Back to Journals » Psychology Research and Behavior Management » Volume 17
The Levels and Associated Factors for Participation and Autonomy Among People with Parkinson´s Disease: A Cross-Sectional Study
Authors Zhang T, Yao L, Li T, Tian H, Song G
Received 4 November 2023
Accepted for publication 28 February 2024
Published 12 March 2024 Volume 2024:17 Pages 1045—1055
DOI https://doi.org/10.2147/PRBM.S448240
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Bao-Liang Zhong
Tingting Zhang,1,* Lan Yao,1,* Tao Li,2 Haoxin Tian,3 Guirong Song4
1Nursing Department, the First Hospital Affiliated to Dalian Medical University, Dalian, People’s Republic of China; 2Department of Neurology, the First Hospital Affiliated to Dalian Medical University, Dalian, People’s Republic of China; 3The First Clinical College, Dalian Medical University, Dalian, People’s Republic of China; 4Department of Health Statistics, School of Public Health, Dalian Medical University, Dalian, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guirong Song, Email [email protected]
Background: Promoting participation and autonomy (PA) in society has been highlighted as an ultimate goal of rehabilitation for people with chronic diseases by the World Health Organization, but few studies have focused on PA in people with Parkinson’s disease (PD). Therefore, this study aimed to determine the level of PA in PD patients and investigate the associated psychological and behavioural factors.
Methods: PD patients were recruited from the Department of Neurology of the First Hospital Affiliated with Dalian Medical University using convenience sampling for this cross-sectional study. A questionnaire covering social-demographic and disease-related characteristics, Chinese version of Impact on Participation and Autonomy (IPA) Questionnaire, Connor-Davidson Resilience Scale (CD-RISC), Self-rating Depression Scale (SDS), Self-rating Anxiety Scale (SAS), Medical Coping Modes Questionnaire (MCMQ), Social Support Rating Scale (SSRS), Hoehn-Yahr Staging System and Unified Parkinson’s Disease Rating Scale (UPDRS) were used for investigation. A multivariate stepwise linear regression analysis was used to determine the factors that influence IPA.
Results: A total of 326 PD patients responded to all the questionnaires. The patients had a mean IPA score of 46.6 (SD 21.79). Multiple linear regression analyses revealed that UPDRS II (β = 0.35, p < 0.001) had the strongest correlation with IPA, followed by tenacity, which was the second strongest factor (β = − 0.25, p < 0.001). Hoehn-Yahr stage (β = 0.19, p < 0.001) and availability of social support (β =− 0.12, p =0.001) were also strong factors.
Conclusion: The average level of PA among PD patients was at the lower middle-level. Among PD patients, physical function, psychological resilience and social support were the strongest factors associated with PA. These findings provide valuable insights into PD patients’ PA and can help medical professionals identify the early risks of restricted PA among PD patients, implement interventions to promote PA and ultimately achieve rehabilitation.
Keywords: participation and autonomy, psychological resilience, social support, Parkinson’s disease, medical coping modes
Introduction
Parkinson’s disease (PD), which poses a serious danger to elderly people, is a prevalent neurodegenerative condition that has resulted in heavy social and economic burdens worldwide and has a gradually increasing prevalence.1 PD patients typically have trouble performing activities of daily living (ADL) and have limited physical independence due to motor symptoms, such as rigidity, bradykinesia, resting tremor, postural instability, and freezing of gait.2 Moreover, they often experience nonmotor symptoms, including psychosocial problems such as depression, anxiety, stigma, frustration, and fear of the future.3 These symptoms not only negatively affect PD patients’ physical outcomes but also lead to reduced family functioning, limited social and economic activity, and decreased quality of life (QoL).4 Thus, for patients, PD impairs their physical and emotional health substantially. To date, there is no cure for PD beyond symptomatic relief, which slows the neurodegenerative process;5 thus, the treatment and rehabilitation of PD should focus on better rehabilitation outcomes, such as maintaining and improving patient-related QoL and social participation levels.
The World Health Organization (WHO) has highlighted that promoting participation in society is the ultimate goal of rehabilitation in people with chronic diseases according to the conception of the International Classification of Functioning, Disability, and Participation (ICF).6 Participation or social participation is defined as involvement in a life situation and covers an individual’s experience in life activities and social roles, such as socializing, work, entertainment, civic life, and religious practice. Furthermore, Cardol et al7 emphasized the value of “autonomy” in the context of “participation”, which refers more to autonomy and the personal fulfilment of roles than to normal role fulfilment. Autonomy has been considered a fundamental prerequisite for effective participation and was described as “the ability to make choices, to feel in control of which activities to engage in and in what manner these activities are performed”.8 The concepts of participation and autonomy (PA) are strongly connected. The Impact on Participation and Autonomy Questionnaire (IPAQ), developed by Cardol et al9 is a reliable and valid instrument for assessing PA in individuals with chronic disorders and is able to capture the full extent of participation.
Although PD patients are acknowledged to experience a decline in QoL according to many studies,4 few studies have focused on their PA, so there is still limited understanding of the complexity of PA and how care services can promote them for PD patients. Hence, comprehensively understanding the nature of PA in PD patients and exploring the influencing factors are important tasks for facilitating effective intervention to help patients reintegrate into society.
To fill this gap, our study investigated the level of PA in Chinese PD patients and revealed its associated factors. In addition to objective factors such as sociodemographic characteristics and PD-related physiological function commonly studied, our study focused more on psychological and behavioural factors, including resilience, coping modes and social support. Psychological resilience is a positive psychological attribute that can help individuals adapt and determine effective responses under harsh circumstances; therefore, it serves a considerable protective factor in chronic disease rehabilitation.10 Additionally, studies have demonstrated that social support positively impacts the QoL of patients with PD.11 Perception of social support has been reported to be useful in promoting PA in individuals after stroke,12 but there is a lack of similar studies on PD patients. Moreover, medical coping modes were defined as “the set of cognitive and behavioural strategies that the patient employed in dealing with their disease-specific stressful encounter”13 and classified into three types. Compared with resignation and avoidance, confrontation is generally considered positive and active. Several studies revealed that avoidance and resignation were associated with elevated levels of psychological distress in PD patients.14 However, the effects of medical coping modes on PA in PD patients have not been extensively investigated and are worthy of further exploration.
In brief, this study aimed to determine the level of PA among PD patients and examine the effects of vital psychological and behavioural factors covering resilience, coping styles and social support on PA. Consequently, this study can offer novel insights into the PA of PD patients and can help medical professionals identify early risks of restricted PA among PD patients, implement multimodal interventions to promote PA and fulfil their rehabilitation potential.
Methods
Participants
Participants were recruited from the Department of Neurology of the First Hospital Affiliated with Dalian Medical University by convenience sampling from February 2018 to May 2018. Participants were included if they met the following criteria: (1) were older than 18 years old; (2) had a confirmed diagnosis of PD according to the standard set by the Chinese Medical Committee, Neurology Branch, Parkinson’s Disease and Motor Disorders Group and confirmed by neurological specialists; and15 (3) were approved to participate in the study. The exclusion criteria were patients with the following conditions: (1) secondary PD; (2) Parkinsonism-plus syndrome; (3) severe organ dysfunctions, respiratory failure, or malignant cancer; (4) a history of dementia, mental deficiency, or other psychiatric diseases; and (5) visual, aural, or verbal impairment.
With approximately 30 variables potentially associated with PD patients’ PA, the minimum sample size was approximately 300 participants according to Kendall’s principle of approximately 10 subjects per independent variable in the linear regression analysis. Furthermore, to accommodate a 15% attrition rate, the sample size of this survey was expanded to 345 patients.
Data Collection
Each participant was informed about the purpose of the research through face-to-face instructions to assure voluntary participation. Written informed consent was obtained from each participant and the study was approved by the institutional ethics committee of the First Hospital Affiliated with Dalian Medical University. Researchers provided instructions about completing the questionnaire, administered the questionnaire survey, and collected the questionnaires immediately following completion.
Measures
The key variables collected included (1) perceived participation and autonomy; (2) resilience; (3) anxiety and depression; (4) medical coping modes; (5) social support; (6) physical function; and (7) sociodemographic and disease-related characteristics, including age, sex, marital status, education level, knowledge about PD, complications of PD and so on (Supplementary Table 1).
Impact on Participation and Autonomy (IPA) Questionnaire
The original English version of the IPA (IPA-E) questionnaire is a self-report questionnaire consisting of 32 items and five dimensions devised to assess perceived PA.9 Based on the IPA-E, the Chinese version of the IPA (IPA-C) was first translated and adapted by Li et al.16 The IPA-C consists of 25 items and four dimensions: Autonomy Indoors (7 items), Family Role (7 items), Autonomy Outdoors (5 items), and Social Relations (6 items). The IPA-C is a 5-point scale ranging from “excellent” (0) to “very poor” (4). The total possible score on the IPA-C ranges from 0–100, where a lower score indicates better self-perceived PA. The IPA-C was first used in stroke survivors, with reported Cronbach’s α values of 0.78–0.96 for each domain and test-retest reliability between 0.97 and 0.98.16
Standardized scores can be calculated based on the mean item scores. In this study, the standardized total and domain scores were classified into three levels: “good PA” (score = 0–1), “fair PA” (score >1 and score<3), and “poor PA” (score = 3–4).
Connor-Davidson Resilience Scale (CD-RISC)
The original English version of the CD-RISC was constructed by Connor & Davidson17 to assess resilience and was viewed as a measure of stress-coping ability. The CD-RISC comprises 25 items, each rated on a 5-point scale (0–4), with higher scores reflecting greater resilience. The Chinese version of the CD-RISC was first translated and adapted by Yu & Zhang,18 which included 25 items, each rated on a 5-point scale (0–4), encompassed by three factors: tenacity (13 items), strength (8 items) and optimism (4 items). The total score of the Chinese version of the CD-RISC ranges from 0–100 points, and higher scores reflect greater resilience. The Chinese version of the CD-RISC is as reliable and valid as the English version for measuring resilience in Chinese society.18
Self-Rating Depression Scale (SDS) and Self-Rating Anxiety Scale (SAS)
The SDS and SAS were developed by Zung.19 Each questionnaire comprises 25 items, each rated on a 4-point scale(0–4), with higher scores reflecting greater depression or anxiety. The rough score is obtained by aggregating the original questionnaire score. Then, the standard score is obtained by rounding the integer part of the product of the rough score and 1.25 up. The higher the standard score is, the more obvious the symptoms of anxiety and depression are.
Medical Coping Modes Questionnaire (MCMQ)
The original MCMQ was developed by Feifel.13 The MCMQ is suitable for patients with a variety of diseases. Its Chinese version consists of 20 items and includes three subscales, namely, “confrontation”, “avoidance”, and “acceptance-resignation”. The questionnaire is rated on a 4-point Likert scale ranging from 1 (never) to 4 (fully met). For each subscale, a higher average score indicates that the individual more often used this corresponding coping mode.
Social Support Rating Scale (SSRS)
The SSRS was designed by Xiao20 based on the actual situation in China and related foreign research results. The scale consists of 10 items and includes three dimensions, namely, objective support, subjective support and availability of support. The higher the score is, the greater the degree of social support. The Cronbach´s α coefficients of each dimension and total scale ranged from 0.89 to 0.94, and the content validity ranged from 0.724 to 0.835, indicating good reliability and validity.
Hoehn and Yahr (H-Y) Stage System
The H-Y stage system has been used worldwide to evaluate the disease severity or stage in PD patients.21 The patients were divided into eight stages according to their type of disorder (unilateral or bilateral) and degree of balance difficulty.
Unified Parkinson Disease Rating Scale (UPDRS)
The UPDRS has been widely used to evaluate the severity of motor and nonmotor symptoms in patients with PD. UPDRS Parts I, II and III consist of 4, 13 and 14 items, respectively.22 Items are rated on a Likert-type additive scale with five response choices ranging from 0 (best condition) to 4 (worst condition). Higher scores indicate worse status or function. The UPDRS-I measures the mental status of the PD patients, including intelligence, thoughts, and emotions. Scores range from 0 to 16, with higher scores indicating worse mental status. The UPDRS II assess the performance on ADL, including walking, speaking, writing, dressing, and personal hygiene. The UPDRS III evaluates motor function, including facial expression, rigidity, bradykinesia, resting tremor, postural instability, and freezing of gait.
Statistical Analyses
Analyses were performed with IBM SPSS Statistics 25.0 (IBM Corp.). The mean and standard deviation were used to describe variables with normal distributions, and the median and quartile were used to describe variables with nonnormal distributions. Percentages were used to describe categorical variables. One-way analysis of variance (ANOVA) was used to explore the differences in IPA among the groups with different sociodemographic and disease-related characteristics. Spearman correlation was performed to investigate the associations between the IPA scores and the SSRS, MCMQ,CD-RISC, SDS, SAS and UPDRS scores. All tests were two-sided, and p values <0.05 were used to indicate statistical significance. Multivariate stepwise linear regressions with a p value of entry less than 0.01 and a p value of removal less than 0.05 were conducted to identify influencing factors on IPA and each domain. Before constructing each linear regression model, collinearity diagnosis was performed, and the variance inflation factors (VIFs) of the independent variables were all less than 5; therefore, there was no strong collinearity.
Results
Participant Characteristics
In total, 326 patients with PD fully answered the questionnaire, for a response rate of 94.5%. A total of 45.1% were female. The mean (±SD) age of the patients was 68.07±9.02 years, ranging from 40 to 89 years. The mean age of PD onset was 62.06±9.76 years, ranging from 33 to 66 years. The median duration of PD according to quartile was 5 (3,9) years, ranging from 0 to 34 years. Approximately all of the patients (82.2%) lived with their spouse, and 76.1% were cared for by their spouse (Supplementary Table 1).
PA Levels in Patients with PD
Descriptive statistics of the IPA are presented in Table 1. The mean IPA score was 46.6 (SD 21.79). According to the comparison of standardized scores, the highest score was for autonomy outdoors, followed by family role, autonomy indoors, and social relations, representing the reverse order of ranking according to PA level. A total of 29.8%, 26.1%, 12.3% and 3.7% of the participants reported poor PA in terms of autonomy outdoors, family role, autonomy indoors, and social relations, respectively. These results indicated that more severely restricted PA were found in the domains of autonomy outdoors and family role. Overall, 9.8%, 72.7%, and 17.5% of the participants exhibited poor, fair and good PA, respectively.
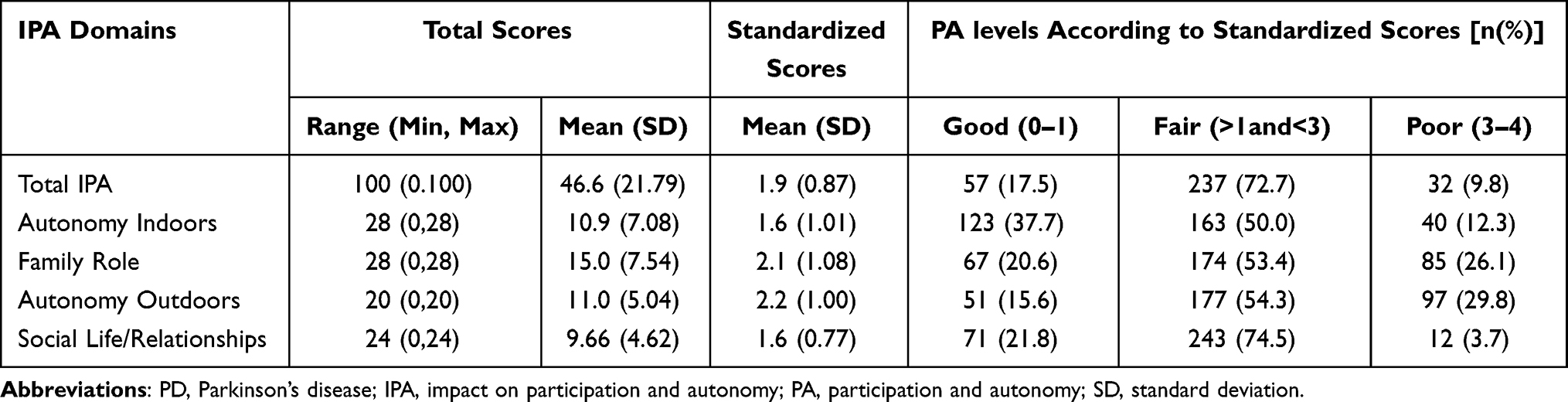 |
Table 1 Descriptive Statistics of the IPA Among Patients with PD (n = 326) |
Comparison of IPA Scores of PD Patients with Different Characteristics
The univariate analysis results according to patients’ sociodemographic and disease-related characteristics are presented in Table 2. The scores for the IPA or some of its domains were significantly different among the groups related to these characteristics, namely, age group (p<0.01), education level (p<0.05), monthly income (p<0.01), working status (p<0.01), living arrangement (p<0.05), caregivers (p<0.01), duration of PD (p<0.01), other chronic diseases (p<0.05), complications of PD (p<0.01), subsequent consultation (p<0.05), knowledge about PD (p<0.01), and H-Y stage (p<0.001). The above variables were taken into account when a multiple linear regression model of the scores for IPA was constructed.
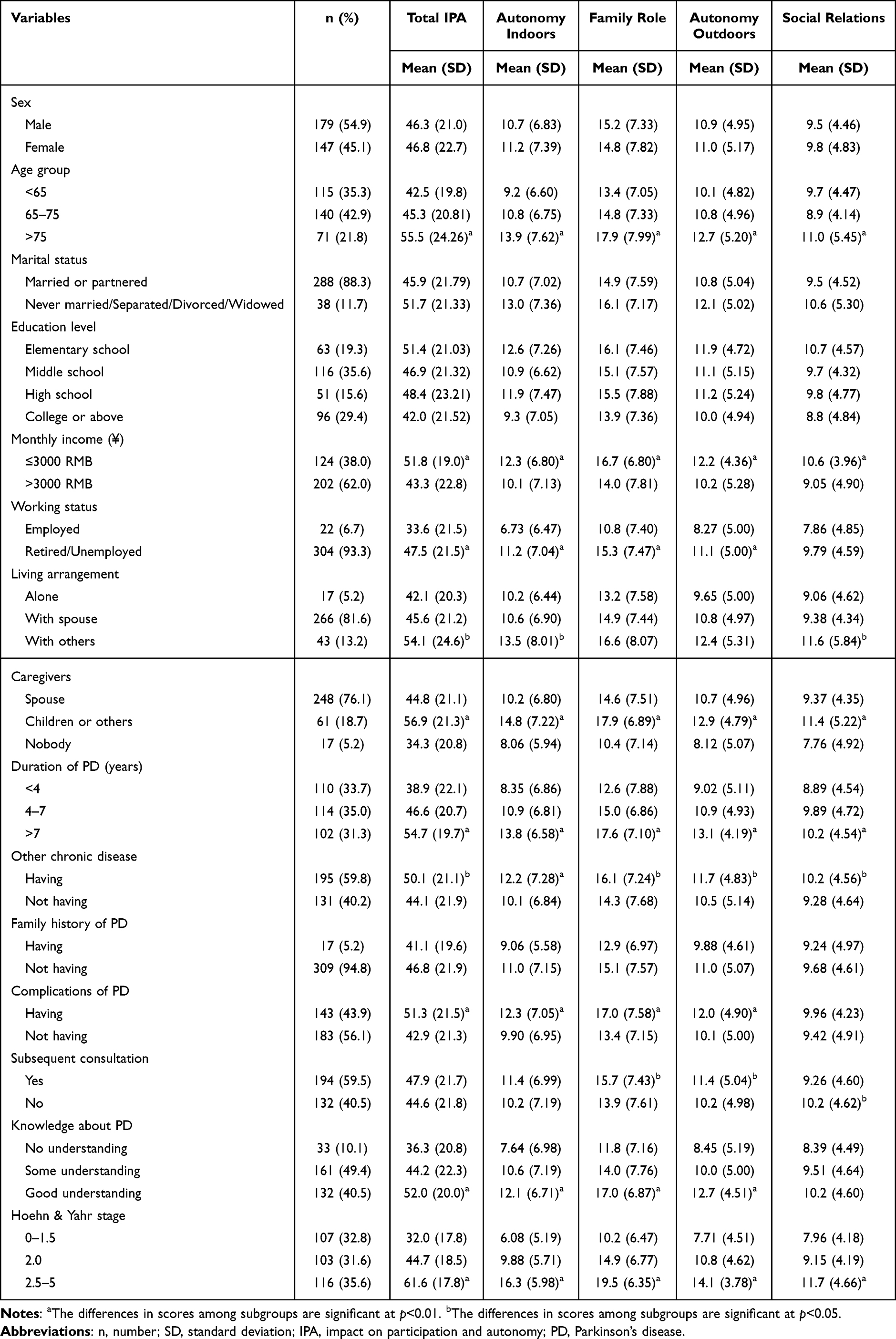 |
Table 2 Comparison of IPA Scores of PD Patients with Different Characteristics |
Correlations Between the Scores for IPA and the Scores for the SSRS, MCMQ, CD-RISC, SDS, SAS and UPDRS
The associations between the IPA scores and the key variables are summarized in Table 3. Social support was significantly related to IPA (r =−0.15~-0.51, p<0.05); that is, the stronger the social support was, the better the PA. Additionally, resilience displayed the same association with IPA (r =−0.35~-0.49, p<0.001). However, the more serious the symptoms of anxiety were, the poorer the PA. In addition, the stronger the resignation of coping styles was, the poorer the PA. The above variables, except for depression, were also taken into account when a multiple linear regression model of the IPA was constructed.
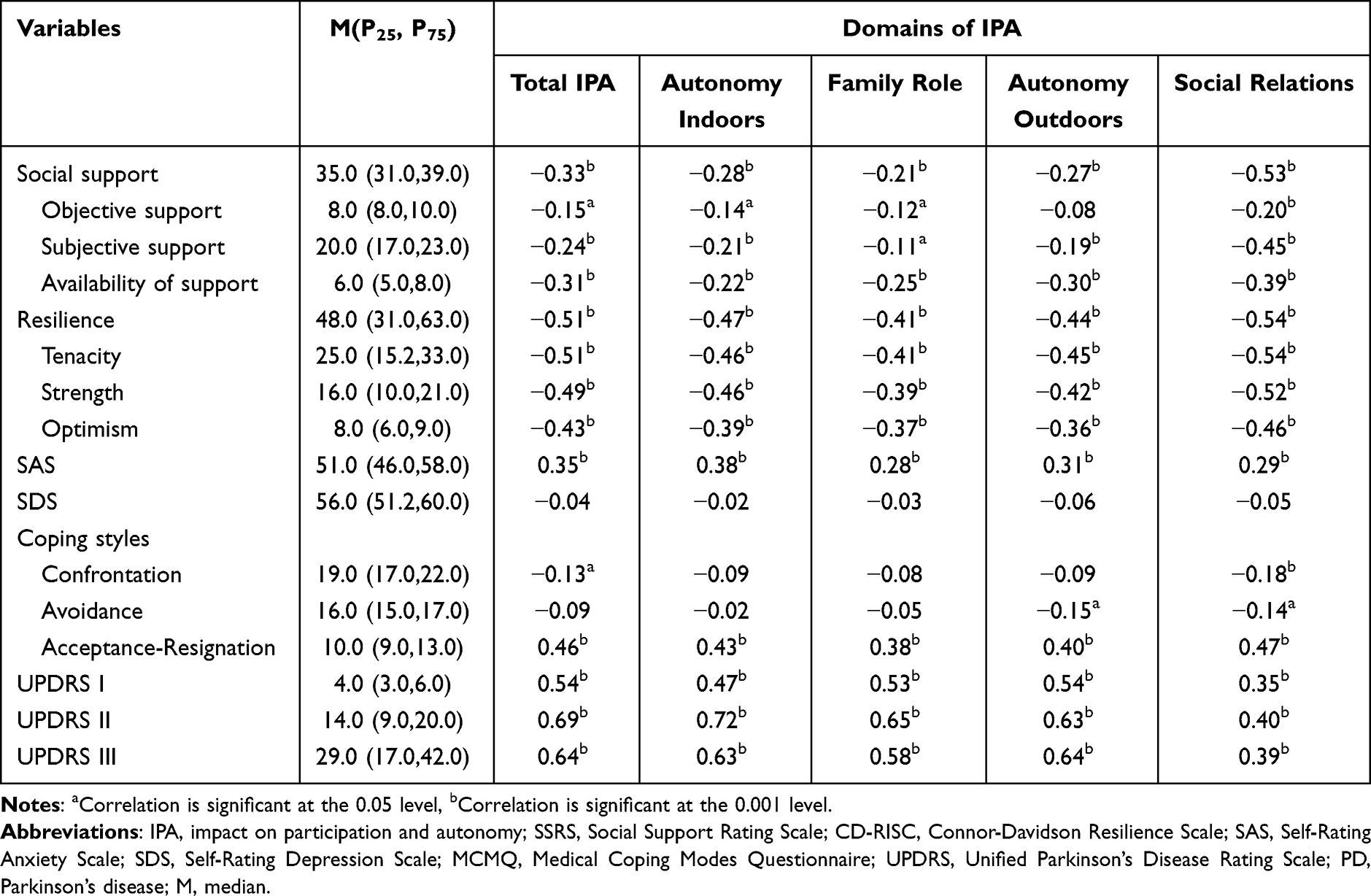 |
Table 3 Correlations Between the Scores for IPA and the Scores for the SSRS, MCMQ, CD-RISC, SDS, SAS and UPDRS Among PD Patients |
Associated Factors on IPA
Multiple linear regression analyses of factors influencing the incidence of IPA are summarized in Table 4. The model was significant and explained 64.1% of the IPA (adjusted R2 = 0.64). The performance on activities of daily living assessed by the UPDRS-II (β = 0.35, p < 0.001) had the strongest correlation with IPA, followed by tenacity, which was the second strongest factor (β= −0.25, p < 0.001). Additionally, Hoehn-Yahr stage (β = 0.19, p < 0.001) and availability of social support (β =−0.12, p =0.001) were stronger factors. Supplementary Table 2 shows the influencing factors on each domain of the IPA. UPDRS-II score had the strongest correlation with autonomy indoors (β = 0.47, p < 0.001) and family role(β = 0.30, p < 0.001), while tenacity (a domain of resilience) had the strongest correlations with autonomy outdoors(β = −0.24, p < 0.001) and social relations (β = −0.35, p < 0.001). Tenacity and strength were the second strongest factors correlated with autonomy indoors (β = −0.22, p < 0.001) and family role (β = −0.20, p < 0.001), respectively. H-Y stage was also a strong factor correlated to autonomy outdoors (β = 0.23, p < 0.001) and autonomy indoors (β =0.21,p < 0.001). Moreover, availability of social support (β = −0.21, p < 0.001) was the second strongest factor correlated with social relations, and resignation (β = 0.14, p <0.01) was the third strongest factor.
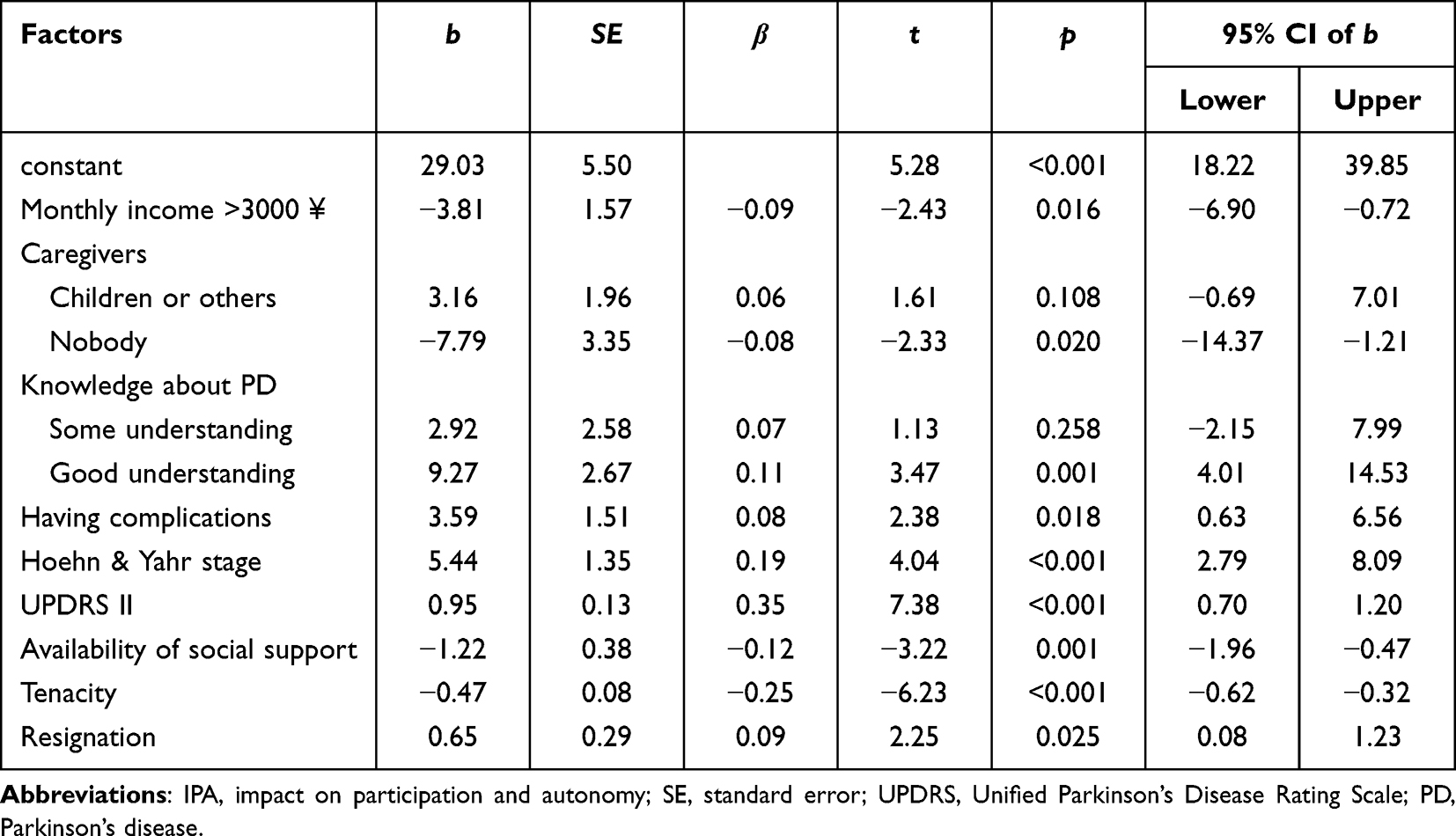 |
Table 4 Multiple Linear Regression Analysis of Influencing Factors on IPA Among PD Patients |
Discussion
The first aim of our study was to reveal the level and features of PA among PD patients from China. In our study, the mean score for the IPA was 46.6 (SD 21.79), which was similar to the results of the study by Guo et al23 (mean = 48.98, SD 16.92). Therefore, PD patients demonstrated a lower middle-level of PA. Moreover, the PD patients perceived poorer PA in autonomy outdoors and in family roles than in autonomy indoors and social relations. Restriction in autonomy outdoors might be attributed to patients’ motor symptoms. Several qualitative studies have reported that motor symptoms, such as shaking, trembling, freezing, and exacerbation of physical disability, usually hamper individuals with PD’s ability to perform outdoor activities.24 In addition, perceived stigma and social embarrassment from physical symptoms (eg, falls, tremors, speech difficulty) and patient image changes have led people with PD to retreat from society. More restrictions in the family role might be due to the patient’s inability to perform ADL and to the family caregivers’ excessive protection, which can reinforce the patient’s identity as a patient and weaken their family roles.25
As expected, physical function was the most important factor affecting PD patients’ PA. The ADL performance assessed by the UPDRS-II was the strongest factor correlated with IPA and the domains of autonomy indoors and family role, and the H-Y stage was also a stronger factor connected to autonomy indoors and outdoors. That is, worse physical function was correlated with greater restriction of the patients’ independence and a lower PA. Thus, improving patients’ physical function, controlling clinical symptoms and preventing disease exacerbation are the first priorities of treatment and rehabilitation for PD patients, and PD care should include providing health education to patients and improving medication compliance to obtain more ideal rehabilitation.
In addition to physical function, psychological resilience was one of the strongest correlates of IPA; in particular, tenacity (a domain of resilience) was most strongly correlated with the domains of autonomy outdoors and social relations. Psychological resilience can be understood as the ability to cope with and adapt to loss, hardship, or adversity in an efficient manner. One of its domains, tenacity, reflects an individual’s equanimity, promptness, perseverance, and sense of control when facing situations of hardship and challenge. Another domain, strength, reflects the individual’s capacity to recover and become strong after setbacks and past experiences.18 A study on PD found higher resilience to be significantly associated with less disability and better health-related QOL.26 Hence, resilience clearly appears to have a strong “protective” impact on PA in patients with PD. However, PD patients demonstrated lower middle-level resilience, with a median score of 48. Some studies have underscored the concept of resilience as something that can be modified as an active process;26 therefore, from the view of positive psychology, it is important to focus on resilience-fostering interventions in therapeutic and rehabilitative settings to increase patients’ PA levels.
In addition, our findings showed that social support was significantly correlated with IPA (r=−0.15~-0.51, p<0.05); that is, the stronger the social support was, the greater the level of PA. These findings are consistent with previous studies of stroke patients and PD patients.23,25 Social support refers to the care, assistance and resources provided by others, such as family, partners, friends or significant others, and the community. Social support plays a vital role in maintaining both physical and mental well-being. Adequate social support has been shown to effectively mitigate stress, ultimately reducing the occurrence of associated psychosomatic disturbances. Poor social support has been found to be significantly associated with greater depressive symptoms and worse functional status in patients with PD, as demonstrated in studies by Ghorbani Saeedian et al27 and Cheng et al.28 Moreover, older PD patients appear to be particularly vulnerable to the negative impacts resulting from a lack of social support.28 Vescovelli et al29 discovered that social support has a specific role in promoting the social inclusion and work engagement of PD patients, which subsequently contributes to the maintenance of their life satisfaction despite the limitations imposed by their condition. Therefore, social support can play a crucial role in improving the social well-being of individuals with PD. Remarkably, the availability of social support had a stronger impact on PA than did subjective social support and objective social support according to our multiple factor analyses. PD patients may worry about being a burden, leading to social withdrawal and a reluctance to be with friends and participate in activities,30 so that they may be reluctant to seek help and have poor perceptions of social support. Therefore, it is evident that not only should more comprehensive social support be provided for PD patients but also that their perception and availability of such support should be enhanced to improve their level of PA.
Our findings showed that acceptance-resignation of coping styles was positively correlated with total IPA and each domain; that is, the greater the acceptance-resignation of coping styles was, the lower the level of PA. Multiple factor analyses also revealed that acceptance-resignation was a strong factor impacting total IPA and social relations. These findings are consistent with previous studies of stroke patients.25 Several studies have shown that PD patients often adopt negative coping styles, such as avoidance or acceptance-resignation. When faced with worsening symptoms of the disease without the possibility of a cure, patients often resort to negative coping strategies, actively choosing to avoid social interactions and isolating themselves from society, reducing their social contact.31 Evans and Norman14 demonstrated that the use of avoidance and resignation as coping strategies was associated with elevated levels of psychological distress, both cross-sectionally and prospectively, for PD patients. Therefore, health care professionals should provide education or information for patients in daily care, help them solve problems, encourage them to face life and illness with a positive attitude, and enhance their coping skills to lay the foundation for decreasing social isolation and improving PA levels.
PD patients not only suffer from motor disability but also from psychological distress, and anxiety is common among them. A meta-analysis showed that the average incidence of anxiety disorders in PD patients was 31%.32 The results of this study showed that the more serious the symptoms of anxiety were, the poorer the PA. Symptoms of anxiety were associated with unpredictability in social settings, fear of potential falls, or a sense of unwelcomeness from others, which could all restrict PD patients’ PA.24
This study has several limitations that should be addressed. First, the sample was conveniently drawn from a certain neurology department, and the participants might exhibit different disease-related characteristics from the nonparticipants who usually stay at home, which limits the representativeness of the sample. Second, a cross-sectional design was used in our study, which could not capture the dynamic trend of PA among the targeted population. Third, no definite causal inference could be made about the effect of some factors on PD patients’ PA based on cross-sectional data. Finally, there could be additional factors influencing PA that were not accounted for in this study. In the future, experimental studies or longitudinal studies involving a wider sample and additional potential factors are needed to explore these causal effects.
Conclusions
In conclusion, the average level of PA among PD patients was at the lower middle-level, being affected by various factors, and physical function, psychological resilience and social support were the strongest factors. To promote patient PA, rehabilitation therapy for physical function is the most important factor, followed by psychological resilience and social support, which positively impact PA levels. Therefore, medical staff can employ methods such as family-based care, patient training, and multimodal rehabilitation interventions to help patients improve their daily activities, foster resilience, utilize social support, reduce negative emotions, enhance adaptive abilities, and promote social participation.
Data Sharing Statement
The datasets used in the present study are available from the corresponding author upon reasonable request.
Ethics Statement
All participants involved in the study were informed about the purpose of the study, and all research procedures were conducted in accordance with the 1964 Declaration of Helsinki. This study was approved by the institutional ethics committee of the First Hospital Affiliated with Dalian Medical University (Ethics Approval No. PJ-KS-KY-2017-133).
Acknowledgments
The authors thank all the study participants with PD and the support of their caregivers and the health workers of the Department of Neurology who fully supported us in conducting this study.
Author Contributions
All authors made significant contributions to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article was submitted; and agreed to be accountable for all aspects of the work.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest.
References
1. Dorsey ER, Elbaz A, Nichols E, et al. Global, regional, and national burden of Parkinson’s disease, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018;17(11):939–953. doi:10.1016/S1474-4422(18)30295-3
2. Kluger B, Brown RP, Aerts S, et al. Determinants of objectively measured physical functional performance in early to mid-stage Parkinson disease. Pm&r. 2014;6(11):992–998. doi:10.1016/j.pmrj.2014.05.013
3. Kluger BM, Brown RP, Aerts S, Schenkman M. Management of Parkinson disease in 2017: personalized approaches for patient-specific needs. JAMA. 2017;318(9):791. doi:10.1001/jama.2017.7914
4. Schrag A, Jahanshahi M, Quinn N. How does Parkinson’s disease affect quality of life? A comparison with quality of life in the general population. Mov Disord. 2000;15(6):1112–1118. doi:10.1002/1531-8257(200011)15:6<1112::AID-MDS1008>3.0.CO;2-A
5. The Lancet. Parkinson’s disease: a complex disease revisited. Lancet. 2017;390(10093):430. doi:10.1016/S0140-6736(17)31997-9.
6. World health organization. International Classification of Functioning, Disability and Health (ICF). Geneva: World health organization; 2001.
7. Cardol M, de Haan RJ, de Jong BA, van den Bos GAM, de Groot IJM. Psychometric properties of the impact on Participation and Autonomy Questionnaire. Arch Phys Med Rehabil. 2001;82(2):210–216. doi:10.1053/apmr.2001.18218
8. Törnbom K, Hadartz K. Sunnerhagen KS.Self-Perceived Participation and Autonomy at 1-Year Post Stroke: a Part of the Stroke Arm Longitudinal Study at the University of Gothenburg (SALGOT Study). J Stroke Cerebrovascular Dis. 2018;27(4):1115–1122. doi:10.1016/j.jstrokecerebrovasdis.2017.11.028
9. Cardol M, de Haan RJ, de Jong BA, van den Bos GAM, de Groot IJM. The development of a handicap assessment questionnaire: the Impact on Participation and Autonomy (IPA). Clin rehabilitat. 1999;13(5):411–419. doi:10.1191/026921599668601325
10. Shamaskin-Garroway AM, Lageman SK, Rybarczyk B. The roles of resilience and nonmotor symptoms in adjustment to Parkinson’s disease. J Health Psychol. 2016;21(12):3004–3015. doi:10.1177/1359105315590268
11. Simpson J, Haines K, Lekwuwa G, Wardle J, Crawford T. Social support and psychological outcome in people with Parkinson’s disease: evidence for a specific pattern of associations. Br J Clin Psychol. 2006;45(4):585–590. doi:10.1348/014466506X96490
12. Erler K, McKinnon S, Sullivan V, Inzana R. Examining social support and participation after stroke. Am J Occup Ther. 2019;73(4 Supplement 1):7311515296p1. doi:10.5014/ajot.2019.73S1-PO4043
13. Feifel H, Strack S, Nagy VT. Coping strategies and associated features of medically ill patients. Psychosomatic Med. 1987;49(6):616–625. doi:10.1097/00006842-198711000-00007
14. Evans D, Norman P. Illness representations, coping and psychological adjustment to Parkinson’s disease. Psychol Health. 2009;24(10):1181–1196. doi:10.1080/08870440802398188
15. Chinese Medical Committee. Diagnosis criteria of Parkinson disease in China. Chin J Neurol. 2016;49(4):268–271. doi:10.3760/cma.j.issn.1006-876.2016.04.002.
16. Li H, Cui M, Zhou L. Revising and analysing the reliability and validity of Chinese version of impact on participation and autonomy questionnaire. Chin J Rehabil Med. 2012;27(10):923–927. doi:10.3969/j.issn.1001-1242.2012.10.007
17. Connor KM, Davidson JRT. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depression Anxiety. 2003;18(2):76–82. doi:10.1002/da.10113
18. Yu X, Zhang J. Factor analysis and psychometric evaluation of the Connor-Davidson Resilience Scale (CD-RISC) with Chinese people. Social Behavior and Personality. 2007;35(1):19–30. doi:10.2224/sbp.2007.35.1.19
19. Zung W. The measurement of affects: depression and anxiety. Modern Trends in Pharmacopsychiatry. 2012;7:170–188. doi:10.1159/000395075
20. Xiao S. Theoretical basis and research application of Social Support Rating Scale. J Clin Psychol. 1994;4(2):98–100.
21. Hoehn MM. Parkinsonism: onset, progression, and mortality. Neurology. 1967;17(5):427–442. doi:10.1212/wnl.17.5.427
22. Movement Disorder Society Task Force on Rating Scales for Parkinson’s Disease. The Unified Parkinson’s Disease Rating Scale (UPDRS): status and recommendations. Mov Disord. 2003;18(7):738–750. doi:10.1002/mds.10473.
23. Guo H, Chen Y, Wang Q, Liu Y, Yang H. Analysis of status quo and influencing factors of social participation of patients with Parkinson´s disease. Chin Nurs Res. 2022;36(22):4018–4024. doi:10.12102/j.issn.1009-6493.2022.22.013
24. Ahn S, Springer K, Gibson JS. Social withdrawal in Parkinson’s disease: a scoping review. Geriatric Nurs. 2022;48:258–268. doi:10.1016/j.gerinurse.2022.10.010
25. Li Y, Zhang W, Ye M, Zhou L. Perceived participation and autonomy post‐stroke and associated factors: an explorative cross‐sectional study. Journal of Advanced Nursing. 2021;77(3):1293–1303. doi:10.1111/jan.14670
26. Robottom BJ, Gruber-Baldini AL, Anderson KE, et al. What determines resilience in patients with Parkinson’s disease? Parkinsonism Related Disord. 2012;18(2):174–177. doi:10.1016/j.parkreldis.2011.09.021
27. Ghorbani Saeedian R, Nagyova I, Krokavcova M, Skorvanek M, Rosenberger J, Gdovinova Z. ea al.The role of social support in anxiety and depression among Parkinson’s disease patients. Disability Rehabil. 2014;36(24):2044–2049. doi:10.3109/09638288.2014.886727
28. Cheng Y, Liu C, Mao C, Qian J, Liu K, Ke G. Social support plays a role in depression in Parkinson’s disease: a cross-section study in a Chinese cohort. Parkinsonism Related Disord. 2008;14(1):43–45. doi:10.1016/j.parkreldis.2007.05.011
29. Vescovelli F, Sarti D, Ruini C. Subjective and psychological well-being in Parkinson’s Disease: a systematic review. Acta Neurol Scand. 2018;138(1):12–23. doi:10.1111/ane.12946
30. Frazier L. Coping with disease-related stressors in Parkinson’s disease. Gerontologist. 2000;40(1):53–63. doi:10.1093/geront/40.1.53
31. He Y, Zhang S, Yin A, Liu S, Huang X. Mediating effect of coping style on relationship between psychosocial adaption and stigma of patients living with Parkinson’ disease. Journal of Nurses Training. 2020;35(17):1537–1542. doi:10.16821/j.cnki.hsjx.2020.17.001
32. Broen MPG, Narayen NE, Kuijf ML, Dissanayaka NNW, Leentjens AFG. Prevalence of anxiety in Parkinson’s disease: a systematic review and meta‐analysis. Mov Disord. 2016;31(8):1125–1133. doi:10.1002/mds.26643
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Mediating Effect of Perceived Social Support and Medical Coping Modes Between Psychological Resilience and Meaning in Life in COVID-19 Patients
Zhang L, Jiang M, Wang L, Zheng J, Wang W
Patient Preference and Adherence 2023, 17:571-582
Published Date: 7 March 2023
The Influence of Social Support on the Mental Health of Elderly Individuals in Healthy Communities with the Framework of Mental Toughness
Zhang C, Dong C
Psychology Research and Behavior Management 2023, 16:2977-2988
Published Date: 4 August 2023
Social Support and Social Adjustment Among Chinese Secondary School Students: The Mediating Roles of Subjective Well-Being and Psychological Resilience

Yu L, Wu X, Zhang Q, Sun B
Psychology Research and Behavior Management 2024, 17:3455-3471
Published Date: 7 October 2024
Psychological Resilience and Sleep Quality Among the Elderly: The Mediating Role of Social Support
Li J, Zhang J, Hou Y, Cui Y, Wang Q, Ouyang A, Cai M, Hua Y
Nature and Science of Sleep 2025, 17:2469-2483
Published Date: 3 October 2025
The Relationship Between Demoralisation, Medical Coping Style, Resilience and Perceived Social Support in Patients with Colorectal Cancer
Li Y, Liu Z, Lu X, Chai X, Bai N, Chen Y
Patient Preference and Adherence 2025, 19:3285-3294
Published Date: 22 October 2025