Back to Journals » Therapeutics and Clinical Risk Management » Volume 22
The ESINEA Study: A Novel Screening Tool for Identifying Patient Safety Incidents and Adverse Events in Hospitalized Patients–An Index-Date Cohort Evaluation
Authors Dueñas Lopez FC ![]() , Fernández-Arroyo García A, Rivera Núñez MA, Díaz-Pollán B, Sobrino Jiménez C, Murillo Gayo C, Mendieta Azcona C, Jiménez Núñez C, Yagüe de Antonio G, Narrillos Martín I
, Fernández-Arroyo García A, Rivera Núñez MA, Díaz-Pollán B, Sobrino Jiménez C, Murillo Gayo C, Mendieta Azcona C, Jiménez Núñez C, Yagüe de Antonio G, Narrillos Martín I ![]() , Guijarro Eguinoa J, Ojeda Feo JJ, González de la Viuda MA, Bautista Reina MDC, Fernández Velilla Peña M, Jiménez-Gonzalez M, Duque Alcorta M, Álvarez-Montero M
, Guijarro Eguinoa J, Ojeda Feo JJ, González de la Viuda MA, Bautista Reina MDC, Fernández Velilla Peña M, Jiménez-Gonzalez M, Duque Alcorta M, Álvarez-Montero M ![]() , González Muñoz M, Lorente Romeo M, Buitrago Sánchez NM
, González Muñoz M, Lorente Romeo M, Buitrago Sánchez NM ![]() , Rogozina O, López Ortego P, Pardo Puras R
, Rogozina O, López Ortego P, Pardo Puras R ![]() , Torres Santos Olmo RM, Iniesta Pérez S
, Torres Santos Olmo RM, Iniesta Pérez S ![]() , Chajma Izquierdo S, Martín López S, Del Rosal T
, Chajma Izquierdo S, Martín López S, Del Rosal T ![]() , Parra Ramírez P
, Parra Ramírez P ![]() , Villán Villán YF, Martín Vega A, Ramírez E
, Villán Villán YF, Martín Vega A, Ramírez E ![]()
Received 3 September 2025
Accepted for publication 16 March 2026
Published 20 May 2026 Volume 2026:22 565087
DOI https://doi.org/10.2147/TCRM.S565087
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Fiorela C Dueñas Lopez,1 Alba Fernández-Arroyo García,2 M Angélica Rivera Núñez,3 Beatriz Díaz-Pollán,4 Carmen Sobrino Jiménez,5 Concepción Murillo Gayo,6 Covadonga Mendieta Azcona,7 Cristina Jiménez Núñez,5 Gema Yagüe de Antonio,8 Inés Narrillos Martín,9 Javier Guijarro Eguinoa,1 José Jonay Ojeda Feo,10 María Asunción González de la Viuda,11 María del Carmen Bautista Reina,12 María Fernández Velilla Peña,13 María Jiménez-Gonzalez,14 Marta Duque Alcorta,15 Miguel Álvarez-Montero,1 Miguel González Muñoz,16 Miguel Lorente Romeo,17 Nelson M Buitrago Sánchez,18 Olga Rogozina,1 Paloma López Ortego,19 Ramón Pardo Puras,1 Rosario Maria Torres Santos Olmo,20 Silvia Iniesta Pérez,21 Susana Chajma Izquierdo,22 Susana Martín López,1 Teresa Del Rosal,23 Paola Parra Ramírez,24 Yuri Fabiola Villán Villán,25 Alberto Martín Vega,26 Elena Ramírez1
1Clinical Pharmacology Department, General Hospital, La Paz University Hospital-Idipaz, School of Medicine, Autonomous University of Madrid, Madrid, Spain; 2Hemato-Oncology Department, Children’s Hospital, La Paz University Hospital, Madrid, Spain; 3Patient Safety Unit, General Hospital, La Paz University Hospital, Madrid, Spain; 4Infectious Diseases Unit, Internal Medicine Department, General Hospital, La Paz University Hospital, Madrid, Spain; 5Hospital Pharmacy Department, General Hospital, La Paz University Hospital, Madrid, Spain; 6Geriatrics Department, General Hospital, La Paz University Hospital, Madrid, Spain; 7Angiology and Vascular Surgery Department, General Hospital, La Paz University Hospital, Madrid, Spain; 8Functional Area of Quality, General Hospital, La Paz University Hospital, Madrid, Spain; 9General Surgery Department, General Hospital, La Paz University Hospital, Madrid, Spain; 10Office of Sustainable Development and Agenda 2030, General Hospital, La Paz University Hospital, Madrid, Spain; 11Legal Department, General Hospital, La Paz University Hospital, Madrid, Spain; 12San José Pavilion, Cantoblanco Hospital, La Paz University Hospital, Madrid, Spain; 13Radiodiagnosis Department, General Hospital, La Paz University Hospital, Madrid, Spain; 14UCICEC (Analysis and Statistics Platform), General Hospital, La Paz University Hospital, Madrid, Spain; 15Clinical Analysis Department, General Hospital, La Paz University Hospital, Madrid, Spain; 16Immunology Department, General Hospital, La Paz University Hospital, Madrid, Spain; 17Information Technology Department, General Hospital, La Paz University Hospital, Madrid, Spain; 18Radiodiagnosis Department, Children’s Hospital, La Paz University Hospital, Madrid, Spain; 19Neonatology Department, Children’s Hospital, La Paz University Hospital, Madrid, Spain; 20Digital Strategy, and Innovation, General Hospital, La Paz University Hospital, Madrid, Spain; 21Gynecology Department, Maternity Hospital, La Paz University Hospital, Madrid, Spain; 22Rehabilitation Department, Carlos III Hospital, La Paz University Hospital, Madrid, Spain; 23Infectious Diseases Unit, Pediatrics Department, Children’s Hospital, La Paz University Hospital, Madrid, Spain; 24Endocrinology and Nutrition Department, General Hospital, La Paz University Hospital, Madrid, Spain; 25Preventive Medicine Department, General Hospital, La Paz University Hospital, Madrid, Spain; 26CSUR Coordination, General Hospital, La Paz University Hospital, Madrid, Spain
Correspondence: Alberto Martín Vega, Email [email protected] Elena Ramírez, Email [email protected]
Background: This study, ESINEA, investigated the period prevalence and characteristics of Patient Safety Incidents (PSIs) at La Paz University Hospital. PSIs were operationally defined as healthcare-related events with the potential to cause patient harm, including near misses, incidents, and adverse events (AEs) resulting in actual injury. Recognizing the critical importance of patient safety and the limitations of existing AE detection methods, the study aimed to improve identification and understanding of these incidents.
Methodology: An index-date inpatient cohort study was conducted, including all patients hospitalized at La Paz University Hospital on April 23rd, 2023 (n=870 episodes), with follow-up from admission to discharge. The methodology involved two phases: (i) electronic health records screening using a novel trigger-based tool, and (II) expert adjudication to confirm the PSIs and AEs, serving as the reference standard for tool validation.
Results: The population showed a high rate of urgent admissions (79%) and a predominance of older patients (75– 85 years old, 19.5%). Phase I identified at least one positive screening trigger in 58% of patients. Following expert adjudication, the period prevalence of PSI was 47.9% (95%CI: 45.16– 50.72), and AEs were confirmed in 27% (95% CI: 24.17– 30.06). Phase II confirmed that PSI accounted for 92.35% of the positive screening. The most frequent incidents occurred during “patient care and follow-up” (29.95%), followed by “Healthcare-Associated Infections” (17.21%). Vulnerability to PSI was significantly higher among older patients, those with longer hospital stays, and those with higher comorbidity burdens. Although 34.17% of PSIs were deemed preventable, slightly lower than the expected 40%;the analysis identified 88 distinct types of improvement actions to enhance patient safety.
Conclusion: The ESINEA study identified a high period prevalence of AEs (27%) in hospitalized patients, which is higher than the estimated 10% prevalence often cited. Although direct comparisons require caution due to differences in detection sensitivity and study design, these findings underscore the need for enhanced care coordination, infection prevention, and stricter protocol adherence, particularly among vulnerable populations.
Plain Language Summary: Why was this Study done?
Patient safety is a top priority in hospitals, but it can be difficult to get a clear picture of how often harmful incidents happen. We conducted this study because the usual methods for finding these incidents, known as Adverse Events, often miss important information. Our goal was to use a new, more accurate tool to better understand the true rate of these events and find ways to prevent them.
What did the Researchers do and find?
Our team at La Paz University Hospital reviewed the medical records of 870 hospitalized patients. We discovered that 27% of patients experienced at least one Adverse Event. This is much higher than the widely used estimate of 10%. Most of these incidents were related to general patient care and follow-up or were infections acquired in the hospital. We also found that older adults and people with longer hospital stays or multiple health conditions faced a higher risk. Importantly, more than a third of all incidents could have been prevented.
What do these Results mean?
These findings show that preventable harm in hospitals is a larger problem than previously thought. Our results highlight a clear need for hospitals to improve patient care coordination, strengthen infection prevention, and ensure clinical guidelines are strictly followed. By doing this, we can make hospital stays safer for everyone, especially for our most vulnerable patients.
Keywords: adverse events, epidemiology, incidents, patient safety, patient safety incidents, preventability, patient safety culture, improvement actions, hospital setting, surveillance
Introduction
Patient Safety Incident (PSIs) are a variety of healthcare-related events that might cause patient damage. These include near misses (incidents or circumstances in which an error or potential hazard is detected before reaching the patient, preventing injury), incidents (where an event occurs that could have caused harm but does not, due to chance or intervention), and adverse events (AEs). Patient safety is defined as “the absence of preventable harm to a patient and reduction of risk of unnecessary harm associated with health care to an acceptable minimum”. Within the broader health system context, it is “a framework of organized activities that creates cultures, processes, procedures, behaviors, technologies and environments in health care that consistently and sustainably lower risks, reduce the occurrence of avoidable harm, make error less likely and reduce impact of harm when it does occur.1
Adverse events related to hazardous care are a major public health concern, accounting for one of the top ten causes of death and disability worldwide. According to the World Health Organization, nearly one in every ten patients is harmed in a healthcare setting, resulting in more than three million deaths annually. 1 More than half of the harm (one out of every 20 patients) is preventable in Organization for Economic Co-operation and Development countries, AEs account for a significant part (15%) of total hospital activity and expenditures.1,2
A 2008 systematic review found out that hospitalization-related adverse events occurred at an average rate of 9.2%, with 43.5% potentially preventable Of the adverse events observed, 7.4% could be directly related to the patient’s mortality, while 7% could cause lifelong disability.3 These figures may be underestimated because the data was collected using a two-stage retrospective record review technique involving trained nurses and physicians, a method known to have limitations in identifying all events, and because many studies exclude adverse events that occur after discharge. It is also known that detection methods like voluntary reporting (used for comparison in a minority of studies within this review) typically underestimate AE rates. More recent data is required to accurately represent the current situation.
In Spain, the Ministry of Health, commissioned many studies to investigate the scope and determinants of healthcare-associated risks. These include the ENEAS study4 which reported a 9.3% incidence of AEs, with 42.8% considered preventable; SYREC study,5 which detected a 33.8% AE rate; and ESHMAD study,6 which found an 11.9% prevalence of AEs. These findings illustrate the important need for initiatives that improve patient safety in healthcare settings.
The optimal epidemiological approach for investigating AEs is determined by the research aims, which must strike a balance between bias minimization and AE identification validity. While national studies frequently rely on retrospective designs -often limited by variable clinical record quality- and prospective studies offer high reliability at a significant resource-cost, this study utilizes an index-date inpatient cohort design.
Unlike a strictly cross-sectional prevalence study, which may be susceptible to survival bias and underrepresent short-lived events,7 our approach identified all patients hospitalized on a specific reference date (April 23, 2023) and followed their entire clinical course from admission to discharge. This design ensures a comprehensive longitudinal view of each hospitalization episode while maintaining the efficiency of point-in-time sampling.
Detection was supported by a novel, pre-defined screening tool designed to identify a broad spectrum of potential PSIs, thereby enhancing the detection of AEs. The objective was to identify priority issues in patient safety, to study the characteristics, and distribution of PSIs, and to evaluate the diagnostic yield of the screening tool. By analyzing each hospitalization episode within the index-date cohort from admission to discharge, these findings provide a granular evidence base to develop targeted preventive strategies, minimize the impact of incidents and ultimately enhance patient safety at La Paz University Hospital.
Existing trigger-based tools, such as the Global Trigger Tool, have demonstrated utility for adverse event surveillance but are limited by dependence on documentation, high false-positive rates, and variability in reviewer interpretation. The ESINEA approach was developed to address these limitations through an integrated design that combines an adapted trigger set tailored to the local electronic health record, a structured two-step data collection and analysis notebook, and a three-phase workflow embedded within hospital patient safety structures. Key features include standardized training of reviewers, participation of Functional Risk Management Unit and Patient Safety Officer collaborators, and consensus-based expert adjudication of screened cases. Together, these elements aim to improve detection sensitivity while enhancing specificity, interpretability, and practical applicability for institutional patient safety improvement.
Materials and Methods
Hypothesis and Objectives
This study hypothesizes that at least 10% of hospitalized patients may experience AEs, with at least 40% being preventable. The main objective was to identify priority areas and issues regarding patient safety in order to improve the safety culture at La Paz University Hospital. Specific objectives included determining the period prevalence of patients experiencing PSIs, describing the characteristics of the most common PSIs; assessing the preventability of identified AEs; analyzing the distribution of AEs among various healthcare departments; and examining patient attributes linked to AEs.
Design
This observational study used an index-date inpatient cohort design with follow-up through discharge. All patients with an active hospitalization episode at La Paz University Hospital on April 23rd, 2023 were included and retrospectively reviewed from admission to discharge to identify Patients Safety Incidents (PSIs). This design allows estimations of PSI and AE period prevalence while capturing events occurring throughout the hospitalization episode. All patients admitted to the selected units, regardless of admission cause, were included and screened for potential PSIs. The study protocol was approved by the Ethics Committee of La Paz University Hospital (ID: PI-5266. February 9, 2023), which also waived the requirement for informed consent given the study’s retrospective design. All patient data were anonymized prior to analysis, and the study was conducted in accordance with the principles of the Declaration of Helsinki.
Selection Criteria
Study Variables
This study investigates the impact of several independent variables, categorized as: patient-related factors (age and sex); healthcare elements (type of admission, medical specialty, length of stay); and disease or procedure specifics (primary diagnosis using ICD-9-CM/ICD-10-CM codes, American Society of Anesthesiologists (ASA) classification, Charlson Index). Additionally, it examines variables detailing the impact of an Adverse Event (AE), including any AE-induced extended stay, the difference in stay length with and without an AE, additional resulting procedures or treatments, and the specific phase of the care process (from organizational management to patient follow-up, identified by a binary Yes/No indicator) where the AE occurred.
The study considered three dependent variables: near misses, incidents, and AEs.
Instruments
a) Screening form: Episodes meeting at least one predefined trigger were considered positive screenings and advanced to Phase II. The complete list of triggers, definitions, and decision rules used in the screening process is provided in Supplementary Materials 1. The screening Form consists of seven modules:
- M1: Previous hospitalization
- M2: Care-related incidents
- M3: Healthcare-associated infections (HAIs)
- M4: Medication-related incidents
- M5: Treatment-related incidents
- M6: Test-related incidents
- M7: Diagnosis-related incidents
b) The two-step Data Collection Notebook software application: first, PSI registration records incident details like location, healthcare process phase, impact type, evolution, severity, frequency, detectability, potential remedies, preventability, and prevention methods. Second, Incident and AE Analysis and Improvement Actions, cover analysis methodology, process steps, actions taken, outcomes, and categories (Supplementary Materials 2).
Sample Size Calculation
The sample size was equal to the total population of hospitalized patients during the study period.
Data Collection
The HCIS (Hospital Clinical Information System) provides data for the ESINEA network database. Demographic, disease and procedure information came from the Spanish National Hospital Discharge Data Set (CMBD), coded according to ICD-9-CM/ICD-10-CM codes. ASA (American Society of Anesthesiologists) classifications were obtained from the HCIS export.
Data Analysis
A descriptive and associational analysis of the variables was performed. Proportions were estimated for qualitative variables, while measures of central tendency and dispersion were utilized for quantitative variables. The age categorization follows the World Health Organization (WHO) Life Stage Classification. The Charlson Comorbidity Index was calculated according to the methodology of Sundararajan et al (2002),8 which adapts the Charlson Comorbidity Index calculation methodology from ICD-9-CM to ICD-10-CM.
The modified Wald method was used to compute the 95% confidence interval for prevalence (see https://www.graphpad.com/quickcalcs/ConfInterval1.cfm). The sensitivity, specificity, and predictive values of the screening instrument were calculated. A univariate analysis of independent and dependent variables, as well as logistic regression, were carried out using R Studio Version 2024.04.1+748 (2024.04.1+748). For the analysis, three independent variables were considered: “Length of Stay”, “Charlson Comorbidity Index”, and “ASA Physical Status Classification”. Missing data were most relevant for ASA physical status classification, which was not documented for a subset of episodes. Given that ASA recording is influenced by clinical and procedural documentation practices, missingness was considered likely related to documentation processes rather than outcomes alone. To minimize loss of information, missing ASA values were handled using a single imputation approach based on available clinical and procedural information recorded in the electronic health record, preserving the original ASA category structure. The imputation strategy was applied only to ASA and was used for multivariable modelling. As a sensitivity analysis, multivariable models were re-estimated excluding ASA, and the direction and magnitude of associations for the remaining covariates were unchanged.
Length of stay (LOS) was analyzed as an exposure-time proxy and association variable rather than a causal predictor, acknowledging that PSIs and AEs may both contribute to and result from prolonged hospitalization.
Procedure
The information collection procedure was divided into three phases, detailed in Figure 1, and included six steps leading to the final report. Collaborators from the Functional Risk Management Unit (FRMU) or Patient Safety Officers (PSOs) at the hospital participated in each step.
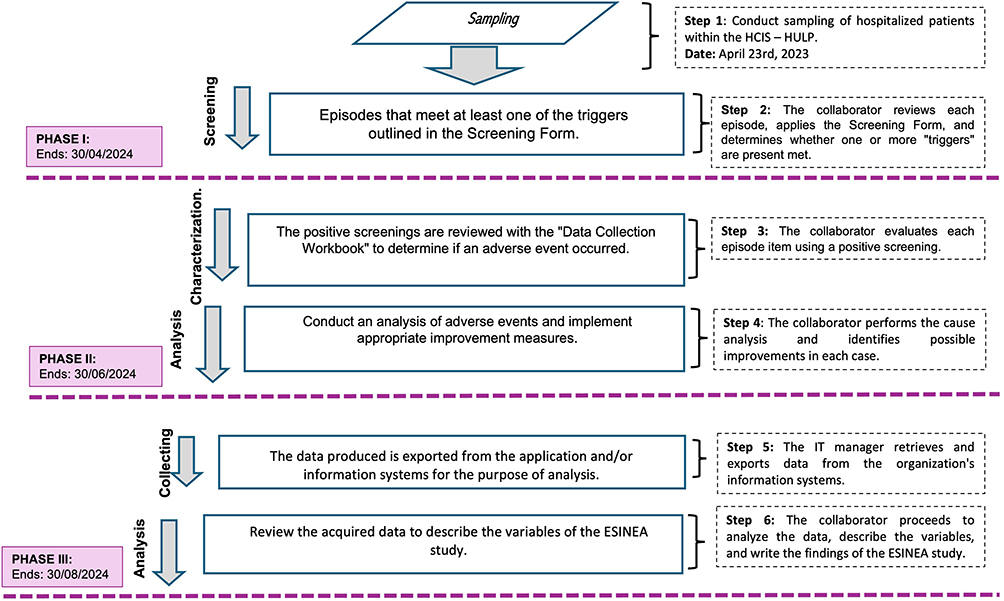 |
Figure 1 A three-phase, 6-step workflow was developed for sample selection, screening, PSI characterization, AE analysis, data collection, and final report preparation. Note: Purple boxes indicate the three study phases; bold text identifies key process actions (Sampling, Screening, Analysis); and italics denote initial sampling steps. |
In Phase I, collaborators completed the screening forms by reviewing electronic medical records associated with randomly assigned hospitalization episodes. During Phase II, all positive screenings were evaluated by a panel of experts experienced in patient safety incidents and adverse event analysis, as well as in the implementation of improvement actions within the FRMU or PSO. Each positive screening was independently assessed by a minimum of two patient safety specialists, with any disagreements resolved through consensus discussion. Confirmed Patient Safety Incidents (PSIs) and Adverse Events (AEs) resulting from this adjudication process were regarded as the reference standard for assessing the performance of the screening tool. Performance metrics including sensitivity, specificity, positive predictive value, and negative predictive value were calculated by comparing the screening results from Phase I with the adjudication outcomes in Phase II. Moreover, the expert panel conducted a comprehensive analysis of confirmed PSIs and recommended corresponding improvement actions. Phase II concluded at the point of patient discharge. Finally, in Phase III, all collected data were integrated to produce the final study report.
The performance of the screening tool was assessed utilizing expert adjudication outcomes from Phase II as the reference standard. Results from Phase I screening were compared to Phase II-confirmed Patient Safety Incidents (PSIs) and Adverse Events (AEs) to evaluate the tool’s capacity to accurately identify true events. Sensitivity was defined as the proportion of confirmed PSIs/AEs correctly identified by at least one positive screening trigger during Phase I. Specificity was characterized as the proportion of hospitalization episodes lacking confirmed PSIs/AEs that did not exhibit any positive screening triggers. The positive predictive value (PPV) denoted the proportion of positive Phase I screenings subsequently confirmed as PSIs/AEs during expert adjudication, whereas the negative predictive value (NPV) indicated the proportion of negative screenings verified as absence of PSIs/AEs. These metrics were computed at the level of hospitalization episodes by directly comparing Phase I screening outcomes with Phase II adjudication results. This methodology permitted the evaluation of the screening tool’s performance within the framework of routine clinical documentation and expert review.
A full confusion matrix is not presented, as all performance metrics were derived directly from the episode-level comparison between Phase I screening outcomes and Phase II expert adjudication results.
Results
On April 23rd, 2023, 882 patient admissions episodes were recorded. Four Home Hospitalization patients were excluded for not meeting hospitalization criteria. Additionally, eight episodes from the Pediatric Intensive Care Medicine were excluded because, in this department, medical records were primarily recorded on paper format rather than in the HCIS. Period prevalence estimates are documented at the patient level, whereas counts of PSIs and AEs represent the event-level burden; individual patients may experience multiple events within a single hospitalization. Of the 870 episodes finally included, 58% (504 patients) had a positive screening, with an average of 2.51 positive screenings per patient. Of these positive screenings, 92.35% (1232) corresponded to PSIs, of which 48.9% (603 adverse events in 235 patients) were classified as AEs, with 36.5% deemed preventable.
The period prevalence of PSIs among the patients in the study was 47.9% (417/870) [95% CI 45.16% - 50.72%], of which 27% (235/870) were AEs [95% CI 24.17%-30.06%]. The flowchart of the study is presented in Figure 2.
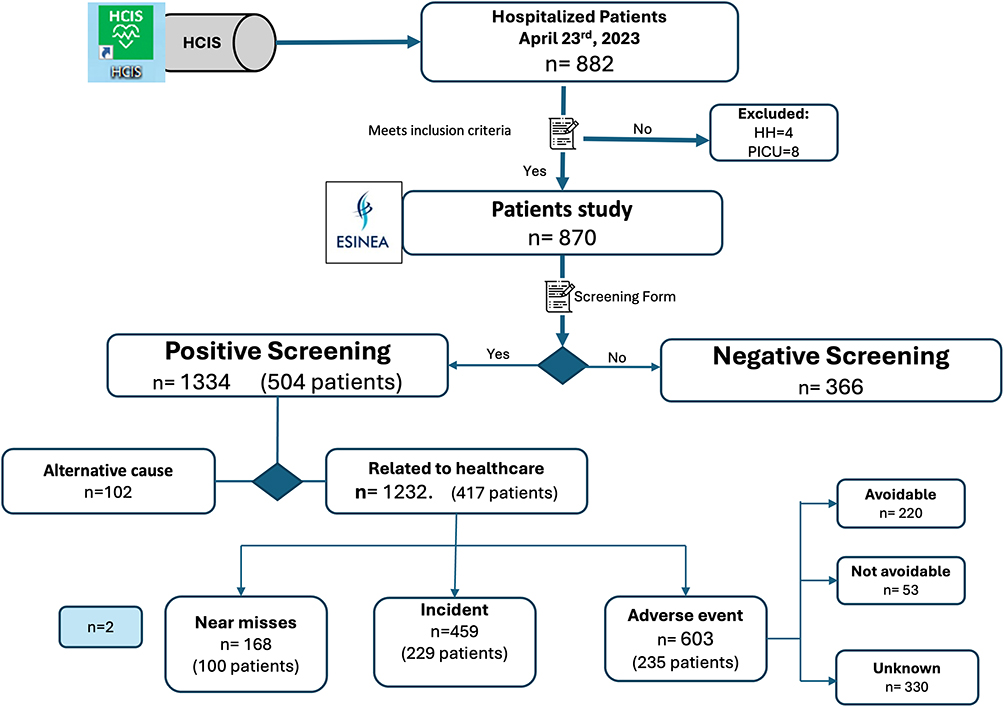 |
Figure 2 ESINEA 2023’s Flowchart. Notes: Bold text identifies the primary patient cohorts and final adjudication outcomes (Adverse Event, Incident); arrows indicate the progression of the review protocol. |
Sample Characteristics
Sex distribution was about equal, with 49% (428) males and 51% (442) females. Older adults (>65 years) made up the majority of patients (53%), followed by adults (25–64 years) (29%), pediatric patients (<18 years) (16%), and young adults (18–25 years) (2%). Within the older adult group, the subgroup aged 75–85 was the most representative, accounting for 19.5%. The median age was 67 years, with a mean age of 61.2 years (Supplementary Material, Figure S1).
Among the 870 patients, the most common ICD-10 diagnoses were “Diseases of the circulatory system” with 140 patients (16%) and “Diseases of the respiratory system” with 110 patients (12.6%) (Supplementary Tables S1 and S2).
The distribution of episodes across the five centers, from smallest to largest, was as follows: 76 episodes (8.74%) in Hospital Carlos III, 82 episodes (9.43%) in the Children’s Hospital, 90 episodes (10.34%) in the Maternity Hospital, 110 episodes (12.64%) in Cantoblanco, and 512 episodes (58.85%) in the General Hospital. The most common admission type was urgent, representing 79% of all episodes. Scheduled admissions accounted up 19% of the sample, with admissions following outpatient procedures accounting for the remaining 2%.
Most of the hospital stays (33.45%) lasted between 11 and 30 days (291 cases). This was followed by shorter stays of 0 to 5 days, which represented 21.26% of the total (Supplementary Material, Figure S2). The most common discharge category was “discharge without follow-up”, representing 87.36% of the total. This was followed by “discharge due to death” (6.09%) and “transfer to another hospital” (3.68%).
The 870 hospitalization episodes were distributed across 31 departments: Internal Medicine was the predominant department with 20.80% (181/870) of the episodes, followed by Pulmonology with 7.59% (66/870), Intensive Care Medicine with 6.90% (60/870), Geriatrics with 6.09% (53/870), Pediatrics with 5.86% (51/870), and General and Digestive Surgery with 5.86% (51/870) of the episodes (Supplementary Material, Figure S3).
PHASE I. Screening Results
Of the 870 patients evaluated, 42% (366 patients) had a negative screening, while the remaining 58% (504 patients) had at least one positive “trigger” in the screening. Figure 3a shows the distribution of triggers by module. The “M2 - Associated with Care” module concentrated the highest number of triggers (36.3%, 584), followed by “M3 - Associated with Healthcare-Related Infections” (18.8%, 304) and “M1 - Previous Hospitalization” (17.4%, 281). These three modules represented 72.5% of the total triggers identified. Among the 504 episodes with positive screening, 1334 triggers were identified. Figure 3b shows that the Internal Medicine, Intensive Care Medicine, and Cardiology departments concentrated the highest number of positive screenings.
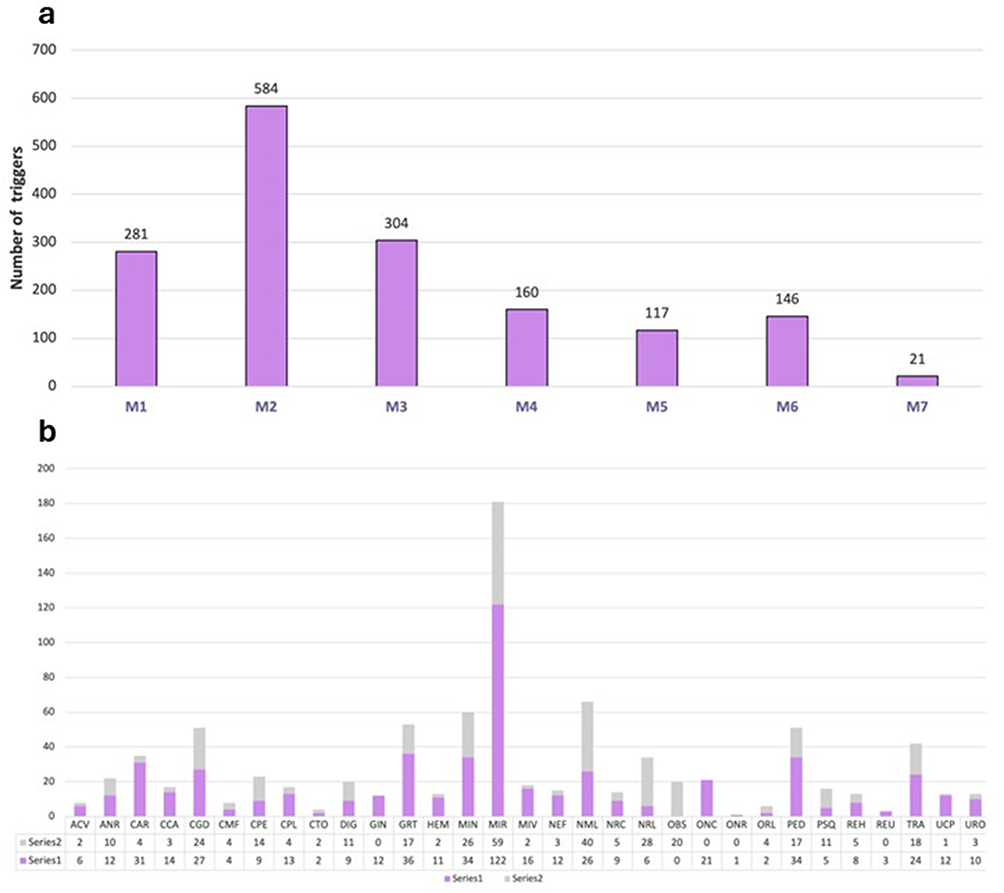 |
Figure 3 (a) Distribution of positive screenings by modules. (b) Distribution of positive and negative screenings by specialty. Notes: M1–M7 in bold represent the specific tool modules. In chart (b), purple bars (Series 1) represent positive screenings and gray bars (Series 2) represent negative screenings. |
Screening Tool Validation
The screening tool showed a sensitivity of 98.13% (95% CI 97.29–98.77), specificity of 76.87% (95% CI 72.71–80.57), and a positive predictive value (PPV) of 92.22% (95% CI 90.61–95.77) for a period prevalence of 72.27% (95% CI 70.07–74.36). The negative predictive value (NPV) was 72.27% (95% CI 70.07–74.36).
PHASE II. PSIs
Demographic Characteristics of Patients and the Distribution of PSIs
A total of 1232 PSIs were identified in 417 individuals. The gender distribution among these patients was balanced, with 202 (48.4%) females and 215 (51.6%) males. The median age was 70 years, while the mean age was 63.15 years, suggesting a slight skew toward older age groups. This is further supported by the fact that the largest proportion of patients, 91 (21.8%), fell into the “Older Adult 75–85 years” category. This highlights the period prevalence of PSIs among older individuals.
The most frequent length of hospital stay among the 417 patients was “11 to 30 days”, accounting for 156 patients (37.4%), followed by “31 to 100 days” with 118 patients (28.3%). When considering 1232 PSIs, the most common duration shifted to 31 to 100 days (490 cases, 39.8%), followed by 11 to 30 days (368 cases, 29.9%).
The most frequent patient profile associated with PSIs was elderly persons aged 75 to 85 years, implying that this age group may be more vulnerable to experiencing AEs during hospitalization. Furthermore, PSIs increased significantly (p<0.001) throughout hospital stays lasting between 31–100 days. This data emphasizes the higher risk of PSIs associated with long-term hospital stays and the need for heightened vigilance and targeted interventions to enhance patient safety, particularly among older patients.
The Charlson Comorbidity Index, which correlates comorbidity burden with long-term mortality risk, was used to categorize patients. A score of 0–1 indicates no significant comorbidity, a score of 2 represents low comorbidity, and a score of 3 or higher signifies substantial comorbidity. In this study, an analysis of the Charlson Index in relation to PSIs revealed that 47.8% (589 cases) had no comorbidity, 21.9% (270 cases) had mild comorbidity, and 30.1% (371 cases) exhibited high comorbidity. While most cases (47.8%) did not have significant comorbidities, a notable proportion (30.1%) presented with high comorbidity burdens (Figure 4a). This distribution underscores the importance of considering comorbidity in the evaluation and management of patients, as it may influence the risk of PSIs and overall patients’ outcomes.
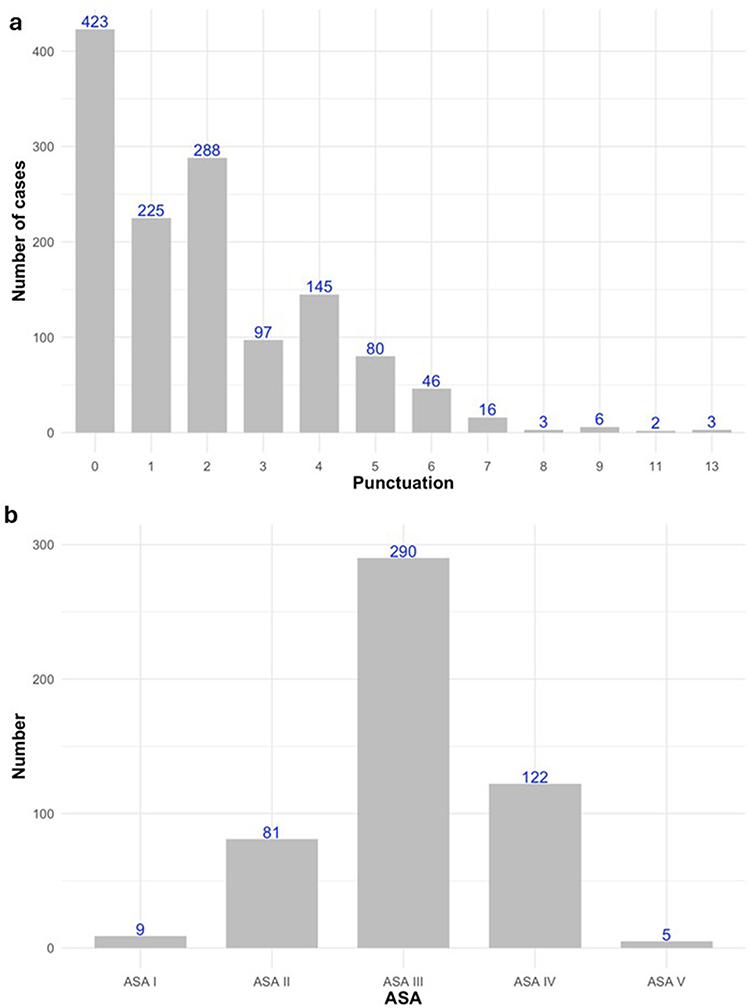 |
Figure 4 (a) The distribution according to Charlson Comorbidity Index among the PSIs. (b)The distribution of ASA classifications among the PSIs. Note: Blue numbers above the bars indicate the exact case count for each category; bold text on the axes identifies the classification variables (Punctuation, ASA). |
A total of 719 surgical interventions were performed on 174 patients with PSIs, with a maximum of 9 surgeries per patient, reflecting both the frequency and complexity of these procedures. Of these 719 surgeries, the ASA scale had been exported from HCIS for 472. However, ASA assessments were missing for 247 of the surgical interventions. This inconsistency in documentation may warrant a review of the information system to ensure quality information for all surgical patients. The distribution of ASA classifications among the PSIs is shown in Figure 4b.
Characteristics of PSI
Type
According to the type of the incident, 13.64% (168 cases) of the events were near-misses, 37.26% (459 cases) were incidents, and (603) 48.94% were AEs. Two patient safety-related incidents were not classified.
Phase of Care
Five phases accounted for approximately 80% of the identified PSIs. “Patient Care and Follow-up” emerged as the phase with the highest number of PSIs (369 cases, representing 29.95% of the total), followed by the “Healthcare-Related Infection” (212 cases, 17.21%) and “Therapeutic Procedures” (166 cases, 13.47%). Notably, “Medication and Vaccines” (134 cases, 10.88%) and “Surgical Procedures” (105 cases, 8.52%) also accounted for a substantial proportion of PSIs. Figure 5a illustrates the distribution of PSIs across phases of the healthcare process.
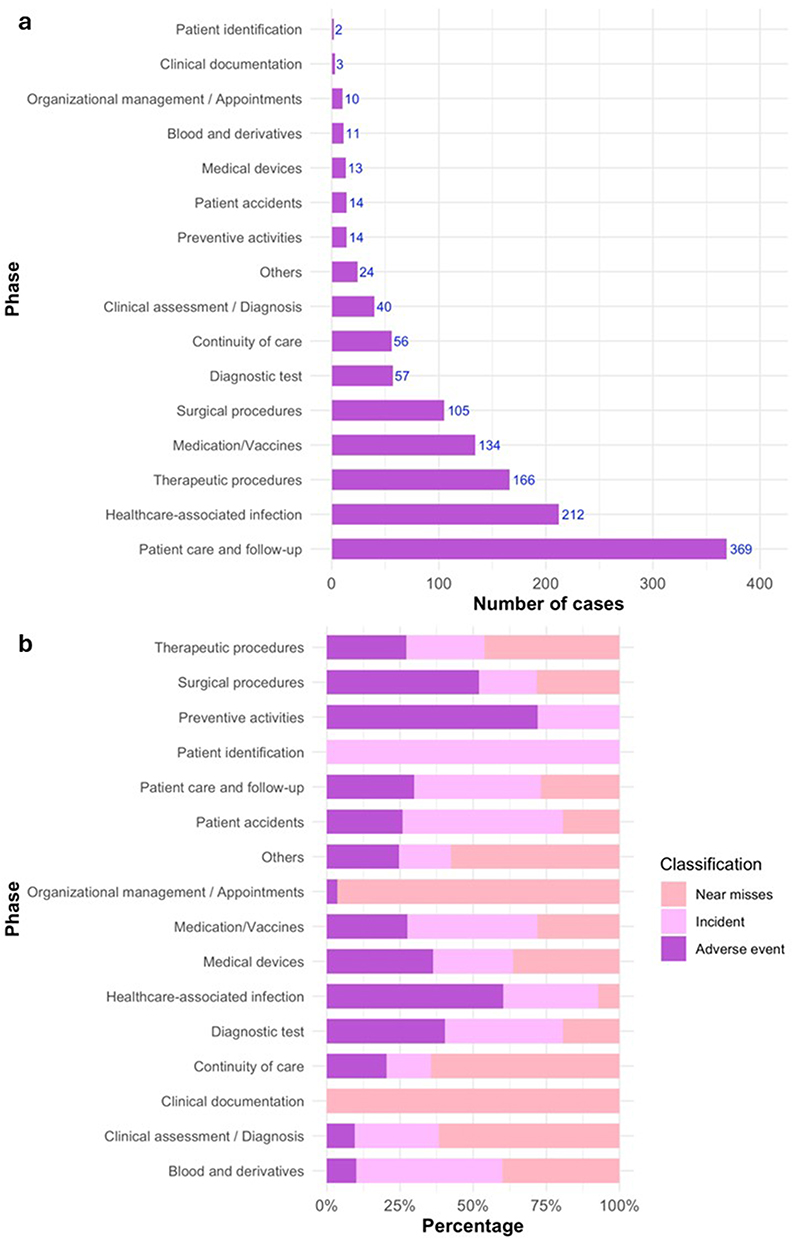 |
Figure 5 (a) Distribution of PSIs across phases of the healthcare process. (b) Distribution of PSI type according to the event phase. Notes: Bold text is used to highlight the critical phases of care where incidents are concentrated; colors distinguish the types of incidents (Near misses, Incidents, Adverse Events) to facilitate visual comparison. |
In the analysis of PSIs, the following distribution type was observed:
- AE: The majority of AE (n=304) occurred during the “Patient care and follow-up” and “Healthcare-associated infection” phases, representing around 50% of the overall total.
- Incidents: The “Patient care and follow-up” phase had the greatest incidents, with 173 (38%). It is followed by three phases, which account 39% of all incidents: “Healthcare-associated infection”, “Medication and vaccines” and “Therapeutic procedures”.
- Near misses: 95 near misses occurred in the “Patient care and follow-up”, “Therapeutic procedures” and “Continuity of care” phases, representing 56% of the total.
These findings identify certain areas where interventions and preventive actions may be particularly crucial for enhancing patient safety. Figure 5b shows the distribution of PSI type according to the event phase.
Departments
The distribution of PSIs by hospital discharge department revealed that the four most common departments were: Internal Medicine with 234 cases (19.0%), Cardiology with 190 cases (15.4%), Intensive Medicine with 78 cases (6.3%), and Hematology with 67 cases (5.4%) (Supplementary Material Figure S4a illustrates the number of PSIs across hospital discharge department).
The following departments exhibited AEs rates (n≥10) exceeding 50%, ordered from highest to lowest rate: Pediatric (PED) (31/34 = 91.2%), Hematology (51/67 = 76.1%), Psychiatry (PSQ) (7/10 = 70%), Angiology and Vascular Surgery (9/13 = 69.2%), Anesthesiology (16/26 = 61.5%), Neurology (20/34 = 58.8%), Neurosurgery (17/32 = 53.1%), Internal Medicine (119/234 = 51.07%), Pulmonology (27/53 = 50.9%), Intensive Medicine (10/20 = 50%) (Supplementary Material Figure S4b shows PSI type across departments).
Preventability
Preventability was unknown in 53.2% of the cases. However, in 34.2% of the cases, PSIs may have been avoided, suggesting potential for improving patient safety. In the case of AEs, the preventability rate exceeds 50%.
Severity, Frequency, Detectability, Feasibility of Solution, and Information Level
The distribution of the severity of PSIs was as follows: 41.64% were classified as “moderate”, 19.64% as “severe”, and 6.98% as “very severe”. Notably, over 50% of those classified under “severe” or “very severe” were AEs.
According to the frequency of incidents, it was estimated that 40.34% occurred on a “weekly” basis, followed by 25.08% with a “monthly” frequency, and 14.12% occurring “annually”. The highest percentage of AEs occurred “monthly”.
Most PSIs (90.42%) were detectable, with “Always” (45.78%) and “In many cases” (44.64%) being the most frequent categories. Most AEs were primarily concentrated in the “In many cases” detectability category.
The analysis of PSIs solutions feasibility revealed that 51.79% were considered “feasible with difficulties”, 23.86% “highly feasible”, and 23.86% “unlikely to be feasible”. Most of AEs were classed as “feasible with difficulties”, suggesting a possible correlation between the complexity of the solution and the occurrence of AEs.
Information regarding the level of communication about PSIs (to patients, families, and colleagues) was unavailable in over 50% of cases, limiting the understanding of communication practices and subsequent actions taken in response to these incidents. Despite the limitations in documentation, it was noted that the PSI was communicated to staff in 30% of cases, and to patients or family members in 60%.
Data Analysis
Patients with PSIs had an average stay of 53.75 days ± 50.60, significantly longer than those without a PSI, who stayed 24.05 days ± 37.24. This difference was statistically significant (p < 0.001), indicating a strong association between PSIs and extended hospital stays.
Similarly, the analysis of the “Charlson Comorbidity Index” showed a statistically significant difference between the two groups. Patients with a PSI had a higher average Charlson index score (1.98 ± 2.01) compared to those without a PSI (1.47 ± 1.84), indicating a greater burden of comorbidity. This difference was also highly significant (p < 0.001).
The ASA classification analysis showed that patients with a PSI had a higher average ASA score (2.90 ± 0.80) than those without a PSI (2.62 ± 0.89), suggesting an increased anesthetic risk and more complex medical conditions. This difference was also highly significant (p < 0.001).
A multivariable logistic regression model assessed the relationship between Length of Stay, Charlson Comorbidity Index, ASA classification, and the presence of at least one PSI. Each additional day in hospital increases the probability of a PSI by 1% (OR = 1.01, 95% CI: 1.01–1.02, p < 0.001). Each point increase in the Charlson Comorbidity Index, raises the PSI risk by 18% (OR = 1.18, 95% CI: 1.08–1.31, p < 0.001). Likewise, a point increase in the ASA classification boosts the likelihood of a PSI by 33% (OR = 1.33, 95% CI: 1.09–1.62, p = 0.006).
Analysis and Improvement Actions
The expert team carried out a comprehensive review of the 885 identified PSIs (ESINEA cases) across various hospital phases, excluding the Children´s Hospital, which was analyzed as a single block. A total of 451 improvement actions were proposed, categorized into 88 distinct types of interventions. These actions were designed to address the root causes of the incidents and prevent their recurrence by implementing strategies aimed at enhancing patient safety (Supplementary Table S3).
Discussion
The ESINEA study, conducted across five hospitalization centers of La Paz University Hospital, provided a comprehensive characterization of PSIs, highlighting the current state of patient safety and identifying areas for improvement to mitigate PSI impacts. Additionally, the study involved 32 healthcare professionals from diverse fields, training them in key aspects of PSI identification and systematic analysis.
While longitudinal incidence studies are often lengthy and costly, requiring detailed analysis of each patient episode.4,9 Traditional cross-sectional prevalence studies -though more efficient for characterization- may be susceptible to survival bias and often produce high rates of false positives.10,11 To mitigate these limitations, such studies often employ structured clinical review forms to clarify the review process and provide a more robust AE analysis.12
In this context, our research utilized an index-date inpatient cohort design. This approach allowed for the estimation of period prevalence by analyzing each hospitalization episode from admission to discharge, effectively combining the efficiency of point-in-time sampling with the robustness of longitudinal follow-up. To further minimize documentation dependence and interpretation variability, ESINEA implemented these structured forms within a rigorous two-step adjudication process. Trigger-based review is a well-established approach for identifying AEs and monitoring patient safety over time. The Institute for Healthcare Improvement (IHI) Global Trigger Tool (GTT) is a well-known tool for this purpose,11 with high sensitivity rates—80% for Internal Medicine and 90% for General Surgery, making it suitable for use as a screening system. The tool’s Positive Predictive Value (PPV) is 40%, while its Negative Predictive Value (NPV) is 50%. However, these values can vary significantly depending on the prevalence of AEs in different patient populations.13,14 The ESINEA study’s novel screening tool, adapted from GTT, shows high efficiency with 98.13% sensitivity (95% CI: 97.20–98.77) and 92.22% PPV (95% CI: 90.64–93.55). This tool accurately identifies AEs. By collaborating with diverse healthcare professionals with a rigorous index-date inpatient cohort design, ESINEA has analyzed the period prevalence, characteristics, and causes of AEs, yielding internationally comparable results.
Compared to ESHMAD study (2019),6 ESINEA demonstrated a higher rate of positive screenings (58% vs. 36.6%), and a greater average of positive items per patient (2.51 vs. 1.9). ESINEA’s screening tool also exhibited substantially higher sensitivity (98.13% vs. 48%). Although La Paz University Hospital data within ESHMAD showed similar positive screenings rate to ESINEA (41.7%), ESINEA false positive rate was considerably lower (7.7% vs. 61.9%).
The ESHMAD study reported a 15.7% prevalence of AEs and a 1.3% prevalence of incidents (events with potential for harm) at La Paz University Hospital. The ESINEA study found a substantially higher AEs prevalence of 27%, The AE period prevalence observed in ESINEA study was higher than commonly cited estimates in the literature. However, direct comparisons should be interpreted with caution, as differences in study design, operational definitions, and case-finding intensity can substantially influence observed rates. Both studies identified “Therapeutic procedures” as the third most frequent event phase of occurrence, but ESHMAD reported “Healthcare-associated infections (HAIs)” as most common (31.8%), whereas “Care and follow-up” events predominated in ESINEA (29.95%). ESINEA also observed a broader distribution of AEs across care phases, suggesting differences in risk profiles between the studies. This highlights the need for standardized and sensitive detection tools for a better understanding of AE incidence and characteristics.
ESINEA identified that 20.5% of AEs occurred during the “Healthcare-Associated Infections (HAIs)” phase, with nosocomial pneumonia and urinary tract infections (UTIs) being the most frequent. This aligns with the EPINE 2023 study, an annual cross-sectional prevalence study of healthcare-associated infections, which reported a 9.13% (84/920) HAI prevalence. Respiratory infections, including pneumonia and lower respiratory tract infections, were the most common infections in the EPINE study.15
Several methodological considerations warrant explicit discussion. The index-date inpatient cohort design, while efficient for surveillance, may introduce day-of-week or seasonal bias and is dependent on the completeness and quality of clinical documentation. In addition, although expert adjudication was performed using standardized procedures and consensus review, some degree of heterogeneity among reviewers is inherent to incident analysis methodologies. These factors were mitigated through structured review tools, standardized training, and consensus-based adjudication but should be considered when interpreting the findings.
Associations identified between patient characteristics and the occurrence of PSIs particularly length of hospital stay should be interpreted cautiously. Length of stay likely reflects both increased exposure time and underlying clinical complexity and may act as both a contributor to and a consequence of patient safety incidents. Accordingly, results are presented as associations rather than implying causal directionality.
Since 2014, La Paz University Hospital implemented the SINOIRES (System for Reporting Patient Safety Incidents),16 a confidential, anonymous, and non-punitive system designed to report PSIs. SINOIRES was based on principles of non-punitivity, confidentiality for patients and involved professionals, independent expert analysis, and timely feedback, with explicit management support. The 2023 SINOIRES report (internal data), which recorded 1145 PSIs, showed a distribution of reports across hospital areas like ESINEA, except in emergency (12%), home hospitalization HADO (1%), and outpatient consultations (3%), which ESINEA did not include. Incident distribution differed, with 66% occurring at the Children’s Hospital (34%), and the General Hospital (33%) in SINOIRES, compared to a predominance of the General Hospital in ESINEA. Both ESINEA and SINOIRES identified “Patient care and follow-up”, “Medication/vaccines”, and “Surgical procedures” as the most frequent phases. However, ESINEA detected a significantly higher proportion of PSIs in the “Patient care and follow-up” phase (29.95%), likely due to its focus on incidents directly impacting patient care. Regarding phases of care, SINOIRES recorded the highest frequency in the “Medication/vaccines” (17.19%), followed by “Patient care and follow-up” (14.44%), “Continuity of care” (13.46%), “Surgical procedures” (11.20%), and “Therapeutic procedures” (8.94%). In contrast, ESINEA identified “Patient care and follow-up” as the most frequent (29.95%), followed by “Healthcare-associated infections” (17.21%), “Therapeutic procedures” (13.47%), “Medication and vaccines” (10.88%), and “Surgical procedures” (8.52%). The higher reporting of medication-related incidents in SINOIRES likely reflects the impact of the Hospital Pharmacy Department’s prescription review program. This program proactively identifies and corrects prescription errors, often undetected in HCIS, through rigorous review and communication with physicians, thus enhancing patient safety. Medication-related incidents reported to SINOIRES were not included in ESINEA. SINOIRES rated 86% of proposed solutions as “Highly feasible”, while ESINEA rated them “Feasible with difficulties” in 51.8% of cases (p<0.001). This difference may stem from variations in reporter and collaborator profiles, evaluation criteria, or the organizational contexts. SINOIRES’ greater optimism may facilitate solution adoption, whereas ESINEA’s more cautious approach poses challenges. The low detection rate of identification errors in ESINEA may result from unstructured HCIS documentation (eg, ID bracelets) and reliance on voluntary reporting.
Comparisons between ESINEA and voluntary reporting systems such as SINOIRES should be interpreted in the context of their differing objectives and detection mechanisms. While reporting systems primarily capture voluntarily reported incidents, often emphasizing near misses and medication-related events, ESINEA is designed to systematically identify documented PSIs and AEs through structured medical record review. These approaches therefore capture different but complementary event universes and together provide a more comprehensive understanding of patient safety risks within hospital settings.
The overall lack of detailed documentation regarding PSI communication (50%) represents a clear area for improvement within patient safety protocols. Despite this limitation in documentation, the available data reveals some interesting trends. PSIs were reported as being communicated to staff in 30% of cases, while communication with patients or their family members occurred more frequently, in 60% of cases where this information was documented. This discrepancy tentatively suggests that there might be a higher rate of communication with patients and families compared to healthcare colleagues regarding PSIs. Effective communication across all stakeholders is crucial for shared decision-making, coordinated care, and ensuring patient-centered care. Standardizing documentation practices related to PSI communication could enhance transparency and improve patient safety outcomes.
ESINEA confirms that prolonged hospital stays are associated with a higher incidence of AEs. This is due to patient condition decline, increased care complexity, and prolonged exposure to risks like nosocomial infections, medication errors, and procedural complications, and the necessity for using invasive devices for extended periods. Key risk factors included advanced age, comorbidity, disease severity, and major surgery. AEs were most prevalent among older adults and Intensive Care patients, followed by those in Cardiology and Internal Medicine.
These findings are consistent with existing literature, which demonstrates the increased vulnerability of older and critically ill patients due to multiple comorbidities and fragility. Furthermore, specialties like Intensive Care and Cardiology, which involve complex interventions, have higher complication risks4,17,18. Factors such as nosocomial infections, medication errors, and diagnostic delays also contribute to longer hospital stays and more frequent AEs.19–22 Collectively, these findings emphasize the critical need for evidence-based patient safety strategies aimed at mitigating AEs and improving the quality of care for vulnerable patient populations.
In this context, healthcare organizations that establish comprehensive patient safety structures such as appointing a patient safety officer, implementing a patient safety plan, creating an incident reporting system, and providing support for second victims— may be more effective in promoting a patient safety culture and improving the documentation of AEs in patient records.23 This may contribute to ESINEA’s success in detecting a high number of AEs, along with the importance of expert training in both clinical specialties and patient safety for the ESINEA collaborators.
Strengths and Limitations of the Study
ESINEA is a valuable tool for patient safety monitoring in a tertiary hospital, identifying issues, evaluating trends, and providing knowledge on AEs risk factors. Limitations include its index-date cohort design, possible underreporting, evaluation team heterogeneity (inherent in the methodology), and limited generalizability. Regarding the specific findings, the notably high number of urgent admissions could be attributed to the study being conducted on a Saturday, a day when the proportion of patients admitted for scheduled surgery is typically lower.
The high frequency of “Other” responses in the A module of screening form, Healthcare-associated infections, and Med/vaccines modules, suggests the need for qualitative analysis to assess items clarity, evaluator adequacy, or the necessity of new items.
This study has several methodological limitations. The index-date sampling strategy may introduce day-of-week or seasonal bias, as reflected by the high proportion of urgent admissions. In addition, trigger-based detection depends on the quality and completeness of clinical documentation, and adjudication involved multiple reviewers with different clinical backgrounds. These limitations were mitigated through standardized training, structured review tools, and consensus-based expert adjudication.
Conclusions
The ESINEA study estimated the period prevalence of PSIs per hospitalization episode and characteristics of patient safety issues at the participating hospitalization centers of La Paz University Hospital (General Hospital, Children’s Hospital, Maternity Hospital, Carlos III Hospital, and Cantoblanco Hospital). Key findings include:
- Proposed improvements focus on strengthening patient care, enhancing infection prevention and optimizing clinical procedures.
- The identified AE period prevalence reflects a substantial burden of patient harm among hospitalized patients. Comparisons with commonly cited estimates should be interpreted cautiously due to differences in study design, definitions, and detection sensitivity. Data analysis revealed a vulnerable patient profile for PSIs, including advanced age, Charlson Comorbidity Index, and length of hospitalization.
- Although lower than expected (40%), a significant 34.2% of PSIs were found to be preventable, with over half of AEs being avoidable, highlighting the importance of preventive strategies.
- The proposed activities focus on improving patient care, infection prevention (particularly for nosocomial infections), and optimizing clinical procedures to reduce variability and improve adherence to protocols and guidelines. This study underscores the need for a strong patient safety culture across the participating centers, encouraging active participation from all healthcare professionals, and establishing a robust safety framework that includes dedicated resources, patient safety leads, and specialized training for healthcare professionals.
- Future implementation of ESINEA in other hospital settings will be essential to evaluate its generalizability and role in routine patient safety surveillance.
Abbreviations
ACV, Angiology and Vascular Surgery; AE, Adverse Event; ESINEA, del español “Estudio de Incidentes y Eventos Adversos”; ANR, Anesthesia and Resuscitation; CAR, Cardiology; CCA, Cardiac Surgery; CEIC, Ethics and Clinical Research Committee; CGD, General and Digestive Surgery; CMF, Maxillofacial Surgery; CPE, Pediatric Surgery; CPL, Plastic and Reconstructive Surgery; CRD, Data Collection Notebook; CTO, Thoracic Surgery; DIG, Digestive; GIN, Gynecology; GRT, Geriatrics; HCIS, Functions as an electronic management and information system for clinical history; HEM, Hematology; HH, Home Hospitalization; HULP, La Paz University Hospital, which integrates, General Hospital, Children’s Hospital, Maternal Hospital, Carlos III Hospital, and Cantoblanco Hospital; IC, Confidence Interval; MIN, Neonatal Intensive Care Medicine; MIR, Internal Medicine; MIV, Intensive Medicine; NEF, Nephrology; NML, Pulmonology; NRC, Neurosurgery; NRL, Neurology; OBS, Obstetrics; ONC, Medical Oncology; ONR, Radiation Oncology; ORL, Otorhinolaryngology; PED, Pediatrics; PICU, Pediatric Intensive Care Unit; PSI, Patient Safety Incidents; PSQ, Psychiatry; REA, Trauma Shock; REH, Rehabilitation; REU, Rheumatology; RSP, Patient Safety Managers; TRA, Traumatology and Orthopedic Surgery; UCI, Intensive Care Unit; UFGR, Functional Unit of Risk Management; URO, Urology; VP, Predictive Value, Positive (P), Negative (N).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that there are no conflicts of interest regarding the publication of this article. No financial or personal relationships that could inappropriately influence or bias the content of the manuscript have been identified.
References
1. World Health Organization (WHO). OMS Seguridad del paciente. WHO [Internet]. World Health Organization; 2021 [cited November 2021]; Available from: http://www.who.int/es/new-room/fact-sheets/detail/patient-safety.
2. Slawomirski L, Auraaen A, Klazinga NS. The economics of patient safety: strengthening a value-based approach to reducing patient harm at national level. OECD 2017. Available from: https://www.oecd.org/content/dam/oecd/en/publications/reports/2017/06/the-economics-of-patient-safety_258f9682/5a9858cd-en.pdf.
3. de Vries EN, Ramrattan MA, Smorenburg SM, Gouma DJ, Boermeester MA. The incidence and nature of in.hospital adverse events: a systematic review. Qual Saf Health Care. 2008;17(3):216–17. doi:10.1136/qshc.2007.023622
4. Aranaz Andrés JM, Aibar Remón C, Vitaller Burillo J, Ruiz López P. National Study on Adverse Events Related to Hospitalization: ENEAS 2005. [Internet] Madrid: Ministry of Health and Consumer Affairs; 2006. [Spanish text]Available from: http://www.seguridaddelpaciente.es/resources/contenidos/castellano/2006/ENEAS.pdf.
5. Incidents and Adverse Events in Intensive Care Medicine. Safety and Risk in the Critically Ill Patient. SYREC 2007 Report, May 2009. Madrid: Ministry of Health, Social Policy and Equality; 2010. [Spanish text] Available from: https://seguridaddelpaciente.sanidad.gob.es/informacion/publicaciones/2010/docs/syrec.pdf.
6. Valencia-Martín JL, Martin-Delgado J, Pardo-Hernández A, Vicente-Guijarro J, Requena-Puche J, Aranaz Andrés JM; ESHMAD Director Group, external advisers. The Study on Safety in Hospitals in the Region of Madrid (ESHMAD) design: screening and analysis of incidents and adverse events”. J Healthc Qual Res. 2021. doi:10.1016/j.jhqr.2021.03.007
7. IBEAS Study. Prevalence of adverse events in hospitals in Latin America. Reports, Studies, and Research 2010. Ministry of Health, Social Policy and Equality. Available from: https://seguridaddelpaciente.sanidad.gob.es/informacion/publicaciones/2010/docs/INFORME_IBEAS.pdf.
8. Sundararajan V, Henderson T, Perry C, Muggivan A, Quan H, Ghali WA. New ICD-10 version of the Charlson comorbidity index predicted in-hospital mortality. J Clin Epidemiol. 2004;57(12):1288–1294. doi:10.1016/j.jclinepi.2004.03.012
9. Brennan TA, Leape LL, Laird NM, et al. Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard Medical Practice Study I. N Engl J Med. 1991;324(6):370–376. doi:10.1056/NEJM199102073240604
10. Aranaz Andrés JM, Limón Ramírez R, Aibar Remón C, et al; IBEAS Teamwork. Comparison of two methods to estimate adverse events in the IBEAS Study (Ibero-American study of adverse events): cross-sectional versus retrospective cohort design. BMJ Open. 2017;7(10):e016546. doi:10.1136/bmjopen-2017-016546
11. Michel P, Quenon JL, de Sarasqueta AM, Scemama O. Comparison of three methods for estimating rates of adverse events and rates of preventable adverse events in acute care hospitals. BMJ. 2004;328(7433):199. doi:10.1136/bmj.328.7433.199
12. Woloshynowych M, Neale G, Vincent C. Case record review of adverse events: a new approach. Qual Saf Health Care. 2003;12(6):411–415. doi:10.1136/qhc.12.6.411
13. Guzmán-Ruiz O, Ruiz-López P, Gómez-Cámara A, Ramírez-Martín M. Detección de eventos adversos en pacientes adultos hospitalizados mediante el método Global TriggerTool [Detection of adverse events in hospitalized adult patients by using the Global Trigger Tool method]. Rev Calid Asist. 2015;30(4):166–174. Spanish. doi:10.1016/j.cali.2015.03.003
14. Nebeker JR, Stoddard GJ, Rosen A. Considering sensitivity and positive predictive value in comparing the performance of triggers systems for iatrogenic adverse events triggers and targeted injury detection systems (TIDS) [Internet]. AHRQ. 2009 [consultado 24 de julio de 2017]. Available from: https://archive.ahrq.gov/news/events/other/triggers/triggers2.html.
15. EPINE Study Group. EPINE-EPPS Study No. 33:2023. Spain Report. Prevalence of infections (healthcare-associated and community-acquired) and antimicrobial use in acute hospitals (Version 1.0) [Spanish text]. 2024. Available from: https://epine.es/api/documento-publico/2023%20EPINE%20Informe%20Espa%C3%B1a%2025012024.pdf/reports-esp. [
16. Ramírez E, Martín A, Villán Y, et al. Effectiveness and limitations of an incident-reporting system analyzed by local clinical safety leaders in a tertiary hospital: prospective evaluation through real-time observations of patient safety incidents. Medicine. 2018;97(38):e12509. doi:10.1097/MD.0000000000012509
17. Vincent C, Neale G, Woloshynowych M. Adverse events in British hospitals: preliminary retrospective record review. BMJ. 2001;322(7285):517–519. doi:10.1136/bmj.322.7285.517
18. Requena J, Aranaz JM, Gea MT, et al. Evolution of the adverse effects prevalence related to healthcare in hospitals of the Valencia community. Rev Calid Asist. 2010;25(5):244–249. doi:10.1016/j.cali.2010.03.007
19. Mikos M, Banaszewska A, Kutaj-Wąsikowska H, et al. Occurrence of adverse events in the activity of hospital wards in the opinions of doctors and nursing management staff. Ann Agric Environ Med. 2020;27(2):306–309. doi:10.26444/aaem/106234
20. Cantor N, Durr KM, McNeill K, et al. Increased mortality and costs associated with adverse events in intensive care unit patients. J Intensive Care Med. 2022;37(8):1075–1081. doi:10.1177/08850666221084908
21. Ahmed AH, Thongprayoon C, Schenck LA, et al. Adverse in-hospital events are associated with increased in-hospital mortality and length of stay in patients with or at risk of acute respiratory distress syndrome. Mayo Clin Proc. 2015;90(3):321–328. doi:10.1016/j.mayocp.2014.12.015
22. Kannan S, Bruch JD, Song Z. Changes in hospital adverse events and patient outcomes associated with private equity acquisition. JAMA. 2023;330(24):2365–2375. doi:10.1001/jama.2023.23147
23. World Health Organization. Global patient safety report 2024. [Internet]. Geneva: World Health Organization; 2024. Available from: https://seguridaddelpaciente.sanidad.gob.es/informacion/publicaciones/2024/docs/Global_patient_safety_report_2024._Geneva_World_Health_Organization_2024.pdf.
24. Culture of patient safety in Spain: perceptions and trends of professionals in healthcare organizations, 2024. Collaboration of the Spanish Society for Quality Healthcare, the Foundation for Research, Teaching and Innovation in Patient Safety, and the Undersecretariat of Healthcare Quality of the Ministry of Health. Available from: https://seguridaddelpaciente.sanidad.gob.es/informacion/publicaciones/2024/docs/Cultura-de-seguridad-del-paciente-en-Espana_Estudio-SECA-FIDISP.pdf.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Epidemiology and Survival of Kaposi’s Sarcoma by Race in the United States: A Surveillance, Epidemiology, and End Results Database Analysis
Ragi SD, Moseley I, Ouellette S, Rao B
Clinical, Cosmetic and Investigational Dermatology 2022, 15:1681-1685
Published Date: 18 August 2022
Hospital Work Conditions and the Mediation Role of Burnout: Residents and Practicing Physicians Reporting Adverse Events
Jarrar M, Al-Bsheish M, Albaker W, Alsaad I, Alkhalifa E, Alnufaili S, Almajed N, Alhawaj R, Al-Hariri MT, Alsunni AA, Aldhmadi BK, Alumran A
Risk Management and Healthcare Policy 2023, 16:1-13
Published Date: 5 January 2023
Impact of Target Management Card on Patient Safety in the Emergency Department: A Mixed Methods Study
Chen L, Yang H, Cui S, Ye D
Risk Management and Healthcare Policy 2023, 16:1905-1914
Published Date: 18 September 2023
Application of Multidimensional Quality Management Tools in the Management of Medical Adverse Events
Yuan B, Song S, Tang X, Ma Z
Risk Management and Healthcare Policy 2024, 17:91-99
Published Date: 9 January 2024
Hope is Not a Strategy: Key Lessons from COVID-19 for Future Health Crises
Knudsen SV, Kristensen I, Kure-Biegel N, Bech M, Agerbak H, Hansen CP, Mohr-Jensen C, Valentin JB, Petersen MB, Mainz J
Risk Management and Healthcare Policy 2024, 17:3247-3256
Published Date: 21 December 2024