Back to Journals » Neuropsychiatric Disease and Treatment » Volume 20
The Inter-Relationships Between Depressive Symptoms and Suicidality Among Macau Residents After the “Relatively Static Management” COVID-19 Strategy: A Perspective of Network Analysis
Authors Lam MI ![]() , Cai H, Chen P, Lok KI, Chow IHI, Si TL, Su Z, Ng CH
, Cai H, Chen P, Lok KI, Chow IHI, Si TL, Su Z, Ng CH ![]() , An FR, Xiang YT
, An FR, Xiang YT
Received 21 November 2023
Accepted for publication 19 January 2024
Published 3 February 2024 Volume 2024:20 Pages 195—209
DOI https://doi.org/10.2147/NDT.S451031
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Mei Ieng Lam,1,2 Hong Cai,2,3 Pan Chen,2,3 Ka-In Lok,4 Ines Hang Iao Chow,2 Tong Leong Si,2 Zhaohui Su,5 Chee H Ng,6 Feng-Rong An,7 Yu-Tao Xiang2,3
1Education Department, Kiang Wu Nursing College of Macau, Macau SAR, People’s Republic of China; 2Unit of Psychiatry, Department of Public Health and Medicinal Administration, & Institute of Translational Medicine, University of Macau, Macao SAR, People’s Republic of China; 3Centre for Cognitive and Brain Sciences, University of Macau, Macao SAR, People’s Republic of China; 4Faculty of Health Sciences and Sports, Macao Polytechnic University, Macao, People’s Republic of China; 5School of Public Health, Southeast University, Nanjing, People’s Republic of China; 6Department of Psychiatry, The Melbourne Clinic and St Vincent’s Hospital, University of Melbourne, Richmond, Victoria, Australia; 7Beijing Key Laboratory of Mental Disorders, National Clinical Research Center for Mental Disorders & National Center for Mental Disorders, Beijing Anding Hospital; Advanced Innovation Center for Human Brain Protection, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Chee H Ng, Department of Psychiatry, The Melbourne Clinic and St Vincent’s Hospital, University of Melbourne, Richmond, Victoria, Australia, Email [email protected] Yu-Tao Xiang, Faculty of Health Sciences, University of Macau, 1/F, Building E12, Macau, People’s Republic of China, Email [email protected]
Background: Suicidality is a global public health problem which has increased considerably during the coronavirus disease 2019 (COVID-19) pandemic. This study examined the inter-relationships between depressive symptoms and suicidality using network analysis among Macau residents after the “relatively static management” COVID-19 strategy.
Methods: An assessment of suicidal ideation (SI), suicide plan (SP), suicide attempt (SA) and depressive symptoms was conducted with the use of individual binary response items (yes/no) and Patient Health Questionnaire (PHQ-9). In the network analysis, central and bridge symptoms were identified in the network through “Expected Influence” and “Bridge Expected Influence”, and specific symptoms that were directly associated with suicidality were identified via the flow function. Network Comparison Tests (NCT) were conducted to examine the gender differences in network characteristics.
Results: The study sample included a total of 1008 Macau residents. The prevalence of depressive symptoms and suicidality were 62.50% (95% CI = 59.4– 65.5%) and 8.9% (95% CI = 7.2– 10.9%), respectively. A network analysis of the sample identified SI (“Suicidal ideation”) as the most central symptom, followed by SP (“Suicide plan”) and PHQ4 (“Fatigue”). SI (“Suicidal ideation”) and PHQ6 (“Guilt”) were bridge nodes connecting depressive symptoms and suicidality. A flow network revealed that the strongest connection was between S (“Suicidality”) and PHQ6 (“Guilt”), followed by S (“Suicidality”) and PHQ 7 (“Concentration”), and S (“Suicidality”) and PHQ3 (“Sleep”).
Conclusion: The findings indicated that reduction of specific depressive symptoms and suicidal thoughts may be relevant in decreasing suicidality among adults. Further, suicide assessment and prevention measures should address the central and bridge symptoms identified in this study.
Keywords: COVID-19, depression, suicidality, adults, network analysis
Introduction
Suicidality is a major public health problem globally.1 Every year, more than 700,000 people die by suicide, and it is estimated that one person dies every 40 seconds. The coronavirus disease 2019 (COVID-19) pandemic is one of the major risk factors impacting on suicidality.2–5 Since the start of the COVID-19 pandemic, mental health professionals have been concerned about rising suicide rates, with warnings such as “Suicide epidemic triggered by COVID-19”6 and “Dual pandemic of suicide and COVID-19”.7 A meta-analysis examining suicidality during the COVID-19 pandemic found an increase rate for suicidal ideation (SI) (10.81%), suicide attempts (SA) (4.68%), and self-harm (9.63%) when compared to studies conducted prior to COVID-19 pandemic.8 Another meta-analysis revealed that the prevalence rate of SI among hospitalized and non-hospitalized populations was 1.134 (95% CI: 1.048–1.227) to 1.142 times (95% CI: 1.018–1.282) higher, while the prevalence of SA was also 1.14 times higher (95% CI: 1.053–1.233) to 1.32 (95% CI: 1.17–1.489) than the corresponding figures during the pre-pandemic period.9 Suicide is not only a leading cause of death among the general population,10 but also places a heavy burden on affected families, communities, and societies worldwide.1 Therefore, suicide prevention has become a global imperative especially during the COVID-19 pandemic. Furthermore, the mass lockdowns, social isolation, and economic consequences of the pandemic11–13 might have resulted in an increase of physical and mental (ie, depression), behavioral (ie, panic buying), financial (ie, unemployment) and psychosocial (ie, racism) problems which could contribute to the risk of suicidality.3,8,14 Therefore, understanding the association between mental health problems (eg, depression) and suicidality during the pandemic is essential for developing the relevant public health strategies and guidelines to address these problems.15
The association between suicidality and mental health problems, particularly depression, has been well established. For instance, depressive symptoms were positively associated with suicidality,16,17 and were among the most prominent predictive factors for SI, suicide plan (SP)18 and SA.17 It is estimated that suicide is 25 times more likely to occur in people with depression than in the general population.19 Meanwhile, a significant increase in depressive symptoms was also observed during the COVID-19 pandemic.20 Increased depressive symptoms can be associated with fear of being infected with COVID-19, social distancing, and changing economic conditions.12,21,22 A meta-analysis of 162,639 participants across 17 counties found that the overall prevalence of depressive symptoms was 28% during the COVID-19 pandemic.13 The more intense the lockdown measures, the higher the risk of depression. For instance, a study of 55,589 participants from 40 countries found that with increasing lockdown intensity, the risk of developing depressive symptoms increased by more than 1.7 times.21 The greater the depressive symptoms, the higher the probability of suicidal thoughts and behaviors emerging during the COVID-19 pandemic.3,23,24
The Macau Special Administrative Region of China (Macau SAR), located on the west of the Pearl Delta River estuary in southern China, heavily depends upon international visitors to sustain its social and economic existence. The long-term persistence of COVID-19-related travel restrictions and quarantine prevention policy caused intense economic damage in Macau.25 However, Macau SAR implemented stringent restriction and quarantine policy during the sixth wave of the pandemic in the Region, dubbed “618” wave, which occurred from June 18 to August 7, 2022, and resulted in 705 new confirmed cases (38.7%) and 1116 asymptomatic infections (61.3%). Macau SAR authorized a “relatively static management” for 12 days, closing down public institutions such as schools, casinos, and cinemas26 to control the sources of infection and cut off the channels of transmission. These measures, as well as the “dynamic zero COVID” prevention policy taken by Macau and mainland China, were very successful in reducing the spread of COVID-19.27,28 However, the economy was adversely affected and has not yet recovered to its pre-pandemic levels.29 As a result, there has been an increase rate of psychological problems,30 such as depression and suicidality. For example, previous studies found that the prevalence of depressive symptoms and SI among Macau residents were 38.5% and 13.5%, respectively,31 which were substantially higher than the initial wave of COVID-19 outbreak in UK and Brazil in 2020.32 Moreover, suicide rates increased during the COVID-19 pandemic.33 In 2020, suicide cases (n=69) increased by 23% over 2019 (n=50), while suicide cases in Macau during the first three quarters of 2022 (n=65) were 70% higher than in the same period in 2021.34 During both significant outbreaks of COVID-19 in 2020 and 2022, the overall suicide rates in Macau were 9.8 and 9.67 per 100,000 individuals,34,35 respectively, which was higher than the global suicide rate in 2019 (9.0 per 100,000 people).36 Thus, it is imperative to investigate the inter-relationships between suicidality and depression after the “relatively static management” COVID-19 strategy in Macau.
Network analysis (NA) offers a novel perspective for investigating psychiatric problems conceptualized as a causal interplay between symptom systems.37 In network theory, the symptoms as variables are represented by nodes, the connection between the nodes are represented by edges,38 and the central node is the most influential symptom with a large number of connection in a network which is linked to other symptoms.38,39 NA provides a perspective into how symptoms of a syndrome interact with each other and can help identify which symptoms are most influential or central to a syndrome, which can be prioritized for intervention.40
Although NA was widely applied to various psychiatric disorders among numerous subgroups of the population during the COVID-19 pandemic,31,41,42 there is a lack of research on the specific interrelationship between depressive symptoms and suicidality in the general population. For instance, prior network analyses focused on depressive symptoms among Hong Kong residents43 and mental health symptoms and suicidality among young adults aged 10–35 years during the COVID-19 pandemic.44 Another network analysis study examined psychiatric symptoms (eg, anxiety and depression) and suicidality among adolescents in Macau45 and college students in China.46 Most studies also focused on young populations, as suicide is a leading cause of death in this subpopulation.1 To date, no studies have examined the specific correlates of suicidality among Macau adult residents, particularly during the pandemic, despite the upward trend of suicide in this population. Understanding the relationship between depressive symptoms and suicidality is crucial to reducing suicide risks. Hence, this study examined the inter-relationships between depressive symptoms and suicidality using network analysis among Macau adult residents after the “relatively static management” COVID-19 strategy.
Methods
Participants and Procedure
This was a cross-sectional study using snowball sampling method conducted from July 26 to September 9, 2022, during which Macau SAR government implemented the “relatively static management” of the sixth wave of the pandemic. Face-to-face interviews were not possible during the COVID-19 outbreaks due to lockdowns and social distancing. Following previous studies,31,47,48 participants were invited to participate in this survey on an anonymous and voluntary basis through a Quick Response code (QR code) that was linked to an invitation and assessment instruments on key social network platforms’ advertisements such as WeChat, Instagram, and Facebook. To be eligible, participants were (1) local residents who lived in Macau during the 618 COVID-19 wave and experienced the “relatively static management” COVID-19 strategy; (2) aged 18 years or above; (3) able to understand the purpose and content of the survey. The study was approved by the Institutional Review Board of the University of Macau (Ethnics approval number: SSHRE22-APP05-FHS) which adhered to the principles of the Declaration of Helsinki. Participants are provided electronic written informed consent.
Measures
Basic socio-demographic data were collected, including age, gender, marital status, living situation, education level, and employment status. A number of variables related to COVID-19 were also recorded, including concern about COVID-19, quarantine status during the COVID-19 pandemic, fear of infection, economic loss caused by the pandemic, monthly income, regular physical activity, chronic physical illness, and psychiatric disorders during the outbreak.
The validated Chinese version of the self-report Patient Health Questionnaire (PHQ-9) was used to measure depression.49,50 The PHQ-9 consists of nine items referring to the past two weeks which is based on the Diagnostic and Statistical Manual of Disorders-IV (DSM-IV) criteria for depression,50 with each item scoring between 0 (“not at all”) and 3 (“nearly every day”); the PHQ-9 total score ranges from 0 to 27, with a higher total score indicating more depressive symptoms.51 The PHQ-9 items include: anhedonia (PHQ1), sad mood (PHQ2), sleep (PHQ3), fatigue (PHQ4), appetite (PHQ5), guilt (PHQ6), concentration (PHQ7), motor disturbance (PHQ8), and suicidal ideation (PHQ9).52
In this study, suicidality in the past week consists of SI, suicide plan (SP), and SA.53,54 SI refers to having thoughts or wishes about ending one’s own life but not making plans for death;53,55 SP refers to preparing to use a specific method to end one’s own life;56 SA is defined by the act of self-injury to end one’s own life.53,55 Following previous studies,45,57 the item on Suicidal ideation (PHQ9) was excluded from the network analysis as it was duplicating the suicidal ideation (SI) component of suicidality. Standard questions on suicidality with (yes/no) responses were used as recommended in previous studies;45,58,59 the SI was evaluated with the question, “During the ‘618 COVID-19 outbreak’, have you had thoughts that you would be better off dead?”. SP was assessed with the question, “During the ‘618 COVID-19 outbreak’, have you made a plan for suicide?” while SA was measured with the question, “During the ‘618 COVID-19 outbreak’, have you attempted suicide?”. A participant was defined as “having suicidality” if he or she answered “yes” to any of the three questions. For those in need of mental health services, information regarding mental health resources (eg, contact information for helplines and hotline services) was provided at the end of the survey.
Data Analysis
Network Estimation
For statistical analyses, R software60 was used to conduct the network analysis. In the network model, each node is represented as an individual symptom; each edge is regarded as the association between two nodes. Stronger correlations were represented by thicker edges, while a positive correlation was indicated with a green edge and a negative correlation with a red edge.61 To assess the polychoric correlations between all survey items in the network model, a Graphical Gaussian Model (GGM) with graphic least absolute shrinkage and selection operator (LASSO) and an Extended Bayesian Information Criterion (EBIC) model were adopted,62 which could enhance prediction accuracy, interpretability and optimality of the network model.63 Due to the skewed distribution of mean scores on study items, non-parametric correlations were computed using nonparanormal transformations.64 An evaluation of network estimation was performed using the “estimateNetwork” function in R packages “bootnet” with “EBICglasso” as the default method.62 A network visualization was conducted using the R packages’ qgraph’62 and “ggplot2” was used to optimize its visual representation.62,65
Centrality and Stability
The network structure’s expected influence (EI) was calculated using the R package qgraph61 to evaluate the importance of each node in the network model. Compared with traditional centrality indices such as node strength, EI is particularly suitable for networks that could distinguish between positive and negative edges.66 In the network model, the nodes with a greater EI were deemed more important and influential.31 To identify bridge symptoms in the network model that associate with two or more psychiatric syndromes,67 the “bridge” function of the R package “networktools” (version 1.5.0) was used to calculate the bridge expected influence.68 Compared to bridge symptoms with lower expected influence values, those with higher expected influence values were associated with a higher risk of contagion between different communities of symptoms.69 Predictability of each node70 and control of confounding effects in basic demographic data71,72 in the network model were estimated using the R package “mgm”. The value of predictability is indicated as the linkage between its neighboring node.31 Moreover, the “flow” function in the R package “qgraph” was used to examine particular depressive symptoms that were directly related to suicidality.61
In addition, the stability and accuracy of network model were assessed using the “bootnet” function in R package (Version 1.4.3)62 with 1000 permutations of case dropping bootstrap procedure for each node. A correlation stability coefficient (CS-coefficient) was used to assess the network’s stability. A correlation greater than 0.7 indicated that a maximum proportion of cases could be dropped, representing a 95% probability that original centrality indices correlate with the centrality of subset networks.62 Following previous studies,31,45,62 a CS-coefficient value of above 0.25 was regarded as stable in the network model, while a value of above 0.5 was regarded as preferable stable A non-parametric bootstrapped difference test was performed to assess the difference between pairs of nodes and edges. The difference between two nodes or edges was significant if zero was excluded from the 1000-bootstrap 95% confidence interval (CI). Bootstrapped 95% CI was used to estimate edge accuracy, with a narrower CI representing a more trustworthy network.62
Network Comparison Test
As recommended previously,45 to test the differences in depression and suicidality network models between genders, an analysis of gender differences in network structure and global strength was performed using Network Comparison Test (NCT), with “NetworkComparisonTest” in R package (Version 2.2.1)73 with 1000 permutations.
Results
Study Sample
In total, 1020 Macau residents were invited to participate in the study, and 1008 met the inclusion criteria and completed the assessment, representing a participation rate of 98.82%. The mean age of participants was 38.4 years (standard deviation (SD)=11.5 years) and 26.7% of participants (n=269) were male. The prevalence rates of depression (PHQ-9 ≥ 5) and overall suicidality during the 618 COVID-19 wave were 62.5% (95% CI = 59.4–65.5%) and 8.9% (95% CI = 7.2–10.9%), respectively, while the rates of SI, SP, and SA were 8.4% (95% CI = 6.8–10.3%), 3.5% (95% CI = 2.4–4.8%), and 3.3% (95% CI = 2.3–4.6%), respectively. The PHQ and suicidality assessments are presented in Supplementary Table S1, which shows means, standard deviations, skewness, and kurtosis.
Network Structure and Centrality measures Analysis
Figure 1 presents the network structure of depression and suicidality among Macau residents after the “relatively static management” COVID-19 strategy conducted by EBICglasso model. The mean predictability in this sample was 0.511, representing on average 51.1% of each node’s variance that could be explained by its neighboring nodes. In the network model, the connection with the strongest positive edge was SP (“Suicide plan”) - SA (“Suicide attempt”), followed by PHQ7 (“Concentration”) - PHQ8 (“Motor disturbance”), and PHQ1 (“Anhedonia”) - PHQ4 (“Fatigue”). The correlation between PHQ item and suicidality are shown in Supplementary Table S2. Additionally, the flow network of suicidality with PHQ items is presented in Figure 2. The S (“Suicidality”) - PHQ 6 (“Guilt”) was the strongest edge, followed by S (“Suicidality”) – PHQ7 (Concentration), and S (“Suicidality”)-PHQ3 (“Sleep”).
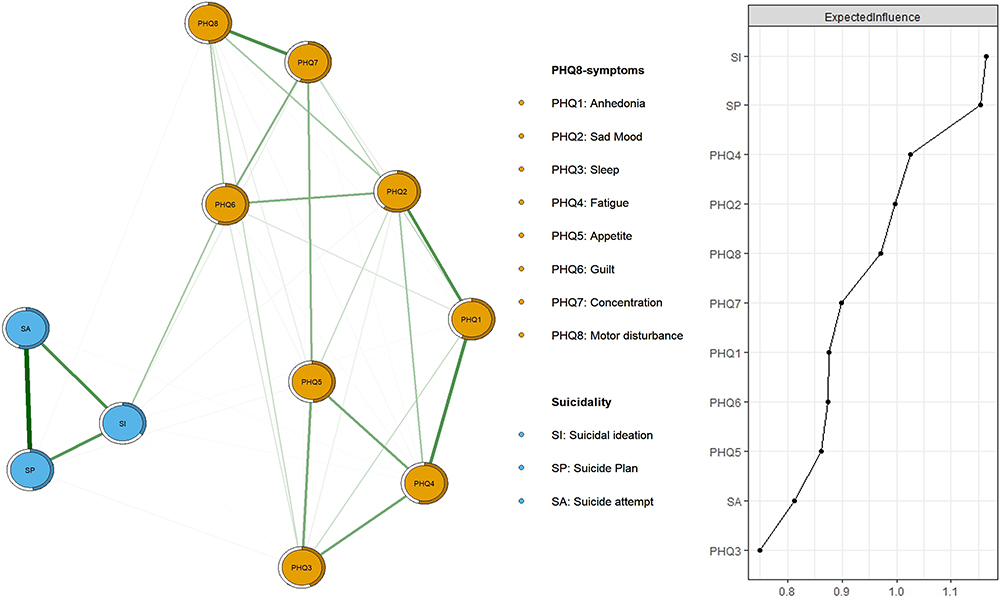 |
Figure 1 The network structure of depressive symptoms and suicidality among Macau residents shortly after the “relatively static management” COVID-19 strategy. |
 |
Figure 2 Flow network of suicidality. |
In terms of network centrality measured by EI, the three nodes with the highest EI centrality were SI (“Suicidal ideation”), SP (“Suicide plan”) and PHQ4 (“Fatigue”), whereas PHQ 3 (“Sleep”), SA (“Suicide attempt”), and PHQ5 (“Appetite”) had the lowest EI centrality (Figure 1). As shown in Figure 3, the two key bridge symptoms examined by bridge EIs linking PHQ-8 and suicidality communities were SI (“Suicidal ideation”) and PHQ6 (“Guilt”).
 |
Figure 3 The network structure of depressive symptoms and suicidality with bridge connections among Macau residents shortly after the “relatively static management” COVID-19 strategy. |
Figure 4 illustrates the assessment of network stability; the network structure is stable with a CS-coefficient of EI of 0.361, which indicates that 36% of the sample can be dropped without significantly affecting the network structure. In terms of the accuracy of the network, bootstrap 95% CIs for estimated edge weights revealed a narrow range, as shown in Supplementary Figure S1A. As most of the edge weights were non-zero, the majority of the edges were considered accurate and stable. Additionally, most comparisons of edge weights were statistically significant according to bootstrapped difference tests as presented in Supplementary Figure S1B, suggesting that the network model was reliable.
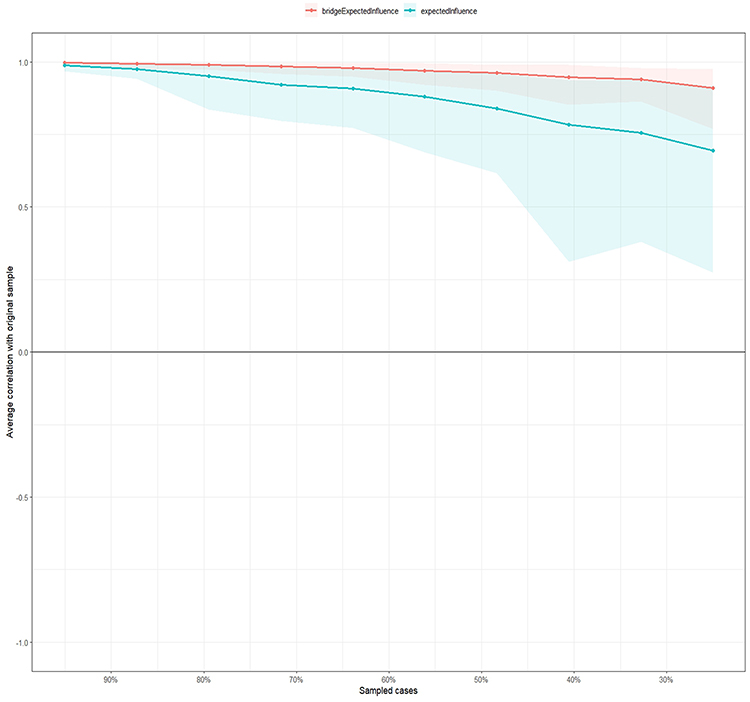 |
Figure 4 The stability of centrality and bridge centrality indices using case-dropping bootstrap. |
The Confounding Effects of Basic Demographic Data on Depressive Symptoms and Suicidality
Demographic factors such as gender, age, marital status, and level of education were found to be significantly associated with depressive symptoms and suicidality in previous studies.74–77 Marriage, for instance, was both a risk and protective factor of depression in different studies.75,78 Lower education and females were associated with higher risk of depression,78 while women were also more likely to have suicidal behaviors.79 It is likely that lower level of education could adversely affect depression through interfering with cognitive development,80 while the lower social position for women in some areas78 could also increase the risk of depression. Previous research has found that age might serve as a mediator between certain mental problems (eg, anorexia and bulimia nervosa) and SA.81 Moreover, age showed a negative relationship with emotional distress, which could be attributed to higher levels of optimism and external control among older adults.82 A study found that during the COVID-19 pandemic, age was negatively associated with suicidal thoughts among residents in Mexico83 and China.84 In contrast, another study found that male gender was a risk factor for suicidal thoughts among the general population.83 Therefore, to examine the inter-relationship between depressive symptoms and suicidality, it is important to minimize the confounding effects caused by basic demographic variables. Following previous research,72,85,86 the depressive symptoms and suicidality network models, with the structure indexes, were re-evaluated after controlling for age, marital status, gender, and education level (Supplemental Figure S2). Compared to the original network, the re-calculated network model did not find any significant structure change after controlling for the confounding variables (strength: rs = 0.77 [0.54; 0.95]).
Gender Differences in Network Models
The comparison of gender differences in network models did not find significant differences in network edge weight (M=0.21, P=0.488), or global strength (network strength: 4.94 in female participants; 5.05 in male participants; S=0.11, P=0.459) (see Supplementary Figures S3–S5).
Discussion
To the best of our knowledge, this was the first study to explore prevalence of depressive symptoms and suicidality and their inter-relationships using network analysis among Macau residents after the “relatively static management” COVID-19 strategy. Both depressive symptoms and suicidality were common. Network analysis revealed that SI (“Suicidal ideation”) was the most central symptom with the highest centrality, followed by SP (“Suicide plan”) and PHQ4 (“Fatigue”). In addition, SI (“Suicidal ideation”) and PHQ6 (“Guilt”) served as bridge nodes linking depressive symptoms with suicidality. Finally, as shown in the Flow network, the strongest connection was between nodes S (“Suicidality”) and PHQ 6 (“Guilt”), followed by edges between S (“Suicidality”) and PHQ 7 (“Concentration”) and S (“Suicidality”) and PHQ3 (“Sleep”).
SI and SP were the most influential in our sample network which is aligned with previous adults’ COVID-19 network analysis.87 SI was also identified as the bridge symptom. A global survey across 17 countries on the general population found that the lifetime prevalence of SI was 9.2%, while the corresponding prevalence rates of SP and SA were 3.1% and 2.7%, respectively.88 SI is a robust predictor of SP and SA16,89 as 60% of those with SI could transition to SP and SA within 12 months,88 and with an increase of one unit in the severity of SI, the rate of SA occurrence could increase by 4.4 times.90 SI and SP also trigger depressive symptoms as bridge symptoms in the network. In accordance with the differential activation theory of suicidality, depression and suicidality could easily be activated by each other because of the configuration formation between SI and depression during early episodes of depression.91–93 In particular, depression recurrence was significantly related to previous episodes of SI91 and suicidal symptoms94 in longitudinal studies of major depression patients, in which more suicidal symptoms were associated with more significant depressive symptoms.94,95 Similarly, a machine learning study found that suicidality was the top predictor of persistent and recurrent depression over three years.96 In tandem with those studies, our findings suggest that SI and SP have prominent roles in linking depression and suicidality during the COVID-19 pandemic. Despite the importance of SI and SP, there are still insufficient diagnostic criteria for suicidal ideation and inadequate understanding of passive suicidal behavior.94 Passive suicidal thoughts was highly related to SA and suicide in a previous study.97 Meanwhile, the risk factors and assessment of SP are still unclear.98 Furthermore, most of the treatments that target depression failed to reduce suicidal thoughts and behavior adequately,99 whereas an earlier meta-analysis reported that prior SI was the strongest predictor of future suicidal thoughts and behaviors.98,100 Thus, instead of focusing on specific treatment of depressive symptoms, early screening and treatment may need to target central symptoms such as SI and SP in suicide prevention.
“Fatigue” was another prominent central symptom in this network analysis, which is in accordance with previous findings from a depression network among adults and older adults during the COVID-19 outbreak43,101,102 as well as the network analysis of depression and suicidality among adolescents.103 The term “Fatigue” refers to a lack of energy, or often referred to as fatigue104,105 or exhaustion.106 Fatigue is a crucial influencer of other depressive symptoms, such as anhedonia,107,108 hopelessness, and impaired concentration,109 as well as a contributor to the development of psychiatric disorders (ie, depression and psychotic disorders).107,108 In addition, fatigue was regarded as a key symptom to influence suicidality in this study. These results also support previous findings that found that greater severity of fatigue could result in a higher risk of suicidality,59,110 cognitive and functional impairment.110 On the other hand, the COVID-19 pandemic in itself is a significant risk factor for fatigue that is related to infection19,111 and restriction of outdoor activities caused by lockdowns.112 Likewise, persistent fatigue, which is a somatic symptom of depression,108 is highly prevalent in long COVID,19,113–115 with prevalence rates of 42.5% according to a meta-analysis study,116 which may contribute to the risk of suicidal thoughts and behaviors.115 This may be due to inflammatory impairment of the brain19 leading to dysregulation of neurotransmitters3 or cognitive damage.115 Despite the importance of fatigue in depression and suicidality, fatigue as a screening symptom for depression was considered to be less sensitive than other depressive symptoms, such as anhedonia.104 Hence, loss of energy should be further addressed in screening and preventive measures for suicidality and depression.
“Guilt” was identified as a bridge symptom in this network model, which is consistent with another study on depression and anxiety of adolescents during the later stages of the COVID-19 pandemic in China. People often experience strong guilt feelings during the COVID-19 pandemic associated with the emergence of anger and blaming towards others (ie, doctors, neighbors, and health authorities),117 financial loss/worries111,118 or through witnessing infection or death.119 In relation to guilt, people often experience worthlessness105 and negative evaluation or self-blame due to their behavior,120 which could lead to the development of depressive symptoms. Guilt, or negative self-reflection, can be triggered by depression.121 A previous study of general adult population found that guilt was strongly linked with depression.122 Negative self-evaluation due to guilt often leads to painful, overwhelming emotions, while the perception of self-worthlessness can induce suicidality.123 Moreover, ‘Guilt’ was the most robust flow connection to suicidality in this network analysis which is consistent with previous studies. For instance, an earlier study reported that feeling worthless due to a traumatic experience was the most significant factor related to SA among 20 depression symptoms in patients with major depressive disorder (MDD).124 Similarly, guilt was also found to have a significant association with SI among adults who attended mental health services.125 In addition, the depression network101 reported that guilt was strongly linked with SI among Wuhan residents during the COVID-19 pandemic in China.
“Concentration“ and ”Sleep” were the other strong connection to suicidality, which is in line with previous suicidality and depression network analysis among a community population in Korea.109 People with depression tend to experience decreased ability to think or make decisions.105 An earlier study demonstrated that psychosocial dysfunction was predominantly influenced by poor concentration in patients with depression (ie, inability to manage work, household, and relationships, and impairment of social and private activities).126 Further, impairment of psychosocial function is a risk factor for suicidality as well (Franklin et al, 2017). On the other hand, ‘sleep’ refers to insomnia or hypersomnia.105 Insomnia was highly prevalent during the COVID-19 pandemic (Bai et al, 2022b; Li et al, 2020; Morin et al, 2021) associated with COVID-19-related stress, social distancing, and economic burden.127,128 Sleep dysfunction such as insomnia was strongly associated with suicidality17 and found to be a significant predictor of SI129 and SA.130 In particular, a meta-analysis of longitudinal studies determined that insomnia had the most substantial connection with SI among those with sleep disturbances.131 Greater levels of insomnia was associated with greater SI intensity,129 SI maintenance,131 and SA occurrence.130 A decrease in serotonin, which is an essential neurotransmitter in the central nervous system that regulates sleep and impulse control,132,133 may explain the association between sleep problems and suicidality among depression patients. Apart from the biological mechanisms of sleep and suicidality, dysfunctional cognition and attitudes about sleep may also contribute to insomnia and suicidal thoughts.134 Moreover, concern about current sleeping patterns was the central symptom of depression and insomnia network among the Korean general population during the COVID 19 pandemic.135
In this study, “SI”, “SP” and “Fatigue” were identified as central symptoms in the depression and suicidality network mode, which are the most influential symptoms that could be targeted in treatment.40 Thus, early screening and treatment that target SI and SP, as well as those that address lack of energy, should be prioritized for Macau residents in need. Additionally, “Guilt” was identified as a bridge node with the strongest connection to suicidality in this study; therefore, future research should also target feelings of guilt. Mindfulness-based cognitive therapy, in which depressed patients cultivate a non-judgmental attitude to reduce rumination from negative thinking, could significantly reduce depression and SI.136 Further, we found that insomnia was also associated with suicidality. Cognitive Behavioral Therapy for Insomnia (CBT-I) is an effective intervention for both insomnia and suicidality, which aims to change sleep maladaptive beliefs and attitudes and dysfunctional sleep cognition.137 However, most of studies on the association between sleep and suicidality were based on cross-sectional study design, and therefore, causality between them could not be examined.131,138 Further prospective studies are needed.
The merits of this study included its large sample size and advanced network analysis identifying links between depressive symptoms and suicidality. However, the main limitations should be acknowledged. First, this was a non-experimental, cross-sectional study; hence, causal relationships between suicidality and depressive symptoms could not be determined. It is necessary to conduct future intervention research and longitudinal studies in order to analyze the possible causal relationships and dynamic changes between suicidality and symptoms of depression in adults over time. Second, this study was conducted in the Macau SAR, so the results may not be applicable to other regions because COVID-19 policies and trajectories differ from region to region. Third, due to the risk of COVID-19 infection, snowball sampling via an online survey might have resulted in selection biases which decreased the representativeness of the population. Lastly, biases in recall and social desirability could not be controlled due to the use of self-report assessment in the study.
In conclusion, central symptoms (eg, “Suicidal ideation”, “Suicide plan”, “Fatigue”) and key bridge symptoms (eg, “Suicidal ideation” and “Guilt”) identified in this study might serve as crucial targets in the screening, prevention and treatment for adults with depression and suicidality during the pandemic. Future research should prioritize improving assessment and intervention based on central and bridge symptoms for those in need.
Data Sharing Statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors. Requests to access the datasets should be directed to [email protected].
Ethics Approval and Consent to Participate
The study was approved by the Institutional Review Board of the University of Macau (Ethics approval number: SSHRE22-APP05-FHS) which adhered to the principles of the Declaration of Helsinki. Participants are provided electronic written informed consent.
Acknowledgments
The authors are grateful to all participants and clinicians involved in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Suicide. Available from: https://www.who.int/news-room/fact-sheets/detail/suicide.
2. Fitzpatrick KM, Harris C, Drawve G. How bad is it? Suicidality in the middle of the COVID-19 pandemic. Suicide Life Threat Behav. 2020;50(6):1241–1249. doi:10.1111/sltb.12655
3. Efstathiou V, Stefanou MI, Siafakas N, et al. Suicidality and COVID-19: suicidal ideation, suicidal behaviors and completed suicides amidst the COVID-19 pandemic (Review). Exp Ther Med. 2022;23(1):107. doi:10.3892/etm.2021.11030
4. Shoib S, Gaitan Buitrago JET, Shuja KH, et al. Suicidal behavior sociocultural factors in developing countries during COVID-19. Encephale. 2022;48(1):78–82. doi:10.1016/j.encep.2021.06.011
5. Reger MA, Stanley IH, Joiner TE. Suicide mortality and coronavirus disease 2019-A perfect storm? JAMA Psychiatry. 2020;77(11):1093–1094. doi:10.1001/jamapsychiatry.2020.1060
6. Mannix R, Lee LK, Fleegler EW. Coronavirus Disease 2019 (COVID-19) and firearms in the United States: will an epidemic of suicide follow? Ann Internal Med. 2020;173(3):228–229. doi:10.7326/M20-1678
7. Banerjee D, Kosagisharaf JR, Sathyanarayana Rao TS. ‘The dual pandemic’ of suicide and COVID-19: a biopsychosocial narrative of risks and prevention. Psychiatry Res. 2021;295:113577. doi:10.1016/j.psychres.2020.113577
8. Dube JP, Smith MM, Sherry SB, Hewitt PL, Stewart SH. Suicide behaviors during the COVID-19 pandemic: a meta-analysis of 54 studies. Psychiatry Res. 2021;301:113998. doi:10.1016/j.psychres.2021.113998
9. Yan Y, Hou J, Li Q, Yu NX. Suicide before and during the COVID-19 pandemic: a systematic review with meta-analysis. Int J Environ Res Public Health. 2023;20(4):3346. doi:10.3390/ijerph20043346
10. Centers for Disease Control and Prevention. Leading Causes of Death Reports, 1981 - 2020. Available from: https://wisqars.cdc.gov/fatal-leading.
11. Byrne A, Barber R, Lim CH. Impact of the COVID‐19 pandemic – a mental health service perspective. Prog Neurol Psychiatry. 2021;25:2.
12. Killgore WDS, Cloonan SA, Taylor EC, Allbright MC, Dailey NS. Trends in suicidal ideation over the first three months of COVID-19 lockdowns. Psychiatry Res. 2020;293:113390. doi:10.1016/j.psychres.2020.113390
13. Luo M, Guo L, Yu M, Jiang W, Wang H. The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public - A systematic review and meta-analysis. Psychiatry Res. 2020;291:113190. doi:10.1016/j.psychres.2020.113190
14. Moutier C. Suicide Prevention in the COVID-19 Era: transforming Threat Into Opportunity. JAMA Psychiatry. 2020. doi:10.1001/jamapsychiatry.2020:3746
15. Taylor S. The Psychology of Pandemics. Annu Rev Clin Psychol. 2022;18(1):581–609. doi:10.1146/annurev-clinpsy-072720-020131
16. Kim BJ, Kihl T. Suicidal ideation associated with depression and social support: a survey-based analysis of older adults in South Korea. BMC Psychiatry. 2021;21(1):409. doi:10.1186/s12888-021-03423-8
17. Wiebenga JXM, Dickhoff J, Merelle SYM, et al. Prevalence, course, and determinants of suicide ideation and attempts in patients with a depressive and/or anxiety disorder: a review of NESDA findings. J Affect Disord. 2021;283:267–277. doi:10.1016/j.jad.2021.01.053
18. Burke TA, Jacobucci R, Ammerman BA, et al. Identifying the relative importance of non-suicidal self-injury features in classifying suicidal ideation, plans, and behavior using exploratory data mining. Psychiatry Res. 2018;262:175–183. doi:10.1016/j.psychres.2018.01.045
19. Sher L. Post-COVID syndrome and suicide risk. QJM. 2021;114(2):95–98. doi:10.1093/qjmed/hcab007
20. Deng J, Zhou F, Hou W, et al. The prevalence of depression, anxiety, and sleep disturbances in COVID-19 patients: a meta-analysis. Ann N Y Acad Sci. 2021;1486(1):90–111. doi:10.1111/nyas.14506
21. Fountoulakis KN, Karakatsoulis G, Abraham S, et al. Results of the COVID-19 mental health international for the general population (COMET-G) study. Eur Neuropsychopharmacol. 2022;54:21–40. doi:10.1016/j.euroneuro.2021.10.004
22. Fountoulakis KN, Apostolidou MK, Atsiova MB, et al. Self-reported changes in anxiety, depression and suicidality during the COVID-19 lockdown in Greece. J Affect Disord. 2021;279:624–629. doi:10.1016/j.jad.2020.10.061
23. Efstathiou V, Papadopoulou A, Pomini V, et al. A one-year longitudinal study on suicidal ideation, depression and anxiety during the COVID-19 pandemic. Asian J Psychiatr. 2022;73:103175. doi:10.1016/j.ajp.2022.103175
24. Panfil AL, Lungeanu D, Tamasan S, et al. Suicidality related to the COVID-19 lockdown in Romania: structural equation modeling. Front Psychiatry. 2022;13:818712. doi:10.3389/fpsyt.2022.818712
25. McCartney G, Pinto J, Liu M. City resilience and recovery from COVID-19: the case of Macao. Cities. 2021;112:103130. doi:10.1016/j.cities.2021.103130
26. Government Portal of Macau Special Administrative Region of China . Report on the Macao SAR government’s response to the ”618” pandemic. Avaiable from: https://www.gcs.gov.mo/detail/pt/N22GIkjA4P.
27. Liu J, Liu M, Liang W. The Dynamic COVID-Zero Strategy in China. China CDC Wkly. 2022;4(4):74–75. doi:10.46234/ccdcw2022.015
28. Zhao YJ, Xu JQ, Bai W, et al. COVID-19 prevention and control strategies: learning from the Macau model. Int J Biol Sci. 2022;18(14):5317–5328. doi:10.7150/ijbs.70177
29. Government of the Macao Special Administrative Region. Report of Macao gross domestic product (in Chinese). Statistics and Census Bureau of the government of the Macao special administrative region. Available from: https://www.dsec.gov.mo/zh-MO/Statistic?id=901.
30. Bai W, Sha S, Cheung T, Su Z, Jackson T, Xiang YT. Optimizing the dynamic zero-COVID policy in China. Int J Biol Sci. 2022;18(14):5314–5316. doi:10.7150/ijbs.75699
31. Bai W, Zhao YJ, Cai H, et al. Network analysis of depression, anxiety, insomnia and quality of life among Macau residents during the COVID-19 pandemic. J Affect Disord. 2022;311:181–188. doi:10.1016/j.jad.2022.05.061
32. Cheung T, Lam SC, Lee PH, Xiang YT, Yip PSF. International research collaboration on C. Global imperative of suicidal ideation in 10 countries amid the COVID-19 pandemic. Front Psychiatry. 2020;11:588781. doi:10.3389/fpsyt.2020.588781
33. LUSA. Suicide cases increase, citizens advised to seek help. Macau News Agency. Available from: https://www.macaubusiness.com/suicide-cases-increase-citizens-advised-to-seek-help/.
34. Government of Macau Special Administrative Region of China Health Bureau. Monitoring results in suicide death. Available from: https://www.ssm.gov.mo/apps1/InjureRegPrevent/ch.aspx#clg5055.
35. Government of Macao Special Adninstrative Region Statistic and Censue Service. Demographic Statistics. Available from: https://www.dsec.gov.mo/ts/#!/step2/KeyIndicator/zh-MO/240.
36. World Health Organization. Suicide worldwide in 2019: global health estimates. Global epidemiology of suicide; 2021:4.
37. Borsboom D, Cramer AO. Network analysis: an integrative approach to the structure of psychopathology. Annu Rev Clin Psychol. 2013;9:91–121. doi:10.1146/annurev-clinpsy-050212-185608
38. Hevey D. Network analysis: a brief overview and tutorial. Health Psychol Behav Med. 2018;6(1):301–328. doi:10.1080/21642850.2018.1521283
39. Fried EI, Epskamp S, Nesse RM, Tuerlinckx F, Borsboom D. What are ‘good’ depression symptoms? Comparing the centrality of DSM and non-DSM symptoms of depression in a network analysis. J Affect Disord. 2016;189:314–320. doi:10.1016/j.jad.2015.09.005
40. Borsboom D. A network theory of mental disorders. World Psychiatry. 2017;16(1):5–13. doi:10.1002/wps.20375
41. Cai H, Bai W, Liu H, et al. Network analysis of depressive and anxiety symptoms in adolescents during the later stage of the COVID-19 pandemic. Transl Psychiatry. 2022;12(1):98. doi:10.1038/s41398-022-01838-9
42. Liu J, Hao J, Sun Y, Shi Z. Network analysis of population flow among major cities and its influence on COVID-19 transmission in China. Cities. 2021;112:103138. doi:10.1016/j.cities.2021.103138
43. Cheung T, Jin Y, Lam S, et al. Network analysis of depressive symptoms in Hong Kong residents during the COVID-19 pandemic. Transl Psychiatry. 2021;11(1):460. doi:10.1038/s41398-021-01543-z
44. Junus A, Yip PSF. Preventing comorbidity between distress and suicidality: a network analysis. Npj Mental Health Res. 2023;2(1):2. doi:10.1038/s44184-023-00022-1
45. Cai H, Chow IHI, Lei S-M, et al. Inter-relationships of depressive and anxiety symptoms with suicidality among adolescents: a network perspective. J Affective Disorders. 2022. doi:10.1016/j.jad.2022.12.093
46. Yang T, He Y, Wu L, et al. The relationships between anxiety and suicidal ideation and between depression and suicidal ideation among Chinese college students: a network analysis. Heliyon. 2023;9(10):e20938. doi:10.1016/j.heliyon.2023.e20938
47. Cai H, Bai W, Sha S, et al. Identification of central symptoms in Internet addictions and depression among adolescents in Macau: a network analysis. J Affect Disord. 2022;302:415–423. doi:10.1016/j.jad.2022.01.068
48. Liu C, Liu D, Huang N, et al. The combined impact of gender and age on post-traumatic stress symptoms, depression, and insomnia during COVID-19 outbreak in China. Front Public Health. 2020;8:620023. doi:10.3389/fpubh.2020.620023
49. Chen S, Fang Y, Chiu H, Fan H, Jin T, Conwell Y. Validation of the nine-item Patient Health Questionnaire to screen for major depression in a Chinese primary care population. Asia Pac Psychiatry. 2013;5(2):61–68. doi:10.1111/appy.12063
50. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
51. Wang W, Bian Q, Zhao Y, et al. Reliability and validity of the Chinese version of the Patient Health Questionnaire (PHQ-9) in the general population. Gen Hosp Psychiatry. 2014;36(5):539–544. doi:10.1016/j.genhosppsych.2014.05.021
52. Williams N. PHQ-9. Occup Med. 2014;64(2):139–140. doi:10.1093/occmed/kqt154
53. Posner K, Oquendo MA, Gould M, Stanley B, Davies M. Columbia classification algorithm of suicide assessment (C-CASA): classification of suicidal events in the FDA’s pediatric suicidal risk analysis of antidepressants. Am J Psychiatry. 2007;164(7):1035–1043. doi:10.1176/appi.ajp.164.7.1035
54. Cai H, Xie XM, Zhang Q, et al. Prevalence of suicidality in major depressive disorder: a systematic review and meta-analysis of comparative studies. Front Psychiatry. 2021;12:690130. doi:10.3389/fpsyt.2021.690130
55. Turecki G, Brent DA. Suicide and suicidal behaviour. Lancet. 2016;387(10024):1227–1239. doi:10.1016/S0140-6736(15)00234-2
56. Nock MK, Borges G, Bromet EJ, Cha CB, Kessler RC, Lee S. Suicide and suicidal behavior. Epidemiol Rev. 2008;30(1):133–154. doi:10.1093/epirev/mxn002
57. Price M, Legrand AC, Brier ZMF, Hebert-Dufresne L. The symptoms at the center: examining the comorbidity of posttraumatic stress disorder, generalized anxiety disorder, and depression with network analysis. J Psychiatr Res. 2019;109:52–58. doi:10.1016/j.jpsychires.2018.11.016
58. Li H, Luo X, Ke X, et al. Major depressive disorder and suicide risk among adult outpatients at several general hospitals in a Chinese Han population. PLoS One. 2017;12(10):e0186143. doi:10.1371/journal.pone.0186143
59. Zhang L, Cai H, Bai W, et al. Prevalence of suicidality in clinically stable patients with major depressive disorder during the COVID-19 pandemic. J Affect Disord. 2022;307:142–148. doi:10.1016/j.jad.2022.03.042
60. R Core Team. R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing; 2020.
61. Epskamp S, Cramer AOJ, Waldorp LJ, Schmittmann VD, Borsboom D. qgraph: network visualizations of relationships in psychometric data. Journal of Statistical Software. 2012;48(4):1–18. doi:10.18637/jss.v048.i04
62. Epskamp S, Borsboom D, Fried EI. Estimating psychological networks and their accuracy: a tutorial paper. Behav Res Methods. 2018;50(1):195–212. doi:10.3758/s13428-017-0862-1
63. Yang Y, Zhang DY, Li YL, et al. Prevalence, correlates, and network analysis of Internet addiction symptoms among Chinese pregnant and postpartum women. J Affect Disord. 2022;298(Pt A):126–133. doi:10.1016/j.jad.2021.10.092
64. Liu H, Han F, Yuan M, Lafferty J, Wasserman L. High-dimensional semiparametric Gaussian copula graphical models. Ann Stat. 2012;40(4). doi:10.1214/12-AOS1037
65. Villanueva RAM, Chen ZJ, ggplot2: elegant Graphics for Data Analysis. Measurement. 2019;173:160–167. doi:10.1080/15366367.2019.1565254
66. Robinaugh DJ, Millner AJ, McNally RJ. Identifying highly influential nodes in the complicated grief network. J Abnorm Psychol. 2016;125(6):747–757. doi:10.1037/abn0000181
67. Cramer AO, Waldorp LJ, van der Maas HL, Borsboom D. Comorbidity: a network perspective. Behav Brain Sci. 2010;33(2–3):137–150. doi:10.1017/S0140525X09991567
68. Payton J. Tools for Identifying Important Nodes in Networks. Available from: https://cran.r-project.org/web/packages/networktools/index.html.
69. Jones PJ, Ma R, McNally RJ. Bridge centrality: a network approach to understanding comorbidity. Multivariate Behav Res. 2021;56(2):353–367. doi:10.1080/00273171.2019.1614898
70. Haslbeck JMB, Waldorp LJ. How well do network models predict observations? On the importance of predictability in network models. Behav Res Methods. 2018;50(2):853–861. doi:10.3758/s13428-017-0910-x
71. Armour C, Fried EI, Deserno MK, Tsai J, Pietrzak RH. A network analysis of DSM-5 posttraumatic stress disorder symptoms and correlates in U.S. military veterans. J Anxiety Disord. 2017;45:49–59. doi:10.1016/j.janxdis.2016.11.008
72. Cai H, Bai W, Yue Y, et al. Mapping network connectivity between internet addiction and residual depressive symptoms in patients with depression. Front Psychiatry. 2022;13:997593. doi:10.3389/fpsyt.2022.997593
73. van Borkulo CD, van Bork R, Boschloo L, et al. Comparing network structures on three aspects: a permutation test. Psychol Methods. 2022;28:1273–1285. doi:10.1037/met0000476
74. Victor SE, Klonsky ED. Correlates of suicide attempts among self-injurers: a meta-analysis. Clin Psychol Rev. 2014;34(4):282–297. doi:10.1016/j.cpr.2014.03.005
75. Brown CR, Hambleton IR, Sobers-Grannum N, et al. Social determinants of depression and suicidal behaviour in the Caribbean: a systematic review. BMC Public Health. 2017;17(1):577. doi:10.1186/s12889-017-4371-z
76. Calik G. Factors associated with anxiety and depression level in patients with a suicide attempt. Annal Clin Analy Med. 2020;11(Suppl_1):1.
77. Cheng JK, Fancher TL, Ratanasen M, et al. Lifetime suicidal ideation and suicide attempts in Asian Americans. Asian Am J Psychol. 2010;1(1):18–30. doi:10.1037/a0018799
78. Van de Velde S, Bracke P, Levecque K. Gender differences in depression in 23 European countries. Cross-national variation in the gender gap in depression. Soc sci med. 2010;71(2):305–313. doi:10.1016/j.socscimed.2010.03.035
79. Li Y, Li Y, Cao J. Factors associated with suicidal behaviors in mainland China: a meta-analysis. BMC Public Health. 2012;12(1):524. doi:10.1186/1471-2458-12-524
80. Lee J. Pathways from Education to Depression. J Cross Cul Gerontol. 2011;26(2):121–135. doi:10.1007/s10823-011-9142-1
81. Goldstein A, Gvion Y. Socio-demographic and psychological risk factors for suicidal behavior among individuals with anorexia and bulimia nervosa: a systematic review. J Affective Disorders. 2019;245:1149–1167. doi:10.1016/j.jad.2018.12.015
82. Jiménez M, Montorio I, Izal M. The association of age, sense of control, optimism, and self-esteem with emotional distress. Developmental Psychology. 2017;53:1398–1403. doi:10.1037/dev0000341
83. Oguntayo R. Age, gender, environmental degradation worry, and excessive precautionary behaviors of COVID-19 and suicidal thoughts: a border city-based survey. Curr Psychol. 2023. doi:10.1007/s12144-023-05367-6
84. Li S, Liu S, Zhang P, et al. Suicidal ideation in the general population in China after the COVID-19 pandemic was initially controlled. J Affect Disord. 2023;323:834–840. doi:10.1016/j.jad.2022.12.036
85. Dalege J, Borsboom D, van Harreveld F, van der Maas HLJ. Network analysis on attitudes: a brief tutorial. Soc Psychol Personal Sci. 2017;8(5):528–537. doi:10.1177/1948550617709827
86. Marchetti I. Hopelessness: a Network Analysis. Cognitive Ther Res. 2018;43(3):611–619. doi:10.1007/s10608-018-9981-y
87. Abdul Karim M, Ouanes S, Reagu SM, Alabdulla M. Network analysis of anxiety and depressive symptoms among quarantined individuals: cross-sectional study. BJPsych Open. 2021;7(6):e222. doi:10.1192/bjo.2021.1060
88. Nock MK, Borges G, Bromet EJ, et al. Cross-national prevalence and risk factors for suicidal ideation, plans and attempts. Br J Psychiatry. 2008;192(2):98–105. doi:10.1192/bjp.bp.107.040113
89. Chan LF, Shamsul AS, Maniam T. Are predictors of future suicide attempts and the transition from suicidal ideation to suicide attempts shared or distinct: a 12-month prospective study among patients with depressive disorders. Psychiatry Res. 2014;220(3):867–873. doi:10.1016/j.psychres.2014.08.055
90. Park EH, Hong N, Jon DI, Hong HJ, Jung MH. Past suicidal ideation as an independent risk factor for suicide behaviours in patients with depression. Int J Psychiatry Clin Pract. 2017;21(1):24–28. doi:10.1080/13651501.2016.1249489
91. Williams JM, Crane C, Barnhofer T, Van der Does AJ, Segal ZV. Recurrence of suicidal ideation across depressive episodes. J Affect Disord. 2006;91(2–3):189–194. doi:10.1016/j.jad.2006.01.002
92. Williams JMG, Van der Does AJW, Barnhofer T, Crane C, Segal ZS. Cognitive reactivity, suicidal ideation and future fluency: preliminary investigation of a differential activation theory of hopelessness/suicidality. Cognitive Ther Res. 2007;32(1):83–104. doi:10.1007/s10608-006-9105-y
93. Lau MA, Segal ZV, Williams JM. Teasdale’s differential activation hypothesis: implications for mechanisms of depressive relapse and suicidal behaviour. Behav Res Ther. 2004;42(9):1001–1017. doi:10.1016/j.brat.2004.03.003
94. Heuschen C, Mocking RJT, Zantvoord JB, et al. Suicidal ideation in remitted major depressive disorder predicts recurrence. J Psychiatr Res. 2022;151:65–72. doi:10.1016/j.jpsychires.2022.04.005
95. Dold M, Bartova L, Fugger G, et al. Major Depression and the Degree of Suicidality: results of the European Group for the Study of Resistant Depression (GSRD). Int J Neuropsychopharmacol. 2018;21(6):539–549. doi:10.1093/ijnp/pyy009
96. Fialho AR, Montezano BB, Ballester PL, et al. Predicting 3-year persistent or recurrent major depressive episode using machine learning techniques. Psych Res Communic. 2022;2(3):100055. doi:10.1016/j.psycom.2022.100055
97. Liu RT, Bettis AH, Burke TA. Characterizing the phenomenology of passive suicidal ideation: a systematic review and meta-analysis of its prevalence, psychiatric comorbidity, correlates, and comparisons with active suicidal ideation. Psychol Med. 2020;50(3):367–383. doi:10.1017/S003329171900391X
98. Franklin JC, Ribeiro JD, Fox KR, et al. Risk factors for suicidal thoughts and behaviors: a meta-analysis of 50 years of research. Psychol Bull. 2017;143(2):187–232. doi:10.1037/bul0000084
99. Fehling KB, Selby EA. Suicide in DSM-5: current evidence for the proposed suicide behavior disorder and other possible improvements. Front Psychiatry. 2020;11:499980. doi:10.3389/fpsyt.2020.499980
100. Ribeiro JD, Franklin JC, Fox KR, et al. Self-injurious thoughts and behaviors as risk factors for future suicide ideation, attempts, and death: a meta-analysis of longitudinal studies. Psychol Med. 2016;46(2):225–236. doi:10.1017/S0033291715001804
101. Zhao N, Li W, Zhang SF, et al. Network analysis of depressive symptoms among residents of Wuhan in the later stage of the COVID-19 pandemic. Front Psychiatry. 2021;12:735973. doi:10.3389/fpsyt.2021.735973
102. Jin Y, Sun HL, Lam SC, et al. Depressive symptoms and gender differences in older adults in Hong Kong during the COVID-19 pandemic: a network analysis approach. Int J Biol Sci. 2022;18(10):3934–3941. doi:10.7150/ijbs.69460
103. Gijzen MWM, Rasing SPA, Creemers DHM, Smit F, Engels R, De Beurs D. Suicide ideation as a symptom of adolescent depression. a network analysis. J Affect Disord. 2021;278:68–77. doi:10.1016/j.jad.2020.09.029
104. Sibitz I, Berger P, Freidl M, et al. ICD-10 or DSM-IV? Anhedonia, fatigue and depressed mood as screening symptoms for diagnosing a current depressive episode in physically ill patients in general hospital. J Affective Disorders. 2010;126:245–251. doi:10.1016/j.jad.2010.03.023
105. Oliván-Blázquez B, Rubio E, García-Sanz O, Magallón-Botaya R. Correlation between diagnosis of depression and symptoms present in primary care patients. Actas Espanolas de Psiquiatria. 2016;44(2):55–63.
106. Doyle F, Conroy R, McGee H, Delaney M. Depressive symptoms in persons with acute coronary syndrome: specific symptom scales and prognosis. J Psychosom Res. 2010;68(2):121–130. doi:10.1016/j.jpsychores.2009.07.013
107. Klein DF. Endogenomorphic depression: a conceptual and terminological revision. Arch Gen Psychiatry. 1974;31(4):447–454. doi:10.1001/archpsyc.1974.01760160005001
108. Billones RR, Kumar S, Saligan LN. Disentangling fatigue from anhedonia: a scoping review. Transl Psychiatry. 2020;10(1):273. doi:10.1038/s41398-020-00960-w
109. Suh WY, Lee J, Yun JY, Sim JA, Yun YH. A network analysis of suicidal ideation, depressive symptoms, and subjective well-being in a community population. J Psychiatr Res. 2021;142:263–271. doi:10.1016/j.jpsychires.2021.08.008
110. Nyer M, Mischoulon D, Alpert JE, et al. College students with depressive symptoms with and without fatigue: differences in functioning, suicidality, anxiety, and depressive severity. Ann Clin Psychiatry. 2015;27(2):100–108.
111. Zavlis O, Butter S, Bennett K, et al. How does the COVID-19 pandemic impact on population mental health? A network analysis of COVID influences on depression, anxiety and traumatic stress in the UK population. Psychol Med. 2021:1–9. doi:10.1017/S0033291721000635
112. Sepúlveda-Loyola W, Rodríguez-Sánchez I, Pérez-Rodríguez P, et al. Impact of social isolation due to COVID-19 on health in older people: mental and physical effects and recommendations. j nutr health aging. 2020;24(9):938–947. doi:10.1007/s12603-020-1500-7
113. Twomey R, DeMars J, Franklin K, Culos-Reed SN, Weatherald J, Wrightson JG. Chronic fatigue and postexertional malaise in people living with long COVID: an observational study. Phys Ther. 2022;102(4). doi:10.1093/ptj/pzac005
114. Sandler CX, Wyller VBB, Moss-Morris R, et al. Long COVID and Post-infective Fatigue Syndrome: a Review. Open Forum Infect Dis. 2021;8(10):ofab440. doi:10.1093/ofid/ofab440
115. Gasnier M, Choucha W, Radiguer F, et al. Comorbidity of long COVID and psychiatric disorders after a hospitalisation for COVID-19: a cross-sectional study. J Neurol Neurosurg Psychiatry. 2022;93:1091–1098. doi:10.1136/jnnp-2021-328516
116. Salari N, Khodayari Y, Hosseinian-Far A, et al. Global prevalence of chronic fatigue syndrome among long COVID-19 patients: a systematic review and meta-analysis. Biopsychosoc Med. 2022;16(1):21. doi:10.1186/s13030-022-00250-5
117. Guo Q, Zheng Y, Shi J, et al. Immediate psychological distress in quarantined patients with COVID-19 and its association with peripheral inflammation: a mixed-method study. Brain Behav Immun. 2020;88:17–27. doi:10.1016/j.bbi.2020.05.038
118. Brooks SK, Webster RK, Smith LE, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. 2020;395(10227):912–920. doi:10.1016/S0140-6736(20)30460-8
119. Cavalera C. COVID-19 Psychological Implications: the Role of Shame and Guilt. Front Psychol. 2020;11:571828. doi:10.3389/fpsyg.2020.571828
120. Gilbert P. The origins and nature of compassion focused therapy. Br J Clin Psychol. 2014;53(1):6–41. doi:10.1111/bjc.12043
121. Dainer-Best J, Trujillo LT, Schnyer DM, Beevers CG. Sustained engagement of attention is associated with increased negative self-referent processing in major depressive disorder. Biol Psychol. 2017;129:231–241. doi:10.1016/j.biopsycho.2017.09.005
122. Luck T, Luck-Sikorski C. Feelings of guilt in the general adult population: prevalence, intensity and association with depression. Psychol Health Med. 2021;26(9):1143–1153. doi:10.1080/13548506.2020.1859558
123. O’Connor RC, Kirtley OJ. The integrated motivational-volitional model of suicidal behaviour. Philos Trans R Soc Lond B Biol Sci. 2018;373:1754. doi:10.1098/rstb.2017.0268
124. Jeon HJ, Park JI, Fava M, et al. Feelings of worthlessness, traumatic experience, and their comorbidity in relation to lifetime suicide attempt in community adults with major depressive disorder. J Affect Disord. 2014;166:206–212. doi:10.1016/j.jad.2014.05.010
125. Kealy D, Treeby MS, Rice SM. Shame, guilt, and suicidal thoughts: the interaction matters. Br J Clin Psychol. 2021;60(3):414–423. doi:10.1111/bjc.12291
126. Fried EI, Nesse RM. The impact of individual depressive symptoms on impairment of psychosocial functioning. PLoS One. 2014;9(2):e90311. doi:10.1371/journal.pone.0090311
127. Morin CM, Bjorvatn B, Chung F, et al. Insomnia, anxiety, and depression during the COVID-19 pandemic: an international collaborative study. Sleep Med. 2021;87:38–45. doi:10.1016/j.sleep.2021.07.035
128. Serafini G, Parmigiani B, Amerio A, Aguglia A, Sher L, Amore M. The psychological impact of COVID-19 on the mental health in the general population. QJM. 2020;113(8):531–537. doi:10.1093/qjmed/hcaa201
129. McCall WV, Blocker JN, D’Agostino R, et al. Insomnia severity is an indicator of suicidal ideation during a depression clinical trial. Sleep Med. 2010;11(9):822–827. doi:10.1016/j.sleep.2010.04.004
130. Simmons Z, Burlingame G, Korbanka J, et al. Insomnia symptom severity is associated with increased suicidality and death by suicide in a sample of patients with psychiatric disorders. Sleep. 2021;44(7). doi:10.1093/sleep/zsab032
131. Harris LM, Huang X, Linthicum KP, Bryen CP, Ribeiro JD. Sleep disturbances as risk factors for suicidal thoughts and behaviours: a meta-analysis of longitudinal studies. Sci Rep. 2020;10(1):13888. doi:10.1038/s41598-020-70866-6
132. Singareddy RK, Balon R. Sleep and suicide in psychiatric patients. Ann Clin Psychiatry. 2001;13(2):93. doi:10.3109/10401230109148954
133. Liu X, Buysse DJ. Sleep and youth suicidal behavior: a neglected field. Curr Opin Psychiatry. 2006;19(3):288–293. doi:10.1097/01.yco.0000218600.40593.18
134. McCall WV, Batson N, Webster M, et al. Nightmares and dysfunctional beliefs about sleep mediate the effect of insomnia symptoms on suicidal ideation. J Clin Sleep Med. 2013;9(2):135–140. doi:10.5664/jcsm.2408
135. Cha EJ, Jeon HJ, Chung S. Central Symptoms of Insomnia in Relation to Depression and COVID-19 Anxiety in General Population: a Network Analysis. J Clin Med. 2022;11(12):3416. doi:10.3390/jcm11123416
136. Tseng HW, Chou FH, Chen CH, Chang YP. Effects of Mindfulness-Based Cognitive Therapy on Major Depressive Disorder with Multiple Episodes: a Systematic Review and Meta-Analysis. Int J Environ Res Public Health. 2023;20(2):1555. doi:10.3390/ijerph20021555
137. Edinger JD, Means MK. Cognitive-behavioral therapy for primary insomnia. Clin Psychol Rev. 2005;25(5):539–558. doi:10.1016/j.cpr.2005.04.003
138. Drapeau CW, Nadorff MR. Suicidality in sleep disorders: prevalence, impact, and management strategies. Nat Sci Sleep. 2017;9:213–226. doi:10.2147/NSS.S125597
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Understanding Comorbidity Between Non-Suicidal Self-Injury and Depressive Symptoms in a Clinical Sample of Adolescents: A Network Analysis
Niu S, Yin X, Pan B, Chen H, Dai C, Tong C, Chen F, Feng X
Neuropsychiatric Disease and Treatment 2024, 20:1-17
Published Date: 4 January 2024
Intrinsic Association Between Death Anxiety and Depression Among Men Living with HIV/AIDS in China: A Network Analysis
Zheng C, Liang L, Kiyum M, Yuan T, Fei J, Wang H, Gao J, Liu X, Mei S, Du N
Psychology Research and Behavior Management 2024, 17:4073-4085
Published Date: 29 November 2024
Family Functioning, Anxiety and Depression in Chinese Higher Vocational School Students: A Network Analysis
Ye L, Chen S, Chen QW, Luo X
Psychology Research and Behavior Management 2024, 17:4399-4412
Published Date: 25 December 2024
Echoes of Strain: A Two-Year Longitudinal Study on the Impact of China’s Zero-COVID Policy on College Students’ Insomnia and Depressive Symptoms
Wang S, Zou X, Tang Q, Zhang L, Liu X, Liu G, Tao Y
Nature and Science of Sleep 2025, 17:81-96
Published Date: 13 January 2025
Network Analysis of Anxiety, Insomnia, Depression, and Suicide Attempts in Chinese Outpatients with Somatic Symptom Disorder
Fang J, Tang H, Liao H, Zhong Y, Li Y, Liao Y, Li Y
Neuropsychiatric Disease and Treatment 2025, 21:1091-1105
Published Date: 22 May 2025