")
Back to Journals » Risk Management and Healthcare Policy » Volume 16
Impact of Target Management Card on Patient Safety in the Emergency Department: A Mixed Methods Study
Authors Chen L, Yang H , Cui S, Ye D
Received 28 June 2023
Accepted for publication 13 September 2023
Published 18 September 2023 Volume 2023:16 Pages 1905—1914
DOI https://doi.org/10.2147/RMHP.S427988
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Lixia Chen,1 Heng Yang,2 Shaomei Cui,2,* Danjuan Ye2,*
1Department of Nursing, The Fourth Affiliated Hospital, Zhejiang University School of Medicine, Yiwu, Zhejiang, People’s Republic of China; 2Department of Emergency, The Fourth Affiliated Hospital, Zhejiang University School of Medicine, Yiwu, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lixia Chen, Department of Nursing, The Fourth Affiliated Hospital, Zhejiang University School of Medicine, N0.N1 Shangcheng Avenue, Yiwu City, Zhejiang Province, People’s Republic of China, Tel +1 596 882 9886, Email [email protected]
Purpose: This study aimed to investigate the potential impact of the Target Management Card on patient safety in the emergency department.
Patients and Methods: A mixed method design was developed, combining a one-group pretest-posttest design with a qualitative study. Target Management Cards were formulated for 32 emergency nurse practitioners and focus group interviews were conducted after the intervention. Wilcoxon’s signed rank test was used to compare pre-test and post-test scores. The interview data were subject to content analysis.
Results: After developing the Target Management Card, there were significant improvements in safety behaviors (Z = 4.709, p < 0.01) and perception of patient safety (Z = 4.257, p < 0.01) among emergency nurse practitioners. The nurses in the focus group interviews agreed that the Target Management Card could improve patient safety by warning and supervising nursing work in the emergency department, promoting a positive change in nurses’ attitudes and behaviors toward patient safety.
Conclusion: Our study found that nurses and nursing managers jointly formulating Target Management Cards in emergency departments significantly enhances patient safety.
Keywords: target management card, patient safety, patient safety culture, mixed methods, emergency department
Introduction
The World Health Assembly (WHA) adopted a Global Patient Safety Action Plan for the period of 2021–2030 to eliminate avoidable harm in health care.1 The World Health Organization (WHO) defines patient safety as preventing errors and adverse events that occur in patients while providing health care.2 The safety of patients is a critical component of quality care for healthcare facility personnel who aim to provide safe and effective patient care.3 Poor patient safety has become the third leading cause of death in the United States in recent years and a serious public health issue worldwide.4 This has been reflected in the increasing incidence of patient safety events, such as adverse medical events and safety risks.5 In 2018, the National Health Commission of the People’s Republic of China required medical institutions to create a positive patient safety culture and internalize the concept of patient safety into daily clinical practices.
Patient safety culture refers to the product of individual and group values, attitudes, perceptions, competencies, and patterns of behavior in an organization.6 Establishing and cultivating a patient safety culture in healthcare facilities is critical to improving patient safety and quality of care, contributing to patient satisfaction and job satisfaction7,8 Developing a patient safety culture is the key to improving patient safety and quality of care in the nursing environment.9 A positive patient safety culture includes reporting errors, nonpunitive responses to errors, management support, effective communication, and organizational learning.10 All of these contribute positively to patient satisfaction, family satisfaction, and the well-being of medical staff and can even reduce the number of hospital admissions.11 Healthcare institutions must establish and improve a safety culture to reduce adverse events related to healthcare services and protect patients from nursing errors.12
Patient safety and safety culture are essential aspects of providing high-quality health care, especially in the emergency department in modern health care.13 Medical emergency departments are dynamic and complex environments with high patient flows that are fast-paced and unpredictable Patients are also vulnerable to adverse events due to errors made by clinical nurses and physicians in the emergency room.14,15 The incidence of adverse events in medical institutions ranges from 2.9% to 16.6%, but 25% to 50% of which are considered preventable.16 Therefore, creating a positive patient safety culture in the emergency department is necessary to improve patient safety.
In healthcare facilities, nurses are responsible for continuously monitoring and caring for patients during hospitalization. As a key safety link between patients and other healthcare providers, nurses promote patient safety and improve patient prognosis.17,18 Alanazi et al19 found that nurses’ positive safety attitude is strongly related to patient safety in reducing falls, medication errors, stress injuries, and medical-related infections. Furthermore, statistics from healthcare institutions indicate that most adverse events are attributable to the absence of a safety culture among nurses rather than the lack of expertise among nursing staff.20 The targeted intervention in the patient safety culture is considered the primary strategy to promote patient safety and improve the quality of medical and health institutions.21 Developing a positive patient safety culture in hospitals is a crucial strategy to enhance patient safety and reduce adverse events.22 As a result, based on the unique characteristics and specialty of the emergency nurse working environment, it is crucial to implement a patient safety culture and innovative contextual intervention to ensure that emergency nurses constantly improve their awareness of patient safety.
In his seminal text from his book, “The Practice of Management”, Drucker introduced the concept of Management by Objectives as a managerial strategy.23 The target management technique is characterized by a high level of critical stakeholders’ engagement in goal setting and performance evaluation. Through a collaborative effort, managers and employees define objectives, thereby enhancing employee motivation and the efficacy of implementation. Notably, the target management process is heavily contingent upon iterative feedback mechanisms.24 Empirical evidence suggests a significant and positive influence of target management on employee behavior. The concept of management by objectives has been popular in nursing interventions in recent years.25 The use of target management in post-management, nursing quality, adverse events, and other areas has enhanced nursing quality, optimized human resource management, reduced incidence of unplanned extubation, and other favorable outcomes.
The review by Hesselink et al suggests that adverse event reporting systems and simulation-based patient training are promising interventions to enhance patient safety within emergency departments.26 Amaniyan et al identified that deficiencies in organizational management and workflow oversight in emergency departments negatively affect patient safety.27 The expertise of medical personnel is vital to patient outcomes and safety culture in medical facilities. The significant factor that hampers the cultivation of a safety-centric culture is negative attitudes among staff. Hence, exploring intervention methodologies is crucial for altering emergency nursing staff attitudes toward ensuring patient safety.28
Although research exists that investigates strategies to enhance the culture of patient safety within emergency departments, there is a paucity of effective interventions aimed at improving patient safety governance across the continuum of emergency care.26 In this study, the Target Management Card (TMC) is a tool designed in collaboration with nurses and nursing managers to achieve patient safety goals. To improve the behavior and attitude of emergency nurses and maintain patient safety, this study intervened in the emergency care chain using the target management card. This study aimed to understand nurses’ perceptions of patient safety culture after jointly formulating TMC with nursing managers and to investigate the potential impact of the (TMC) on patient safety in the emergency department.
Materials and Methods
Study Design
A mixed method study was developed, combining a one-group pre-test-post-test design (quantitative study) with focus group interviews (qualitative study). The quantitative study was conducted to determine the effect of TMC, followed by the qualitative study to explore the cognition of TMC among emergency nurses. Quantitative research cannot provide in-depth explanations of the data acquired from the intervention. In focus groups, data is often more vivid and richer than in one-on-one interviews since group interaction can facilitate more profound and in-depth interactions.29 The qualitative study followed the Consolidated Criteria for Reporting Qualitative Studies (COREQ) guidelines.30
Study Settings and Subjects
The study was conducted from October to December 2021 in the emergency department of the Fourth Affiliated Hospital Zhejiang University School of Medicine in China. The hospital is a Class A general hospital in Zhejiang Province with 1141 open beds. The convenience sampling method was used to recruit research participants. The recruitment information was released in a WeChat group. The inclusion criteria were as follows: (a) emergency department nurse with a nursing license; (b) working experience of not less than two years; (c) informed consent and voluntary participation in this study. Nurses were excluded if (a) they were trainee nurses, (b) they were nurses with advanced study, and (c) they were on maternity leave or sick leave. Burns and Grove suggested that at least 30 nurses are needed in the observation group in a quantitative study.31 Focus group interviews with an acceptable minimum number of participants is 6–10.32 In this study, 34 emergency department nurses were recruited, assuming a 10% loss to follow-up.
The study was conducted during the COVID-19 pandemic, and all participants wore N95 respirators and received the new crown vaccine. Participants in focus groups were separated by more than one meter during talks.
Method 1-Quantitative Study Phase
Study Intervention
A patient safety quality control team was established before the study that consisted of an associate chief nurse, two nurses in charge, and a nurse with a master’s degree. Responsibilities of the quality control team were: (1) retrospective analysis of nursing safety events and hidden danger events in the emergency department in the past year and conduct data analysis and root cause analysis of the adverse events; (2) develop TMC. For further comprehensive details, kindly refer to Supplementary Material 1; (3) discussing and setting target values with nurses; (4) supervising the implementation of the research program; (5) reaching agreement on authority, conditions, rewards, and punishments with nurses. Before being used in the emergency department, the TMC was submitted for evaluation to the Fourth Affiliated Hospital Nursing Quality and Safety Management Committee of Zhejiang University School of Medicine. It was used in clinical practice after receiving clearance.
First, TMC was formulated with the contents of medication errors, specimen collection, drug extravasation, occupational exposure, unplanned extubation, patient falls, stress injuries, identification errors of identity information, and target time management of patients with a single disease. Second, nurses and the patient safety quality control team jointly set the target value. For example, the target value 1 represented 1 medication error while 0 represented no medication errors. The corresponding system of rewards and sanctions was established. Should nurses achieve the predetermined objectives, they would be eligible for equitable incentives, such as a week-long consecutive leave or a book of personal interest. Conversely, if the target values were not met, appropriate penalties would be enforced, including eight hours of uncompensated service to the department or a monetary fine of 200 yuan. Finally, the patient safety quality control team conducted a “patient safety month” activity and monitored the completion of the target value. The activity was organized in the last week of each month and a different patient safety theme was set for each month. The theme content involved items of the TMC and patient safety. Past adverse events associated with the theme content were examined, and strategies developed to avoid them were analyzed. Relevant guidelines, literature, and nursing standards were studied. After three months of the intervention, the patient safety quality control team and nurses jointly conducted self-evaluation and manager evaluation, where nurses summarized experience and lessons in the target implementation, and target managers evaluated the target results and offered suggestions.
Data Collection
General information, including age, gender, marital status, education level, working experience, positional title, and nature of employment, was collected from the research participants.
The Patient Safety Culture Assessment Scale (PSCAC) was revised by Fanglei Chen33 from the Safety Attitudes Questionnaire (SAQ).34 This scale can evaluate nurses’ perception of patient safety culture with a total of 24 items in five dimensions: teamwork climate, job satisfaction, stress recognition, safety climate, and perceptions of management. A Likert-5 scale with a total score of 24 to 120 was used. The higher the score, the better the nurse perceives the patient safety culture. PSCAC has good reliability and validity with Cronbach’s alpha coefficient of 0.886, which makes it adequate for China’s cultural environment.33
The Chinese version of the Nurse Safety Behavior Questionnaire (NSBQ) was developed by Rong.35 The scale can measure the performance of medical staff in protecting patients from harm or promoting patient safety in their work, with 12 items in one dimension. A Likert-5 scale was used with 1–5 points recording never-always. Higher scores indicate better performance in nurse safety behaviors. It was found that NSBQ had a Cronbach’s alpha coefficient of 0.915.35
Data were collected one day (T0) before the implementation of TMC and immediately after the intervention (T1). The data collected in the T0 phase were patient safety culture and safety behavior scores of emergency department nurses in the conventional work mode. The data collected in stage T1 were the scores of patient safety culture and safety behavior of emergency nurses after the implementation of TMC. T0 and T1 were separated by 90 days. Before the intervention, emergency nurse practitioners received informed consent, including the purpose and significance of the study, voluntary participation, withdrawal at any time, and anonymity protection. Nurses were required to fill out all the items in the questionnaire honestly according to their actual situation with the assistance of two research team members.
Data Analysis
Demographic data were presented as frequencies and percentages. The normal distribution was determined by the Shapiro–Wilk test. The Wilcoxon signed-rank test was used to analyze changes in scores before and after the intervention. Statistical significance (p-value) was assessed using a 2-tailed test. The significance threshold was set at p < 0.05. All statistical analyses were conducted using JASP, Version 0.17.3.0, and SPSS, Version 22.0 (SPSS Inc., Chicago, IL, USA).
Method 2-Qualitative Study Phase
Data Collection
At the end of the intervention phase, the research team explained the purpose and significance of the focus group interview to the nurses Four focus group interviews were conducted in January 2022, with eight people in each group. We chose nurses who work together since homogeneous groups would help nurses express their opinions.36 The research team discussed the development of interview guidelines based on the purpose and significance of the study: (a) What do you think about patient safety? What is your understanding of patient safety in the emergency department? (b) What role do you think the TMC will play in your nursing work? (c) What changes in your clinical care behaviors and attitudes have resulted from the TMC? (d) How will the TMC impact your future nursing work? Before the start of the focus groups, the date was agreed upon with the participating emergency department nurses. The interview host ensured that each focus group participant had an equal opportunity to express their opinions.37 In the emergency department library, participants conducted focus groups in a quiet, undisturbed area for approximately 60 min. Chen, the first author, worked in the emergency department for 16 years, served as the host during the focus groups, and two researchers observed and recorded essential data such as the atmosphere of the focus groups, the nurses’ expressions, gestures, and tone of voice.
Data Analysis
Traditional content analysis was used to analyze the data.38 The interview data included recorded interviews and observations transcribed verbatim by two researchers (C LX, YH). After repeatedly reading the interview data to understand the participants’ experiences better, Two authors (Y DJ, C SM) detailed the raw data encoding and statement after reading the interview data repeatedly to understand the participants’ experiences better. The authors held discussions during the encoding process to synchronize any discrepancies in the encoded data. Examples of the analytical process are shown in Table 1.
 |
Table 1 Examples of the Analytical Process |
Two researchers recorded the interview data and the emotional reactions of the interviewees verbatim to improve the credibility of the collected data. Our goal was to eliminate any bias in interpreting the meaning expressed by the participants to increase the verifiability of the data. Qualitative and quantitative data were analyzed separately, and the results were combined during the discussion phase. Analyzing qualitative results can help clarify quantitative results and interpret them.
Ethical Considerations
Human Research Ethics Committee, the Fourth Affiliated Hospital of Zhejiang University School of Medicine approved this study as being in accordance with the principles of medical ethics. Written informed consent was obtained from each participant, including information about the study’s purpose, significance, risks, benefits, and publication of anonymized responses. The participants were informed that the interview would be recorded, and they could withdraw at any time. All data were anonymized and used only for this study. Data from the questionnaire and focus group interviews were anonymous and confidential.
Results
Quantitative results
General Information
A total of 34 emergency nurse practitioners were recruited for this study. After excluding one on maternity leave and one on sick leave, 32 nurses were finally included in the quantitative study. Participants tended to be younger, ranging in age from 24 to 34 years. The average age was 28.88 years, and there were 22 (68.75%) females. Demographic data are shown in Table 2.
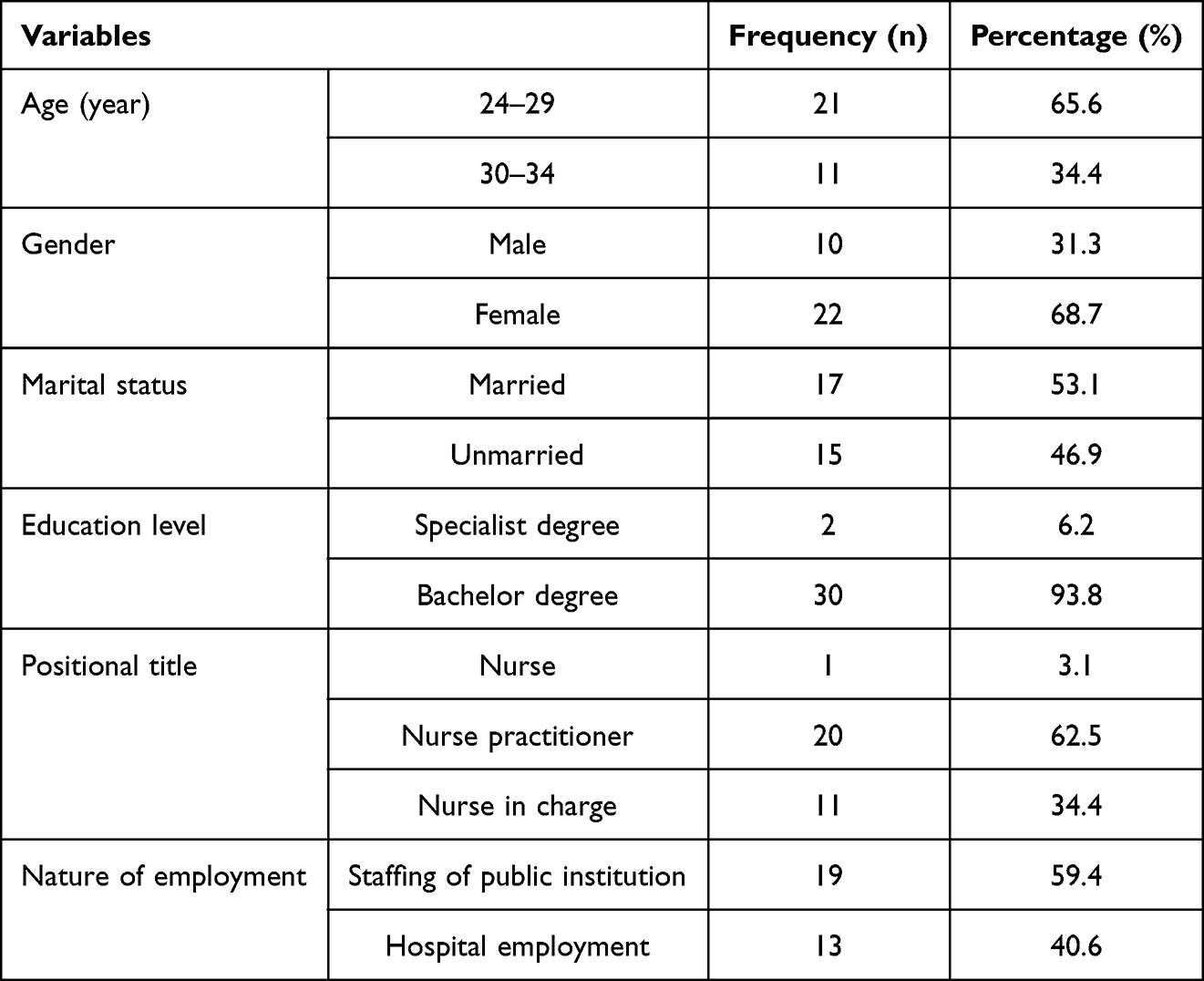 |
Table 2 Demographic Data of the Study Participants (n = 32) |
Impact of TMC on Patient Safety in the Emergency Department
Table 3 displays the overall PSCAC and NSBQ scores and the pretest and posttest scores for each dimension. Compared to T0, the total score of perception of patient safety culture and safety behaviors of nurses in the emergency department at T1 was significantly higher. PSCAC had a substantially lower median pretest total score (97.5) than the median posttest total score (108), and NSBQ had a significantly lower median pretest total score (45) than the median posttest total score (56). The posttest scores for all PSCAC dimensions were higher than the pretest values. The Shapiro–Wilk test of normality test (p < 0.05), the data do not conform to the normal distribution. Non-parametric test, the Wilcoxon signed rank test, was used for analysis. This difference was statistically significant (Z = 4.257, p < 0.01, 95% CI: 0.718–0.935; Z = 4.709, p < 0.01, 95% CI: 0.929–0.985). It can be considered that the target management card has different effects on patient safety culture and the safety behavior of nurses in the emergency department.
 |
Table 3 Comparison of Perception of Patient Safety Culture and Safety Behaviors of Nurses Before and After Intervention (n = 32) |
Qualitative results
A total of 32 nurses expressed interest in participating in the focus groups. The perception of emergency nurses concerning patient safety following the implementation of the TMC was explored. A total of three themes and nine sub-themes were obtained from the focus group interview. See Table 4.
 |
Table 4 Category and Sub-Category |
Importance of Patient Safety
Emergency nurses were aware of the importance of patient safety and believed that patient safety and medical safety are inseparable. Participants expressed that patient safety is crucial and doctors and nurses are responsible for ensuring patient safety. Doctors and nurses are responsible for ensuring the safety of patients when they are admitted to the hospital, as well as keeping them informed about their needs. Patients may experience anxiety and fear if adverse events or unexpected injuries occur. Thus, ensuring the safety of patients and meeting their medical needs can help improve patient satisfaction and the sense of achievement among medical staff. It also contributes to shorter treatment times, lower medical costs, the greater influence of departments and hospitals, and positive hospitals attributes and brands. Respondents’ responses are quoted below:
Medical workers are benevolent; it is necessary for them to pay attention to patient safety. If patient safety is guaranteed, as a nurse, I will not be disturbed by disputes or adverse events. (Group 1, P2, P5)
If adverse events or unintended injuries occur to a patient, I will feel nervous and afraid. (Group 3, P6).
Patients will compare the medical quality and service attitude of different hospitals. Ensuring patient safety and improving medical quality will make more patients visit our hospital. (Group 4, P1, P3)
Warning and Supervision Functions of the TMC on Nursing Work in the Emergency Department
All nurses indicated that the development of TMC positively affects patient safety. Some nurses pointed out that they had clear goals and responsibilities after setting the TMC with target values. Nurses stated that they would pay more attention to patient safety in their work under pressure and motivation. Nurses also commented that TMCs played a warning and supervisory role in nursing work by avoiding adverse events, striving for the target value, and ensuring patient safety.
Signing the TMC mainly serves as a warning to let me understand the key points in nursing work. (Group 2, P8).
The target value in the TMC lets me know what the focus of my work is and take care of patients more purposefully. (Group 3, P4).
The target value of each project is the rules and regulations of my work, which are invisible constraints and supervise my behaviors. (Group 4, P7).
Positive Changes in the Attitude and Behavior of Emergency Department Nurses Toward Patient Safety After TMC
Nurse practitioners reported that their attitudes and behaviors changed after signing the TMC. Nurses focused more on patient safety, organized their work reasonably, and improved the safety of nursing behaviors. With the implementation of the TMC, nursing behaviors became standardized and restrictive, and nursing operations were subject to nursing operation standards, rules, and regulations. TMC enables emergency nurses to actively consider patient safety, broaden their thinking, and provide patients with more comprehensive and individualized nursing care.
In the past, the importance of patient safety was not high. (Group 3, P4).
In the past, nursing patients would be relatively mechanical. After signing the TMC, I would think about ensuring patient safety. Colleagues would discuss and remind each other to standardize nursing behaviors. (Group 2, P6)
Rethinking nursing operations to provide individualized patient care. (Group 4, P4).
Discussion
Through a mixed-method study, we analyzed the impact of TMC developed jointly by nurses and nursing managers on patient safety in the emergency department to improve patient safety. We used the one-group pretest-posttest design to verify the intervention to exclude the interference of heterogeneity and related factors. Focus group interviews were then conducted further to clarify the effect and role of the intervention.
All five dimensions of the PSCAC and total scores were higher after the intervention, suggesting that emergency nurse practitioners perceived patient safety culture better after developing TMC. Nurses reported improved perceptions of stress recognition, management, job satisfaction, safety, and teamwork climate. Teamwork climate and job satisfaction are non-negligible in medical institutions. With the increasing complexity of the healthcare system, effective teamwork and a safe working climate, and teamwork climate are necessary to ensure patient safety and provide high-quality care.39 Studies have demonstrated that nurses’ job satisfaction is negatively correlated with the incidence of adverse events and medication errors in healthcare institutions.40 By developing a TMC jointly with nursing managers, nurses can become involved in patient safety management, creating a highly structured work environment and a positive teamwork atmosphere, and establishing a patient safety culture by improving emergency department nurses’ awareness and attitude.41 Participants in focus groups expressed that TMCs have a warning and supervisory role, which results in a greater emphasis on patient safety, and a more cautious and comprehensive approach to patient care in their work. Following collaborative efforts with managers to develop the TMC and establish an associated system of rewards and penalties, there was a notable increase in the enthusiasm and diligence of nursing staff in patient care. This collaboration also promoted the development of a patient safety culture.
The total score of NSBQ after the intervention was higher than those before the intervention, which was consistent with previous studies that managers’ values and awareness of patient safety culture can affect nurses’ safety behaviors; also, the underlying message of TMC is the importance of patient safety.40 In the focus group interviews, emergency nurse practitioners expressed that patient safety is critical and closely related to the safety of nurses. The development of TMC improved the level of safety culture, promoted their formation of positive patient safety awareness, standardized nursing safety behaviors, and formed a safe working concept and behavior mode, thus minimizing the incidence of adverse events and ensuring patient safety.42 TMC also advised emergency nurses to actively consider improving patient safety, guiding their behavior, and providing individualized, comprehensive, and safe nursing care. In the NSBQ, items 2 and 6 scored higher, indicating nurses were more likely to learn from past events, follow safety regulations, and ensure patient safety.
Our study has implications for nursing management in the emergency department. Patient safety culture is crucial to high-quality care, especially in the emergency department.43 The emergency department nursing managers should pay attention to the culture of patient safety and formulate positive safety strategies. Nursing staff should establish a positive attitude toward patient safety culture to reduce the occurrence of adverse events and ensure patient safety.
There are some limitations in this study. Firstly, time effects may have altered the study outcomes due to the period between the pretest and posttest, as participants worked longer. A one-group pretest-posttest design limited the study. Time-effect analyses based on randomized controlled trials will be needed in the future. Secondly, this study used a convenience sampling method with potential selection bias, which may limit the generalizability of our results to other populations. Lastly, this study did not conduct any follow-up and evaluated the effects of the intervention. Further research is required to determine whether target management cards have a longer-lasting positive or negative impact on emergency department nurses. To improve the study’s universality, more multi-center, large-sample data should be added. There is a need for more rigorous and higher-quality scientific research designs in the future.
Conclusion
In the emergency department, establishing a safety culture is considered a prerequisite for patient safety. In this study, emergency nurse practitioners collaborated with nursing managers to formulate TMC. The objective was to enhance the safety culture among nurses, rectify negative attitudes toward patient safety, standardize safety-related behaviors, and mitigate the occurrence of adverse events to ensure patient safety. Therefore, the TMC enhanced patient safety by fostering a positive patient safety culture in the emergency department.
Abbreviations
TMC, Target Management Card; PSCAC, Patient Safety Culture Assessment Scale; NSBQ, Nurse Safety Behavior Questionnaire.
Data Sharing Statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. World Health Organization. Global patient safety action plan 2021–2030. Available from: https://www.who.int/publications/i/item/9789240032705.
2. Institute of Medicine (US) Committee on Quality of Health Care in America. To Err is Human: Building a Safer Health System. In: Kohn LT, Corrigan JM, Donaldson MS, eds. Washington (DC): National Academies Press (US); 2000.
3. Astier-Peña MP, Torijano-Casalengua ML, Olivera-Cañadas G, Silvestre-Busto C, Agra-Varela Y, Maderuelo-Fernández JÁ. Are Spanish primary care professionals aware of patient safety? Eur J Public Health. 2015;25(5):781–787. doi:10.1093/eurpub/ckv066
4. Makary MA, Daniel M. Medical error-the third leading cause of death in the US. BMJ. 2016;353:i2139. doi:10.1136/bmj.i2139
5. Chen JJ, Yang Q, Zhao QH, et al. Reliability and validity of the Chinese version of the second victim experience and support tool. Chin Nurs Manag. 2019;19:991–995.
6. Nieva VF, Sorra J. Safety culture assessment: a tool for improving patient safety in healthcare organizations. Qual Saf Health Care. 2003;12(Suppl 2):ii17–ii23. doi:10.1136/qhc.12.suppl_2.ii17
7. Kong LN, Zhu WF, He S, et al. Attitudes towards patient safety culture among postgraduate nursing students in China: a cross-sectional study. Nurse Educ Pract. 2019;38:1–6. doi:10.1016/j.nepr.2019.05.014
8. Al-Surimi K, Almuhayshir A, Ghailan KY, Shaheen NA. Impact of patient safety culture on job satisfaction and intention to leave among healthcare workers: evidence from middle east context. Risk Manag Healthc Policy. 2022;15:2435–2451. doi:10.2147/RMHP.S390021
9. Weaver SJ, Lubomksi LH, Wilson RF, Pfoh ER, Martinez KA, Dy SM. Promoting a culture of safety as a patient safety strategy: a systematic review. Ann Intern Med. 2013;158(5 Pt 2):369–374. doi:10.7326/0003-4819-158-5-201303051-00002
10. Lee SE, Scott LD, Dahinten VS, Vincent C, Lopez KD, Park CG. Safety culture, patient safety, and quality of care outcomes: a literature review. West J Nurs Res. 2019;41(2):279–304. doi:10.1177/0193945917747416
11. DiCuccio MH. The relationship between patient safety culture and patient outcomes: a systematic review. J Patient Saf. 2015;11(3):135–142. doi:10.1097/PTS.0000000000000058
12. Occelli P, Quenon JL, Kret M, et al. Improving the safety climate in hospitals by a vignette-based analysis of adverse events: a cluster randomised study. Int J Qual Health Care. 2019;31(3):212–218. doi:10.1093/intqhc/mzy126
13. Alsabri M, AlGhallabi M, Al-Qadasi F, et al. Patient safety culture in emergency departments of Yemeni public hospitals: a survey study. Front Emerg Med. 2021;5(2):21. doi:10.18502/fem.v5i2.5618
14. Källberg AS, Ehrenberg A, Florin J, Östergren J, Göransson KE. Physicians’ and nurses’ perceptions of patient safety risks in the emergency department. Int Emerg Nurs. 2017;33:14–19. doi:10.1016/j.ienj.2017.01.002
15. Han JH, Roh YS. Teamwork, psychological safety, and patient safety competency among emergency nurses. Int Emerg Nurs. 2020;51:100892. doi:10.1016/j.ienj.2020.100892
16. Han Y, Kim JS. Cross-sectional Study on patient safety culture, patient safety competency, and adverse events. West J Nurs Res. 2020;42(1):32–40. doi:10.1177/0193945919838990
17. Van Bogaert P, Timmermans O, Weeks SM, van Heusden D, Wouters K, Franck E. Nursing unit teams matter: impact of unit-level nurse practice environment, nurse work characteristics, and burnout on nurse reported job outcomes, and quality of care, and patient adverse events--a cross-sectional survey. Int J Nurs Stud. 2014;51(8):1123–1134. doi:10.1016/j.ijnurstu.2013.12.009
18. Sim J, Joyce-McCoach J, Gordon R, Kobel C. Development of a data registry to evaluate the quality and safety of nursing practice. J Adv Nurs. 2019;75(9):1877–1888. doi:10.1111/jan.13967
19. Alanazi FK, Sim J, Lapkin S. Systematic review: nurses’ safety attitudes and their impact on patient outcomes in acute-care hospitals. Nurs Open. 2022;9(1):30–43. doi:10.1002/nop2.1063
20. Aouicha W, Tlili MA, Sahli J, et al. Patient safety culture as perceived by operating room professionals: a mixed-methods study. BMC Health Serv Res. 2022;22(1):799. doi:10.1186/s12913-022-08175-z
21. Świtalski J, Wnuk K, Tatara T, et al. Interventions to increase patient safety in long-term care facilities-umbrella review. Int J Environ Res Public Health. 2022;19(22):15354. doi:10.3390/ijerph192215354
22. El-Jardali F, Dimassi H, Jamal D, Jaafar M, Hemadeh N. Predictors and outcomes of patient safety culture in hospitals. BMC Health Serv Res. 2011;11(1):45. doi:10.1186/1472-6963-11-45
23. Drucker PF. The Practice of Management: A Study of the Most Important Function in America Society. Harper & Brothers. 1954.
24. George S, Al Jaber MK, Salem MJ, AlSaad AJ. The impact of management by objectives on employee behaviour and performance. paper presented at the 2021.
25. Ding X, Zhou Q, Yuan Y, Fan Y, Zhou RR, Yang Y. Effects of psychological nursing intervention based on management by objectives on health behavior and family satisfaction of pediatric inpatients. Indian J Pharm Sci. 2021;83(Spl Iss 2). doi:10.36468/pharmaceutical-sciences.spl.261
26. Hesselink G, Berben S, Beune T, Schoonhoven L. Improving the governance of patient safety in emergency care: a systematic review of interventions. BMJ Open. 2016;6(1):e009837. doi:10.1136/bmjopen-2015-009837
27. Amaniyan S, Faldaas BO, Logan PA, Vaismoradi M. Learning from patient safety incidents in the emergency department: a systematic review. J Emerg Med. 2020;58(2):234–244. doi:10.1016/j.jemermed.2019.11.015
28. Afework A, Tamene A, Tesfaye A, Tafa A, Gemede S. Status and factors affecting patient safety culture at dilla university teaching hospital: a mixed-method cross-sectional study. Risk Manag Healthc Policy. 2023;16:1157–1169. doi:10.2147/RMHP.S419990
29. Rabiee F. Focus-group interview and data analysis. Proc Nutr Soc. 2004;63(4):655–660. doi:10.1079/pns2004399
30. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
31. White A. Using samples to provide evidence. In: Schmidt N, Brown J, editors. Evidence Based Practice for Nurses. Sudbury, MA: Jones & Bartlett Learning; 2012:246–271.
32. Morgan DL. Focus Groups as Qualitative Research, Second Ed. Thousand Oaks, CA: SAGE publications; 1996.
33. Chen FL, Zhou L. Patient safety culture assessment scale: design and establishment. Nurs J Chin PLA. 2009;26(1):1–4.
34. Sexton JB, Helmreich RL, Neilands TB, et al. The safety attitudes questionnaire: psychometric properties, benchmarking data, and emerging research. BMC Health Serv Res. 2006;6(1):44. doi:10.1186/1472-6963-6-44
35. Rong YF, Zhu ZY. The Relationship Between Patient Safety Culture and Safety Behavior. Taiwan: Tzu Chi University; 2009.
36. Jayasekara RS. Focus groups in nursing research: methodological perspectives. Nurs Outlook. 2012;60(6):411–416. doi:10.1016/j.outlook.2012.02.001
37. Oxenbøll-Collet M, Egerod I, Christensen V, Jensen J, Thomsen T. Nurses’ and physicians’ perceptions of confusion assessment method for the intensive care unit for delirium detection: focus group study. Nurs Crit Care. 2018;23(1):16–22. doi:10.1111/nicc.12254
38. Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–1288. doi:10.1177/1049732305276687
39. Ammouri AA, Tailakh AK, Muliira JK, Geethakrishnan R, Al Kindi SN. Patient safety culture among nurses. Int Nurs Rev. 2015;62(1):102–110. doi:10.1111/inr.12159
40. Kunaviktikul W, Wichaikhum O, Nantsupawat A, et al. Nurses’ extended work hours: patient, nurse and organizational outcomes. Int Nurs Rev. 2015;62(3):386–393. doi:10.1111/inr.12195
41. Üy G, Ö G, Sönmez M. A survey of the patient safety culture of hospital nurses in Turkey. Collegian. 2016;23(2):225–232. doi:10.1016/j.colegn.2015.02.005.
42. Wang AM, Wang XH, Du HX, Yu CL, Lu XR. Path analysis of safety behavior status and related influencing factors of newly recruited nurses. Chin J Nurs. 2022;57(3):318–325. doi:10.3761/j.issn.0254-1769.2022.03.011
43. Alshyyab MA, FitzGerald G, Albsoul RA, Ting J, Kinnear FB, Borkoles E. Strategies and interventions for improving safety culture in Australian emergency departments: a modified delphi study. Int J Health Plann Manage. 2021;36(6):2392–2410. doi:10.1002/hpm.3314
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.