Back to Journals » Drug Design, Development and Therapy » Volume 19
Effects of Continuous Perioperative Esketamine Infusion on Postoperative Depression in Breast Cancer Patients: A Randomized Controlled Double-Blind Trial
Authors Shen M ![]() , Xuan Y, Chen K
, Xuan Y, Chen K ![]() , Lei W, Huang Y, Wang J, Sun J, Lu X
, Lei W, Huang Y, Wang J, Sun J, Lu X
Received 16 May 2025
Accepted for publication 23 October 2025
Published 29 October 2025 Volume 2025:19 Pages 9685—9695
DOI https://doi.org/10.2147/DDDT.S540781
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Mengting Shen,1,2 Ye Xuan,1,2 Kaiyu Chen,1,2 Weiping Lei,2 Yaqin Huang,2 Junhui Wang,3 Jianliang Sun,1,2,* Xinlei Lu2,*
1The Fourth School of Clinical Medicine, Zhejiang Chinese Medical University, Hangzhou First People’s Hospital, Hangzhou, Zhejiang, People’s Republic of China; 2Department of Anesthesiology, Affiliated Hangzhou First People’s Hospital, School of Medicine, Westlake University, Hangzhou, Zhejiang, People’s Republic of China; 3Affiliated Luqiao Hospital, HangZhou City University School of Medicine, Taizhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jianliang Sun, Email [email protected] Xinlei Lu, Email [email protected]
Background: Comorbid depressive symptoms are prevalent in patients with breast cancer, which adversely impacts postoperative recovery outcomes. Esketamine has emerged as a promising intervention for perioperative depression due to its rapid and sustained effects. This study aims to investigate the impact of the continuous intravenous infusion of esketamine during the perioperative period on postoperative depressive symptoms in breast cancer patients.
Methods: In this randomized, double-blind, controlled trial, 96 female patients aged 18– 65 years undergoing unilateral modified radical mastectomy were enrolled. Participants were randomly assigned to one of two groups. The esketamine group received 0.5 mg/kg and 0.25 mg/kg/h esketamine and the normal saline group received 5 mL and 0.25 mL/kg/h normal saline during anesthesia induction and maintenance, respectively. The primary outcome was the Hamilton Depression Rating Scale (HAMD-17) score on postoperative day 30 (POD-30). Secondary outcomes included HAMD-17 scores on POD 1 and 3; self-Rating Depression Scale (SDS) scores on POD 1, 3, and 30; serum levels of brain-derived neurotrophic factor (BDNF) and serotonin (5-hydroxytryptamine, 5-HT) after surgery; relative changes in heart rate (HR) and mean arterial pressure (MAP) before and after intubation; time to awakening; Visual Analog Scale (VAS) pain scores; and adverse events related to esketamine.
Results: The HAMD-17 score on POD-30 was significantly lower in the esketamine group [3.00 (2.08– 4.10)] than in the normal saline group [5.00 (4.00– 6.20)]. Regarding secondary outcomes, HAMD-17 scores on POD 1 and 3 were significantly lower in the esketamine group. SDS scores on POD 1, 3, and 30 were also significantly lower in the esketamine group. Compared with the saline group, the esketamine group exhibited significantly higher postoperative levels of BDNF and serotonin. Additionally, VAS scores at 30 minutes after extubation were significantly lower in the esketamine group. There was no significant difference in the incidence of adverse reactions between the two groups.
Conclusion: Perioperative continuous administration of esketamine reduces postoperative depression scores in patients undergoing breast cancer surgery.
Trial Registration: Chinese Clinical Trial Registry. Identifier: ChiCTR2200061575.
Keywords: esketamine, perioperative period, breast cancer, postoperative depression, brain-derived neurotrophic factor, 5-hydroxytryptamine, pain
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Matthewson has been published for this article.
Introduction
Breast cancer remains the most common cancer among women worldwide. In 2022, breast cancer was a leading cause of cancer-related death among women, with approximately 2.3 million new cases and 670,000 deaths.1 Advancements in early detection and treatment strategies have increased the relative survival rate and extended the lifespan of breast cancer patients in China.2 However, breast cancer patients often face post-surgical challenges, such as body image impairment, marital issues, surgical trauma, pain, and psychological stress, which can lead to various psychological symptoms. A review of 71 articles published between January 2000 and November 2021 by Javan Biparva et al estimated the overall prevalence of depression among breast cancer patients to be 30.2%.3 Depression and anxiety can affect physiological functions, treatment adherence, and quality of life of breast cancer patients, and may significantly impact the cancer recurrence and mortality of these patients.4 Therefore, in addition to cancer management, the diagnosis and treatment should consider reducing physical and psychological stress experienced by these patients.
Recent clinical trials have increasingly demonstrated the rapid antidepressant effects of esketamine (S-ketamine) and ketamine (a mixture of R-ketamine and S-ketamine),5,6 which is also effective in patients who are unresponsive to traditional antidepressants.7 Previous studies have indicated that ketamine enhances the synthesis, release, and tropomyosin receptor kinase B (TrkB) activation of brain-derived neurotrophic factor (BDNF),8,9 and that blocking BDNF signaling abolishes its antidepressant effects.8 Serotonin (5-hydroxytryptamine, 5-HT) neurotransmission is also involved in the rapid antidepressant action of ketamine.10
Furthermore, in vitro studies showed that S-ketamine (such as esketamine) had a four-fold higher affinity for NMDA receptors than R-ketamine,11 and could reduce the complications typically associated with R-ketamine, such as psychotomimetic effects. Paul et al found that esketamine had fewer side effects while producing similar antidepressant effects as ketamine, thus demonstrating better tolerability.12 In 2019, the United States Food and Drug Administration approved the use of intranasal esketamine in combination with oral antidepressants for depression treatment.13 It has been already shown to have antihyperalgesic effects, providing benefits comparable to those of ketamine.14,15
Previous research on esketamine to prevent post-surgical depression in breast cancer patients has often focused on single applications or short-term postoperative depression management.16 Our current randomized controlled prospective clinical trial aimed to investigate the impact of a continuous infusion of esketamine on the postoperative severity of short-term and long-term depression in breast cancer patients. We aimed to provide appropriate perioperative treatment regimens to prevent and treat depressive symptoms after radical mastectomy, ensuring a comfortable and safe perioperative experience for breast cancer patients.
Methods
Study Design, Participant Selection, and Ethical Approval
This randomized controlled double-blind clinical trial was performed at the Hangzhou First People’s Hospital, affiliated with Westlake University School of Medicine, in China, from October 2023 and April 2024. The study protocol was approved by the hospital ethics committee in June 2022 (Approval No. IIT-20220502-0068-01). The trial was prospectively registered at the Chinese Clinical Trial Registry (www.chictr.org.cn) on June 29, 2022 (Registration No. ChiCTR2200061575, https://www.chictr.org.cn/showproj.html?proj=172370). All study participants signed written informed consents. This conduct and reporting of this clinical trial adhered to the CONSORT guidelines.
The inclusion criteria were female patients who met the following conditions: 1) aged 18–65 years; 2) scheduled for undergo modified radical mastectomy for unilateral breast cancer; 3) had an American Society of Anesthesiologists (ASA) classification of I–II; 4) had a body mass index (BMI) of 18–40 kg/m2; 5) provided their fully informed written consent. The exclusion criteria were patients who met the following conditions: 1) had a history of mental illnesses such as schizophrenia, mania, or other psychiatric disorders; 2) had received psychotropic medication; 3) had uncontrolled high blood pressure or elevated intraocular pressure; 4) had other serious systemic diseases (including severe heart, kidney, or liver disease); 5) were allergic to the drugs used in this study; 6) receiving opioid medication or experiencing chronic pain.
Randomization and Blinding
Upon obtaining written informed consent, the patients were randomized to an esketamine group or a normal saline group at a 1:1 ratio once entering the preoperative waiting area. A random number table was generated using Excel, in which an even number designated the esketamine group and an odd number designated the normal saline group.
This was a double-blind study. One researcher was responsible for the study blinding, including the random number table and the preparation of the research medication. One researcher and a research assistant were responsible for intraoperative anesthesia management. The evaluators were blinded to the allocation group and were responsible for postoperative follow-up, data collection, and statistical analysis. Both the anesthesiologist and the patients remained blinded throughout the entire process.
Monitoring
On the day prior to surgery, patients were assessed in the ward using the 17-item Hamilton Depression Rating Scale (HAMD-17) and the Self-Rating Depression Scale (SDS). After the patient entered the operating room and during the entire anesthesia and surgery process, the heart rate (HR), oxygen saturation (SPO2), blood pressure (BP), and bispectral index (BIS) were recorded every 10 minutes. Venous blood samples were collected prior to anesthesia induction to determine preoperative serum levels of serotonin (5-HT) and brain-derived neurotrophic factor (BDNF).
Anesthetic Treatment
The trial medication was prepared by the researchers in accordance with the group assignment, diluted it to a specific volume with normal saline, and then delivered it to the anesthesiologist.
The anesthesiologist induced anesthesia using 0.05 mg/kg midazolam, 2 mg/kg propofol, 0.2 mg/kg cisatracurium, and 0.5 μg/kg sufentanil. In the esketamine group, after the loss of consciousness with anesthesia induction, patients were administered 0.5 mg/kg esketamine (diluted to 5 mL with normal saline). During the anesthesia maintenance phase, esketamine was administered at a rate of 0.25 mg/kg/h (diluted to 1 mg/mL with normal saline). In the normal saline group, after the loss of consciousness with anesthesia induction, patients received 5 mL of normal saline. During the anesthesia maintenance phase, normal saline was administered at a rate of 0.25 mL/kg/h. All medications were administered by an anesthesiologist who was blinded to group assignment. During the anesthesia maintenance phase, intravenous-inhalation combined anesthesia was used. A combination of 3–5 mg/kg/min propofol, 0.1–0.3 μg/kg/min remifentanil, and 0.5 MAC sevoflurane were used to maintain the depth of anesthesia based on the target BIS value (40–60). Additionally, 0.05 mg/kg cisatracurium and at 0.1 μg/kg sufentanil were administered every 50 minutes. Before suturing the skin, 2 mg of tropisetron was administered to prevent postoperative nausea and vomiting (PONV), and then sevoflurane and esketamine were discontinued. At the end of the surgery, propofol and remifentanil were discontinued. Patients were transferred to the post-anesthesia care unit (PACU) while intubated, where non-invasive blood pressure (NIBP), HR, and SpO2 were monitored. PACU nurses recorded extubation time and time of discharge from the operating room. Thirty minutes after extubation, the Visual Analog Scale (VAS) score was assessed. Patients were discharged from the PACU to the ward only when their Aldrete score reached 9.
All patients were subjected to a standardized postoperative pain management protocol. This included prophylactic intravenous administration of 5 µg sufentanil before skin closure to reduce the risk of incident pain. During the postoperative period, if a patient’s VAS score reached 4 or higher, additional analgesia was provided using intravenous flurbiprofen axetil at a single dose of 50 mg, administered 3–4 times per day, with a maximum total daily dose of 200 mg. Follow-up assessments, including relevant depression and pain scales, were conducted on postoperative days 1, 3, and 30.
Outcome Measurements
The primary outcome was depression that was measured with the HAMD-17 assessed on postoperative days 30.
Secondary outcomes included: HAMD-17 scores on postoperative days 1 and 3, and SDS scores on postoperative days 1, 3, and 30.
Venous blood samples were collected after surgery. Serum levels of serotonin 5-HT and BDNF were determined using enzyme-linked immunosorbent assay (ELISA). All samples were processed in the same laboratory following standardized procedures. The same ELISA kits were used for all measurements: human 5-hydroxytryptamine (5-HT) ELISA kit (Cat: JL10725; J&L Biological) and human brain derived neurotrophic factor (BDNF) ELISA kit (Cat: JL11683; J&L Biological).
Changes in heart rate (HR) and mean arterial pressure (MAP) before and after tracheal intubation were recorded. To account for inter-individual differences in baseline hemodynamic parameters and to better assess hemodynamic tolerance to the loading dose, post-induction changes in heart rate and blood pressure were expressed as relative changes from baseline. Specifically, the difference between the post-induction and pre-induction values was divided by the pre-induction value:
Relative change = (post-induction value − pre-induction value) / pre-induction value
This dimensionless metric reflects the proportionate change from baseline for each parameter. Recovery time was also recorded.
In addition, an 11-point VAS scale was used to evaluate the postoperative pain intensity 30 minutes after extubation (T3), on postoperative day 1 (T4), and on postoperative day 2 (T5). The perioperative pain management was recorded. Adverse events related to esketamine, including psychotomimetic side effects (hallucinations and nightmares), dizziness, agitation, and PONV, were continuously monitored for 72 h postoperatively.
Sample Size Calculation
This study was designed as a superiority trial. The sample size was calculated using G*Power software 3.1. Based on a study reported by Liu et al,16 a single administration of esketamine to prevent and treat postoperative depression reduced HAMD-17 scores 1 week postoperatively compared with the blank control group (9.4 ± 3.0 vs 11.2 ± 3.6). Using an effect size of 0.544, α = 0.05, and β = 0.2, the required sample size was calculated to be 80 participants. Considering the potential loss to follow-up or withdrawal from the study, we targeted to recruit 48 patients per group, for a total of 96 patients.
Statistical Analysis
Statistical analyses were performed using SPSS (version 27.0, IBM Corporation, Armonk, NY, USA). The Kolmogorov–Smirnov test was used to assess the normality of the data distribution. Normally distributed continuous variables were presented as mean (standard deviation). The two-sample independent t test was used for comparisons. Non-normally distributed continuous data were reported as median (interquartile range) and analyzed using the Mann–Whitney U-test. To account for multiple comparisons, the Bonferroni correction was applied, yielding an adjusted significance threshold of p < 0.0167 (0.05/3). Categorical data were presented as frequencies or rates and compared using a Chi-square (χ2) test. All graphs in this study were created using GraphPad Prism 10.0 (GraphPad Software, CA, USA). A P-value < 0.05 was considered statistically significant.
Results
Participant Characteristics
A total of 96 patients were initially enrolled. Six patients were excluded, including three who declined to participate, one with poorly controlled blood pressure, and one with a history of benzodiazepine use. Ultimately, 90 patients were randomly assigned to the study intervention. Subsequently, five patients in the esketamine group and five in the saline group were excluded due to loss to follow-up or withdrawal of consent. The final analysis included 80 patients, with 40 in each group. Detailed information regarding patient selection is presented in the flow chart (Figure 1).
 |
Figure 1 CONSORT flow diagram. |
No significant differences were observed between the groups in terms of demographic or clinical characteristics, including age, body mass index (BMI), ASA classification, duration of surgery, TNM stage, HAMD-17, and SDS scores on the day before surgery, and pre-anesthesia Heart rate, Mean arterial pressure, and serum levels of 5-HT and BDNF (Table 1).
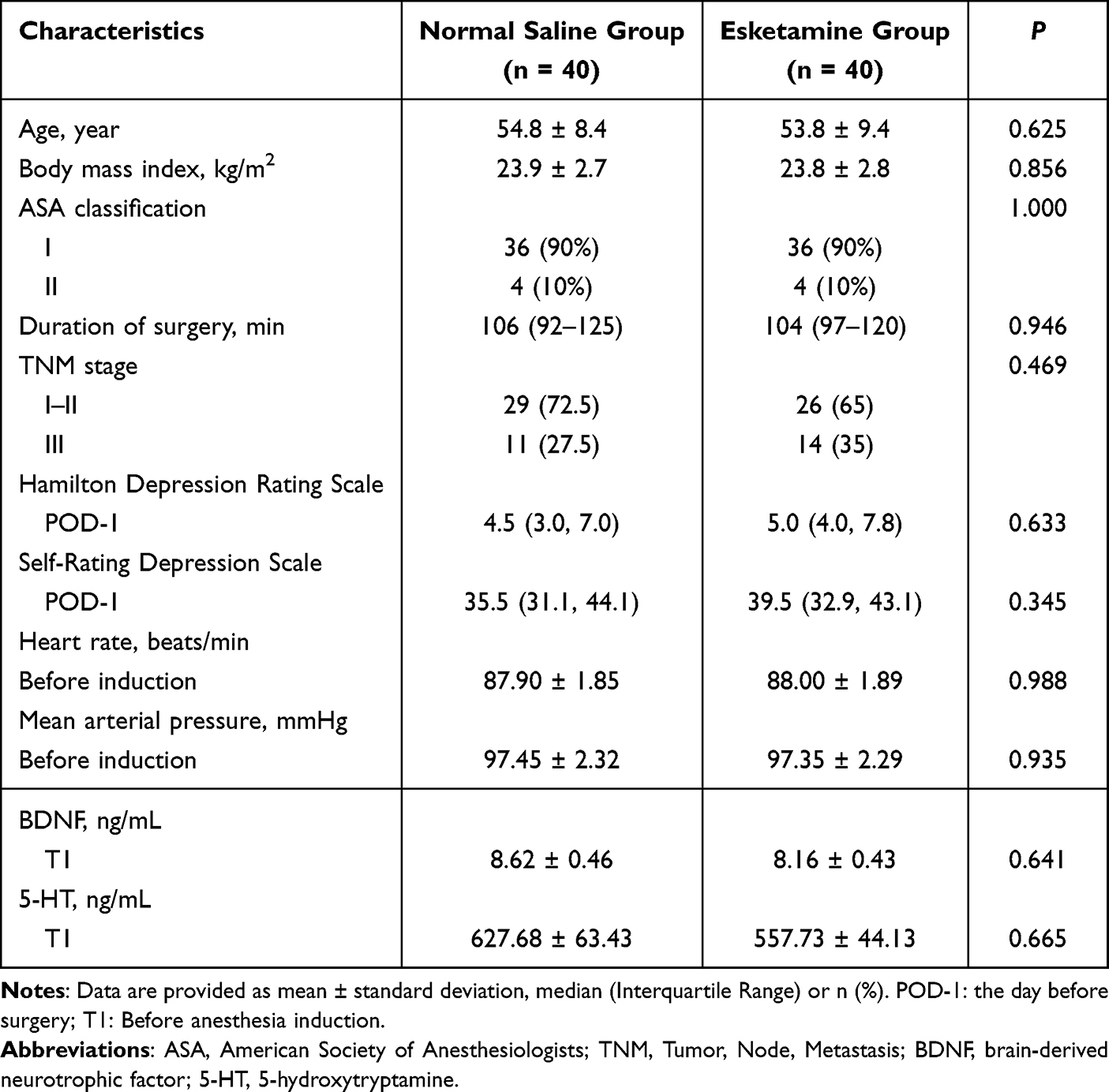 |
Table 1 Baseline Characteristic Comparisons Between Two Groups |
Postoperative Depressive Scores
The HAMD-17 score on POD-30 was significantly lower in the esketamine group [3.00 (2.08–4.10)] compared with the normal saline group [5.00 (4.00–6.20)]. On both POD-1 and POD-3, HAMD-17 scores in the esketamine group were significantly lower than those in the saline group. Similarly, SDS scores in the esketamine group were significantly lower than those in the saline group on POD-1, POD-3, and POD-30 (P < 0.0167) (Table 2 and Figure 2).
 |
Table 2 Postoperative Depression Comparisons Between Two Groups |
 |
Figure 2 Comparisons of the Hamilton Depression Rating Scale-17 (A) and the Self-Rating Depression Scale (B) scores between two groups. Data are presented as median with interquartile range. *P < 0.05; **P < 0.01, *** P < 0.001. POD-1: the day before surgery. Abbreviation: POD, postoperative day. |
Biomarker Changes
After surgery, both BDNF (10.79±0.58 ng/mL vs 6.49±0.32 ng/mL; P=0.004) and 5-HT (634.75±45.57 ng/mL vs 462.46±36.11 ng/mL; P<0.001) levels were significantly higher in the esketamine group than the normal saline group (Table 3).
 |
Table 3 Blood Brain-Derived Neurotrophic Factor (BDNF) and 5-Hydroxytryptamine (5-HT) Concentrations Before and After Surgery |
Perioperative Safety and Recovery
Relative changes in HR and MAP after induction were calculated as described above. A positive value indicates an increase relative to baseline, while a negative value indicates a decrease. No notable differences were observed between the two groups in HR or MAP relative changes, or in recovery time (P>0.05). The VAS score was significantly lower in the esketamine group compared to the normal saline group 30 minutes after extubation (3.75±0.14 vs 4.33±0.15, (P<0.0167), although there were no statistically significant differences in the VAS scores between the two groups 1 or 3 days postoperatively (P>0.0167) (Table 4).
 |
Table 4 Outcome Measurements Before and After Surgery |
Adverse events were evaluated for each group (Table 5). Two patients in the esketamine group experienced tachycardia and one patient had post-induction hypertension, whereas these events were not reported in the normal saline group. The difference was not statistically significant (P>0.05). The incidence of nausea and vomiting was higher in the esketamine than normal saline group (10 vs 7 patients), without a statistically significant difference (P = 0.586). Additionally, four incidences of neuropsychiatric symptoms (P = 0.116) and four incidences of dizziness (P = 0.116) were observed in the esketamine group, but no cases of diplopia, hallucinations, or agitation were reported.
 |
Table 5 Adverse Event Comparisons Between Two Groups |
Discussion
In our study, administering esketamine after the patient lost consciousness during anesthesia induction at 0.5 mg/kg and then continuing it at 0.25 mg/kg/h during anesthesia maintenance resulted in significantly lower scores on HAMD-17 in the esketamine group compared to the normal saline group at 30 days postoperatively. Postoperative HAMD-17 and SDS scores in the esketamine group were significantly lower than those in the normal saline group at three postoperative time points (Table 2 and Figure 2). This suggested that esketamine reduced the severity of postoperative depressive symptoms in breast cancer patients during the perioperative period. Liu et al administered 0.125 mg/kg of ketamine, esketamine, or normal saline to 303 breast cancer patients with mild to moderate depression after anesthesia induction.16 Compared to the control group, the HAMD-17 scores in the ketamine and esketamine groups were significantly lower 3 days, 1 week, and 1 month postoperatively. Moreover, esketamine had a pronounced effect on reducing postoperative depression in breast cancer patients. Their study provided the first evidence that esketamine effectively reduced postoperative depression in breast cancer patients with mild and moderate depression, and its effect was superior to that of ketamine. Wang et al administered an intravenous injection of 0.2 mg/kg esketamine to 64 breast cancer patients undergoing unilateral modified radical mastectomy for breast cancer who had no preoperative depression.17 Compared to the control group, a single sub-anesthetic dose of esketamine produced lower postoperative Patient Health Questionnaire-9 (PHQ-9) scores for subthreshold depressive symptoms on the first postoperative day (P = 0.047). However, there were no statistically significant differences in PHQ-9 scores between the two groups 3, 7, or 30 days postoperatively. Zhang et al randomly divided 90 patients undergoing modified radical mastectomy for breast cancer to an esketamine group or a control group.18 The esketamine group received esketamine (0.5 mg/kg) for anesthesia induction, followed by continuous infusion of esketamine (0.5 mg/kg/h) and remifentanil for maintenance. The control group was induced with sufentanil and maintained with remifentanil. The total quality of recovery-15 scores were significantly higher in the esketamine group on POD-1 and POD-2. The mini-mental state examination results indicated that esketamine promoted postoperative cognitive function recovery on POD-1 but had no significant effect on POD-2.
Across these studies, esketamine was administered at varying doses and via different methods during the perioperative period, and all studies reported some degree of improvement in postoperative depression scores and symptoms. However, the duration of postoperative improvement varied among studies when compared with control groups, which could be attributed to the use of different assessment scales across these trials.
In the present study, postoperative serum levels of 5-HT and BDNF were significantly higher in the esketamine group than in the normal saline group. Previous clinical studies have also reported that esketamine increases serum levels of 5-HT and BDNF in postpartum women, as well as in patients with uterine or thyroid cancer.19–21
These findings provide new insights into the potential application of esketamine for alleviating postoperative depression in patients with breast cancer. Specifically, the antidepressant effects of esketamine appear to be associated with increased peripheral biomarkers, such as BDNF and serotonin.22
The analgesic effect of esketamine should not be overlooked. In this study, the postoperative pain scores in the esketamine group were lower than those in the normal saline group (Table 4). Although there were no significant differences between the two groups on postoperative days 1 and 3, the significant pain intensity difference 30 minutes after extubation indicated that esketamine produced an analgesic effect in the early postoperative period. A systematic evaluation covering various surgical procedures, including abdominal, thoracic, and gynecological surgeries, showed that intravenous injection of esketamine as an adjunct to general anesthesia effectively improved analgesia by reducing the pain intensity and the need for opioids in the early postoperative period.23 Koppert et al found that intravenous infusion of esketamine reduced the degree of opioid-induced hyperalgesia.24 Combined with its antidepressant effect, the comprehensive effects of esketamine during the perioperative period significantly improved patient comfort and the overall postoperative experience.
In this study, some patients in the esketamine group experienced adverse reactions, such as tachycardia, nausea, and vomiting. The incidence of postoperative nausea and vomiting (PONV) was higher in the esketamine group than in the normal saline group (10 cases vs 7 cases). However, all cases were transient and resolved within the first postoperative day, with none severe enough to require additional pharmacological intervention. There were no statistically significant differences compared to the normal saline group (Table 5). Ketamine was once a commonly used clinical anesthetic, however, its popularity significantly decreased with the introduction of propofol, inhaled anesthetics, and opioids because the latter drugs have fewer side effects.25 Nevertheless, adding esketamine to general anesthesia to improve postoperative mood has been shown to have low incidences of drug-related side effects due to the relatively low doses used.26 Our study also showed that adding esketamine to general anesthesia did not affect hemodynamics before and after anesthesia induction or the time to awakening and extubation. These findings were consistent with previous research and suggested that esketamine has good tolerability and safety at appropriate doses.25 However, further evaluation of its potential risks in long-term use, especially in high-risk patients, is still needed.
Limitations
Our study had several limitations. First, the study sample size was small, with only 80 patients, and the study focused only on female breast cancer patients. The generalizability of the results requires further validation. Larger, multicenter clinical trials should be conducted to verify the efficacy and safety of esketamine in different types of cancer patients. This study did not explore the optimal drug dosage, and future research should investigate the antidepressant dose-response relationship of esketamine. Second, although this study observed the antidepressant effect of esketamine within 30 days postoperatively, research on its long-term efficacy remains scarce. The long-term antidepressant efficacy and side effects of esketamine, particularly its potential impact on biomarkers associated with antidepressant response, should be a focus of future research.
Conclusion
Perioperative continuous infusion of esketamine effectively reduced postoperative depression scores in patients undergoing breast cancer surgery. Esketamine might exert its antidepressant effects by modulating 5-HT and BDNF levels. Further studies are warranted to verify its long-term efficacy and safety.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the Jianliang Sun and Xinlei Lu upon reasonable request.
Ethics Approval and Consent to Participate
This study was performed in line with the principles of the Declaration of Helsinki and approved by the Medical Ethics Committee of the Affiliated Hangzhou First People’s Hospital, School of Medicine, Westlake University (IIT-20220502-0068-01). The study was registered at the China Clinical Trials Registry (registration number: ChiCTR2200061575; Date of Registration: 2022-06-29). Written informed consent was obtained from all participants, or, when applicable, from their legal representatives.
Acknowledgments
We thank LetPub (www.letpub.com.cn) for linguistic assistance and pre-submission expert review.
Funding
This work was supported by the National Natural Science Foundation General Project (Project Approval Number: 82271445), the Construction Fund of Key Medical Disciplines of Hangzhou (Anesthesia and Pain Medicine OO20200484), and the Zhejiang Provincial Medical and Health Science and Technology Program Youth Innovation Project (No.: 2023RC054).
Disclosure
The authors declare no competing interests.
References
1. Ferlay J, Colombet M, Soerjomataram I, et al. Cancer statistics for the year 2020: an overview. Int J Cancer. 2021;149:778–789. doi:10.1002/ijc.33588
2. Tao X, Li T, Gandomkar Z, Brennan PC, Reed WM. Incidence, mortality, survival, and disease burden of breast cancer in China compared to other developed countries. Asia Pac J Clin Oncol. 2023;19(6):645–654. doi:10.1111/ajco.13958
3. Javan Biparva A, Raoofi S, Rafiei S, et al. Global depression in breast cancer patients: systematic review and meta-analysis. PLoS One. 2023;18(7):e0287372. doi:10.1371/journal.pone.0287372
4. Wang X, Wang N, Zhong L, et al. Prognostic value of depression and anxiety on breast cancer recurrence and mortality: a systematic review and meta-analysis of 282,203 patients. Mol Psychiatry. 2020;25(12):3186–3197. doi:10.1038/s41380-020-00865-6
5. Wilkinson ST, Sanacora G. Considerations on the off-label use of ketamine as a treatment for mood disorders. JAMA. 2017;318(9):793–794. doi:10.1001/jama.2017.10697
6. Sanders B, Brula AQ. Intranasal esketamine: from origins to future implications in treatment-resistant depression. J Psychiatr Res. 2021;137:29–35. doi:10.1016/j.jpsychires.2021.02.020
7. Singh JB, Fedgchin M, Daly E, et al. Intravenous esketamine in adult treatment-resistant depression: a double-blind, double-randomization, placebo-controlled study. Biol Psychiatry. 2016;80(6):424–431. doi:10.1016/j.biopsych.2015.10.018
8. Lepack AE, Fuchikami M, Dwyer JM, Banasr M, Duman RS. BDNF release is required for the behavioral actions of ketamine. Int J Neuropsychopharmacol. 2014;18(1):pyu033. doi:10.1093/ijnp/pyu033
9. Pałucha-Poniewiera A, Podkowa K, Pilc A. Role of AMPA receptor stimulation and TrkB signaling in the antidepressant-like effect of ketamine co-administered with a group II mGlu receptor antagonist, LY341495, in the forced swim test in rats. Behav Pharmacol. 2019;30(6):471–477. doi:10.1097/FBP.0000000000000471
10. Pehrson AL, Roberts D, Khawaja A, McNair R. The role of serotonin neurotransmission in rapid antidepressant actions. Psychopharmacology. 2022;239(6):1823–1838. doi:10.1007/s00213-022-06098-5
11. Molero P, Ramos-Quiroga JA, Martin-Santos R, Calvo-Sánchez E, Gutiérrez-Rojas L, Meana JJ. Antidepressant efficacy and tolerability of ketamine and esketamine: a critical review. CNS Drugs. 2018;32(5):411–420. doi:10.1007/s40263-018-0519-3
12. Paul R, Schaaff N, Padberg F, Möller HJ, Frodl T. Comparison of racemic ketamine and S-ketamine in treatment-resistant major depression: report of two cases. World J Biol Psychiatry. 2009;10(3):241–244. doi:10.1080/15622970701714370
13. Bahr R, Lopez A, Rey JA. Intranasal esketamine (SpravatoTM) for use in treatment-resistant depression in conjunction with an oral antidepressant. Pharm Ther. 2019;44(6):340–375. doi:10.1017/S0033291709006011
14. Xie M, Liang Y, Deng Y, Li T. Effect of S-ketamine on postoperative pain in adults post-abdominal surgery: a systematic review and meta-analysis. Pain Physician. 2023;26(4):327–335. doi:10.36076/ppj.2023.26.327
15. Hung KC, Kao CL, Ho CN, et al. The impact of perioperative ketamine or esketamine on the subjective quality of recovery after surgery: a meta-analysis of randomised controlled trials. Br J Anaesth. 2024;132(6):1293–1303. doi:10.1016/j.bja.2024.03.012
16. Liu P, Li P, Li Q, et al. Effect of pretreatment of S-ketamine on postoperative depression for breast cancer patients. J Invest Surg. 2021;34(8):883–888. doi:10.1080/08941939.2019.1710626
17. Wang H, Te R, Zhang J, et al. Effects of a single subanesthetic dose of esketamine on postoperative subthreshold depressive symptoms in patients undergoing unilateral modified radical mastectomy: a randomised, controlled, double-blind trial. BMC Psychiatry. 2024;24(1):315. doi:10.1186/s12888-024-05753-9
18. Zhang J, Jia D, Li W, Li X, Ma Q, Chen X. General anesthesia with S-ketamine improves the early recovery and cognitive function in patients undergoing modified radical mastectomy: a prospective randomized controlled trial. BMC Anesthesiol. 2023;23(1):214. doi:10.1186/s12871-023-02161-6
19. Jiang Q, Qi Y, Zhou M, et al. Effect of esketamine on serum neurotransmitters in patients with postpartum depression: a randomized controlled trial. BMC Anesthesiol. 2024;24(1):293. doi:10.1186/s12871-024-02681-9
20. Wang J, Wang Y, Xu X, Peng S, Xu F, Liu P. Use of various doses of S-ketamine in treatment of depression and pain in cervical carcinoma patients with mild/moderate depression after laparoscopic total hysterectomy. Med Sci Monit. 2020;26:e922028. doi:10.12659/MSM.922028
21. Bi X, Dai J, Li J. The effect of esketamine on postoperative anxiety and depression in patients with thyroid cancer: a randomized, double-blind, placebo-controlled, parallel-group trial. Medicine. 2025;104(18):e42284. doi:10.1097/MD.0000000000042284
22. Johnston JN, Zarate CA, Kvarta MD. Esketamine in depression: putative biomarkers from clinical research. Eur Arch Psychiatry Clin Neurosci. 2024;275:1559–1572. doi:10.1007/s00406-024-01865-1
23. Wang X, Lin C, Lan L, Liu J. Perioperative intravenous S-ketamine for acute postoperative pain in adults: a systematic review and meta-analysis. J Clin Anesth. 2021;68:110071. doi:10.1016/j.jclinane.2020.110071
24. Koppert W, Sittl R, Scheuber K, Alsheimer M, Schmelz M, Schüttler J. Differential modulation of remifentanil-induced analgesia and postinfusion hyperalgesia by S-ketamine and clonidine in humans. Anesthesiology. 2003;99(1):152–159. doi:10.1097/00000542-200307000-00025
25. Luo T, Deng Z, Ren Q, Mu F, Zhang Y, Wang H. Effects of esketamine on postoperative negative emotions and early cognitive disorders in patients undergoing non-cardiac thoracic surgery: a randomized controlled trial. J Clin Anesth. 2024;95:111447. doi:10.1016/j.jclinane.2024.111447
26. Liu LL, Hu JH, Pan JJ, Liu H, Ji FH, Peng K. An intraoperative sub-anesthetic dose of esketamine on postoperative depressive symptoms in perimenopausal women with breast cancer undergoing modified radical mastectomy: protocol for a randomized, triple-blinded, controlled trial. Int J Gen Med. 2023;16:3373–3381. doi:10.2147/IJGM.S421265
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Predicting Response to Radiotherapy in Breast Cancer-Induced Bone Pain: Relationship Between Pain and Serum Cytokine Expression Levels After Radiotherapy
Lou Y, Cao H, Wang R, Chen Y, Zhang H
Journal of Pain Research 2022, 15:3555-3562
Published Date: 11 November 2022
An Intraoperative Sub-Anesthetic Dose of Esketamine on Postoperative Depressive Symptoms in Perimenopausal Women with Breast Cancer Undergoing Modified Radical Mastectomy: Protocol for a Randomized, Triple-Blinded, Controlled Trial
Liu LL, Hu JH, Pan JJ, Liu H, Ji FH, Peng K
International Journal of General Medicine 2023, 16:3373-3381
Published Date: 8 August 2023
Treatment Modalities for Aromatase Inhibitor-Associated Musculoskeletal Syndrome (AIMSS): A Scoping Review of Prospective Treatment Studies
Bobo JA, Lubrano B, Rosario-Concepcion R, Cuartas-Abril A, Advani P, Chumsri S, Bruce BK
Journal of Pain Research 2025, 18:1853-1889
Published Date: 7 April 2025
Effect of Intraoperative Intravenous Infusion of Esketamine Combined with Dexmedetomidine on Postoperative Sleep Disturbance in Patients Undergoing Radical Mastectomy
Geng X, Pu Y, Hu Z, Zhang H, Wang M, Fang C, Lv G, Li W, Zhang X, Fan X, Liu S, Chen X, Wu J
Drug Design, Development and Therapy 2025, 19:4629-4640
Published Date: 31 May 2025
Effect of Perioperative Subanesthetic Dose of Esketamine on Postoperative Recovery Quality in Patients Undergoing Laparoscopic Gastrointestinal Surgery: A Randomised, Double-Blind, Controlled Trial
Zhang Y, Li S, Wu C, Song L, Hu L, Lu J
Drug Design, Development and Therapy 2025, 19:6637-6646
Published Date: 1 August 2025