Back to Journals » Patient Related Outcome Measures » Volume 14
The Pattern of Admission, Clinical Characteristics, and Outcomes Among Patients Admitted to the Intensive Care Unit of a Tertiary Hospital in Tanzania: A 5-Year Retrospective Review
Authors Kassam N, Adebayo PB, Matei IM, Aghan E, Somji S, Kadelya SP, Abha Y, Swai FE, Mabusi M, Hameed K, Mbithe H, Thawer A ![]() , Makakala MC, Bakshi FA, Chuwa H, Ng'wanasayi M, Wambura CM, Mvungi RS, Orwa J, Sharma M, Udeani G, Surani S
, Makakala MC, Bakshi FA, Chuwa H, Ng'wanasayi M, Wambura CM, Mvungi RS, Orwa J, Sharma M, Udeani G, Surani S
Received 26 October 2023
Accepted for publication 18 November 2023
Published 7 December 2023 Volume 2023:14 Pages 383—392
DOI https://doi.org/10.2147/PROM.S441293
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Robert Howland
Nadeem Kassam,1 Philip B Adebayo,1 Iris Martin Matei,1 Eric Aghan,2 Samina Somji,1 Samwel Paul Kadelya,1 Yasson Abha,1 Frank Elton Swai,2 Mangaro Mabusi,1 Kamran Hameed,1 Hanifa Mbithe,1 Alyyah Thawer,1 Mandela Charles Makakala,1 Fatma Amirali Bakshi,1 Harrison Chuwa,1 Masolwa Ng’wanasayi,1 Casmir M Wambura,1 Robert Sostenes Mvungi,1 James Orwa,3 Munish Sharma,4 George Udeani,5 Salim Surani5
1Department of Internal Medicine, Aga Khan Health Service, Dar-es-Salaam, Tanzania; 2Department of Family Medicine, Aga Khan University Medical College, Nairobi, Kenya; 3Department of Population Health, Aga Khan University Medical College, Nairobi, Kenya; 4Department of Medicine, Division of Pulmonology and Critical Care, Baylor Scott and White Medical Center, Temple, Texas, USA; 5Department of Pharmacy, A&M University, College Station, Texas, USA
Correspondence: Nadeem Kassam, Department of Internal Medicine, Aga Khan Health Service, Dar-es-Salaam, Tanzania, Email [email protected]
Introduction: Despite the implementation of complex interventions, ICU mortality remains high and more so in developing countries. The demand for critical care in Sub-Saharan Africa is more than ever before as the region experiences a double burden of rising rates of non-communicable diseases (NCD) in the background battle of combating infectious diseases. Limited studies in Tanzania have reported varying factors associated with markedly high rates of ICU mortality. Investigating the burden of ICU care remains crucial in providing insights into the effectiveness and challenges of critical care delivery.
Material and Methods: A single-center retrospective study that reviewed records of all medically admitted patients admitted to the ICU of the Aga Khan Hospital, Dar-es-Salaam, from 1st October 2018 to 30th April 2023. To define the population in the study, we used descriptive statistics. Patients’ outcomes were categorized based on ICU survival. Binary logistic regression was run (at 95% CI and p-value < 0.05) to identify the determinants for ICU mortality.
Results: Medical records of 717 patients were reviewed. The cohort was male (n=472,65.8%) and African predominant (n=471,65.7%) with a median age of 58 years (IQR 45.0– 71.0). 17.9% of patients did not survive. The highest mortality was noted amongst patients with septic shock (29.3%). The lowest survival was noted amongst patients requiring three organ support (n=12,2.1%). Advanced age (OR 1.02,CI 1.00– 1.04), having more than three underlying comorbidities (OR 2.50,CI 1.96– 6.60), use of inotropic support (OR 3.58,CI 1.89– 6.80) and mechanical ventilation (OR 9.11,CI 4.72– 18.11) showed association with increased risk for mortality in ICU.
Conclusion: The study indicated a much lower ICU mortality rate compared to similar studies conducted in other parts of Sub-Saharan Africa. Advanced age, underlying multiple comorbidities and organ support were associated with ICU mortality. Large multi-center studies are needed to highlight the true burden of critical care illness in Tanzania.
Keywords: critical care, Tanzania, mortality, epidemiological profile
Introduction
The Intensive Care Unit (ICU) is a specialized unit serving patients with severe and life-threatening illnesses requiring intense and sophisticated treatment to maintain normal physiological function.1 Mortality in ICUs remains high even with the utility of the latest and most costly equipment. ICU mortality in many African countries2–9 both in the public and private sector, is markedly high and exceeds by multiple folds when compared to ICUs in High-Income Countries (HICs).1,7,10 Documented ICU mortality rates exceeds; 25% in Ethiopia,5 35% in Tanzania2,3 and Uganda9 and approaches 60% in Kenya.6 Over the past two decades, ICU care in the developed world has noticeably improved in technologies and the quality of care it can provide, resulting in an improved survival rate.10 These trends have not been consistently observed in developing and resource-limited settings, including Sub-Saharan Africa (SSA).6 The development of Critical care in SSA, especially in the public sector, has been a challenge,11 largely due to a shortage of resources and a lack of sufficiently skilled personnel compounded by poor health-seeking behaviors by the public.
Despite the COVID-19 pandemic placing SSA in an unchartered region and calling upon urgent development of ICU care, there remain limitations in scaling up appropriate critical care in the region.12 With the African continent currently experiencing a double burden of rising rates of Non-Communicable diseases (NCD) in the background battle of combating infectious diseases and an aging population, the demand for critical care is more than ever before.13 ICU care in Tanzania has been poorly described, with large variations reported in the public and private sectors.2–4 Most ICUs in Tanzania are developed in tertiary and private hospitals in urban areas, not serving most of the population living in rural areas.14 Given the recent initiatives of the Tanzanian government post-COVID-19 pandemic to increase the critical care capacity in the country, this analysis is timely to serve as an information platform for developing healthcare policies in the region. No study to date has assessed ICU outcomes in well-resourced settings in Tanzania, comparable to many tertiary-level hospitals in High-Income Countries (HIC).
This study aimed to identify clinical characteristics and elaborate on risk factors associated with ICU mortality. The study was carried out amongst the ICU patients who were admitted at the Aga Khan Hospital located in Dar-es-Salaam, Tanzania. This study will add to the prevailing limited critical care literature from this region.
Methodology
Study Design
We conducted a retrospective cross-sectional study that reviewed records of medical patients15 admitted to the ICU of the Aga Khan Hospital Dar-es-Salaam, Tanzania, from 1st October 2018 to 31st April 2023.
Study Setting
The Aga Khan Hospital is Tanzania’s first and only Joint Commission International (JCI) accredited hospital. It provides level three care to critically ill patients. It can treat 15 patients in its ICU. The 15-bed ICU is divided into 7 beds for general critically ill patients, 4 reserved for pediatric patients, and 4 for cardiac patients. The ICU of the Aga Khan Hospital is able to provide level III services to critically ill patients.1 The Unit is capable of providing invasive and non- invasive monitoring of vitals. The organization of the ICU utilizes an open model system run by a multidisciplinary team comprising of the physician of primary specialty, the nutritionist, the physiotherapist and led by a full-time critical care specialist. The nurse-to-patient ratio is 1:1. Resident doctors in the internal medicine department from Aga Khan University actively participate in the care of medically admitted patients.
Study Population
All consecutive patients aged 18 years and above meeting the institution’s strict admitting criteria admitted with a medical diagnosis as well as having a final ICU outcome were studied. The study excluded patients admitted for observation, those without a complete set of inpatient data, and those suspected or diagnosed with COVID-19 disease.
Data Collection
The primary investigator identified the patients from the department’s admission registry, and patient files were retrieved from the institutional medical records. Medical doctors working in the ICU volunteered as research assistants to collect all the necessary data, both in paper-based and electronic formats. Data collected included the following: basic demographic information, source of admission (transferred from ward, emergency), underlying comorbid illness, available laboratory data, admitting diagnosis, organ support, interventions, and relevant admitting section. In cases with more than one critical care diagnosis, entity that was associated with worst prognosis was chosen as the lead diagnosis. The collected data was incorporated into a Microsoft Excel 2010 (Redmond, WA, USA). The data collected was randomly rechecked by the primary investigator to ensure that it was accurate and complete.
Data Analysis
Proportions and frequencies were used to represent Categorical variables. They were compared with the use of chi-squared or Fisher’s exact tests. Means and medians were utilized to represent continuous variables and the comparison was done with the aid of Mann Whitney tests or independent t-tests. Statistical significance was set at P- value <0.05. Any variable demonstrating statistical or clinical significance in explaining ICU mortality was considered in the multivariate model. We used p-values, odds ratio (95% confidence interval) and, binary logistic regression to present determinants of ICU mortality. IBM Statistical Package for Social Sciences version 23.0 was used to perform statistical analysis.
Ethical Consideration
Aga Khan University Ethical Research Committee (AKU ERC) at provided ethical approval for the research (AKU/2023/012/fb/09/013).
Results
A total of 717 patients were included in the study out of which (n=128,17.9%) died and (n= 589,82.1%) survived. Table 1 below illustrates the general and clinical characteristics of the study population and provides a comparison between Survivors and non-survivors. Our cohort was predominately African (n=471,65.7%) with the majority being male (n=472, 65.8%) having a median age of 58 years (IQR 45–71.0). The majority of ICU admission were admitted from the emergency department (n=643, 92.8%). When survivors and non -survivors were compared, the higher median age of 65.5 years (IQR 51.8–75.2), greater BMI 27.2 kg/m2(IQR 24.1–31.1) and prolonged length of stay of 4 days (IQR 2.0–8.2) was noted amongst the non- survivors as seen in Table 1 below.
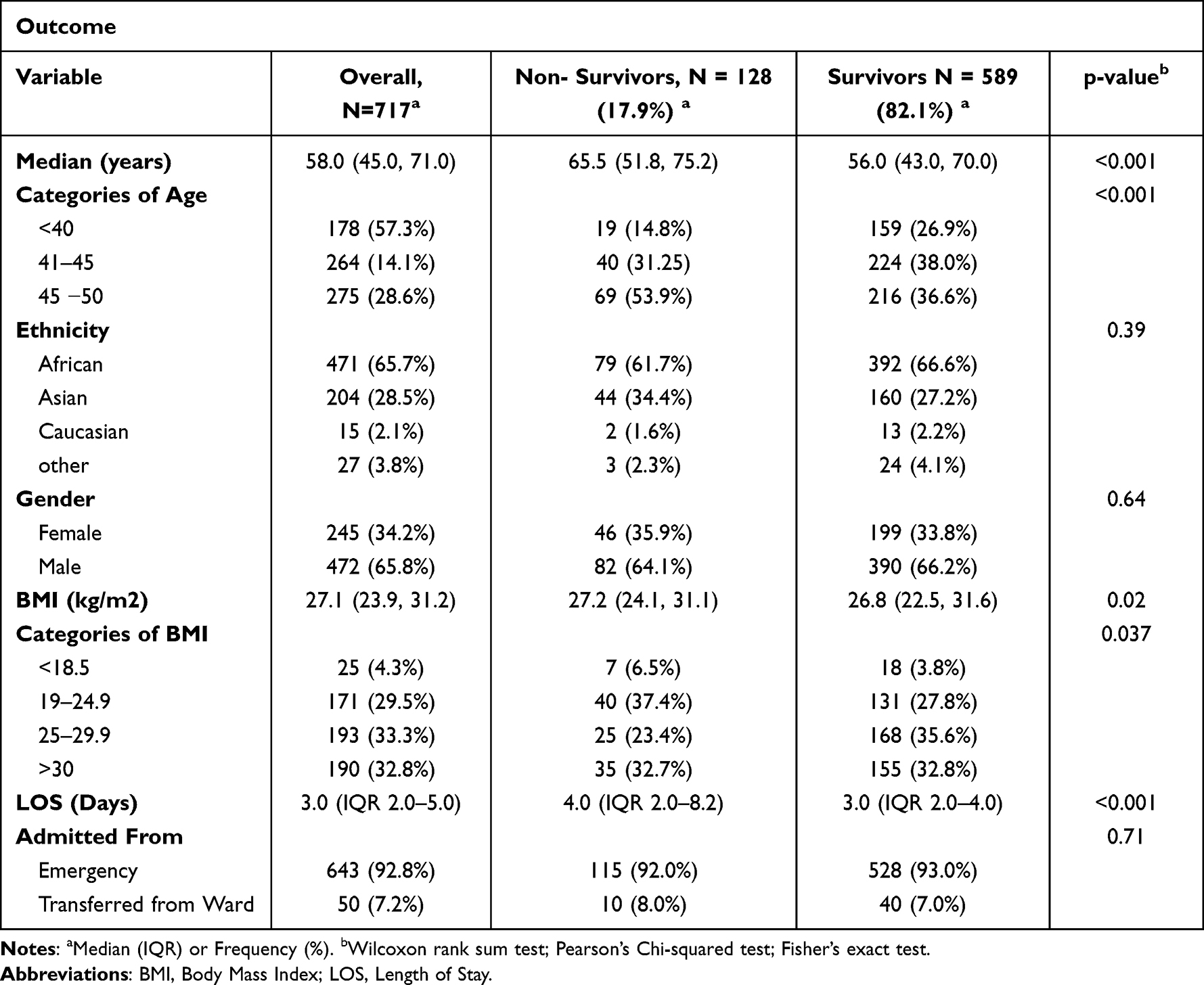 |
Table 1 Demographic characteristics of the study Population |
The majority of the cohort suffered from an infectious (n= 175,24.4%), neurology (n=111,15.5%), and cardiology-related- condition (n=110,15.4%). The highest mortality was noted amongst those admitted with an infectious disease condition (n=40, 31.2%), as seen in Table 2 below.
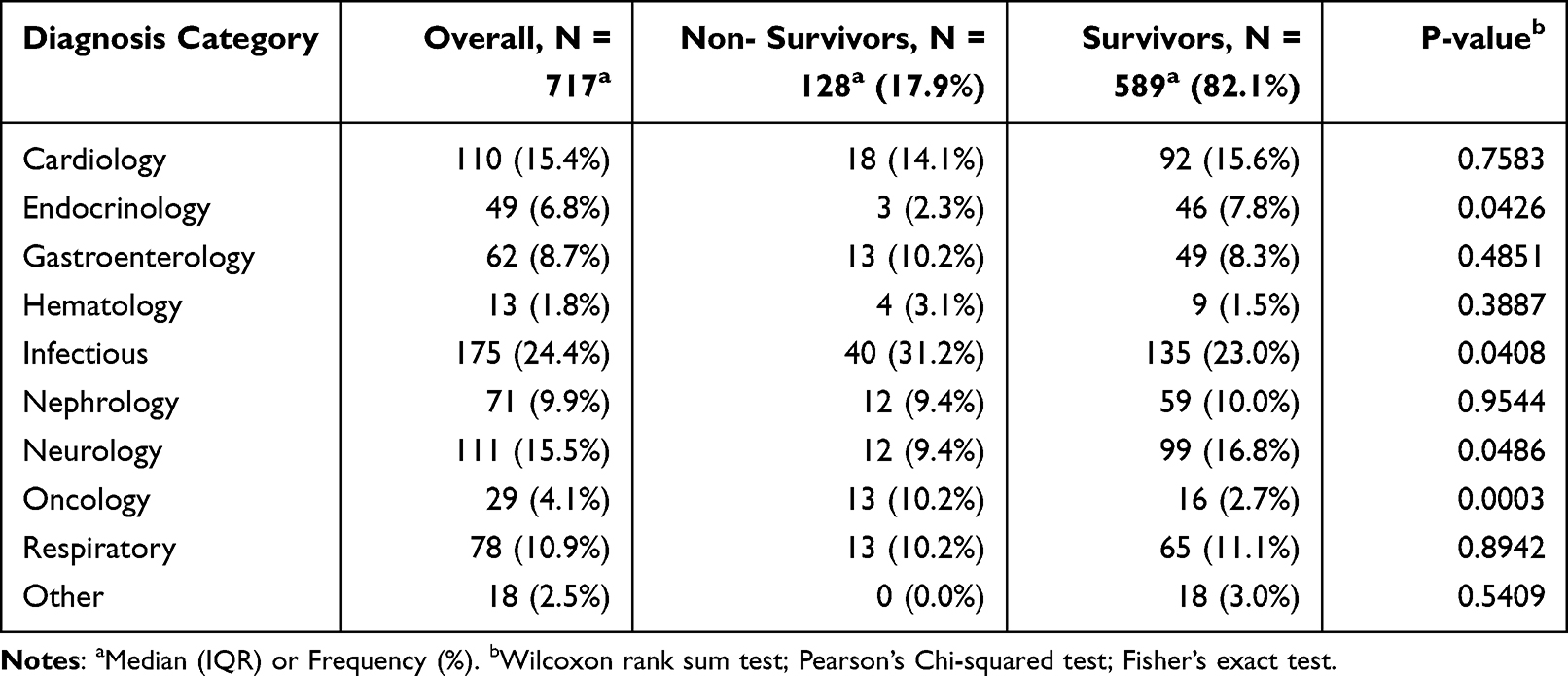 |
Table 2 Admitting Category of the Study Population |
Figure 1 below illustrates the most common ICU diagnosis in our cohort. The mortality was highest in patients with septic shock (29.3%).
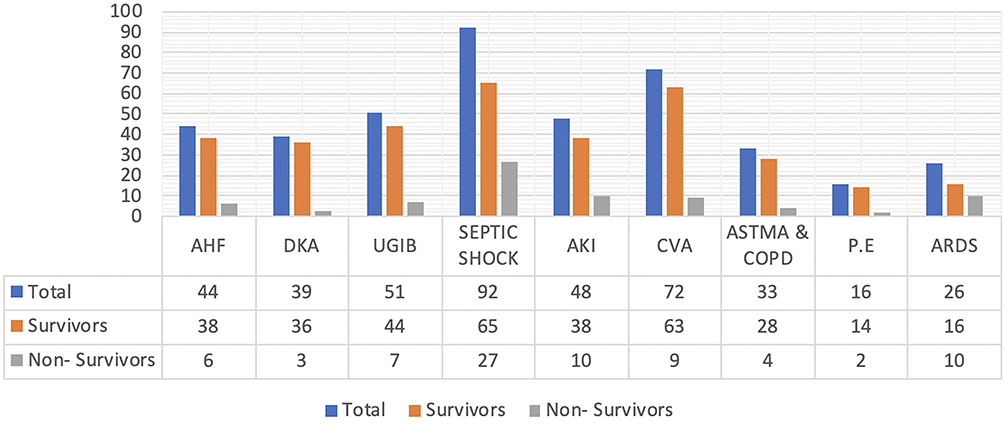 |
Figure 1 Most common ICU diagnosis among medically admitted patients. Abbreviations: AHF, Acute Heart Failure; DKA, Diabetic Ketoacidosis; UGIB, Upper Gastrointestinal bleeding; AKI, Acute Kidney Injury; CVA, Cerebrovascular accident; COPD, Chronic Obstructive pulmonary disease; PE, Pulmonary Embolism; ADS, Acute Respiratory Distress Syndrome. |
Table 3 below illustrates underlying comorbid illness in our cohort and provides a comparison between survivors and non-survivors. Multiple comorbidities, if present, were reported. The most common comorbid condition was hypertension (n= 315,43.9%) and Diabetes Mellitus (n= 220,30.7%). The highest mortality was amongst those with Chronic Kidney Disease (CKD) (n=28,21.9%), and the Lowest survival rate was among those with more than three comorbid conditions (n=22,3.7%).
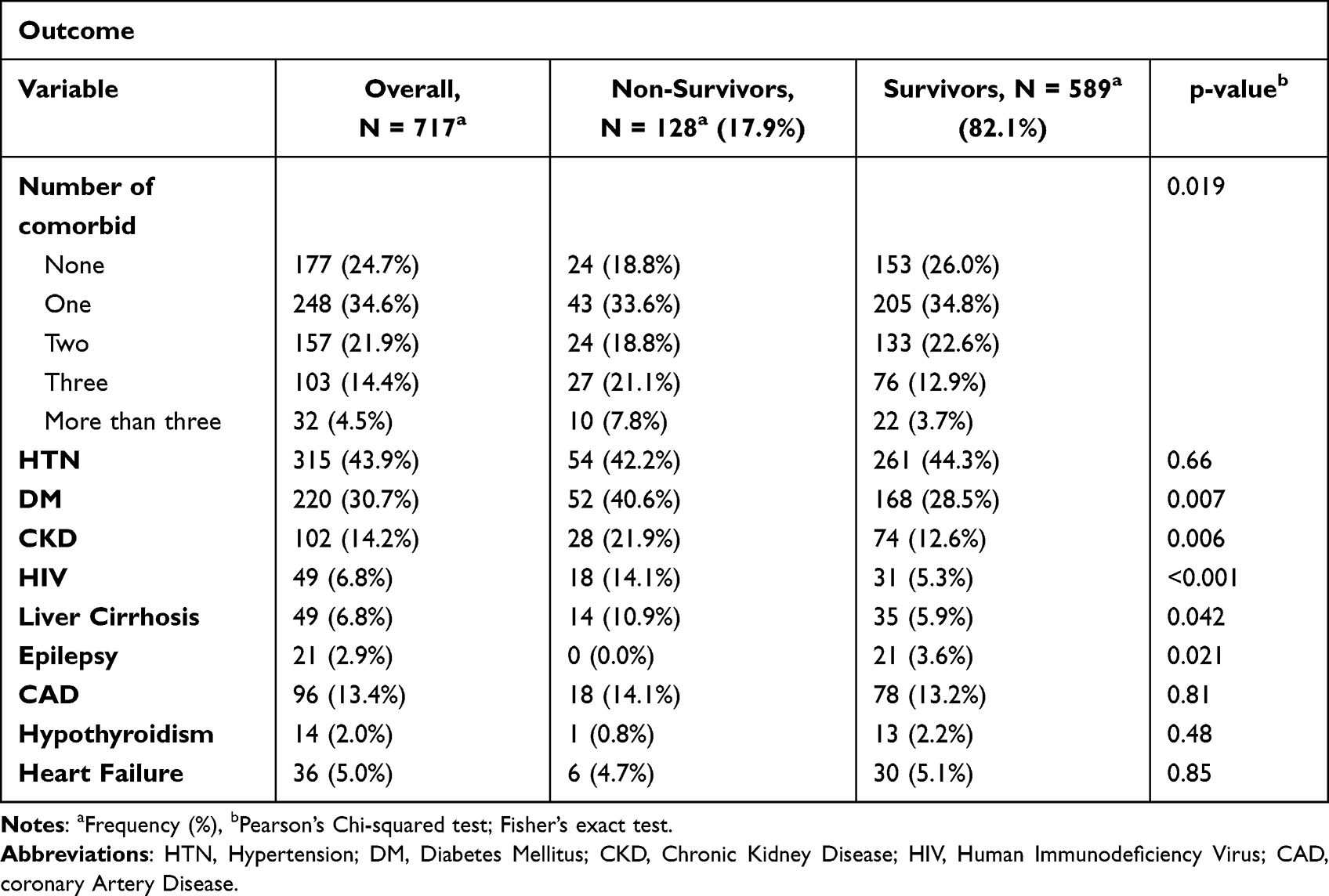 |
Table 3 Underlying Comorbid Illness in Our Cohort |
Table 4 below illustrates the type of organ support patients received within the first hour of ICU admission. Of the 717 patients (n=420, 59.3%) did not receive any organ support within the first hour of ICU admission. The highest mortality was noted amongst those who received inotropic support within the first hour of ICU admission (n= 72.56.2%). The highest survival rate was also noted amongst those who required no organ support in the first hour of ICU admission (n- 397,68.2%).
 |
Table 4 Type of Organ Support Within the First Hour of ICU Admission |
Figure 2 below illustrates the values of C-reactive protein (CRP) at the time of admission. The mean CRP value was 88.4 mg/L (±108.9). A higher CRP value was seen among the non - survivors 115 mg/L (±123.8) when compared with the survivors 82 mg/L (±107)
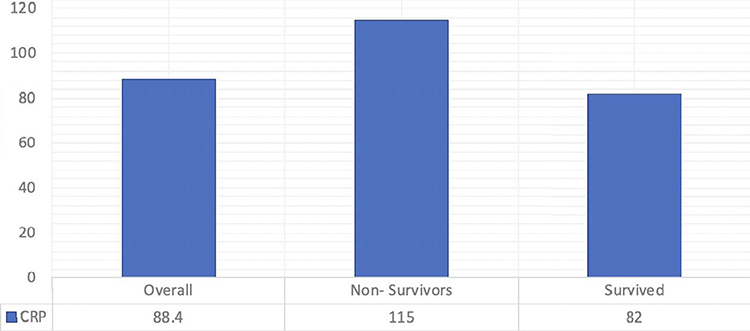 |
Figure 2 Admitting CRP values between survivors and non - survivors. P-value 0.005 (Welch Two Sample t-test). |
Advanced age (OR 1.02, 95% CI 1.00–1.04), having more than three underlying comorbidities (OR 2.50, 95% CI 1.96–6.60), use of inotropic support (OR 3.58, 95% CI 1.89–6.80) and mechanical ventilation (OR 9.11, 95% CI 4.72–18.11) within the first hour were associated with increased mortality as seen in Table 5 below.
 |
Table 5 Factors Associated with ICU Mortality |
Discussion
Per our literature search, studies on medical admissions to the ICU over a five years in Tanzania are scarce. The ICU mortality at the Aga Khan Hospital Dar es Salaam was 17.9%. In our study, mortality was the highest in patients with septic shock. Previous findings from the Aga Khan Hospital Dar-es-salaam that looked into the performance of predictive scoring models reported similar findings.4 Our study results depict a very low ICU mortality rate when compared to similar studies done in Tanzania2,3 and other countries in Sub-Saharan Africa.5–9,16–18 The discrepancy can be chiefly attributed to the level of care that the hospital provides, which is comparable in various ways to facilities in High-Income Countries (HICs). The ICU of the Aga Khan Hospital Dar-es-Salaam is a well-structured and resourceful unit run by a multidisciplinary team able to provide level III care1 to all its admitted patients. Additionally, the Aga Khan Hospital Dar es Salaam is a teaching hospital of the Aga Khan University. The majority of the healthcare workers at the hospital are linked with academic activities at the university. Numerous studies have reported low ICU mortality and better outcomes in major teaching hospitals when compared to non-teaching hospitals.19,20 This is purely centered on constant and evidence-based updated practice. Our study did not report on the acuity of patients on admission, which may differ from one setting to the other, thus making it difficult to precisely compare mortality rates. Our in-ICU mortality rates are similar when compared to developed countries in Northern America and Europe7,21–23 as well as in some parts of Asia.24,25
Globally, septic shock is the leading cause of death among adults admitted to the ICU and the results of our study also reflected a similar trend.26 Various systemic reviews and meta-analyses have reported an average in-ICU mortality rate between 30–40%.27–29 Regional disparities exist, with higher mortality rates reported in low and Low Middle-Income Countries (LMICs).30 Despite various advances in medical care and life-saving interventions, the Septic shock mortality paradox can be explained by its rapid progression,31 delayed health-seeking behavior,32 aging,33 comorbidities,31 resistant pathogens34 and its heterogeneous approach.35 The in-ICU mortality rate among patients with septic shock at our center was approximately 30%, in line with global31 and previously conducted studies at our center4 but much lower when compared to studies done in other parts of Africa.2,3,6,36,37 The infectious disease section of the hospital has made great efforts in setting up a well-equipped laboratory and a comprehensive antibiotic stewardship program able to deliver time-sensitive results and combat antimicrobial resistance. Nonetheless, this is insufficient and might not be applicable in the public sector due to resource limitations. Thus, the sole weapon that cuts across every community is advocating preventive measures such as good hygiene practices, early and prompt referrals, better control of underlying comorbid illness, and access to age-matched vaccinations. Despite the sepsis syndrome having a greater impact on short-term mortality, survivors also suffer from long-term sequelae affecting cognitive and organ function as well as increased risk of rehospitalization.38 The scope of the current study was beyond long-term follow-up, but our observations are well within published reports.
The study identified increasing age, comorbidities (more than three), and the need for organ support as key factors associated with ICU mortality. Increasing age has been well-studied among various ICU cohorts and found to be an independent risk factor.39 Several studies have reported a stepwise increase in ICU mortality among individuals after the age of 60 years.40 Increased age is associated with various underlying comorbidities in addition to their principal diagnosis mitigating the multimorbidity state, frailty, and polypharmacy, posing a challenge even prior admission. The number of older patients requiring ICU admission is expected to increase given the aging global population and confers uncertainty of its short- and long-term benefits.41 Thus, this study advocates the improvement of geriatric medicine and palliative care, especially in resource-limited settings, as well as the use of illness-predictive scoring models in clinical practice to scientifically predict outcomes. More than one-third of patients who succumbed to death in the ICU had more than three underlying comorbid conditions. Our study did not specifically identify a particular comorbid condition related to ICU mortality, but NCD42 has been shown to influence the course of admission and negatively impact outcomes. Thus, admitting physicians should collectively identify high-risk individuals and guide discussion about realistic outcomes prior to admission.
The study also identified Inotropes and mechanical ventilation to be key factors associated with in-ICU mortality. This can be justified by the acuity of the patients requiring organ support for respiratory failure and hemodynamic compromise. Several studies have reported similar findings.43–45 These findings do not underscore the importance of these interventions but prove the existence of the double-edged sword. Inotropes induce myocardial ischemia and arrhythmias as well as render critically ill patients to central line-associated bloodstream infection (CLABSI). Due to the study’s retrospective nature, we could not elucidate the specific inotropic agent associated with increased mortality. Nevertheless, few reports have indicated specific agent, dose, and time-dependent associations.46 Despite mechanical ventilation being considered a lifesaving and beneficial intervention, it can also directly predispose an individual to increased risk of death through ventilator-associated complications, lung injury, and the development of nosocomial infection. Hence, ICU teams need to continuously adapt and refine approaches to improve outcomes amongst mechanically ventilated patients and cautiously monitor critically ill patients on organ support.
Limitations of the Study
Despite this being one of the largest studies to be conducted among critically admitted medical patients in Tanzania. This study had multiple limitations. Firstly, due to its retrospective nature, only limited charts and medical files were retrieved, and not all necessary variables were studied, especially physiological and laboratory parameters. Multiple diagnoses in a patient might have skewed the validity of the exact mortality rates of a specific condition. The Single-center nature, more so in the private- sector, limits the results generalizability.
Conclusion
In summary, this is the first paper in Tanzania to review 5-year data of medically admitted patients to the ICU of a private tertiary hospital. The in-ICU mortality was reported to be 17.9%, much lower than another sub-Saharan cohort. Patients admitted with septic shock had the highest in ICU mortality. The elderly with multiple comorbidities requiring organ support would likely not survive hospital discharge. A large multi-center national prospective study will highlight the true burden of critical care illness in Tanzania.
Future Direction
It is expected the burden of critical care will increase in SSA. Consequently, capacity building, infrastructure enhancement, telemedicine, contextual research, and policy development are areas that require enormous development to match the needs of the African continent.
Data Sharing Statement
The data set can be made available upon request from the corresponding author.
Ethical Approval
The study was approved by the Aga Khan University, East Africa Ethical Research Committee (AKU, EA ERC). The National Institute for Medical Research (NIMR) in Tanzania mandates the AKU, EA ERC to approve health research conducted by Tanzanian students. The hospital’s ethical committee and the AKU, EA, ERC exempted the primary investigator from acquiring informed consents from the study participants, since the study design did not affect the rights and welfare of the patients. This study was conducted in accordance with the Declaration of Helsinki. Reference (AKU/2023/012/fb/09/013).
Acknowledgment
We would like to thank the emergency department and the Intensive Care Unit (ICU) of the Aga Khan Hospital, Dar-es- Salaam, Tanzania.
Disclosure
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Marshall JC, Bosco L, Adhikari NK, et al. What is an intensive care unit? A report of the task force of the world federation of societies of intensive and critical care medicine. J Crit Care. 2017;37:270–276. doi:10.1016/j.jcrc.2016.07.015
2. Sadiq AM, Kilonzo KG, Tsima BM. Pattern of diseases and clinical outcomes in medical intensive care unit at a tertiary hospital in northeastern Tanzania: a three-year retrospective study. PLoS One. 2023;18(2):e0282269. doi:10.1371/journal.pone.0282269
3. Sawe HR, Mfinanga JA, Lidenge SJ, et al. Disease patterns and clinical outcomes of patients admitted in intensive care units of tertiary referral hospitals of Tanzania. BMC Int Health Hum Rights. 2014;14(1):26. doi:10.1186/1472-698X-14-26
4. Kassam N, Aghan E, Somji S, Aziz O, Orwa J, Surani SR. Performance in mortality prediction of SAPS 3 And MPM-III scores among adult patients admitted to the ICU of a private tertiary referral hospital in Tanzania: a retrospective cohort study. Peer J. 2021;9:e12332. doi:10.7717/peerj.12332
5. Demass TB, Guadie AG, Mengistu TB, et al. The magnitude of mortality and its predictors among adult patients admitted to the intensive care unit in Amhara Regional State, Northwest Ethiopia. Sci Rep. 2023;13(1):12010. doi:10.1038/s41598-023-39190-7
6. Lalani HS, Waweru-Siika W, Mwogi T, et al. Intensive care outcomes and mortality prediction at a national referral hospital in Western Kenya. Ann Am Thorac Soc. 2018;15(11):1336–1343. doi:10.1513/AnnalsATS.201801-051OC
7. Eya J, Ejikem M, Ogamba C. Admission and mortality patterns in intensive care delivery at Enugu State University of science and technology teaching hospital: a three-year retrospective study. Cureus. 2022;14(7):e27195. doi:10.7759/cureus.27195
8. Mandeng Ma Linwa E, Binam Bikoi C, Tochie Noutakdie J, et al. In-ICU outcomes of critically ill patients in a reference Cameroonian intensive care unit: a retrospective cohort study. Crit Care Res Pract. 2023;2023:6074700. doi:10.1155/2023/6074700
9. Ttendo SS, Was A, Preston MA, Munyarugero E, Kerry VB, Firth PG. Retrospective descriptive study of an intensive care unit at a Ugandan Regional Referral Hospital. World J Surg. 2016;40(12):2847–2856. doi:10.1007/s00268-016-3644-5
10. van der Sluijs AF, van Slobbe-Bijlsma ER, Chick SE, Vroom MB, Dongelmans DA, Vlaar APJ. The impact of changes in intensive care organization on patient outcome and cost-effectiveness-a narrative review. J Intensive Care. 2017;5(1):13. doi:10.1186/s40560-016-0207-7
11. Okafor UV. Challenges in critical care services in Sub-Saharan Africa: perspectives from Nigeria. Indian J Crit Care Med. 2009;13(1):25–27. doi:10.4103/0972-5229.53112
12. Kifle F, Boru Y, Tamiru HD, et al. Intensive Care in Sub-Saharan Africa: a National Review of the Service Status in Ethiopia. Anesth Analg. 2022;134(5):930–937. doi:10.1213/ANE.0000000000005799
13. Nyirenda MJ. Non-communicable diseases in sub-Saharan Africa: understanding the drivers of the epidemic to inform intervention strategies. Int Health. 2016;8(3):157–158. doi:10.1093/inthealth/ihw021
14. Kazibwe J, Shah HA, Kuwawenaruwa A, et al. Resource use, availability and cost in the provision of critical care in Tanzania: a systematic review. BMJ Open. 2022;12(11):e060422. doi:10.1136/bmjopen-2021-060422
15. Reyes H. What is Internal Medicine? Rev Med Chil. 2006;134(10):1338–1344. doi:10.4067/s0034-98872006001000020
16. Riviello ED, Kiviri W, Fowler RA, et al. Predicting mortality in low-income country iCUs: the Rwanda Mortality Probability Model (R-MPM). PLoS One. 2016;11(5):e0155858. doi:10.1371/journal.pone.0155858
17. Onyekwulu FA, Anya SU. Pattern of admission and outcome of patients admitted into the intensive care unit of University of Nigeria Teaching Hospital Enugu: a 5-year review. Niger J Clin Pract. 2015;18(6):775–779. doi:10.4103/1119-3077.163291
18. Kedir S, Berhane A, Bayisa T, Wuletaw T. Admission patterns and outcomes in the medical intensive care unit of St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia. Ethiop Med J. 2017;55(1):19–26.
19. Ayanian JZ, Weissman JS. Teaching hospitals and quality of care: a review of the literature. Milbank Q. 2002;80(3):569–593. doi:10.1111/1468-0009.00023
20. Burke LG, Frakt AB, Khullar D, Orav EJ, Jha AK. Association between teaching status and mortality in US hospitals. JAMA. 2017;317(20):2105–2113. doi:10.1001/jama.2017.5702
21. Vincent JL, Marshall JC, Namendys-Silva SA, et al. Assessment of the worldwide burden of critical illness: the intensive care over nations (ICON) audit. Lancet Respir Med. 2014;2(5):380–386. doi:10.1016/S2213-2600(14)70061-X
22. Capuzzo M, Volta C, Tassinati T, et al. Hospital mortality of adults admitted to intensive care units in hospitals with and without intermediate care units: a multicentre European cohort study. Crit Care. 2014;18(5):551. doi:10.1186/s13054-014-0551-8
23. Zimmerman JE, Kramer AA, Knaus WA. Changes in hospital mortality for United States intensive care unit admissions from 1988 to 2012. Crit Care. 2013;17(2):R81. doi:10.1186/cc12695
24. Moran JL, Solomon PJ, Moerbeek M. Outcome ACf, resource evaluation of A, New Zealand Intensive Care S. Fixed effects modelling for provider mortality outcomes: analysis of the Australia and New Zealand Intensive Care Society (ANZICS) adult patient data-base. PLoS One. 2014;9(7):e102297. doi:10.1371/journal.pone.0102297
25. Oh TK, Kim HG, Song IA. Epidemiologic study of intensive care unit admission in South Korea: a nationwide population-based cohort study from 2010 to 2019. Int J Environ Res Public Health. 2022;20(1):81. doi:10.3390/ijerph20010081
26. Cao L, Xiao M, Wan Y, et al. Epidemiology and mortality of sepsis in intensive care units in prefecture-level Cities in Sichuan, China: a prospective multicenter study. Med Sci Monit. 2021;27:e932227.
27. Namgung M, Ahn C, Park Y, Kwak IY, Lee J, Won M. Mortality among adult patients with sepsis and septic shock in Korea: a systematic review and meta-analysis. Clin Exp Emerg Med. 2023;10(2):157–171. doi:10.15441/ceem.23.005
28. Bauer M, Gerlach H, Vogelmann T, Preissing F, Stiefel J, Adam D. Mortality in sepsis and septic shock in Europe, North America and Australia between 2009 and 2019- results from a systematic review and meta-analysis. Crit Care. 2020;24(1):239. doi:10.1186/s13054-020-02950-2
29. Vincent JL, Jones G, David S, Olariu E, Cadwell KK. Frequency and mortality of septic shock in Europe and North America: a systematic review and meta-analysis. Crit Care. 2019;23(1):196. doi:10.1186/s13054-019-2478-6
30. Stephen AH, Montoya RL, Aluisio AR. Sepsis and septic shock in low- and middle-income countries. Surg Infect. 2020;21(7):571–578. doi:10.1089/sur.2020.047
31. Mahapatra S, Heffner AC. Septic Shock. StatPearls. Treasure Island (FL) ineligible companies. Disclosure: Alan Heffner declares no relevant financial relationships with ineligible companies. 2023.
32. Guarino M, Perna B, Cesaro AE, et al. 2023 update on sepsis and septic shock in adult patients: management in the emergency department. J Clin Med. 2023;12(9):3188. doi:10.3390/jcm12093188
33. Liang SY. Sepsis and other infectious disease emergencies in the elderly. Emerg Med Clin North Am. 2016;34(3):501–522. doi:10.1016/j.emc.2016.04.005
34. Busani S, Serafini G, Mantovani E, et al. Mortality in patients with septic shock by multidrug resistant bacteria: risk factors and impact of sepsis treatments. J Intensive Care Med. 2019;34(1):48–54. doi:10.1177/0885066616688165
35. Polat G, Ugan RA, Cadirci E, Halici Z. Sepsis and septic shock: current treatment strategies and new approaches. Eurasian J Med. 2017;49(1):53–58. doi:10.5152/eurasianjmed.2017.17062
36. Kwizera A, Dunser M, Nakibuuka J. National intensive care unit bed capacity and ICU patient characteristics in a low income country. BMC Res Notes. 2012;5(1):475. doi:10.1186/1756-0500-5-475
37. Andrews B, Muchemwa L, Kelly P, Lakhi S, Heimburger DC, Bernard GR. Simplified severe sepsis protocol: a randomized controlled trial of modified early goal-directed therapy in Zambia. Crit Care Med. 2014;42(11):2315–2324. doi:10.1097/CCM.0000000000000541
38. Shankar-Hari M, Rubenfeld GD. Understanding long-term outcomes following sepsis: implications and challenges. Curr Infect Dis Rep. 2016;18(11):37. doi:10.1007/s11908-016-0544-7
39. Akinosoglou K, Schinas G, Almyroudi MP, Gogos C, Dimopoulos G. The impact of age on intensive care. Ageing Res Rev. 2023;84:101832. doi:10.1016/j.arr.2022.101832
40. Nielsson MS, Christiansen CF, Johansen MB, Rasmussen BS, Tonnesen E, Norgaard M. Mortality in elderly ICU patients: a cohort study. Acta Anaesthesiol Scand. 2014;58(1):19–26. doi:10.1111/aas.12211
41. Abuhasira R, Anstey M, Novack V, Bose S, Talmor D, Fuchs L. Intensive care unit capacity and mortality in older adults: a three nations retrospective observational cohort study. Ann Intensive Care. 2022;12(1):20. doi:10.1186/s13613-022-00994-x
42. Simpson A, Puxty K, McLoone P, Quasim T, Sloan B, Morrison DS. Comorbidity and survival after admission to the intensive care unit: a population-based study of 41,230 patients. J Intensive Care Soc. 2021;22(2):143–151. doi:10.1177/1751143720914229
43. Gao F, Zhang Y. Inotrope use and intensive care unit mortality in patients with cardiogenic shock: an analysis of a large electronic intensive care unit database. Front Cardiovasc Med. 2021;8:696138. doi:10.3389/fcvm.2021.696138
44. Motiejunaite J, Deniau B, Blet A, Gayat E, Mebazaa A. Inotropes and vasopressors are associated with increased short-term mortality but not long-term survival in critically ill patients. Anaesth Crit Care Pain Med. 2022;41(1):101012. doi:10.1016/j.accpm.2021.101012
45. Soares Pinheiro FGM, Santana Santos E, Barreto IDC, et al. Mortality predictors and associated factors in patients in the intensive care unit: a cross-sectional study. Crit Care Res Pract. 2020;2020:1483827. doi:10.1155/2020/1483827
46. Sato R, Ariyoshi N, Hasegawa D, et al. Effects of inotropes on the mortality in patients with septic shock. J Intensive Care Med. 2021;36(2):211–219. doi:10.1177/0885066619892218
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.