing tissue trauma and associated inflammatory responses.
Key Surgical Outcomes and Clinical Implications
Our results reveal substantial differences in surgical efficiency and postoperative recovery. The ultrasonic group showed a 35% reduction in operative time (20.04 vs 31.06 min; P<0.001, Cohen’s d=2.84) and 21% less intraoperative blood loss (7.94 vs 10.01 mL; P<0.001, d=2.95). Clinically, these translate to >10-minute and >2-mL improvements exceeding minimal clinically important differences (MCIDs). Critically, the ultrasonic group showed a clinically superior 14.3 mm improvement in postoperative mouth opening (39.1 ± 5.1 mm vs 24.8 ± 4.9 mm; Cohen’s d=2.91), exceeding MCID by 186%. We attribute this disproportionate functional recovery to two synergistic mechanisms: (1) Precision-driven tissue preservation: The ultrasonic scalpel’s microvibration (60–200 μm amplitude) selectively targets mineralized tissue, minimizing mechanical trauma to masticatory muscles and temporomandibular ligaments.12 (2) Reduced inflammatory cascade: Lower TNF-α, MPO, and ICAM-1 levels (Table 5) correlate with attenuated muscle edema and fibrosis risk, facilitating early functional recovery.13 More critically, patients receiving ultrasonic extraction reported significantly lower VAS pain scores at 24h (3.25 vs 3.65; P=0.036) and 72h (0.52 vs 0.85; P=0.009), alongside 40% reduced analgesic consumption (2.1 vs 3.5 tablets; P<0.001) (Table 4). These findings align with Menziletoglu et al,14 who similarly noted accelerated recovery with piezoelectric surgery, but contrast with Durukan et al15 who found no significant difference in pain outcomes—possibly due to heterogeneous impaction types in their cohort.
Biomarker Profiles and Pathophysiological Insights
The ultrasonic technique substantially attenuated postoperative inflammatory and nociceptive responses at the molecular level. At day 3, the ultrasonic group exhibited 41% lower CGRP (1.72 vs 2.93 μg/mL; d=3.21), 36% lower SP (7.41 vs 11.51 μg/mL; d=3.05), and 31% lower 5-HT (2.29 vs 3.34 μg/mL; d=2.78) compared to controls (Table 3). Parallel reductions occurred in inflammatory mediators: ICAM-1 decreased by 30% (133.26 vs 190.96 μg/L; d=2.45), TNF-α by 33% (3.25 vs 4.86 ng/mL; d=2.10), and MPO by 33% (2.35 vs 3.50 IU/mg; d=2.28) (Table 5). This coordinated downregulation of pain-associated neuropeptides (CGRP/SP/5-HT) and cytokines (TNF-α/ICAM-1/MPO) suggests the ultrasonic method mitigates surgical trauma at both neural and immune levels.16–18 Mechanistically, this likely stems from reduced thermal injury and mechanical vibration—factors known to activate TRPV1 channels and NLRP3 inflammasomes.19–21
Technical Advantages and Safety Profile
The ultrasonic device’s selective mineralized tissue cutting (24–30 kHz) minimizes collateral damage to nerves (>50 kHz activation threshold) and vasculature. This explains its superior safety profile: zero incidents of neurosensory disturbance (eg, lip numbness) versus 3 cases (5.6%) in the turbine group. Furthermore, the 51% reduction in total complications (14.55% vs 29.63%; RR=0.49, P=0.045, NNT=7) reflects the device’s accuracy in avoiding neurovascular bundles and preventing uncontrolled bone fractures—advantages not fully captured by individual complication rates due to limited sample size. This aligns with studies reporting fewer neurological deficits in ultrasonic osteotomy.22 Our findings corroborate Scarano et al23 regarding alveolar preservation but extend evidence to pain biomarker modulation—a novel contribution to the field.
Several limitations warrant acknowledgment: (1) retrospective single-center design limits generalizability; (2) short-term follow-up (72h) precludes assessment of chronic pain or nerve recovery; (3) surgeons were unblinded to techniques due to device distinctiveness; and (4) homogeneous impactions (Pell & Gregory C1) may not reflect complex cases. Future multi-center RCTs with longer follow-up, diverse impaction classes, and standardized biomarker sampling protocols are needed to validate these findings.
Conclusion
In this cohort of Pell & Gregory Class C1 mandibular third molars, ultrasonic bone scalpel extraction demonstrated clear advantages over turbine drilling: reduced operative time, attenuated inflammatory responses (as evidenced by TNF-α/ICAM-1/MPO levels), diminished pain biomarker expression (CGRP/SP/5-HT), and lower patient-reported pain scores. These benefits, coupled with its favorable safety profile, position ultrasonic osteotomy as a preferred technique for impacted tooth removal when resources permit.
Disclosure
Ge Wang and Hui Wang are-co-first authors for this study. The authors report no conflicts of interest in this work.
References
1. Ye ZX, Qian WH, Wu YB, Yang C. Pathologies associated with the mandibular third molar impaction. Sci Prog. 2021;104(2):368504211013247. PMID: 33913399; PMCID: PMC10454952. doi:10.1177/00368504211013247
2. Palikaraki G, Mitsea A, Sifakakis I. Effect of mandibular third molars on crowding of mandibular teeth in patients with or without previous orthodontic treatment: a systematic review and meta-analysis. Angle Orthod. 2024;94(1):122–132. PMID: 37848193; PMCID: PMC10928940. doi:10.2319/032323-205.1
3. Altinöz HC, Gökbudak R, Bayraktar A, Belli S. A pilot study of measurement of the frequency of sounds emitted by high-speed dental air turbines. J Oral Sci. 2001;43(3):189–192. PMID: 11732739. doi:10.2334/josnusd.43.189
4. Shackelford D, Casani JA. Diffuse subcutaneous emphysema, pneumomediastinum, and pneumothorax after dental extraction. Ann Emerg Med. 1993;22(2):248–250. PMID: 8427441. doi:10.1016/s0196-0644(05)80214-8
5. Wang Q, Zhang T. Application of an ultrasonic bone knife combined with a dental electric motor in the extraction of mandibular middle and low impacted teeth. BMC Oral Health. 2024;24(1):18. PMID: 38178077; PMCID: PMC10768189. doi:10.1186/s12903-023-03788-0
6. Blagova B, Krastev D, Malinova L. Conventional drilling versus ultrasound and laser osteotomy in mandibular third molar surgery: a comparative study. Lasers Surg Med. 2023;55(10):862–870. Epub 2023 Oct 9. PMID: 37811576. doi:10.1002/lsm.23730
7. Kim S, Liu M, Simchon S, Dörscher-Kim JE. Effects of selected inflammatory mediators on blood flow and vascular permeability in the dental pulp. Proc Finn Dent Soc. 1992;88 Suppl 1:387–392. PMID: 1508895.
8. Kopp S. Neuroendocrine, immune, and local responses related to temporomandibular disorders. J Orofac Pain. 2001;15(1):9–28. PMID: 11889652.
9. Song Y, Zhao H, Liu J, Fang C, Miao R. Effects of citral on lipopolysaccharide-induced inflammation in human umbilical vein endothelial cells. Inflammation. 2016;39(2):663–671. PMID: 26658749. doi:10.1007/s10753-015-0292-0
10. Tian M, Dong J, Wang Z, Lu S, Geng F. The effects and mechanism of Kangfuxin on improving healing quality and preventing recurrence of gastric ulcer. Biomed Pharmacother. 2021;138:111513. PMID: 33761454. doi:10.1016/j.biopha.2021.111513
11. de Santana-Santos T, de Souza-Santos a A, Martins-Filho PR, da Silva LC, de Oliveira E Silva ED, Gomes AC. Prediction of postoperative facial swelling, pain and trismus following third molar surgery based on preoperative variables. Med Oral Patol Oral Cir Bucal. 2013;18(1):e65–e70. doi:10.4317/medoral.18039
12. Sivolella S, Brunello G, Panda S, Schiavon L, Khoury F, Del Fabbro M. The bone lid technique in oral and maxillofacial surgery: a scoping review. J Clin Med. 2022;11(13):3667. doi:10.3390/jcm11133667
13. Rashid N, Subbiah V, Agarwal P, et al. Comparison of piezosurgery and conventional rotatory technique in transalveolar extraction of mandibular third molars: a pilot study. J Oral Biol Craniofacial Res. 2020;10(4):615–618. doi:10.1016/j.jobcr.2020.08.021
14. Menziletoglu D, Tassoker M, Kubilay-Isik B, Esen A. The assesment of relationship between the angulation of impacted mandibular third molar teeth and the thickness of lingual bone: a prospective clinical study. Med Oral Patol Oral Cir Bucal. 2019;24(1):e130–e135. PMID: 30573722; PMCID: PMC6344005. doi:10.4317/medoral.22596
15. Durukan P, Salt O, Ozkan S, Durukan B, Kavalci C. Cervicofacial emphysema and pneumomediastinum after a high-speed air drill endodontic treatment procedure. Am J Emerg Med. 2012;30(9):2095.e3–6. Epub 2012 Feb 4. PMID: 22306391. doi:10.1016/j.ajem.2012.01.006
16. Matsumoto S, Koyanagi N, Matsuo M, et al. A case of widespread emphysema following the extraction of mandibular third molar under intravenous sedation. Masui. 2001;50(3):278–280. Japanese. PMID: 11296440.
17. Scarano A, Murmura G, Sinjiari B, et al. Expansion of the alveolar bone crest with ultrasonic surgery device: clinical study in mandible. Int J Immunopathol Pharmacol. 2011;24(2 Suppl):71–75. PMID: 21781449. doi:10.1177/03946320110240S213
18. Robiony M, Polini F, Costa F, Zerman N, Politi M. Ultrasonic bone cutting for surgically assisted rapid maxillary expansion (SARME) under local anaesthesia. Int J Oral Maxillofac Surg. 2007;36(3):267–269. PMID: 17112705. doi:10.1016/j.ijom.2006.08.013
19. Scolozzi P. Buccal corticotomy using piezosurgery as a surgical approach for removal of deeply impacted mandibular teeth: an alternative procedure to avoid pitfalls associated with the conventional technique. J Stomatol Oral Maxillofac Surg. 2022;123(2):142–146. PMID: 33930598. doi:10.1016/j.jormas.2021.04.012
20. Närhi M. Interaction between the autonomic and sensory nerves in the dental pulp. Proc Finn Dent Soc. 1989;85(4–5):389–393. PMID: 2699764.
21. Pan WZ, Shi CX, Tian M, Yu JG. Anti-CD11c antibody, Efalizumab attenuate ventilator-induced lung injury. Eur Rev Med Pharmacol Sci. 2014;18(15):2182–2190. PMID: 25070825.
22. Liu J, Hua C, Pan J, Han B, Tang X. Piezosurgery vs conventional rotary instrument in the third molar surgery: a systematic review and meta-analysis of randomized controlled trials. J Dental Sci. 2018;13(4):342–349. doi:10.1016/j.jds.2016.09.006
23. Scarano A, Piattelli A, Murmura G, Iezzi G, Assenza B, Mancino C. Delayed expansion of the atrophic mandible by ultrasonic surgery: a clinical and histologic case series. Int J Oral Maxillofac Implants. 2015;30(1):144–149. PMID: 25615922. doi:10.11607/jomi.2753
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Temporal Changes in Ankle Joint Pathology, Pain and Secondary Osteoporosis in Collagen-Induced Arthritis Rats
Liu Q, Nan N, Li W, Dong M, Pu W, Liu Y, Zhao J, Hao H
Journal of Inflammation Research 2024, 17:9795-9804
Published Date: 26 November 2024
Application of Multidisciplinary Rehabilitation Nursing in Patients with Brucellar Spondylitis and Its Effects on Pain, Inflammation, and Immune Function
Zhang Y, Zuo X, Yang X, Li R, Wang H, Yu J, Yang X
Journal of Multidisciplinary Healthcare 2025, 18:3813-3826
Published Date: 2 July 2025
Immune Mechanisms and Pain in Intervertebral Disc Degeneration
Cheng H, Wang L, Huang C, Yang Z, Wu H, Fang Z
Journal of Inflammation Research 2025, 18:16843-16855
Published Date: 1 December 2025