Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
The Relationship Between Visceral Fat Obesity and the Atherogenic Combined Index in Patients with Type 2 Diabetes Mellitus
Authors Li Y ![]() , Ma X, Zhao X, Peng Y, Du W, Gao G
, Ma X, Zhao X, Peng Y, Du W, Gao G ![]() , Ji B
, Ji B
Received 19 December 2025
Accepted for publication 2 June 2026
Published 10 July 2026 Volume 2026:19 588794
DOI https://doi.org/10.2147/DMSO.S588794
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Donald McClain
Yaru Li,1,2 Xuan Ma,1,2 Xinbo Zhao,2 Yan Peng,2 Wenhua Du,2 Guanqi Gao,2 Baolan Ji2
1School of Clinical Medicine, Shandong Second Medical University, Weifang, Shandong, 261000, People’s Republic of China; 2Department of Endocrinology, Linyi People’s Hospital, Shandong Second Medical University, Linyi, Shandong, 276034, People’s Republic of China
Correspondence: Baolan Ji, Department of Endocrinology, Linyi People’s Hospital, Shandong Second Medical University, North Side of the Intersection of Wohushan Road and Wuhan Road in Lanshan District, Linyi, Shandong, 276034, People’s Republic of China, Email [email protected]
Purpose: The presence of abdominal obesity, characterized by an accumulation of visceral fat area (VFA), has been identified as a significant risk factor for the development of type 2 diabetes mellitus (T2DM) and its associated complications. Substantial evidence has proven that it’s strongly associated with lipid metabolism. The atherogenic combined index (ACI) is a novel non-traditional lipid index, but there is no clear evidence to explore the relationship with visceral fat obesity (VFO). Our study aimed to interpret this relationship in T2DM.
Methods: In accordance with the research objective, this cross-sectional study retrospectively included 2,323 patients with T2DM from February 2020 to March 2023. The clinical and biochemical data were measured. VFA measurement was conducted at the umbilicus level using a dual bioelectrical impedance analysis. VFO was redefined as VFA ≥ 100 cm2. The formula of ACI was based on triglyceride, non-high-density lipoprotein cholesterol and high-density lipoprotein cholesterol. Patients were categorized into the VFO group and the non-VFO group, which were then further divided according to gender.
Results: The incidence of VFO was found to be higher among males than females. Among participants of both genders, the level of ACI was found to be significantly increased in the VFO group compared with the non-VFO group (both p < 0.001). As the ACI increased, the incidence of VFO increased concomitantly. Univariate correlation analysis revealed a positive correlation between ACI and VFO (correlation coefficient: 0.223, p < 0.001 in females; correlation coefficient: 0.302, p < 0.001 in males). Logistic regression analysis indicated that ACI was associated with VFO independently (OR: 1.797, p = 0.029 in females; OR: 2.501, p < 0.001 in males).
Conclusion: The ACI had been found to be independently correlated with VFO in patients with T2DM in both genders. This finding had the potential to facilitate the monitoring and management of VFO in T2DM.
Keywords: atherogenic combined index, type 2 diabetes mellitus, visceral fat obesity, visceral fat area
Introduction
Obesity represents a considerable public health concern, exhibiting a strong correlation with diabetes and its related complications. In particular, abdominal obesity, characterized by an increased visceral fat area (VFA), plays a critical role in the development and progression of diabetes and its complications.1 The risk of diabetes-related complications is further aggravated in patients with type 2 diabetes mellitus (T2DM), due to excessive visceral fat.2–5 The International Atherosclerosis Society and the International Chair on Cardiometabolic Risk Working Group on Visceral Obesity provide a synopsis of the extant evidence for visceral adiposity as emerging risk factors for T2DM, atherosclerosis and cardiovascular disease, which suggests that public health messages should emphasize visceral fat in addition to excess weight.6 Consequently, ascertaining risk factors associated with increased VFA in patients with T2DM is imperative for enhancing metabolic risk assessment and administration.
It is universally recognized that computed tomography (CT) and magnetic resonance imaging (MRI) are the gold standards for diagnosing VFA,7 but CT is costly and involves ionizing radiation, while MRI is time-consuming. Finding easy indices to use to monitor visceral fat obesity (VFO) is critical. Excess visceral adipose tissue releases large amounts of fatty acids, thereby affecting lipid metabolism.8 Traditional and non-traditional lipid markers have been shown to be closely associated with VFA, such as cholesterol (TC), triglyceride (TG), remnant cholesterol (RC), atherogenic index of plasma (AIP) and others.9,10 This study introduced a novel lipid index, the atherogenic combined index (ACI), calculated from TG, non-high-density lipoprotein cholesterol (non-HDL-c) and HDL-c levels, which capacity to reflect a more comprehensive lipid profile distinguishes it from other lipid indices and emerging evidence from multiple studies supports its potential utility as a biomarker for coronary artery disease (CAD) and metabolic dysfunction-associated steatotic liver disease (MASLD).11,12 Therefore, we speculated that this index may be closely related to VFO. Up to the present, the extant research in this area is limited, and the potential relationships between ACI and VFO have yet to be explored. The objective of this study was to explore the potential correlation between ACI and VFO, with the purpose that ACI may facilitate the early monitoring and management of VFO in patients with T2DM.
However, CT and MRI are not suitable for routine screening, whereas bioelectrical impedance analysis (BIA) represents a more accessible, efficient, and relatively inexpensive approach for VFA assessment and has been recommended as a useful clinical tool for VFA measurement.13,14 Additionally, epidemiological and clinical evidence have confirmed distinct gender-related differences in visceral fat distribution, lipid profiles and cardiovascular disease incidence, with males have a higher prevalence of VFO, reproductive-age females exhibit naturally higher HDL-c levels and sex is significantly associated with cardiovascular disease incidence in patients with T2DM.15–17 Therefore, this study employed a sex-stratified approach to examine the relationship between ACI and VFO, with VFA assessment by BIA.
Methods
Study Participants
This cross-sectional study retrospectively collected data on patients with T2DM who were hospitalized at Linyi People’s Hospital from February 2020 to March 2023. The criteria for inclusion were as follows: (1) A diagnosis of T2DM was made based on the 1999 World Health Organization diagnostic criteria; (2) The age of the subject was 18 years or older. The following exclusion criteria were applied: (1) Type 1 diabetes, acute diabetic conditions, or other particular forms of diabetes; (2) Severe liver dysfunction, defined as a history of liver failure or a current diagnosis, and severe kidney dysfunction; (3) The lack of case data, including patients with missing VFA data and missing data for calculating ACI.
General Conditions and Physical Examinations
The participant’s basic information, including age, sex, height, weight, duration of diabetes mellitus, smoking and alcohol habits, and blood pressure data measured with a standard electronic sphygmomanometer, was obtained from medical records. Body mass index (BMI) was calculated based on weight and height, using the formula BMI = weight (kg) / height (m)2. VFA measurement was conducted at the umbilicus level using a dual BIA (Omron HDS-2000, Kyoto, Japan).18 The VFO was defined as VFA ≥ 100 cm2.
Biochemical Measurements and Indices Calculations
After a full night of fasting, routine blood tests were conducted on patients in the early morning hours, encompassing a comprehensive range of parameters including fasting plasma glucose (FPG), TC, TG, HDL-c, low-density lipoprotein cholesterol (LDL-c), aspartate aminotransferase (AST), alanine aminotransferase (ALT), γ-glutamyl transferase (GGT), serum creatinine (Scr), uric acid (UA) and platelets. Hemoglobin (Hb) was measured utilizing biochemical autoanalyzer (Cobas c 702, Roche, Germany), while glycated hemoglobin (HbA1c) levels were determined employing high-performance liquid chromatography. The calculation formulas for the corresponding lipid indices are outlined below. The indicators of lipid metabolism in this study were expressed in mmol/L. When calculating ACI, the relevant variables were converted from mmol/L to mg/dL according to standard conversion ratios. (1) TG/HDL-c = TG/HDL-c;19 (2)Non-HDL-c = TC − HDL-c;20 (3) AIP = log10 (TG/HDL-c);21 (4) Lipoprotein combine index (LCI) = TC × TG × LDL-c/HDL-c;22 (5) Platelet/HDL-c ratio (PHR) = platelet/HDL-c;23 (6) Castelli’s risk index I (CRI-I) = TC/HDL-c;24 (7) Castelli’s risk index II (CRI-II) = LDL-c/HDL-c;24 (8) RC = TC − HDL-c − LDL-c;25 (9) Atherogenic coefficient (AC) = (TC-HDL-c)/HDL-c;26 (10) ACI = log10 (TG × Non-HDL-c/HDL-c).12
Statistical Analysis
The data were analyzed using SPSS version 25.0 (SPSS Inc., Chicago, IL, USA). Continuous variables that were normally distributed were presented as the mean ± standard deviation (SD), while those that were abnormally distributed were presented as the median and interquartile range. The independent-samples t-test and Mann–Whitney U-test were utilized to conduct a comparative analysis of continuous variables that were distributed normally and abnormally, respectively. The chi-square test was utilized for the purpose of conducting comparisons between categorical variables. For the data of the ACI categorical groups, we used the analysis of variance (ANOVA) to perform multiple comparison tests for normally distributed data and the Kruskal–Wallis test to address the issue of abnormally distributed data. Univariate correlation analysis was performed for selecting the variables with statistical significance. Correlation coefficients and variance inflation factors (VIF) were used to assess multicollinearity between lipid indices. The independent variables related to the VFO were analyzed using binary logistic stepwise forward regression. The statistical significance of the observed findings was determined by a two-tailed P-value cut off of < 0.05.
Results
Baseline Clinical and Biochemical Characteristics
Table 1 presents a comprehensive overview of the clinical characteristics exhibited by the participants in this study. In both male and female groups, compared with the non-VFO group, the following variables were significantly higher (all p < 0.05): BMI, VFA, SFA, SBP, DBP, TG, FPG, ALT, GGT, UA, Scr, TG/HDL-c, Non-HDL-c, AIP, LCI, PHR, CRI-I, CRI-II, RC, Non-HDL/HDL-c, LDL-c/HDL-c, TC/HDL-c, RC/HDL-c, AC and ACI. Furthermore, HDL-c levels were significantly lower in the VFO group (p < 0.001). No statistically significant differences were observed in duration of diabetes, TC, LDL-c and platelets (all p > 0.05). In the male group, the percentage of smoking and drinking, AST and Hb demonstrated a marked increase (all p < 0.05), while age and HbA1c levels were lower in the VFO group (p < 0.05). In the female group, age revealed a marked increase (p = 0.013). Nonetheless, no discernible differences were observed with respect to the percentage of smoking and drinking, HbA1c, AST and Hb in females (all p > 0.05). In addition, according to the ACI levels, the participants were divided into four groups: for males, Q1 (1.53–2.36), Q2 (2.36–2.63), Q3 (2.63–2.89) and Q4 (2.89–3.94); for females, Q1 (1.38–2.32), Q2 (2.32–2.59), Q3 (2.59–2.80) and Q4 (2.80–3.73). Figure 1 shows the change in VFO incidence according to ACI quartiles. Results showed that as the ACI quartile grouping increased, the incidence of VFO in males was 33.1%, 50.2%, 63.1% and 73.1%, while the incidence in females was 16.1%, 22.5%, 35.0% and 42.5%. Additionally, we examined other anthropometric variables, biochemical variables and metabolic indicators, to observe how they changed with increasing ACI quartiles (as shown in Appendix Table 1).
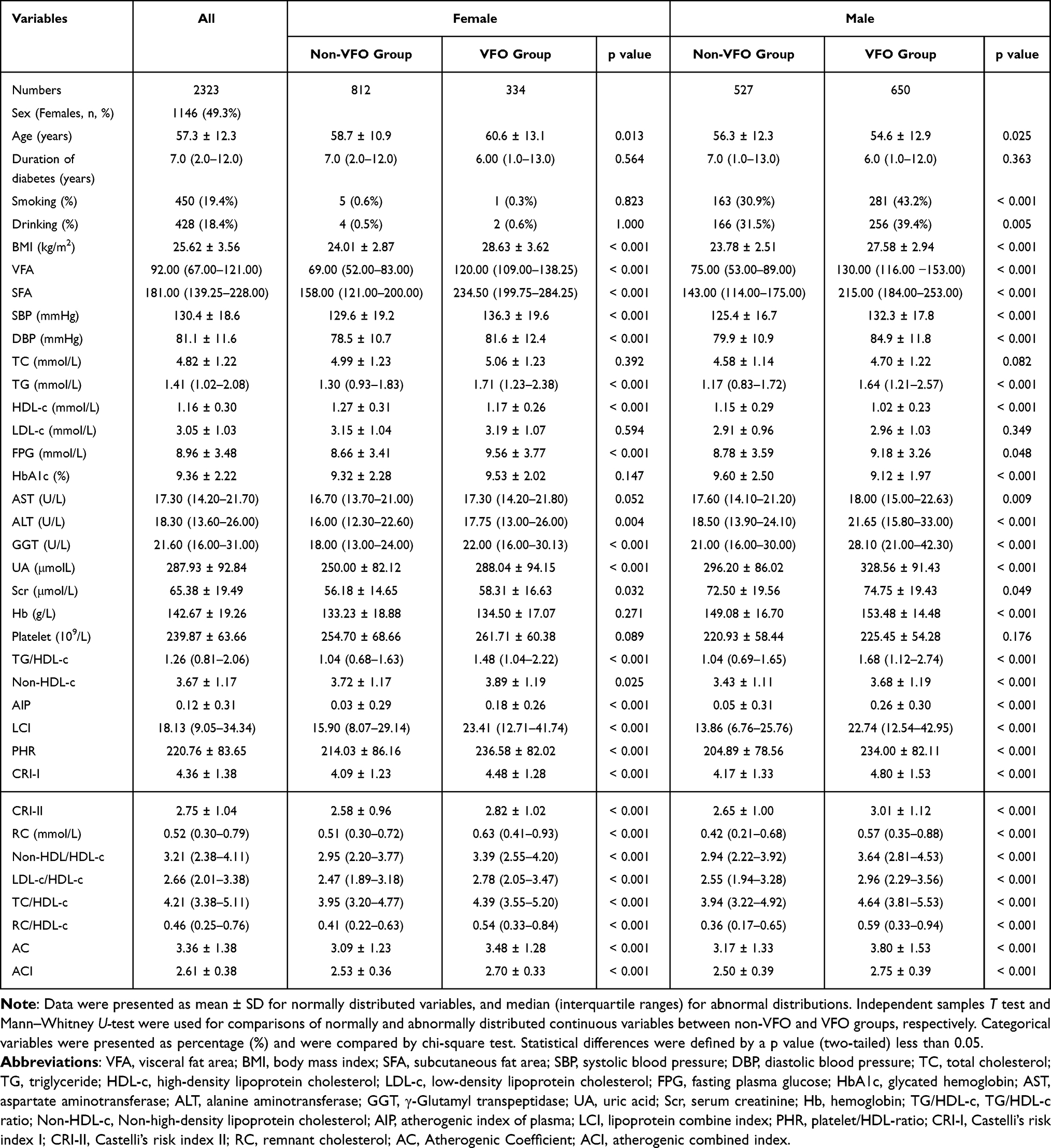 |
Table 1 Clinical and Biochemical Characteristics by Presence of VFO |
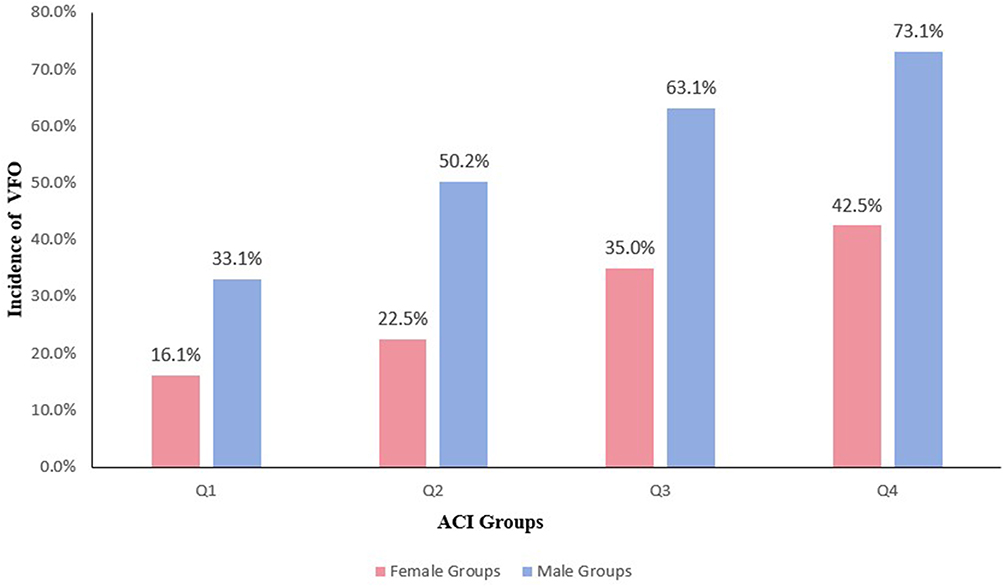 |
Figure 1 The bar chart shows the prevalence of VFO stratified by ACI quartiles. Blue represents male groups, red represents female groups. |
Univariate Analysis
As demonstrated in Table 2, the association between VFO and each variable was assessed employing Spearman correlation analysis. In two groups, the findings indicated a positive correlation between BMI, SFA, SBP, DBP, TG, FPG, ALT, GGT, UA, Hb, TG/HDL-c, Non-HDL-c, AIP, LCI, PHR, CRI-I, CRI-II, RC, Non-HDL/HDL-c, LDL-c/HDL-c, TC/HDL-c, RC/HDL-c, AC and ACI with VFO (all p < 0.05). HDL-c was found to be negatively correlated with VFO (all p < 0.001). Duration of diabetes, TC and LDL-c were found to be non-significantly correlated with VFO (all p > 0.05). In the male group, the findings revealed a positive correlation between the smoking, drinking, AST and Scr with VFO (all p < 0.05). Age and HbA1c levels were found to be negatively correlated with VFO (all p < 0.05). No statistically significant differences were observed with respect to the platelets (p = 0.151) in males. As shown in Figure 2A, the Spearman correlation coefficients between variables in the male group range from −0.5 to 1.0, where 1.0 represents a perfect positive correlation and −0.5 represents a moderately negative correlation. The findings revealed a positive correlation between VFO and age, HbA1c and platelets in the female group (all p < 0.05). Smoking, drinking, AST and Scr were found to be non-significant correlations of VFO in females (all p > 0.05). As demonstrated in Figure 2B, the Spearman correlation coefficients between the variables in the female group range from −0.5 to 1.0, where 1.0 represents a perfect positive correlation and −0.5 represents a moderately negative correlation.
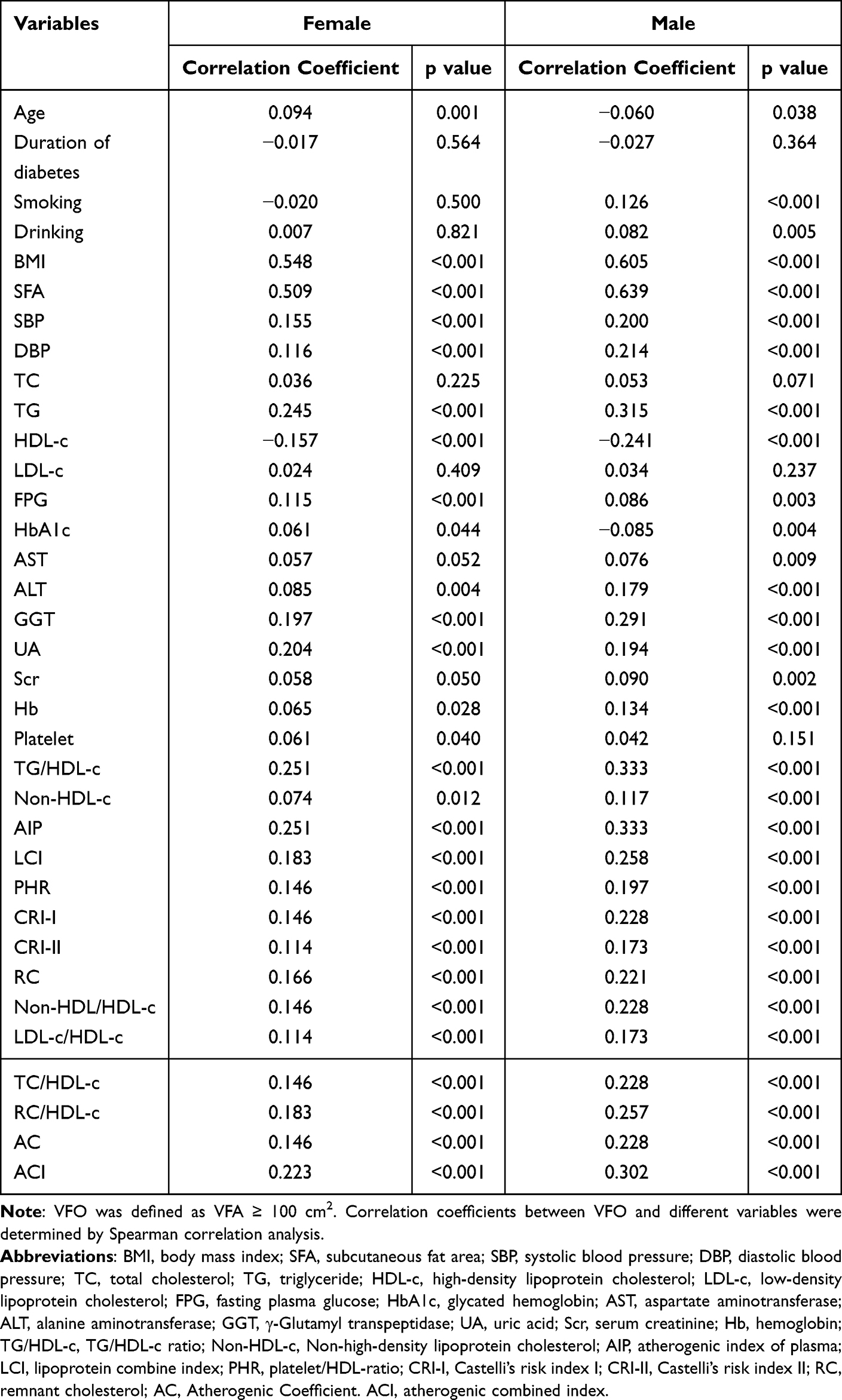 |
Table 2 The Correlation Between VFO and Different Variables by Univariate Analysis |
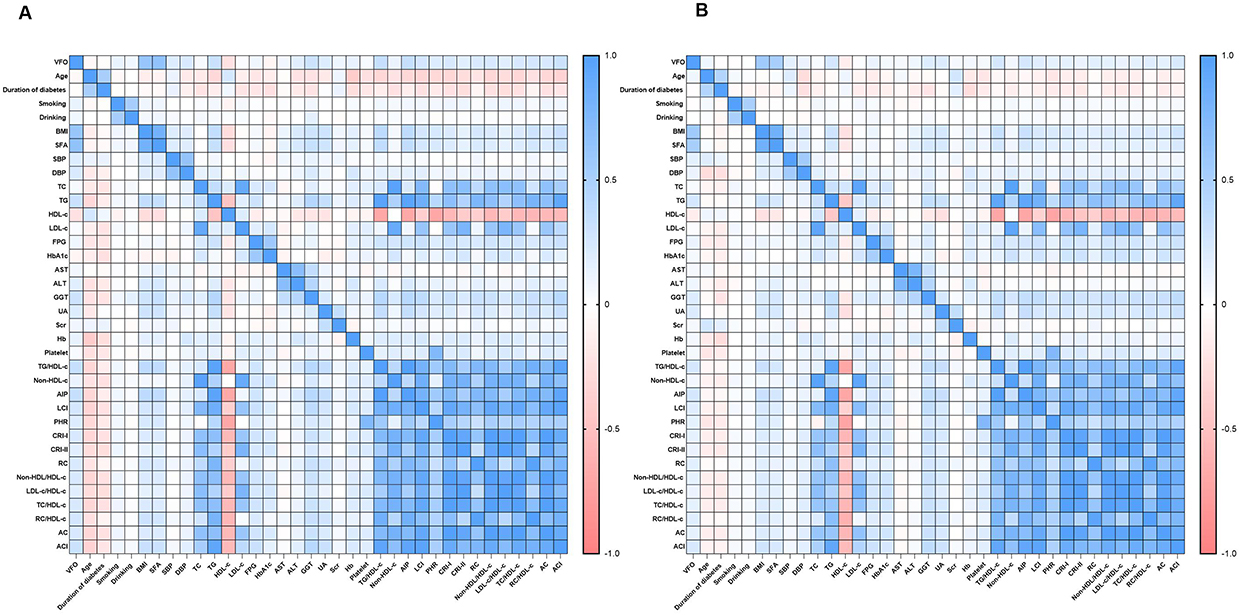 |
Figure 2 The heatmap shows the Spearman correlation coefficients among variables. (A) male groups; (B) female groups. Blue represents a strong positive correlation (close to +1), red represents a strong negative correlation (close to −1), and white indicates a weak or no correlation (close to 0). |
Logistic Regression Analysis
The potential confounding variables initially included in this study were based on literature reports from previous similar studies and clinically verified factors associated with obesity. As mentioned above, variables with statistical significance in the univariate correlation analysis were included in the regression model. VFO was served as the dependent variable (Table 3). In the male group, our study adjusting for age, smoking, drinking, BMI, SFA, SBP, DBP, TG, HDL-c, FPG, HbA1c, AST, ALT, GGT, UA, Scr, Hb, TG/HDL-c, Non-HDL-c, AIP, LCI, PHR, CRI-I, CRI-II, RC, Non-HDL/HDL-c, LDL-c/HDL-c, TC/HDL-c, RC/HDL-c, AC and ACI, the results showed that ACI (OR: 2.501; 95% CI: 1.585–3.946), smoking (OR: 1.745; 95% CI: 1.248–2.439), BMI (OR: 1.278; 95% CI: 1.164–1.404), SFA (OR: 1.025; 95% CI: 1.019–1.030), DBP (OR: 1.025; 95% CI: 1.011–1.041), age (OR: 1.023; 95% CI: 1.008–1.039) and GGT (OR: 1.012; 95% CI: 1.002–1.022) were independently associated with VFO. Figure 3A shows a forest plot of the factors identified by the male group as being independently associated with VFO through logistic regression analysis. In the female group, the following parameters were entered into the logistic regression analysis as independent variables according to the findings of univariate analysis (Table 3): age, BMI, SFA, SBP, DBP, TG, HDL-c, FPG, HbA1c, ALT, GGT, UA, Hb, platelets, TG/HDL-c, Non-HDL-c, AIP, LCI, PHR, CRI-I, CRI-II, RC, Non-HDL/HDL-c, LDL-c/HDL-c, TC/HDL-c, RC/HDL-c, AC and ACI. The results of the study indicated that ACI (OR: 1.797; 95% CI:1.061–3.045), BMI (OR: 1.478; 95% CI 1.356–1.612), FPG (OR: 1.051; 95% CI 1.000–1.104), age (OR: 1.043; 95% CI 1.028–1.060), GGT (OR: 1.016; 95% CI 1.001–1.032) and SFA (OR: 1.005; 95% CI 1.001–1.009) were independently associated with VFO. Figure 3B presents a forest plot of the factors identified by the female group through logistic regression analysis that are independently associated with VFO.
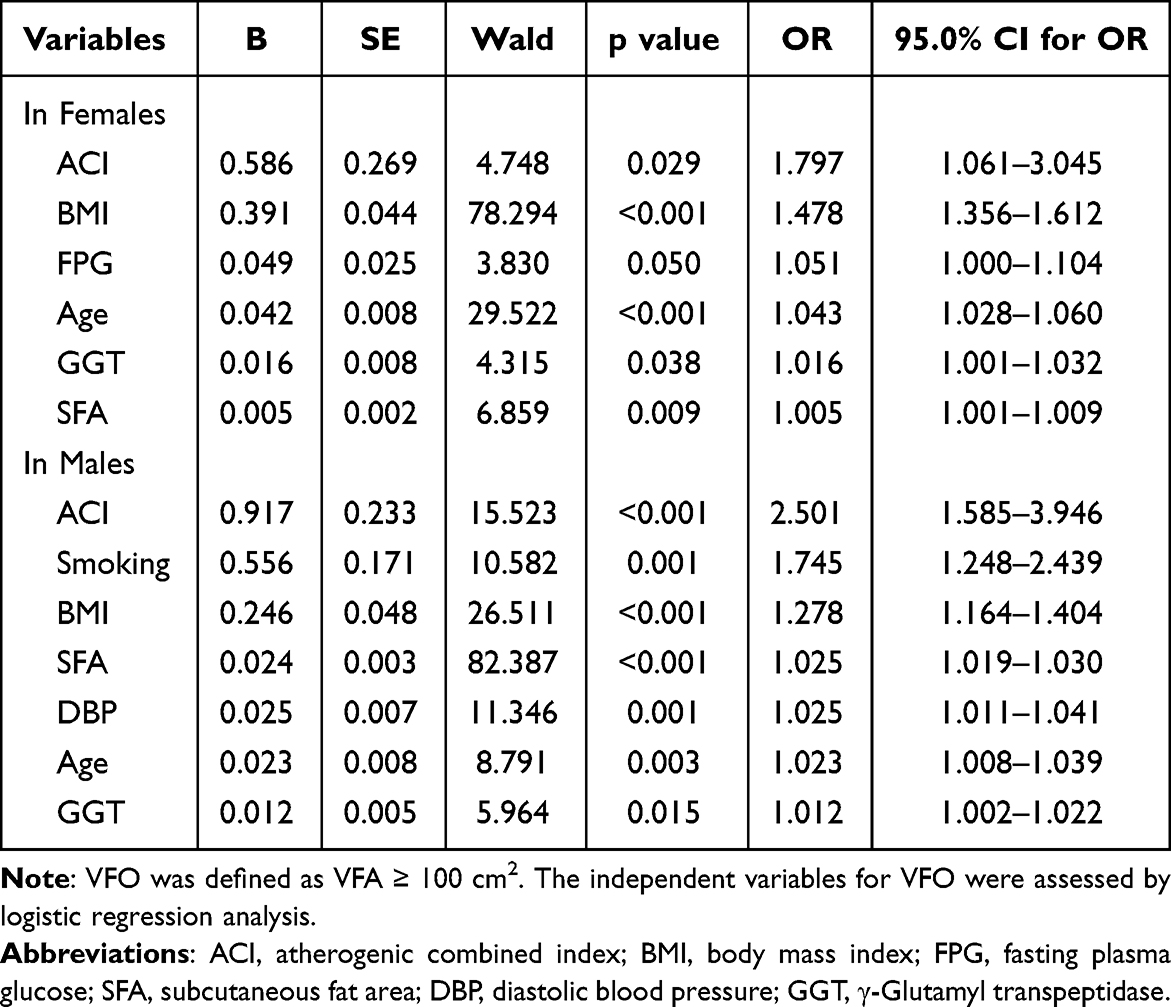 |
Table 3 The Independent Variables for VFO |
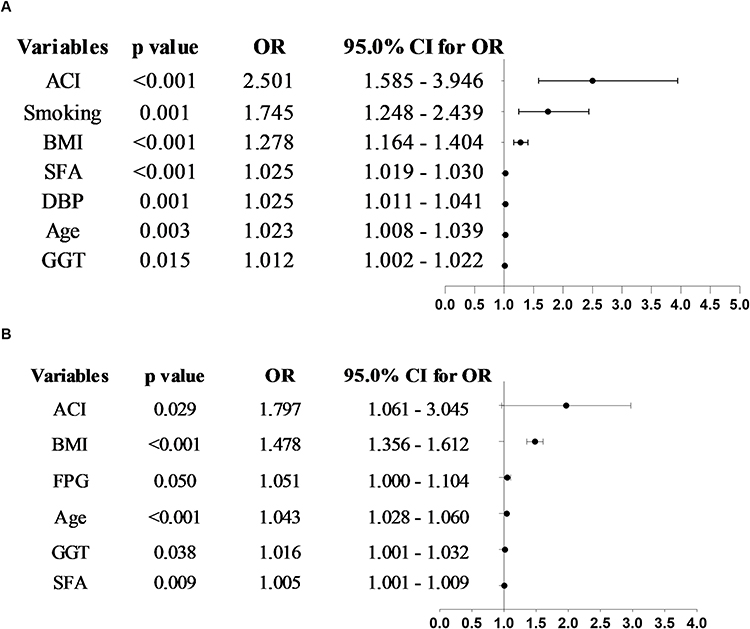 |
Figure 3 Forest plot of factors independently associated with VFO. (A) male groups; (B) female groups. |
Furthermore, it is necessary to point out that due to the similarity of the metrics that comprised the lipid indices, we performed a multicollinearity analysis. We assessed multicollinearity among these variables using correlation coefficients and VIF. The results showed that there was indeed a covariance problem between TG/HDL-c, Non-HDL-c, AIP, LCI, CRI-I, CRI-II, RC, Non-HDL-c/HDL-c, LDL-c/HDL-c, TC/HDL-c, RC/HDL-c, AC and ACI (as shown in Appendix Tables 2–4). Therefore, after adjusting for common confounders, we further analyzed the correlation between each of the above lipid indices and VFO separately, and the results still showed that OR, p-value, Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC) of ACI are superior to other variables (shown in Appendix Tables 5 in males and Appendix Tables 6 in females), which further confirmed the significant correlation between ACI and VFO.
Discussion
This study was designed to explore the relationship between the ACI and VFO in T2DM patients, the core findings perfectly address and achieve this objective. We not only confirmed a significant positive correlation between ACI and VFO, but also identified that ACI had an independent relationship with VFO in both genders, filling the research gap regarding the unclear relationship between this novel non-traditional lipid index and VFO in patients with T2DM.
Visceral fat accumulation is a well-recognized key driver of T2DM progression and its cardiometabolic complications.27 This finding established a novel bridge between lipid atherogenicity and visceral fat metabolism in T2DM. Existing studies have confirmed the value of traditional and non-traditional lipid indices such as TC, TG, RC and AIP and others in predicting VFO.9,10 These results further demonstrated that ACI had a more robust association with VFO, which retained significance in the regression model after adjusting for other lipid indices, enriching the panel of lipid indices for VFO in T2DM. In addition, our previous study illustrated that ACI had independently associated with MASLD in T2DM,11 the current findings form a complementary evidence base for ACI’s clinical value in evaluating metabolic comorbidities (VFO and MASLD) in T2DM.
The present study revealed the association between ACI and VFO previously unobserved. Nevertheless, the potential mechanisms underlying the correlation between the two remain unproven. The ACI was initially proposed as a potential novel index, which synthesizes a more comprehensive lipid profile compared to other indices, including TG, non-HDL-c and HDL-c levels.12 The typical lipid changes observed in obese individuals with VFO are characterized by atherogenic dyslipidaemia, including increased TG and non-HDL-c levels and decreased HDL-c levels.28 Adipocyte dysfunction leads to an influx of lipids into the liver, which in turn causes hypertriglyceridemia by increasing very low-density lipoprotein (VLDL-c) synthesis.29 The non-HDL-c incorporates all plasma lipoproteins, including LDL-c, triglyceride-rich lipoproteins (TRL), TRL remnants, and lipoprotein [Lp(a)].30 Studies have identified a strong correlation between metabolic syndrome, such as obesity and non-HDL-c.31 Obesity triggers a relative deficiency of lipoprotein lipase, a leptin imbalance, and increased hepatic lipase and endothelial lipase activity, which together lead to decreased levels of HDL-c.32 The above rationale supports the correlation between ACI and VFO.
Furthermore, the results of this study demonstrated a strong correlation between obesity indicators (BMI and SFA), age, GGT and VFO in both male and female subjects. Obesity may increase the biological age of certain tissues and cell types, which may be a potential mechanism for the link between age and VFO.33 GGT is a vital indicator of MASLD,34 VFO is closely associated with MASLD,35 this further validated the correlation of GGT in VFO. In the female group, FPG demonstrated a positive correlation with VFO. Chronically elevated lipid levels have been found to disrupt glucose homeostasis, whereas exposure to high glucose has been shown to trigger synergistic glucolipotoxic effects.36 This indicates that heightened blood glucose levels may result in lipid metabolism disorders, which consequently influence visceral fat metabolism. In the male group, smoking and DBP demonstrated a positive correlation with VFO. Study has confirmed that smoking onset and continued smoking may causally increase abdominal adiposity.37 VFO may play a crucial role in activating the sympathetic nervous system and the renin-angiotensin-aldosterone system, resulting in an increased risk of developing hypertension.38 The complex and interrelated nature of VFO’s determinants may underlie this observation.
Limitations
However, it is crucial to acknowledge the limitations of this study. Firstly, due to the intrinsic limitations of cross-sectional studies, it was difficult to determine whether there was a causal relationship between ACI and VFO. Secondly, the collected data were the measurement results for the major patients after administration of glucose-lowering and lipid-lowering drugs, determined by treatment needs and risk assessment. It was not feasible to eliminate the bias caused by these factors. Thirdly, studies have confirmed that the measurement accuracy of BIA is lower than that of CT and MRI.39 And its reliability may be affected by conditions that influence the body’s hydration status, including diabetes.40 Therefore, further gold standard methods are required for verification in the future. Finally, although waist circumference is a very important indicator of abdominal obesity, it was not included in our database. Instead, we included VFA and SFA, which the study indicated were strongly associated with VFO.41 In the future, multicenter, large-scale, longitudinal or interventional studies should be conducted to investigate the relationship between ACI and VFO in T2DM in depth and further explore the cut-off values or risk thresholds.
Conclusion
In summary, among the various lipid parameters, the unconventional lipid parameter ACI was independently associated with the occurrence of VFO in patients with T2DM. In view of the crucial function of VFO in the development of T2DM and CAD, the independent association of ACI may render it a prospective target for early intervention and management.
Data Sharing Statement
The raw data supporting the conclusions of this article will be made available by the corresponding author, without undue reservation.
Ethics Approval and Consent to Participate
The study was undertaken in accordance with the Declaration of Helsinki and was ratified by the Ethics Committee of Linyi People’s Hospital (approval number: 202404-H-018, approval date: April 2024). The studies were undertaken in compliance with the local legislation and institutional requirements. All participants provided written informed consent prior to enrolment.
Author Contributions
YL: Conceptualization, Formal analysis, Writing– original draft, Data curation. XM: Writing– original draft, Formal analysis. XZ: Writing– original draft, Methodology. YP: Writing– review & editing, Resource, Conceptualization, Software. WD: Writing – review & editing, Conceptualization, Software. GG: Writing – review & editing, Formal Analysis, Supervision. BJ: Writing – review & editing, Visualization, Resources, Project administration, Validation, Funding acquisition, Supervision.
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by grants from the Key Research and Development Program of Linyi City (2024YX004).
Disclosure
The authors declare no competing interests in this study.
References
1. Takanari J, Misu M, Goto K, et al. Effects of Oligonol(®) supplementation on abdominal fat in japanese overweight volunteers: a randomized, double-blind, placebo-controlled, parallel group study. J Nutr Sci Vitaminol. 2025;71(4):357–12. doi:10.3177/jnsv.71.357
2. Wu QW, He YH, Li PH, et al. Exploring the link between visceral fat and cardiovascular disease in type 2 diabetes: evidence from ct measurements. Front Endocrinol. 2025;16:1635282. doi:10.3389/fendo.2025.1635282
3. Zhao P, Li Q, Du T, Zhou Q. Association of different obesity indexes with diabetic kidney disease in patients with type 2 diabetes mellitus: a cross-sectional study. Sci Rep. 2024;14(1):21571. doi:10.1038/s41598-024-73106-3
4. Sun L, Zhang X, Yang J, Yuan J, Lei X. Lower visceral fat is related to diabetic peripheral neuropathy. Diabetes Metab Syndr Obes. 2024;17:2967–2974. doi:10.2147/dmso.S471715
5. Hua S, Yao D, Wu S, Chen M, Li L, Li B. Association between visceral fat area and diabetic retinopathy among people with type 2 diabetes mellitus: a cross-sectional study in Ningbo, Zhejiang Province, China. Front Med Lausanne. 2024;11:1327805. doi:10.3389/fmed.2024.1327805
6. Neeland IJ, Ross R, Després JP, et al. Visceral and ectopic fat, atherosclerosis, and cardiometabolic disease: a position statement. Lancet Diabetes Endocrinol. 2019;7(9):715–725. doi:10.1016/s2213-8587(19)30084-1
7. Fang H, Berg E, Cheng X, Shen W. How to best assess abdominal obesity. Curr Opin Clin Nutr Metab Care. 2018;21(5):360–365. doi:10.1097/mco.0000000000000485
8. Luo J, Wang Y, Mao J, et al. Features, functions, and associated diseases of visceral and ectopic fat: a comprehensive review. Obesity. 2025;33(5):825–838. doi:10.1002/oby.24239
9. Raghu Teja K, Durgaprasad BK, Vijayalakshmi P. Evaluation and comparative correlation of abdominal fat related parameters in obese and non-obese groups using computed tomography. Curr Med Imaging. 2021;17(3):417–424. doi:10.2174/1573405616666201008145801
10. Ma X, Jiang X, Gao G, et al. Association of conventional and unconventional lipid profiles with visceral fat area in overweight/obese individuals with type 2 diabetes mellitus. Diabetes Metab Syndr Obes. 2025;18:1025–1034. doi:10.2147/dmso.S506490
11. Sheng J, Shi S, Ma X, Zhao H, Gao G, Ji B. Atherogenic combined index is independently associated with masld in type 2 diabetes: a cross-sectional study. Diabetes Metab Syndr Obes. 2025;18:3041–3052. doi:10.2147/dmso.S523139
12. Toprak K, Kaplangöray M, Karataş M, et al. Atherogenic combined index: validation of a coronary artery disease predictive biomarker. Arch Med Res. 2024;55(7):103065. doi:10.1016/j.arcmed.2024.103065
13. Qin Q, Yang Y, Chen J, et al. Bioelectrical impedance analysis versus quantitative computer tomography and anthropometry for the assessment of body composition parameters in China. Sci Rep. 2021;11(1):11076. doi:10.1038/s41598-021-90641-5
14. Dastidar SG, Gargari P, Das D, Chowdhury S. Comparison of bioelectrical impedance analyser (bia) with dual-energy x-ray absorptiometry (dxa) scan in assessing the body composition of adult individuals with type 2 diabetes mellitus. Indian J Endocrinol Metab. 2024;28(5):510–516. doi:10.4103/ijem.ijem_350_23
15. Rodrigues IG, Arcoverde G, Do Nascimento CLC, et al. Sex-specific differences in visceral and subcutaneous adiposity accumulation and their association with metabolic abnormalities. J Obes. 2025;2025:7240063. doi:10.1155/jobe/7240063
16. Kelly RK, Harris K, Muntner P, Woodward M. Variations in sex differences in major cardiometabolic risk factors by age and menopause status: results from the UK Biobank. Open Heart. 2025;12(1). doi:10.1136/openhrt-2025-003182
17. Gisinger T, He JH, Oyeka CP, et al. Sex hormones and cardiovascular risk in type 2 diabetes: cohort study of the look ahead trial. Diabetes Care. 2026;49(3):497–501. doi:10.2337/dc25-2465
18. Cai N, Chen M, Feng P, et al. Relationships between obesity and prevalence of gout in patients with type 2 diabetes mellitus: a cross-sectional population-based study. BMC Endocr Disord. 2024;24(1):137. doi:10.1186/s12902-024-01672-8
19. Baneu P, Văcărescu C, Drăgan SR, et al. The triglyceride/hdl ratio as a surrogate biomarker for insulin resistance. Biomedicines. 2024;12(7). doi:10.3390/biomedicines12071493
20. Romaszko J, Gromadziński L, Buciński A. Friedewald formula may be used to calculate non-HDL-C from LDL-C and TG. Front Med Lausanne. 2023;10:1247126. doi:10.3389/fmed.2023.1247126
21. Min Q, Wu Z, Yao J, et al. Association between atherogenic index of plasma control level and incident cardiovascular disease in middle-aged and elderly Chinese individuals with abnormal glucose metabolism. Cardiovasc Diabetol. 2024;23(1):54. doi:10.1186/s12933-024-02144-y
22. Wu W, Wu D, Cao C, et al. Lipoprotein combine index is associated with non-alcoholic fatty liver disease: a 5-year longitudinal cohort study in non-obese Chinese populations with normal lipids. Front Med. 2025;12:1618576. doi:10.3389/fmed.2025.1618576
23. Jia S, Ye X, Kong Y, Wang Z, Wu J. Association of high-density lipoprotein cholesterol-based inflammatory markers with masld and significant liver fibrosis in us adults: insights from NHANES 2017-2020. Clin Transl Gastroenterol. 2025;16(8):e00873. doi:10.14309/ctg.0000000000000873
24. Igharo OG, Akinfenwa Y, Isara AR, et al. Lipid profile and atherogenic indices in nigerians occupationally exposed to e-waste: a cardiovascular risk assessment study. Maedica. 2020;15(2):196–205. doi:10.26574/maedica.2020.15.2.196
25. Sandesara PB, Virani SS, Fazio S, Shapiro MD. The forgotten lipids: triglycerides, remnant cholesterol, and atherosclerotic cardiovascular disease risk. Endocr Rev. 2019;40(2):537–557. doi:10.1210/er.2018-00184
26. Assani MZ, Novac MB, Dijmărescu AL, et al. Potential association between atherogenic coefficient, prognostic nutritional index, and various obesity indices in diabetic nephropathy. Nutrients. 2025;17(8). doi:10.3390/nu17081339
27. Jin J, Lei Y, Zheng J, et al. Visceral fat area loss reduces 10-year atherosclerotic cardiovascular disease risk in Chinese population with type 2 diabetes mellitus: a prospective cohort study. Lipids Health Dis. 2025;24(1):308. doi:10.1186/s12944-025-02711-6
28. Nussbaumerova B, Rosolova H. Obesity and Dyslipidemia. Curr Atheroscler Rep. 2023;25(12):947–955. doi:10.1007/s11883-023-01167-2
29. Bays HE, Kirkpatrick CF, Maki KC, et al. Obesity, dyslipidemia, and cardiovascular disease: a joint expert review from the obesity medicine association and the national lipid association 2024. J Clin Lipidol. 2024;18(3):e320–e350. doi:10.1016/j.jacl.2024.04.001
30. Raja V, Aguiar C, Alsayed N, et al. Non-HDL-cholesterol in dyslipidemia: review of the state-of-the-art literature and outlook. Atherosclerosis. 2023;383:117312. doi:10.1016/j.atherosclerosis.2023.117312
31. Mardi P, Abdi F, Ehsani A, et al. Is non-high-density lipoprotein associated with metabolic syndrome? A systematic review and meta-analysis. Front Endocrinol. 2022;13:957136. doi:10.3389/fendo.2022.957136
32. Stadler JT, Marsche G. Obesity-related changes in high-density lipoprotein metabolism and function. Int J Mol Sci. 2020;21(23). doi:10.3390/ijms21238985
33. Tsao YC, Chen JY, Yeh WC, Li WC. Gender- and age-specific associations between visceral obesity and renal function impairment. Obes Facts. 2019;12(1):67–77. doi:10.1159/000496626
34. Wang SW, Wang C, Cheng YM, Hsieh TH, Wang CC, Kao JH. Liver and atherosclerotic risk of alcohol consumption in patients with metabolic dysfunction-associated Steatotic Liver Disease. Atherosclerosis. 2025;403:119161. doi:10.1016/j.atherosclerosis.2025.119161
35. Liu C, Li N, Sheng D, et al. Increased visceral fat area to skeletal muscle mass ratio is positively associated with the risk of metabolic dysfunction-associated steatotic liver disease in a Chinese population. Lipids Health Dis. 2024;23(1):104. doi:10.1186/s12944-024-02100-5
36. Lytrivi M, Castell AL, Poitout V, Cnop M. Recent Insights Into Mechanisms of β-Cell Lipo- and Glucolipotoxicity in Type 2 Diabetes. J Mol Biol. 2020;432(5):1514–1534. doi:10.1016/j.jmb.2019.09.016
37. Carrasquilla GD, García-Ureña M, Romero-Lado MJ, Kilpeläinen TO. Estimating causality between smoking and abdominal obesity by Mendelian randomization. Addiction. 2024;119(6):1024–1034. doi:10.1111/add.16454
38. Tałałaj M, Bogołowska-Stieblich A, Wąsowski M, Sawicka A, Jankowski P. The influence of body composition and fat distribution on circadian blood pressure rhythm and nocturnal mean arterial pressure dipping in patients with obesity. PLoS One. 2023;18(1):e0281151. doi:10.1371/journal.pone.0281151
39. Thomas DM, Crofford I, Scudder J, Oletti B, Deb A, Heymsfield SB. Updates on methods for body composition analysis: implications for clinical practice. Curr Obes Rep. 14(1):8. doi:10.1007/s13679-024-00593-w
40. Castillo Castro C, González Arellanes R, Camacho Mondragón CG, et al. Agreement between bioelectrical impedance analysis and dual-energy x-ray absorptiometry to estimate fat mass in hispanic adults with type 2 diabetes mellitus: a cross-sectional study. Clin Med Insights Endocrinol Diabetes. 2024;17:11795514241274691. doi:10.1177/11795514241274691
41. Xu Z, Liu Y, Yan C, et al. Measurement of visceral fat and abdominal obesity by single-frequency bioelectrical impedance and CT: a cross-sectional study. BMJ Open. 2021;11(10):e048221. doi:10.1136/bmjopen-2020-048221
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Visceral Fat Obesity Correlates with Frailty in Middle-Aged and Older Adults
Li B, Li Y, Zhang Y, Liu P, Song Y, Zhou Y, Ma L
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2877-2884
Published Date: 19 September 2022
Association Between Coronary Artery Calcium Score and Bone Mineral Density in Type 2 Diabetes Mellitus with Different Visceral Fat Area
Yang Y, Li L, Zhang Y, Yang H, Bai J, Lv H, Fu S
Diabetes, Metabolic Syndrome and Obesity 2022, 15:3949-3960
Published Date: 16 December 2022
Association of Conventional and Unconventional Lipid Profiles with Visceral Fat Area in Overweight/Obese Individuals with Type 2 Diabetes Mellitus
Ma X, Jiang X, Gao G, Ban B, Sheng J, Shi S, Zhao H, Ji B
Diabetes, Metabolic Syndrome and Obesity 2025, 18:1025-1034
Published Date: 4 April 2025
J-Shaped Relationship Between Visceral Fat Area and Large-Nerve Fiber Dysfunction Estimated by Vibration Perception Threshold in Type 2 Diabetes: A Cross-Sectional Study
Tang D, Gu X, Xuan Y, Liu Q, Lu L
Diabetes, Metabolic Syndrome and Obesity 2025, 18:2935-2943
Published Date: 20 August 2025
Quantitative CT Assessment of Skeletal Muscle and Abdominal Fat Distribution: Predictive Value for Type 2 Diabetes Mellitus
Zhang B, Wu Z, Jiang C, Li N, An X, Tian L, Cai Y, Zou Y, Tang Y
Diabetes, Metabolic Syndrome and Obesity 2025, 18:4153-4163
Published Date: 11 November 2025