")
Back to Journals » Psychology Research and Behavior Management » Volume 16
The Influence of Social Support on the Mental Health of Elderly Individuals in Healthy Communities with the Framework of Mental Toughness
Received 23 March 2023
Accepted for publication 28 June 2023
Published 4 August 2023 Volume 2023:16 Pages 2977—2988
DOI https://doi.org/10.2147/PRBM.S413901
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Cheng Zhang,1 Caisheng Dong2
1College of Law, Jiangnan University, Wuxi, Jiangsu, 214122, People’s Republic of China; 2School of Philosophy and Sociology, Jilin University, Changchun, Jilin, 130012, People’s Republic of China
Correspondence: Caisheng Dong, Email [email protected]
Introduction: This work aims to explore the impacts of social support measures such as analyzing greening urban spaces and improving greenspace quality on the mental health of the elderly based on the mental resilience framework to build a healthy community.
Methods: Through literature research and a questionnaire survey, this study designs a questionnaire including basic information, a life satisfaction scale, a positive and negative emotion scale, social support rating scale, a life orientation test-revised version, and psychological resilience scale. In order to classify the scales, machine learning (ML) approaches are applied in this work.
Results: The results demonstrate great variations in the scores of the elderly with various health problems in the domain of psychological resilience (p< 0.001). Social support and subjective well-being are strongly related (p< 0.001). Additionally, positive correlations are observed among perceived, objective, and support use (p< 0.001).
Conclusion: Finally, it is found that psychological resilience and social support play a significant role in mediating mental health problems in elderly individuals. Therefore, social support measures such as analyzing greening urban spaces and improving greenspace quality can be adopted to improve the mental health of the elderly to build healthy communities. On this basis, this work is of certain reference value and practical significance for the construction of healthy communities and the positive influence on the mental health of elderly individuals.
Keywords: machine learning, ML, psychological resilience, social support, mental health of elderly individuals, greening urban spaces, greenspace quality, healthy community
Introduction
In the stage of rapid social and economic development, the area of green urban space is shrinking, and the quality of green space is declining seriously.1 Meanwhile, the social structure has also undergone obvious changes, among which the proportion of the elderly has increased significantly,2 and the construction of healthy communities has become one of the key concerns in the healthy development of society. China, the largest developing nation in the world, possesses one of the oldest populations and the highest aging rates globally. In general, the elderly population in the community exhibits characteristics such as aging, disabilities, dementia, low birth rates, and empty nests.3 According to the data from the seventh national population census in China, the population aged 60 and above accounts for 18.7%. Among them, the proportion of the population aged 65 and above is as high as 13.50%. Compared to the global average of 9.3% for the population aged 65 and above, China demonstrates a significantly higher degree of population aging. However, it is still lower than the average level of developed countries (19.3%).4 The intensification of the aging trend has increased social security expenditure, individual physiological needs, and many other problems. Among them, the mental health problems caused by aging have received more attention. It will change with their age and physical conditions, such as Alzheimer’s, depression, anxiety, and other diseases. Thus, it negatively affects the quality of life and happiness of the elderly and seriously delays the construction of healthy communities.5,6 Therefore, research on the mental health of the elderly has become the focus of scholars in related fields. Age-related health issues are intimately correlated with each family’s happiness and suffering and reflect the stability of social and economic progress. Psychologists have given much attention to the study of psychomotor function. Psychological resilience is viewed as a personal trait or skill. The psychological fact that psychological functioning and development may still flourish in the absence of adversity or threat is implied by this phrase.7,8
The health issues of the elderly are closely related to the joys and sorrows of each family. Still, they are also a sign of the country’s and society’s stable development and the basis for constructing a healthy community. Therefore, psychomotor-related research has attracted wide attention from psychologists, and there are many studies on the mental health of elderly individuals from the perspective of psychological resilience. For example, Karadag et al used a questionnaire to analyze the relationship between psychological resilience and social support in hemodialysis patients. They found a strong and significant correlation between the multidimensional perceived social support scale and psychological resilience.9 Brooks et al explored the influencing factors related to psychological resilience. They identified protective factors such as training, experience, perceived (personal) ability, and social support as influences related to psychological resilience.10 Lipskaya-Velikovsky conducted a survey that included standard measures of psychological distress, participation in activities of daily living, social connectedness, resilience, and quality of life (QOL). It was found that psychological distress, the participation dimension, social connection, and self-efficacy could explain QOL, while the participation dimension was a mediating variable of QOL.11 McKenna et al studied the origin and concept of psychological resilience, summarized the existing resilience measurement tools, and integrated the relevant factors, predictors, and results of psychological resilience of family caregivers of patients with Carney complexes (CNCs). Although the definitional concepts of healthy adaptation and balance are consistent, there is still inconsistency in the definition and assessment of psychological resilience.12 These studies have demonstrated that social support has a favorable effect on the mental health and general mental well-being of elderly individuals and that there is a substantial relationship between social support and psychological resilience. Social support and psychological fortitude can also play a variety of moderating functions. A general definition of social support is any interpersonal social resource that involves either the existence or influence of healthy human interactions. The buffering concept contends that as social support grows, so should the impact of socioeconomic disadvantage on mental health.13
In short, in view of today’s aging problem, exploring the impact of social support measures such as urban green space analysis and improving the quality of green space on the mental health of the elderly has important practical significance for building a healthy smart city community. Through literature research and questionnaire surveys, relevant influencing factors are analyzed to examine the impact of social support on the mental health of the elderly. Machine learning is used to classify various social support measures. This study aims to provide experimental guidelines to help society intervene in the mental health of older adults. Additionally, the study recommends social support measures such as increasing urban green space and improving the quality of green space to improve the mental health of the elderly and build a healthy community. This analysis provides a rare opportunity to examine whether social support attenuates negative social effects on mental health equitably.
The overall organizational structure of this work is as follows. Introduction is the introduction, which expounds on the background and status quo related to the urban ecological environment and the mental health of the elderly. This part summarizes the current research gaps and puts forward the innovations and contributions of this research. Materials and Methods is the method to investigate the impact and relationship of social support, such as mental health and the ecological environment, through a questionnaire survey. Results and Discussion is the results and discussion, descriptive and correlation analysis of the questionnaire results. Based on the results, corresponding recommendations are discussed and presented. Conclusion is the conclusion, briefly describing the results, limitations, and prospects.
Materials and Methods
Analysis of the Psychological Resilience Framework
Psychology believes that people can protect themselves and adapt to the environment. Mental resilience is divided into four states - The initial stage balancing physical, mental, and spiritual states.14 With the introduction of stress and setbacks, equilibrium will be disrupted, and individuals begin to reintegrate resources and adapt to the environment. The result of the recombination is shown in Figure 1.
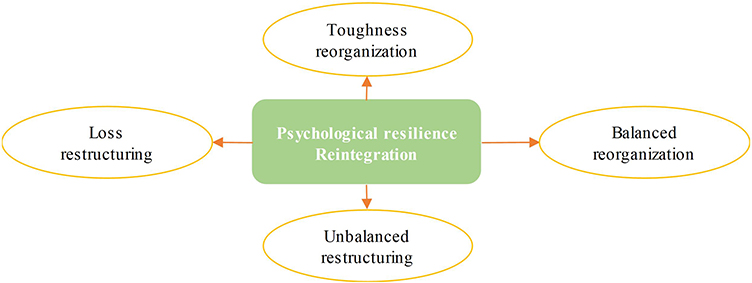 |
Figure 1 Schematic diagram of psychological resilience recombination results. |
Figure 1 illustrates that some people may rearrange resilience and increase their psychological qualities, while others enter a loss-making reorganization mode and see a decline in psychological quality. Self-efficacy refers to the capacity to communicate and seek assistance, and one’s physical well-being frequently influences one’s capacity for psychological resilience. High self-efficacy is positively correlated with psychological adaptation and resilience in individuals. Therefore, enhancing psychological resilience can enable people to better adapt to the real world, develop themselves, and realize their value.15 The psychological resilience framework considers both the reconfiguration that happens due to a person’s psychological resilience and the interaction process between the individual and the outcome. The construction process of the frame is illustrated in Figure 2.
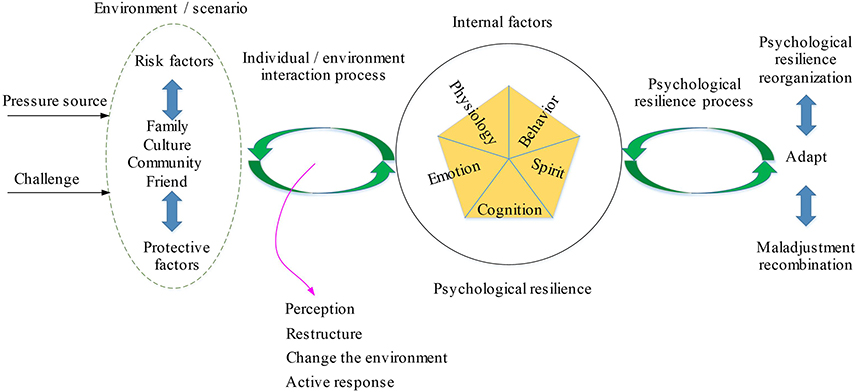 |
Figure 2 Schematic diagram of the psychological resilience framework. |
As shown in Figure 2, the psychological resilience framework mainly includes six main aspects, four of which are influencing factors (stressor or challenge, environment, individual internal resilience factor, and outcome), and the other two are interaction processes, which are the process of human-environment interaction and the process of resilience between people and outcomes. Psychological resilience is a dynamic adjustment process. Psychological resilience can continuously change in the dynamic adjustment of individuals and the environment. Whether setbacks, stressful events, or positive events, it helps to affect the intensity of psychological resilience to a certain extent. Thus, psychological resilience is an ability that can be improved through training.
Related Theoretical Knowledge of Mental Health
As a classification of human health, many scholars have studied mental health. In Grossman’s health demand theory, consumption and investment are considered comprehensively and combined with the health investment function, other commodity investment functions, and time and income constraints to maximize consumer utility.16,17 Individuals aim at maximizing utility in different periods, the initial health is exogenous, and the health capital stock owned by individuals in the later period depends on health investment, which is an endogenous variable. The health stock will generate benefits, and the utility function of the entire life cycle of an individual is expressed as Eq. (1):

In Eq. (1), Hi refers to the health capital stock, i=0 represents the initial health capital stock, πi refers to the unit income of health capital, and Zi refers to the consumption of other commodities except for health, which is the investment in other consumer goods and can be expressed as follows:

In Equation (2), Xi refers to the general consumer goods that can be purchased, ti refers to the production time of other commodities, and E refers to human capital other than health.
The health capital stock will continue to depreciate with the growth of the individual’s age. For example, when the individual gradually becomes elderly, δi refers to the depreciation rate. Therefore, it is necessary to invest in health capital. Equation (3) represents the increase in health capital. Healthy capital increment equals healthy net investment (gross investment - depreciation).

In Equation (3), Ii refers to health capital investment.

In Eq. (4), tHi refers to the health increase through investment and the time during which health can be increased through investment.
Therefore, Eqs. (1)–(4) constitute the individual health demand model, and the solution of the above equation is the health demand function when the individual’s utility is maximized. From a practical standpoint, the mental health assessment scale is used to gauge and assess each person’s mental state, that is, to gauge and categorize each person’s mental state using scales to ascertain if they are experiencing mental diseases or illnesses. Generally, mental health refers to being free of mental disorders or mental illnesses. Therefore, it is thought that the mental health of the elderly is a healthy and lasting pleasant mental state that may be evaluated and drawn in this work.
Influence of Social Support on the Mental Health of Elderly Individuals in Healthy Communities
Everyone has a support system. Social support is a dimension to test individual social adaptability. Multiple subjects provide social support, and the support content is actual and perceptible. From its source analysis, it can be summarized as support from social networks, communities, and close partners.18 The concept theory of “social support” is applied to guide the understanding of the comprehensive network of disadvantaged groups, assist disadvantaged groups in finding available support resources around them, and connect support points into a support network. Social support is utilized to provide services to elderly individuals, and its network structure is shown in Figure 3.
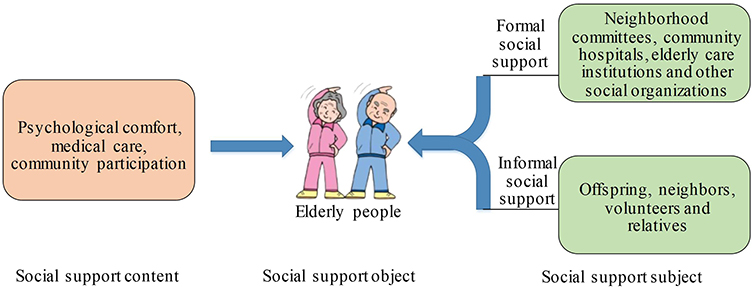 |
Figure 3 Diagram of social support networks for older persons in a healthy community. |
From Figure 3, the social support network of the elderly includes social support content, social support object, and social support subject. The object of social support refers to elderly individuals, and the subject of social support includes two aspects: formal social support and informal social support. Among them, social work services belong to formal social support. Its real significance in community home-based care services is to form a close support network from the support links from families, social organizations, and grassroots governments to improve personal life satisfaction and the level of community home-based care services. Of course, the construction of healthy communities cannot be separated from the support of the ecological environment. Studies have shown that increasing urban green space can significantly enhance people’s pleasure and reduce their risk of mental health diseases.19
Mental Health Questionnaire and Scale Evaluation
Questionnaire Design
The questionnaire used in this work consists of six parts: a basic information questionnaire, a life satisfaction scale, positive and negative affect scales, social support rating scale, a life orientation test-revised version, and psychological resilience scale.
Subjective well-being is investigated using the Life Satisfaction, Positive Affect, and Negative Affect scales. After the scores of each variable are standardized, the calculation formula of subjective well-being is expressed as happiness= life satisfaction+ positive emotion- negative emotion. Among them, the life satisfaction scale20 measures the cognitive component of subjective well-being. The scale consists of 5 items, scored on 5 points, with numbers 1–5 representing “very disagree” to “very agree”; the higher the score, the more satisfied with life. The Cronbach α of the life satisfaction scale is 0.831. The Positive Affect and Negative Affect Scale is used to measure the emotional component of subjective well-being,21 with a 5-point score, ranging from “almost none” to “very much”, with 1–5, respectively. Among them, the Cronbach α of the positive and negative emotion subscales are 0.872 and 0.886, respectively.
The Social Support Rating Scale22 is used to evaluate the social support status of individuals. The scale includes objective support, subjective support, and support utilization. The higher the total score, the better the individual’s social support status. A 4-point scale is used, where 1= none; 2= very little; 3= normal range; 4= full support. The Cronbach α of the social support rating scale is 0.778.
Life Orientation Test-Revised23 adopts a 5-point Liken scoring standard, 1=strongly disagree, 5=strongly agree. The higher the total score, the more optimistic the individual is. The Cronbach’s α for the Life Orientation Test-Revised Scale is 0.635.
The Mental Resilience Scale24 measures the positive psychological qualities that help individuals adapt to difficult situations or face stressful events. A 5-point scale is used, with one being strongly disagreed and five being very agreed. The higher the total score, the higher the level of individual psychological resilience. Among them, the Cronbach α of the Mental Toughness Scale is 0.910.
Additionally, the ML algorithm is introduced here for classification analysis to verify the feasibility of each scale.
Survey Objects and Methods
This work uses an offline questionnaire survey to investigate elderly individuals at home in Changchun. Data collection is from March 1, 2022, to September 1, 2022. The inclusion criteria for the experimenters are 1. age 65 and above; 2. living in Changchun city; 3. self-considered healthy, without suffering from diseases that affect memory and cognitive abilities; 4. not suffering from serious psychological disorders; 5. have not received cognitive training or participated in any clinical research; 6. willing to participate in the research and sign the informed consent. The exclusion criteria are 1. age does not meet the requirements; 2. they do not live in Changchun City; 3. suffer from diseases that affect memory and cognitive ability; 4. suffer from serious psychological disorders; 5. have received cognitive training or have participated in other clinical research; 6. have not signed the informed consent or are unwilling to participate in the research.
The questionnaires are anonymous, and the results are kept confidential. Additionally, the subjects are informed that the data are only used for academic research, and a small gift is given. A total of 251 questionnaires were distributed, and 243 questionnaires were recovered, with a recovery rate of 96.81%. After eliminating the questionnaires with obvious errors and missing questions, there were 228 valid questionnaires, and the effective rate of the questionnaires was 93.83%. Cronbach’s alpha was used to test the reliability and validity of the questionnaire.
Statistical Methods of Data
Statistic Package for Social Science (SPSS) 19.0 was adopted to perform descriptive statistics, difference tests, and correlation analysis on the data. In the difference test, the independent sample t-test was used to compare two groups, and one-way ANOVA was used to compare multiple groups. When the variances were homogenous, the least significant difference (LSD) method was employed for post hoc multiple comparisons; when the variances were unequal, the Welch test was used, and Tamhane’s T2 method was used for multiple comparisons. p < 0.05 indicated a significant difference.
Results and Discussion
In this section, the reliability of this survey is evaluated based on Cronbach’s alpha. Table 1 shows Cronbach’s α test questionnaire results. According to Table 1, the mean value of Cronbach’s alpha in the questionnaire is 0.819. This implies that the questionnaire created in this study has good internal consistency and stability and high credibility and is reasonable and effective. Furthermore, descriptive statistics, difference tests, and correlation analysis are performed in this work to examine the disparities in scores for each scale and dimension of health status. The study adhered to the guidelines of the Declaration of Helsinki and was approved by the Ethics Committee of Jiangnan University. Written informed consent was voluntarily obtained from all participants.
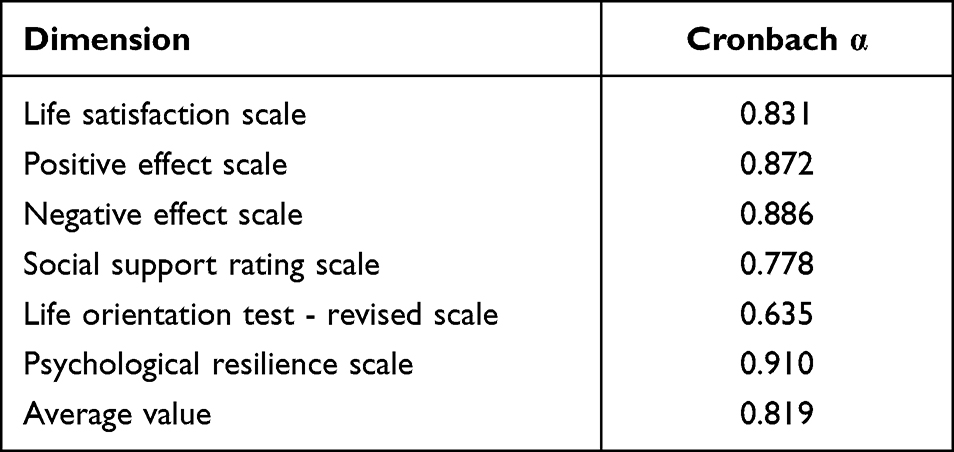 |
Table 1 Cronbach’s Alpha Test Results for Questionnaire Results |
Descriptive Statistics and Analysis
Demographic descriptive statistics were conducted on the results of this questionnaire, as shown in Table 2. All the respondents were elderly, and there was no significant difference in the proportion of males and females. Additionally, from the perspective of activity ability and chronic disease, the number of healthy elderly individuals is less than half. In addition, residents account for a large proportion of the survey subjects. From the perspective of income and housing ownership, it is found that the overall society is generally good, but there are still large differences among individuals.
 |
Table 2 Descriptive Statistics |
Variance Analysis
The score differences of each scale and dimension in health status are analyzed, as shown in Figures 4 and 5, respectively.
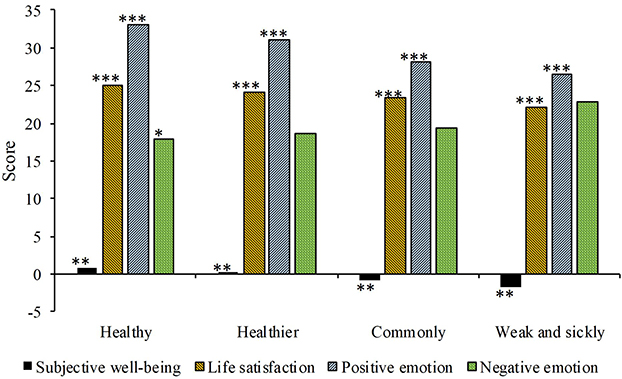 |
Figure 4 The score differences of each dimension of subjective well-being in health status (***p < 0.001, **p < 0.01, and *p < 0.05). |
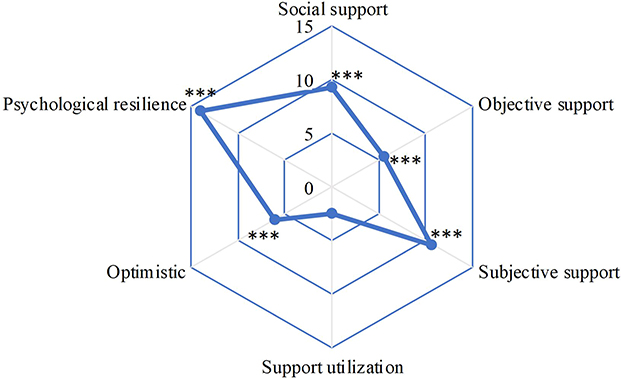 |
Figure 5 The results of the differences in the scores of social support, optimism, and psychological resilience in health status (***p < 0.001, **p < 0.01, and *p < 0.05). |
The multiple tests using LSD reveal that in terms of subjective well-being, life satisfaction, and positive emotions, the elderly in good health score the highest (p < 0.01). The elderly in good health also scored higher than the elderly, who were generally frail and sick (p < 0.001). In addition, an obvious difference (p < 0.001) is found between elderly individuals in general and elderly individuals who are frail and sick (p < 0.001). Elderly individuals who are frail and sick have the lowest scores on the total score and each dimension. For the negative sentiment, the Tamhane method is used for post hoc multiple comparisons due to variance heterogeneity. The results show that elderly individuals in good health have the lowest score (p < 0.05).
As demonstrated in Figure 5, the elderly who are healthy had the highest score in subjective support (p < 0.001). The elderly who are in better health score higher than those generally frail and sick (p < 0.001). After the LSD post hoc multiple test comparison, the healthy elderly scored the highest objective support score (p < 0.001). The difference in the support utilization scores of the elderly among different health conditions reached a marginally significant level (p = 0.063 > 0.05). In the dimension of optimism and psychological resilience, the scores of the elderly with different health conditions were obviously different (p < 0.001). The post hoc test suggests that the elderly in good health score the highest (p < 0.001), and the healthy elderly show higher scores (p < 0.01).
Correlation Analysis
Further correlation analysis of subjective well-being to social support, optimism, and psychological resilience of the elderly is shown in Figure 6. The correlation analysis between social support and optimism and the psychological resilience of the elderly is shown in Figure 7. In Figure 6, the correlation analysis of the elderly’s subjective well-being and social support shows they are positively correlated (p < 0.001). Except for the insignificant correlation between support utilization and negative affect, the subjective well-being subdimension shows a positive correlation with all dimensions of the social support scale. The correlation analysis between the elderly’s subjective well-being and optimism shows an obvious correlation (p < 0.001). The correlation analysis between the elderly’s subjective well-being and psychological resilience shows that psychological resilience is positively correlated with the total score of subjective well-being (p < 0.001); it is positively and negatively associated with life satisfaction and positive emotion (p < 0.001) and negative emotion (p < 0.001), respectively.
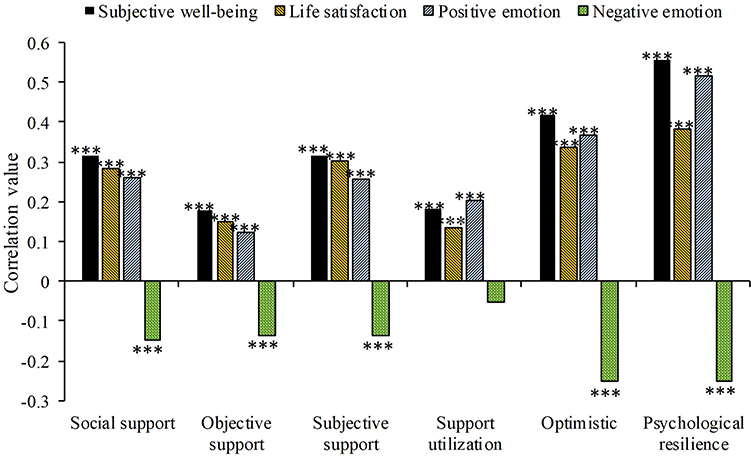 |
Figure 6 Correlation analysis results of elderly subjective well-being with social support, optimism, and psychological resilience (*** p < 0.001). |
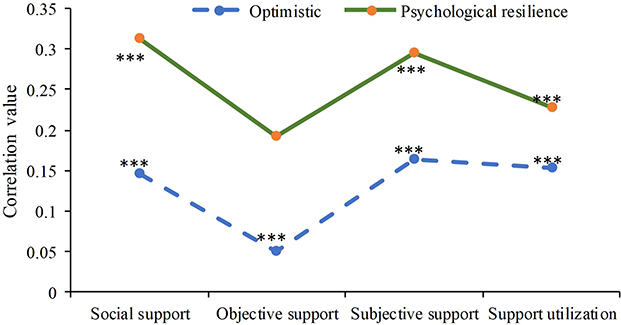 |
Figure 7 Correlation analysis results of elderly social support with optimism and psychological resilience (*** p < 0.001). |
Correlation analysis is carried out on the optimism of the elderly and their social support status (Figure 7). Optimism is positively correlated with the total social support score (p < 0.0.001), but its correlation with objective support is insignificant. Further correlation analysis is conducted between elderly psychological resilience and social support. The results suggest that psychological resilience is positively associated with the total score of social support, objective support, subjective support, and support utilization (p < 0.001).
Machine Learning Analysis
Figure 8 shows the generated confusion matrix employing an ML algorithm.
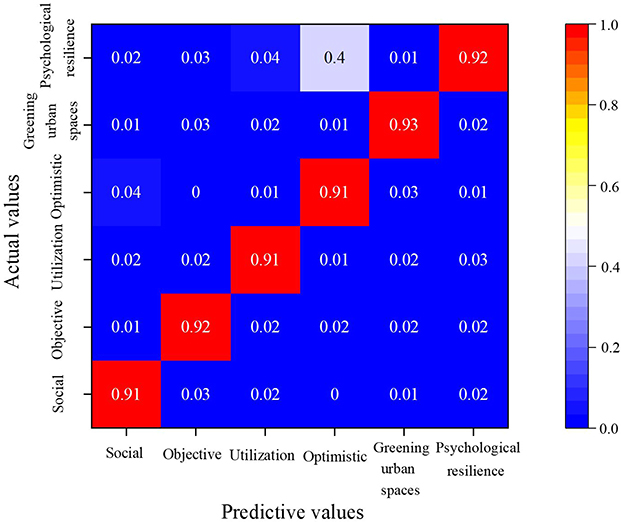 |
Figure 8 Classification confusion matrix using an ML algorithm. |
As shown in Figure 8, by using ML to analyze the actual and predicted values of various social support measures and mental resilience, the mental resilience framework can classify social support, and it is verified that the ML algorithm can effectively identify various social support measures for elderly individuals with optimism and mental resilience framework.
Discussion and Suggestions
Identifying senior social support with optimism and psychological resilience using ML algorithms is a hot topic. To maintain interpersonal relationships and to obtain more care and assistance, several academics have also noted that social activities and physical health are helpful.25 However, older people with poor health frequently have restricted ranges of mobility, which limits their access to care and assistance from others.26 According to the findings of this poll, the aged in excellent health had the highest subjective well-being, life satisfaction, and pleasant emotions. This finding demonstrates that health status is a major factor influencing the subjective well-being of elderly individuals. Scholars in relevant domains agree with the findings.27 As a result, health status should be recognized as a significant element influencing subjective well-being. A further examination from the standpoint of social support reveals that healthy elderly individuals receive higher social assistance.
Furthermore, there is a substantial positive link between subjective well-being and social support, and all social support variables show significant relationships except support use and negative affect. Most researchers’ studies28,29 confirm the major effect of emotional support individuals feel on their physical and mental condition and well-being experience. The significance of psychological resilience in mediating social support and subjective well-being is important when elderly individuals lack psychological resilience. Their subjective well-being declines significantly. Numerous factors, such as physical frailty, illness, disability, and decreased mobility, put pressure on elderly individuals. Negative mental states may have a greater impact on the quality of life and mental health of elderly individuals than physical frailty or disease. Studies have shown that aging-related physical loss can cause elderly individuals’ negative self-perceptions and evaluations. This can result in a subjective feeling of low well-being.30
Through the above discussion and analysis, this work proposes the following suggestions for building healthy communities. First, it should attach importance to the subjective perception of the community elderly to living environment greening and adopt different ideas of greening promotion and social support for different types of space in the living area. For example, appropriate “greening autonomy” strategies should be introduced to enhance subjective greening evaluation and promote physical activity and social interaction among elderly individuals. Second, it is suggested to accelerate the construction of urban parks, optimize the spatial layout of urban parks, enhance the accessibility of parks, improve the quality of the space environment and promote the intensity of use of urban parks by elderly individuals. Meanwhile, it can encourage shared courtyard greening and improve the openness of green space so that the elderly has more convenient access to green space. Third, control of the green sight rate should be strengthened, and full use of lampposts, bridge columns, guardrails, building facades, and other vertical spaces should be made to develop three-dimensional greening. The greening level can be improved by “climbing vines to hang green”. In this case, to achieve the goal of building a healthy community, the mental health of the elderly will be positively affected, and the mental health risk will be significantly reduced.
Conclusion
In conclusion, the impacts of questionnaires on the mental health of elderly individuals are analyzed through literature research and questionnaire surveys. The results show that health status is an important factor affecting the subjective well-being of the elderly. Additionally, all dimensions of social support have significant correlations except support utilization and negative affect. Mental toughness has a significant mediating effect on social support and subjective well-being. Some social support measures can be adopted to build healthy communities which positively affect the mental health of elderly individuals, providing an experimental reference for follow-up interventions for the mental health of the elderly in society. However, there are some shortcomings in this work. For example, the research mainly focuses on the elderly with certain activity abilities and education levels. In order to make the research results more reliable, follow-up research can select special elderly groups for discussion, such as the elderly in nursing homes, so as to obtain information from research surveys of a wider sample.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Qiu S, Wang Z, Liu S. The policy outcomes of low-carbon city construction on urban green development: evidence from a quasi-natural experiment conducted in China. Sustain Cities Soc. 2021;66:102699. doi:10.1016/j.scs.2020.102699
2. Chen LK, Arai H, Assantachai P, et al. Roles of nutrition in muscle health of community-dwelling older adults: evidence-based expert consensus from Asian Working Group for Sarcopenia. J Cachexia Sarcopenia Muscle. 2022;13(3):1653–1672. doi:10.1002/jcsm.12981
3. Rodrigues F, Domingos C, Monteiro D, Morouço P. A review on aging, sarcopenia, falls, and resistance training in community-dwelling older adults. Int J Environ Res Public Health. 2022;19(2):874. doi:10.3390/ijerph19020874
4. Akimov AV, Gemueva KA, Semenova NK. The Seventh Population Census in the PRC: results and prospects of the country’s demographic development. Herald Russ Acad Sci. 2021;91(6):724–735. doi:10.1134/S1019331621060083
5. Caspi A, Houts RM, Ambler A, et al. Longitudinal assessment of mental health disorders and comorbidities across 4 decades among participants in the Dunedin birth cohort study. JAMA Ntwk Open. 2020;3(4):e203221–e203221. doi:10.1001/jamanetworkopen.2020.3221
6. Kim M, Oh J-H, Won CW. Sex-specific differences in lower body fat distribution and association with physical performance among healthy community-dwelling older adults: a pilot study. Int J Environ Res Public Health. 2022;19:4201. doi:10.3390/ijerph19074201
7. AlAteeq DA, Aljhani S, Althiyabi I, Majzoub S. Mental health among healthcare providers during coronavirus disease (COVID-19) outbreak in Saudi Arabia. J Infect Public Health. 2020;13(10):1432–1437. doi:10.1016/j.jiph.2020.08.013
8. Kuranova A, Booij SH, Menne-Lothmann C, et al. Measuring resilience prospectively as the speed of affect recovery in daily life: a complex systems perspective on mental health. BMC Med. 2020;18(1):1–11. doi:10.1186/s12916-020-1500-9
9. Karadag E, Ozlem UG, Hatice ME, Erunal M. The relationship between psychological resilience and social support levels in hemodialysis patients. J Basic Clin Health Sci. 2019;3(1):9–15. doi:10.30621/jbachs.2019.469
10. Brooks S, Amlot R, Rubin GJ, Greenberg N. Psychological resilience and posttraumatic growth in disaster-exposed organisations: overview of the literature. BMJ Mil Health. 2020;166(1):52–56. doi:10.1136/jramc-2017-000876
11. Lipskaya-Velikovsky L. COVID-19 isolation in healthy population in Israel: challenges in daily life, mental health, resilience, and quality of life. Int J Environ Res Public Health. 2021;18(3):999. doi:10.3390/ijerph18030999
12. McKenna O, Fakolade A, Cardwell K, Langlois N, Jiang K, Pilutti LA. Towards conceptual convergence: a systematic review of psychological resilience in family caregivers of persons living with chronic neurological conditions. Health Expect. 2022;25(1):4–37. doi:10.1111/hex.13374
13. Freak-Poli R, Ryan J, Tran T, et al. Social isolation, social support and loneliness as independent concepts, and their relationship with health-related quality of life among older women. Aging Ment Health. 2022;26(7):1335–1344. doi:10.1080/13607863.2021.1940097
14. Tamura S, Suzuki K, Ito Y, Fukawa A. Factors related to the resilience and mental health of adult cancer patients: a systematic review. Support Care Cancer. 2021;29(7):3471–3486. doi:10.1007/s00520-020-05943-7
15. Kuiper H, van Leeuwen C, Stolwijk-Swüste JM, Post MW. Measuring resilience with the Connor–Davidson Resilience Scale (CD-RISC): which version to choose? Spinal Cord. 2019;57(5):360–366. doi:10.1038/s41393-019-0240-1
16. Karaşar B, Canlı D. Psychological resilience and depression during the COVID-19 pandemic in Turkey. Psychiatr Danub. 2020;32(2):273–279. doi:10.24869/psyd.2020.273
17. McDonald SD, Pugh M, Mickens MN. Resilience after spinal cord injury: a scoping review. Am J Phys Med Rehabil. 2020;99(8):752–763. doi:10.1097/PHM.0000000000001371
18. Bhattarai M, Jin Y, Smedema SM, Cadel KR, Baniya M. The relationships among self-efficacy, social support, resilience, and subjective well-being in persons with spinal cord injuries. J Adv Nurs. 2021;77(1):221–230. doi:10.1111/jan.14573
19. Oscilowicz E, Anguelovski I, Triguero-Mas M, García-Lamarca M, Baró F, Cole HV. Green justice through policy and practice: a call for further research into tools that foster healthy green cities for all. Cities Health. 2022;6(5):878–893. doi:10.1080/23748834.2022.2072057
20. Pretorius TB, Padmanabhanunni A. Assessing the cognitive component of subjective well-being: revisiting the satisfaction with life scale with classical test theory and item response theory. African J Psychol Assess. 2022;4:9. doi:10.4102/ajopa.v4i0.106
21. Jia N, Li W, Zhang L, Kong F. Beneficial effects of hedonic and eudaimonic motivations on subjective well-being in adolescents: a two-wave cross-lagged analysis. J Posit Psychol. 2022;17(5):701–707. doi:10.1080/17439760.2021.1913641
22. Wu F, Ren Z, Wang Q, et al. The relationship between job stress and job burnout: the mediating effects of perceived social support and job satisfaction. Psychol Health Med. 2021;26(2):204–211. doi:10.1080/13548506.2020.1778750
23. Hinz A, Schulte T, Finck C, et al. Psychometric evaluations of the Life Orientation Test-Revised (LOT-R), based on nine samples. Psychol Health. 2022;37(6):767–779. doi:10.1080/08870446.2021.1892111
24. Jin X, Xu X, Qiu J, et al. Psychological resilience of second-pregnancy women in China: a cross-sectional study of influencing factors. Asian Nurs Res. 2021;15(2):121–128. doi:10.1016/j.anr.2021.01.002
25. Gibbs LAL, Anderson MI, Simpson GK, Jones KF. Spirituality and resilience among family caregivers of survivors of stroke: a scoping review. NeuroRehabilitation. 2020;46(1):41–52. doi:10.3233/NRE-192946
26. Folayan MO, Oginni O, Arowolo O, El Tantawi M. Internal consistency and correlation of the adverse childhood experiences, bully victimization, self-esteem, resilience, and social support scales in Nigerian children. BMC Res Notes. 2020;13(1):1–6. doi:10.1186/s13104-020-05174-3
27. Carrard V, Kunz S, Peter C. Mental health, quality of life, self-efficacy, and social support of individuals living with spinal cord injury in Switzerland compared to that of the general population. Spinal Cord. 2021;59(4):398–409. doi:10.1038/s41393-020-00582-5
28. Li S, Schulte EM, Cui G, Li Z, Cheng Z, Xu H. Psychometric properties of the Chinese version of the modified Yale Food Addiction Scale version 2.0 (C-mYFAS 2.0): prevalence of food addiction and relationship with resilience and social support. Eating Weight Disord Stud Anorexia Bulimia Obes. 2022;27(1):273–284. doi:10.1007/s40519-021-01174-9
29. Simon J, Helter TM, White RG, van der Boor C, Łaszewska A. Impacts of the Covid-19 lockdown and relevant vulnerabilities on capability well-being, mental health and social support: an Austrian survey study. BMC Public Health. 2021;21(1):1–12. doi:10.1186/s12889-021-10351-5
30. Alnazly E, Khraisat OM, Al-Bashaireh AM, Bryant CL. Anxiety, depression, stress, fear and social support during COVID-19 pandemic among Jordanian healthcare workers. PLoS One. 2021;16(3):e0247679. doi:10.1371/journal.pone.0247679
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.