Back to Journals » Patient Preference and Adherence » Volume 19
The Relationship Between Demoralisation, Medical Coping Style, Resilience and Perceived Social Support in Patients with Colorectal Cancer
Authors Li Y, Liu Z, Lu X, Chai X, Bai N, Chen Y
Received 18 April 2025
Accepted for publication 30 September 2025
Published 22 October 2025 Volume 2025:19 Pages 3285—3294
DOI https://doi.org/10.2147/PPA.S535288
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ramón Morillo-Verdugo
Yunyun Li,1,2 Zhimin Liu,1,2 Xingyao Lu,1,2 Xiaoying Chai,3 Ning Bai,3 Ying Chen4
1Affiliated Hospital of Jiangnan University, Wuxi, Jiangsu, People’s Republic of China; 2Jiangnan University, Wuxi, Jiangsu, People’s Republic of China; 3Endocrine Department, Affiliated Hospital of Jiangnan University, Wuxi, Jiangsu, People’s Republic of China; 4Oncology Department, Affiliated Hospital of Jiangnan University, Wuxi, Jiangsu, People’s Republic of China
Correspondence: Ning Bai, Endocrine Department, Affiliated Hospital of Jiangnan University, 1000 Hefeng Road, Binhu District, Wuxi, Jiangsu, 214000, People’s Republic of China, Tel +86 18762692562, Email [email protected] Ying Chen, Oncology Department, Affiliated Hospital of Jiangnan University, 1000 Hefeng Road, Binhu District, Wuxi, Jiangsu, 214000, People’s Republic of China, Tel +86 18762692562, Email [email protected]
Objective: To explore the severity of demoralisation in patients with colorectal cancer (CRC) and its relationship with medical coping style, psychological resilience and perceived social support.
Methods: This cross-sectional study sequentially recruited a total of 253 patients with CRC between August 2023 and April 2024. Socio-demographic and clinical information were collected using a survey. The Demoralisation Scale II (DS-II) was used to assess demoralisation, and results from a Chinese version of the medical coping style questionnaire, a perceived social support scale and a simplified psychological resilience scale were collected. Pearson correlation and multiple linear regression analyses were performed to analyse the relationship between demoralisation and other variables.
Results: The mean score of the DS-II was 11.71 ± 6.32, with 40.7%, 44.3% and 15% of patients with CRC exhibiting low, moderate and high levels of demoralisation, respectively. Demoralisation was significantly correlated with gender, education level, marital status, occupation, family residence, family per capita monthly income, health insurance type, presence of a caregiver, past medical history, number of chronic diseases, length of hospitalisation, number of hospitalisations, disease stage, metastasis and presence of an enterostomy (p < 0.05). Multiple linear regression analysis indicated that metastasis, medical coping style, social support and psychological resilience were independent risk factors significantly associated with demoralisation in patients with CRC (adjusted R2 = 0.801; p < 0.05).
Conclusion: Demoralisation is associated with medical coping style, social support and psychological resilience in patients with CRC. Early and regular monitoring using specially designed and effective tools is essential. This innovative study combines demoralization with coping, support, and resilience to reveal its profound impact on nursing practice and enhance the quality of patient care.
Keywords: colorectal cancer, medical coping style, social support, psychological resilience, demoralisation scale
Introduction
Colorectal cancer (CRC) is a globally prevalent malignancy with a rising incidence. China has the highest annual rates of new cases and CRC-related deaths.1 While advances in early detection and treatment have reduced CRC incidence and mortality in developed countries, there has been a notable increase in early-onset CRC cases in recent years. As gastrointestinal tumours progress and physical function declines, patients often experience anxiety, depression, fear and a sense of meaninglessness, which contribute to demoralisation.2 Psychological stress faced by patients with CRC stems from negative cultural perceptions of cancer, family care expectations, uneven medical resources and inadequate social support. These factors lead to negative coping styles, weakened resilience and feelings of isolation, which, in turn, trigger demoralisation.
Demoralisation is a psychological state characterised by an inability to adapt to prolonged stress or disease, leading to feelings of hopelessness, despair and, occasionally, suicidal tendencies.3,4 It is important to distinguish demoralisation from depression. The core symptom of depression is pleasure deficit, with a decrease in the ability to experience happiness. It is often manifested as a persistent state of depression, with changes in cognitive function, mood, physical movement and mental aspects.5 However, demoralisation is often related to long-term serious illness or coping difficulties in its advanced stages, and it significantly differs from depression.6 Ignatius et al investigated 922 patients and found that some patients suffered from demoralisation but did not experience depression.7 Overall, the diagnosis of demoralisation is more critical than that of depression.
With advancements in research, demoralisation has transitioned from a physical and mental variable to a diagnosable framework.8 It is now recognised as a psychological indicator and is included in the Diagnostic and Statistical Manual of Mental Disorders as a mental behavioural symptom.9 Numerous studies have been conducted to assess the factors associated with demoralisation, including demographic characteristics and physical, mental and psychosocial factors;10–13 however, the results of this study were limited by the small number of patients examined. Furthermore, the current status of demoralisation in patients with CRC and its relationship with other experiences remain unexplored in mainland China. Hence, our study analyses the factors influencing demoralisation in patients with CRC and explores its relationship with medical coping style, social support and psychological resilience.
Materials and Methods
Participants
The cross-sectional study was conducted from August 2023 to April 2024 at the Affiliated Hospital of Jiangnan University. Convenience sampling method was used in this study because it is more efficient in terms of time and cost, and because it is able to address the specific situation of patients with colorectal cancer, collect relevant data quickly, and facilitate the analysis of the relationship between variables. Patients with colorectal cancer were recruited through hospital oncology departments, community health centers, and patient groups, with emphasis on research assistance, confidentiality, voluntary participation, and necessary support. The inclusion criteria were as follows: (1) patients aged >18 y; (2) those with CRC confirmed by pathological examination; (3) patients with no cognitive impairment and the ability to understand the research questionnaire; and (4) those who had given their informed consent and voluntary participation. Patients were excluded if they had obvious cognitive deficits, a history of mental illness or hearing impairments. Out of 260 eligible patients, 253 (97.3%) completed the study, while seven withdrew for various reasons (including loss of interest). The study was approved by the ethics committee of our hospital.
Data Collection
A face-to-face questionnaire was administered to participants using standardised, consistent explanatory language. The participants completed the questionnaire independently; however, for those with dyslexia, the researcher provided explanations for each item and assisted with survey completion. Data were collected using a general information questionnaire, the Demoralisation Scale II (DS-II), the Medical Coping Modes Questionnaire (MCMQ), a Chinese version of the Perceived Social Support Scale (C-PSSS) and the 10-Item Connor–Davidson Resilience Scale (CD-RISC-10).
The general information questionnaire included demographic information and clinical characteristics, including age, gender, education and occupation, number of hospitalizations, duration of hospitalization (divided into 4 groups according to the length of hospitalization: 1–6 months, 7–12 months, 13–24 months, > 24 months), and was completed independently by the patients; the medical history, tumor stage, treatment modality, and the presence or absence of metastasis were collected from the clinical records.
This study employed the simplified Chinese version of the Demoralization Scale-II (DS-II) to assess the level of demoralization in patients with colorectal cancer. The scale was originally developed by Robinson et al to evaluate psychological states such as hopelessness, helplessness, and loss of meaning in patients with severe illnesses.14 The Chinese version of the DS-II was cross-culturally adapted by the research team through a standardized process, including forward translation, synthesis, back-translation, expert committee review, and pre-testing. The wording of some items was simplified to improve patient compliance and comprehension during completion, making it more suitable for psychological assessment in Chinese cancer patient populations. The scale was adapted from the DS-II by simplifying certain items and enhancing patient-reported compliance, making it more suitable for psychological assessment in populations with cancer. The DS-II contains a total of 16 items divided into two dimensions: (I) “meaning and purpose” and (II) “distress and coping ability”. Each item was scored along a Likert 3-level ranking (0 = “never”; 1 = “occasionally”; and 2 = “often”), with scores ranging from 0 to 32 points. A total score of <9 points represented a mild loss of mind, a score of 10–19 was classified as a moderate loss of mind and a score of >20 indicated a severe loss of mind. The Chinese version of the DS-II demonstrated good internal consistency in our Chinese, with a Cronbach’s α coefficient of 0.877.15
The MCMQ was used to measure the coping styles of patients and is commonly used to assess a patient’s medical coping style with respect to a specific disease.16 The MCMQ has three subscales: facing, avoidance and submission with test–retest reliability of 0.64, 0.85 and 0.67, respectively.
The PSSS, originally compiled by Dahlem,17 was used to assess the level of social support perceived by individuals and can directly reflect the support they experience. The C-PSSS was translated by Jiang Qianjin, and the Cronbach’s α coefficient of this scale was 0.93, demonstrating satisfactory reliability.
The CD-RISC-10 was used to assess patient resilience and provided a rapid assessment of this trait.18 The scale includes 10 items, each scored on a 5-point Likert scale (0 = “almost never”; 1 = “rarely”; 2 = “sometimes”; 3 = “often” and 4 = “always”), for a total score range of 0–40. A higher total score indicates a higher level of psychological resilience.
Statistical Analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences software version 25 (SPSS Inc., Chicago, IL, USA). A t-test was used for inter-group comparisons, whereas a one-way analysis of variance was employed for multigroup comparisons. Pearson correlation analysis was used for correlations between different variables. Variables with significant differences were included as independent variables in a multiple linear regression analysis using a forward stepwise process. All p-values were two-tailed, with p < 0.05 indicating a statistically significant difference.
Quality Control
Uniform training was provided to investigators to ensure survey consistency, questionnaires were anonymised to increase credibility, two-person data entry and verification were used to reduce errors, on-site supervision was implemented to ensure questionnaire quality and standard statistical methods were used to analyse data to ensure analytical accuracy. Together, these measures safeguarded the scientific nature of the study and the validity of the data.
Results
Current Status of Demoralisation in Patients with Colorectal Cancer
The overall demoralisation score was 11.71 ± 6.32, with a “meaning and purpose” score of 5.71 ± 2.91 and a “distress and coping ability” score of 6.08 ± 3.80 (Table 1). In terms of demoralisation severity, 40.7% of patients exhibited mild demoralisation (5.39 ± 1.81), 44.3% showed moderate demoralisation (14.08 ± 2.87) and 15.0% experienced severe demoralisation (21.87 ± 1.93).
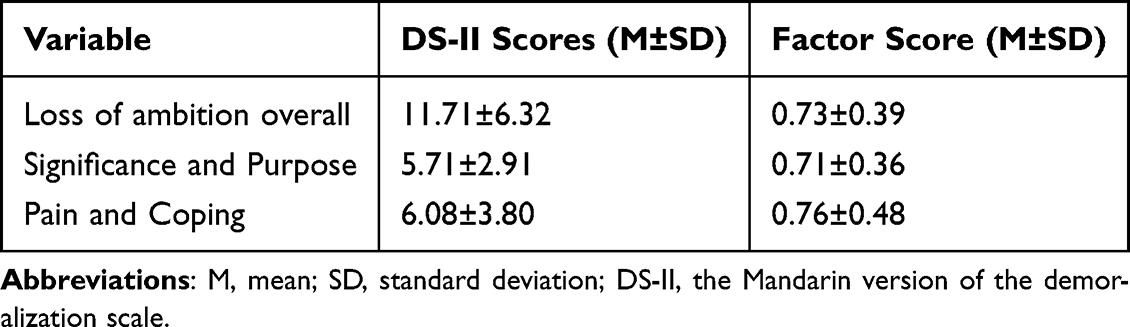 |
Table 1 The Demoralization Scale (DS-II) Scores (N = 253) |
Univariate and Correlation Analyses
In this study, the demoralisation status of patients with CRC was analysed in relation to demographic and disease-related data. The results indicated that demoralisation scores were significantly influenced by factors such as gender, education level, marital status, occupation, family residence, family per capita monthly income, type of health insurance, presence of a caregiver, past medical history, number of chronic diseases, length of hospitalisation, number of hospitalisations, disease stage, presence of an enterostomy, and metastasis (p < 0.05). However, there was no statistically significant difference in demoralisation scores with respect to age, cancer site or treatment modality (p > 0.05) (Table 2). A correlation analysis revealed that DS-II scores were significantly positively correlated with yielding and avoiding medical coping styles and significantly negatively correlated with the facing medical coping style. Additionally, DS-II scores were significantly negatively correlated with scores on the C-PSSS and CD-RISC-10, as shown in Table 3. This suggests that sociodemographic and illness factors significantly influence morale, negative coping is associated with low morale, and social support and psychological resilience contribute to morale.
 |
Table 2 Comparison of the DS-Total Among Groups with Different Demographic Characteristics and Clinical Features (N = 253) |
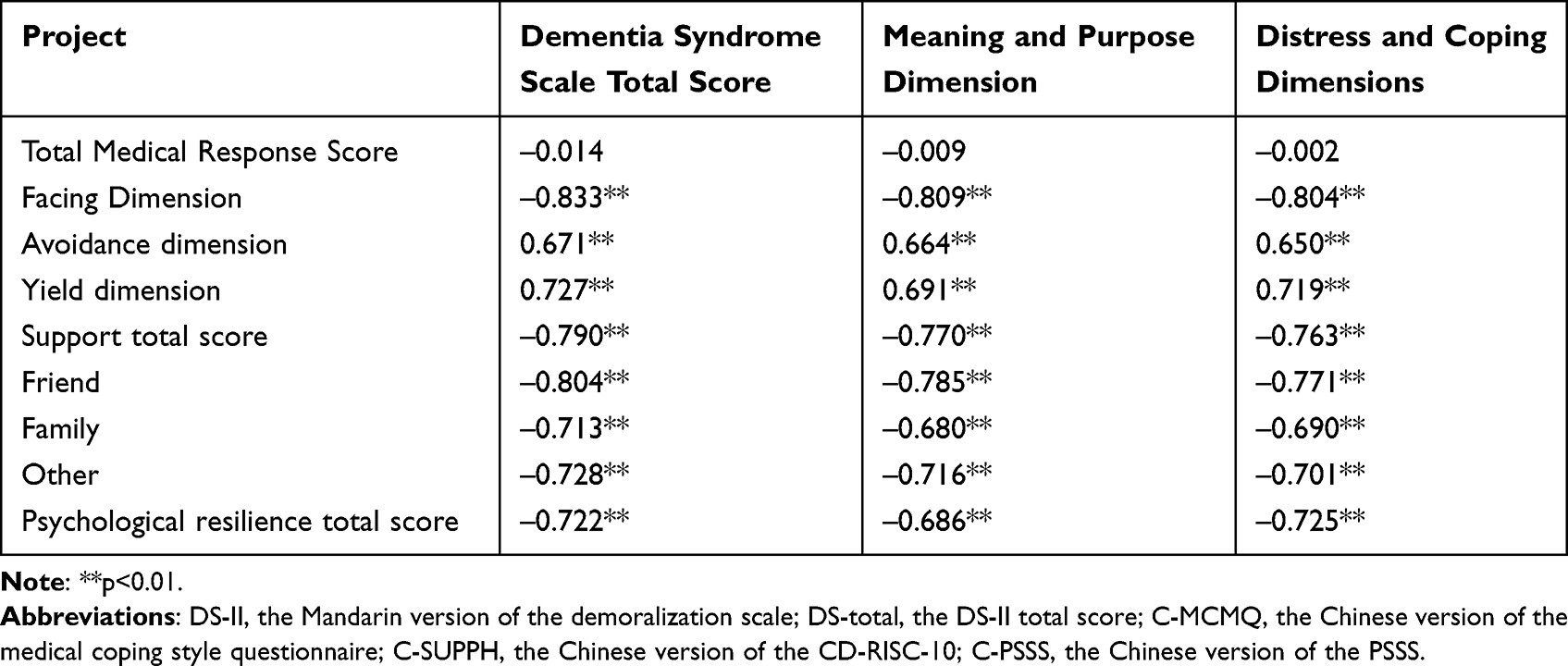 |
Table 3 Correlations of the Total DS-II and Its Subscales with the C-MCMQ Subscales, PSSS, and CD-RISC-10 |
Multiple Regression Analysis for the Influencing Factors of Demoralisation
Statistically significant independent variables identified in the univariate analysis and Pearson correlation analysis were included in the regression equation, resulting in the inclusion of 14 independent variables for predicting demoralisation. The results indicated that coping through yielding (β = 0.164), presence or absence of metastasis (β = 0.085), facing (life stress psychological coping resilience) (β = –0.321), total social support score (β = –0.251) and total psychological resilience score (β = –0.115) were the main factors influencing loss of will in patients with CRC. The final model explained over half of the variance in demoralisation status (adjusted R2 = 0.801; p < 0.001) (Table 4). Multiple regression analyses revealed that submission coping and disease transfer exacerbated demoralization, while facing attitudes, social support, and psychological resilience were protective factors.
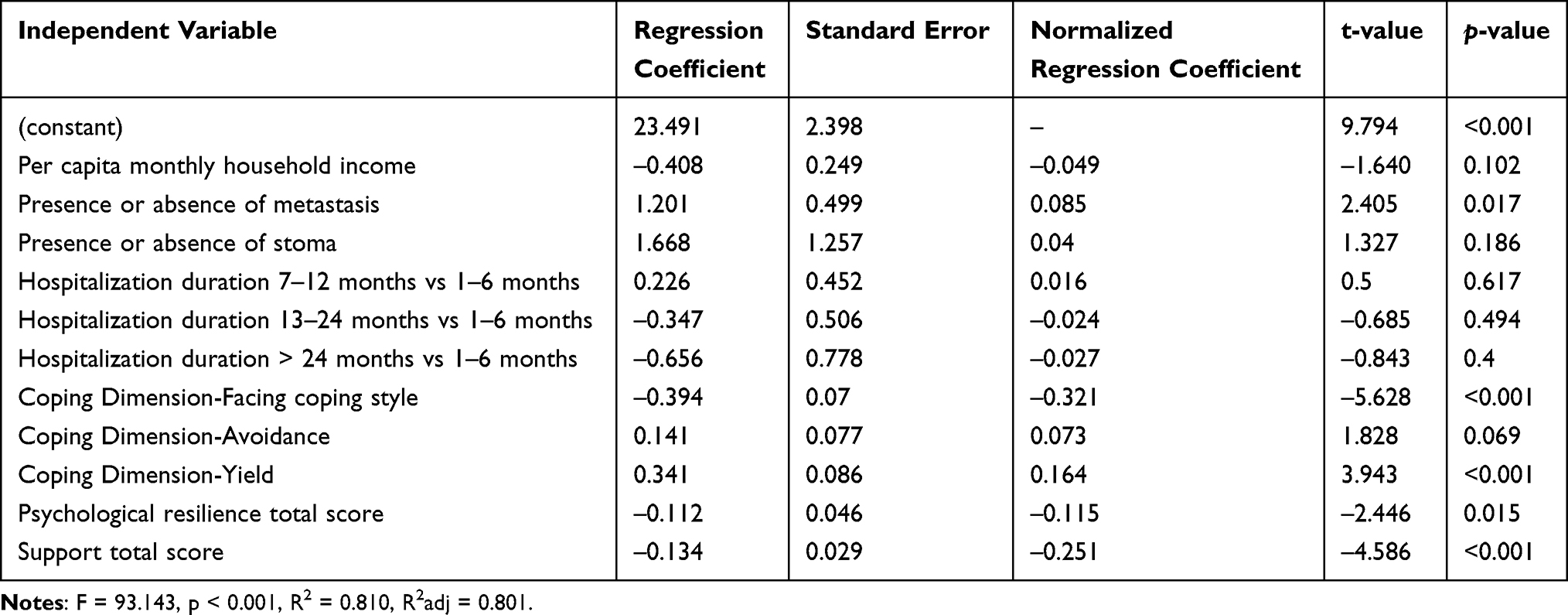 |
Table 4 Results of Multiple Linear Regression on the Variables Associated with Demoralization |
Discussion
This study identified 103 cases of low-grade demoralisation (40.7%), 112 cases of moderate demoralisation (44.3%) and 38 cases of high demoralisation (15%), with a mean score of 11.71 ± 6.32. These results are similar to those of previous studies19 but higher than those reported in studies by Vehling et al20 and Grassi et al.21 These differences may be attributable to variations in study populations, as well as regional and cultural factors. Among the demoralisation dimensions in patients with CRC, the scores of “significance and purpose” were 5.71 ± 2.91, whereas the scores of “distress and coping ability” were 6.08 ± 3.80. The reason for these scores may be that a CRC diagnosis will greatly impact patients’ psychology. As the disease progresses and physical symptoms and the side effects of treatment manifest, patients become increasingly prone to depression, irritability and anxiety, and this is reflected in the higher “distress and coping ability” scores. Nanni et al investigated 195 outpatients with cancer and found that 25.1% demonstrated moderate to severe demoralisation, with 8.2% displaying potential suicidal tendencies.12 These findings were significantly lower than those of the current study. Based on the scores and grading of demoralisation syndrome, the occurrence of demoralisation syndrome in patients with CRC in this study is more severe. A systematic review reveals that demoralisation syndrome is an independent risk factor for suicide.22,23 Consequently, healthcare professionals should be vigilant in identifying early signs of demoralisation in patients with CRC and intervene promptly to prevent suicidal ideation or behaviour, ensuring patient safety and fostering a safe and supportive medical environment.
Medical coping styles play an important role in patient demoralisation. Studies have shown that patients who adopt positive coping strategies tend to manage their emotions better and reduce symptoms such as depression and anxiety.24 However, some studies have also pointed out that negative coping styles, such as avoidance and denial, may exacerbate patients’ sense of demoralisation.25 This suggests that we should pay attention to patients’ coping styles and provide targeted psychological interventions in our clinical practice. The psychological stress caused by tumours significantly increases patients’ stress levels, leading individuals to adopt different coping strategies, which are generally categorised into three types: facing, avoiding and yielding. Positive-facing strategies can reduce an individual’s stress level and psychological pressure; however, adopting avoidance and yielding strategies can lead to an excessive psychological burden on individuals and affect both their physical and mental health.26
The results of this study reveal that demoralisation is negatively correlated with the facing coping style and positively correlated with the avoiding and yielding coping styles. Facing, a positive coping style, improves stress adaptability and cognitive evaluation level by fostering hope, self-adjustment and a belief in one’s ability to fight diseases, thereby alleviating feelings of demoralisation. In contrast, yielding (or submission), a negative coping style, reflects an individual’s subconscious belief that they cannot withstand the overwhelming stress of illness. Some studies have also suggested that a possible reason patients adopt a medical response is their lack of understanding of the disease, lack of confidence in disease recovery and inability to face the disease. Therefore, healthcare professionals should emphasise the importance of active coping strategies in promoting health. They should guide patients in understanding diseases, participating in disease management and treatment decisions and improving their coping abilities.
Social support refers to the material and emotional assistance individuals receive from various sources, including relatives, friends, colleagues, teams and communities.27 Social support enables patients to face stressful events with a more positive attitude, affects immune function, improves patients’ social adaptability and quality of life, and improves patient prognosis. Therefore, strong social support is essential for successful post-cancer psychological adjustment.28 Numerous studies have revealed a negative correlation between social support and demoralisation across various groups, including patients with cancer,20,29 parents of patients30 and psychiatrists.31 The results of this study indicate that perceived social support is negatively correlated with demoralisation in patients with CRC and is a protective factor against demoralisation. Patients with higher social support tend to receive more financial and emotional assistance, have better access to information and medical resources, and experience reduced psychological stress. Furthermore, improved communication and positive emotional exchanges between patients with strong social support and their spouses help alleviate negative emotions. Given these findings, it is important to monitor patients for signs of demoralisation and actively enhance their social support networks to mitigate its effects.
Our findings indicate that psychological resilience is a negative predictor of demoralisation in patients with CRC. This aligns with previous results, which revealed a negative correlation between psychological resilience and demoralisation in survivors of prostate cancer.32 Psychological resilience is an essential component of psychological crisis intervention. Individuals with high resilience tend to adopt a more positive outlook, effectively utilising both internal and external resources to cope with stress and trauma, thereby reducing negative psychological impacts and achieving better adaptation and recovery.33 Therefore, enhancing psychological resilience in patients with CRC may help mitigate the onset of a demoralisation syndrome.
Meaningful results provide clear guidance to healthcare providers, facilitate the development of individualised treatment plans and enhance the effectiveness of psychosocial support, thereby improving patients’ quality of life and treatment adherence. These findings can guide medical teams to enhance patients’ psychological status by conducting coping skills training to help patients adopt positive coping strategies, implementing resilience enhancement programmes to improve patients’ ability to face their illnesses and constructing a social support network to enhance the care felt by patients. These measures can help reduce patients’ psychological burden and improve treatment compliance and quality of life by providing psychological support for the overall recovery of patients with CRC.
This paper explores the theoretical interactions between demoralisation and medical coping styles, individual resilience and perceived social support in patients with CRC. Innovative in a practical sense, the findings are expected to guide clinical practice and provide more effective psychological support and intervention strategies for patients.
This study has several limitations. First, cross-sectional designs and convenience sampling cannot accurately infer a causal relationship between any single variable and demoralisation in patients with CRC. Second, the self-reported nature of the survey used in this study could lead to bias. Third, the results could be further biased by the use of convenience sampling and the recruitment of patients from a single study site. Therefore, future studies should use multicenter studies and increase the overall sample size. Fourth, the high R2 value achieved in our model, while indicative of strong explanatory power, may signal overfitting. This necessitates future validation in larger and more diverse populations to ensure the model’s generalizability beyond the present study sample.
Future research could also add depth by observing how demoralisation fluctuates over time in response to disease progression or treatment stages, testing specific interventions aimed at enhancing resilience and social support to assess whether these factors effectively reduce demoralisation scores, and examining demoralisation among different demographic subgroups (eg by age or cancer site) to uncover any variations not captured in this study.
Conclusion
This study explored the current state of demoralisation in patients with CRC and its relationship with medical coping styles, psychological resilience and social support. The findings provide new evidence for the associations among these important variables, and this may assist caregivers in more effectively addressing demoralisation syndrome in patients facing CRC during the treatment, recovery or end-of-life stages of the disease.
Data Sharing Statement
All data generated or analyzed during this study are included in this article. The data that support the findings of this study are available from the corresponding author, [BN], upon reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the declaration of Helsinki. This study was approved by the Medical Ethics Committee of Jiangnan University Affiliated Hospital. All patients signed informed consent before completing the questionnaire. (Approval Number: LS2024071).
Acknowledgments
Thank you to all the patients who participated in this study; your participation was crucial to the success of this study. Special thanks go to the Affiliated Hospital of Jiangnan University for your great assistance; your cooperation greatly facilitated the recruitment and implementation of the study. In addition, sincere thanks to all the volunteers and staff for their hard work, as your contributions were crucial to the smooth running of this study.
Funding
This study was supported by the China Postdoctoral Science Foundation (2023M731344).
Disclosure
The authors declare that they have no conflict of interest.
References
1. Cao W, Chen HD, Yu YW, Li N, Chen WQ. Changing profiles of cancer burden worldwide and in China: a secondary analysis of the global cancer statistics 2020. Chin Med J. 2021;134(7):783–791. doi:10.1097/CM9.0000000000001474
2. Tang L, Li Z, Pang Y. The differences and the relationship between demoralization and depression in Chinese cancer patients. Psychooncology. 2020;29(3):532–538. doi:10.1002/pon.5296
3. Kissane DW. Demoralisation: its impact on informed consent and medical care. Med J Aust. 2001;175(10):537–539. doi:10.5694/j.1326-5377.2001.tb143714.x
4. Tang PL, Wang HH, Chou FH. A systematic review and meta-analysis of demoralization and depression in patients with cancer. Psychosomatics. 2015;56(6):634–643. doi:10.1016/j.psym.2015.06.005
5. de Figueiredo JM. Depression and demoralization: phenomenologic differences and research perspectives. Compr Psychiatry. 1993;34(5):308–311. doi:10.1016/0010-440X(93)90016-W
6. Lo C, Hales S, Chiu A, et al. Managing Cancer And Living Meaningfully (CALM): randomised feasibility trial in patients with advanced cancer. BMJ Support Palliat Care. 2019;9(2):209–218. doi:10.1136/bmjspcare-2015-000866
7. Ignatius J, De La Garza R. Frequency of demoralization and depression in cancer patients. Gen Hosp Psychiatry. 2019;60:137–140. doi:10.1016/j.genhosppsych.2019.04.013
8. Kissane DW, Bobevski I, Gaitanis P, et al. Exploratory examination of the utility of demoralization as a diagnostic specifier for adjustment disorder and major depression. Gen Hosp Psychiatry. 2017;46:20–24. doi:10.1016/j.genhosppsych.2017.01.007
9. The L. ICD-11. Lancet. 2019;393(10188):2275. doi:10.1016/S0140-6736(19)31205-X
10. Lee CY, Fang CK, Yang YC, et al. Demoralization syndrome among cancer outpatients in Taiwan. Support Care Cancer. 2012;20(10):2259–2267. doi:10.1007/s00520-011-1332-4
11. Li YC, Ho CH, Wang HH. Demoralization in cancer patients and related factors in Taiwan. Cancer Nurs. 2017;40(1):E54–e60. doi:10.1097/NCC.0000000000000352
12. Nanni MG, Caruso R, Travado L, et al. Relationship of demoralization with anxiety, depression, and quality of life: a Southern European study of Italian and Portuguese cancer patients. Psychooncology. 2018;27(11):2616–2622. doi:10.1002/pon.4824
13. Julião M, Nunes B, Barbosa A. Prevalence and factors associated with demoralization syndrome in patients with advanced disease: results from a cross-sectional Portuguese study. Palliat Support Care. 2016;14(5):468–473. doi:10.1017/S1478951515001364
14. Robinson S, Kissane DW, Brooker J, et al. Refinement and revalidation of the demoralization scale: the DS-II-internal validity. Cancer. 2016;122(14):2251–2259. doi:10.1002/cncr.30015
15. Ou N, Hu X, Qi S, et al. Sinicization of asthenia syndrome scale II and its reliability and validity in cancer patients. Chin Gen Pract. 2021;24(23):2998–3004. [In Chinese].
16. Shen X. A test report of 701 cases of the Chinese version of the medical coping style questionnaire. J Behav Med. 2000;1:22–24. [In Chinese].
17. Dahlem NW, Zimet GD, Walker RR. The multidimensional scale of perceived social support: a confirmation study. J Clin Psychol. 1991;47(6):756–761. doi:10.1002/1097-4679(199111)47:6<756::AID-JCLP2270470605>3.0.CO;2-L
18. Campbell-Sills L, Stein MB. Psychometric analysis and refinement of the Connor-davidson Resilience Scale (CD-RISC): validation of a 10-item measure of resilience. J Trauma Stress. 2007;20(6):1019–1028. doi:10.1002/jts.20271
19. Bovero A, Botto R, Adriano B, Opezzo M, Tesio V, Torta R. Exploring demoralization in end-of-life cancer patients: prevalence, latent dimensions, and associations with other psychosocial variables. Palliat Support Care. 2019;17(5):596–603. doi:10.1017/S1478951519000191
20. Vehling S, Mehnert A. Symptom burden, loss of dignity, and demoralization in patients with cancer: a mediation model. Psychooncology. 2014;23(3):283–290. doi:10.1002/pon.3417
21. Grassi L, Rossi E, Sabato S, Cruciani G, Zambelli M. Diagnostic criteria for psychosomatic research and psychosocial variables in breast cancer patients. Psychosomatics. 2004;45(6):483–491. doi:10.1176/appi.psy.45.6.483
22. Fang CK, Chang MC, Chen PJ, et al. A correlational study of suicidal ideation with psychological distress, depression, and demoralization in patients with cancer. Support Care Cancer. 2014;22(12):3165–3174. doi:10.1007/s00520-014-2290-4
23. Vehling S, Kissane DW, Lo C, et al. The association of demoralization with mental disorders and suicidal ideation in patients with cancer. Cancer. 2017;123(17):3394–3401. doi:10.1002/cncr.30749
24. Fasano J, Shao T, Huang HH, Kessler AJ, Kolodka OP, Shapiro CL. Optimism and coping: do they influence health outcomes in women with breast cancer? A systemic review and meta-analysis. Breast Cancer Res Treat. 2020;183(3):495–501. doi:10.1007/s10549-020-05800-5
25. Vargas-Román K, Tovar-Gálvez MI, Liñán-González A, Cañadas de la Fuente GA, de la Fuente-Solana EI, Díaz-Rodríguez L. Coping strategies in elderly colorectal cancer patients. Cancers. 2022;14(3):608. PMID: 35158876; PMCID: PMC8833470. doi:10.3390/cancers14030608
26. Feifel H, Strack S, Nagy VT. Coping strategies and associated features of medically ill patients. Psychosom Med. 1987;49(6):616–625. doi:10.1097/00006842-198711000-00007
27. Gottlieb BH, Bergen AE. Social support concepts and measures. J Psychosom Res. 2010;69(5):511–520. doi:10.1016/j.jpsychores.2009.10.001
28. You J, Lu Q. Social constraints and quality of life among Chinese-speaking breast cancer survivors: a mediation model. Qual Life Res. 2014;23(9):2577–2584. doi:10.1007/s11136-014-0698-4
29. Robinson S, Kissane DW, Brooker J, Burney S. A systematic review of the demoralization syndrome in individuals with progressive disease and cancer: a decade of research. J Pain Symptom Manage. 2015;49(3):595–610. doi:10.1016/j.jpainsymman.2014.07.008
30. Okado Y, Bierman KL, Welsh JA. Promoting school readiness in the context of socio-economic adversity: associations with parental demoralization and support for learning. Child Youth Care Forum. 2014;43(3):353–371. doi:10.1007/s10566-013-9242-x
31. Gabel S. Demoralization in mental health organizations: leadership and social support help. Psychiatr Q. 2012;83(4):489–496. doi:10.1007/s11126-012-9217-3
32. Chien CH, Pang ST, Chuang CK, et al. Exploring psychological resilience and demoralisation in prostate cancer survivors. Eur J Cancer Care. 2022;31(6):e13759.
33. Dreer LE, Cox MK, McBrayer A, Neumeier WH, Herman C, Malone LA. Resilience among caregivers of injured service members: finding the strengths in caregiving. Arch Phys Med Rehabil. 2019;100(4s):S76–s84. doi:10.1016/j.apmr.2018.12.027
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Influence of Social Support on the Mental Health of Elderly Individuals in Healthy Communities with the Framework of Mental Toughness
Zhang C, Dong C
Psychology Research and Behavior Management 2023, 16:2977-2988
Published Date: 4 August 2023
The Levels and Associated Factors for Participation and Autonomy Among People with Parkinson´s Disease: A Cross-Sectional Study
Zhang T, Yao L, Li T, Tian H, Song G
Psychology Research and Behavior Management 2024, 17:1045-1055
Published Date: 12 March 2024
Social Support and Social Adjustment Among Chinese Secondary School Students: The Mediating Roles of Subjective Well-Being and Psychological Resilience

Yu L, Wu X, Zhang Q, Sun B
Psychology Research and Behavior Management 2024, 17:3455-3471
Published Date: 7 October 2024
Psychological Resilience and Sleep Quality Among the Elderly: The Mediating Role of Social Support
Li J, Zhang J, Hou Y, Cui Y, Wang Q, Ouyang A, Cai M, Hua Y
Nature and Science of Sleep 2025, 17:2469-2483
Published Date: 3 October 2025