Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Type 2 Diabetes Mellitus and Chronic Obstructive Pulmonary Disease – from Pathophysiology to Effective Management Overview
Authors Prisacaru V ![]() , Covantsev S
, Covantsev S ![]() , Ceasovschih A, Sivapalan P, Tural S
, Ceasovschih A, Sivapalan P, Tural S ![]() , Corlateanu A
, Corlateanu A ![]() , Deleanu OC
, Deleanu OC
Received 14 March 2026
Accepted for publication 22 May 2026
Published 3 June 2026 Volume 2026:21 609302
DOI https://doi.org/10.2147/COPD.S609302
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Zijing Zhou
Victor Prisacaru,1 Serghei Covantsev,2 Alexandr Ceasovschih,3 Pradeesh Sivapalan,4,5 Seda Tural,6 Alexandru Corlateanu,7 Oana Claudia Deleanu8
1Department of Endocrinology, Nicolae Testemitanu State University of Medicine and Pharmacy, Municipal Clinical Hospital No. 1 “Gheorghe Palade”, Chisinau, Republic of Moldova; 2Department of Surgical Oncology, Federal State Autonomous Institution National Medical Research Centre “Treatment and Rehabilitation Centre” of the Ministry of Health of the Russian Federation, Moscow, Russia; 3Grigore T. Popa University of Medicine and Pharmacy, Iasi, Romania; 4Department of Clinical Medicine, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark; 5Copenhagen Respiratory Research, Department of Medicine, Copenhagen University Hospital—Herlev and Gentofte, Copenhagen, Denmark; 6Department of Chest Disease, Yedikule Chest Diseases and Thoracic Surgery Training and Research Hospital, University of Health Sciences, Istanbul, Turkey; 7Division of Pneumology and Allergology, Department of Internal Medicine, Nicolae Testemitanu State University of Medicine and Pharmacy, Chisinau, Republic of Moldova; 8Departament of Pneumology, UMF “Carol Davila”, Bucuresti, Romania
Correspondence: Alexandru Corlateanu, Division of Pneumology and Allergology, Department of Internal Medicine, Nicolae Testemițanu State University of Medicine and Pharmacy, Chisinau, Republic of Moldova, Email [email protected]
Abstract: Type 2 diabetes mellitus (T2DM) and chronic obstructive pulmonary disease (COPD) are two chronic conditions with significant global impact and high incidence, frequently occurring as comorbidities. This article analyzes the particularities of pathophysiological, genetic, and epigenetic interactions, as well as the therapeutic implications in patients with both conditions. Additionally, the clinical management of these patients is investigated in correlation with updated international guidelines, such as the Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2026 and the American Diabetes Association (ADA) 2026. The importance of rigorous monitoring, personalized treatment, and the use of modern therapies with proven benefits—including sodium-glucose cotransporter 2 inhibitors (SGLT2i) and glucagon-like peptide-1 (GLP-1) receptor agonists—is highlighted. The conclusion emphasizes the necessity of an integrated, multidisciplinary approach aimed at preventing complications, reducing cardiovascular risk, and improving the quality of life in comorbid patients.
Keywords: chronic obstructive pulmonary disease, type 2 diabetes mellitus, systemic inflammation, cardiovascular risk, sodium–glucose cotransporter 2 inhibitors, glucagon-like peptide-1 receptor agonists
Introduction
The interconnection between type 2 diabetes mellitus and chronic obstructive pulmonary disease (COPD) has become a central focus in recent medical research. This shift is driven by the continuous global rise in the prevalence of both diseases. Studying the relationship between these conditions is vital because they share key pathophysiological aspects. These include systemic inflammation, oxidative stress, and metabolic alterations. From these shared pathways arises a significant clinical and therapeutic interdependence.1
According to the GOLD 2026 report, COPD remains one of the top three causes of mortality worldwide. It is responsible for approximately 3 million deaths annually. The global prevalence is estimated at around 10% among adults aged ≥40 years. Widespread underdiagnosis further accelerates disease progression. Consequently, it increases the healthcare burden associated with comorbidities. In parallel, type 2 diabetes mellitus continues to show a rising prevalence worldwide. Estimates from the International Diabetes Federation indicate that approximately 589 million adults currently live with diabetes. This figure represents over 10% of the adult population. This high prevalence is coupled with shared risk factors like chronic low-grade inflammation, aging, smoking, obesity, and a sedentary lifestyle. Together, these factors drive the epidemiological overlap between type 2 diabetes mellitus and COPD. This reality aligns perfectly with the current recommendations of the ADA 2026 guidelines.2,3
Recent epidemiological data show that approximately 30% of patients with COPD also suffer from type 2 diabetes mellitus. The coexistence of these pathologies leads to a severe decline in clinical outcomes. It also causes an increased frequency of hospitalizations and higher mortality rates. The simultaneous presence of these diseases is explained by shared pathogenic mechanisms. Chronic inflammation and insulin resistance act as key drivers, continuously amplifying and worsening each other.4
Systemic inflammation is a crucial driving mechanism, mainly mediated by tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6). However, the link between COPD and insulin resistance is fundamentally multifactorial. This connection must be framed within the broader context of multimorbidity, rather than following a single causal pathway. In line with the updated GOLD report, this relationship involves multiple interacting mechanisms. Factors such as smoking, obesity, physical inactivity, and chronic hypoxia play major synergistic roles. Adipokine dysregulation and frequent corticosteroid use further compound this risk. These molecules and risk factors directly disrupt glucose metabolism. They alter pancreatic β-cell function and increase the overall risk of diabetes. In parallel, manifest hyperglycemia in diabetes exacerbates systemic oxidative stress. This metabolic stress further impairs pulmonary function. Ultimately, this interaction establishes a dangerous vicious cycle between the two conditions.1,4
A recent study based on Mendelian randomization demonstrates a confirmed causal relationship between these conditions. The data indicate that COPD may be a direct triggering factor for the development of type 2 diabetes mellitus.5 This finding carries clear clinical implications. It underscores the need for regular glycemic monitoring in COPD patients and systematic pulmonary function assessment in diabetic patients. The ultimate goal remains early detection and timely management of these comorbidities.5
Likewise, another recent study demonstrates that patients affected simultaneously by both diseases face a significantly higher risk of cardiovascular complications. These include heart failure and major coronary events, compared to patients with only a single pathology. Mortality is also significantly higher in cases of concomitant involvement. This study strongly confirms the importance of a complex, multidisciplinary approach to managing these patients.4
The duration of type 2 diabetes also negatively influences the progression of COPD. Patients with a diabetes duration of more than 7 years face a significantly higher mortality risk than those with a shorter duration. This underscores the absolute necessity of early, aggressive management to avoid long-term complications.6
Regarding therapeutic strategies, recent data offer insights of multidisciplinary interest. Studies show that the use of sodium-glucose cotransporter 2 inhibitors (SGLT2i) is associated with a significant reduction in severe COPD-related outcomes. These include fewer hospitalizations and a reduced need for non-invasive ventilation.7 This clinical benefit can improve the control and clinical evolution of both conditions. It also indirectly reflects a decrease in severe acute exacerbations. The prospect of developing unified therapeutic strategies based on these shared pathways holds strong potential.1,7
Type 2 diabetes mellitus and COPD are chronic conditions with a major global impact. Their epidemiological overlap leads to mutual aggravation. Shared elements like inflammation, insulin resistance, and oxidative stress justify an integrated approach. This strategy must focus on prevention, early diagnosis, and treatment tailored to comorbidities. However, how can clinical management be optimized when the pulmonary and metabolic systems progressively deteriorate each other? Addressing this compelling challenge requires moving beyond isolated, single-organ treatments. Therefore, the primary objective of this review is to provide a comprehensive analysis of these shared pathways. We will evaluate current pharmacological interferences based on the latest 2026 guidelines. Furthermore, we will discuss the role of genetic and epigenetic biomarkers in advancing personalized medicine.
Materials and Methods
A narrative review of the literature was conducted across databases such as PubMed/MEDLINE, Scopus, and Web of Science, using the search terms “COPD”, “type 2 diabetes mellitus”, “systemic inflammation”, “oxidative stress”, “cardiovascular risk”, “SGLT2 inhibitors”, and “GLP-1 receptor agonists”. To help readers assess the relevance of the data, the timeframe for the literature search was restricted to articles published within the last 10 years, with a particular emphasis on recent evidence from the past 5 years. Inclusion criteria encompassed peer-reviewed original studies, comprehensive reviews, meta-analyses, and updated international guidelines (ADA 2026 and GOLD 2026) that addressed the pathophysiological mechanisms or therapeutic strategies in patients with comorbid COPD and type 2 diabetes. Articles were excluded if they were individual case reports, non-peer-reviewed commentaries, abstracts lacking full-text availability, or studies without direct relevance to the research objectives. The selected sources were meticulously reviewed to synthesize the current evidence.
Results
Genetic Factors
The comorbidity between COPD and type 2 diabetes mellitus is frequently observed in clinical practice. An increasing number of studies support the idea that both diseases, having a chronic inflammatory character, may be influenced or determined by shared genetic and epigenetic factors. The presence of these factors not only contributes to the simultaneous onset of the diseases but may also explain the increased severity observed in such patients.
Recent studies show that certain genes may influence the risk of both COPD and type 2 diabetes mellitus. For example, it is well known that variations in the ADRB2 gene, which encodes the beta-2 adrenergic receptor, can affect how the body responds to oxidative stress and inflammation. These genetic variations can impair both pulmonary function in COPD and insulin sensitivity in patients with type 2 diabetes mellitus. Another relevant example is the PPARG gene, which is directly involved in glucose metabolism and inflammatory processes. This effect is well documented in type 2 diabetes and is increasingly associated with COPD risk through modulation of the pulmonary inflammatory cascade.8
Notably, a 2025 study utilizing modern bioinformatics and AI techniques identified a highly significant set of 186 shared genes that undergo alterations in both diseases. Among these, CADPS, EDNRB, THBS4, and TMEM27 were prominently recognized as valuable potential genetic biomarkers. With increasing accessibility to genetic sequencing technologies, these markers could become essential tools in everyday clinical practice for early diagnosis and targeted intervention.9
Epigenetic Factors
In addition to heredity, gene expression can be modified by environmental factors through epigenetic mechanisms—such as DNA methylation, histone modifications, or microRNAs. In COPD, epigenetic changes have been detected in lung tissue cells, being involved in chronic inflammation and tissue destruction. DNA methylation has been shown to have transgenerational effects, and early genetic analysis (eg, from umbilical cord blood at birth) could have strong predictive value.10
In diabetes mellitus, these changes are directed toward the function of pancreatic beta cells and mechanisms involved in insulin sensitivity. For instance, exposure to environmental pollutants or an unbalanced diet can lead to the methylation of certain genes, which consequently causes metabolic imbalance.10,11
Another element involved in COPD is the role of macrophages. A study conducted in 2024 investigated the mechanism of epigenetic changes and their influence on macrophage activity. According to this study, influencing factors contribute to DNA methylation and histone modification. These, in turn, drive the transition of macrophages from a “reparative” M2 phenotype to an inflammatory M1 phenotype. This transition reduces the phagocytic capacity of macrophages, promotes the inflammatory response, and modulates the immune response in a way that aggravates COPD.9,12
However, it is crucial to note that, to date, there are no validated epigenetic markers definitively shared between COPD and diabetes mellitus. The current evidence regarding epigenetic overlap remains largely based on plausible biological associations rather than established causal mechanisms.
Therapeutic Implications
Understanding these underlying molecular links offers a strong perspective for personalized medicine. The identification of shared genetic biomarkers, such as the aforementioned 186-gene set, directly paves the way for early diagnosis and the development of personalized therapeutic strategies tailored to the comorbid patient.12
Implementing these genetic profiling methods in clinical practice could significantly enhance treatment efficacy and allow for the timely prediction of clinical evolution. While targeting epigenetic pathways (eg, through histone deacetylase inhibitors) represents a promising future research direction for developing novel therapies, their clinical application will require the definitive validation of shared causal mechanisms.
Pathophysiology
COPD and diabetes mellitus are often comorbid conditions and share a series of pathophysiological mechanisms that contribute to the mutual aggravation of these diseases. The interaction between these conditions is not merely a superimposition of mechanisms but rather a network of interdependent processes. The main pathophysiological mechanisms linking to COPD and type 2 diabetes are schematically illustrated in Figure 1.
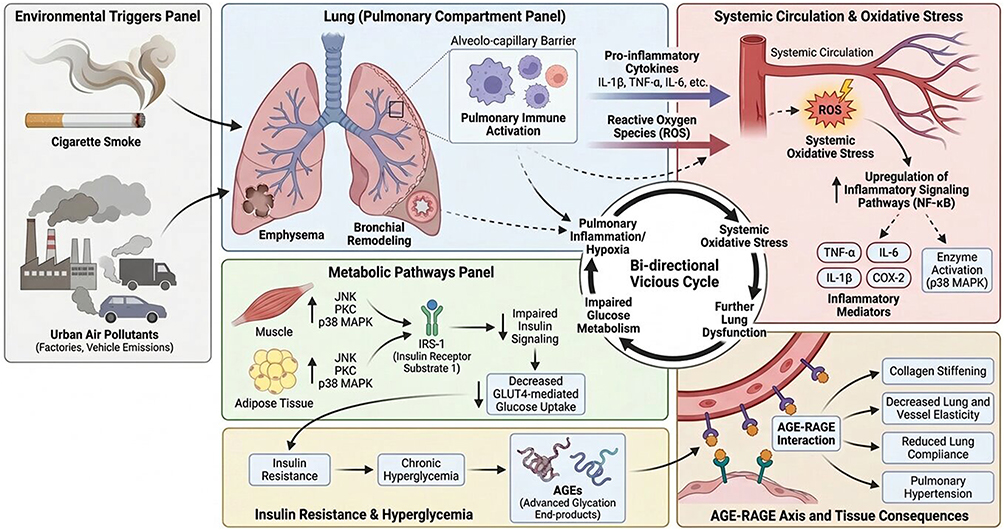

To elucidate the pathophysiological interaction, we must begin with cigarette smoke and other pollutants which, upon reaching the pulmonary alveoli, interact with macrophages. This process initiates several key downstream mechanisms:
Activated macrophages release pro-inflammatory cytokines such as TNF-α, IL-6, interleukin 1 beta (IL-1β), interleukin 8 (IL-8), and chemokines, attracting neutrophils and T lymphocytes, leading to alveolar-bronchial destruction and remodeling. Some of these cytokines cross the alveolo-capillary barrier and trigger systemic inflammation.13
Activated macrophages and neutrophils also produce superoxide, peroxide, and nitrites, collectively known as reactive oxygen species (ROS). In systemic circulation, ROS overwhelm antioxidant systems, resulting in oxidative stress—an important pathogenic factor.14
ROS and cytokines have the capacity to activate nuclear factor kappa B (NF-κB), thereby inducing the transcription of pro-inflammatory genes such as TNF-α, IL-6, IL-1β, and cyclooxygenase 2 (COX-2). Additionally, p38 mitogen-activated protein kinase (p38 MAPK) signals the production of stress proteins and enzymes such as matrix metalloproteinase-9 (MMP-9), elastase, and collagenases—responsible for bronchial remodeling and destruction of pulmonary parenchyma (emphysema).
Cytokines such as TNF-α and IL-6, released systemically from the lungs, alter the function of insulin receptor substrate-1 (IRS-1). Instead of being tyrosine-phosphorylated, IRS-1 is serine-phosphorylated, which blocks insulin signaling. This means that, despite the presence of insulin, glucose is not efficiently absorbed by cells—resulting in insulin resistance. Moreover, ROS activate enzymes such as p38 MAPK, c-Jun N-terminal kinase (JNK), protein kinase C (PKC), which have the same negative effect on IRS-1 and glucose transporter type 4 (GLUT-4), blocking glucose uptake in muscle and adipose tissues.14
Advanced glycation end products (AGEs) result from the non-enzymatic reaction between excess glucose and proteins/lipids/collagen types. They slowly accumulate in various tissues under conditions of chronic hyperglycemia. AGEs bind to their receptors for advanced glycation end products (RAGE), located on endothelial, alveolar, and immune cells. Activation of RAGE leads to the reactivation of NF-κB, further driving the transcription of pro-inflammatory cytokines and ROS production, particularly in the lungs and blood vessels. Additionally, AGEs cause collagen stiffening, reducing the elasticity of vessels and pulmonary tissue, thereby worsening COPD (by reducing lung compliance) and contributing to pulmonary hypertension.15
Thus, an integrated mechanism emerges: pulmonary inflammation and hypoxia induce systemic oxidative stress, alter glucose metabolism and insulin production, while hyperglycemia generates ROS and AGEs that further deteriorate lung function and exacerbate insulin resistance.16
Cardiovascular Risk
COPD and type 2 diabetes mellitus, as two chronic conditions with significant epidemiological impact on morbidity and mortality, also have a substantial influence on the patient’s cardiovascular prognosis. Although they affect different organs, more and more studies confirm the dramatic impact of this comorbidity on the cardiovascular system. This impact is not coincidental but is mediated by shared pathogenic links such as chronic inflammation, oxidative stress, and endothelial dysfunction.17
Systemic inflammation is characteristic of both conditions. In COPD, persistent airway inflammation extends systemically through elevated serum levels of cytokines such as IL-6, TNF- α, and C-reactive protein (CRP). In type 2 diabetes mellitus, chronic inflammation contributes to the exacerbation of insulin resistance and the progression of cardiovascular complications. In the comorbidity between COPD and type 2 diabetes, the inflammatory background is intensified, significantly increasing the susceptibility to major cardiovascular events.18
A study conducted in 2023 on a cohort of 120,000 patients with type 2 diabetes showed that approximately 12% of them also had COPD. In this study, overall mortality, as well as cardiovascular and respiratory mortality, were significantly higher in patients with COPD. Additionally, the risk of hospitalization due to heart failure was elevated, emphasizing the double burden of these diseases.19
Another notable observation is that the simultaneous presence of type 2 diabetes and COPD significantly increases the disproportionate risk of heart failure. A study based on medical registries in Sweden compared a cohort of comorbid patients to the general population. According to the results of this study, the group of interest had a fourfold higher risk of developing heart failure. This interaction suggests a pathological synergy between COPD and type 2 diabetes mellitus.20
Beyond the persistent chronic inflammation seen in COPD, progressive decline in pulmonary function is another negative factor for patients with type 2 diabetes. A recent prospective study demonstrated that a decrease in spirometric indices, such as forced expiratory volume in 1 second (FEV1), is associated with an increased incidence of cardiovascular events in patients with type 2 diabetes. Therefore, systematic spirometric evaluation of comorbid patients may serve as a risk stratification factor.21
Modern therapeutic approaches can significantly reduce cardiovascular risk even in the presence of comorbidities. In 2022 the EMPA-REG OUTCOME trial was conducted. In this study, Empagliflozin, an SGLT2 inhibitor, significantly reduced the risk of cardiovascular death and hospitalization for heart failure in patients with comorbidities including COPD. This cardiovascular risk reduction benefit appears to be independent of pulmonary function, suggesting that certain antihyperglycemic agents may exert favorable pleiotropic effects.22
Therefore, comorbid patients represent a vulnerable group with elevated cardiovascular risk. These patients require an integrated, multidisciplinary clinical approach, which should include meticulous glycemic monitoring, optimization of respiratory therapy, comprehensive management of cardiovascular risk, and pharmacological interventions with proven potential to reduce mortality. Moreover, early diagnosis could be essential in preventing the severe, often irreversible or fatal complications.17
Pharmacological Interferences in COPD and Type 2 Diabetes Comorbidity
The coexistence of COPD and diabetes mellitus in the same patient can be a challenge for clinicians because the treatment intended for one of the diseases can negatively influence the manifestations and evolution of the other. Effective pharmacological management in such patients requires a deep understanding of drug interactions and a complex therapeutic approach. Rigorous glycemic control is one of the keys to effective management of comorbid patients. Maintaining glycated hemoglobin (HbA1c) below 7% can significantly reduce the frequency of COPD exacerbations by improving inflammatory processes and slowing the impairment of pulmonary parenchyma.
Inhaled and systemic corticosteroids are one of the pillars of COPD treatment due to their strong anti-inflammatory effect and ability to reduce the number of exacerbations, improving disease progression. Despite these advantages, prolonged use of systemic corticosteroids can alter carbohydrate metabolism, contributing to the decompensation of diabetes mellitus. Thus, patients who receive systemic glucocorticoid treatment require regular reevaluation of glycemic values with adjustment of antidiabetic treatment as needed.1,2
It should be noted that, according to a meta-analysis conducted in 2021, the use of inhaled corticosteroids does not have a significant effect on the onset or progression of diabetes mellitus.23
Regarding oral antidiabetic therapy, we must mention Metformin, which for many years has been the first-line oral antidiabetic drug in the treatment of type 2 diabetes mellitus. Its curative effects refer to improving insulin sensitivity and reducing hepatic glucose production. Besides its direct effects on carbohydrate metabolism, metformin has proven anti-inflammatory and antioxidant effects which undoubtedly are beneficial in COPD. However, in patients with advanced COPD and chronic hypoxemia, there is an increased risk of lactic acidosis, which requires caution in the use of metformin, avoiding its initiation in unstable patients, and carefully monitoring of respiratory function, and lactate levels.24
Another promising class of oral antidiabetics is SGLT2 inhibitors, which inhibit renal glucose reabsorption and promote its excretion in urine. This class of oral antidiabetics offers cardiovascular and renal benefits demonstrated by recent studies. The use of SGLT2 inhibitors in patients with COPD is beneficial by reducing the risk of severe COPD-related outcomes, such as hospitalizations and the need for non-invasive ventilation; however, since consistent improvements in respiratory function have not been definitively demonstrated, this metabolic treatment should be framed primarily as a strategy to reduce severe acute events. Caution is required due to the increased risk of dehydration and hydro-electrolytic disturbances.7,25
GLP-1 receptor agonists contribute to glucose-dependent insulin secretion and inhibit glucagon secretion, contributing to glycemic control. Another advantage of this class of antidiabetics is the increased potential for weight loss and significant reduction in cardiovascular risk, being indicated in patients with ischemic heart disease (IHD) in medical history. Recent studies suggest that GLP-1 agonists may have additional anti-inflammatory effects on the respiratory pathways, providing a supplementary benefit to patients with COPD.26–28
The combination of SGLT2 inhibitors and GLP-1 agonists offers superior glycemic control, cardiovascular and renal benefits, as well as potential anti-inflammatory effects. This combined therapy may be beneficial in patients with COPD and type 2 diabetes, addressing multiple aspects of comorbidities. However, combined therapy may increase the risk of adverse effects, such as urinary tract infections, requiring careful monitoring and individualization of treatment.25,30
Statin therapy has been associated with a reduced risk of severe exacerbations in patients with chronic obstructive pulmonary disease (COPD), particularly in those with cardiovascular comorbidities or type 2 diabetes mellitus. Recent evidence suggests that statins may lower both the risk of hospitalization due to COPD exacerbations and overall mortality, although some studies are limited by size and methodology.31,32
The pleiotropic effects of statins include anti-inflammatory, antioxidant, and immunomodulatory properties, which may contribute to reducing systemic inflammation associated with COPD. Recent meta-analyses indicate that statin therapy can improve pulmonary function, exercise capacity, and symptom burden in patients with COPD26,28 In parallel, international guidelines for diabetes and dyslipidemia recommend statins as first-line therapy for reducing cardiovascular risk in patients with type 2 diabetes, with treatment intensity tailored to overall risk.1 Therefore, in patients with diabetes–COPD comorbidity, statins may provide a dual benefit by addressing cardiovascular risk and modulating systemic inflammation, without being indicated as disease-modifying therapy for COPD itself.29,31
Management of patients with COPD and diabetes mellitus requires an integrated approach involving collaboration between pulmonologists, endocrinologists, cardiologists, and other specialists. Careful monitoring of metabolic and respiratory parameters, adjustment of therapy according to clinical evolution, and patient education are essential for optimizing therapeutic outcomes.
Discussion
Management Strategies
Evaluating the specialized literature in order to elucidate the optimal management for comorbid patients with type 2 diabetes mellitus and COPD, it is inevitable to consult the current clinical recommendations. In the case of COPD, we refer to Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2026, and respectively for type 2 diabetes mellitus, the American Diabetes Association (ADA) 2026 guideline. Knowing that comorbid patients present an increased risk of cardiovascular events, metabolic and respiratory decompensations, it is vital to know the key moments for the optimal management of these patients. Consulting the sources mentioned above, we can highlight an integrated, individualized, and evidence-based therapeutic approach.
Risk and comorbidity assessment is one of the important directions that needs to be addressed. The ADA 2026 guideline mentions that patients with type 2 diabetes mellitus often present cardiovascular complications, renal failure, and chronic pulmonary diseases including COPD. From here it follows that rigorous glycemic control, blood pressure monitoring, and blood lipid management are essential to reduce overall risks.28 Furthermore, this multidimensional interaction emphasizes that cardiovascular and metabolic stability heavily influences long-term respiratory outcomes.4 In turn, GOLD 2026 emphasizes that COPD is often accompanied by metabolic comorbidities including type 2 diabetes mellitus, and monitoring and management of these must be initiated from the diagnostic stage.2 Table 1 provides an overview of key management considerations in patients with comorbid COPD and type 2 diabetes mellitus, differentiating specific therapeutic impacts and precise safety precautions for each pharmacological class.
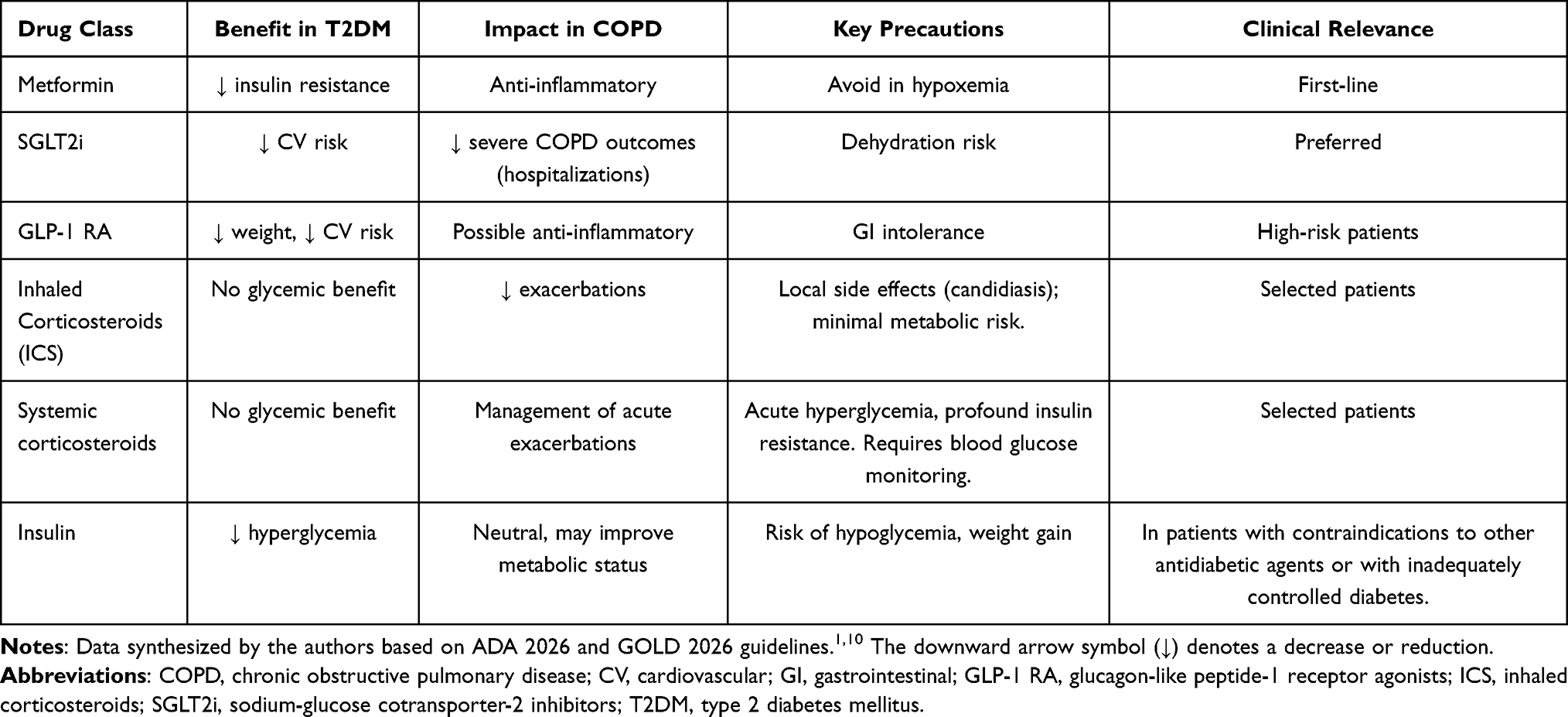 |
Table 1 Integrated Management of Comorbid COPD and Type 2 Diabetes Mellitus |
Optimizing glycemic control is particularly important in comorbid patients, especially considering the pulmonary context. ADA 2026 recommends metformin as the first-line treatment, with the addition of agents with proven cardiovascular and renal benefits such as SGLT2i or GLP-1 RA. It also recommends avoiding sulfonylureas when possible, which carry an increased risk of hypoglycemia and may potentially mask the early signs of a pulmonary exacerbation.28 Similarly, inhaled or systemic glucocorticoids (ICS) in COPD can complicate glycemic control. However, it is critical to distinguish their metabolic risks: while inhaled corticosteroids (ICS) primarily pose a risk of localized effects and minimal systemic absorption modifying long-term HbA1c only in susceptible individuals, systemic corticosteroids induce acute, profound insulin resistance and severe glycemic spikes. For this reason, GOLD 2026 recommends cautious use of corticosteroids, indicating them only for patients with blood eosinophilia or frequent exacerbations.2
Regarding respiratory pharmacological management, the GOLD 2026 guidelines recommend long-acting bronchodilators, including long-acting β2-agonists (LABA) and long-acting muscarinic antagonists (LAMA) as the basic therapy. These, having a metabolically neutral profile, are preferable for comorbid patients. This combined dual bronchodilation therapy may be beneficial in patients with COPD and comorbid type 2 diabetes by maximizing lung function without disrupting glucose homeostasis. The guideline also mentions new preparations such as ensifentrine and dupilumab, promising agents also for comorbid patients.2
We cannot fail to mention in this section the non-pharmacological management, which is covered quite extensively in both guidelines. A balanced diet, regular physical exercise according to functional capacities, and weight reduction are essential common strategies that bring benefits both in type 2 diabetes mellitus and in COPD. Regular monitoring of HbA1c is essential, being recommended at least annually according to the ADA guidelines. Respiratory reevaluation is recommended after exacerbations or adapted to the clinical and functional response of the patient.2,28
The clinical utility of newly identified molecular markers represents a cornerstone for optimizing these management strategies. Specifically, translating the bioinformatic identification of the 186 shared genes—including CADPS, EDNRB, THBS4, and TMEM27—into routine screening protocols could revolutionize early diagnosis.9 Testing patients with an established COPD diagnosis for these specific genetic variations could help clinicians identify individuals at a critically high risk of developing type 2 diabetes long before manifest hyperglycemia occurs, a clinical necessity underscored by recent causal insights.5 This subclinical window allows for the implementation of aggressive, personalized preventive strategies, such as targeted lifestyle modifications and the early initiation of metabolically beneficial therapies like SGLT2i or GLP-1 RA.1 Furthermore, recognizing a patient’s specific genetic profile enables a tailored therapeutic approach, guiding the selection of pharmacological agents that address shared pathways and shifting the paradigm from generic treatment to precision medicine.4
Future Research Directions
The integration of advanced bioinformatic tools and multi-omics analysis represents the next frontier in unraveling the complex interactome between COPD and metabolic dysregulation. Future longitudinal studies are urgently required to clinically validate the predictive power of the shared 186-gene set in diverse patient cohorts.9 Moreover, expanding bioinformatic pipelines to map specific protein-protein interactions will be essential for discovering entirely new therapeutic targets. Another highly promising area is the development of targeted epigenetic therapies. Since environmental factors actively drive histone modifications and DNA methylation—such as the phenotypic shift of macrophages from the reparative M2 state to the pro-inflammatory M1 state—reversing these processes holds significant therapeutic potential.12 Investigating the safety and efficacy of selective histone deacetylase (HDAC) inhibitors or microRNA-targeted therapeutics could provide novel pathways to arrest both chronic airway destruction and pancreatic beta-cell decline.2,12 However, until these epigenetic mechanisms are definitively proven as causal rather than associative across both conditions, extensive translational research utilizing integrated clinical networks remains vital.1,4
Conclusion
The relationship between type 2 diabetes mellitus and COPD transcends a simple statistical association, outlining a clinical picture with profound systemic implications. The common understanding of pathogenic mechanisms, genetic susceptibility, and therapeutic considerations allows for a reassessment of screening, treatment, and monitoring strategies. The integration of current guidelines into clinical practice, alongside the judicious use of therapies with pleiotropic benefits, offers the opportunity for personalized medicine, capable of responding to the complex challenges of comorbidity. Interdisciplinary collaboration thus becomes not only useful but essential for optimizing patient care.
Abbreviations
ADA, American Diabetes Association; AGEs, advanced glycation end products; COPD, chronic obstructive pulmonary disease; COX-2, cyclooxygenase 2; CRP, C-reactive protein; FEV1, forced expiratory volume in 1 second; GLP-1, glucagon-like peptide 1; GLP-1 RA, glucagon-like peptide-1 receptor agonists; GLUT-4, glucose transporter type 4; GOLD, Global Initiative for Chronic Obstructive Lung Disease; HbA1c, glycated hemoglobin; IHD, ischemic heart disease; IL, interleukin; IL-1β, interleukin 1 beta; IL-6, interleukin 6; IL-8, interleukin 8; IRS-1, insulin receptor substrate 1; JNK, c-Jun N-terminal kinase; LABA, long-acting β2-agonists; LAMA, long-acting muscarinic antagonists; MAPK, mitogen-activated protein kinase; MMP-9, matrix metalloproteinase 9; NF-κB, nuclear factor kappa B; PKC, protein kinase C; RAGE, receptor for advanced glycation end products; ROS, reactive oxygen species; SGLT2, sodium–glucose cotransporter 2; SGLT2i, sodium–glucose cotransporter 2 inhibitors.
Disclosure
The authors report no conflicts of interest, financial or otherwise.
References
1. Cazzola M, Rogliani P, Ora J, et al. Hyperglycaemia and chronic obstructive pulmonary disease. Diagnostics. 2023;13(21):3362. doi:10.3390/diagnostics13213362
2. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for prevention, diagnosis and management of COPD: 2026 report. GOLD; 2026.
3. International Diabetes Federation. IDF Diabetes Atlas.
4. Anghel L, Ciubară A, Patraș D, Ciubară AB. Chronic obstructive pulmonary disease and type 2 diabetes mellitus: complex interactions and clinical implications. J Clin Med. 2025;14(6):1809. doi:10.3390/jcm14061809
5. Wang T, Li J, Huang C, et al. COPD and type 2 diabetes mellitus: a Mendelian randomization study. Front Endocrinol. 2024;15:1302641.
6. Su J, Li M, Wan X, et al. Associations of diabetes, prediabetes and diabetes duration with the risk of chronic obstructive pulmonary disease: a prospective UK Biobank study. Diabetes Obes Metab. 2023;25(9):2575–10. doi:10.1111/dom.15142
7. Yen FS, Wei JC, Huang YH, et al. SGLT-2 inhibitors and the risk of COPD exacerbations and mortality in COPD patients. Ann Am Thorac Soc. 2025;22(2):164–174. doi:10.1513/AnnalsATS.202407-703OC
8. Ji Q, Meng Y, Han X, Yi C, Chen X, Zhan Y. Bioinformatic insights and XGBoost identify shared genetics in chronic obstructive pulmonary disease and type 2 diabetes. Clin Respir J. 2025;19(3):e70057. doi:10.1111/crj.70057
9. Liang Q, Wang Y, Li Z. Comprehensive bioinformatics analysis identifies metabolic and immune-related diagnostic biomarkers shared between diabetes and COPD using multi-omics and machine learning. Front Endocrinol. 2024;15:1475958. doi:10.3389/fendo.2024.1475958
10. Benincasa G, DeMeo DL, Glass K, Silverman EK, Napoli C. Epigenetics and pulmonary diseases in the horizon of precision medicine: a review. Eur Respir J. 2021;57(6):2003406. doi:10.1183/13993003.03406-2020
11. Eriksson Ström J, Kebede Merid S, Pourazar J, et al. Chronic obstructive pulmonary disease is associated with epigenome-wide differential methylation in BAL lung cells. Am J Respir Cell Mol Biol. 2022;66(6):638–647. doi:10.1165/rcmb.2021-0403OC
12. Zhang F, Cui Y, Zhang T, Yin W. Epigenetic regulation of macrophage activation in chronic obstructive pulmonary disease. Front Immunol. 2024;15:1445372.
13. Qi Y, Yan Y, Tang D, et al. Inflammatory and immune mechanisms in COPD: current status and therapeutic prospects. J Inflamm Res. 2024;17:6603–6618. doi:10.2147/JIR.S478568
14. Yaribeygi H, Sathyapalan T, Atkin SL, Sahebkar A. Molecular mechanisms linking oxidative stress and diabetes mellitus. Oxid Med Cell Longev. 2020;2020:8609213. doi:10.1155/2020/8609213
15. Reynaert NL, Vanfleteren LEGW, Perkins TN. The AGE-RAGE axis and the pathophysiology of multimorbidity in COPD. J Clin Med. 2023;12(10):3366. doi:10.3390/jcm12103366
16. Barnes PJ. Inflammatory mechanisms in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2016;138(1):16–27. doi:10.1016/j.jaci.2016.05.011
17. Polman R, Hurst JR, Uysal OF, Mandal S, Linz D, Simons S. Cardiovascular disease and risk in COPD: a state of the art review. Expert Rev Cardiovasc Ther. 2024;22(4–5):177–191. doi:10.1080/14779072.2024.2333786
18. Sattar N, Presslie C, Rutter MK, McGuire DK. Cardiovascular and kidney risks in individuals with type 2 diabetes: contemporary understanding with greater emphasis on excess adiposity. Diab Care. 2024;47(4):531–543. doi:10.2337/dci23-0041
19. Raslan AS, Quint JK, Cook S. All-cause, cardiovascular and respiratory mortality in people with type 2 diabetes and chronic obstructive pulmonary disease in England: a cohort study using the CPRD. Int J Chron Obstruct Pulmon Dis. 2023;18:1207–1218. doi:10.2147/COPD.S407085
20. Smith C, Hasselgren M, Sandelowsky H, Ställberg B, Hiyoshi A, Montgomery S. Disproportionately raised risk of adverse outcomes in patients with COPD and comorbid type 2 diabetes or depression: swedish register-based cohort study. Respir Res. 2025;26(1):84. doi:10.1186/s12931-025-03160-6
21. Chen C, Huang Z, Liu L, Su B, Feng Y, Huang Y. Lung function impairment and risks of incident cardiovascular diseases and mortality among people with type 2 diabetes: a prospective cohort study. Diabetes Care. 2025;48(5):728–736. doi:10.2337/dc24-2188
22. Anker SD, Sander LE, Fitchett DH, et al. Empagliflozin in patients with type 2 diabetes mellitus and chronic obstructive pulmonary disease. Diab Res Clin Pract. 2022;186:109837. doi:10.1016/j.diabres.2022.109837
23. Pu X, Liu L, Feng B, et al. Association between inhaled corticosteroid use and risk of hyperglycemia in COPD patients: systematic review and meta-analysis. Respir Res. 2021;22:201. doi:10.1186/s12931-021-01789-7
24. Andreadi A, Muscoli S, Tajmir R, et al. Recent pharmacological options in type 2 diabetes and synergic mechanism in cardiovascular disease. Int J Mol Sci. 2023;24(2):1646. doi:10.3390/ijms24021646
25. Marfella R, Prattichizzo F, Sardu C, et al. GLP-1 receptor agonists-SGLT-2 inhibitors combination therapy and cardiovascular events after acute myocardial infarction in patients with type 2 diabetes. Cardiovasc Diabetol. 2024;23:10. doi:10.1186/s12933-023-02118-6
26. Miravitlles M. Improving outcomes of chronic obstructive pulmonary disease through the treatment of comorbidities: one step beyond. Am J Respir Crit Care Med. 2023;208(10):1017–1019. doi:10.1164/rccm.202309-1546ED
27. Chen X, Hu F, Chai F, Chen X Effect of statins on pulmonary function in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis of randomized controlled trials. J Thorac Dis. 2023;15(7):3944–3952. doi:10.21037/jtd-23-1042
28. Covantsev S, Corlateanu O, Volkov S, et al. COPD and diabetes mellitus: down the rabbit hole. Curr Respir Med Rev. 2022;18(2):95–103. doi:10.2174/1573398X18666220411123508
29. American Diabetes Association. Standards of medical care in diabetes—2026. Diab Care. 2025;48(Suppl 1):S1–S350. doi:10.2337/dc25-SINT
30. Li J, Li Y, Zhang P, et al. The efficacy and safety of the combination therapy with GLP-1 receptor agonists and SGLT-2 inhibitors in type 2 diabetes: a systematic review and meta-analysis. Front Pharmacol. 2022;13:838277. doi:10.3389/fphar.2022.838277
31. Marx N, Federici M, Schütt K, et al. 2023 ESC Guidelines for the management of cardiovascular disease in patients with diabetes. Eur Heart J. 2023;44(39):4043–4140. doi:10.1093/eurheartj/ehad192
32. Sule NO, Suissa S. Statins and mortality in COPD: a methodological review of observational studies. COPD. 2023;20(1):284–291. [Zhang F, et al. Statins and mortality in COPD: a methodological review of observational studies. Respir Med. 2023; 210: 106752.] doi:10.1080/15412555.2023.2242489
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Framework for Exploration of Statistical Heterogeneity in Multi-Database Studies: A Case Study Using EXACOS-CV Studies
Rhodes KM, Garbe E, Müllerová H, Ekwaru P, Kossack N, Baak BN, Lobier M, Hawkins NM, Nordon C
Clinical Epidemiology 2025, 17:551-565
Published Date: 14 June 2025
Association Between the Aggregate Index of Systemic Inflammation and Non-Dipper Blood Pressure Pattern in Hypertensive Patients with Type 2 Diabetes Mellitus
Yıldırım A, Taş A, Parmak MG, Ateş MS, Sökmen E
Journal of Inflammation Research 2026, 19:604172
Published Date: 25 May 2026