Back to Journals » Journal of Inflammation Research » Volume 19
Association Between the Aggregate Index of Systemic Inflammation and Non-Dipper Blood Pressure Pattern in Hypertensive Patients with Type 2 Diabetes Mellitus
Authors Yıldırım A, Taş A, Parmak MG ![]() , Ateş MS
, Ateş MS ![]() , Sökmen E
, Sökmen E ![]()
Received 6 March 2026
Accepted for publication 13 May 2026
Published 25 May 2026 Volume 2026:19 604172
DOI https://doi.org/10.2147/JIR.S604172
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Qing Lin
Alp Yıldırım, Alperen Taş, Müzeyyen Gizem Parmak, Muhammet Salih Ateş, Erdoğan Sökmen
Department of Cardiology, Ahi Evran University Faculty of Medicine, Kırsehir, Turkey
Correspondence: Muhammet Salih Ateş, Email [email protected]
Purpose: This study aimed to investigate the association between the Aggregate Index of Systemic Inflammation (AISI) and non-dipper blood pressure (BP) pattern in hypertensive (HT) patients with type 2 diabetes mellitus (DM). Given the well-established role of systemic inflammation in circadian BP regulation, we hypothesized that elevated AISI levels would be associated with impaired nocturnal BP decline.
Patients and Methods: A total of 356 newly diagnosed HT patients with type 2 DM and 170 normotensive control subjects were included in this observational study. HT patients were further classified as dipper (n=186) or non-dipper (n=170) based on 24-hour ambulatory blood pressure monitoring (ABPM). AISI was calculated using neutrophil, lymphocyte, platelet, and monocyte counts. Correlation analyses were performed to evaluate the relationship between AISI and ambulatory BP parameters. Multivariate logistic regression analysis with a backward stepwise method was conducted to determine independent predictors of non-dipper status. Receiver operating characteristic (ROC) curve analysis was used to assess the discriminative performance of AISI and other inflammatory indices.
Results: AISI and ln(AISI) levels were significantly higher in non-dipper HT patients than in dipper HT patients and normotensive controls (p< 0.001 for all). Ln(AISI) was positively correlated with nighttime systolic and diastolic BP (p< 0.05). In multivariate logistic regression analysis, ln(AISI) emerged as the strongest independent predictor of non-dipper blood pressure pattern (OR: 14.13, 95% CI: 3.68– 54.32, p< 0.001). In ROC analysis, ln(AISI) showed the highest discriminative performance for identifying non-dipper status, with a sensitivity of 71.0% and specificity of 74.1% at a cutoff value of 5.80 (AUC: 0.757, p< 0.001), outperforming NLR, PLR, SII, and SIRI.
Conclusion: Elevated AISI levels were independently associated with non-dipper blood pressure pattern in hypertensive patients with type 2 diabetes mellitus. These findings suggest that AISI may serve as a practical and integrative biomarker for identifying high-risk patients with impaired circadian blood pressure regulation.
Keywords: aggregate index of systemic inflammation, non-dipper hypertension, ambulatory blood pressure monitoring, type 2 diabetes mellitus, systemic inflammation
Introduction
Hypertension continues to represent a major global health burden and remains a leading contributor to cardiovascular morbidity and mortality.1 Although substantial progress has been achieved in pharmacological treatment and lifestyle-based prevention strategies, many patients still develop progressive vascular injury and target organ damage over time. This heterogeneity in clinical outcomes suggests that factors beyond absolute blood pressure (BP) levels play a decisive role in cardiovascular risk determination.2
Accumulating evidence indicates that the circadian pattern of BP variation is a critical modifier of cardiovascular prognosis. Under normal physiological conditions, BP decreases during nocturnal sleep, a phenomenon referred to as the dipping pattern.3 In contrast, an attenuated or absent nocturnal decline, known as the non-dipper pattern, has been consistently linked to adverse cardiovascular consequences, including myocardial remodeling, arterial stiffening, cerebrovascular events, and increased mortality. Despite its clinical relevance, the biological mechanisms responsible for impaired nocturnal BP reduction are not yet fully elucidated.4
Systemic inflammation has emerged as a key pathophysiological contributor to circadian BP dysregulation. Chronic low-grade inflammatory activity promotes endothelial dysfunction, oxidative stress, and autonomic imbalance, all of which interfere with physiological nocturnal vasodilation. Inflammatory mediators may also influence central autonomic regulation and renal sodium handling, thereby sustaining elevated nighttime BP levels.5
The coexistence of type 2 diabetes mellitus (DM) further amplifies these adverse mechanisms. Diabetes-related metabolic disturbances, including insulin resistance and chronic hyperglycemia, accelerate vascular inflammation, platelet activation, and immune dysregulation. As a result, hypertensive (HT) patients with type 2 DM exhibit a substantially higher prevalence of non-dipper BP patterns and experience a disproportionately increased cardiovascular risk compared with non-diabetic HT individuals.6
Beyond classical metabolic disturbances, type 2 diabetes mellitus is increasingly recognized as a complex immunometabolic disorder characterized by chronic low-grade inflammation, oxidative stress, and endothelial dysfunction. These interrelated mechanisms contribute to vascular remodeling, autonomic dysregulation, and impaired circadian blood pressure control. At the molecular level, hyperglycemia-induced oxidative stress, advanced glycation end-product formation, and inflammatory cytokine activation play a central role in vascular injury and impaired nocturnal blood pressure decline.7
Recent advances in biomedical research have provided novel experimental platforms to better understand these complex mechanisms. In particular, three-dimensional organoid models and organ-on-a-chip technologies have emerged as innovative tools for studying disease pathophysiology in a controlled microenvironment. These approaches allow detailed investigation of cellular interactions, inflammatory pathways, and vascular responses in diabetes, thereby offering new insights into the mechanisms underlying cardiometabolic diseases.8
In recent years, hematological inflammatory markers calculated using standard laboratory blood tests have emerged as accessible tools for cardiovascular risk assessment.9 Markers such as the neutrophil-to-lymphocyte ratio (NLR),9 platelet-to-lymphocyte ratio (PLR),10 systemic immune-inflammation index (SII),11 and systemic inflammation response index (SIRI)12 have been shown to reflect different aspects of immune activation and have been associated with hypertension severity, abnormal BP patterns, and cardiovascular outcomes. However, these indices differ substantially in the biological pathways they represent. NLR mainly reflects the balance between neutrophil-mediated innate immune activation and lymphocyte-related adaptive immune regulation, whereas PLR emphasizes platelet-associated inflammatory and thrombotic activity. SII incorporates platelet and neutrophil counts relative to lymphocytes, and SIRI additionally includes monocyte-mediated inflammatory activity. Although these markers are clinically useful, each captures only selected components of the inflammatory response and may therefore provide an incomplete representation of the multidimensional immune-inflammatory burden involved in non-dipper hypertension.13
The Aggregate Index of Systemic Inflammation (AISI) is a composite measure that consolidates neutrophil, lymphocyte, platelet, and monocyte counts, thereby offering an integrated representation of systemic inflammatory burden.14 By simultaneously reflecting innate immune activation, thrombocytic activity, and adaptive immune regulation, AISI may offer a broader insight into inflammation-driven cardiovascular pathophysiology. While previous studies have linked AISI to unfavorable outcomes in various inflammatory and cardiometabolic conditions, its association with circadian BP patterns in HT patients with type 2 DM remains insufficiently explored.15
Based on this background, we hypothesized that elevated AISI levels would be independently associated with impaired nocturnal blood pressure decline and non-dipper blood pressure pattern in hypertensive patients with type 2 diabetes mellitus. Accordingly, the present study aimed to evaluate the relationship between AISI and nocturnal blood pressure dipping status in this population. In addition, we sought to compare the predictive and discriminative performance of AISI with other commonly used inflammatory indices, including NLR, PLR, SII, and SIRI, in identifying non-dipper blood pressure behavior.
Methods
Data were retrospectively collected at a tertiary referral institution between January 2024 and November 2025 in order to examine the relationship between AISI values and circadian blood pressure variation among hypertensive patients with type 2 diabetes. During the specified study period, documentation of patients who had undergone continuous 24-hour ambulatory blood pressure assessment in the cardiology outpatient setting was retrospectively evaluated.
Participants eligible for enrollment were adults (≥18 years) with verified essential hypertension and concomitant type 2 diabetes mellitus. The diagnosis of diabetes was determined in accordance with widely recognized international criteria, including elevated fasting plasma glucose (≥126 mg/dL), a 2-hour post–oral glucose tolerance test value ≥200 mg/dL following a 75-g glucose load, glycated hemoglobin (HbA1c) ≥6.5%, or documented physician-confirmed diabetes necessitating pharmacological therapy. Exclusion criteria comprised the presence of secondary forms of hypertension, systemic inflammatory or autoimmune disorders, hematological diseases, active infectious processes, malignancy, substantial hepatic impairment, established chronic renal dysfunction, overt heart failure symptoms, hemodynamically significant valvular abnormalities, sustained arrhythmias including atrial fibrillation, recent acute coronary events, as well as insufficient clinical or biochemical data precluding reliable evaluation.
Application of the study selection criteria resulted in a final cohort of 356 hypertensive participants with type 2 diabetes. The reference group consisted of 170 normotensive volunteers matched demographically to the study population and free of any prior clinical diagnosis of hypertension or diabetes. A schematic representation outlining participant screening procedures, exclusion phases, and final cohort categorization is provided in the flowchart (Figure 1).
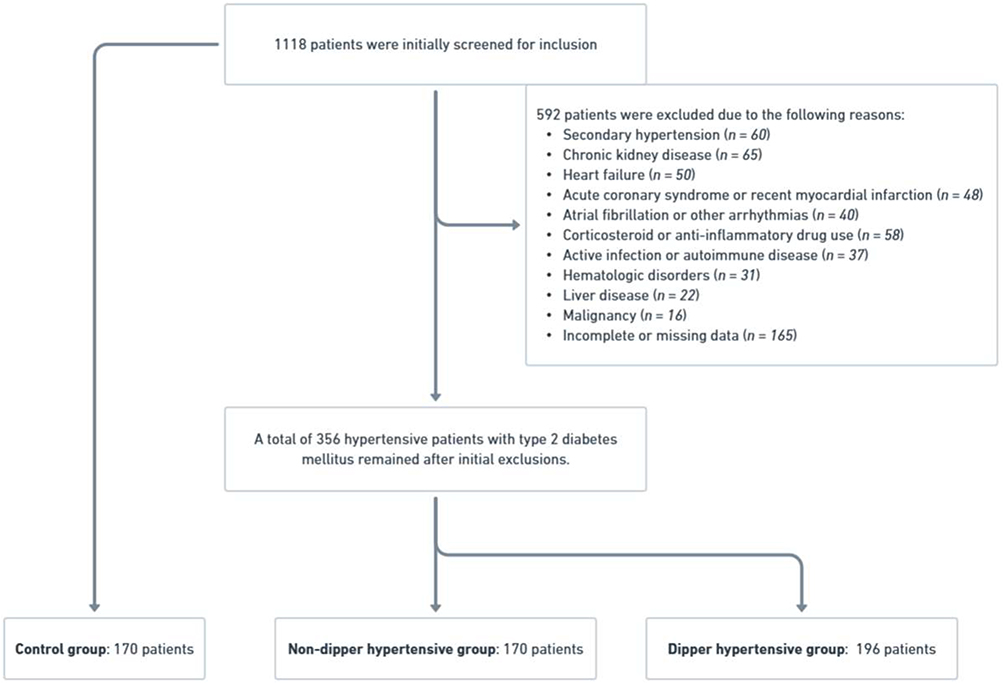 |
Figure 1 Flowchart of participant screening, exclusion criteria, and final cohort classification. |
All enrolled individuals were subjected to 24-hour ambulatory blood pressure evaluation with a validated oscillometric apparatus. The monitoring protocol included automated measurements at 30-minute intervals during daytime activity (06:00–22:00) and at hourly intervals throughout the nocturnal phase (22:00–06:00). Ambulatory BP recordings were considered technically adequate when at least 70% of the expected measurements were successfully obtained, corresponding to a minimum of 14 valid daytime readings and at least 7 valid nighttime readings. For each participant, separate mean systolic and diastolic blood pressure values were determined for the full 24-hour recording, the daytime phase, and the nocturnal phase.
The nocturnal BP decline was defined as the percentage reduction in mean nighttime systolic BP relative to mean daytime systolic BP. Patients exhibiting a nocturnal systolic BP decrease of 10% or greater were classified as having a dipper BP pattern, whereas those with a reduction of less than 10% were categorized as non-dippers. Using this definition,16 individuals with hypertension were classified according to dipping status as either dipper or non-dipper.
Venous blood samples were obtained after an overnight fasting period of at least 8 hours. Complete blood count parameters, including total white blood cell, neutrophil, lymphocyte, platelet, and monocyte counts, were measured using an automated hematology analyzer. The AISI was calculated using the following formula: neutrophil count × platelet count × monocyte count / lymphocyte count.17 In addition to AISI, other inflammation-based indices, including the NLR, PLR, SII, and SIRI, were calculated for comparative analyses.
Routine biochemical parameters, including fasting glucose, glycated hemoglobin, serum creatinine, blood urea nitrogen, and lipid profile components, were determined using standardized laboratory methods. Transthoracic echocardiography was performed by experienced cardiologists who were blinded to ABPM results, using a commercially available ultrasound system. Assessment of left ventricular ejection fraction was carried out using the biplane Simpson methodology, and standard cardiac imaging parameters were obtained in accordance with up-to-date guideline directives. All clinical, laboratory, and ambulatory blood pressure data were collected using standardized institutional protocols and recorded in a consistent manner by trained healthcare personnel.
The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. Ethical approval was obtained from the Ethics Committee of Ahi Evran University Faculty of Medicine (Approval No: 2025–18/236, Date: 25.11.2025) as well as from the Kırşehir Provincial Directorate of Health (Approval No: 294519317).
Given the retrospective nature of the study and the use of fully anonymized data, the requirement for written informed consent was waived by the institutional review board. Patient confidentiality was strictly maintained throughout the study, and all data were handled in compliance with applicable data protection regulations.
Statistical Analysis
All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 26.0 (IBM Corp., Armonk, NY, USA). The distribution of continuous variables was evaluated using the Kolmogorov–Smirnov test. As the majority of continuous variables did not follow a normal distribution according to the Kolmogorov–Smirnov test, non-parametric statistical methods were applied throughout the analyses. In light of the skewed distribution observed in the majority of variables, continuous measures were presented as median (IQR), and discrete variables were displayed as numerical counts accompanied by corresponding percentages. Comparisons among three groups (non-dipper, dipper, and control) were performed using the Kruskal–Wallis test. Differences in categorical parameters were assessed by means of the chi-square statistical method.
Correlations between the AISI and clinical, hematological, and ambulatory BP parameters were analyzed using Spearman’s rank correlation coefficient. Variables with a p value < 0.05 in univariate logistic regression analysis were entered into a multivariate logistic regression model using the backward stepwise likelihood ratio (LR) method to identify independent predictors of non-dipper hypertension. Results were reported as β coefficients, odds ratios (ORs), and 95% confidence intervals (CIs).
The discriminative ability of inflammatory indices—including the natural logarithm of AISI (Ln[AISI]), NLR, PLR, SII, and SIRI for predicting non-dipper status was evaluated using receiver operating characteristic (ROC) curve analysis. The area under the curve (AUC), 95% confidence interval (CI), and optimal cut-off values (determined by the Youden index) were calculated for each parameter. Statistical significance was defined as a two-sided p value below 0.05.
Results
A total of 356 HT patients with type 2 DM and 170 normotensive individuals were included in the final analysis. According to 24-hour ABPM, HT patients were categorized as having a non-dipper (n=170) or dipper (n=186) BP pattern.
An overview of the participants’ demographic features, clinical findings, and laboratory measurements at baseline is provided in Table 1. Age distribution, sex ratio, smoking status, and the prevalence of coronary artery disease and chronic obstructive pulmonary disease were comparable among non-dipper HT patients, dipper HT patients, and normotensive controls (all p>0.05). Body mass index, fasting plasma glucose, glycated hemoglobin, serum creatinine, blood urea nitrogen, hemoglobin levels, and left ventricular ejection fraction did not differ significantly across the groups. In contrast, total cholesterol, low-density lipoprotein cholesterol, and triglyceride concentrations were significantly higher in both HT groups compared with the control group (all p<0.001), whereas high-density lipoprotein cholesterol levels were similar among the three groups.
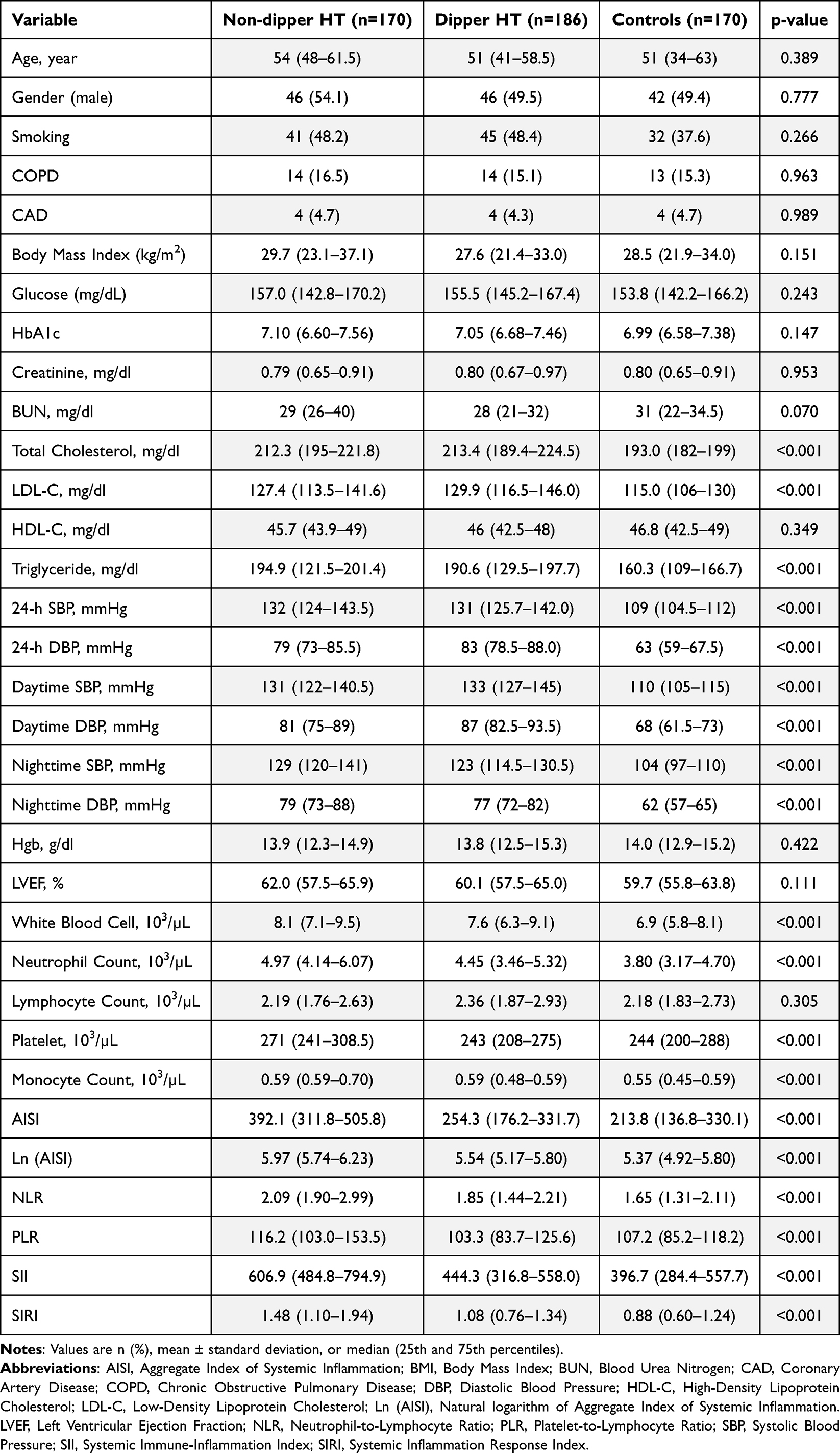 |
Table 1 Baseline Clinical, Biochemical, Echocardiographic, and Ambulatory Blood Pressure Monitoring Parameters of Patients According to Non-Dipper Hypertension, Dipper Hypertension, and Control Groups |
Ambulatory BP parameters showed marked differences between groups. Mean 24-hour, daytime, and nighttime systolic and diastolic BP values were significantly elevated in HT patients compared with normotensive controls (all p<0.001). When HT subgroups were compared, nighttime systolic and diastolic BP values were significantly higher in the non-dipper group than in the dipper group (both p<0.001).
Comparisons of inflammatory and hematological parameters revealed significant group differences. White blood cell, neutrophil, platelet, and monocyte counts were higher in non-dipper HT patients compared with dipper HT patients and control subjects (all p<0.001), whereas lymphocyte counts did not differ significantly among the groups. Accordingly, AISI, Ln(AISI), NLR, PLR, SII, and SIRI were progressively increased from controls to dipper HT patients and were highest in non-dipper HT patients (all p<0.001).
Correlation analyses evaluating the relationship between AISI and clinical variables in HT patients are presented in Table 2. Ln(AISI) showed strong positive correlations with NLR, PLR, SII, and SIRI (all p<0.001). In addition, Ln(AISI) demonstrated significant positive correlations with body mass index, blood urea nitrogen levels, nighttime systolic BP, and nighttime diastolic BP. Analysis did not show a significant correlation of Ln(AISI) with age, markers of glycemic control, lipid variables, daytime blood pressure parameters, hemoglobin concentration, or left ventricular ejection fraction.
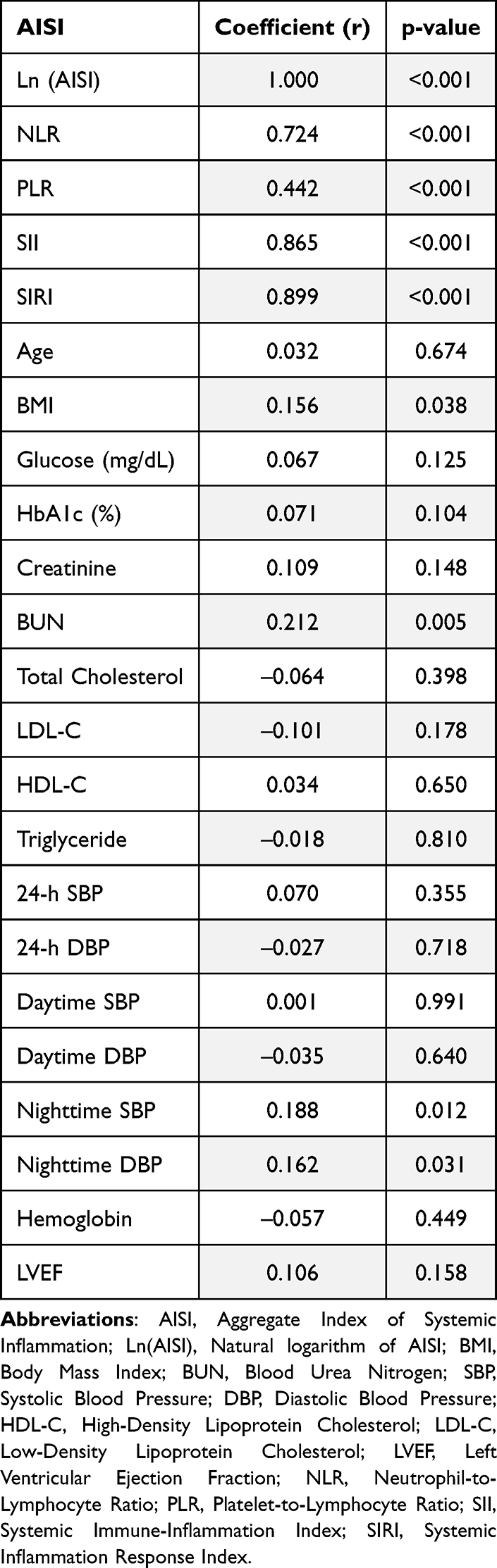 |
Table 2 Bivariate Correlation Analysis According to AISIin Hypertensive Patients |
Univariate and multivariate logistic regression analyses examining factors associated with non-dipper BP pattern are shown in Table 3. In univariate analysis, Ln(AISI), NLR, PLR, SII, SIRI, body mass index, blood urea nitrogen, and nighttime BP parameters were significantly associated with non-dipper status. Multivariate logistic regression employing a backward selection strategy demonstrated that Ln (AISI) remained an independent determinant of non-dipper blood pressure pattern. (β=2.649, odds ratio=14.134, 95% confidence interval: 3.678–54.315, p<0.001). Other inflammatory indices did not retain independent significance after multivariate adjustment.
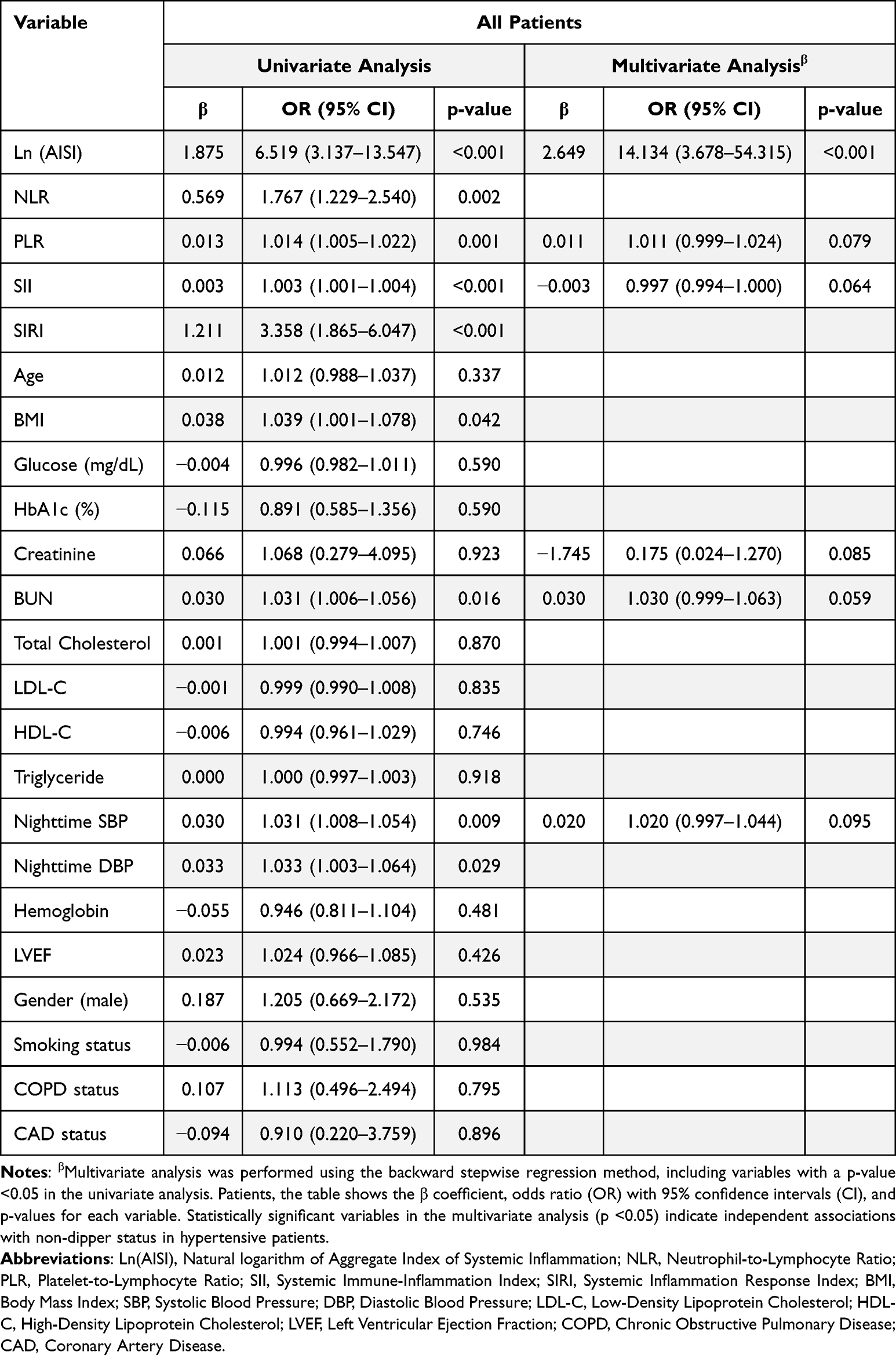 |
Table 3 Univariate and Multivariate Logistic Regression Analyses for Factors Associated with Non-Dipper Status in Hypertensive Patients |
Receiver operating characteristic curve analyses evaluating the discriminative performance of inflammatory indices are illustrated in Figure 2. Ln(AISI) demonstrated the highest area under the curve (AUC=0.757, p<0.001) for distinguishing non-dipper HT patients. An optimal cutoff value of 5.80 yielded a sensitivity of 71.0% and a specificity of 74.1%. The AUC values for SII, SIRI, NLR, and PLR were 0.725, 0.704, 0.671, and 0.657, respectively (all p<0.001) (Table 4).
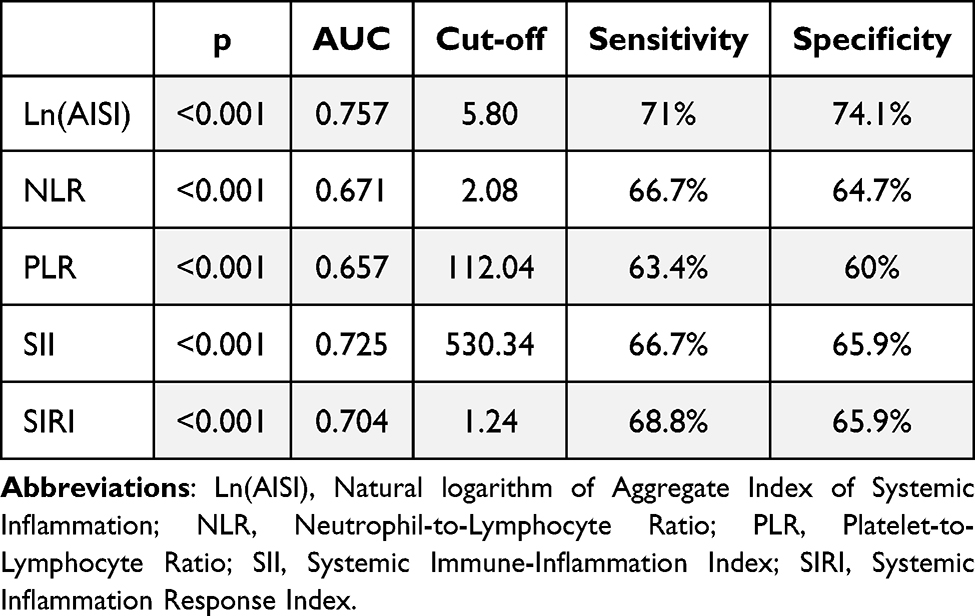 |
Table 4 Receiver Operating Characteristic (ROC) Analysis Illustrating the Diagnostic Performance of Inflammatory Indices |
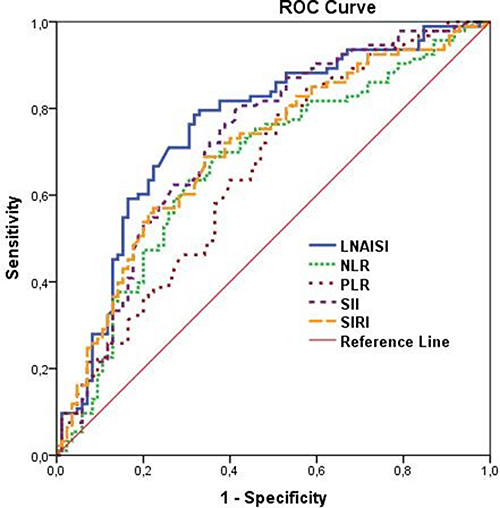 |
Figure 2 Receiver operating characteristic (ROC) curves illustrating the diagnostic performance of inflammatory indices—Ln(AISI), NLR, PLR, SII, and SIRI—for predicting non-dipper blood pressure pattern in newly diagnosed hypertensive patients. |
Discussion
The results indicate that AISI concentrations were significantly greater in non-dipper hypertensive patients with type 2 diabetes and were strongly correlated with attenuated nocturnal blood pressure decline. Among all evaluated inflammatory indices, including NLR, PLR, SII, and SIRI, Ln(AISI) exhibited the highest discriminative performance for identifying non-dipper status. These results indicate that an integrated inflammatory burden reflecting neutrophil activation, platelet reactivity, monocyte-driven chronic inflammation, and lymphocyte suppression provides superior risk stratification compared with isolated or dual-ratio inflammatory biomarkers.
Consistent with our findings, previous studies have established that non-dipper hypertension is closely associated with enhanced systemic inflammation, endothelial dysfunction, sympathetic overactivation, and increased cardiovascular risk.4 Earlier investigations reported that elevated NLR and PLR levels were independently associated with blunted nocturnal BP decline, suggesting that innate immune activation and platelet-driven inflammation contribute to circadian BP dysregulation.18,19 Similarly, SII20 and SIRI21 have been shown to be significantly higher in non-dipper individuals and to correlate with arterial stiffness and target organ damage. In our study, NLR, PLR, SII, and SIRI were all significantly elevated in non-dipper patients and showed significant associations in univariate analysis; however, their predictive performance remained consistently inferior to that of AISI. This observation emphasizes that single- or dual-axis inflammatory markers may not adequately capture the full complexity of immune-mediated vascular injury underlying the non-dipper phenotype.
In patients with type 2 DM, the interaction between inflammation and circadian BP regulation becomes even more pronounced.5 Chronic glucose dysregulation is associated with heightened oxidative stress, increased formation of glycation-related products, endothelial dysfunction, and persistent activation of innate immune responses. Diabetic patients exhibit increased neutrophil activation, platelet hyperreactivity, monocyte infiltration, and impaired lymphocyte-mediated immune regulation.22 These alterations accelerate arterial stiffness, impair baroreflex sensitivity, and disrupt physiological nocturnal BP reduction.23 Our findings extend this framework by demonstrating that AISI, as a unified marker of these immune alterations, robustly identifies diabetic HT patients with impaired circadian BP regulation.
At the cellular level, neutrophils contribute to vascular injury through the release of reactive oxygen species, myeloperoxidase, and neutrophil extracellular traps, all of which promote endothelial damage and nitric oxide depletion. Activated platelets amplify this inflammatory environment by releasing thromboxane A2 and adhesion molecules, facilitating leukocyte recruitment, microvascular thrombosis, and vasoconstriction. Monocytes differentiate into macrophages within the vascular wall, driving foam cell formation and vascular remodeling, whereas lymphopenia reflects impaired adaptive immune control. By integrating these four cellular axes, AISI captures both innate immune activation and adaptive immune suppression within a single quantitative parameter.24
Another important mechanistic link involves autonomic nervous system dysregulation. Non-dipper hypertension is characterized by persistent nocturnal sympathetic activation and attenuated parasympathetic tone. Inflammatory cytokines such as tumor necrosis factor-α and interleukin-6 directly stimulate central sympathetic outflow while simultaneously impairing endothelial nitric oxide bioavailability, thereby preventing physiological nocturnal vasodilation.25 The significant correlations observed between AISI and nighttime systolic and diastolic BPs in our study support the presence of this bidirectional neuro-inflammatory interaction.
Beyond neurohumoral mechanisms, systemic inflammation also disrupts renal sodium handling and nocturnal volume regulation. Pro-inflammatory cytokines impair tubular sodium excretion and activate the intrarenal renin–angiotensin–aldosterone system, leading to nocturnal volume retention and salt-sensitive hypertension.26 In patients with type 2 DM, these effects are further aggravated by early diabetic nephropathy and glomerular hyperfiltration, even in the absence of overt chronic kidney disease.27 The independent association between AISI and non-dipper status observed in our cohort may therefore also reflect inflammation-mediated nocturnal sodium sensitivity and altered pressure–natriuresis relationships.
Oxidative stress-driven vascular remodeling represents another major contributor to circadian BP disruption. Activated neutrophils and monocytes generate excessive reactive oxygen species, leading to uncoupling of endothelial nitric oxide synthase and sustained nocturnal vasoconstriction. Platelets further exacerbate oxidative vascular injury through microvascular aggregation and thromboxane-mediated vasoconstriction.28 The combined effect of these processes results in increased nocturnal vascular resistance and impaired diurnal vascular relaxation.5 By integrating multiple cellular contributors to oxidative injury, AISI likely reflects the cumulative oxidative–inflammatory burden shaping nocturnal vascular tone.17
In addition to oxidative stress–mediated vascular injury, emerging evidence suggests that modulation of inflammatory and oxidative pathways may represent a potential therapeutic target in cardiometabolic diseases. Recent experimental studies have highlighted the role of targeted molecular interventions in regulating protein degradation pathways and inflammatory signaling cascades, thereby influencing vascular homeostasis. Although these approaches remain largely in the preclinical stage, they provide valuable insight into the complex interaction between inflammation, oxidative stress, and vascular dysfunction.29
Furthermore, the role of gut microbiota and related metabolic pathways has gained increasing attention in recent years. Alterations in gut microbial composition may contribute to systemic inflammation, oxidative stress, and endothelial dysfunction, all of which are implicated in hypertension and abnormal circadian blood pressure patterns. While the direct clinical implications of these findings remain to be fully elucidated, they underscore the multifactorial nature of cardiometabolic disease and highlight potential avenues for future therapeutic strategies.29
Preclinical studies have shown that prolonged inflammatory stimulation can dysregulate circadian clock gene pathways operating in vascular smooth muscle and endothelial cellular compartments. Suppression of core clock genes such as BMAL1 and PER2 under inflammatory conditions leads to attenuation of physiological diurnal oscillations in vascular contractility and endothelial responsiveness.30 This molecular circadian disruption provides a mechanistic explanation for the persistent nocturnal BP elevation observed in non-dipper patients.5 From this perspective, AISI may not only reflect systemic inflammation but also serve as a surrogate marker of inflammation-driven circadian clock dysregulation at the vascular cellular level.
Immune–metabolic crosstalk also plays a central role in non-dipper hypertension among diabetic patients.31 Insulin resistance induces a pro-inflammatory shift in adipose tissue macrophages toward an M1 phenotype, leading to sustained secretion of pro-HT adipokines and inflammatory mediators. These mediators interfere with insulin-mediated vasodilation and perpetuate nocturnal sympathetic activation.32 Lymphopenia, which is embedded within the AISI formula, may further indicate impaired immunoregulatory balance in this metabolic–inflammatory axis.33 Accordingly, elevated AISI values in non-dipper diabetic HT patients likely mirror the convergence of immune dysregulation, metabolic stress, and neurohumoral activation.17
From an epidemiological perspective, non-dipper hypertension has consistently been associated with increased risks of stroke, heart failure, chronic kidney disease progression, and all-cause mortality.34 However, identifying non-dipper patients in routine clinical practice remains challenging because of limited accessibility of ABPM. In this regard, AISI offers a pragmatic, low-cost alternative for preliminary risk stratification. Patients with markedly elevated AISI values may be prioritized for ambulatory BP assessment, thereby optimizing healthcare resources while improving early detection of high-risk circadian BP phenotypes.
Although NLR, PLR, SII, and SIRI were all significantly associated with non-dipper status in our cohort, their predictive performance remained inferior to that of AISI. This finding underscores the concept that composite indices integrating multiple inflammatory cell lines provide a more comprehensive representation of systemic inflammation than single- or dual-ratio markers. Given the distinct yet complementary biological roles of neutrophils, monocytes, platelets, and lymphocytes in vascular inflammation, the superiority of AISI appears both statistically and pathophysiologically coherent.
Our results also carry important therapeutic implications. Chronotherapy studies have demonstrated that nighttime administration of anti-HT medications improves dipping status and reduces cardiovascular risk.35 Incorporating AISI into clinical decision-making algorithms may facilitate individualized chronotherapeutic strategies by identifying patients most likely to benefit from targeted nocturnal BP modulation. Moreover, anti-inflammatory strategies, including lifestyle modification, weight reduction, optimization of glycemic control, and potentially novel immunomodulatory therapies, may represent adjunctive approaches for restoring normal circadian BP rhythm in patients with elevated AISI.
Ateş et al recently demonstrated that pan-immune-inflammation value (PIV) was independently associated with non-dipper blood pressure pattern in newly diagnosed hypertensive patients.36 However, unlike their study, which focused on a general hypertensive population, our investigation specifically evaluated hypertensive individuals with concomitant type 2 diabetes mellitus — a population characterized by amplified inflammatory burden and autonomic dysregulation. Furthermore, we comparatively assessed AISI alongside NLR, PLR, SII, and SIRI, demonstrating superior discriminative performance of AISI. These findings extend previous observations by highlighting that an integrated inflammatory index may have greater clinical relevance in high-risk cardiometabolic phenotypes.
The findings of this research should be interpreted in light of several important limitations. The observational and cross-sectional design precludes causal inference between AISI and non-dipper BP pattern. The exclusive inclusion of hypertensive patients with type 2 diabetes may reduce the external validity of the results for hypertensive populations lacking diabetic comorbidity. Inflammatory indices were measured at a single time point, precluding evaluation of longitudinal changes in AISI. Although comprehensive multivariate adjustments were performed, residual confounding cannot be entirely excluded. Finally, long-term cardiovascular outcomes were not assessed, limiting prognostic interpretation. Additionally, no formal sample size calculation was performed due to the retrospective design of the study, which may limit the statistical power of the findings.
Additional prospective investigations incorporating longitudinal assessment are necessary to better understand the evolving interplay between systemic inflammation and circadian blood pressure dysregulation. Serial AISI measurements may help identify transitions between dipper and non-dipper phenotypes and better define inflammatory trajectories over time. Integrating AISI with measures of arterial stiffness, sympathetic activity, endothelial function, and circadian gene expression may further refine mechanistic understanding and risk stratification. Additionally, randomized clinical trials evaluating AISI-guided chronotherapy and anti-inflammatory interventions could provide decisive evidence for its translational clinical utility.
Conclusion
Elevated AISI levels were independently associated with non-dipper blood pressure pattern in hypertensive patients with type 2 diabetes mellitus. Among the evaluated inflammatory indices, AISI demonstrated superior discriminative performance, highlighting its potential clinical value as an integrative biomarker of circadian blood pressure dysregulation.
However, the findings of this study should be interpreted in light of certain limitations, including its retrospective design and the lack of longitudinal outcome data. Future prospective studies with larger cohorts are warranted to validate these findings and to further explore the potential role of AISI in risk stratification and personalized management of hypertensive patients with diabetes. Therefore, these findings should be considered preliminary and require further validation in large-scale prospective studies.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Author Contributions
Alp Yıldırım: Conceptualization, Methodology, Data curation, Formal analysis, Writing – original draft.
Alperen Taş: Methodology, Formal analysis, Validation, Writing – review & editing, Supervision.
Müzeyyen Gizem Parmak: Data curation, Investigation, Resources, Writing – review & editing, Validation Muhammet.
Salih Ateş: Conceptualization, Supervision, Project administration, Writing – review & editing.
Erdoğan Sökmen: Investigation, Resources, Data curation, Supervision, Writing – review & editing, Methodology.
All authors made substantial contributions to the conception and design of the study, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Funding
No funding is available.
Disclosure
The authors report no conflicts of interest in this article.
References
1. Zhou B, Perel P, Mensah GA, Ezzati M. Global epidemiology, health burden and effective interventions for elevated blood pressure and hypertension. Nat Rev Cardiol. 2021;18(11):785–14. doi:10.1038/s41569-021-00559-8
2. McEvoy JW, McCarthy CP, Bruno RM, et al. 2024 ESC Guidelines for the management of elevated blood pressure and hypertension. Eur Heart J. 2024;45(38):3912–4018. doi:10.1093/eurheartj/ehae178
3. Gavriilaki M, Anyfanti P, Nikolaidou B, et al. Nighttime dipping status and risk of cardiovascular events in patients with untreated hypertension: a systematic review and meta-analysis. J Clin Hypertens. 2020;22(11):1951–1959. doi:10.1111/jch.14039
4. Huart J, Persu A, Lengelé JP, Krzesinski JM, Jouret F, Stergiou GS. Pathophysiology of the nondipping blood pressure pattern. Hypertension. 2023;80(4):719–729. doi:10.1161/hypertensionaha.122.19996
5. Faraci FM, Scheer F. Hypertension: causes and consequences of circadian rhythms in blood pressure. Circ Res. 2024;134(6):810–832. doi:10.1161/circresaha.124.323515
6. Manea V, Leucuţa DC, Pop C, Popescu MI. The predictive risk factors associated with non-dipper profile in patients with type 2 diabetes and hypertension. Med Pharm Rep. 2024;97(3):270–279. doi:10.15386/mpr-2749
7. Weinberg Sibony R, Segev O, Dor S, Raz I. Overview of oxidative stress and inflammation in diabetes. J Diabetes. 2024;16(10):e70014. doi:10.1111/1753-0407.70014
8. Sakthivel V, Dharshan SS, Namasivayam SKR, Arockiaraj J. Advances in 3D Organoids and organ-on-a-chip systems for biomedical research. J Biomed Mater Res A. 2026;114(1):e70028. doi:10.1002/jbma.70028
9. Bhat T, Teli S, Rijal J, et al. Neutrophil to lymphocyte ratio and cardiovascular diseases: a review. Expert Rev Cardiovascul Ther. 2013;11(1):55–59.
10. Pruc M, Peacock FW, Rafique Z, et al. The prognostic role of platelet-to-lymphocyte ratio in acute coronary syndromes: a systematic review and meta-analysis. J Clin Med. 2023;12(21):6903.
11. Yang Y, Tu R, Zhu L, et al. Association between systemic immune-inflammation index and 10-year risk of cardiovascular disease in the United States (NHANES 1999–2018). Exp Biol Med. 2025;250:10704.
12. Xia Y, Xia C, Wu L, Li Z, Li H, Zhang J. Systemic Immune Inflammation Index (SII), System Inflammation Response Index (SIRI) and risk of all-cause mortality and cardiovascular mortality: a 20-year follow-up cohort study of 42,875 US adults. J Clin Med. 2023;12(3). doi:10.3390/jcm12031128
13. Ghasemi S, Mortezagholi B, Movahed E, et al. Systematic review and meta-analysis of the association of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio with periodontitis. Eur J Med Res. 2024;29(1):581.
14. Jiang Y, Luo B, Lu W, et al. Association between the aggregate index of systemic inflammation and clinical outcomes in patients with acute myocardial infarction: a Retrospective Study. J Inflamm Res. 2024;17:7057–7067. doi:10.2147/jir.S481515
15. Wang R, Chen R, Tao W, Cheng X. Nonlinear associations between the aggregate index of systemic inflammation and cardiovascular disease in adults: evidence from NHANES 2011-2020. BMC Public Health. 2025;25(1):3031. doi:10.1186/s12889-025-24320-9
16. Koike T, Imamura T, Tomoda F, et al. Factors associating with non-dipping pattern of nocturnal blood pressure in patients with essential hypertension. J Clin Med. 2023;12(2). doi:10.3390/jcm12020570
17. Xiu J, Lin X, Chen Q, et al. The aggregate index of systemic inflammation (AISI): a novel predictor for hypertension. Front Cardiovasc Med. 2023;10:1163900. doi:10.3389/fcvm.2023.1163900
18. Petramala L, Circosta F, Cremonesi L, et al. Neutrophil-lymphocyte ratio and subclinical atherosclerosis in essential hypertensive patients. Front Cardiovasc Med. 2025;12:1579930. doi:10.3389/fcvm.2025.1579930
19. Drugescu A, Roca M, Zota IM, et al. Relationships between easily available biomarkers and non-dipper blood pressure pattern in patients with stable coronary artery disease. Life. 2023;13(3). doi:10.3390/life13030640
20. Çırakoğlu ÖF, Yılmaz AS. Systemic immune-inflammation index is associated with increased carotid intima-media thickness in hypertensive patients. Clin Exp Hypertens. 2021;43(6):565–571. doi:10.1080/10641963.2021.1916944
21. Kaplangoray M, Toprak K, Caglayan C, et al. Could the systemic inflammatory response index be a marker for the non-dipper pattern in newly diagnosed hypertensive patients? Cardiovasc Toxicol. 2025;25(4):559–569. doi:10.1007/s12012-025-09977-3
22. Forbes JM, Cooper ME. Mechanisms of diabetic complications. Physiol Rev. 2013;93(1):137–188. doi:10.1152/physrev.00045.2011
23. Jia G, Sowers JR. Hypertension in diabetes: an update of basic mechanisms and clinical disease. Hypertension. 2021;78(5):1197–1205.
24. Libby P. The changing landscape of atherosclerosis. Nature. 2021;592(7855):524–533. doi:10.1038/s41586-021-03392-8
25. Harrison DG, Guzik TJ, Lob HE, et al. Inflammation, immunity, and hypertension. Hypertension. 2011;57(2):132–140. doi:10.1161/hypertensionaha.110.163576
26. Crowley SD, Rudemiller NP. Immunologic effects of the renin-angiotensin system. J Am Soc Nephrol. 2017;28(5):1350–1361. doi:10.1681/asn.2016101066
27. Tuttle KR, Bakris GL, Bilous RW, et al. Diabetic kidney disease: a report from an ADA Consensus Conference. Diabetes Care. 2014;37(10):2864–2883. doi:10.2337/dc14-1296
28. Montezano AC, Touyz RM. Oxidative stress, Noxs, and hypertension: experimental evidence and clinical controversies. Ann Med. 2012;44(1):S2–16. doi:10.3109/07853890.2011.653393
29. Mohammed V, Haridevamuthu B, Kumaradoss KM, Namasivayam SKR, Arockiaraj J. Marine-Derived molecular glue degraders: a new frontier in targeted protein degradation for treatment of multi-factorial diseases. Biotechnol Appl Biochem. 2026;73(2):871–895. doi:10.1002/bab.70055
30. Anea CB, Zhang M, Stepp DW, et al. Vascular disease in mice with a dysfunctional circadian clock. Circulation. 2009;119(11):1510–1517. doi:10.1161/circulationaha.108.827477
31. DeFronzo RA, Ferrannini E, Groop L, et al. Type 2 diabetes mellitus. Nat Rev Dis Primers. 2015;1:15019. doi:10.1038/nrdp.2015.19
32. Lumeng CN, Saltiel AR. Inflammatory links between obesity and metabolic disease. J Clin Invest. 2011;121(6):2111–2117. doi:10.1172/jci57132
33. Hotamisligil GS. Inflammation, metaflammation and immunometabolic disorders. Nature. 2017;542(7640):177–185. doi:10.1038/nature21363
34. Fagard RH, Thijs L, Staessen JA, Clement DL, De Buyzere ML, De Bacquer DA. Night-day blood pressure ratio and dipping pattern as predictors of death and cardiovascular events in hypertension. J Hum Hypertens. 2009;23(10):645–653. doi:10.1038/jhh.2009.9
35. Hermida RC, Crespo JJ, Domínguez-Sardiña M, et al. Bedtime hypertension treatment improves cardiovascular risk reduction: the Hygia Chronotherapy Trial. Eur Heart J. 2020;41(48):4565–4576. doi:10.1093/eurheartj/ehz754
36. Ateş MS, Yıldırım A, Sökmen E. Association between pan-immune-inflammation value and dipper/non-dipper status in newly diagnosed hypertensive patients. J Inflamm Res. 2025;6217–6228.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Type 2 Diabetes Mellitus and Chronic Obstructive Pulmonary Disease – from Pathophysiology to Effective Management Overview
Prisacaru V, Covantsev S, Ceasovschih A, Sivapalan P, Tural S, Corlateanu A, Deleanu OC
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:609302
Published Date: 3 June 2026