Back to Journals » Neuropsychiatric Disease and Treatment » Volume 22
The Moderating Role of Social Functioning in the Relationship Between Stigma and Quality of Life in Rural Chinese Patients with Schizophrenia: A Cross-Sectional Study
Authors Wang Q ![]() , Fu T
, Fu T ![]() , Chen S
, Chen S ![]() , Zhang K
, Zhang K
Received 27 December 2025
Accepted for publication 10 March 2026
Published 20 March 2026 Volume 2026:22 592035
DOI https://doi.org/10.2147/NDT.S592035
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Taro Kishi
Qianqian Wang,1,2,* Tinghan Fu,1,2,* Shasha Chen,1,2,* Kai Zhang2– 4
1School of Mental Health and Psychological Sciences, Anhui Medical University, Hefei, People’s Republic of China; 2Department of Psychiatry, The Fourth Affiliated Hospital of Anhui Medical University, Hefei, People’s Republic of China; 3Anhui Psychiatric Center, Anhui Medical University, Hefei, People’s Republic of China; 4Chaohu Hospital of Anhui Medical University, Hefei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Kai Zhang, Department of Psychiatry, The Fourth Affiliated Hospital of Anhui Medical University, Hefei, 238000, People’s Republic of China, Tel/Fax +86-551-82324114, Email [email protected]
Purpose: Individuals with schizophrenia often face significant stigma, social functioning impairments, and poor quality of life. However, the interrelationship among these factors remains insufficiently explored. This study investigates whether social functioning moderates the relationship between stigma and quality of life among rural Chinese individuals with schizophrenia.
Patients and Methods: A cross-sectional study was conducted with 815 rural schizophrenia patients from Chaohu, China. Participants completed the Social Functioning Deficit Screening Scale (SDSS, higher scores indicate poorer social functioning/greater social disability), Social Impact Scale (SIS), the two global items of the WHOQOL-BREF to index overall QOL (higher scores indicate better QOL), Patient Health Questionnaire-9 (PHQ-9), and Insomnia Severity Index (ISI). Moderation analysis was performed using SPSS version 25.0 with the PROCESS macro (version 4.1, Model 1), with PHQ-9 and ISI entered as covariates, examining the stigma × SDSS interaction.
Results: Stigma (β = − 0.132, p < 0.001) and social functional impairment (β = − 0.166, p < 0.001) were both significant independent negative predictors of quality of life. The moderating effect of social functional impairment was significant (β for interaction = 0.094, p = 0.003), explaining an additional 0.85% of the variance (ΔR2 = 0.0085, p = 0.003). Simple slope analysis indicated that stigma had a significantly stronger negative impact on quality of life among individuals with mild social functional impairment (β = − 0.028, p < 0.001), while no significant effect was observed in those with severe impairment (β = − 0.006, p = 0.332). Johnson-Neumann analysis revealed a significant negative impact of stigma in individuals with lower levels of social disability (63.1%).
Conclusion: Social functioning plays a significant moderating role in the relationship between stigma and quality of life in patients with schizophrenia(PWS). Stigma primarily impairs quality of life among patients with better social functioning. These findings suggest the need for a functionally stratified intervention model, prioritizing stigma reduction for patients with higher social functioning while focusing on symptom management and functional recovery for those with greater impairment.
Keywords: schizophrenia, stigma, social functioning, quality of life
Introduction
Schizophrenia is a severe mental disorder characterized by both positive symptoms (such as delusions, hallucinations, disorganized thinking) and negative symptoms (reduced speech, blunted affect, social withdrawal), which significantly impair social functioning. The global lifetime prevalence of schizophrenia is approximately 1%13.1 According to data from the 2019 Global Burden of Disease (GBD 2019), nearly 24 million people worldwide were affected by schizophrenia in 2019.2 Schizophrenia often persists or recurs throughout a patient’s lifetime, severely impairing social functioning and quality of life (QOL) while imposing substantial economic burdens on families and society.3 The World Health Organization (WHO) defines quality of life as a multidimensional construct encompassing physical, psychological, social, and environmental well-being,4 and it is widely recognized as a crucial indicator in schizophrenia research. Consequently, enhancing the QOL for people with schizophrenia (PWS) has become a central objective in modern mental health care and a key marker of treatment success.
Among the numerous factors influencing QOL, stigma recognized as a pernicious and pervasive psychosocial stressor, exerting numerous and highly destructive consequences at the individual, familial, and societal levels.5–7 Stigma operates through multiple mechanisms, including stereotypes (beliefs about dangerousness and incompetence), prejudice (fear and negative attitudes), and discrimination (social avoidance and exclusion).8 Two interrelated dimensions are most frequently studied: public stigma, referring to negative beliefs and discriminatory attitudes held by the general population,8 and self-stigma, the process by which individuals with mental illness internalize societal negative perceptions of their condition,9 with over 40% of PWS experiencing high levels of stigmatization.5,10 A substantial body of evidence has demonstrated that both public and self-stigma independently and negatively predict QOL in this population.11,12 Individuals who anticipate or encounter rejection, devaluation, and discrimination report poorer subjective well-being, reduced life satisfaction, and lower social participation.12
Concurrently, social dysfunction — defined as an impaired ability to engage in routine social activities and maintain social relationships13 — is a hallmark feature of schizophrenia.14 It typically precedes psychotic episodes, persists chronically throughout the illness, and is associated with increased experiences of stigma and diminished QOL.15 In the existing literature, social functioning (or its inverse, social dysfunction/social functioning deficits/social disability) has been consistently identified as an independent determinant of QOL, distinct from symptom severity and cognitive deficits.14,15
Notably, previous studies have largely treated stigma and social functioning as independent predictors of QOL,14–16 examining their main effects in isolation. While this approach has established that both factors matter, it leaves a critical question unanswered: Does the impact of stigma on QOL vary depending on patients’ level of social functioning? In statistical terms, this question concerns moderation rather than mediation. A moderator is a variable that alters the strength or direction of the association between an independent variable (stigma) and a dependent variable (QOL). This is conceptually distinct from mediation, which posits a causal pathway whereby an independent variable influences an outcome through an intermediary variable. In the present study, we are not proposing that stigma improves or worsens QOL because it affects social functioning (mediation); rather, we hypothesize that social functioning may modify—either amplifying or buffering—the relationship between stigma and QOL (moderation).
The theoretical rationale for this moderating hypothesis is grounded in two competing possibilities. On one hand, patients with better-preserved social functioning may possess greater resilience, larger social support networks, and more effective coping resources, which could buffer the negative impact of stigma on their QOL. On the other hand, individuals with higher social functioning are typically more integrated into community life, more exposed to stigmatizing encounters in workplaces, markets, and social gatherings, and may possess greater insight into their illness and societal devaluation.17,18 This heightened awareness and exposure could render them more vulnerable to stigma’s psychological harms,19–21 thereby exacerbating its negative effect on QOL.22 In contrast, for individuals with severe social dysfunction, QOL may be predominantly determined by core symptoms and functional limitations,23 potentially attenuating the unique contribution of stigma. These competing hypotheses—buffering versus exacerbating—remain empirically untested.
This study focuses specifically on rural China, a context that may fundamentally shape each element of this hypothesized moderation model. First, regarding stigma exposure, rural communities in China are typically characterized by dense, kin-based networks and limited anonymity—what sociologists term “acquaintance societies” (shuren shehui).24 In such settings, information about an individual’s illness spreads rapidly, and stigma extends beyond the patient to encompass the entire family through the cultural mechanism of “face” (mianzi, reputation) loss.19 A schizophrenia diagnosis can lead to marriage difficulties for siblings, exclusion from community activities, and lasting damage to family reputation. This collective, inescapable nature of rural stigma may amplify its psychological impact compared to urban environments where individuals can selectively disclose their condition.24.25 Second, access to mental health services in rural China remains severely constrained. Psychiatric resources are concentrated in big cities, leaving vast rural areas with few trained professionals, limited psychiatric clinics, and virtually no community-based rehabilitation programs.25 Patients in remote villages often travel hours for brief consultations, and many rely on primary care physicians with minimal psychiatric training. Geographic barriers, transportation costs, and lost work time create formidable obstacles to consistent treatment, medication adherence, and psychosocial intervention.26 This service scarcity may allow symptoms to persist and social functioning to deteriorate further, potentially modifying how stigma translates into QOL outcomes. Third, social networks in rural areas present a paradox: extended families provide instrumental support, yet these same networks can become chronic stressors if members harbor stigmatizing attitudes or pressure patients to conceal their illness.24 Unlike urban patients who may selectively build alternative support systems, rural individuals are embedded in inescapable social webs where their diagnosis is common knowledge, leaving little room for privacy or identity management.24,25 Fourth, functional outcomes in rural contexts are intimately tied to the capacity for physical labor essential for family survival. Social functioning deficits—reduced motivation, social withdrawal—directly translate into inability to contribute to farm work or household chores, potentially intensifying feelings of worthlessness and amplifying stigma’s negative impact on QOL.24–28
Understanding whether and how social functioning moderates the stigma-QOL relationship carries direct clinical implications. If stigma exerts a stronger negative effect among patients with better social functioning, this subgroup might derive particular benefit from targeted stigma-reduction interventions (cognitive restructuring, narrative enhancement, peer support).17,29 Conversely, if stigma’s impact is attenuated among severely impaired patients, initial treatment efforts might prioritize functional rehabilitation and symptom management before stigma-focused work can be effectively introduced. Such a functionally stratified approach could optimize resource allocation and personalize intervention strategies.
To the best of our knowledge, no previous study has empirically examined the moderating role of social functioning in the stigma-QOL relationship among individuals with schizophrenia, particularly within the understudied context of rural China. To address this gap, the present study aims to: (1) investigate whether social functioning deficits moderate the association between stigma and QOL in a large sample of clinically stable rural Chinese patients with schizophrenia; and (2) determine the direction of this moderating effect—specifically, whether better social functioning buffers against or exacerbates the negative impact of stigma on QOL. Based on the competing theoretical possibilities outlined above, we hypothesize that a significant moderating effect exists but do not prespecify its direction, treating this as an exploratory investigation.
Materials and Methods
Participants
This is a multi-center, cross-sectional study conducted from September to October 2022 in rural communities of Chaohu City, Anhui Province, China. Participants were recruited from 6 suburban districts and 12 townships in the Chaohu region. All participants were enrolled in the Severe Mental Disorder Management Database System in Chaohu City, Anhui Province, which contains over 3000 registered users. The initial sample was selected using stratified sampling from this database, with strata defined by township and village to ensure geographic representativeness of the rural population.
A total of 1,205 questionnaires were distributed, and 815 valid responses were collected, yielding a response rate of 67.6%. The primary reasons for non-participation and invalid questionnaires were: (1) incomplete responses with missing data on key variables (n = 187, 15.5%); (2) refusal to complete the assessment (n = 142, 11.8%); and (3) inability to comprehend or complete the questionnaires due to cognitive or symptom severity (n = 61, 5.1%). Missing data for the remaining variables were minimal (< 5%) and were handled by listwise deletion, as this approach is considered acceptable given the large sample size and low proportion of missingness.30,31
Inclusion criteria were as follows: (1) a confirmed diagnosis of schizophrenia according to the ICD-10 criteria, verified by attending psychiatrists at Chaohu Hospital of Anhui Medical University; (2) clinical stability, defined as no more than a 50% change in the dose of any major psychotropic medication over the past three months;32 (3) an age range of 18 to 75 years; (4) provision of informed consent. Exclusion criteria included: (1) a history of other severe neurological disorders; (2) severe physical illness; (3) history of psychoactive substance abuse; (4) pregnancy or breastfeeding; (5) unwillingness or inability to participate in the assessment.
This study received approval from the Ethics Committee of Chaohu Hospital, Anhui Medical University (No.202212-kyxm-13). All procedures adhered to the principles set out in the Declaration of Helsinki. Written informed consent was obtained from all participants and their legal guardians.
Instruments
Demographic and Clinical Characteristics
We used a self-designed questionnaire to collect sociodemographic and clinical data, including age, gender, body mass index (BMI), education level, religious beliefs, marital status, employment status, average annual household income, smoking history, drinking history, lifestyle habits, duration of illness, and treatment history.
Stigma
The Chinese version of the Social Impact Scale (SIS) was used to assess the level of stigma experienced by the patients.33,34 The SIS consists of 24 items across four dimensions: social rejection, economic insecurity, internalized shame, and social isolation. Items are rated on a 4-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = agree, 4 = strongly agree). The total score is calculated as the sum of all 24 items, ranging from 24 to 96, with higher scores indicating greater perceived stigma. The scale demonstrated excellent internal consistency in this study (Cronbach’s α = 0.927).
Social Functioning
Social functioning was assessed using the Social Disability Screening Schedule (SDSS). The SDSS comprises 10 items evaluating performance across various social roles and domains. Each item is rated on a 3-point scale (0 = no impairment, 1 = partial impairment, 2 = severe impairment), with an additional option for “Not Applicable” when the role context does not apply to the respondent.
In this study, items 2 (marital functioning) and 3 (parental functioning) showed substantial proportions of “Not Applicable” responses. Specifically, 325 participants (39.9%) selected “Not Applicable” for item 2, and 346 participants (42.5%) selected “Not Applicable” for item 3. This pattern reflects the relatively low marriage and fertility rates among individuals with schizophrenia in China, resulting in a considerable subset of patients for whom these role domains are not relevant.35–40
Including these items with conventional scoring (treating “Not Applicable” as 0) would artificially inflate social functioning scores for patients who simply do not occupy these roles, rather than reflecting their true functional capacity in applicable domains. Moreover, the substantial proportion of “Not Applicable” responses would reduce the effective sample size for these items and potentially bias the total score. Therefore, items 2 and 3 were excluded from the total SDSS score calculation. The total SDSS score was based on the remaining 8 items, ranging from 0 to 16, with higher scores indicating more severe social functional impairment (poorer actual social functioning).
To assess the robustness of this decision, we conducted a sensitivity analysis using the full 10-item SDSS scale, with “Not Applicable” responses coded as 0. The moderating effect of social functioning on the stigma-QOL relationship remained highly consistent across both versions. In the primary 8-item model, the interaction term (stigma × social functioning) yielded β = 0.330, p = 0.010. In the sensitivity analysis using the 10-item scale, the interaction term remained significant with β = 0.322, p = 0.013. The nearly identical effect sizes and significance levels confirm that our findings are robust and not attributable to the exclusion of items 2 and 3. The 8-item scale demonstrated good reliability (Cronbach’s α = 0.899), while the full 10-item scale yielded a Cronbach’s α of 0.871.
Quality of Life (QOL)
The measurement of quality of life was based on two general items from the World Health Organization Quality of Life-BREF (WHOQOL-BREF):41,42 (1) “How would you rate your quality of life?” and (2) “How satisfied are you with your health?” Each item is scored on a 5-point Likert scale (1 = very poor/very dissatisfied to 5 = very good/very satisfied). The total QOL score was calculated as the sum of these two items, yielding a possible range of 2 to 10, with higher scores indicating better subjective quality of life. Previous research indicates that these two items show good consistency with the full WHOQOL-BREF.43 The internal consistency for these two items in this study was acceptable (Cronbach’s α = 0.661).
Covariates
Given their strong association with quality of life, depressive symptoms and insomnia were included as covariates in the statistical model.
Depressive Symptoms
We assessed depressive symptoms using the Patient Health Questionnaire-9 (PHQ-9). The total score is calculated as the sum of all 9 items, ranging from 0 to 27, with higher scores indicating more severe depressive symptoms. The Chinese version of the PHQ-9 is widely used in China and demonstrates good reliability and validity.44 In this study, Cronbach’s α was 0.828.
Insomnia
Insomnia severity was measured using the Insomnia Severity Index (ISI). The total score is calculated as the sum of all 7 items, ranging from 0 to 28, with higher scores reflecting more severe clinical insomnia. The Chinese version of the ISI has demonstrated good reliability, validity, and internal consistency.45 The Cronbach’s α for the scale in this study was 0.957.
Statistical Analysis
Data analysis was performed using IBM SPSS Statistics (version 25.0) with the PROCESS macro (version 4.1) developed by Hayes.
Descriptive Analysis
Participants were divided into two groups based on the median SDSS score (cutoff = 11). The high social dysfunction group was defined as those with an SDSS total score ≥11 (n = 417, 51%), while the low social dysfunction group consisted of those with an SDSS total score <11 (n = 398, 49%). Independent samples t-tests (for continuous variables) and chi-square tests (for categorical variables) were employed to compare baseline characteristics between the two groups. All test statistics, exact p-values, and effect sizes (Cohen’s d for t-tests, Cramer’s V for χ2-tests) are reported in Table 1.
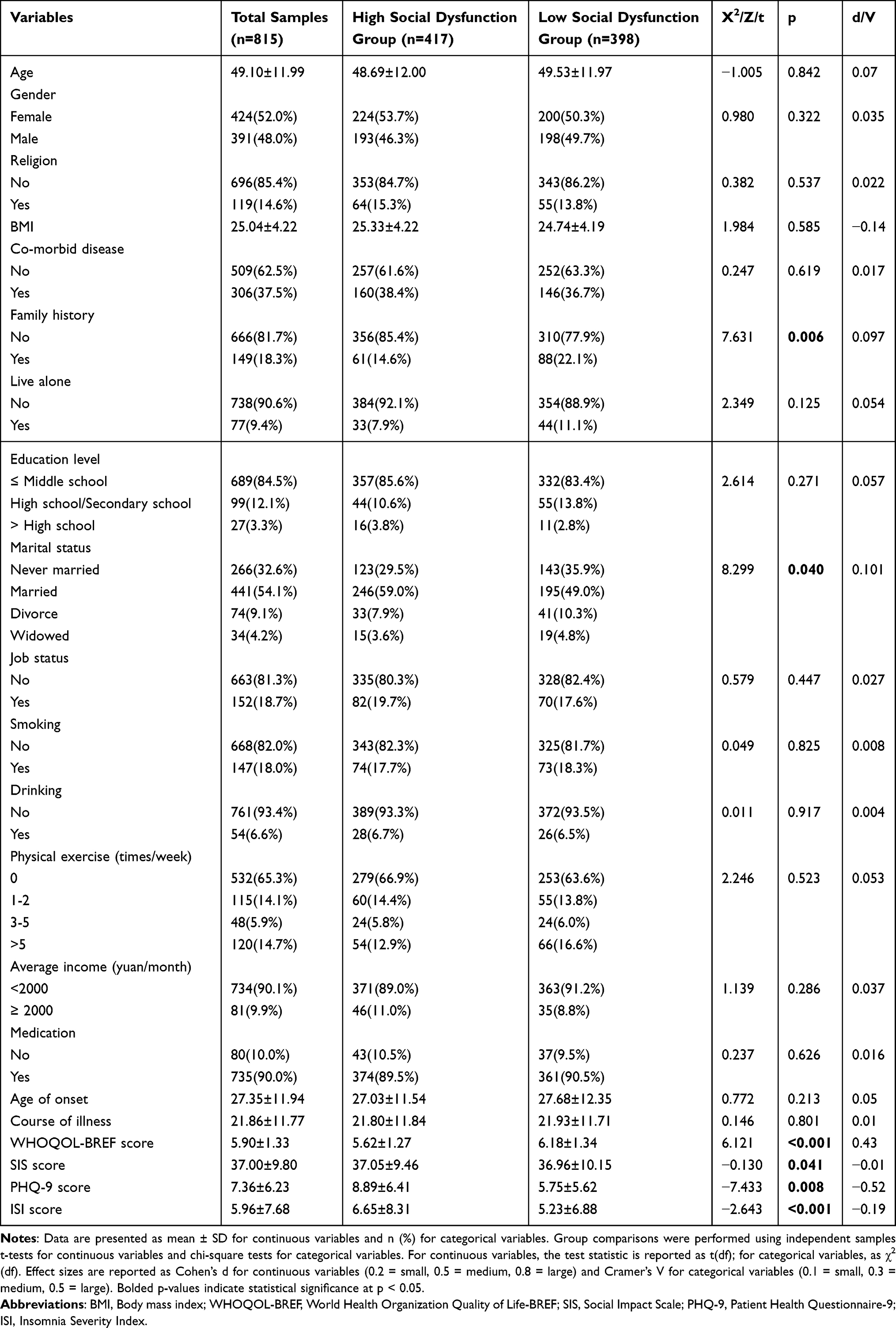 |
Table 1 Demographic and Clinical Characteristics of the Total Sample |
Bivariate Correlations
Prior to analysis, the normality of continuous variables was assessed using the Shapiro–Wilk test. Correlation analyses (Pearson or Spearman) were subsequently performed to assess bivariate relationships among stigmatization, social functioning, QOL, depressive symptoms, and insomnia.
Moderation Analysis
The primary analysis employed PROCESS Model 1 to test the moderating effect of social functioning on the relationship between stigma and QOL. In this model, QOL served as the dependent variable (Y), stigma (SIS total score) as the independent variable (X), and social functioning (SDSS total score) as the moderator (W). To reduce multicollinearity and facilitate interpretation of the interaction term, both the independent variable and moderator were mean-centered prior to analysis. The model controlled for two covariates: depressive symptoms (PHQ-9 total score) and insomnia (ISI total score). A 95% confidence interval was calculated using 5,000 bootstrap samples. A significant moderating effect was indicated if the confidence interval for the interaction term (X × W) did not include zero.
Effect Size for Interaction
To quantify the magnitude of the moderating effect, we report the change in R2 (ΔR2) attributable to the interaction term, along with both unstandardized (B) and standardized (β) regression coefficients. This approach allows readers to gauge the clinical significance of the interaction beyond mere statistical significance.
Post-Hoc Power Analysis
Although the large sample size (N = 815) suggests adequate power, we conducted a post-hoc power analysis using G*Power 3.1 to formally assess the detectable effect size. With α = 0.05, power = 0.80, and 5 predictors in the model, our sample had 80% power to detect a small-to-moderate interaction effect of f2 ≥ 0.02 (equivalent to ΔR2 ≥ 0.02).
Simple Slopes and Johnson-Neyman Technique
When a significant moderating effect was present, simple slope analysis was conducted to examine the conditional effect of stigma on QOL at different levels of social functioning (mean, mean ± 1 standard deviation). Additionally, the Johnson-Neyman technique was applied to identify the precise region of significance for the moderator, detailing the specific SDSS score at which the effect of stigma on QOL transitions between significance and non-significance. The Johnson-Neyman threshold is reported on the original 8-item SDSS metric (range 0–16) to enhance clinical interpretability.
Sensitivity Analyses
To address concerns about limited covariate adjustment, we conducted additional sensitivity analyses incorporating key sociodemographic and clinical covariates available in our dataset, including age, sex, education level (categorized), illness duration, presence of comorbid physical illness, and antipsychotic medication type. These covariates were added sequentially to the primary moderation model to assess the stability of the interaction term. The results of these sensitivity analyses are briefly summarized in the Results section.
Results
Demographic and Clinical Characteristics
The final analysis included 815 clinically stable PWS. As detailed in the Participants section, missing data for the primary analysis variables were minimal and listwise deletion was applied. Based on the predetermined cutoff (SDSS score ≥ 11 for the 8 items), the sample was divided into a “high social dysfunction group” (n = 417, 51%) and a “low social dysfunction group” (n = 398, 49%). Comparisons of demographic and clinical characteristics between the two groups are shown in Table 1.
The two groups were comparable on most demographic variables, including age (48.69 ± 12.00 vs. 49.53 ± 11.97 years, p = 0.842), gender distribution (p = 0.322), educational attainment (p = 0.271), employment status (p = 0.447), BMI (p = 0.585), comorbid physical diseases (p = 0.619), living situation (p = 0.125), medication use (p = 0.626), age of onset (p = 0.213), illness duration (p = 0.801), and lifestyle factors such as smoking (p = 0.825) and drinking (p = 0.917). (all p > 0.05).
However, significant between-group differences emerged for several clinical measures. Patients in the high social dysfunction group reported significantly lower QOL scores (5.62 ± 1.27 vs. 6.18 ± 1.34; t = 6.07, p < 0.001, Cohen’s d = 0.43), higher PHQ-9 scores (8.89 ± 6.41 vs. 5.75 ± 5.62; t = 7.45, p < 0.001, d = 0.52), and higher ISI scores (6.65 ± 8.31 vs. 5.23 ± 6.88; t= 2.70, p = 0.007, d = 0.19) compared to those in the low dysfunction group. The high dysfunction group also exhibited slightly higher stigma scores (SIS: 37.05 ± 9.46 vs. 36.96 ± 10.15; t = 4.19, p = 0.041, d = 0.29). Additionally, family history of psychiatric disorders was more prevalent in the low dysfunction group (22.1% vs. 14.6%; χ2 = 7.63, p = 0.006, Cramer’s V = 0.10), and marital status distribution differed significantly between groups (χ2 = 8.30, p = 0.040, V = 0.10).
Bivariate Correlations
Given that all continuous variables showed significant deviations from normality (Shapiro–Wilk p < 0.05), Spearman’s rank correlation coefficients were calculated to examine bivariate associations among social functioning deficits, quality of life, stigma, depressive symptoms, and insomnia (Table 2). As expected, QOL was significantly negatively correlated with all other clinical variables: social functioning deficits (ρ = −0.274, p < 0.01), stigma (ρ = −0.293, p < 0.01), depressive symptoms (ρ = −0.430, p < 0.01), and insomnia (ρ = −0.226, p < 0.01). These findings indicate that poorer quality of life is associated with greater social functioning impairments, higher perceived stigma, more severe depressive symptoms, and more severe insomnia. Stigma showed significant positive correlations with depressive symptoms (ρ = 0.306, p < 0.01) and insomnia (ρ = 0.216, p < 0.01), but no significant correlation with social functioning deficits (ρ = 0.020, p > 0.05). Social functioning deficits were positively correlated with depressive symptoms (ρ = 0.292, p < 0.01) and insomnia (ρ = 0.051, p < 0.01). Depressive symptoms and insomnia were strongly positively correlated (ρ = 0.469, p < 0.01).
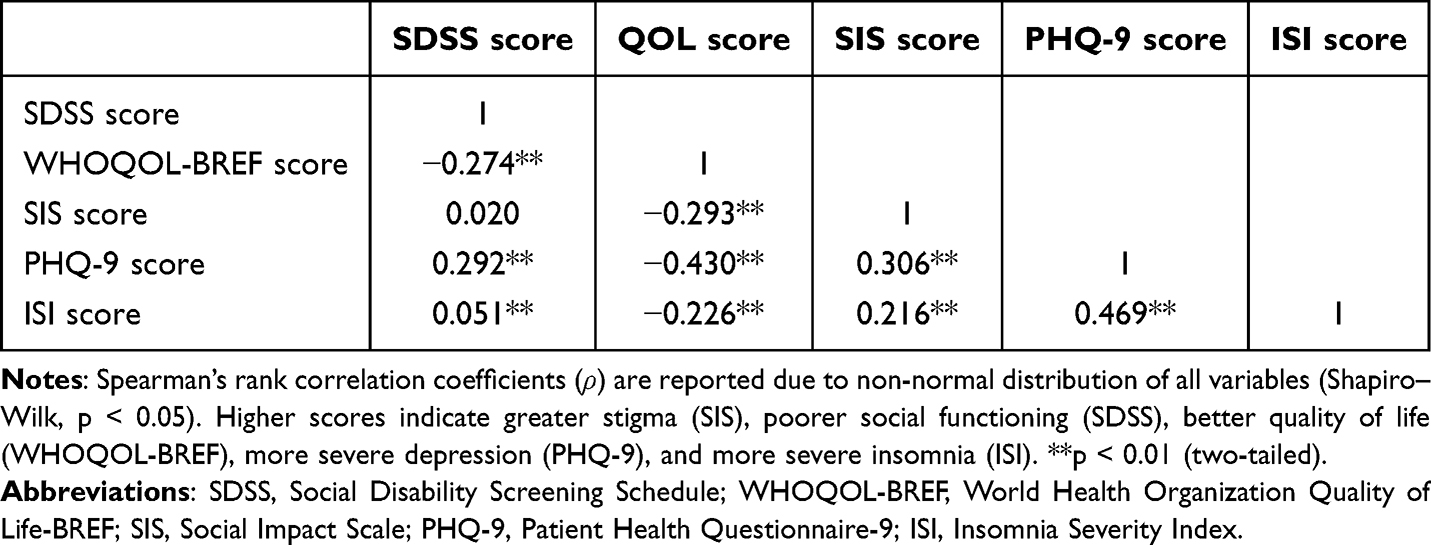 |
Table 2 Correlation Analysis of Social Functioning Deficit, Quality of Life, Stigma, Depression, and Insomnia |
The pattern of correlations supports the examination of social functioning as a moderator rather than a mediator, as stigma and social functioning deficits were not significantly correlated, suggesting they may influence quality of life through relatively independent pathways.
Moderating Effect of Social Functioning Deficits on the Relationship Between Stigma and QOL
Hierarchical regression analysis using PROCESS Model 1 was conducted to test the moderating effect of social functioning deficits on the stigma–QOL relationship. In the first block, mean-centered stigma (CENSIS), mean-centered social functioning deficits (CENSDSS), and covariates (CENPHQ9, CENISI) were entered; the second block added the interaction term (CENSIS × CENSDSS). The overall model was significant, F(5, 809) = 61.11, p < 0.001, explaining 23.6% of the variance in quality of life (R2 = 0.236).
As shown in Table 3, both stigma (B = −0.017, β= −0.123, p < 0.001) and social functioning deficits (B = −0.048, β= −0.166, p < 0.001) had significant negative effects on QOL. Crucially, the interaction between stigma and social functioning deficits was statistically significant (B = 0.002, β = 0.094, p = 0.003), accounting for an additional 0.85% of the variance in QOL (ΔR2 = 0.0085, p= 0.003).
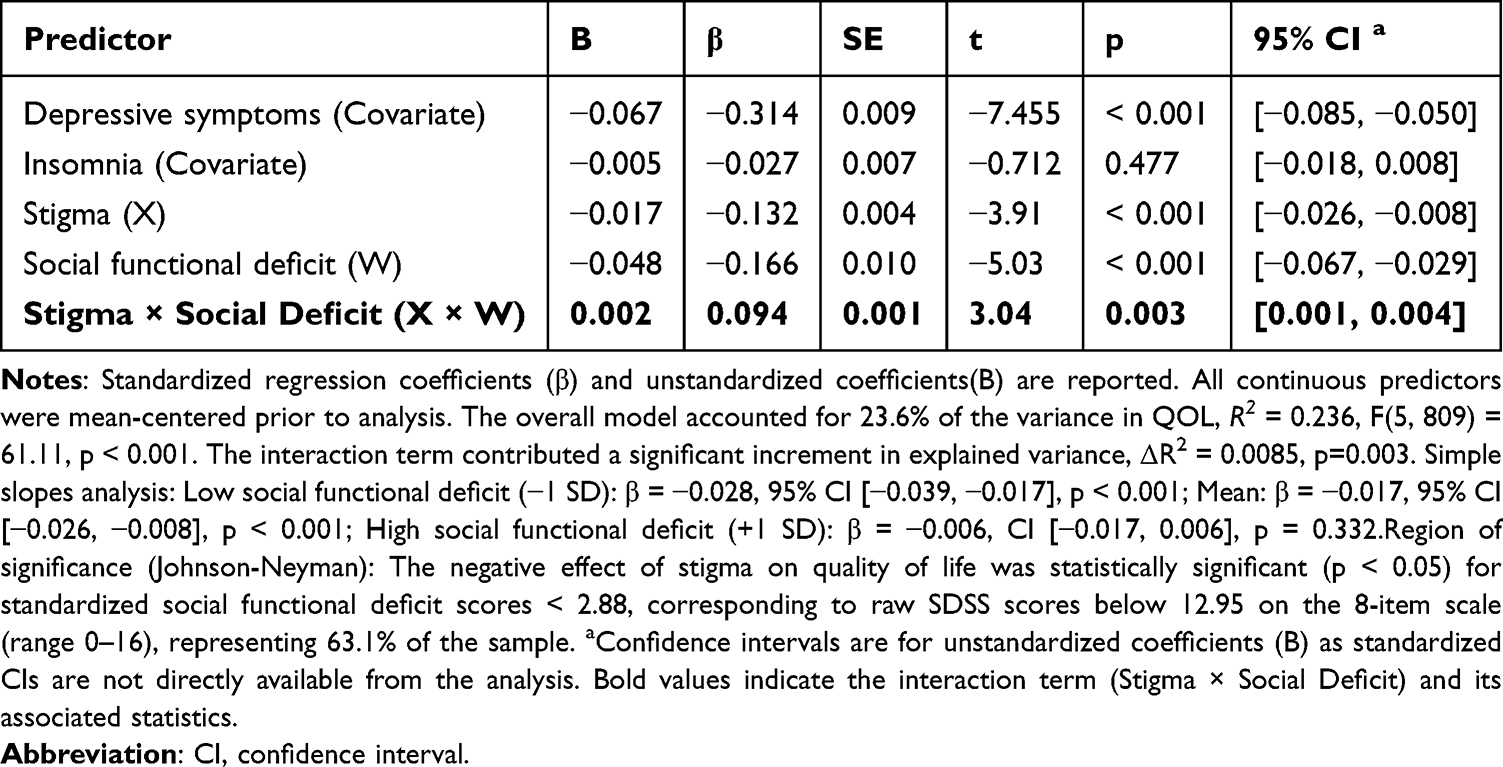 |
Table 3 Moderating Role of Social Functional Deficits on Stigma and QOL |
To interpret this interaction, a simple slope analysis was conducted. As illustrated in Figure 1, the negative association between stigma and QOL was significant and strongest among patients with low social functioning deficits (β = −0.028, 95% CI [−0.039, −0.017], p < 0.001), attenuated among those with moderate deficits (β = −0.017, 95% CI [−0.026, −0.008], p < 0.001), and non-significant among those with high deficits (β = −0.006, 95% CI [−0.017, 0.006], p = 0.332).
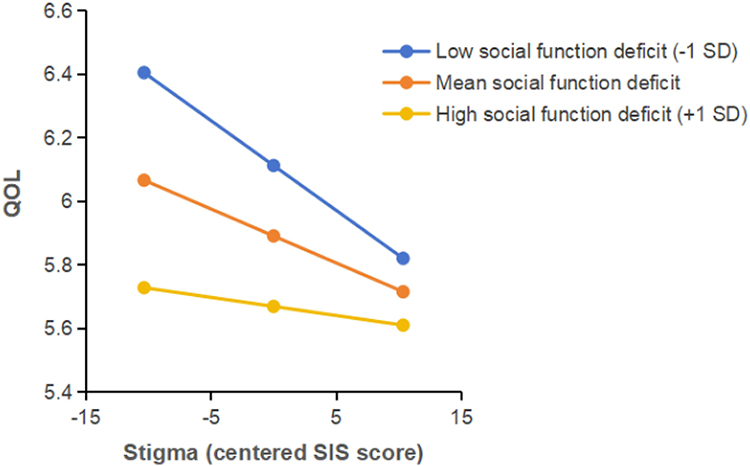 |
Figure 1 Moderating effect of social functional deficit on the relationship between stigma and QOL. Notes: Simple slopes of stigma on quality of life at three levels of social functioning deficits. The three lines represent the predicted QOL values for patients with low social functioning deficits (better functioning, −1 SD below the mean), moderate deficits (mean), and high deficits (poorer functioning, +1 SD above the mean), based on the full range of centered stigma scores (CENSIS, range approximately −10.34 to 10.34). The x-axis represents centered stigma scores (CENSIS), and the y-axis represents quality of life scores (sum of two WHOQOL-BREF global items, range 2–10). The Johnson–Neyman technique indicated that the negative effect of stigma on QOL was statistically significant (p < 0.05) for participants with centered SDSS scores below 2.88, corresponding to raw SDSS scores below 12.95 on the original 8-item scale (range 0–16), representing 63.1% of the sample. |
To precisely delineate the boundary of this moderation effect, we further applied Johnson-Neyman techniques. The results indicated that the negative impact of stigma on QOL was significant (p<0.05)for participants with centered SDSS scores below 2.88, corresponding to raw SDSS scores below 12.95 on the original 8-item scale (range 0–16),representing 63.1% of the sample(seeFigure S1, Supplementary Materials for a visual representation of the conditional effect across the full range of SDSS scores). These findings remained robust in sensitivity analyses adjusting for additional sociodemographic and clinical covariates and when using the full 10-item SDSS scale(all p<0.05).
Sensitivity Analyses
To assess the robustness of the moderating effect, we conducted additional sensitivity analyses incorporating key sociodemographic and clinical covariates available in the dataset, including age, sex, education level (categorized), illness duration, presence of comorbid physical illness, and antipsychotic medication type. These covariates were added sequentially to the primary moderation model. The interaction term (stigma × social functioning deficits) remained statistically significant in all models (all p < 0.05), with ΔR2 values ranging from 0.008 to 0.010, indicating that the findings were robust to adjustment for potential confounders.
Furthermore, to verify that the exclusion of SDSS items 2 and 3 did not bias the results, we conducted a sensitivity analysis using the full 10-item SDSS scale (with“Not Applicable”responses coded as 0). The interaction term remained significant (β = 0.32, p = 0.013), with a ΔR2 of 0.008, nearly identical to the primary 8-item model. This confirms that the observed moderating effect is not an artifact of the item deletion procedure.
Discussion
This study examined the moderating role of social functioning deficits in the relationship between stigma and QOL among clinically stable PWS in rural China. The findings revealed that both stigma and social functioning deficits were independently associated with poorer QOL. More importantly, social functioning deficits significantly moderated the stigma–QOL association: the negative impact of stigma on QOL was strongest among patients with better social functioning (lower deficits), attenuated among those with moderate deficits, and non-significant among those with severe deficits. These results provide novel insights into how the interplay between stigma and social functioning shapes subjective well-being in this underserved population.
Sample Characteristics and Group Comparisons
The sample comprised 815 clinically stable patients, of whom 51% exhibited high social functioning deficits (SDSS≥11). Consistent with previous research,46,47 patients with greater social functioning deficits reported significantly lower QOL, more severe depressive symptoms, and greater insomnia compared to those with milder deficits. Although the absolute difference in stigma scores between the two groups was small, it reached statistical significance(p = 0.041), with the high social dysfunction group reporting slightly higher perceived stigma. These findings underscore the clinical complexity of patients with poorer social functioning, who carry a heavier burden of comorbid symptoms and diminished well-being. The observed differences highlight the importance of considering social functioning as a key stratifying variable in both clinical research and practice.
Bivariate Associations
Spearman correlation analyses revealed that QOL was significantly negatively correlated with social functioning deficits (ρ = −0.274, p < 0.01), stigma (ρ = −0.293, p < 0.01), depressive symptoms (ρ = −0.430, p < 0.01), and insomnia (ρ = −0.226, p < 0.01), consistent with a substantial body of literature documenting the multifaceted determinants of QOL in schizophrenia.7,48–50 Notably, while social functioning deficits showed moderate correlations with depressive symptoms and insomnia, they were not significantly correlated with stigma (ρ = 0.020, p > 0.05). This pattern suggests that stigma and social functioning deficits may influence QOL through relatively independent pathways,51,52 providing empirical justification for examining social functioning as a moderator rather than a mediator in the subsequent analysis.
Interpretation of the Moderating Effect
Consistent with our exploratory hypothesis, social functioning deficits moderated the relationship between stigma and QOL, though the direction of the effect aligned with the vulnerability hypothesis rather than the buffering hypothesis. Patients with better social functioning—who are more likely to be integrated into community life, engaged in social roles, and possess greater awareness of societal attitudes7,17—appeared more susceptible to the detrimental effects of stigma. Specifically, the negative association between stigma and QOL was strongest among patients with low social functioning deficits(β = −0.028, 95% CI [−0.039, −0.017], p < 0.001), attenuated among those with moderate deficits(β = −0.017, 95% CI [−0.026, −0.008], p < 0.001), and non-significant among those with high deficits (β = −0.006, 95% CI [−0.017, 0.006], p = 0.332). In contrast, among patients with severe social functioning deficits, QOL may be predominantly determined by core symptoms and basic functional limitations,23 potentially attenuating the unique contribution of stigma.
It is important to interpret this moderating effect in the context of its magnitude. The interaction term accounted for an additional 0.85% of the variance in QOL (ΔR2 = 0.0085, p= 0.003) representing a small but statistically significant effect according to conventional guidelines.53,54 While this increment may appear modest, it is comparable to effect sizes reported for other psychosocial moderators in schizophrenia research55,56 and underscores that stigma does not operate uniformly across all patients. Even a small effect can have clinical relevance when identifying subgroups for targeted intervention.
Limitations and Methodological Considerations
Several limitations should be considered when interpreting the findings. First, the cross-sectional design precludes causal inferences and cannot establish temporal ordering between stigma, social functioning, and QOL. Longitudinal studies are needed to examine whether changes in stigma precede changes in QOL, and whether social functioning moderates this trajectory over time.
Second, measurement constraints may have influenced the results. The use of two global items from the WHOQOL-BREF to assess QOL, although practical and previously validated,38 may not capture the full multidimensionality of this construct. It is possible that stigma and social functioning differentially affect specific QOL domains (such as psychological and social relationships), which could not be disentangled in the present study. Additionally, measurement constraints related to the SDSS should be acknowledged. The exclusion of items 2 (marital functioning) and 3 (parental functioning) due to high “Not Applicable” rates (39.9% and 42.5%, respectively) was justified psychometrically and supported by sensitivity analyses showing consistent results with the full 10-item scale (β= 0.32, p = 0.013). However, this modification may limit comparability with studies using the complete instrument. The non-significant association between stigma and social functioning deficits in the severe impairment group could reflect a floor effect: patients with the most severe deficits may have limited variability in SDSS scores, reducing statistical power to detect moderation effects within this subgroup. Furthermore, the assessment of depressive symptoms and insomnia relied on self-report measures (PHQ-9 and ISI), which may be subject to recall bias and do not substitute for clinical interviews. This limitation is particularly relevant given that self-reported symptoms may be influenced by stigma-related distress or social desirability concerns. Future research should consider incorporating clinician-administered assessments to validate these findings.
Third, the observed moderating effect could be influenced by unmeasured confounders. We lacked measures of symptom severity (positive and negative symptoms), cognitive function, and illness insight—factors that may affect both social functioning and QOL and could alter the stigma–QOL relationship.57,58 Future studies should include these variables to test whether the moderating effect of social functioning persists after more comprehensive adjustment.
Fourth, potential selection bias should be acknowledged. Although participants were recruited through systematic sampling, 390 individuals were excluded due to incomplete data or refusal to participate. However, comparisons between included and excluded participants revealed no significant differences in available demographic characteristics (all p>0.05), mitigating this concern to some extent.
Fifth, the present sample spanned a wide age range (18–75 years), and it is plausible that the experience and impact of stigma may differ across the lifespan. Older adults in rural communities may face more intense community-driven stigma due to longstanding social networks and traditional beliefs, whereas younger patients may be more vulnerable to internalized stigma as they navigate identity formation and social integration.59,60 Although our sensitivity analyses adjusted for age as a covariate and demonstrated that the core moderating effect remained robust, this statistical adjustment does not fully capture potential qualitative differences in stigma experiences across age groups. The Social Impact Scale (SIS) used in this study measures overall perceived stigma but does not distinguish between community-driven stigma and internalized stigma—a distinction that may be particularly relevant for understanding age-specific patterns. Future research employing multidimensional stigma measures (such as distinguishing enacted, anticipated, and internalized stigma) is needed to elucidate whether age moderates not only the strength but also the nature of the stigma–social functioning–QOL relationship. Similarly, sex differences, illness stage, and cognitive decline (particularly among older participants) may influence both stigma experiences and social functioning outcomes.61,62 While our sensitivity analyses adjusted for sex and illness duration, the lack of direct measures of cognitive function and illness insight limits our ability to fully account for these factors. Studies incorporating comprehensive neuropsychological assessments and stage-of-illness stratification would provide a more nuanced understanding of how individual characteristics shape thestigma–social functioning–QOL dynamic.
Finally, the study was conducted in a single rural region of China (Chaohu City, Anhui Province), which may limit generalizability to other populations with different cultural, economic, and healthcare contexts. Multicenter studies across diverse regions are warranted.
Clinical Implications
The present findings offer preliminary, hypothesis-generating insights for clinical practice. The observation that stigma exerts a stronger negative impact on QOL among patients with better social functioning suggests that stigma-reduction interventions may be particularly beneficial for this subgroup. Approaches such as psychoeducation, cognitive restructuring, narrative enhancement and cognitive therapy (NECT), and peer support groups could help these individuals cope with perceived discrimination and internalized shame.63,64
For patients with severe social functioning deficits, the primary therapeutic target may need to be functional rehabilitation before stigma-focused work can be effectively introduced. Interventions aimed at improving basic daily living skills, social competence, and community integration65 may enhance functional capacity, potentially creating a foundation upon which these individuals can later engage with stigma-related concerns. This functionally stratified approach aligns with the growing emphasis on personalized, stage-specific interventions in schizophrenia care.66
Given the modest effect size (ΔR2 =0.0085), these recommendations should be viewed as tentative and require validation in longitudinal and intervention studies. The small incremental variance explained by the interaction also highlights that many other factors—including symptom severity, cognitive function, and social support—contribute to QOL and should not be overlooked in comprehensive treatment planning.
Conclusion
In summary, this is the first study to examine the role of social functioning in the relationship between stigma and QOL. This cross-sectional study demonstrates that social functioning deficits moderate the relationship between stigma and QOL in clinically stable PWS in rural China. The negative association between stigma and QOL was significantly stronger among patients with better social functioning, while it was non-significant among those with severe deficits (ΔR2 = 0.0085, p = 0.003). These findings suggest that the impact of stigma on QOL is not uniform across all patients, and may inform functionally stratified intervention approaches — prioritizing stigma reduction for those with better functioning and functional rehabilitation for those with severe deficits. However, given the cross-sectional design, modified SDSS scoring, brief QOL measure, modest effect size, wide age range, and reliance on self-reported depression and insomnia, these results require validation in longitudinal studies with comprehensive assessments.
Acknowledgments
The authors thank The Fourth Affiliated Hospital of Anhui Medical University.
Funding
This study was supported by the Key Project of Research Fund of Anhui Institute of Translational Medicine (2023zhyx-B18), the Hengrui innovative drug research project of Anhui Provincial Health Commission (AHWJ2023BAc10004), the Key Research Project on Enhancing Medical Service Capabilities of County Medical Institutions of National Health Commission Hospital Management Research Institute (PS202518), the Anhui Province Traditional Chinese Medicine Inheritance and Innovation Research Program (2025CCCX003), the Huainan Science and Technology Plan Project (2023A286), and the Research Fund of Anhui Medical University (2023xkj064). The funders had no role in the study design, data collection, and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. McCutcheon RA, Reis Marques T, Howes OD. Schizophrenia—an overview. JAMA Psychiatry. 2020;77(2):201–15. doi:10.1001/jamapsychiatry.2019.3360
2. Solmi M, Seitidis G, Mavridis D, et al. Incidence, prevalence, and global burden of schizophrenia - data, with critical appraisal, from the Global Burden of Disease (GBD) 2019. Mol Psychiatry. 2023;28(12):5319–5327. doi:10.1038/s41380-023-02138-4
3. Germain N, Kymes S, Löf E, Jakubowska A, François C, Weatherall J. A systematic literature review identifying associations between outcomes and quality of life (QoL) or healthcare resource utilization (HCRU) in schizophrenia. J Med Econ. 2019;22(5):403–413. doi:10.1080/13696998.2019.1576694
4. Whoqol Group. The World Health Organization quality of life assessment (WHOQOL): position paper from the World Health Organization. Soc Sci Med. 1995;41(10):1403–1409. doi:10.1016/0277-9536(95)00112-k
5. Parrott S, Eckhart N. Stigma in the news: the representation and trivialization of stigma in U.S. Health Commun. 2021;36(4):440–447. doi:10.1080/10410236.2019.1693132
6. Valery KM, Prouteau A. Schizophrenia stigma in mental health professionals and associated factors: a systematic review. Psychiatry Res. 2020;290:113068. doi:10.1016/j.psychres.2020.113068
7. Gagiu C, Dionisie V, Manea MC, Mazilu DC, Manea M. Internalized stigma, self-esteem, and perceived social support as psychosocial predictors of quality of life in adult patients with schizophrenia. J Clin Med. 2024;13(22):6959. doi:10.3390/jcm13226959
8. Dubreucq J, Plasse J, Franck N. Self-stigma in serious mental illness: a systematic review of frequency, correlates, and consequences. Schizophr Bull. 2021;47(5):1261–1287. doi:10.1093/schbul/sbaa181
9. Eliasson ET, McNamee L, Swanson L, Lawrie SM, Schwannauer M. Unpacking stigma: meta-analyses of correlates and moderators of personal stigma in psychosis. Clin Psychol Rev. 2021;89:102077. doi:10.1016/j.cpr.2021.102077
10. Brohan E, Elgie R, Sartorius N, Thornicroft G, GAMIAN-Europe Study Group. Self-stigma, empowerment and perceived discrimination among people with schizophrenia in 14 European countries: the GAMIAN-Europe study. Schizophr Res. 2010;122(1–3):232–238. doi:10.1016/j.schres.2010.02.1065
11. Reisinger BAA, Gleaves DH. Comparing social stigma of dissociative identity disorder, schizophrenia, and depressive disorders. J Trauma Dissociat. 2023;24(2):171–184. doi:10.1080/15299732.2022.2119459
12. Morgades-Bamba CI, Fuster-Ruizdeapodaca MJ, Molero F. Internalized stigma and its impact on schizophrenia quality of life. Psychol Health Med. 2019;24(8):992–1004. doi:10.1080/13548506.2019.1612076
13. Gu Y, Peng H, Dai J, et al. Evaluation of paliperidone on social function in patients with chronic schizophrenia. Gen Psychiatry. 2018;31(2):e000011. doi:10.1136/gpsych-2018-000011
14. Chen P, Hong W. Neural circuit mechanisms of social behavior. Neuron. 2018;98(1):16–30. doi:10.1016/j.neuron.2018.02.026
15. Kimhy D, Tay C, Vakhrusheva J, et al. Enhancement of aerobic fitness improves social functioning in individuals with schizophrenia. Eur Arch Psychiatry Clin Neurosci. 2021;271(2):367–376. doi:10.1007/s00406-020-01220-0
16. Degnan A, Berry K, Humphrey C, Bucci S. The relationship between stigma and subjective quality of life in psychosis: a systematic review and meta-analysis. Clin Psychol Rev. 2021;85:102003. doi:10.1016/j.cpr.2021.102003
17. Luo H, Li Y, Yang BX, Chen J, Zhao P. Psychological interventions for personal stigma of patients with schizophrenia: a systematic review and network meta-analysis. J Psychiatr Res. 2022;148:348–356. doi:10.1016/j.jpsychires.2022.02.010
18. Ohi K, Sumiyoshi C, Fujino H, et al. A 1.5-Year longitudinal study of social activity in patients with schizophrenia. Front Psychiatry. 2019;10:567. doi:10.3389/fpsyt.2019.00567
19. Lysaker PH, Davis LW, Warman DM, Strasburger A, Beattie N. Stigma, social function and symptoms in schizophrenia and schizoaffective disorder: associations across 6 months. Psychiatry Res. 2007;149(1–3):89–95. doi:10.1016/j.psychres.2006.03.007
20. Ebuenyi ID, Regeer BJ, Ndetei DM, Bunders-Aelen JFG, Guxens M. Experienced and anticipated discrimination and social functioning in persons with mental disabilities in kenya: implications for employment. Front Psychiatry. 2019;10:181. doi:10.3389/fpsyt.2019.00181
21. Şengün Inan F, Sarı A, Çetinkaya Duman Z. ‘They don’t include me and my family in a normal picture…’ perspectives of people with schizophrenia on family stigma and its effects on their lives. Int J Ment Health Nurs. 2025;34(1):e70015. doi:10.1111/inm.70015
22. Sedić B, Štrkalj Ivezić S, Petrak O, Ilić B. Differences in resilience, self-stigma and mental health recovery between patients with schizophrenia and depression. Psychiatry Danub. 2021;33(Suppl 4):518–528.
23. Lu Z, Sun J, Zhao G, et al. Schizophrenia: from mechanism to therapy. Sci China Life Sci. 2026. doi:10.1007/s11427-025-2990-0
24. Yang LH. Application of mental illness stigma theory to Chinese societies: synthesis and new directions. Singapore Med J. 2007;48(11):977–985.
25. Xu J, Wang J, King M, et al. Rural-urban disparities in the utilization of mental health inpatient services in China: the role of health insurance. Int J Health Econ Manag. 2018;18(4):377–393. doi:10.1007/s10754-018-9238-z
26. Ying Y, Dong L, Zhang L, Kong F, Yang J, Huang X. Rural-urban differences in the association between home-based community care services satisfaction and mental health status among older adults in Zhejiang Province, China: a cross-sectional study. Front Public Health. 2024;12:1449670. doi:10.3389/fpubh.2024.1449670
27. Zhang Z, Sun K, Jatchavala C, et al. Overview of stigma against psychiatric illnesses and advancements of anti-stigma activities in six Asian Societies. Int J Environ Res Public Health. 2019;17(1):280. doi:10.3390/ijerph17010280
28. Ran MS, Hall BJ, Su TT, et al. Stigma of mental illness and cultural factors in Pacific Rim region: a systematic review. BMC Psychiatry. 2021;21(1):8. doi:10.1186/s12888-020-02991-5
29. Gao X, Wu L, Jin G, Yu K, Yu X. Effects of mindfulness-based interventions on insight and stigma in patients with schizophrenia: a systematic review and meta-analysis. Front Psychiatry. 2025;16:1655057. doi:10.3389/fpsyt.2025.1655057
30. Zheng S, Wang R, Zhang S, et al. Depression severity mediates stigma and quality of life in clinically stable people with schizophrenia in rural China. BMC Psychiatry. 2023;23(1):826. doi:10.1186/s12888-023-05355-x
31. Schoemann AM, Moore EWG, Yagiz G. How and why to follow best practices for testing mediation models with missing data. Int J Psychol. 2025;60(1):e13257. doi:10.1002/ijop.13257
32. Li YC, Bai W, Cai H, et al. Suicidality in clinically stable bipolar disorder and schizophrenia patients during the COVID-19 pandemic. Transl Psychiatry. 2022;12(1):303. doi:10.1038/s41398-022-02045-2
33. Fife BL, Wright ER. The dimensionality of stigma: a comparison of its impact on the self of persons with HIV/AIDS and cancer. J Health Soc Behav. 2000;41(1):50–67.
34. Pan AW, Chung L, Fife BL, Hsiung PC. Evaluation of the psychometrics of the social impact scale: a measure of stigmatization. Int J Rehabil Res. 2007;30(3):235–238. doi:10.1097/MRR.0b013e32829fb3db
35. Aggarwal S, Grover S, Chakrabarti S. A comparative study evaluating the marital and sexual functioning in patients with schizophrenia and depressive disorders. Asian J Psychiatr. 2019;39:128–134. doi:10.1016/j.ajp.2018.12.021
36. Bhatia T, Franzos MA, Wood JA, Nimgaonkar VL, Deshpande SN. Gender and procreation among patients with schizophrenia. Schizophr Res. 2004;68(2–3):387–394. doi:10.1016/j.schres.2003.08.009
37. Mansour H, Kandil K, Wood J, et al. Reduced fertility and fecundity among patients with bipolar I disorder and schizophrenia in Egypt. Psychiatry Invest. 2011;8(3):214–220. doi:10.4306/pi.2011.8.3.214
38. Zhang L, Chen Y, Sun Y, Zhou Y, Li Q, Jia Y. Prevalence of sexual dysfunction in Chinese patients with schizophrenia: a systematic review and meta-analysis. Sex Med. 2024;12(2):qfae009. doi:10.1093/sexmed/qfae009
39. Lo LE, Kaur R, Meiser BG, Green MJ. Risk of schizophrenia in relatives of individuals affected by schizophrenia: a meta-analysis. Psychiatry Res. 2020;286:112852. doi:10.1016/j.psychres.2020.112852
40. Foley DL, Mackinnon A, Morgan VA, et al. Common familial risk factors for schizophrenia and diabetes mellitus. Aust N Z J Psychiatry. 2016;50(5):488–494. doi:10.1177/0004867415595715
41. The WHOQOL Group. Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol Med. 1998;28(3):551–558. doi:10.1017/s0033291798006667
42. Kruithof N, Haagsma JA, Karabatzakis M, et al. Validation and reliability of the abbreviated World Health Organization Quality of Life Instrument (WHOQOL-BREF) in the hospitalized trauma population. Injury. 2018;49(10):1796–1804. doi:10.1016/j.injury.2018.08.016
43. Li M, Xia L, Yang Y, et al. Depression, anxiety, stress, and their associations with quality of life in a nationwide sample of psychiatrists in China during the COVID-19 pandemic. Front Psychol. 2022;13:881408. doi:10.3389/fpsyg.2022.881408
44. Bian CD, He XY, Qian J, Wu WY, Li CB. Application of the patient health questionnaire depression symptom cluster scale in general hospitals. J Tongji Univer. 2009;30(05):136–140.
45. Chung KF, Kan KK, Yeung WF. Assessing insomnia in adolescents: comparison of insomnia severity index, athens insomnia scale and Sleep Quality Index. Sleep Med. 2011;12(5):463–470. doi:10.1016/j.sleep.2010.09.019
46. Porcelli S, Van Der Wee N, van der Werff S, et al. Social brain, social dysfunction and social withdrawal. Neurosci Biobehav Rev. 2019;97:10–33. doi:10.1016/j.neubiorev.2018.09.012
47. Mittal VA, Chang WC, Walker EF. Negative symptoms across developmental stages in psychosis spectrum. Schizophr Res. 2026;289:100–105. doi:10.1016/j.schres.2026.01.018
48. Gaebel W, Zäske H, Hesse K, et al. Promoting stigma coping and empowerment in patients with schizophrenia and depression: results of a cluster-RCT. Eur Arch Psychiatry Clin Neurosci. 2020;270(5):501–511. doi:10.1007/s00406-019-01064-3
49. Caqueo-Urízar A, Urzúa A, Habib J, et al. Relationships between social stigma, stigma experience and self-stigma and impaired quality of life in schizophrenia across three Latin-American countries. Eur Arch Psychiatry Clin Neurosci. 2020;270(5):513–520. doi:10.1007/s00406-019-01035-8
50. Kashiwagi H, Matsumoto J, Miura K, et al. Neurocognitive features, personality traits, and social function in patients with schizophrenia with a history of violence. J Psychiatr Res. 2022;147:50–58. doi:10.1016/j.jpsychires.2022.01.012
51. Mao Z, Tian L, Sun Y, Dong F, Wang C, Bo Q. Quality of life and its predictors in first-episode schizophrenia and individuals at clinical high-risk for psychosis. BMC Psychiatry. 2023;23(1):793. doi:10.1186/s12888-023-05303-9
52. Durgoji S, Muliyala KP, Jayarajan D, Chaturvedi SK. Quality of life in schizophrenia: what is important for persons with schizophrenia in India? Indian J Psychol Med. 2019;41(5):420–427. doi:10.4103/IJPSYM.IJPSYM_71_19
53. Martins D, Paduraru M, Paloyelis Y. Heterogeneity in response to repeated intranasal oxytocin in schizophrenia and autism spectrum disorders: a meta-analysis of variance. Br J Pharmacol. 2022;179(8):1525–1543. doi:10.1111/bph.15451
54. Howes OD, Chapman GE. Understanding variability: the role of meta-analysis of variance. Psychol Med. 2024. doi:10.1017/S0033291724001971
55. Carey EG, Ridler I, Ford TJ, Stringaris A. Editorial perspective: when is a ‘small effect’ actually large and impactful? J Child Psychol Psychiatr. 2023;64(11):1643–1647. doi:10.1111/jcpp.13817
56. Jagan S, Mohd Daud TI, Chia LC, et al. Evidence for the effectiveness of psychological interventions for internalized stigma among adults with schizophrenia spectrum disorders: a systematic review and meta-analyses. Int J Environ Res Public Health. 2023;20(8):5570. doi:10.3390/ijerph20085570
57. Cai R, Zhu Z, Li Y, et al. Relationship between negative symptoms, cognitive function and social function in schizophrenia: new insight from a network analysis. Front Psychiatry. 2025;16:1623147. doi:10.3389/fpsyt.2025.1623147
58. Taha SM, Abdelraof AI, El-Monshed AH, Amr M, Elhay ESA. Insight and empathy in schizophrenia: impact on quality of life and symptom severity. Arch Psychiatr Nurs. 2024;52:60–68. doi:10.1016/j.apnu.2024.07.013
59. Pribadi T, Lin EC, Chen PS, Lee SK, Fitryasari R, Chen CH. Factors associated with internalized stigma for Indonesian individuals diagnosed with schizophrenia in a community setting. J Psychiatr Ment Health Nurs. 2020;27(5):584–594. doi:10.1111/jpm.12611
60. Chen J, Zhang Y, Chen S, Wang W. Navigating stigma and somatization: a qualitative exploration of mental health experiences among middle-aged adults in rural China. BMC Psychol. 2025;13(1):400. doi:10.1186/s40359-025-02707-y
61. Gonzales L, Saperstein AM, Qian M, Gorecki A, Medalia A. Psychiatric and functional correlates of stigma associated with cognitive impairment in schizophrenia. Psychiatry Res. 2024;342:116233. doi:10.1016/j.psychres.2024.116233
62. Fekih-Romdhane F, Ben Ali S, Ghazouani N, et al. Gender-based differences in internalized stigma and its predictors among patients with schizophrenia: a cross-sectional Tunisian study. Middle East Curr Psych. 2025;32(1):15. doi:10.1186/s43045-025-00582-2
63. Shih CA, Huang JH, Yang MH. Anti-stigma psychosocial intervention effects on reducing mental illness self-stigma and increasing self-esteem among patients with schizophrenia in Taiwan: a quasi-experiment. Asian J Psychiatr. 2022;73:103171. doi:10.1016/j.ajp.2022.103171
64. Dai J, Sun D, Li B, et al. Mixed-Mode Mindfulness-based cognitive therapy for psychological resilience, self esteem and stigma of patients with schizophrenia: a randomized controlled trial. BMC Psychiatry. 2024;24(1):179. doi:10.1186/s12888-024-05636-z
65. Kadakia A, Fan Q, Shepherd J, et al. Point-in-time survey of healthcare resource utilization, employment, quality of life and caregiver status by disease severity in patients with schizophrenia in the US. Curr Med Res Opin. 2022;38(3):469–478.
66. DeLisi LE. A lifetime of mental health treatments for people with schizophrenia: update and narrative review. Curr Opin Psychiatry. 2024;37(3):140–146. doi:10.1097/YCO.0000000000000926
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Impact of Childhood Trauma and Adult Separation Anxiety Disorder on Quality of Life in Individuals with Schizophrenia
Karaytuğ MO, Tamam L, Demirkol ME, Namlı Z, Gürbüz M, Yeşiloğlu C
Neuropsychiatric Disease and Treatment 2023, 19:181-196
Published Date: 23 January 2023
Personal and Social Functioning and Health-Related Quality of Life in Patients with Schizophrenia Treated with the Long-Acting Injectable Antipsychotic Risperidone ISM
Litman R, Naber D, Anta L, Martínez J, Filts Y, Correll CU
Neuropsychiatric Disease and Treatment 2023, 19:219-232
Published Date: 25 January 2023
Social Stigma Toward Individuals with Schizophrenia in a Lebanese Population
Tantawi SA, Kamaleddine AN, Alhajj LA, Naous SM, Kamaleddine NN, Chung S, Joo SW
Neuropsychiatric Disease and Treatment 2024, 20:561-570
Published Date: 8 March 2024
Systematic Literature Review of Studies Reporting Measures of Functional Outcome or Quality of Life in People with Negative Symptoms of Schizophrenia
Hadzi Boskovic D, Smith-Palmer J, Pöhlmann J, Pollock RF, Hwang S, Bruhn D
Patient Related Outcome Measures 2024, 15:199-217
Published Date: 17 June 2024
A Study on the Current Situation of Stigma and Its Influencing Factors Among Chinese Patients with Port-Wine Stains
Ran X, Yang X, Lin X, Yu W, Shang Y, Liang J, Shen L
Clinical, Cosmetic and Investigational Dermatology 2025, 18:1297-1308
Published Date: 26 May 2025