Back to Journals » Journal of Pain Research » Volume 18
Treatment Modalities for Aromatase Inhibitor-Associated Musculoskeletal Syndrome (AIMSS): A Scoping Review of Prospective Treatment Studies
Authors Bobo JA, Lubrano B, Rosario-Concepcion R, Cuartas-Abril A, Advani P, Chumsri S ![]() , Bruce BK
, Bruce BK
Received 24 August 2024
Accepted for publication 12 March 2025
Published 7 April 2025 Volume 2025:18 Pages 1853—1889
DOI https://doi.org/10.2147/JPR.S492891
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Justin Andrew Bobo,1 Barbara Lubrano,2 Raul Rosario-Concepcion,3 Alejandra Cuartas-Abril,2 Pooja Advani,4 Saranya Chumsri,4,5 Barbara K Bruce2
1Department of Molecular Pharmacology & Experimental Therapeutics, Mayo Clinic, Rochester, MN, USA; 2Department of Psychiatry & Psychology, Mayo Clinic, Jacksonville, FL, USA; 3Miami Neuroscience Institute, Baptist Health, Miami, FL, USA; 4Department of Medical Oncology, Mayo Clinic, Jacksonville, FL, USA; 5Department of Medicine, Mayo Clinic, Jacksonville, FL, USA
Correspondence: Barbara K Bruce, Department of Psychiatry and Psychology, Mayo Clinic, Florida, 4315 Pablo Oaks Court, Jacksonville, FL, 32224, USA, Tel +1 (904) 953-7286, Fax +1 (904) 953-0461, Email [email protected]
Abstract: Aromatase inhibitors (AI’s) are effective adjuvant treatments for postmenopausal patients with hormone receptor-positive breast cancer. However, AIs are often associated with diffuse joint and muscle pain, referred to as aromatase inhibitor-associated musculoskeletal syndrome (AIMSS), the symptoms of which are associated with negative impacts and reduced adherence to AI therapy. As more interventions for AIMSS continue to be investigated, a scoping review is needed to survey and summarize the types of interventions and outcomes assessed in studies conducted to date, which may help identify areas needing attention or additional focus in future research. Online databases were searched (from inception to January 8, 2025) to identify 74 reports from prospective studies of interventions for AIMSS pain, stiffness, or interference with functioning. Such interventions were classified as pharmacological (14 reports), complementary/alternative (43 reports), or rehabilitative (17 reports). Included papers required the presence of AIMSS symptoms at enrollment. Several interventions were deemed promising for reducing AIMSS symptoms based on positive results from individual reports, including duloxetine (3 reports from 2 studies), vitamin B12 (2 reports), vitamin D (2 reports), calcitonin (1 report), prednisolone (1 report), glucosamine and chondroitin (1 report), various mind-body (14 reports from 12 studies) and traditional medicine interventions (3 reports), and switching to another AI (1 report). Many positive findings were from uncontrolled studies or were from single studies that await replication in independent cohorts, and no studies focused on structured psychological interventions. The durations for all reviewed studies were brief relative to the expected 5– 10-year course of AI therapy. Intervention effects on a wide range of outcomes were studied, including pain or stiffness (70 reports), functioning/disability (34 reports), quality of life (37 reports), mental health symptoms (25 reports), pain self-efficacy (4 reports), and AI persistence (3 reports). However, intervention effects on other important endpoints such as cancer recurrence, survival, healthcare utilization/costs, and caregiver experiences are unclear. The knowledge gaps and limitations identified in this scoping review constitute areas in urgent need of further research and attention.
Keywords: aromatase inhibitor-associated musculoskeletal syndrome, AIMSS, aromatase inhibitors, breast cancer, pain management, musculoskeletal symptoms
Introduction
Breast cancer is the most common type of cancer among postmenopausal women, with approximately 1.4 million diagnosed cases worldwide in 2018, accounting for over 490,000 deaths.1 The early detection of breast cancer increases the odds of a curative outcome with surgery.2,3 Following surgery, adjuvant therapy is often required to decrease the risk of breast cancer recurrence and increase long-term survival.4 For post-surgical patients with early-stage hormone-sensitive breast cancer, aromatase inhibitors (AIs) are effective for reducing the risk of cancer recurrence and early mortality and are considered first-line adjuvant treatments.5,6
Unfortunately, about 46% of AI-treated patients report diffuse joint and muscle pain after starting treatment,7 referred to as AI-associated musculoskeletal syndrome (AIMSS). AIMSS-related pain can be quite severe, so much so that it is a leading risk factor for premature discontinuation of adjuvant AI treatment.8 An estimated 32–50% of patients are only partially adherent to AI treatment and 30% discontinue AIs altogether after 12 months due to pain from AIMSS.9 The importance of this point rests on the expectation that adjuvant treatment with AIs will last 5–10 years, depending on the patient’s risk factors for cancer recurrence. Furthermore, although estimates may vary, the preventive effects of AIs may confer an average societal cost savings of over $17 million (in 2011 USD),10 suggesting the possibility of very high economic impacts of early AI discontinuation and consequent exposure to increased risk of breast cancer relapse and recurrence. The effective management of AIMSS-associated pain may thus increase the odds of persistence on AI therapy, preserving its preventive effects on cancer recurrence and its survival-promoting benefits while generating associated economic savings.
The pathophysiology for AIMSS is unknown, which has limited efforts at developing therapeutic interventions. Currently, there is no established treatment for AIMSS. However, several interventions have been tested that map to at least four major etiological hypotheses for AIMSS: (a) estrogen depletion;9,11,12 (b) activation of inflammatory and/or autoimmune pathways;13,14 (c) alteration of vitamin D activity;15–17 and (d) centrally mediated pain.18
Previous reviews have focused on specific interventions for AIMSS such as acupuncture and physical activity.19–22 The most recent systematic review of the broader spectrum of therapeutics for AIMSS focused on systemic interventions, only two of which were included for meta-analysis due to methodologic heterogeneity and unavailable data.23 The level of evidence was rated as “very uncertain”, thus limiting the ability to provide evidence-based treatment recommendations. Not surprisingly, and despite published guidelines, the management of AIMSS remains driven primarily by expert opinion or practice experience.24
This situation may be expected to change with the accumulation of high-quality evidence. As more interventions continue to be investigated, an updated review is needed to complement prior research syntheses by surveying and summarizing the types of evidence and the scope of interventions and outcomes being studied for (or applied to) AIMSS, including from unpublished (grey literature) sources. There is also an ongoing need to highlight important knowledge gaps as a potential guide for future research. The following research questions were formulated as they pertain to published and unpublished prospective intervention research for AIMSS: (1) What types of treatments have been studied?; (2) What types of outcomes have been focused on?; and (3) What interventions and outcomes need to be researched?
Methods
Inclusion and Exclusion Criteria
A literature search was conducted using PubMed, OVID Medline, EMBASE, SCOPUS, PSYCInfo, and CINAHL (from inception to January 8, 2025) to identify randomized trials, nonrandomized trials, and single-arm prospective (pre/post) studies that included subjects with existing AIMSS and were written in English (see Supplementary Table 1). ClinicalTrials.gov and CENTRAL registers were also searched to identify grey literature citations. We kept the scope of included studies as broad as possible while restricting the search to prospective intervention studies, given the objectives of this scoping review. Research letters, prospective case series, and conference abstracts reporting prospective findings were included if they specified, at minimum, inclusion criteria, intervention(s), outcome(s), and follow-up duration. Conference abstracts linked to published papers were replaced by the full-length research reports when appropriate.
We excluded papers that did not specify the use of AIs for breast cancer treatment. Given our focus on treatment studies, we also excluded reports of interventions to prevent the onset of AIMSS. We also excluded single case reports, case series numbering fewer than 10 subjects, case series with no statistical analyses, systematic or other reviews, and reports of study protocols.
Population/Participants
This review focused on studies of women with breast cancer receiving any AI treatment who had AIMSS symptoms present at baseline or at the beginning of follow-up. We did not restrict potentially eligible studies to a particular stage of breast cancer. However, we expected that study samples would consist primarily of postmenopausal women with stage I–III hormone receptor-positive (HR[+]) breast cancer.
Interventions
All forms of pain symptom management were considered. Interventions in this report were grouped into three broad categories (pharmacological, complementary/alternative, and rehabilitative), with additional sub-categories as defined in Table 1. Pharmacological interventions included endocrine/hormonal, analgesic/anti-inflammatory, and neuromodulatory interventions, as well as therapeutic switching (from one AI to another). Neuromodulatory medications included centrally active medications (eg, antidepressants, anticonvulsants, gabapentinoids, cannabinoids, etc) and peripherally applied agents (eg, capsaicin, botulinum toxin, etc)., consistent with previous research.25. Complementary/alternative interventions included nutritional or supplement-based, physiological or psychophysiological, and traditional medicine therapies.26 Rehabilitative interventions were classified into supervised sport or exercise, physiotherapy (including physical, occupational, and recreational therapies), and psychosocial or educational interventions.
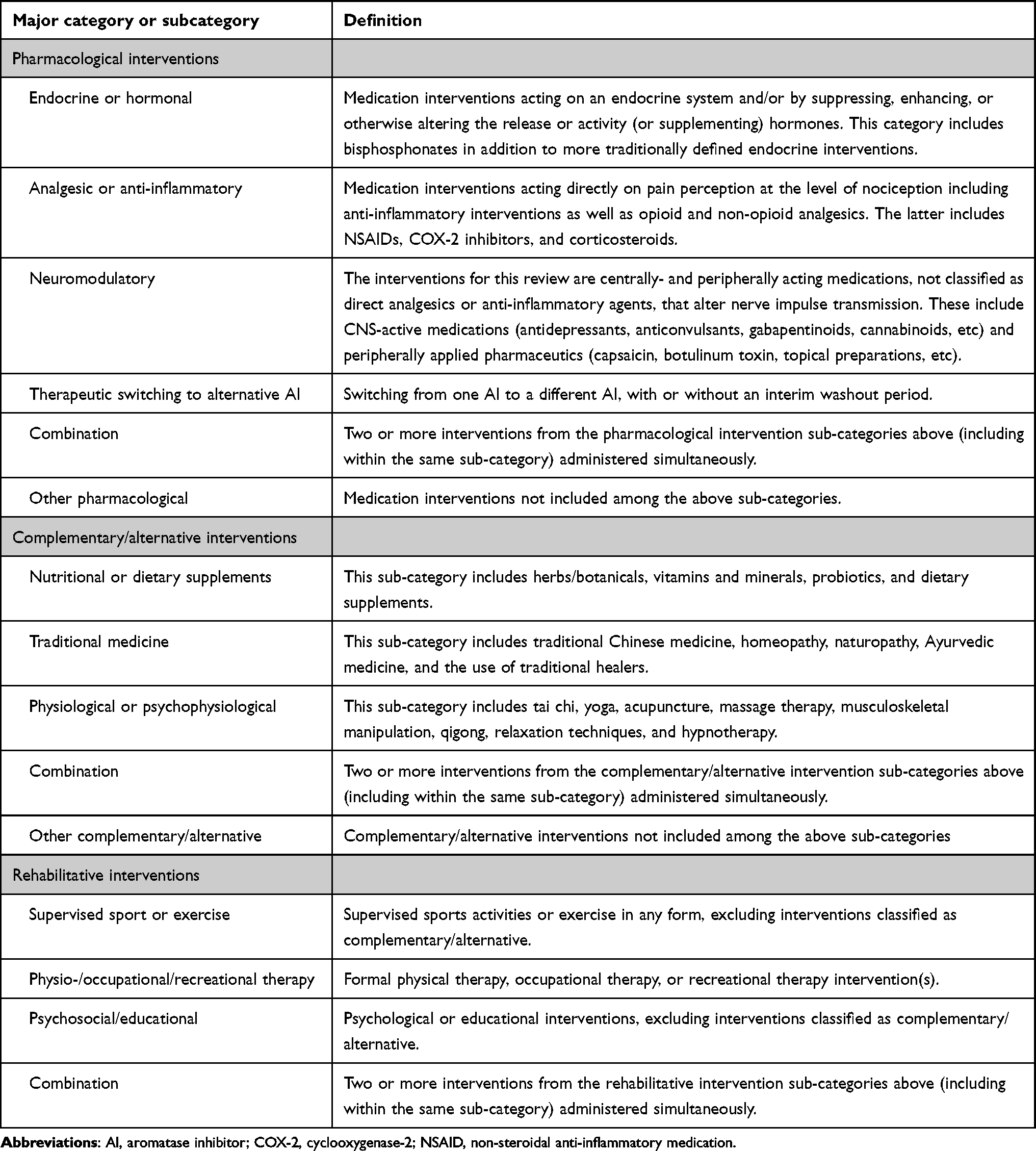 |
Table 1 Categories of Interventions for AIMSS |
Outcomes
We were interested in exploring the scope of outcomes and assessments across the qualifying intervention studies. Given our primary focus on AIMSS, we were interested in assessing outcome domains (eg, pain, stiffness, interference with functioning, etc) as well as specific outcome measures including objective assessments and subjective ratings. For this report, studies that reported pain, stiffness, and functioning outcomes as a secondary endpoint were still included. Although all reported outcomes from the individual reports were tracked, additional outcomes of particular interest included quality of life, mental health symptoms, additional symptoms (eg, fatigue and menopausal symptoms), sexual functioning, pain self-efficacy, persistence with AI therapy, breast cancer recurrence/survival, healthcare utilization/costs, caregiver experiences, and reporting of adverse events related to the intervention(s).
Report Screening and Data Extraction
Two investigators (JAB, BKB) screened titles and abstracts to exclude irrelevant reports. Three investigators (JAB, BL, BKB) then worked in pairs to complete full-text reviews to exclude reports that did not meet inclusion criteria and extract information on qualifying papers. All studies were classified according to report type (research report, conference abstract), study design (randomized parallel-group trial, randomized cross-over trial, nonrandomized study with at least 2 arms, pre/post study, other design, or design unclear), and intervention type. Additional data elements included participant characteristics (age, breast cancer stage), inclusion and exclusion criteria, AIMSS definition, intervention details (including intervention name, dose/intensity of exposure, and duration of exposure), control conditions, co-interventions (if applicable), study endpoints, study duration, reporting of adverse events, and main findings.27
Synthesis of Results
We grouped studies by intervention type (Table 1). Within each intervention type, we summarized the specific intervention subtypes, specific interventions studied, outcomes assessed, and main results. These characteristics were summarized in graphical form, whenever possible. Other design features or outcome characteristics of special note were also recorded if such elements added important context to main objectives of this report. Examples included, but were not limited to, specific adaptations to established treatments and characteristics of investigator-developed assessment measures.
Results
Search Results
The initial search retrieved 2481 records across 6 databases and an additional 517 records from trial registries (Figure 1). After removing duplicates and non-qualifying studies based on title and abstract screening, 145 records were initially sought for retrieval. Two studies were added after bibliographic review. After applying inclusion and exclusion criteria at full-text review, a total of 74 reports met inclusion criteria, 59 of which were published as journal articles,28–85 with 15 reports available as published abstracts (Figure 2a).52,86–99
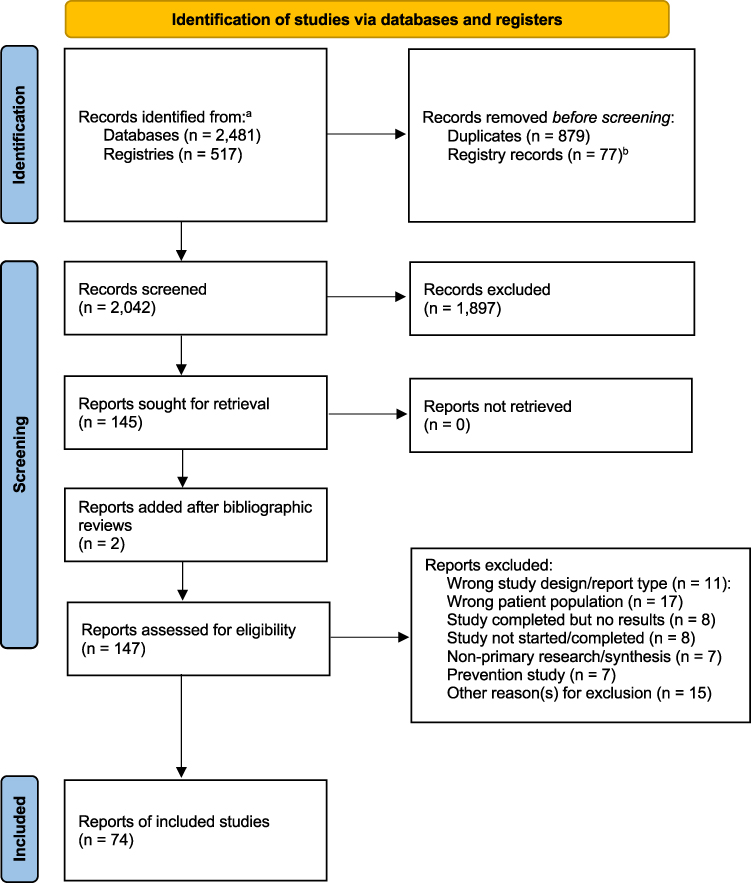 |
Figure 1 PRISMA flow diagram. aThe search date for all databases and clinical trial registries was 08 January 2025. A total of 2998 records were identified (see Supplementary Table 1) – PubMed, n = 292; Ovid MEDLINE, n = 172; SCOPUS, n = 1387; EMBASE, n = 549; CINAHL, n = 71, PsycINFO, n = 10, CENTRAL, n = 408; ClinicalTrials.gov, n = 63). bWithin clinical trials registries, a total of 77 records were removed. Thirty-six records were removed for studies that were recruiting or not yet recruiting (n = 27), withdrawn (n = 15), or in another or unknown status with no results available (n = 4). An additional 42 records of studies listed as complete but with no results available were removed. PRISMA figure adapted from Liberati A, Altman D, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Journal of clinical epidemiology. 2009;62(10). Creative Commons.100. |
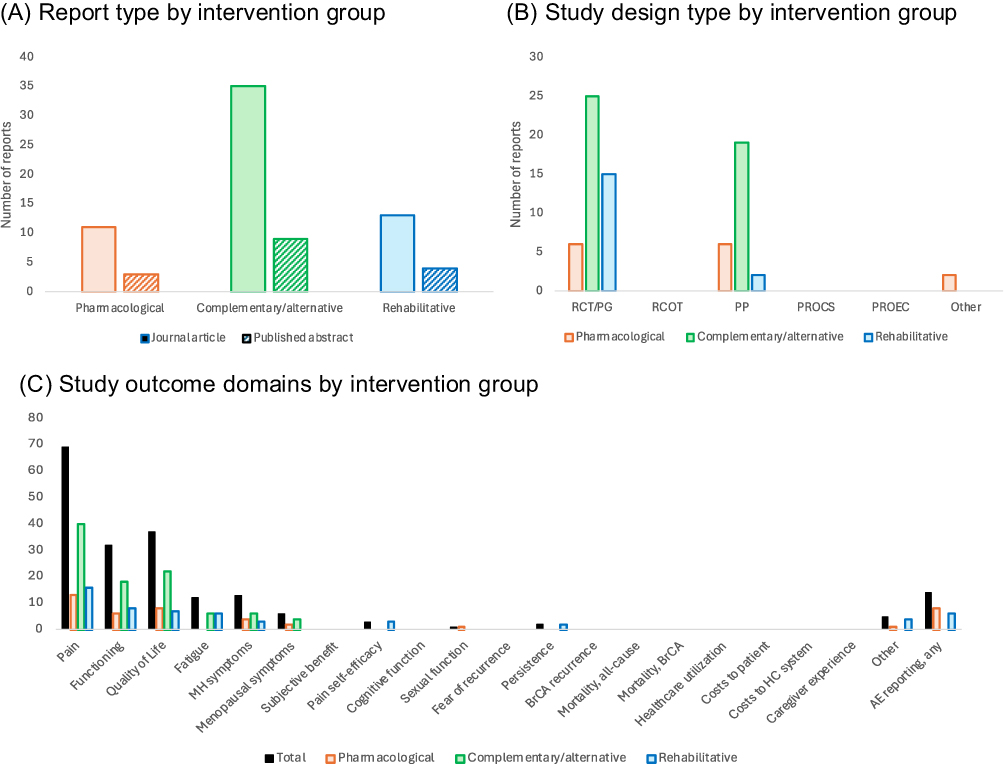 |
Figure 2 Visual summary of reviewed reports. (A) summarizes the total number of reports by report type (journal article [solid bars], published abstract [striped bars]) within subgroups defined by intervention (pharmacological, complementary/alternative, and rehabilitative). (B) summarizes the number of reports according to study design considering the type of intervention (pharmacological [pink bars], complementary/alternative [green bars], and rehabilitative [blue bars]). (C) summarizes the number of reports that include specific outcome domains, total (black bars) and by intervention type (pharmacological [pink bars], complementary/alternative [green bars], and rehabilitative [blue bars]). Abbreviations: AE, adverse event; BrCA, breast cancer; PP, pre/post study design; PROCS, prospective case series; PROEC, prospective study with concurrent/external control group; RCOT, randomized cross-over trial; RCT/PG, randomized controlled trial/parallel-group. |
Description of Included Studies
Study design features, study location, key clinical characteristics of enrollees, and main results of the 74 reviewed reports are presented in Tables 2–4, while the inclusion/exclusion criteria and definitions of AIMSS for each report are presented in Supplementary Tables 1–3. Six reports were included because they extended the results of other reports reviewed herein or presented additional information on outcomes of interest.30,32,33,78,82 Approximately half of the reviewed studies were conducted in the US (n = 40 reports), while 11 were conducted in East Asia, 10 in Europe (including the United Kingdom), 3 in Australia, 3 in South America, and the remaining 4 in Turkey, Egypt, and India (primary site could not be identified in 3 reports). Fifteen of the reviewed reports were published only as conference abstracts. The number of participants across studies ranged from 10 to 256 and the mean or median ages of participants ranged from 44.0 to 69.9 years. In one study, 26 out of 29 participants (89.7%) were reported as being <45 years of age.74 Follow-up durations ranged from 4 weeks to 12 months.
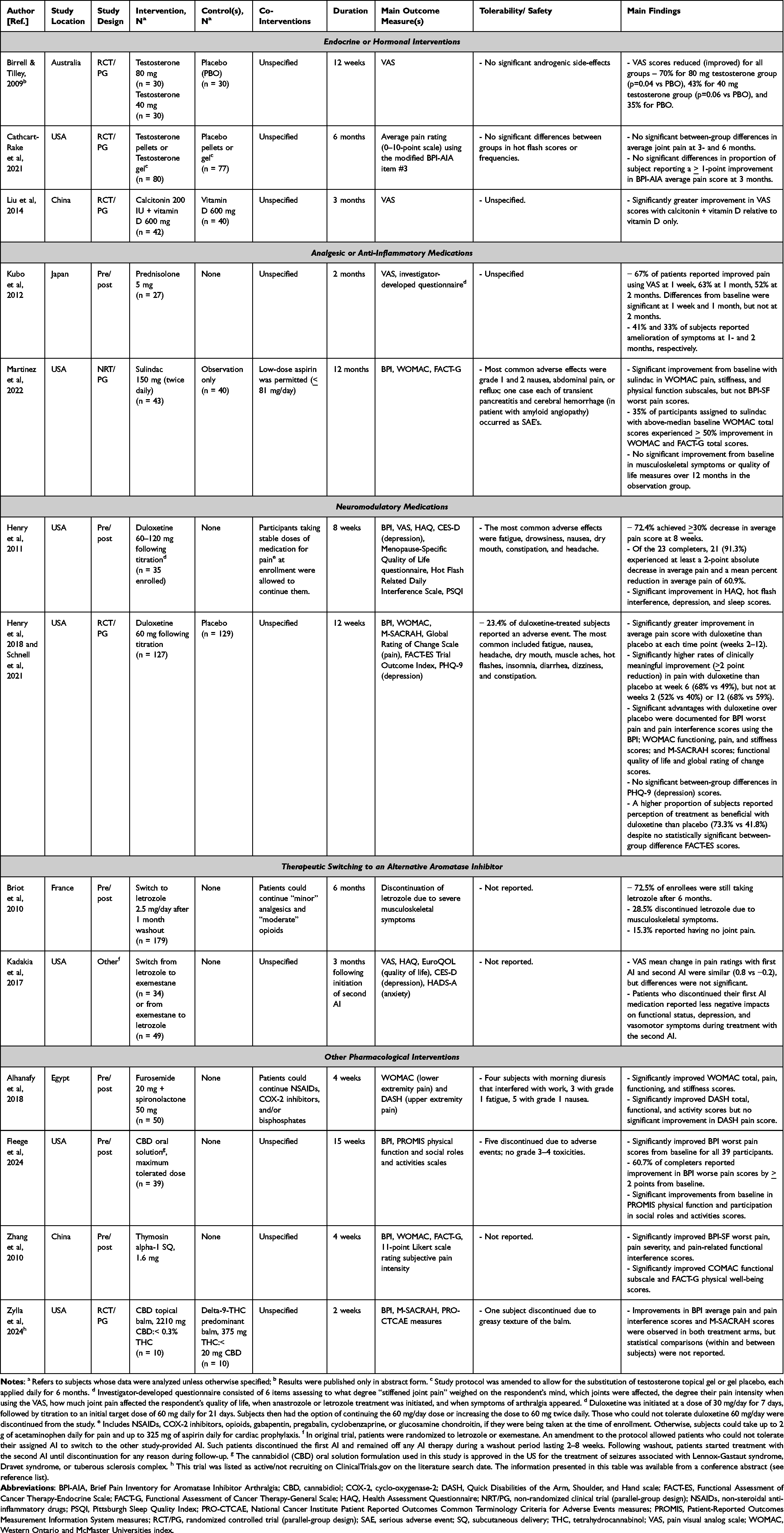 |
Table 2 Prospective Studies of Pharmacological Interventions for AIMSS |
 |
Table 3 Prospective Studies of Complementary/Alternative Interventions for AIMSS |
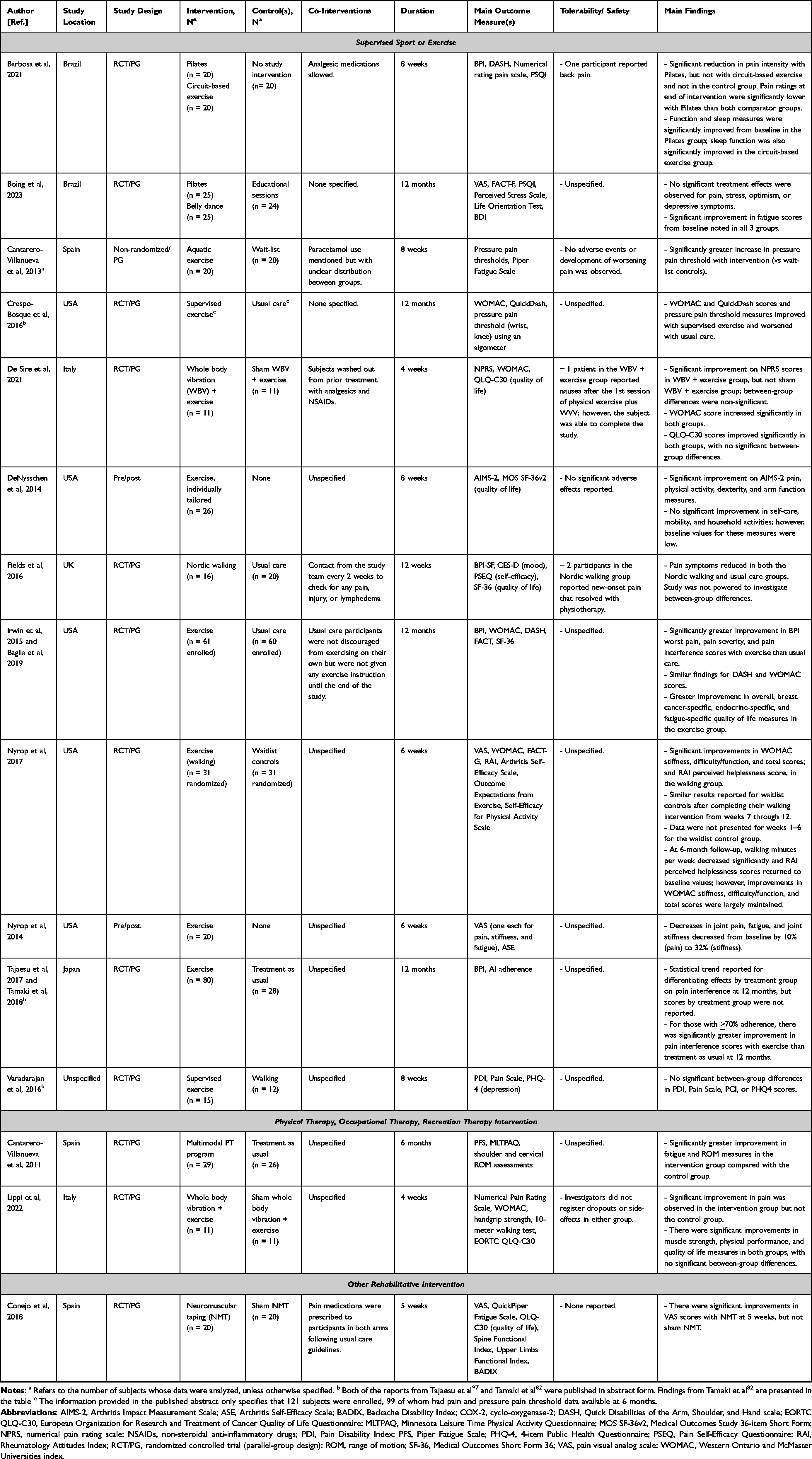 |
Table 4 Prospective Studies of Rehabilitative Interventions for AIMSS |
Most studies enrolled postmenopausal women with Stage I–III, HR[+] breast cancer and required treatment with AIs for at least one month, often longer, as explicit requirements for study enrollment, with either self-reported or clinician-diagnosed joint symptoms that began after starting AI therapy or worsened after AI initiation. Six studies explicitly allowed enrollment of postmenopausal participants with Stage 0 disease.32,53,61,62,65,70 Fourteen studies included (or reported having included) patients with a history of prior taxane use. Metastatic breast cancer (Stage IV), receiving concurrent chemotherapy or radiation therapy, pre-existing arthralgias, recent trauma or surgery to the joints or extremities of interest, and contraindications to the interventions under investigation were common exclusion criteria.
Explicit definitions for AIMSS, including definitions used as inclusion criteria, were provided in most of the included reports (see Supplementary Tables 2–4), several of which required complaints of arthralgias during AI therapy and a pre-specified threshold of subjective pain intensity measured using pain rating scales or on a 10- or 11-point scale (33 reports). In other cases, the definitions of AIMSS required diagnosed or self-reported arthralgias associated with AI treatment (22 reports) or the presence of arthralgias or other joint symptoms in people taking AIs at enrollment (6 reports).
Most of the reviewed reports were from randomized, parallel-group studies that used mainly placebo or sham controls (43 reports). Twenty-six studies used a single-arm, pre/post study design. Two reports involving complementary/alternative treatments were from randomized cross-over studies45,95 and one pharmacological and one rehabilitative intervention study, each, used a non-randomized parallel-group design.39,71 As shown in Figure 2b, randomized trials were the predominant study design for reports on complementary/alternative and rehabilitative interventions, while a more even distribution between randomized trials and pre-post study designs was observed for pharmacological interventions. One study enrolled subjects who had discontinued anastrozole due to musculoskeletal symptoms and were willing to take letrozole as part of a prospective switch study.37 An amendment to the protocol for another study allowed patients to switch to an alternative AI if they could not tolerate their originally assigned AI,62 thus providing the opportunity to study the effects of a therapeutic switch.
Interventions for AIMSS
A summary of interventions for AIMSS is presented in Figure 3. Most reports focused on the effects of complementary/alternative medicine (CAM) approaches (n = 43), followed by rehabilitative (n = 17) and pharmacological interventions (n = 14). The clinical effects of a wide variety of individual treatments were studied within each of these broad categories. Physiological/psychophysiological interventions were the most common broad subtype of intervention studied (26 reports from 21 studies), while the most investigated single group of treatments was acupuncture, electroacupuncture, or acupressure (14 reports from 12 studies).
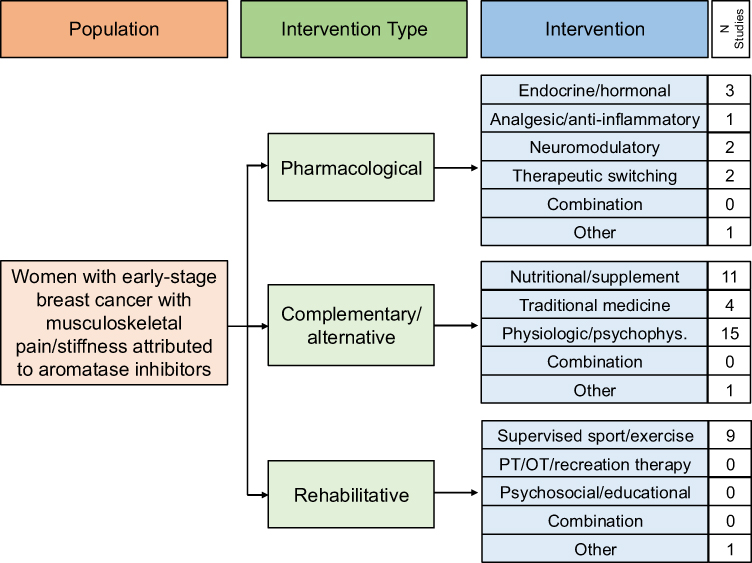 |
Figure 3 Number of reports by specific intervention. Abbreviations: OT, occupational therapy; psychophys., psychophysiologic intervention; PT, physical therapy. |
As shown in Tables 2–4, several treatments were associated with positive therapeutic effects on various measures of AIMSS symptom intensity, dysfunction owing to AIMSS symptoms, or quality of life measures. In many cases, positive results were from small, uncontrolled studies or single studies needing replication in independent cohorts. For example, multiple randomized trials of complementary/alternative treatments supported the effectiveness of acupuncture,45,46,58,59 electroacupuncture,68,69 and yoga.76,83 However, beneficial effects of tai chi and vitamin B12 supplementation were documented only in single-arm studies38,51,53,96 and positive findings for several nutritional/supplemental and traditional medicine interventions (eg, glucosamine and chondroitin, tart cherry extract, other individual dietary supplements, Bionic tiger bone powder, and blue citrus) came only from single reports.49,54,63,65,70,77,80,95
Among the pharmacological interventions, positive effects of calcitonin, prednisolone, furosemide + spironolactone, and sulindac on AIMSS symptoms were documented only in single reports (Table 2).28,64,66,71 Although two reports each suggested possible benefit from the use of cannabinoid-based formulations and from switching AIs,37,62,90,99 duloxetine was the only pharmacological intervention with replicated positive findings in a well-powered randomized trial.56
For rehabilitative interventions, several supervised exercise approaches were found to be helpful. Although multiple reports documented beneficial effects of various forms of exercise on AIMSS symptoms (Table 4), the specific techniques or regimens that were applied in the individual reports varied substantially, making it difficult to subdivide exercise interventions into smaller, more homogenous subgroups. For instance, there were 3 reports of the effects of walking for AIMSS symptoms, one of which involved a combination of supervised and independent Nordic walking,50 while the remaining two reports focused on low-intensity unsupervised or self-directed walking as main interventions.72,73 Other exercise interventions included multimodal regimens that combined resistance training with land-based aerobic exercise,30,47,60,89 whole-body vibration combined with exercise,48 Pilates combined with circuit-based training or dance,36 aquatic aerobic exercise,39 and unspecified directed exercise.98 In one randomized study, participants assigned to the exercise intervention (instead of usual care) could choose to participate in one of three physical activity regimens classified as low-intensity (120–150 minutes per week of walking or running), moderate-intensity (a daily regimen that was publicly broadcasted over the radio), or higher-intensity (climbing stairs).82 We were unable to locate reports from studies of structured individual or group-based psychotherapies or psychoeducational interventions for AIMSS. One report described the effects of a 4-week, physiotherapist-led progressive relaxation exercise intervention; however, the intervention, as described, did not focus specifically on psychological or behavioral reactions to pain.31
Outcomes Assessed
As shown in Figure 2c, the most frequently assessed outcomes across the reviewed reports were pain intensity (70 reports), followed by various measures of quality of life (37 reports) and functioning (34 reports). Relatively fewer reports highlighted adverse intervention effects, and very few studies focused on more downstream outcomes such as persistence on AI therapy. We were unable to locate any reports highlighting intervention effects on other cancer survivorship outcomes such as breast cancer recurrence, survival, fear of disease recurrence, service utilization, care costs, or caregiver experiences.
Most reports of intervention effects on pain outcomes incorporated multiple measures that assessed global pain intensity, pain levels in various body regions or joints, and/or interference with life activities and functioning due to pain symptoms. Pain sensitization (pressure pain thresholds) and pain self-efficacy (subjects’ levels of confidence in their ability to function adequately despite persisting pain) were assessed in two39,89 and four studies,43,50,72,73 respectively. The most frequently used individual pain rating scales were self-administered questionnaires such as the Brief Pain Inventory (BPI, including short-form versions and subscale measures of pain intensity and impact, 43 reports),101 the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC)102 pain scale (25 reports), the 30-item and short versions of the Disabilities of the Arm, Shoulder and Hand (DASH, QuickDASH)103,104 questionnaire (8 reports), modified versions of existing rating scales or investigator developed measures (4 reports), the modified (shortened) version of the Score for the Assessment and Quantification of Chronic Rheumatoid Affections of the Hands (M-SACRAH)105 scale (3 reports), various Patient-Reported Outcomes Measurement Information System (PROMIS)106 pain measures (3 reports), and the Australian/Canadian (AUSCAN)107 Osteoarthritis Hand Index (3 reports). Visual analog scales and similar ordinal measures were used to rate pain intensity and/or interference in 21 reports, while five reports included analgesic medication use or changes in the frequency of analgesic administration as outcome measures. Pain self-efficacy measures included the full or shortened versions of the Pain Self-Efficacy Questionnaire (PSEQ, 3 studies)108 and the Arthritis Self-Efficacy Scale (1 study).109
Functioning and quality of life measures also consisted mainly of self-administered questionnaires including the Functional Assessment of Cancer Therapy (FACT)110 subscales (23 reports), specific subdomains from pain rating scales that assessed perceived functional capacity and quality of life/wellbeing (14 reports), the Health Assessment Questionnaire (HAQ)111 Disability Index and Pain Scale (8 reports), versions of the 36-item Short Form Survey (SF-36)112 quality of life measures (4 reports), EuroQol Group quality of life (EuroQoL)113 measures (3 reports), and the Backache Disability Index (BADIX)114 and Minnesota Leisure Time Physical Activity Questionnaire (1 report each).115 Direct measures of physical functioning were assessed in 11 reports, including the Functional Sit and Reach Test116 and other standardized measures of flexibility, strength, and range of motion.
Intervention effects on mental health symptoms (including perceived levels of stress) and fatigue were assessed in 13 and 12 reports, respectively. Specific mental health outcomes in the reviewed reports were predominantly depressive and anxiety symptoms assessed using subject-reported scales. These scales included the Hospital Anxiety and Depression (HADS)117 depression and/or anxiety subscales (5 reports), the Public Health Questionnaire (PHQ) 9- and 4-item scales118,119 (5 reports), the Center for Epidemiologic Studies Depression Scale (CES-D, 4 reports),120 and the Profile of Mood States (POMS)121 scale (1 report). There were no formal or structured assessments for discrete mental health diagnoses, conditions, or comorbidities based on diagnostic criteria or other standardized definitions. In one report, subjective stress levels were assessed using the Perceived Stress Scale.122
Additional symptom measures in the reviewed reports included assessments of sleep quality (10 reports), the intensity and burden from menopausal symptoms (6 reports), and perceived sexual functioning (one report). The most used sleep measure was the Pittsburgh Sleep Quality Index (7 studies).123 Other sleep measures included the Insomnia Severity Index,124 subjective ordinal ratings, and unspecified measures (one study each). Menopausal symptoms were assessed using the Hot Flash-Related Daily Interference Scale (HFRDIS, 4 reports)125 and the National Surgical Adjuvant Breast and Bowel Project (NSABP) menopause symptom items, hot flash symptoms recorded in diaries, and the Menopause-Specific Quality of Life scale (2 reports each).126
Discussion
This scoping review summarized the existing evidence from prospective studies of the full spectrum of interventions for AIMSS in women with breast cancer. Reviewed interventions included pharmacological treatments with a variety of mechanisms and as diverse an array of complementary/alternative and rehabilitative therapies. Nearly 60% of included studies tested the effects of complementary/alternative interventions. The remaining studies were a more even split between traditional pharmacological interventions and rehabilitative therapies. Most reviewed studies were randomized trials, the majority of which used placebo or sham controls. Although operational definitions of AIMSS and pain or stiffness-related outcome measures had reasonable overlap across studies, other clinical and methodological characteristics such as inclusion and exclusion criteria (which were intervention-dependent, as expected), study designs, sample sizes, non-pain-related outcome measures, co-interventions, and completeness of adverse event reporting varied widely across studies. The evidence base does not yet point to clearly preferred interventions for AIMSS, nor does it provide a clear means of stratifying treatments or channeling them to specific types of patients. Intervention effects on other important endpoints are uncertain (ie, persistence on AIs) or untested (eg, breast cancer recurrence, survival, costs of care, and caregiver experiences).
Prior reviews of interventions for AIMSS have focused on effectiveness for pain symptoms and the quality of that evidence—and not necessarily on providing a comprehensive summary of the full spectrum of AIMSS interventions and outcomes assessed. For instance, a systematic review of 17 studies that investigated systemic therapies for preventing or treating AIMSS in women with early-stage breast cancer highlighted positive findings for duloxetine, testosterone, calcitonin, vitamin D, omega-3 fatty acids, Yi Shen Jian Gu granules, cat’s claw, pure emu oil, and BTBP for improving pain scores.23 The overall evidence for effective and safe systemic treatments for AIMSS was rated as “minimal”. An earlier systematic review of 38 studies also examined the clinical effects of pharmacological and non-pharmacological interventions for treating AIMSS in postmenopausal patients with early breast cancer,22 and called attention to the relatively sparse evidence base for nearly all interventions of interest and the limitations of conclusions that could be drawn from the available literature (through 2016) owing to small sample sizes, heterogeneity of interventions, low clarity in methodological details, and high risks of bias across several studies. The present scoping review also highlights promising treatment approaches across 74 reports published through January 8, 2025, and extends prior reviews by providing a current summary of the full spectrum of interventions and outcomes that have been systematically investigated for treating prevalent AIMSS symptoms.
Guidelines for managing AIMSS symptoms that were recently published by the American Society for Clinical Oncology recommended yoga, other types of exercise, duloxetine, acupuncture, and omega-3 fatty acids (especially for obese patients) as reasonable therapeutic options, along with holding AI treatment followed by re-initiation or therapeutic switch for treatment-resistant cases.24 However, there is still no standardized approach to treating AIMSS and improving AI persistence. The importance of this crucial knowledge gap is highlighted by the positive association between AIMSS pain/discomfort and premature discontinuation of adjuvant AI therapy,14 which may justify applying safe and potentially effective interventions, given the evidence in hand, even if the quality of that evidence is currently less than optimal. Partial adherence, which can limit the effectiveness of oral medications in patients with breast cancer,127 may also be foreseeably related to AIMSS symptoms although, to our knowledge, this has not been thoroughly investigated. Nevertheless, from this perspective, the relative sparsity of direct evidence for improving AI adherence or persistence for any of the reviewed interventions is surprising. Furthermore, as there appears to be no clinically significant difference in the efficacies of different AIs as adjuvant therapies in postmenopausal women with early breast cancer,128 the scarcity of switch studies and head-to-head studies of AIs powered to detect differences in AIMSS and other toxicity profiles is also surprising, calling attention to high-priority areas in need of systematic clinical investigation.
Although the term, AIMSS, would seem to imply the presence of a single syndrome, it is really a collection of diverse symptoms that have in common only their link to a single presumed cause. Indeed, the clinical features of AIMSS classically include joint pain and stiffness; however, additional defining symptoms can include diffuse pain, myalgias, bone pain, carpal tunnel syndrome, morning stiffness, and neuropathic-like pain symptoms.129–131 Beyond localization and distribution, the severity of pain and stiffness can vary widely from patient to patient.129 The proposed pathophysiological or pharmacological mechanisms by which AIs may lead to AIMSS symptoms are also heterogeneous and no unifying etiology has been discovered. As such, it should come as little surprise that a widely diverse array of interventions has been tested. Future prospective studies of the most promising interventions in more clinically homogeneous subgroups of AI-treated breast cancer patients with AIMSS symptoms (based on symptom patterns, presumed underlying etiologies, and other factors) are now needed.
Several of the interventions included in this scoping review such as duloxetine, acupuncture, and exercise (especially when combined with psychological treatment) have shown promise for reducing centrally sensitized pain.132–134 Centrally sensitized pain is a more recent etiological hypothesis for cancer pain in general and for AIMSS in particular.135 Central sensitization is more commonly applied to classical pain syndromes such as fibromyalgia, temporomandibular joint disorder, chronic headache, and complex regional pain syndrome.136 Of interest, breast cancer survivors often report a constellation of symptoms including pain, fatigue, depression, insomnia, and cognitive dulling that are also frequently reported in patients with fibromyalgia and temporomandibular joint disorder.137,138 In a prospective study of pain in breast cancer survivors taking anti-estrogen treatments,129 the authors referenced frequent discrepancies between the objective exam findings and subject-reported pain intensities and functional impairment, which are characteristic of central sensitization. Moreover, a cross-sectional study of the prevalence of three types of pain (nociceptive, neuropathic, or central sensitization) in a cohort of breast cancer survivors with chronic pain documented central sensitization in 44% of participants, 75% of whom were experiencing arthralgia due to AIs or SERMs.16 Although a central sensitization hypothesis for AIMSS awaits confirmation, it may still be an important mechanism to consider given its multifactorial nature and limited response to traditional analgesics.139 Additional studies of interventions for AIMSS that have been shown to have beneficial effects for centrally sensitized pain in other clinical contexts (outside or hormonal treatment effects) are thus encouraged.
Our literature search did not identify any studies investigating the effects of structured psychotherapy or psychoeducational interventions on AIMSS pain, mental health symptoms and functioning, or pain interference in AI-treated women with breast cancer. Such interventions address not only the negative psychological consequences of pain but also key mediators of pain persistence and suffering, including pain catastrophizing, pain-related fear, non-adherence to treatment, and other behavioral markers of poor illness coping.140 Specific evidence-based psychological interventions for chronic non-cancer pain include cognitive-behavioral therapy and acceptance and commitment therapy, although other approaches have shown promise.141 Psychological treatments may also be effective for persistent pain after breast cancer treatment in general, although clinical evidence is preliminary.142 High-quality investigations of individual and group-based psychological interventions for AIMSS symptoms, emotional and physical functioning, quality of life, and AI persistence are needed.
This scoping review has some limitations. The treatment of AIMSS and the identification of clinical predictors of AIMSS onset is a rapidly evolving field of inquiry, and our results are current only up to January 8, 2025. In addition, although our review addressed the full scope of interventions that have been studied for treating existing AIMSS symptoms and correlated outcomes, we excluded reports on interventions to prevent AIMSS occurrence. From a practical point of view, establishing best practices for preventing AIMSS onset may be as high a therapeutic priority as how prevalent AIMSS cases should be managed.
In conclusion, a very broad range of pharmacological, complementary-alternative and rehabilitative interventions have been studied for the treatment of AIMSS. Although the evidence base for AIMSS treatments continues to expand, the existing literature does not yet identify first-line or preferred interventions for AIMSS or a clearly evidence-based means of prioritizing or sequencing treatments based on individual patient characteristics. Our scoping review highlights key gaps that need to be addressed in future AIMSS intervention studies. Most positive findings from individual reports were from uncontrolled studies or single studies that await replication in independent cohorts and high-quality comparative effectiveness investigations are generally lacking. The sample sizes for most of the reviewed studies were small and the durations for all reviewed studies were brief relative to the expected 5–10-year course of AI therapy. There is a critical need for well-powered, longer-term studies that focus on persistence in adjuvant AI treatment and associated survival, as well as thorough comparative cost–benefit analyses across interventions for AIMSS. Well-designed studies of structured psychological treatments are also needed, given the success of these interventions for improving pain-related symptoms, functioning, and pain adjustment in other chronic or persisting pain disorders. And finally, the field awaits additional studies of intervention effects on AI persistence, survival, healthcare utilization, costs of care, and caregiver experiences.
Disclosure
Dr Saranya Chumsri reports grants, personal fees from Novartis, grants from Pfizer, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Heer E, Harper A, Escandor N, et al. Global burden and trends in premenopausal and postmenopausal breast cancer: a population-based study. Lancet Glob Health. 2020;8(8):e1027–e1037. doi:10.1016/S2214-109X(20)30215-1
2. DeSantis CE, Fedewa SA, Sauer AG, et al. Breast cancer statistics, 2015: convergence of incidence rates between black and white women. CA a Cancer J Clin. 2015;66:31–42. doi:10.3322/caac.21320
3. Senkus E, Kyriakides S, Ohno S, et al. Primary breast cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2015;26 suppl 5:V8–V30. doi:10.1093/annonc/mdv298
4. Kerr AJ, Dodwell D, McGale P, et al. Adjuvant and neoadjuvant breast cancer treatments: a systematic review of their effects on mortality. Cancer Treat Rev. 2022;105:102375. doi:10.1016/j.ctrv.2022.102375
5. Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Aromatase inhibitors versus tamoxifen in early breast cancer: patient-level meta-analysis of the randomised trials. Lancet. 2015;386:1341–1352. doi:10.1016/S0140-6736(15)61074-1
6. Burstein HJ, Lacchetti C, Anderson H, et al. Adjuvant endocrine therapy for women with hormone receptor–positive breast cancer: ASCO clinical practice guideline focused update. J Clin Oncol. 2018;36. doi:10.1200/JCO.18.01160
7. Beckwée D, Leysen L, Meuwis K, Adriaenssens N. Prevalence of aromatase inhibitor-induced arthralgia in breast cancer: a systematic review and meta-analysis. Support Care Cancer. 2017;25:1673–1686. doi:10.1007/s00520-017-3613-z
8. Henry NL, Azzouz F, Desta Z, et al. Predictors of aromatase inhibitor discontinuation as a result of treatment-emergent symptoms in early-stage breast cancer. J Clin Oncol. 2012;30:936–942. doi:10.1200/JCO.2011.38.0261
9. Grigorian N, Baumrucker SJ. Aromatase inhibitor-associated musculoskeletal pain: an overview of pathophysiology and treatment modalities. SAGE Open Med. 2022;10:1–5. doi:10.1177/20503121221078722
10. Ito K, Elkin E, Blinder V, et al. Cost-effectiveness of full coverage of aromatase inhibitors for medicare beneficiaries with early breast cancer. Cancer. 2013;119(3):2494–2502. doi:10.1002/cncr.28084
11. Burstein HJ. Aromatase inhibitor-associated arthralgia syndrome. Breast. 2007;16:223–234. doi:10.1016/j.breast.2007.01.011
12. Tenti S, Correale P, Cheleschi S, et al. Aromatase inhibitor-induced musculoskeletal disorders: current knowledge on clinical and molecular aspects. Int J Mol Sci. 2020;21:5625. doi:10.3390/ijms21165625
13. Andrikopoulou A, Fiste O, Liontos M, et al. Aromatase and CKD4/6 inhibitor-induced musculoskeletal symptoms: a systematic review. Cancers. 2021;13:465. doi:10.3390/cancers13030465
14. Hyder T, Marino CC, Ahmad S, et al. Aromatase inhibitor-associated musculoskeletal syndrome: understanding mechanisms and management. Front Endocrinol. 2021;12:713700. doi:10.3389/fendo.2021.713700
15. Garcia-Giralt N, Rodriguez-Sanz M, Prieto-Alhambra D, et al. Genetic determinants of aromatase inhibitor-related arthralgia: the B-ABLE cohort study. Breast Cancer Res Treat. 2013;140:385–395. doi:10.1007/s10549-013-2638-3
16. Niravath P, Chen B, Chapman JW, et al. Vitamin D levels, vitamin D receptor polymorphisms, and inflammatory cytokines in aromatase inhibitor-induced arthralgias: an analysis of CCTG MA.27. Clin Breast Cancer. 2018;18:78–87. doi:10.1016/j.clbc.2017.10.009
17. Suskin J, Shapiro CL. Osteoporosis and musculoskeletal complications related to therapy of breast cancer. Gland Surg. 2018;7:411–423. doi:10.21037/gs.2018.07.05
18. Leysen L, Adriaenssens N, Nijs J, et al. Chronic pain in breast cancer survivors: nociceptive, neuropathic, or central sensitization pain? Pain Prac. 2019;19:183–195. doi:10.1111/papr.12732
19. Bae K, Yoo HS, Lamoury G, et al. Acupuncture for aromatase inhibitor-induced arthralgia: a systematic review. Integr Cancer Ther. 2015;14:496–502. doi:10.1177/1534735415596573
20. Chiu HY, Hsieh YJ, Tsai PS. Systematic review and meta-analysis of acupuncture to reduce cancer-related pain. Eur J Cancer Care. 2017;26(2):e12457. doi:10.1111/ecc.12457
21. Roberts KE, Rickett K, Feng S, et al. Exercise therapies for preventing or treating aromatase inhibitor-induced musculoskeletal symptoms in early breast cancer. Cochrane Database Syst Rev. 2020;1:CD012988. doi:10.1002/14651858.CD012988.pub2
22. Roberts K, Rickett K, Greer R, Woodward N. Management of aromatase inhibitor induced musculoskeletal symptoms in postmenopausal early breast cancer: a systematic review and meta-analysis. Crit Rev Oncol Hematol. 2017;111:66–80. doi:10.1016/j.critrevonc.2017.01.010
23. Roberts KE, Adsett IT, Rickett K, et al. Systemic therapies for preventing or treating aromatase inhibitor‐induced musculoskeletal symptoms in early breast cancer. Cochrane Database Syst Rev. 2022;(1):CD–13167. doi:10.1002/14651858.CD013167.pub2
24. Gupta A, Henry NL, Loprinzi CL. Management of aromatase inhibitor-induced musculoskeletal symptoms. JCO Oncol Pract. 2020;16:733–739. doi:10.1200/OP.20.00113
25. Richards BL, Whittle SL, Buchbinder R. Neuromodulators for pain management in rheumatoid arthritis. Cochrane Database Syst Rev. 2012;1(1):CD008921. doi:10.1002/14651858.CD008921.pub2
26. NCCIH (National Center for Complementary and Integrative Health). Complementary, alternative, or integrative health: what’s in a name? Available from: https://www.nccih.nih.gov/health/complementary-alternative-or-integrative-health-whats-in-a-name.
27. Ramsey I, Corsini N, Hutchinson AD, et al. A core set of patient-reported outcomes for population-based cancer survivorship research: a consensus study. J Cancer Surviv. 2021;15:201–212. doi:10.1007/s11764-020-00924-5
28. Alhanafy AM, Labeeb A, Khalil A. The role of diuretics in treatment of aromatase inhibitors induced musculoskeletal symptoms in women with non metastatic breast cancer. Asian Pac J Cancer Prev. 2018;19:3525–3531. doi:10.31557/APJCP.2018.19.12.3525
29. Vijaya Vani S A, Ananthanarayanan PH, Kadambari D, et al. Effects of vitamin D and calcium supplementation on side effects profile in patients of breast cancer treated with letrozole. Clin Chim Acta. 2016;459:53–56. doi:10.1016/j.cca.2016.05.020
30. Baglia ML, Lin I-H, Cartmel B, et al. Endocrine-related quality of life in a randomized trial of exercise on aromatase inhibitor-induced arthralgias in breast cancer survivors. Cancer. 2019;125:2262–2272. doi:10.1002/cncr.32051
31. Bahcacı U, Atasavun US, Erdogan Iyigu¨n Z, et al. Progressive relaxation training in patients with breast cancer receiving aromatase inhibitor therapy-randomized controlled trial. PLoS One. 2024;19(4):e0301020. doi:10.1371/journal.pone.0301020
32. Bao T, Cai L, Giles JT, et al. A dual-center randomized controlled double blind trial assessing the effect of acupuncture in reducing musculoskeletal symptoms in breast cancer patients taking aromatase inhibitors. Breat Cancer Res Treat. 2013;138:167–174. doi:10.1007/s10549-013-2427-z
33. Bao T, Cai L, Snyder C, et al. Patient-reported outcomes in women with breast cancer enrolled in a dual-center, double-blind, randomized controlled trial assessing the effect of acupuncture in reducing aromatase inhibitor-induced musculoskeletal symptoms. Cancer. 2014;120:381–389. doi:10.1002/cncr.28352
34. Barbosa KDP, da Silva LGT, Garcia PA, et al. Effectiveness of Pilates and circuit-based exercise in reducing arthralgia in women during hormone therapy for breast cancer: a randomized, controlled trial. Support Care Cancer. 2021;29:6051–6059. doi:10.1007/s00520-021-06180-2
35. Barzaghi S, Gozzo S, Giardina G, et al. Acupuncture for the treatment of arthralgia related to adjuvant aromatase inhibitor therapy in postmenopausal breast cancer patients. Ann Oncol. 2015;26(suppl. 6):v3–v25. doi:10.1093/annonc/mdv336.75
36. Boing L, de Bem Fretta T, Lynch BM, et al. Mat Pilates and belly dance: effects on patient-reported outcomes among breast cancer survivors receiving hormone therapy and adherence to exercise. Complementary Therapies Clinl Pract. 2023;50:101683. doi:10.1016/j.ctcp.2022.101683
37. Briot K, Tubiana-Hulin M, Bastit L, et al. Effect of a switch of aromatase inhibitors on musculoskeletal symptoms in postmenopausal women with hormone-receptor positive breast cancer: the ATOLL (articular tolerance of letrozole) study. Breast Cancer Res Treat. 2010;120:127–134. doi:10.1007/s10549-009-0692-7
38. Campbell A, Heydarian R, Ochoa C, et al. Single arm Phase II study of oral vitamin B12 for the treatment of musculoskeletal symptoms associated with aromatase inhibitors in women with early stage breast cancer. Breast J. 2018;24:260–268. doi:10.1111/tbj.12951
39. Cantarero-Villanueva I, Fernandez-Lao C, Caro-Moran E, et al. Aquatic exercise in a chest-high pool for hormone therapy-induced arthralgia in breast cancer survivors: a pragmatic controlled trial. Clin Rehabil. 2013;27:123–132. doi:10.1177/0269215512448256
40. Cantarero-Villanueva I, Fernandez-Lao C, Diaz-Rodriguez L, et al. A multimodal exercise program and multimedia support reduce cancer-related fatigue in breast cancer survivors: a randomized controlled clinical trial. Eur J Int Med. 2011;3:e189–e200. doi:10.1016/j.eujim.2011.08.001
41. Cathcart-Rake E, Novotny P, Leon-Ferre R, et al. A randomized, double-blind, placebo-controlled trial of testosterone for treatment of postmenopausal women with aromatase inhibitor-induced arthralgias: alliance study A221102. Support Care Cancer. 2021;29:387–396. doi:10.1007/s00520-020-05473-2
42. Chan A, De Boer R, Gan A, et al. Randomized phase II placebo-controlled study to evaluate the efficacy of topical pure emu oil for joint pain related to adjuvant aromatase inhibitor use in postmenopausal women with early breast cancer: JUST (Joints Under Study). Support Care Cancer. 2017;25:3785–3791. doi:10.1007/s00520-017-3810-9
43. Yeh CH, Lin W-C, Kwai-Ping Suen L, et al. Auricular point acupressure to manage aromatase inhibitor-induced arthralgia in postmenopausal breast cancer survivors: a pilot study. ONF. 2017;44:476–487. doi:10.1188/17.ONF.476-487
44. Conejo I, Pajares B, Alba E, et al. Effect of neuromuscular taping on musculoskeletal disorders secondary to the use of aromatase inhibitors in breast cancer survivors: a pragmatic randomized clinical trial. BMC Compl Alern Med. 2018;18:180. doi:10.1186/s12906-018-2236-3
45. Crew KD, Capodice JL, Greenlee H, et al. Pilot study of acupuncture for the treatment of joint symptoms related to adjuvant aromatase inhibitor therapy in postmenopausal breast cancer patients. J Cancer Surviv. 2007;1:283–291. doi:10.1007/s11764-007-0034-x
46. Crew KD, Capodice JL, Greenlee H, et al. Randomized, blinded, sham-controlled trial of acupuncture for the management of aromatase inhibitor-associated joint symptoms in women with early-stage breast cancer. J Clin Oncol. 2010;28:1154–1160. doi:10.1200/JCO.2009.23.4708
47. DeNysschen CA, Burton H, Ademuyiwa F, et al. Exercise intervention in breast cancer patients with aromatase inhibitor-associated arthralgia: a pilot study. Eur J Cancer Care. 2014;23:493–501.
48. DeSire A, Lippi L, Ammendolia A, et al. Physical exercise with or without whole-body vibration in breat cancer patients suffering from aromatase inhibitor-induced musculoskeletal symptoms: a pilot randomized clinical study. J Pers Med. 2021;11:1369. doi:10.3390/jpm11121369
49. Desideri I, Lucidi S, Francolini G, et al. Use of an alfa‑lipoic, Methylsulfonylmethane, Boswellia serrata and Bromelain dietary supplement (OPERA®) for aromatase inhibitors‑related arthralgia management (AIA): a prospective phase II trial (NCT04161833). Med Oncol. 2022;39:113. doi:10.1007/s12032-022-01723-x
50. Fields J, Richardson A, Hopkinson J, Fenlon D. Nordic walking as an exercise intervention to reduce pain in women with aromatase inhibitor-associated arthralgia: a feasibility study. J Pain Symptom Manag. 2016;52:548–559.
51. Galantino ML, Callens ML, Cardena GJ, Piela NL, Mao JJ. Tai chi for well-being of breast cancer survivors with aromatase inhibitor-associated arthralgias: a feasibility study. Altern Ther Health Med. 2013;19:38–44.
52. Galantino ML, Desai K, Greene L, et al. Impact of yoga on functional outcomes in breast cancer survivors with aromatase inhibitor-associated arthralgias. Integr Cancer Ther. 2012;11:313–320. doi:10.1177/1534735411413270
53. Gomaa S, West C, Lopez AM, et al. A telehealth-delivered tai chi intervention (TaiChi4Joint) for managing aromatase inhibitor-induced arthralgia in patients with breast cancer during COVID-19: longitudinal pilot study. JMIR Format Res. 2022;6:e34995. doi:10.2196/34995
54. Greenlee H, Crew KD, Shao T, et al. Phase II study of glucosamine with chondroitin on aromatase inhibitor-associated joint symptoms in women with breast cancer. Support Care Cancer. 2013;21:1077–1087. doi:10.1007/s00520-012-1628-z
55. Henry NL, Banerjee M, Wicha M, et al. Pilot study of duloxetine for treatment of aromatase inhibitor-associated musculoskeletal symptoms. Cancer. 2011;117:5469–5475. doi:10.1002/cncr.26230
56. Henry NL, Unger JM, Schott AF, et al. Randomized, multicenter, placebo-controlled clinical trial of duloxetine versus placebo for aromatase inhibitor-associated arthralgias in early-stage breast cancer: SWOG S1202. J Clin Oncol. 2018;36:326–332. doi:10.1200/JCO.2017.74.6651
57. Hershman DL, Unger JM, Crew KD, et al. Randomized multicenter placebo-controlled trial of omega-3 fatty acids for the control of aromatase inhibitor-induced musculoskeletal pain: SWOG S0927. J Clin Oncol. 2015;33:1910–1917. doi:10.1200/JCO.2014.59.5595
58. Hershman DL, Unger JM, Greenlee H, et al. Comparison of acupuncture vs sham acupuncture or waiting list control in the treatment of aromatase inhibitor-related joint pain: a randomized clinical trial. JAMA Network Open. 2022;5:e2241720. doi:10.1001/jamanetworkopen.2022.41720
59. Hershman DL, Unger JM, Greenlee H, et al. Effect of acupuncture vs sham acupuncture or waitlist control on joint pain related to aromatase inhibitors among women with early-stage breast cancer. JAMA. 2018;320:167–176. doi:10.1001/jama.2018.8907
60. Irwin ML, Cartmel B, Gross CP, et al. Randomized exercise trial of aromatase inhibitor-induced arthralgia in breast cancer survivors. J Clin Oncol. 2015;33:1104–1111. doi:10.1200/JCO.2014.57.1547
61. Jacobsen PB, Muchnick S, Marcus S, et al. Pilot study of Iyengar yoga for management of aromatase inhibitor-associated arthralgia in women with breast cancer. Psychooncology. 2015;24:1578–1580. doi:10.1002/pon.3756
62. Kadakia KC, Kidwell KM, Seewald NJ, et al. Prospective assessment of patient reported outcomes and estradiol of drug concentration in patients experiencing toxicity from adjuvant aromatase inhibitors. Breast Cancer Res Treat. 2017;164:411–419. doi:10.1007/s10549-017-4260-2
63. Kiyomi A, Makita M, Iwase T, et al. Clinical significance of female-hormones and cytokines in breast cancer patients complicated by aromatase inhibitor-related osteoarthropathy—efficacy of vitamin E. J Cancer. 2015;6:367. doi:10.7150/jca.10695
64. Kubo M, Onishi H, Kuroki S, et al. Short-term and low-dose prednisolone administration reduces aromatase inhibitor-induced arthralgia in patients with breast cancer. Anticancer Res. 2012;32:2331–2336.
65. Li Y, Zhang Z, Cui F, et al. Traditional Chinese medicine bionic tiger bone powder for the treatment of AI-associated musculoskeletal symptoms. Evid Based Complement Alternat Med. 2017:2478565. 10.1155/2017/2478565.
66. Liu P, Yang DQ, Xie F, et al. Effect of calcitonin on anastrozole-induced bone pain during aromatase inhibitor therapy for breast cancer. Genet Mol Res. 2014;13:5285–5291. doi:10.4238/2014.July.24.7
67. Mao JJ, Bruner DW, Stricker C, et al. Feasibility trial of electroacupuncture for aromatase inhibitor-related arthralgia in breast cancer survivors. Integr Cancer Ther. 2009;8:123–129. doi:10.1177/1534735409332903
68. Mao JJ, Liou KT, Baser RE, et al. Effectiveness of electroacupuncture or auricular acupuncture vs usual care for chronic musculoskeletal pain among cancer survivors: the PEACE randomized clinical trial. JAMA Oncol. 2021;7:720–727. doi:10.1001/jamaoncol.2021.0310
69. Mao JJ, Xie SX, Farrar JT, et al. A randomized trial of electro-acupuncture for arthralgia related to aromatase inhibitor use. Eur J Cancer. 2014;50:267–276. doi:10.1016/j.ejca.2013.09.022
70. Martinez N, Herrera M, Frias L, et al. A combination of hydroxytyrosol, omega‑3 fatty acids and curcumin improves pain and inflammation among early stage breast cancer patients receiving adjuvant hormonal therapy: results of a pilot study. Clin Transl Oncol. 2019;21:489–498. doi:10.1007/s12094-018-1950-0
71. Martinez JA, Wertheim BC, Rose DJ, et al. Sulindac improves stiffness and quality of life in women taking aromatase inhibitors for breast cancer. Breast Cancer Res Treat. 2022;192:113–122. doi:10.1007/s10549-021-06485-0
72. Nyrop KA, Callahan LF, Cleveland RJ, et al. Randomized controlled trial of a home-based walking program to reduce moderate to severe aromatase inhibitor-associated arthralgia in breast cancer survivors. Oncologist. 2017;22:1238–1248. doi:10.1634/theoncologist.2017-0174
73. Nyrop KA, Muss HB, Hackney B, et al. Feasibility and promise of a 6-week program to encourage physical activity and reduce joint symptoms among elderly breast cancer survivors on aromatase inhibitor therapy. J Geriatr Oncol. 2014;5:148–155. doi:10.1016/j.jgo.2013.12.002
74. Oh B, Kimble B, Costa DSJ, et al. Acupuncture for treatment of arthralgia secondary to aromatase inhibitor therapy in women with early breast cancer: pilot study. Acupunct Med. 2013;31:264–271. doi:10.1136/acupmed-2012-010309
75. Peng N, Yu M, Yang G, et al. Effects of the Chinese medicine Yi Shen Jian Gu granules on aromatase inhibitor-associated musculoskeletal symptoms: a randomized, controlled clinical trial. Breast. 2018;37:18–27. doi:10.1016/j.breast.2017.08.003
76. Peppone LJ, Janelsins MC, Kamen C, et al. The effect of YOCAS©® yoga for musculoskeletal symptoms among breast cancer survivors on hormonal therapy. Breast Cancer Res Treat. 2015;150:597–604. doi:10.1007/s10549-015-3351-1
77. Rastelli AL, Taylor ME, Gao F, et al. Vitamin D and aromatase inhibitor-induced musculoskeletal symptoms (AIMSS): a Phase II, double-blind, placebo-controlled, randomized trial. Breast Cancer Res Treat. 2011;129:107–116. doi:10.1007/s10549-011-1644-6
78. Schnell PM, Lustberg MB, Henry NL. Adverse events and perception of benefit from duloxetine for treating aromatase inhibitor-associated arthralgias. JNCI Cancer Spectrum. 2021;5:pkab018. doi:10.1093/jncics/pkab018
79. Shapiro AC, Adlis SA, Robien K, et al. Randomized, blinded trial of vitamin D3 for treating aromatase inhibitor-associated musculoskeletal symptoms (AIMSS). Breast Cancer Res Treat. 2016;155:501–512. doi:10.1007/s10549-016-3710-6
80. Shenouda M, Copley R, Pacioles T, et al. Effect of tart cherry on aromatase inhibitor-induced arthralgia (AIA) in nonmetastatic hormone-positive breast cancer patients: a randomized double-blind placebo-controlled trial. Clin Breast Cancer. 2022;22:e30–e36. doi:10.1016/j.clbc.2021.06.007
81. Sordi R, Castro SN, Lera AT, et al. Randomized, double-blind, placebo-controlled phase II clinical trial on the use of Uncaria tomentosa (cat’s claw) for aromatase inhibitor-induced arthralgia: a pilot study. J Nat Remedies. 2019;19:24–31. doi:10.18311/jnr/2019/22867
82. Tamaki K, Takaesu M, Nagamine S, et al. Final results of the randomized trial of exercise intervention vs. usual care for breast cancer patients with aromatase inhibitor to prevent and improve the aromatase inhibitor induced arthralgia. Cancer Res. 2018;78(4 suppl):P6–11–01–P6–11–01. doi:10.1158/1538-7445.SABCS17-P6-11-01
83. Tsai C-L, Liiu L-C, Liao C-Y, et al. Yoga versus massage in the treatment of aromatase inhibitor‑associated knee joint pain in breast cancer survivors: a randomized controlled trial. Sci Rep. 2021;11:14843. doi:10.1038/s41598-021-94466-0
84. Zhang Q, Tang D, Zhao H. Immunological therapies can relieve aromatase inhibitor-related joint symptoms in breast cancer survivors. Am J Clin Oncol. 2010;33:557–560. doi:10.1097/COC.0b013e3181cae782
85. Zhang X, Peng N, Yu M-W, et al. Chinese medicine Yishen Jiangu Granules on aromatase inhibitor-associated musculoskeletal symptoms. Chin J Integr Med. 2017;24:867–872.
86. Bao T, Betts K, Tarpinian K, et al. Changes in patient-reported outcomes in women with breast cancer in a multicenter double-blind randomized controlled trial assessing the effect of acupuncture in reducing aromatase inhibitor-induced musculoskeletal symptoms (AIMSS). J Clin Oncol. 2012;30(15 suppl):1.
87. Birrell S, Tilley W. Treatment reduces joint morbidities induced by anastrozole therapy in postmenopausal women with breast cancer: results of a double-blind, randomized phase II trial. Cancer Res. 2009;69(24 suppl):804. doi:10.1158/0008-5472.SABCS-09-804
88. Cheng H-L, Yeung WF, Li CY, et al Self-acupressure for pain, fatigue, and sleep disturbance in breast cancer survivors receiving aromatase inhibitors: a pilot trial. Support Care Cancer. 2023;31(suppl 1):S260–S261.
89. Crespo-Bosque M, Brown C, Cartmel B, et al. Pain and sensitization in women with aromatase inhibitor-associated arthralgias. Arthritis Rheumatol. 2016;68(suppl 10):1.
90. Fleege NMG, Miller E, Kidwell KM, et al. The impact of cannabidiol (CBD) on aromatase inhibitor (AI)-associated musculoskeletal symptoms (AIMSS). J Clin Oncol. 2024;42(16 suppl):1.
91. Hershman CL, Unger JM, Crew KD, et al. Omega-3 fatty acids for aromatase inhibitor–induced musculoskeletal symptoms in women with early-stage breast cancer (SWOG S0927). J Clin Oncol. 2014;32(15 suppl):9532. doi:10.1200/jco.2014.32.15_suppl.9532
92. Hershman DL, Unger JM, Greenlee H, et al. Long-term results from a randomized blinded sham- and waitlist-controlled trial of acupuncture for joint symptoms related to aromatase inhibitors in early stage breast cancer (S1200). J Clin Oncol. 2021;39(15 suppl):12018. doi:10.1200/JCO.2021.39.15_suppl.12018
93. Leibel L, Metri K, Prasad R, et al. Effect of Sukshma vyayama yoga on aromatase inhibitor-induced arthralgia in breast cancer patients: a feasibility study conducted on Facebook. Support Care Cancer. 2022;30(suppl 1):S14.
94. Lippi L, de Sire A, Ammendolia A, et al. Abstract P4-10-15: whole-body vibration combined with physical exercise to treat aromatase inhibitor-induced musculoskeletal symptoms in breast cancer women: results of a pilot randomized controlled study. Cancer Res. 2022;82(4 suppl):P4–10–15–P4–10–15. doi:10.1158/1538-7445.SABCS21-P4-10-15
95. Massimino K, Glissmeyer M, Wagie T, et al. Use of blue citrus, a Chinese herbal remedy, to reduce side effects of aromatase inhibitors. J Clin Oncol. 2011;29:170. doi:10.1200/jco.2011.29.27_suppl.170
96. Nahleh ZA, Campbell A, Heydarian R, et al. Effects of oral vitamin B12 for the treatment of aromatase inhibitors (AI)-related musculoskeletal symptoms in women with early stage breast cancer. J Clin Oncol. 2018;36:86. doi:10.1200/JCO.2018.36.7_suppl.86
97. Tajaesu M, Tamaki K, Nagamine S, et al. Abstract P5-12-01: randomized trial of exercise intervention vs. usual care for breast cancer patients with aromatase inhibitor to prevent and improve the aromatase inhibitor induced arthralgia. Cancer Res. 2017;77(4 suppl):P5–12–01–P5–12–01. doi:10.1158/1538-7445.SABCS16-P5-12-01
98. Varadarajan R, Helm E, Arnold C, et al. Directed exercise intervention in breast cancer patients with arthralgias receiving aromatase inhibitors: a randomized pilot study. Cancer Res. 2016;76(4 suppl):P5–12–04–P5–12–04. doi:10.1158/1538-7445.SABCS15-P5-12-04
99. Zylla M, Idossa D, Borrero M, et al. A randomized trial of topical cannabis balms for the treatment of aromatase inhibitor–associated musculoskeletal syndrome (AIMSS). J Clin Oncol. 2024;42(16 suppl):e24129–e24129. doi:10.1200/JCO.2024.42.16_suppl.e24129
100. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;62(10). doi:10.1136/bmj.b2700
101. Cleeland CS, Ryan KM. Pain assessment: global use of the Brief Pain Inventory. Ann Acad Med Singapore. 1994;23:32129–32138.
102. McConnell S, Kolopack P, Davis AM. The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC): a review of its utility and measurement properties. Arthritis Care Res. 2001;45:453–461. doi:10.1002/1529-0131(200110)45:5<453::AID-ART365>3.0.CO;2-W
103. Beaton DE, Katz JN, Fossel AH, et al. Measuring the whole or the parts? Validity, reliability, and responsiveness of the Disabilities of the Arm, Shoulder and Hand outcome measure in different regions of the upper extremity. J Hand Ther. 2001;14:128–146. doi:10.1016/S0894-1130(01)80043-0
104. Mintken PE, Glynn P, Cleland JA. Psychometric properties of the shortened disabilities of the arm, shoulder, and hand questionnaire (QuickDASH) and numeric pain rating scale in patients with shoulder pain. J Shoulder Elbow Surg. 2009;18:920–926. doi:10.1016/j.jse.2008.12.015
105. Sautner J, Andel I, Rintelen B, Leeb BF. Development of the M-SACRAH, a modified, shortened version of SACRAH (score for the assessment and quantification of chronic rheumatoid affections of the hands). Rheumatology. 2004;43:1409–1413. doi:10.1093/rheumatology/keh360
106. Amtmann DA, Cook KF, Jensen MP, et al. Development of a PROMIS item bank to measure pain interference. Pain. 2010;150:173–182. doi:10.1016/j.pain.2010.04.025
107. Askew RL, Cook KF, Keefe FJ, et al. A PROMIS measure of neuropathic pain quality. Value Health. 2016;19:623–630. doi:10.1016/j.jval.2016.02.009
108. Allen KD, DeVellis RF, Renner JB, et al. Validity and factor structure of the AUSCAN osteoarthritis hand index in a community-based sample. Osteoarthritis Cartilage. 2007;15:830–836. doi:10.1016/j.joca.2007.01.012
109. Nicholas MK. The pain self-efficacy questionnaire: taking pain into account. Eur J Pain. 2007;11:153–163. doi:10.1016/j.ejpain.2005.12.008
110. Cella DF, Tulsky DS, Gray G, et al. The functional assessment of cancer therapy (FACT) scale: development and validation of the general measure. J Clin Oncol. 1993;11:570–579. doi:10.1200/JCO.1993.11.3.570
111. Fries J, Spitz PW, Young DY. The dimensions of health outcomes: the health assessment questionnaire, disability and pain scales. J Rheumatol. 1982;9:789–793.
112. Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30:473–483. doi:10.1097/00005650-199206000-00002
113. Rabin R, de Charro F. EQ-5D: a measure of health status from the EuroQol Group. Ann Med. 2001;33:337–343. doi:10.3109/07853890109002087
114. Farasyn A, Meeusen R, Nijs J, Cuesta-Vargas A. Exploration of the validity and reliability of the “backache disability index” (BADIX) in patients with non-specific low back pain. J Back Musculoskelet Rehabil. 2013;26:451–459. doi:10.3233/BMR-130405
115. Richardson MT, Leon AS, Jacobs DR, et al. Comprehensive evaluation of the Minnesota leisure time physical activity questionnaire. J Clin Epidemiol. 1994;47:271–281. doi:10.1016/0895-4356(94)90008-6
116. Duncan P, Weiner DK, Chandler J, Studenski S. Functional reach: a new clinical measure of balance. J Gerontol. 1990;45:M192–M197. doi:10.1093/geronj/45.6.M192
117. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67:361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
118. Kroenke K, Spitzer RL, Williams JBW. The PHQ-9:m validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606–613. doi:10.1046/j.1525-1497.2001.016009606.x
119. Kroenke K, Spitzer RL, Williams JBW, Lowe B. An ultra-brief screening scale for anxiety and depression: the PHQ-4. Psychosomatics. 2009;50:613–621. doi:10.1176/appi.psy.50.6.613
120. Radloff LS. The CES-D Scale: a self-report depression scale for research in the general population. Appl Psychol Measurement. 1977;1:385–401.
121. Norcross JC, Guadagnoli E, Prochaska JO. Factor structure of the profile of mood states (POMS): two partial replications. J Clin Psychol. 1984;40:1270–1277. doi:10.1002/1097-4679(198409)40:5<1270::aid-jclp2270400526>3.0.co;2-7
122. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Social Behav. 1983;24:385–396.
123. Buysse DJ, Reynolds CF, Monk TH, et al. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28:193–213. doi:10.1016/0165-1781(89)90047-4
124. Morin CM, Belleville G, Bélanger L, Ivers H. The Insomnia Severity Index: psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep. 2011;34(5):601–608. doi:10.1093/sleep/34.5.601
125. Carpenter JS. The hot flash related daily interference scale: a tool for assessing the impact of hot flashes on quality of life following breast cancer. J Pain Symptom Manage. 2001;22:979–989. doi:10.1016/S0885-3924(01)00353-0
126. Radtke JV, Terhorst L, Cohen SM. The menopause-specific quality of life (MENQOL) questionnaire: psychometric evaluation among breast cancer survivors. Menopause. 2011;18:289–295. doi:10.1097/gme.0b013e3181ef975a
127. Palmieri FM, Barton DL. Challenges of oral medications in patients with advanced breast cancer. Seminars Oncol Nurs. 2007;23(suppl 2):S17–S22. doi:10.1016/j.soncn.2007.10.004
128. De Placido S, Gallo C, De Laurentiis M, et al. Adjuvant anastrozole versus exemestane versus letrozole, upfront or after 2 years of tamoxifen, in endocrine-sensitive breast cancer (FATA-GIM3): a randomised, Phase 3 trial. Lancet Oncol. 2018;19:474–485. doi:10.1016/S1470-2045(18)30116-5
129. Henry NL, Giles JT, Ang D, et al. Prospective characterization of musculoskeletal symptoms in early stage breast cancer patients treated with aromatase inhibitors. Breast Cancer Res Treat. 2008;111:365–372. doi:10.1007/s10549-007-9774-6
130. Presant CA, Bosserman L, Young T, et al. Aromatase inhibitor-associated arthralgia and/ or bone pain: frequency and characterization in non-clinical trial patients. Clin Breast Cancer. 2007;7:775–778. doi:10.3816/CBC.2007.n.038
131. Sestak I, Sapunar F, Cuzick J. Aromatase inhibitor-induced carpal tunnel syndrome: results from the ATAC trial. J Clin Oncol. 2009;27:4961–4965. doi:10.1200/JCO.2009.22.0236
132. Birkinshaw H, Fridrich CM, Cole P, et al. Antidepressants for pain management in adults with chronic pain: a network meta-analysis. Cochrane Database Syst Rev. 2023;5(5):CD014682. doi:10.1002/14651858.CD014682.pub2
133. Lai H-C, Lin Y-W, Hsieh C-L. Acupuncture-Analgesia-Mediated Alleviation of Central Sensitization. Evid Based Complement Alternat Med. 2019;2019:6173412. doi:10.1155/2019/6173412
134. Deegan O, Fullen BM, Segurado R, Doody C. The effectiveness of a combined exercise and psychological treatment programme on measures of nervous system sensitisation in adults with chronic musculoskeletal pain - a systematic review and meta-analysis. BMC Musculoskelet Disord. 2024;25:140. doi:10.1186/s12891-024-07274-8
135. Nishigami T, Manfuku M, Lahousse A. Central sensitization in cancer survivors and its clinical implications: state of the art. J Clin Med. 2023;12:4606. doi:10.3390/jcm12144606
136. Verspyck E, Attal N. Diagnosing nociplastic pain in cancer survivors: a major step forward. Br J Anaesthesia. 2023;130:515–518.
137. Aaron LA, Burke MM, Buchwald D. Overlapping conditions among patients with chronic fatigue syndrome, fibromyalgia, and temporomandibular disorder. Arch Intern Med. 2000;160:221–227. doi:10.1001/archinte.160.2.221
138. Kidwell KM, Harte SE, Hayes DF, et al. Patient-reported symptoms and discontinuation of adjuvant aromatase inhibitor therapy. Cancer. 2014;120:2403–2411. doi:10.1002/cncr.28756
139. Nijs J, Lahousse A, Fernandez-de-las-Penas C, et al. Towards precision pain medicine for pain after cancer: the cancer pain phenotyping network multidisciplinary international guidelines for pain phenotyping using nociplastic pain criteria. Br J Anaesthesia. 2023;130:611–621. doi:10.1016/j.bja.2022.12.013
140. Sturgeon JA. Psychological therapies for the management of chronic pain. Psychol Res Behav Manag. 2014;7:115–124. doi:10.2147/PRBM.S44762
141. Driscoll MA, Edwards RR, Becker WC, et al. Psychological interventions for the treatment of chronic pain in adults. Psychol Sci Public Interes. 2021;22:52–95. doi:10.1177/15291006211008157
142. Johannsen M, Farver I, Beck N, et al. The efficacy of psychosocial intervention for pain in breast cancer patients and survivors: a systematic review and meta-analysis. Breast Cancer Res Treat. 2013;138:675–690. doi:10.1007/s10549-013-2503-4
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Predicting Response to Radiotherapy in Breast Cancer-Induced Bone Pain: Relationship Between Pain and Serum Cytokine Expression Levels After Radiotherapy
Lou Y, Cao H, Wang R, Chen Y, Zhang H
Journal of Pain Research 2022, 15:3555-3562
Published Date: 11 November 2022
Radiofrequency Ablation for Chronic Lumbar Zygapophyseal Joint Pain Using a V-Shaped Active Tip Needle: An Observational Retrospective Study
Lo Bianco G, Misseri G, Stogicza AR, Cesare G, Li S, Day M, Kennedy DJ, Schatman ME
Journal of Pain Research 2023, 16:1243-1255
Published Date: 11 April 2023
Can the Assessment of the Circadian Rhythm of Pain Be Shortened? A Study of Community-Dwelling Participants with Chronic Pain
Tanaka Y, Fujii R, Shigetoh H, Sato G, Morioka S
Journal of Pain Research 2024, 17:1929-1940
Published Date: 25 May 2024
Effects of Continuous Perioperative Esketamine Infusion on Postoperative Depression in Breast Cancer Patients: A Randomized Controlled Double-Blind Trial
Shen M, Xuan Y, Chen K, Lei W, Huang Y, Wang J, Sun J, Lu X
Drug Design, Development and Therapy 2025, 19:9685-9695
Published Date: 29 October 2025
Management Strategies for Aromatase Inhibitor-Associated Musculoskeletal Symptoms and Their Impact on Treatment Persistence in Postmenopausal Breast Cancer: A Single-Center Retrospective Cohort Study
Liang M, Yuan S, Xue Y, Li J, Chen C
International Journal of Women's Health 2026, 18:603205
Published Date: 25 May 2026