Back to Journals » Journal of Pain Research » Volume 15
The Impact of Scripted Self-Hypnotic Relaxation on the Periprocedural Experience and Anesthesiologist Sedation Use in the Pediatric Cardiac Catheterization Suite: A Prospective Randomized Controlled Trial
Authors Viegas J ![]() , Holtby H, Runeckles K
, Holtby H, Runeckles K ![]() , Lang EV
, Lang EV ![]()
Received 16 May 2022
Accepted for publication 28 September 2022
Published 27 October 2022 Volume 2022:15 Pages 3447—3458
DOI https://doi.org/10.2147/JPR.S373608
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Ellen Soffin
Jacqueline Viegas,1 Helen Holtby,2 Kyle Runeckles,3 Elvira V Lang4
1Cardiac Diagnostic and Interventional Unit, Labatt Family Heart Centre, The Hospital for Sick Children, Toronto, Ontario, Canada; 2Department of Anesthesia, The Hospital for Sick Children, Toronto, Ontario, Canada; 3University Health Network Research Institute, Toronto, Ontario, Canada; 4Hypnalgesics, LLC, Brookline, MA, USA
Correspondence: Jacqueline Viegas, Cardiac Diagnostic and Interventional Unit, Labatt Family Heart Centre, The Hospital for Sick Children, 555 University Ave, Toronto, Ontario, M5G1X8, Canada, Tel +1 416 659 4443, Fax +1 416 813 6404, Email [email protected]
Purpose: To assess the impact on children of self-hypnotic relaxation scripts read by trained staff prior to the induction of anesthesia and/or extubation on the periprocedural experience.
Patients and Methods: A total of 160 children aged 7– 18 years undergoing a cardiac catheterization intervention under general anesthesia were randomized into 4 groups: (1) a pre-procedure (PP-script) read prior to entering the procedural room, (2) a script read prior to extubation (PX-Script), (3) both PP- and PX-Scripts read and (4) no script read. Anxiety and pain were rated on self-reported 0– 10 scales. The modified Yale Preoperative Anxiety Scale was used for preoperative anxiety. The effect of script reading was associated with outcomes by linear regression for continuous variables, and logistic regression for binary variables in two-sided tests at a significance level of 0.05. Results are given in odds ratios (OR) and 95% confidence intervals (CI).
Results: Data were available for 158 patients. Reading the PP-Script prior to anesthesia was associated with a significant reduction in the use of intraoperative sedatives from 30% to 14% (OR 0.40; CI 0.18– 0.88; p = 0.02) by the anesthesiologists, who were blinded to group attribution until extubation. This was despite the children not self-reporting significantly lower levels of anxiety or pain. The PX-Script did not change outcomes. Among groups, there was no significant difference in room time, postoperative recovery time and pain.
Conclusion: Reading a PP-Script for guidance in self-hypnotic relaxation can result in less need for intravenous sedation in the judgment of the anesthesiologist, independent of the children’s self-reported anxiety and pain. This raises interesting questions about subconscious patient–physician interactions affecting pain management.
Clinicaltrials.gov Identifier: NCT02347748.
Keywords: sedation, anesthesia, children, pain, anxiety
Introduction
Induction of general anesthesia can be distressing for children.1–4 High preoperative anxiety is considered a predictor of emergence delirium, postoperative pain, prolonged recovery, and postoperative maladaptive behavior.2,5–7 Premedication with sedatives can alleviate preoperative anxiety,8 but adds some risk and cost, and is not universally accepted.9,10 Thus, attention has been directed towards nonpharmacologic approaches such as parental presence, use of clown doctors, hypnosis, video games, or music, yielding mixed success.4,11
Explicitly remembered awareness under anesthesia is reported to be 0.1–0.2% in adults, and 8–10 times higher in children.12 Subconscious recall of audible events is estimated to be as high as 20–30%.13 On one hand, awareness during general anesthesia has been associated with creation of traumatic memories and symptoms of post-traumatic stress disorder,14–16 on the other hand, therapeutic hypnotic suggestions delivered via earphones under general anesthesia have been associated with reduced postoperative pain and need for drugs in adults.17
The use of self-hypnotic relaxation scripts prior to interventional radiological procedures under conscious sedation resulted in a reduction of anxiety, pain, drug use, procedure time and complications in adult patients.18–20 This study aimed to investigate whether a script, adapted for pediatric use, read prior to percutaneous cardiac interventions under general anesthesia had similar benefits. Since there is debate about the use of audible positive suggestions of healing during anesthesia, we also assessed whether a script read prior to extubation would further improve recovery.
We hypothesize that reading a pre-procedural (PP) self-hypnotic script to patients results in less anxiety prior to induction of anesthesia, a reduced need for sedation, and better procedural and short-term recovery outcomes. We further hypothesize that participants who are read a pre-extubation (PX) script recover better than controls, and the combination of the PP and PX scripts has the greatest positive effect on physical and emotional well-being.
Materials and Methods
Trial Design and Setting
After approval by the Research Ethics Board of The Hospital for Sick Children, Toronto, Canada, which governs all hospital research activity in accordance with the Tri-Council Policy Statement on Ethical Conduct of Research Involving Humans; the International Conference on Harmonization Good Clinical Practice Guidelines; Part C, Division 5 of the Food and Drug Regulations of Canada; Part 4 of the Natural Health Product Regulations; Medical Devices Regulations; the provisions within the Ontario Personal Health Information protection Act; and the Declaration of Helsinki, a prospective randomized controlled trial with 160 patients aged 7–18 years was conducted at the Cardiac Diagnostic and Interventional Unit of a tertiary medical center from January 2014 to August 2018. The site investigators conducted the trial, controlled the data, and performed statistical analyses.
English-speaking children aged 7–18 who were scheduled for cardiac catheterization under general anesthesia were included. Exclusion criteria were cognitive impairment and known dissociative psychiatric disease.
Interventions
The interventions consisted of 1) the reading of a self-hypnotic relaxation pre-procedure script (“PP-Script”) adapted for children from language found to be effective in adults in reducing anxiety, pain and complications of invasive-image guided procedures.18–20 This script was read in the pre-catheterization work-up area, by one of three nurses, trained in procedural hypnotic language (Comfort Talk®, Brookline, MA). It contained relaxing and hypnotic language with suggestions for ego strengthening and coping; 2) The second intervention was the reading of a pre-extubation script (“PX-Script”) containing suggestions for healing and recovery with acknowledgement of the patient’s contribution during the procedure. It was read by one of the same three nurses, immediately after the anesthetic gases were turned off at the end of the procedure and prior to extubation. The scripts are added to the Appendix for informative purposes only and should only be used with the appropriate training in their application.
Participants were randomized to one of the 4 groups: in group 1 they were read the PP-Script, in group 2 the PX-Script, in group 3 both the PP and the PX-Scripts, and in group 4, the control group, they were not read either script.
Outcome Measures
Anxiety and Pain
Patients’ level of anxiety on arrival and prior to meeting the anesthesiologist was measured by the modified Yale Preoperative Anxiety Scale (mYPAS) which has been validated for use with children.1 There are 22 questions in 5 domains, and the overall score is calculated as follows: (activity score/4 + vocalizations score/6 + emotional expressivity score/4 + state of arousal score/4 + parent engagement/4)*20. Overall scores range from a minimum of 23.3 to a maximum of 100.
Pain and anxiety were further assessed on 0–10 verbal self-report scales which have been validated for adult and pediatric populations.21–23 They were recorded upon presentation, and after randomization prior to entering the procedure room. Patients were asked to “Please let us know how comfortable you are right now on a scale of 0–10 with 0 meaning no anxiety or pain at all and 10 worst possible.” The neutral query about comfort levels as an introduction was used to avoid setting expectations of pain and anxiety. Potential enhancement of the pain perception has been associated with use of negative suggestions.24
Pediatric Anesthesia Behavior (PAB)
The effect of the PP-Script on the patient’s behavior during anesthesia induction was measured by the Pediatric Anesthesia Behavior (PAB) scale.25 The PAB correlates strongly with the mYPAS and demonstrates reliability and validity in assessment of both pre-induction behavior and the correlation with postoperative outcomes such as agitation in the Post Anesthesia Care Unit (PACU) and maladaptive behaviors at home. The PAB uses three scores: 1=Happy (calm and controlled; compliant); 2=Sad (tearful and/or withdrawn but compliant); and 3=Mad (loud vocal resistance with screaming or shouting and/or physical resistance to induction requiring physical restraint by staff and/or parents).
Procedural Experience and Drug Use
The procedural experience was assessed in terms of procedure time, drug use, and complications.
Recovery
Immediate recovery measures were time spent in the recovery room, self-reported pain and anxiety, post-procedural drug use, vomiting, and adverse events.
Sample Size
Sample size determination was based on the mYPAS score.1 Levels of ~35±10 (out of 100) are reported in high-stress situations in children. The mean reported differences in outcome in studies examining reduction of preoperative anxiety were 17 for parental acupuncture, 24 for a hypnotic intervention, and 30.75 for use of clowns.26,27 To be able to detect a pairwise difference of 8 points in mYPAS with a power of 85% at a combined alpha level of 0.05 for the full regression model (pairwise alpha level of 0.0166) 35 patients per group are needed, which we increased to 40 per group (15%) to account for dropouts and withdrawal. Sample size was calculated using Power and Sample size (PASS) statistical software v8.0 (NCSS, Kaysville, UT).
Randomization
A statistical colleague external to the research team generated a list of random assignments for 160 subjects using 160 unique study ID numbers. Block randomization was used, and 160 sealed, opaque, sequentially numbered envelopes were prepared. The envelopes contained random group assignment for that study ID to one of the four groups described above.
Procedure Flow and Blinding
The children and/or their parents were approached by one of the research nurses regarding study participation during their pre-catheterization visit. If they were interested, the details were explained, and written, signed informed consent was obtained by one of the study team members during the visit from the parent or legal guardian of the child. Consent for the catheterization procedure itself was also obtained during the same visit.
On the day of the procedure, the admitting registered nurse obtained the baseline patient data, mYPAS rating and pain/anxiety ratings. Upon transfer to the unit in which the cardiac procedure was to be performed, one of the three nurses trained in procedural hypnotic language read the PP-Script, if required by group attribution, and recorded the second mYPAS rating. Afterwards, the anesthesiologist who was blinded to group allocation assessed the child. Premedication was given at the discretion of the anesthesiologist. The most common pre-medication used was oral midazolam 0.5mg/kg mixed with acetaminophen 15mg/kg. Adolescents were given lorazepam 1–2mg. All patients had balanced general anesthesia with a controlled airway. Fentanyl or morphine was routinely used at induction. Additional sedation was optional and coded as given or not.
The child was asked again to rate their pain and anxiety level, just prior to walking into the procedure room with the nurse. The anesthesiologist and other team members were blinded to group attribution, at least until extubation.
Partial group attribution was exposed to the team prior to extubation: reading the PX-Script revealed that the participant was in group 2 (PX-Script) or Group 3 (PP + PX-Scripts) versus group 1 (PP-Script only) or 4=no Script. No-one could distinguish between either group 2 and 3, or 1 and 4, respectively. Staff and participants did not reveal group assignments to the recovery room or in-patient unit staff recording anxiety and pain scores or administering post-procedural pain medication.
Patients were aware of group allocation with regards to the PP-Script but were not consciously aware of the reading of the PX-Script.
Statistical Methods
The analysis was conducted using an intent-to-treat approach. Missing values in outcomes and covariates were not imputed. For each outcome, a linear (continuous) or logistic (binary) regression model was created. Study intervention was coded as a dual set of binary variables (group 1: PP-Script only as 1–0, group 2: PX-Script only 0–1, group 3: both PP-plus PX-Scripts 1–1 and group 4: neither intervention 0–0), using the group with neither intervention as the reference categories and contrasting each group to all others within the regression model. As needed, linear outcomes were investigated for potential mathematical transformations where their distribution significantly deviated from normal. Adjustments for important confounders or variables which failed the test of randomization were integrated in the regression models as needed.
Scores on entry into the procedure room were used as outcomes in a linear regression model using pre-reading scores and group assignment as independent covariates. PP-Script scores were an adjustment factor, while group assignment determined whether the PP-Script reduced the increase in anxiety as the patient entered the procedure room. All data analyses were performed using SAS v9.3 (The SAS Institute, Cary, NC).
For summarizing the effect of the PP-Script on the mYPAS, pain rating, and anxiety rating, estimates (95% CI) as the center of the confidence intervals are given as a measure of the difference with positive numbers reflecting a positive difference, and negative numbers a negative one. Odd ratios (OR) are given for outcomes that are based on binary data (eg present/not present).
Continuous variables are presented in terms of medians (interquartile ranges) and for some measures in means ± standard deviations to allow comparisons in the literature that use the latter.
Wilcoxon-Mann–Whitney tests were used to assess how patients’ anxiety related to the behavior of anesthesiologists with regard to premedication and intraoperative sedatives.
Since different anxiety measures were used for the assessment of anxiety prior to premedication and prior to intubation in the operating room, we used Spearman’s rank correlation coefficient to evaluate the strength of the relationship between the mYPAS and 0–10 anxiety ratings based on the baseline data, when both measures were obtained simultaneously.
Results
Participants
Between January 2014 and July 2018, 160 children were randomized and received their allocated treatment (Figure 1). The data folders on two subjects in the PP group were inadvertently discarded during transfer to the ward from the recovery unit. They are thus not included in the analysis, leaving 158 enrolled patients for analysis which still exceeds the number targeted in the sample analysis.
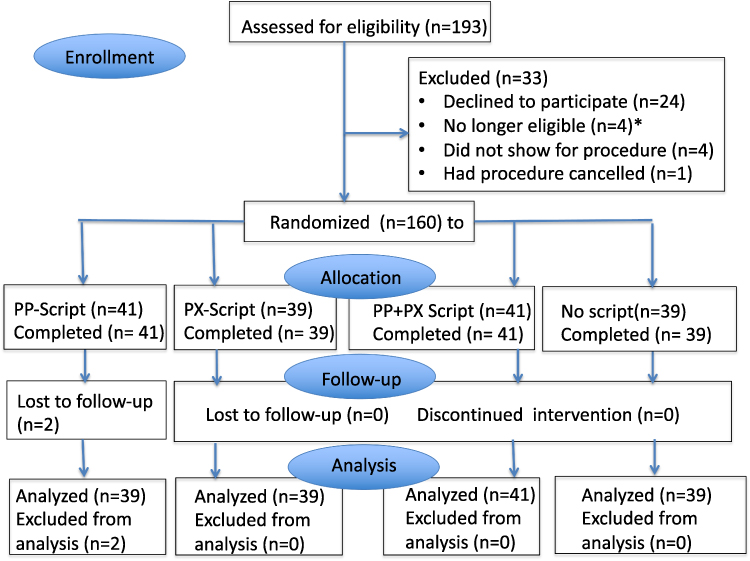 |
Figure 1 Flow chart of patient enrollment. Note: *Participants were no longer eligible as anesthesia was cancelled. |
Patients’ demographics and procedure characteristics are shown in Table 1. Upon induction, all children received a standard dose of analgesic (fentanyl or morphine) with the exception of one patient in group 2.
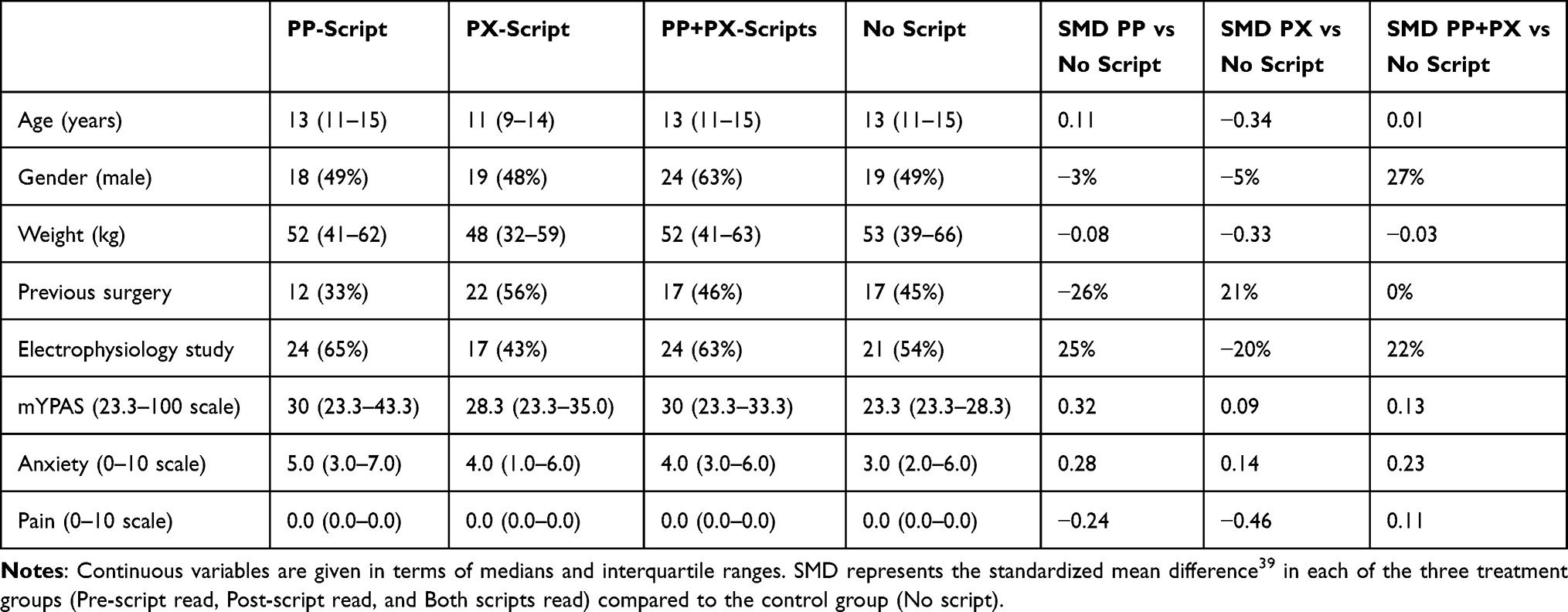 |
Table 1 Patient and Procedure Characteristics at Baseline |
Effects Associated with the Pre-Procedure (PP)-Script
Comparison of Baseline Prior to Randomization
To assess the effect of the PP-Script on subsequent outcomes, groups were combined such that patients who had the script read prior to intubation (groups 1 and 3) were compared to patients who did not have a script read (groups 2 and 4). Their baseline data are given in Table 1.
Both children in the combined No-PP-Script group and PP-Script group reported no pain (0 [0–0] vs 0[0–0]; p=0.14). The baseline mYPAS showed a trend toward lower anxiety in the combined No-PP-Script groups of 23.3 (23.3–28.3) vs the combined PP-Script group (23.3 [23.3–33.3]; p=0.05). The children’s’ self-report of anxiety on the 0–0 scale did not differ significantly between the combined No-PP-Script group and PP-Script group (3.0 [1.0–5.0]) vs (4.0 [2.0–5.0]; p=0.24). In this context, it is important to note that the comparison of the YPAS and 0–10 anxiety ratings at baseline, when both measures were obtained simultaneously, showed the variables to be correlated, but only weakly so (Spearman’s rho = 0.34 (0.19–0.47, p<0.001)).
Immediate Effects on the mYPAS and Premedication
The mYPAS obtained by the nurse after reading/not reading the PP-Script, but prior to the child meeting the anesthesiologist in the preparation room, showed no significant difference among the groups: PP-Script 23.3 (23.3.-35.0) and no PP-Script group 23.3 (23.3–33.3; p=0.68). Estimates of the effect of the PP-Script on anxiety in terms of the center of confidence intervals and 95% confidence intervals for the mYPAS were 0.9 (−0.98–2.79; p=0.63).
The anesthesiologists who were blinded to the children’s group attribution and mYPAS ratings administered premedication to 9 of 77 children in the PP-Script group (12%) and 7 of 81 (9%) in the no-PP-Script group (p=0.60).
To assess whether there was an association between anxiety levels and likelihood of prescribing medication, we compared the mYPAS measures obtained right before the anesthesiologist saw the child among children who received premedication and those who did not: Those who received premedication had significantly higher anxiety levels (37.5 [23.3–49.2]), than those who did not (23.3 [23.3–33.3]; p=0.006).
Intraoperative Effects
The following analyses encompass the time from entry in the procedure room until the point before extubation after which, depending on group attribution, the PX-Script was read (Table 2). Up to this point, the anesthesiologists were still blinded to group attribution. The overall anxiety and pain ratings and PAB scores, by which the anesthesiologists rated the behavior of the children upon entry in the operating room, did not differ significantly among PP-Script and No-PP-Script groups. Estimates of the effect of the PP-Script on anxiety in terms of the center of confidence intervals and 95% confidence intervals were: for 0–10 anxiety ratings 0.43 (−0.26–1.11; p=0.54), and pain ratings 0.15 (−0.07–0.38; p=0.50). Most children (88%) were considered to be “1=Happy (calm and controlled; compliant with induction).”
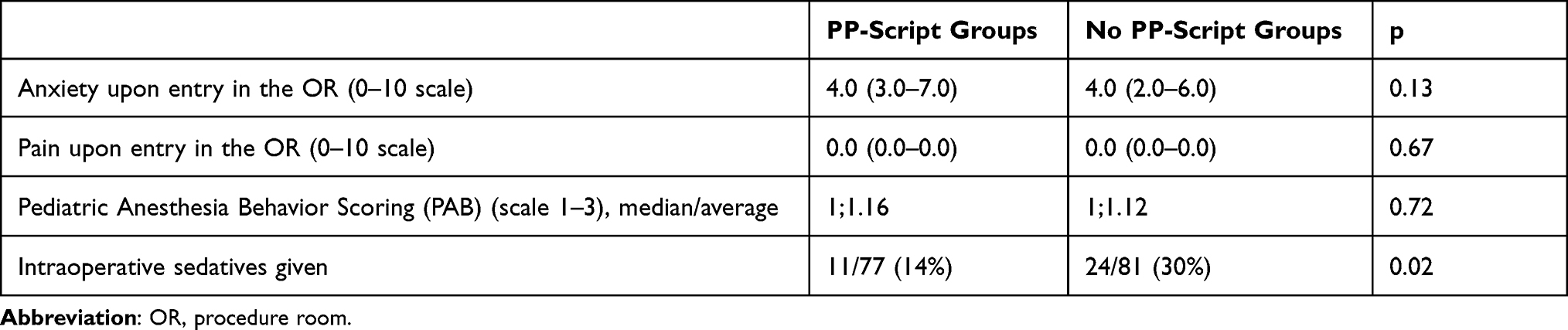 |
Table 2 Effects Associated with Reading of the PP-Script on the Operating Room Experience |
Reading the PP-Script was associated with a significant reduction in the use of intraoperative sedatives (midazolam) by the anesthesiologists (OR 0.40; CI 0.18–0.88; p=0.02). This was despite there being no difference in self-reported anxiety, pain, and PAB score among the groups. Even if one were to postulate that the two patients who had read the PP-Script and whose data were lost to follow-up would both have received sedatives, the result would not have changed and would have remained significant (p=0.048).
When further assessing how anxiety levels affected the decision to give intravenous sedatives, the correlation between anxiety levels, as measured by the mYPAS, and premedication behavior by the anesthesiologists no longer held. Children who received intravenous sedatives in the operating room self-reported anxiety levels of a median of 4.5 (2.0–6.0), those who did not had a median of 4.0 (2.0–7.0; p=0.48). Seven children given premedication did not receive additional sedatives at induction and nine children who had premedication did receive IV sedation intraoperatively.
Pre-Extubation (PX) Script and Overall Effects
Neither the PP- nor PX-Scripts by themselves nor in combination were associated with significant differences in the room time, recovery time, medication use, adverse events, vomiting, or the time course of the pain and anxiety assessments (Tables 3 and 4; Figure 2A and B). At most time points during the recovery period, anxiety ratings were low with >70% scoring 0 or being asleep. Also, the postoperative pain ratings were uniformly low. Overall, participants were stable hemodynamically. Any differences were statistically and clinically insignificant.
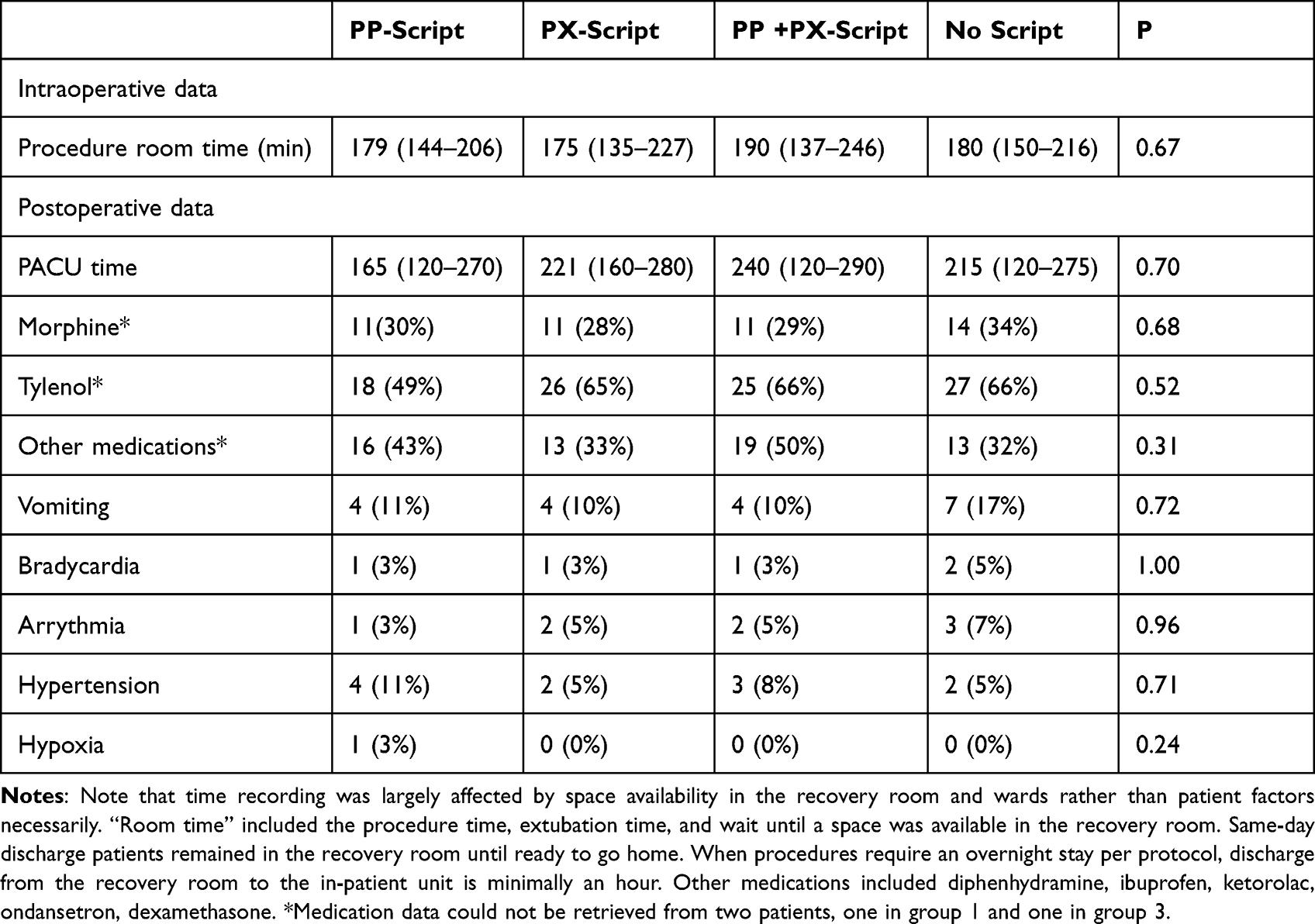 |
Table 3 Procedure Times and Post Recovery Course in the PACU |
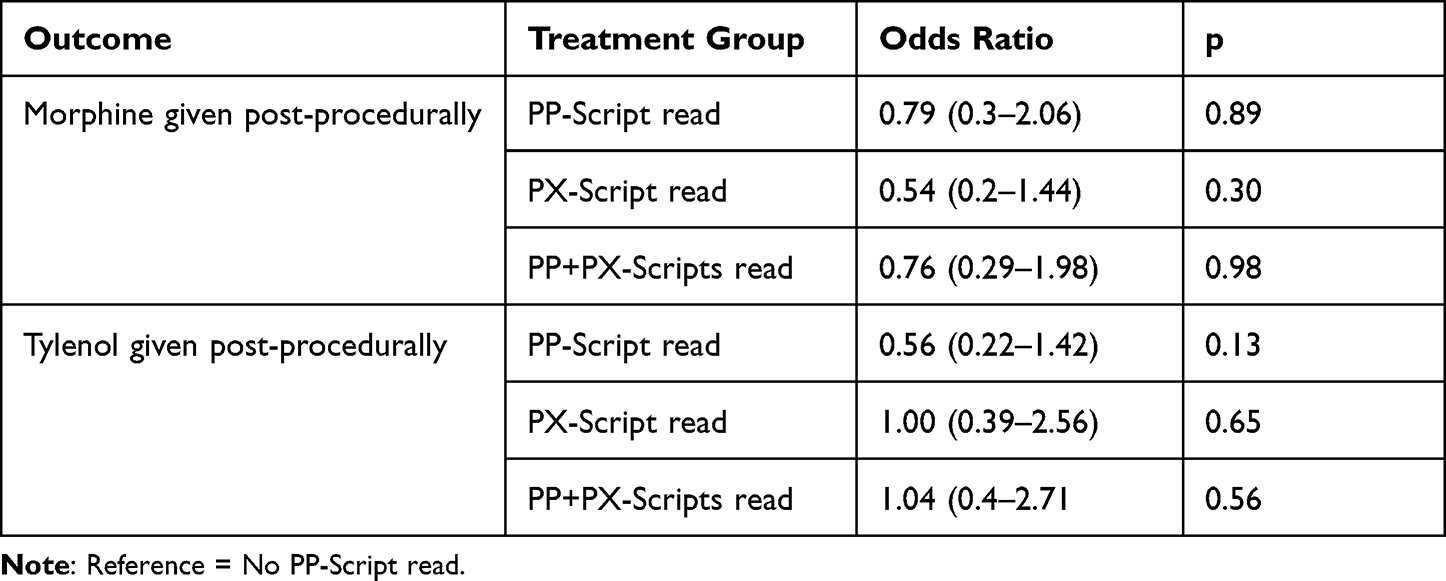 |
Table 4 Odd-Ratios of Post Procedure Outcomes |
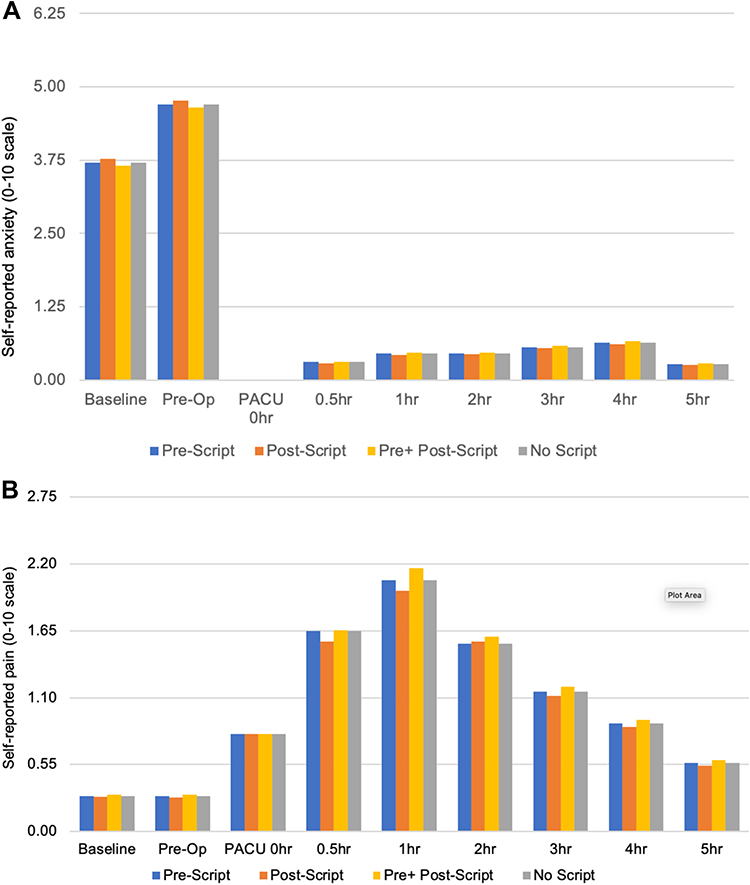 |
Figure 2 Average self-reported anxiety (A) and pain scores (B) on 0–10 scales. Ratings include those at baseline prior to randomization, after randomization, and after arrival in the PACU (Time 0), 0.5, 1, 2, 3, 4, and 6 hrs thereafter. Means were chosen since the majority of postoperative ratings had a median of zero and to facilitate comparisons with the literature. |
Discussion
The key finding is that there was a correlation between reading the PP-Script and the likelihood of receiving intravenous sedation in the operating room. Preceding in the preoperative holding area, the anesthesiologists’ choice to administer oral sedative premedication had been associated with higher measured anxiety levels in the children and had been independent of whether the PP-Script had been read or not. This correlation of sedation with anxiety levels was no longer the case at the time of anesthesia induction in the operating room. There, the main determinant of sedation was whether children had been read the PP-Script. Children to whom the PP-Script had been read received significantly less intravenous sedation on induction of anesthesia even though their anxiety levels were not lower than those of the control group. One interpretation may be that the preoperative use of the self-hypnotic intervention produced physiological effects and/or behavioral responses that the anesthesiologists observed but that were not captured in the instruments used. It is possible that the children who had the PP-Script read may have assimilated its ego strengthening and relaxing elements and/or might have had less sympathetic tone and more stable physiologic parameters.
A study by Eijlers et al with children randomized to virtual reality exposure preoperatively similarly found no impact on children’s anxiety as measured by YPAS and self-reported anxiety, but a significantly reduced frequency of administration of rescue analgesia by blinded recovery room personnel in children with adenoidectomy/tonsillectomy in comparison to children receiving care as usual.28 As Eijlers et al note,28 it may be possible that in a setting like theirs – comparable to the one in this study – where children present with low anxiety levels, treatment effects may not be as discernable as in studies using similar interventions where children present with high anxiety.29 The interval between reading the PP-Script and entry into the operating room was short, possibly too short to allow anxiety to develop. Measurement of anxiety immediately prior to anesthesia might have shown a difference. Several studies in adults show anxiety, measured on 0–10 scales, significantly declined over time in patients having a self-hypnotic relaxation script read to them as compared to an increase in patients having standard care treatment during surgical interventions under conscious sedation.18,20 In a study assessing use of virtual reality immersion versus no audiovisual distraction in children with a preoperative baseline YPAS of 28.3 (23.3–28.3) (median IQR), no change in the score was noted in the test group, but an increase in anxiety in the control group upon entry into the operating room, and a resulting 6.0-point lower mYPAS score (95% confidence interval [CI], 0.7–11.3; P = 0.03) in the test group at that time increased to a 14.5-point lower score (95% CI, 9.3–19.8; P < 0.0001) at induction.30 Similarly, Calipel et al failed to show a difference between children receiving anesthesiologist-guided hypnosis vs midazolam premedication upon entry into the operating room, but demonstrated it at the time of facemask placement. Lengthier protocols with guided imagery also reported reduced anxiety in children prior to induction of anesthesia.31–33
None of the interventions we used was associated with significant effects on postoperative pain, anxiety, recovery, medication use, or incidence of vomiting. Nausea and vomiting in the PACU were also not different in a randomized trial using personalized therapeutic suggestions that used a standard script and details about the child within a story read by mothers on a CD.34 A clinical trial, similar to ours, with children between 10 and 18 years of age who were randomized to receive a short 5–10 min hypnotic induction through trained staff in the operating room also did not show significant effects on the course of postoperative pain, anxiety, and morphine use.35 A randomized study with a lengthier preoperative hypnotic intervention showed a reduction in postoperative pain,32 but a meta-analysis of many other trials failed to do so.33
There is increasing interest in the interactions between the state of mind of patients and treating healthcare professionals. MRI and clinical evidence have shown a complex interdependence for encounters with adult patients.36–38 No such similar studies have been done in children yet to our knowledge. Simultaneous MRI scanning of both adult patients and their clinicians who interacted in live video, while the clinicians used acupuncture to treat evoked pain, showed a brain-to-brain concordance in circuitry with regard to pain/vicarious pain intensity among clinician/patient.36 Increased facial mirroring between patients and clinicians was also associated with a stronger perception of therapeutic alliance and greater analgesia.36 It has not been similarly evaluated whether the states of mind of patient and clinician feed off each other in the assessment of the situation and also affect behavior when treating children. This merits further research.
Limitations
The children in our cohort had relatively low mYPAS ratings from the onset which may have interfered with assessment of the effects of increased anxiety. The relatively low correlation between the YPAS and 0–10 self-reported anxiety measures may indicate that anxiety assessments in children are not as robust as in adults when it comes to prediction of peri- and postoperative outcomes. Not measuring the children’s anxiety right before intubation may have missed differences. Future research may indicate which biometric measures may be best suitable to determine the state of mind of child and anesthesiologist to further elucidate their interaction in that setting.
It is possible that the nursing staff who read the scripts in our study and had been trained in advanced communication and hypnotic language may have also displayed soothing behavior to the children in the control group. Similarly, Duparc-Alegria et al indicated the fact that the nursing staff who provided the scripts in their study had been trained in the hypnotic language techniques that underlie them, and may have integrated them into their natural mode of communication and thereby improved the experience of the patients in the control groups.35
Conclusion
Reading a PP-Script can result in less need for intravenous sedation in the judgment of the anesthesiologist, independent of the children’s self-reported anxiety and pain. This raises interesting questions about subconscious interactions between the patient and the staff directing pain management.
Data Sharing Statement
The authors will make deidentified participant data available to individual researchers who desire those for meta-analyses or other scientifically valid assessment per written/emailed requests specific to their needs and in accordance with their Institutional Review Boards and the Ethics Review Board of The Hospital for Sick Children, Toronto, CA. They will be made available for 7 years. The study scripts are included in the appendix with the caveat that they should only be used with additional training in how to apply them. The study protocol can be found on ClinicalTrials.gov NCT02347748.
Acknowledgments
We gratefully acknowledge the assistance of Janine Barclay RN and Susan Johnston RN, BScN, in their expert reading of the scripts for this study and for their assistance in data collection. We would also like to acknowledge the nursing teams of the Cardiac Diagnostic Interventional Unit, recovery room and cardiac in-patient unit who provided assistance in data collection. We are grateful to the treating cardiologists and anesthesiologists for their support of this project in allowing their patients to participate and to the anesthesia team for their support of and cooperation with the study.
Author Information
Jacqueline Viegas RN
Dr Helen Holtby MB, BS, FRCPC
Kyle Runeckles MSc
Elvira V. Lang MD, PhD, FSIR, FSCEH.
Funding
The research team gratefully thanks the Labatt Family Heart Centre Innovation Fund for the seed funding provided in support of this project (Principal Investigator JV). The study was also supported, in part, by an award from the National Institute of Health/National Center for Complementary and Integrative Medicine (R44AT006296, Principal Investigator EVL). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Health.
Disclosure
Authors Jacqueline Viegas, Helen Holtby, and Kyle Runeckles report no conflicts of interest in this work. Author Elvira V. Lang is owner of Hypnalgesics, LLC d/b/a Comfort Talk®, a company dedicated to the training of frontline staff in communication and hypnotic relaxation techniques; received grants from NIH. In addition, Dr Elvira V Lang has a patent Self Sedation System issued to Hypnalgesics.
References
1. Kain ZN, Mayes LC, Cicchetti DV, Bagnall AL, Finley JD, Hofstadter MB. The Yale preoperative anxiety scale: how does it compare with a “gold standard”? Anesth Analg. 1997;85(4):783–788. doi:10.1213/00000539-199710000-00012
2. Varughese AM, Nick TG, Gunter J, Wang Y, Kurth CD. Factors predictive of poor behavioral compliance during inhaled induction in children. Anesth Analg. 2008;107(2):413–421. doi:10.1213/ane.0b013e31817e616b
3. Yip P, Middleton P, Cyna AM, Carlyle AV. Non-pharmacological interventions for assisting the induction of anaesthesia in children. Cochrane Database Syst Rev. 2009;7(3):CD006447. doi:10.1002/14651858.CD006447.pub2
4. Manyande A, Cyna AM, Yip P, Chooi C, Middleton P. Non-pharmacological interventions for assisting the induction of anaesthesia in children. Cochrane Database Syst Rev. 2015;7:Cd006447. doi:10.1002/14651858.CD006447.pub3
5. Johnston M. Pre-operative emotional states and post-operative recovery. Adv Psychosom Med. 1986;15:1–22.
6. Kain ZN, Caldwell-Andrews AA, Maranets I, et al. Preoperative anxiety and emergence delirium and postoperative maladaptive behaviors. Anesth Analg. 2004;99(6):1648–1654, table of contents. doi:10.1213/01.ANE.0000136471.36680.97
7. Kain ZN, Mayes LC, O’Connor TZ, Cicchetti DV. Preoperative anxiety in children. Predictors and outcomes. Arch Pediatr Adolesc Med. 1996;150(12):1238–1245. doi:10.1001/archpedi.1996.02170370016002
8. Kain ZN, Mayes LC, Wang SM, Caramico LA, Hofstadter MB. Parental presence during induction of anesthesia versus sedative premedication: which intervention is more effective? Anesthesiology. 1998;89(5):1147–1156; discussion 1149A–1110A. doi:10.1097/00000542-199811000-00015
9. Beeby DG, Hughes JO. Behaviour of unsedated children in the anaesthetic room. Br J Anaesth. 1980;52(3):279–281. doi:10.1093/bja/52.3.279
10. Cray SH, Dixon JL, Heard CM, Selsby DS. Oral midazolam premedication for paediatric day case patients. Paediatr Anaesth. 1996;6(4):265–270. doi:10.1111/j.1460-9592.1996.tb00448.x
11. Amedro P, Gavotto A, Gelibert D, et al. Feasibility of clinical hypnosis for transesophageal echocardiography in children and adolescents. Eur J Cardiovasc Nurs. 2019;18(2):163–170. doi:10.1177/1474515118803513
12. Bischoff P, Rundshagen I. Awareness under general anesthesia. Dtsch Arztebl Int. 2011;108(1–2):1–7. doi:10.3238/arztebl.2011.0001
13. Schwender D, Klasing S, Faber-Züllig E, Pöppel E, Peter K. [Conscious and unconscious acoustic perception during general anesthesia]. Der Anaesthesist. 1991;40(11):583–593. German.
14. Sandin RH, Enlund G, Samuelsson P, Lennmarken C. Awareness during anaesthesia: a prospective case study. Lancet. 2000;355(9205):707–711. doi:10.1016/S0140-6736(99)11010-9
15. Ghoneim MM, Block RI, Haffarnan M, Mathews MJ. Awareness during anesthesia: risk factors, causes and sequelae: a review of reported cases in the literature. Anesth Analg. 2009;108(2):527–535. doi:10.1213/ane.0b013e318193c634
16. Davidson AJ. Awareness, dreaming and unconscious memory formation during anaesthesia in children. Best Pract Res Clin Anaesthesiol. 2007;21(3):415–429. doi:10.1016/j.bpa.2007.05.001
17. Nowak H, Zech N, Asmussen S, et al. Effect of therapeutic suggestions during general anaesthesia on postoperative pain and opioid use: multicentre randomised controlled trial. BMJ. 2020;371:m4284. doi:10.1136/bmj.m4284
18. Lang EV, Benotsch EG, Fick LJ, et al. Adjunctive non-pharmacological analgesia for invasive medical procedures: a randomised trial. Lancet. 2000;355(9214):1486–1490. doi:10.1016/S0140-6736(00)02162-0
19. Lang EV, Berbaum KS, Faintuch S, et al. Adjunctive self-hypnotic relaxation for outpatient medical procedures: a prospective randomized trial with women undergoing large core breast biopsy. Pain. 2006;126(1–3):155–164. doi:10.1016/j.pain.2006.06.035
20. Lang EV, Berbaum KS, Pauker SG, et al. Beneficial effects of hypnosis and adverse effects of empathic attention during percutaneous tumor treatment: when being nice does not suffice. J Vasc Interv Radiol. 2008;19(6):897–905. doi:10.1016/j.jvir.2008.01.027
21. Benotsch E, Lang EV, Lutgendorf S, Fick LJ. Preoperative anxiety and procedural pain, anxiety, and physiologic functioning. Ann Behav Med. 1998;209(S):92.
22. Ferreira-Valente MA, Pais-Ribeiro JL, Jensen MP. Validity of four pain intensity rating scales. Pain. 2011;152(10):2399–2404. doi:10.1016/j.pain.2011.07.005
23. Crandall M, Lammers C, Senders C, Savedra M, Braun JV. Initial validation of a numeric zero to ten scale to measure children’s state anxiety. Anesth Analg. 2007;105(5):1250–1253, table of contents. doi:10.1213/01.ane.0000284700.59088.8b
24. Lang EV, Hatsiopoulou O, Koch T, et al. Can words hurt? Patient-provider interactions during invasive procedures. Pain. 2005;114(1–2):303–309. doi:10.1016/j.pain.2004.12.028
25. Beringer RM, Greenwood R, Kilpatrick N. Development and validation of the pediatric anesthesia behavior score--an objective measure of behavior during induction of anesthesia. Paediatr Anaesth. 2014;24(2):196–200. doi:10.1111/pan.12259
26. Vagnoli L, Caprilli S, Messeri A. Parental presence, clowns or sedative premedication to treat preoperative anxiety in children: what could be the most promising option? Paediatr Anaesth. 2010;20(10):937–943. doi:10.1111/j.1460-9592.2010.03403.x
27. Wang SM, Maranets I, Weinberg ME, Caldwell-Andrews AA, Kain ZN. Parental auricular acupuncture as an adjunct for parental presence during induction of anesthesia. Anesthesiology. 2004;100(6):1399–1404. doi:10.1097/00000542-200406000-00011
28. Eijlers R, Dierckx B, Staals LM, et al. Virtual reality exposure before elective day care surgery to reduce anxiety and pain in children: a randomised controlled trial. Eur J Anaesthesiol. 2019;36(10):728–737. doi:10.1097/EJA.0000000000001059
29. Ryu JH, Park JW, Nahm FS, et al. The effect of gamification through a virtual reality on preoperative anxiety in pediatric patients undergoing general anesthesia: a prospective, randomized, and controlled trial. J Clin Med. 2018;7(9):284. doi:10.3390/jcm7090284
30. Jung MJ, Libaw JS, Ma K, Whitlock EL, Feiner JR, Sinskey JL. Pediatric distraction on induction of anesthesia with virtual reality and perioperative anxiolysis: a randomized controlled trial. Anesth Analg. 2021;132(3):798–806. doi:10.1213/ANE.0000000000005004
31. Calipel S, Lucas-Polomeni MM, Wodey E, Ecoffey C. Premedication in children: hypnosis versus midazolam. Paediatr Anaesth. 2005;15(4):275–281. doi:10.1111/j.1460-9592.2004.01514.x
32. Vagnoli L, Bettini A, Amore E, De Masi S, Messeri A. Relaxation-guided imagery reduces perioperative anxiety and pain in children: a randomized study. Eur J Pediatr. 2019;178(6):913–921. doi:10.1007/s00431-019-03376-x
33. Álvarez-García C, Yaban Z. The effects of preoperative guided imagery interventions on preoperative anxiety and postoperative pain: a meta-analysis. Complement Ther Clin Pract. 2020;38:101077. doi:10.1016/j.ctcp.2019.101077
34. Fortier MA, Weinberg M, Vitulano LA, Chorney JM, Martin SR, Kain ZN. Effects of therapeutic suggestion in children undergoing general anesthesia: a randomized controlled trial. Paediatr Anaesth. 2010;20(1):90–99. doi:10.1111/j.1460-9592.2009.03225.x
35. Duparc-Alegria N, Tiberghien K, Abdoul H, Dahmani S, Alberti C, Thiollier AF. Assessment of a short hypnosis in a paediatric operating room in reducing postoperative pain and anxiety: a randomised study. J Clin Nurs. 2018;27(1–2):86–91. doi:10.1111/jocn.13848
36. Ellingsen DM, Isenburg K, Jung C, et al. Dynamic brain-to-brain concordance and behavioral mirroring as a mechanism of the patient-clinician interaction. Sci Adv. 2020;6:43. doi:10.1126/sciadv.abc1304
37. Anzolin A, Isenburg K, Grahl A, et al. Patient-clinician brain response during clinical encounter and pain treatment. Annu Int Conf IEEE Eng Med Biol Soc. 2020;2020:1512–1515. doi:10.1109/EMBC44109.2020.9175608
38. Jensen KB, Petrovic P, Kerr CE, et al. Sharing pain and relief: neural correlates of physicians during treatment of patients. Mol Psychiatry. 2014;19(3):392–398. doi:10.1038/mp.2012.195
39. Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat Med. 2009;28(25):3083–3107. doi:10.1002/sim.3697
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Impact of Opioid Receptor Gene Polymorphism on Fentanyl and Alfentanil’s Analgesic Effects in the Pediatric Perioperative Period
Lilic J, Marjanovic VG, Budic I, Stefanovic N, Stokanovic D, Marjanovic GT, Jevtovic-Stoimenov T, Golubovic M, Zecevic M, Velickovic-Radovanovic R
Pharmacogenomics and Personalized Medicine 2024, 17:41-49
Published Date: 30 January 2024
Mapping Knowledge Landscapes and Evolving Trends of Clinical Hypnotherapy Practice: A Bibliometrics-Based Visualization Analysis
Zhao FY, Li L, Xu P, Kennedy GA, Zheng Z, Wang YM, Zhang WJ, Yue LP, Ho YS, Fu QQ, Conduit R
International Journal of General Medicine 2024, 17:5773-5792
Published Date: 4 December 2024
Enhancing Clinical Nursing Guidance and Optimizing Care Processes for Improved Hand-Foot-and-Mouth Disease Treatment Outcomes
Zhao Y, Ju H
Journal of Multidisciplinary Healthcare 2025, 18:3921-3931
Published Date: 9 July 2025