Back to Journals » International Journal of General Medicine » Volume 18
The Neutrophil Percentage-to-Albumin Ratio as a New Predictor of All-Cause Mortality in Maintenance Hemodialysis Patients
Authors Shi C, Wang J, Liu W, Mo Y ![]() , Huang Y, Wei X, Huo D, Huang A
, Huang Y, Wei X, Huo D, Huang A
Received 29 April 2025
Accepted for publication 15 July 2025
Published 25 July 2025 Volume 2025:18 Pages 4069—4078
DOI https://doi.org/10.2147/IJGM.S533135
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor David E. Stec
Changjing Shi,1,* Juan Wang,2,* Weichen Liu,2 Yiyi Mo,2 Yuan Huang,2 Xiaoxiao Wei,2 Dongmei Huo,2,* Aifang Huang2,*
1Information Technology Center, The First Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi Zhuang Autonomous Region, People’s Republic of China; 2Department of Blood Purification, The First Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi Zhuang Autonomous Region, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Aifang Huang, Department of Blood Purification, The First Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi Zhuang Autonomous Region, 530021, People’s Republic of China, Email [email protected]
Introduction: Neutrophil percentage-to-albumin ratio (NPAR), dually reflecting inflammation and malnutrition, is related to poor prognosis closely in a range of diseases. However, prognostic value of NPAR in maintenance hemodialysis (MHD) patients remains to be confirmed. This study aimed to investigate the association between NPAR and all-cause mortality in MHD patients.
Methods: Patients undergoing maintenance hemodialysis in the blood purification department of The First Affiliated Hospital of Guangxi Medical University from January 2021 to June 2021 were prospectively studied. NPAR was calculated by dividing neutrophils percentage by Albumin. Participants were followed for 36 months, with all-cause mortality as the primary endpoint.
Results: There were 146 male and 80 female MHD patients included in this study, with a median age of 56 years. 53 (23.5%) patients died during the follow-up period. Kaplan–Meier (K–M) analysis revealed significantly lower survival in patients with high NPAR (> 16.96) compared to those with low NPAR (≤ 16.96) (log rank test p=0.000). Multivariate Cox regression has identified NPAR as an independent predictor of all-cause mortality (HR=1.346, 95% CI 1.192– 1.521, p=0.000). Receiver operating characteristic (ROC) analysis demonstrated that the Area Under the Curve (AUC) of NPAR was 0.821 (95% CI: 0.759– 0.882, p=0.000) and had a trend to be better than that of neutrophil-to-lymphocyte ratio (NLR; AUC=0.710), platelet-to-lymphocyte ratio (PLR; AUC=0.647), neutrophil count (AUC=0.606), albumin (ALB; AUC=0.752), and high-sensitivity C-reactive protein (hs-CRP; AUC=0.670).
Conclusion: NPAR is independently associated with all-cause mortality in MHD patients and may serve as an emerging indicator for risk stratification and prognostic management for this group of patients.
Keywords: hemodialysis, neutrophil percentage-to-albumin ratio, mortality
Introduction
Chronic kidney disease affects more than 10% of the population, a considerable number of whom progress to end-stage renal disease (ESRD) eventually and require renal replacement therapy to survive.1 Hemodialysis is one of the most important renal replacement therapies. Although a large number of advances have been made in clinical and basic research over the past decades, maintenance hemodialysis (MHD) patients still face a high risk of mortality. Cardiovascular disease (CVD) is prevalent in MHD patients and is the most common cause of death.2 Chronic inflammation and malnutrition are proved to play a key role in developing CVD in MHD patients and closely associate with mortality.3–5
Neutrophils, key mediators of innate immunity, serve as critical biomarkers of systemic inflammation. Elevated neutrophil percentage is independently associated with adverse outcomes in MHD cohorts.6,7 Conversely, serum albumin, a well-established marker of nutritional status and anti-inflammatory capacity, demonstrates inverse correlations with morbidity and mortality in ESRD.8,9 Mechanistically, hypoalbuminemia exacerbates inflammation, oxidative stress, and endothelial dysfunction, cementing its role as an independent risk factor for poor prognosis.10
Given the synergistic interplay between inflammation and malnutrition in MHD outcomes, recent research has prioritized integrated biomarkers capturing both pathophysiological axes. The neutrophil percentage-to-albumin ratio (NPAR), calculated by dividing neutrophil percentage by serum albumin concentration, theoretically quantifies pro-inflammatory activation (numerator) and nutritional/anti-inflammatory reserve (denominator). As a novel inflammation-nutrition composite index, NPAR has demonstrated robust prognostic utility across diverse conditions such as sepsis, acute coronary syndrome and heart failure.11–14
In recent years, several studies have been reported on the role of NPAR in CKD patients. High NPAR is not only associated with increased risk of CKD, but also a predictor for both all-cause and CVD deaths in advanced CKD patients.15,16 Two studies indicated that NPAR is closely related to the prognosis of peritoneal dialysis (PD) patients, and also found NPAR exhibits superior discriminative performance compared to isolated markers (eg, albumin alone) and other inflammatory ratios (eg, neutrophil-to-lymphocyte ratio NLR, platelet-to-lymphocyte ratio PLR) in predicting PD mortality.17,18 A study demonstrated that an elevated NPAR was correlated to adverse outcome in MHD patients.19 However, data on the relationship between NPAR and mortality are limited. Therefore, in this study, we aimed to investigate the relationship between NPAR and all-cause mortality in MHD patients.
Materials and Methods
Subjects
MHD patients in the Blood Purification Department of The First Affiliated Hospital of Guangxi Medical University from January 2021 to June 2021 were prospectively research. The inclusion criteria were as follows: (1) age >18 years, (2) HD treatment duration >3 months, 4h 2–3 times weekly using standard bicarbonate dialysate. The exclusion criteria were: (1) recent heart failure and acute coronary syndrome within 1 month, (2) recent infections within 1 month, (3) history of kidney transplantation or peritoneal dialysis, (4) hematological disorders, (5) autoimmune diseases, (6) tumors, (7) taking steroids or immunosuppressive drugs.
Follow-Up and Endpoints
All subjects included were followed up for 36 months. The primary endpoint was defined as all-cause mortality. Deaths were confirmed by hospital records for inpatients and death certificates for outpatients. Follow-up terminated if the patient died, received a kidney transplant, transferred to another dialysis center, voluntarily gave up treatment during the follow-up period.
Ethics
This research follows the Helsinki Declaration and has been approved by the Ethics Committee of The First Affiliated Hospital of Guangxi Medical University (NO. 2023-K282-01). Informed consent was obtained from each subject prior to study commencement.
Data Collection
Data were all collected when the patients were included from the hospital’s multi-source database integrated from electronic health records (EHR), laboratory information system (LIS), hemodialysis information system, imaging system and treatment records, and defined as baseline data, including age, sex, etiology of CKD, history of diabetes, Duration of HD, type of vascular access for dialysis, dry weight, body mass index (BMI) and laboratory data. Laboratory data included white blood cell count (WBC), neutrophil count, lymphocyte count, platelet count, percentage of neutrophils, hemoglobin, serum albumin, blood urea nitrogen, creatinine, uric acid, potassium, chloride, calcium, phosphorus, serum ferritin, hypersensitive C-reactive protein (hs-CRP), intact parathyroid hormone (iPTH). When serum albumin was lower than 40 g/L, serum calcium was corrected using the formula: Ca2+ (mmol/L) = total serum Ca2+(mmol/L) + 0.2 × [4-Alb (g/dL)]. All laboratory indicators were tested using blood samples collected before initiation of dialysis. iPTH was measured using immunoradiometric assay, while the rest were analyzed using standard laboratory methods with an autoanalyzer. NPAR was calculated by dividing neutrophils percentage by serum albumin with a formula as: neutrophil percentage (%) ×100/serum albumin (g/dL).20 NLR, and PLR were calculated by dividing neutrophils and platelets by lymphocytes, respectively.
Statistical Analysis
SPSS22.0 statistical software (IBM) was used for the statistical analysis. Regression imputation was used for missing value filling. The normality of distribution of continuous data was evaluated by the Kolmogorov–Smirnov test. Normally distributed continuous variables were expressed as mean ± standard deviation and compared using the t-test of independent samples. Non-normally distributed data were recorded as medians and interquartile range and compared using the Mann–Whitney U-tests. The categorical data were described using counts and percentages and compared using Chi-square test. All research subjects were classified based on the median NPAR. The Pearson’s correlation was used for the normally distributed data, and the Spearman correlation was used for the nonparametric data. The receiver–operating characteristic (ROC) curve was used to identify the predictive ability of NPAR. The Youden index = sensitivity + specificity −1. The optimal cutoff, sensitivity, and specificity of the indicators were obtained by using and the maximum value of the Youden index. All-cause mortality rates were evaluated by Kaplan–Meier analysis with the use of the Log rank test. Univariate and multivariate Cox proportional hazards regression models were used to explore the associations between NPAR and the prognosis of MHD patients. Factors that were significantly related to all-cause mortality were included in multivariate COX regression analysis. Values of p < 0.05 were considered statistically significant.
Results
Baseline Patient Characteristics
As shown in Figure 1 and Table 1, a total of 226 MHD patients were included in the study, with a median age of 56 years, including 146 males (64.6%). Patients were stratified into lower NPAR (≤16.96) and higher NPAR (>16.96) groups according to the median NPAR. Baseline characteristics are summarized in Table 1. Patients in the higher NPAR group were significantly older (median age 58 vs 54 years, p=0.003) and exhibited higher WBC count (7.02×109/L vs 6.27×109/L, p<0.001), higher neutrophil percentages (74.19% vs 63.47%, p<0.001), lower hemoglobin (101.04 g/L vs 112.46 g/L, p<0.001), lower Albumin (3.86 g/dl vs 4.19 g/dl, p=0.000), lower Creatinine (974.37μmol/L vs 1098.97μmol/L, p=0.003), higher Chloride (100.4 mmol/L vs 99.00 mmol/L, p=0.016) and elevated inflammatory markers (NLR: 4.78 vs 2.99, p<0.001; PLR: 199.91vs 153.28, p<0.001; hs-CRP: 8.40 mg/L vs 4.77 mg/L, p<0.001). Non-autogenous arteriovenous fistula (AVF) usage was more prevalent in the higher NPAR group (22.1% vs 8.8%, p=0.006). No significant differences were observed in dialysis duration, BMI, or most biochemical parameters (eg, BUN, potassium, phosphorus).
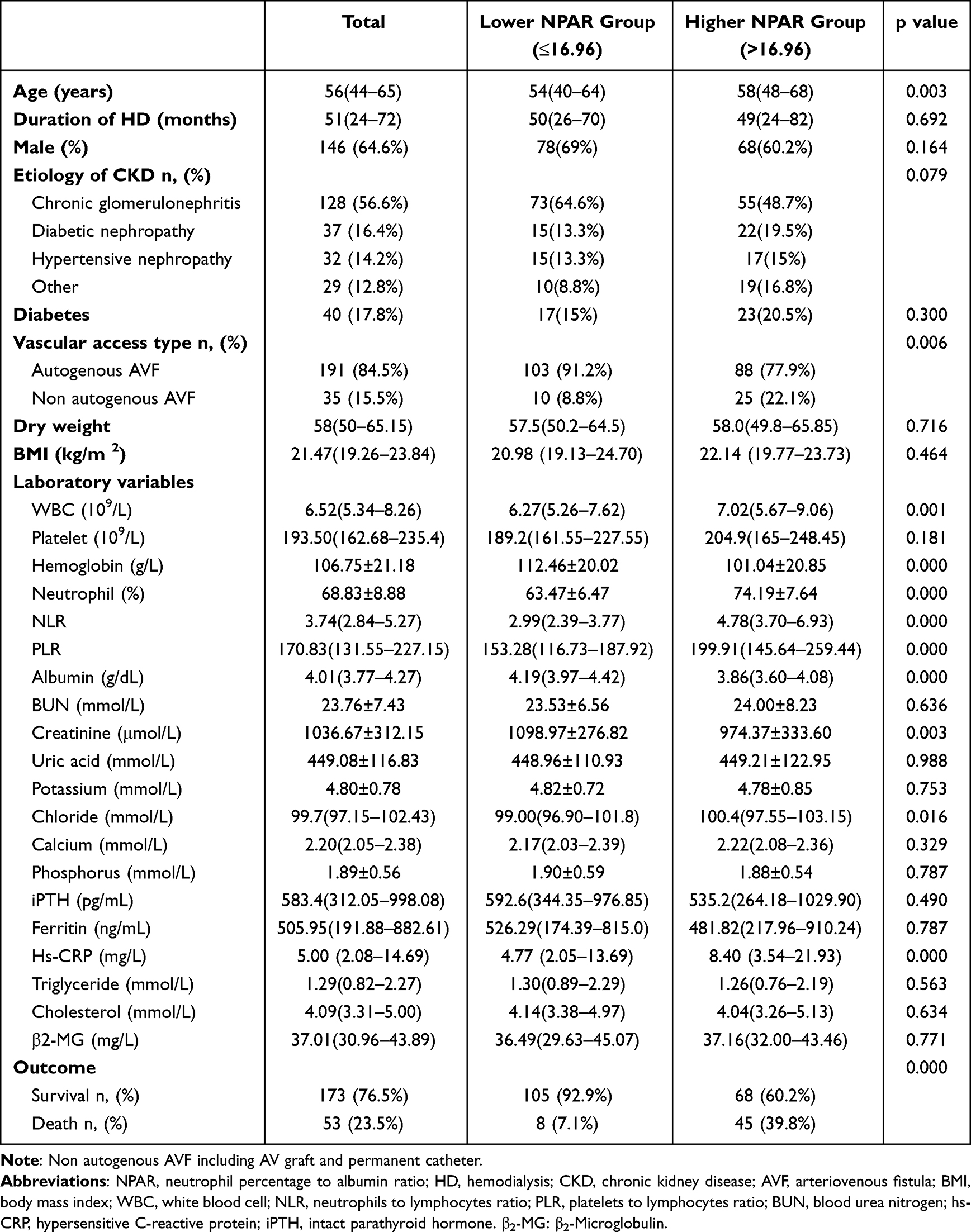 |
Table 1 Characteristics of 226 Maintenance Hemodialysis Patients by NPAR Groups |
 |
Figure 1 Study flow chart. |
Correlation Results Between NPAR and Other Significant Parameters in MHD Patients
NPAR demonstrated significant correlations with inflammatory, nutritional, and clinical parameters (Table 2). It was positively associated with age (r=0.257, p<0.001), WBC count (r=0.303, p<0.001), hs-CRP (r=0.383, p<0.001), NLR (r=0.708, p<0.001), and PLR (r=0.445, p<0.001). Conversely, NPAR showed negative correlations with hemoglobin (r=−0.313, p<0.001), lymphocyte (r=−0.449, p<0.001) and creatinine (r=−0.340, p<0.001).
 |
Table 2 Bivariate Correlation Results Between NPAR and Other Significant Parameters in MHD Patients |
Relationship Between NPAR and All-Cause Mortality in MHD Patients
During the follow-up period, 53 (23.5%) patients died. The mortality rate in the higher NPAR group was significantly higher than that in the lower NPAR group (39.8% vs 7.1%, p=0.000), as shown in Table 1. The Kaplan–Meier survival analysis curve showed that the survival rate of lower NPAR group was significantly higher than that of higher NPAR group (log rank test P=0.000) (Figure 2).
 |
Figure 2 K–M survival curve analysis of MHD patients. |
In the univariate Cox regression analysis, all-cause mortality was associated with age, diabetes mellitus, type of vascular access, WBC, hemoglobin, creatinine, uric acid, phosphorus, NPAR, calcium, and hs-CRP. In multivariate analysis, NPAR remained an independent risk factor (adjusted HR=1.346, 95% CI: 1.192–1.521, p<0.001), alongside age (HR=1.051, 95% CI: 1.024–1.079, p<0.001), non-autogenous AVF (HR=2.564, 95% CI: 1.283–5.123, p=0.008), phosphorus (HR=2.258, 95% CI: 1.176–4.336, p<0.05), and serum calcium (HR=1.080, 95% CI: 1.043–1.118, p<0.001) (Table 3).
 |
Table 3 Univariate and Multivariate Cox Proportional Hazards Regression Analyses of Factors Associated with Mortality |
Prediction of Mortality
Receiver Operating Characteristic (ROC) analysis indicated that the Area Under the Curve (AUC) of NPAR was 0.821 (95% CI: 0.759–0.882, p=0.000), the optimal cutoff was 17.14, with a sensitivity of 0.849 and a specificity of 0.647. The AUC of NPAR had a trend to be better than that of NLR (AUC= 0.710, 95% CI: 0.627–0.793, p=0.000), PLR (AUC=0.647, 95% CI: 0.553–0.741, p=0.001), neutrophil count (AUC=0.606, 95% CI: 0.512–0.700, p=0.019), albumin (AUC=0.752, 95% CI: 0.677–0.826, p=0.000), and hs-CRP (AUC=0.670, 95% CI: 0.583–0.756, p=0.000) (Table 4 and Figure 3).
 |
Table 4 ROC Curves for the Prediction of All-Cause Mortality in MHD Patients of Various Parameters |
 |
Figure 3 ROC curves for the prediction of all-cause mortality in MHD patients of various parameters. |
Discussion
In this prospective study, NPAR was found to be associated with all-cause mortality in MHD patients, and as an independent predictor of mortality, NPAR had a trend to be superior to those traditional inflammation and nutrition markers.21–25 NPAR was also found to be correlated with inflammatory markers, age, and anemia-related parameters in this study. A multicenter study reported recently also discovered high NPAR level was independently associated with a higher increased risk of death in MHD patients.19 These findings provide novel insights into risk stratification and prognostic management for MHD patients.
First, the predictive advantage of NPAR may stem from its dual reflection of systemic inflammation and nutritional status. Albumin, a key hepatic protein, serves as both a sensitive marker of nutritional status and a negative acute-phase reactant in chronic inflammation,26 while elevated neutrophil percentage directly indicates systemic inflammatory activation and activated neutrophil induces and aggravates atherosclerotic cardiovascular disease.27–31 By integrating the interplay between inflammation and nutrition, NPAR may comprehensively capture the pathophysiological features of the “Malnutrition-Inflammation-Atherosclerosis (MIA)” syndrome. MIA is a common condition and associated with poor outcome in ESRD patients.32–34 Unlike hs-CRP reflecting only inflammation or NLR/PLR lacking nutritional assessment, NPAR combines both aspects, potentially explaining its superior predictive efficacy. Interestingly, although BMI as a nutritional indicator and low BMI predicts poor prognosis in MHD patients, we observed no significant linear correlation between NPAR and dry weight/BMI. The reasons may be as follows: (1) Dry weight primarily reflects volume status, while BMI fails to differentiate body composition and predict nutrition status accurately.35,36 (2) Most subjects included in this study had normal BMI, with insufficient high/low-BMI subgroups for stratified analysis. (3) Mortality in hemodialysis population is 10 times higher than that of general population, which is driven more by inflammation and malnutrition than BMI. 37 This underscores unique value of NPAR as a composite marker of the “inflammation-malnutrition axis”, providing prognostic insight independent of weight metrics.
Second, the positive correlations between NPAR and CRP, PLR, and NLR further validate its role as an inflammatory marker. MHD patients often exhibit a microinflammatory state, and persistent inflammation accelerates cardiovascular events and infectious complications by promoting endothelial injury, oxidative stress, and protein-energy wasting.38 Additionally, the negative correlation between NPAR and hemoglobin may suggest inflammation-mediated erythropoietin resistance or iron metabolism dysregulation.39,40 The positive association with age likely reflects the heightened risks of immunosenescence and malnutrition in elderly patients, a phenomenon increasingly recognized in geriatric nephrology.41 These relationships highlight NPAR’s ability to integrate multidimensional pathophysiological processes, thereby enhancing its prognostic value.
From a clinical perspective, NPAR measurement offers distinct advantages: it requires only routine blood tests and biochemical data, incurs no additional costs, and provides immediate results. This makes it particularly suitable for resource-limited settings, aligning with the growing emphasis on cost-effective biomarkers in global nephrology practice42 Dynamic monitoring of NPAR could enable clinicians to identify high-risk patients earlier and tailor anti-inflammatory therapies, nutritional support, or anemia management strategies, potentially improving outcomes. Critically, our identification of an optimal NPAR cutoff at 17.14 provides a clinically actionable threshold for mortality risk stratification in MHD patients.
However, this study has limitations. First, as a single-center analysis, potential selection bias exists, necessitating validation through multicenter prospective cohorts. Second, we measured NPAR for only one time, the optimal cutoff value of NPAR and the prognostic implications of its dynamic changes require further investigation. Third, comparisons with other emerging biomarkers (eg, Klotho protein) were not included, limiting direct benchmarking against cutting-edge prognostic tools. Fourth, the indicators included in this study were limited and may not include all possible prognostic indicators such as residual renal function, therapeutic model, dialysis adequacy, medication, etc. In addition, this is a clinical observational study, the potential mechanisms and their practicality in guiding interventions still need further exploration.
In conclusion, NPAR, dually reflecting inflammation and nutrition, was independently correlated with all-cause mortality in MHD patients. As a simple, cost-effective and available indicator, NPAR can be a routine test to serve the clinic. However, future research should focus on exploring mechanisms, conducting multicenter prospective studies, developing NPAR-based risk scoring systems and validating its role in guiding individualized therapies through interventional trials, ultimately advancing precision management for MHD patients.
Acknowledgments
We are grateful to all participants in this study.
Funding
This study was supported by the Open Project of Guangxi Key Laboratory of Precision Medicine in Cardio-cerebrovascular Diseases Control and Prevention (GXXNXG202103) and Foundation of Guangxi Province Health Commission of China (Z-A20240478).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Hill NR, Fatoba ST, Oke JL, et al. Global prevalence of chronic kidney disease - a systematic review and meta-analysis. PLoS One. 2016;11(7):e0158765. doi:10.1371/journal.pone.0158765
2. Zoccali C, Mallamaci F, Adamczak M, et al. Cardiovascular complications in chronic kidney disease: a review from the European Renal and Cardiovascular Medicine Working Group of the European Renal Association. Cardiovasc Res. 2023;119(11):2017–2032. doi:10.1093/cvr/cvad083
3. Wang Y, Gao L. Inflammation and cardiovascular disease associated with hemodialysis for end-stage renal disease. Front Pharmacol. 2022;13:800950. doi:10.3389/fphar.2022.800950
4. Avesani CM, Sabatino A, Guerra A, et al. A comparative analysis of nutritional assessment using global leadership initiative on malnutrition versus subjective global assessment and malnutrition inflammation score in maintenance hemodialysis patients. J Ren Nutr. 2022;32(4):476–482. doi:10.1053/j.jrn.2021.06.008
5. Okabe H, Muraoka Y, Naka Y, et al. Malnutrition leads to the progression of coronary artery calcification in hemodialysis patients. PLoS One. 2023;18(1):e0280383. doi:10.1371/journal.pone.0280383
6. Reddan DN, Klassen PS, Szczech LA, et al. White blood cells as a novel mortality predictor in haemodialysis patients. Nephrol Dial Transplant. 2003;18(6):1167–1173. doi:10.1093/ndt/gfg066
7. Pifer TB, McCullough KP, Port FK, et al. Mortality risk in hemodialysis patients and changes in nutritional indicators: DOPPS. Kidney Int. 2002;62(6):2238–2245. doi:10.1046/j.1523-1755.2002.00658.x
8. Mehrotra R, Duong U, Jiwakanon S, et al. Serum albumin as a predictor of mortality in peritoneal dialysis: comparisons with hemodialysis. Am J Kidney Dis. 2011;58(3):418–428. doi:10.1053/j.ajkd.2011.03.018
9. Kalantar-Zadeh K, Kilpatrick RD, Kuwae N, et al. Revisiting mortality predictability of serum albumin in the dialysis population: time dependency, longitudinal changes and population-attributable fraction. Nephrol Dial Transplant. 2005;20(9):1880–1888. doi:10.1093/ndt/gfh941
10. Danielski M, Ikizler TA, McMonagle E, et al. Linkage of hypoalbuminemia, inflammation, and oxidative stress in patients receiving maintenance hemodialysis therapy. Am J Kidney Dis. 2003;42(2):286–294. doi:10.1016/S0272-6386(03)00653-X
11. Jiao S, Zhou J, Feng Z, et al. The role of neutrophil percentage to albumin ratio in predicting 1-year mortality in elderly patients with Hip fracture and external validation. Front Immunol. 2023;14:1223464. doi:10.3389/fimmu.2023.1223464
12. Ko CA, Fang KH, Tsai MS, et al. Prognostic value of neutrophil percentage-to-albumin ratio in patients with oral cavity cancer. Cancers. 2022;14(19):4892. doi:10.3390/cancers14194892
13. Lv XN, Shen YQ, Li ZQ, et al. Neutrophil percentage to albumin ratio is associated with stroke-associated pneumonia and poor outcome in patients with spontaneous intracerebral hemorrhage. Front Immunol. 2023;14:1173718. doi:10.3389/fimmu.2023.1173718
14. Liu CF, Chien LW. Predictive role of neutrophil-percentage-to-albumin ratio (NPAR) in nonalcoholic fatty liver disease and advanced liver fibrosis in nondiabetic US adults: evidence from NHANES 2017–2018. Nutrients. 2023;15(8). doi:10.3390/nu15081892
15. Li J, Xiang T, Chen X, et al. Neutrophil-percentage-to-albumin ratio is associated with chronic kidney disease: evidence from NHANES 2009–2018. PLoS One. 2024;19(8):e0307466. doi:10.1371/journal.pone.0307466
16. Rao J, Li Y, Zhang X, et al. The prognostic value of the neutrophil-percentage-to-albumin ratio for all-cause and cardiovascular mortality in chronic kidney disease stages G3a to G5: insights from NHANES 2003–2018. Ren Fail. 2025;47(1):2495861. doi:10.1080/0886022X.2025.2495861
17. Yu Y, Zhong Z, Yang W, et al. Neutrophil percentage-to-albumin ratio and risk of mortality in patients on peritoneal dialysis. J Inflamm Res. 2023;16:6271–6281. doi:10.2147/JIR.S437256
18. Xu M, Huan J, Zhu L, et al. The neutrophil percentage-to-albumin ratio is an independent risk factor for poor prognosis in peritoneal dialysis patients. Ren Fail. 2024;46(1):2294149. doi:10.1080/0886022X.2023.2294149
19. Zhu J, Shi R, Li X, et al. Association between neutrophil percentage-to-albumin ratio and mortality in Hemodialysis patients: insights from a prospective cohort study. BMC Nephrol. 2025;26(1):112. doi:10.1186/s12882-025-04027-0
20. Yu Y, Liu Y, Ling X, et al. The neutrophil percentage-to-albumin ratio as a new predictor of all-cause mortality in patients with cardiogenic shock. Biomed Res Int. 2020;2020:7458451. doi:10.1155/2020/7458451
21. Turkmen K, Guney I, Yerlikaya FH, et al. The relationship between neutrophil-to-lymphocyte ratio and inflammation in end-stage renal disease patients. Ren Fail. 2012;34(2):155–159. doi:10.3109/0886022X.2011.641514
22. Turkmen K, Erdur FM, Ozcicek F, et al. Platelet-to-lymphocyte ratio better predicts inflammation than neutrophil-to-lymphocyte ratio in end-stage renal disease patients. Hemodial Int. 2013;17(3):391–396. doi:10.1111/hdi.12040
23. Ao G, Wang Y, Qi X, et al. Association of neutrophil-to-lymphocyte ratio and risk of cardiovascular or all-cause mortality in chronic kidney disease: a meta-analysis. Clin Exp Nephrol. 2021;25(2):157–165. doi:10.1007/s10157-020-01975-9
24. Yaprak M, Turan MN, Dayanan R, et al. Platelet-to-lymphocyte ratio predicts mortality better than neutrophil-to-lymphocyte ratio in hemodialysis patients. Int Urol Nephrol. 2016;48(8):1343–1348. doi:10.1007/s11255-016-1301-4
25. Ishii H, Aoyama T, Takahashi H, et al. Serum albumin and C-reactive protein levels predict clinical outcome in hemodialysis patients undergoing endovascular therapy for peripheral artery disease. Atherosclerosis. 2013;227(1):130–134. doi:10.1016/j.atherosclerosis.2012.11.034
26. Gama-Axelsson T, Heimburger O, Stenvinkel P, et al. Serum albumin as predictor of nutritional status in patients with ESRD. Clin J Am Soc Nephrol. 2012;7(9):1446–1453. doi:10.2215/CJN.10251011
27. Sadik CD, Kim ND, Luster AD. Neutrophils cascading their way to inflammation. Trends Immunol. 2011;32(10):452–460. doi:10.1016/j.it.2011.06.008
28. Phillipson M, Kubes P. The neutrophil in vascular inflammation. Nat Med. 2011;17(11):1381–1390. doi:10.1038/nm.2514
29. Zhang Y, Li L, Jia L, et al. Neutrophil counts as promising marker for predicting in-hospital mortality in aneurysmal subarachnoid hemorrhage. Stroke. 2021;52(10):3266–3275. doi:10.1161/STROKEAHA.120.034024
30. Luo J, Thomassen JQ, Nordestgaard BG, et al. Neutrophil counts and cardiovascular disease. Eur Heart J. 2023;44(47):4953–4964. doi:10.1093/eurheartj/ehad649
31. Lavillegrand JR, Al-Rifai R, Thietart S, et al. Alternating high-fat diet enhances atherosclerosis by neutrophil reprogramming. Nature. 2024;634(8033):447–456. doi:10.1038/s41586-024-07693-6
32. Mikami R, Mizutani K, Gohda T, et al. Malnutrition- inflammation- atherosclerosis (MIA) syndrome associates with periodontitis in end-stage renal disease patients undergoing hemodialysis: a cross-sectional study. Sci Rep. 2023;13(1):11805. doi:10.1038/s41598-023-38959-0
33. Turkmen K, Kayikcioglu H, Ozbek O, et al. The relationship between epicardial adipose tissue and malnutrition, inflammation, atherosclerosis/calcification syndrome in ESRD patients. Clin J Am Soc Nephrol. 2011;6(8):1920–1925. doi:10.2215/CJN.00890111
34. Maraj M, Kusnierz-Cabala B, Dumnicka P, et al. Malnutrition, inflammation, atherosclerosis syndrome (MIA) and diet recommendations among end-stage renal disease patients treated with maintenance hemodialysis. Nutrients. 2018;10(1):69. doi:10.3390/nu10010069
35. Gracia-Iguacel C, Qureshi AR, Avesani CM, et al. Subclinical versus overt obesity in dialysis patients: more than meets the eye. Nephrol Dial Transplant. 2013;28(Suppl 4):iv175–iv181. doi:10.1093/ndt/gft024
36. Kittiskulnam P, Chertow GM, Kaysen GA, et al. Misclassification of obesity by body mass index among patients receiving hemodialysis. Am J Kidney Dis. 2016;67(4):709–711. doi:10.1053/j.ajkd.2015.09.028
37. de Mutsert R, Snijder MB, van der Sman-de BF, et al. Association between body mass index and mortality is similar in the hemodialysis population and the general population at high age and equal duration of follow-up. J Am Soc Nephrol. 2007;18(3):967–974. doi:10.1681/ASN.2006091050
38. Kaysen GA. The microinflammatory state in uremia: causes and potential consequences. J Am Soc Nephrol. 2001;12(7):1549–1557. doi:10.1681/ASN.V1271549
39. Pergola PE, Devalaraja M, Fishbane S, et al. Ziltivekimab for treatment of anemia of inflammation in patients on hemodialysis: results from a phase 1/2 multicenter, randomized, double-blind, Placebo-Controlled Trial. J Am Soc Nephrol. 2021;32(1):211–222. doi:10.1681/ASN.2020050595
40. Matsuoka T, Abe M, Kobayashi H. Iron metabolism and inflammatory mediators in patients with renal dysfunction. Int J Mol Sci. 2024;25(7):3745. doi:10.3390/ijms25073745
41. Lee TH, Chen JJ, Wu CY, et al. Immunosenescence, gut dysbiosis, and chronic kidney disease: interplay and implications for clinical management. Biomed J. 2024;47(2):100638. doi:10.1016/j.bj.2023.100638
42. Chesnaye NC, Ortiz A, Zoccali C, et al. The impact of population ageing on the burden of chronic kidney disease. Nat Rev Nephrol. 2024;20(9):569–585. doi:10.1038/s41581-024-00863-9
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of Prediction Models for All-Cause Mortality and Cardiovascular Mortality in Patients on Hemodialysis: A Retrospective Cohort Study in China
Yang M, Yang Y, Xu Y, Wu Y, Lin J, Mai J, Fang K, Ma X, Zou C, Lin Q
Clinical Interventions in Aging 2023, 18:1175-1190
Published Date: 28 July 2023
Current Knowledge of Beta-Blockers in Chronic Hemodialysis Patients
Haddiya I, Valoti S
International Journal of Nephrology and Renovascular Disease 2023, 16:223-230
Published Date: 12 October 2023
Neutrophil Percentage-to-Albumin Ratio and Risk of Mortality in Patients on Peritoneal Dialysis
Yu Y, Zhong Z, Yang W, Yu J, Li J, Guo X, Chen J, Mao H, Li Z
Journal of Inflammation Research 2023, 16:6271-6281
Published Date: 21 December 2023
The Relationship Between Fracture and Mortality in a Chinese Maintenance Hemodialysis Patients Cohort
Liu X, Liu Z, Niu Y, Zhang K, Zhang X, Yu C
Journal of Multidisciplinary Healthcare 2024, 17:2031-2038
Published Date: 1 May 2024
The Association Between Lifestyle and All-Cause Mortality in Patients Undergoing Maintenance Hemodialysis: A 3-year Prospective, Observational Study
Zhang L, Zhang S, Tang X
Journal of Multidisciplinary Healthcare 2025, 18:1721-1729
Published Date: 20 March 2025