")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Epidemiology and Survival of Kaposi’s Sarcoma by Race in the United States: A Surveillance, Epidemiology, and End Results Database Analysis
Authors Ragi SD , Moseley I, Ouellette S, Rao B
Received 29 June 2022
Accepted for publication 13 August 2022
Published 18 August 2022 Volume 2022:15 Pages 1681—1685
DOI https://doi.org/10.2147/CCID.S380167
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Sara D Ragi,1 Isabelle Moseley,1 Samantha Ouellette,2 Babar Rao2
1The Warren Alpert Medical School of Brown University, Providence, RI, USA; 2Department of Dermatology, Robert Wood Johnson Medical School, New Brunswick, NJ, USA
Correspondence: Sara D Ragi, Email [email protected]
Abstract: The introduction of highly active antiretroviral treatment (HAART) for acquired immunodeficiency syndrome (AIDS) has led to a significant decrease in the incidence of Kaposi’s sarcoma (KS) in recent years. However, a concomitant increase in racial disparities in KS has arisen. Here, we analyze data from the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) Program for epidemiology and survival of Kaposi’s sarcoma by race. The highest incidence was observed among Black patients (incidence rate (IR), 1.189; 95% confidence interval (CI), 1.092– 1.189), followed by White patients (IR, 0.486; 95% CI, 0.473– 0.498). Relative survival at 1, 3, and 5 years differed significantly by race, with White patients having the highest survival rates (84.26%, 77.79%, and 74.79% at 1, 3, and 5 years respectively) and Black patients demonstrating the lowest (71.50%, 61.37%, and 57.38%), with intermediate survival rates in Asians/Pacific Islanders (AAPI) (80.62%, 71.19%, and 67.28%) and American Indians/Alaska Natives (AIAN) (80.56%, 61.45%, and 61.45%). We conclude that there are significant racial disparities in the incidence, epidemiology, and survival of KS.
Keywords: Kaposi’s sarcoma, racial disparities, race, cancer, soft tissue sarcoma, surveillance, epidemiology, end results program, epidemiology
Introduction
Kaposi’s sarcoma is an angioproliferative mesenchymal neoplasm caused by the human herpesvirus-8 (HHV-8), which is required but not sufficient to cause disease.1 Kaposi’s sarcoma (KS) gained public attention as during the height of the AIDS epidemic in the mid-1980s, when it became an extremely stigmatizing illness. Prior to the AIDS epidemic KS was extremely rare in the United States (US), with an incidence of about two per million people. By the early 1990s, that rate had increased to about 47 per million.1 In recent years, the introduction of highly active antiretroviral treatment (HAART) has led to a significant decrease to about 6 cases per million people.1–3 However, substantial racial disparity has been reported in the incidence and survival of KS patients in the HAART era.2–4 Here, we analyze data from the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEERs) Program for epidemiology and survival of Kaposi’s sarcoma by race.
Methods/Results
Data for KS were collected from the SEER-18 (2000–2018) database. Demographic and treatment information of KS (Table 1) was collected using the rate session tool.
 | 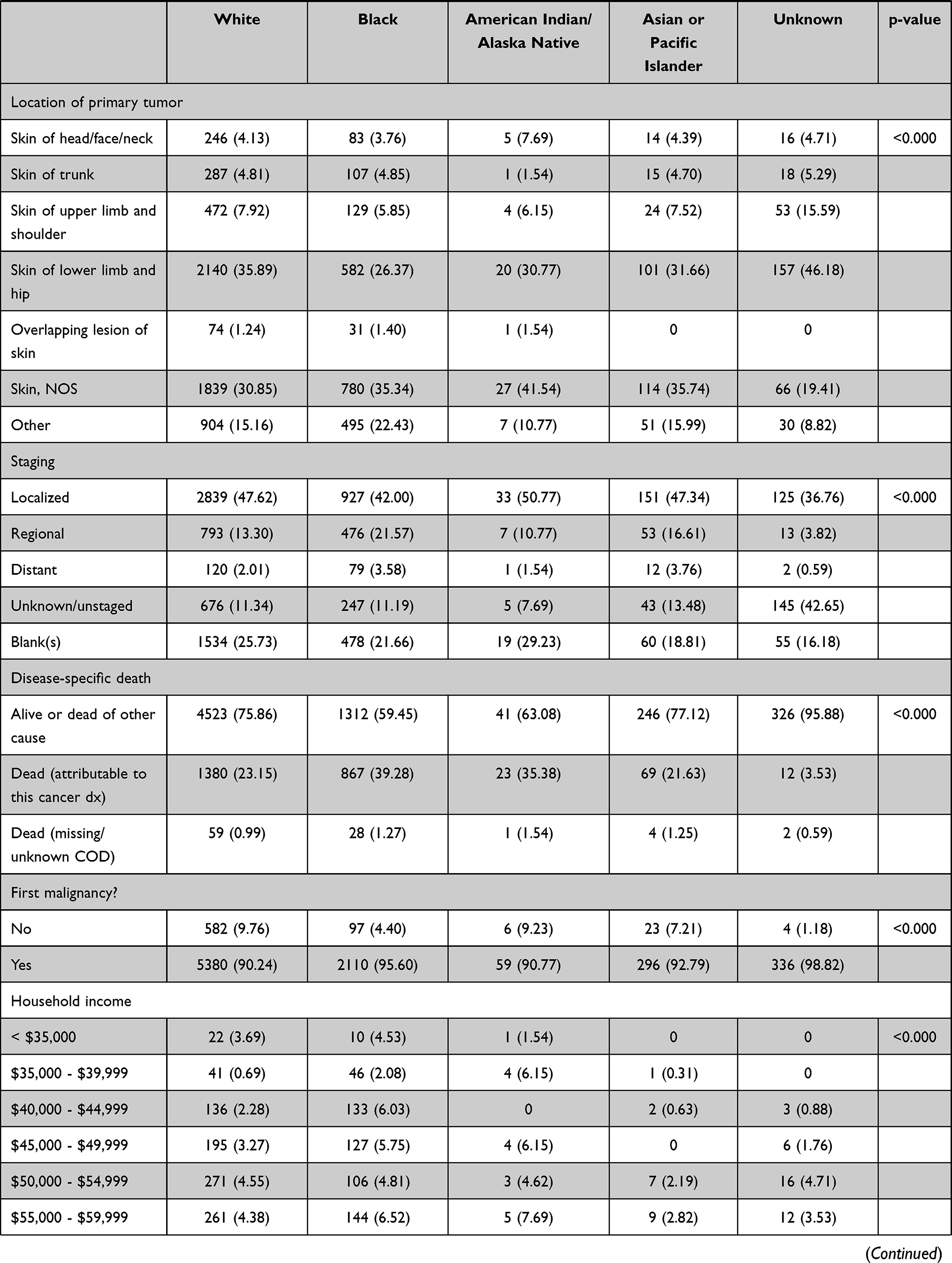 | 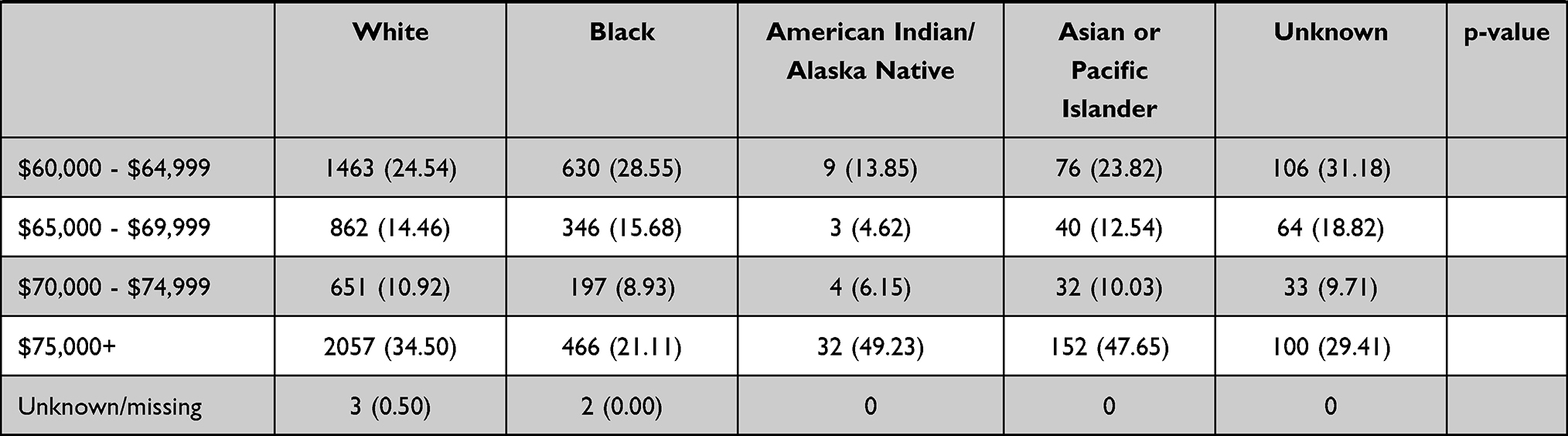 |
Table 1 The Incidence, Relative Survival, and Demographics of Kaposi’s Sarcoma by Race |
Incidence rates are per 100,000 and age-adjusted to the 2000 US Std Population (19 age groups - Census P25-1130) standard. The SEER*Stat software was utilized to generate confidence intervals. Confidence intervals (Tiwari mod) are 95% for rates. SEER groups age of diagnosis into predefined 5-year blocks in order to maintain patient privacy. ICD-10-CM codes were utilized to identify primary tumor location. Within SEER*Stat, we used the survival session function to calculate age-standardized relative survival via the Kaplan–Meier method. In Stata/SE v15.1, we used traditional chi-squared or Fisher exact tests where appropriate to compare demographic characteristics, tumor qualities, treatments, and survival rates among races; p-values are reported in Table 1.
The highest incidence was observed among Black patients (IR, 1.189; 95% CI, 1.092–1.189), followed by White patients (IR, 0.486; 95% CI, 0.473–0.498) and American Indians/Alaska Natives (AIAN; IR, 0.334; 95% CI, 0.252–0.433) with the lowest incidence in Asians/Pacific Islanders (AAPI; IR, 0.198; 95% CI 0.177–0.222). Relative survival at 1, 3, and 5 years differed significantly by race, with White patients having the highest survival rates (84.26%, 77.79%, and 74.79% at 1, 3, and 5 years respectively) and Black patients having the lowest (71.50%, 61.37%, and 57.38%), with intermediate survival rates in AAPI (80.62%, 71.19%, and 67.28%) and AIAN (80.56%, 61.45%, and 61.45%). Distributions for sex, ethnicity, age, tumor location, staging, disease-specific death, whether it was the first malignancy, and household income also differed significantly by race.
In terms of age distribution Black patients reported primary tumors at younger ages compared to White patients, AIAN, and AAPI. Skin of the lower limb/hip was the most common tumor location in White patients and AAPI, while skin, NOS (not otherwise specified) was most commonly reported in Black patients and AIAN. All races were most likely to have a localized tumor at presentation, but Black patients were significantly more likely to have a later stage tumor at presentation compared to all other races. Cause-specific death occurred in 23.15% of White patients, 39.28% of Black patients, 35.38% of AIAN, and 21.63% of AAPI. KS represented the first diagnosed malignancy in 90.24% of White patients, 95.60% of Black patients, 90.77% of AIAN, and 92.29% of AAPI. White and AIAN KS patients were most likely to have yearly household incomes in excess of $75,000, while Black and AAPI KS patients were most likely to have household income between $60,000–$64,999.
Discussion
A SEER-based study by Datta et al evaluating KS patients diagnosed between 1980 and 2004 reported significant improvement in the survival of White patients as compared to Black patients during the HAART era.2 Kumar et al demonstrated that this trend continued for KS patients diagnosed up until 2013.3 KS incidence continued to decline, but the decrease in the age-adjusted incidence rate (AAIR) in Black patients [annual percentage change (APC): −6.2; 95% CI: −8.8 to −3.5] was slower than that in White patients (APC: −10.9; 95% CI: −12.6 to −9.1). The hazard ratio for all-cause mortality in Black KS patients increased from 1.1 (95% CI: 1–1.2) in 1981–1995 to 1.55 (95% CI: 1.4–1.7) in 1996–2013 as compared to White patients.3 These racial disparities in KS incidence and outcomes may be explained by adherence to HAART treatment. HAART treatment compliance and successful HAART treatment is less likely in African American patients as compared to in non-Hispanic White patients which may result in higher rates of HIV and HHV-8 co-infection.4,5 Consistent with prior studies, our findings indicate that, in the US, the incidence of KS is highest among Black patients, who are also more likely to be diagnosed at younger ages and experience the highest mortality rates.2,3 Furthermore, our study supports that this trend continues to 2018. We conclude that, in the United States, Black patients continue to experience a disproportionately high burden of KS. Future studies are needed to determine the underlying cause of this disparity so that it may be addressed by the US healthcare system.
IRB Approval Status
Data were extracted from the SEER-18 (2000–2018) database version 8.3.9. No ethical board approval was necessary because the SEER program provides open-access de-identified data. Furthermore, our research did not constitute human subjects research as per the Brown IRB guidelines as we completed a “Secondary analysis of anonymous data”.
Ethics Statement
Consent requirements were waived for this study as it is based on a publicly available database with anonymized and confidential patient information.
Acknowledgments
We would like to thank the Surveillance, Epidemiology, and End Results Program.
Funding
There is no funding to report.
Disclosure
Ms Ragi, Ms Moseley, Ms Ouellette, and Dr Rao declare that they have no conflicts of interest.
References
1. Cesarman E, Damian B, Krown SE, et al. Kaposi’s sarcoma. Nat Rev Dis Primers. 2019;5(1):9. doi:10.1038/s41572-019-0060-9
2. Datta GD, Kawachi I, Delpierre C, et al. Trends in Kaposi’s sarcoma survival disparities in the United States: 1980 through 2004. Cancer Epidemiol Biomarkers Prev. 2010;19(11):2718–2726. doi:10.1158/1055-9965.EPI-10-0307
3. Kumar V, Soni P, Garg R, et al. Racial disparities in incidence & survival of Kaposi’s sarcoma in the United States. Indian J Med Res. 2019;149(3):354–363. doi:10.4103/ijmr.IJMR_1436_17
4. Simoni JM, Huh D, Wilson IB, et al. Racial/Ethnic disparities in ART adherence in the United States: findings from the MACH14 study. J Acquir Immune Defic Syndr. 2012;60:466–472. doi:10.1097/QAI.0b013e31825db0bd
5. Eltom MA, Jemal A, Mbulaiteye SM, Devesa SS, Biggar RJ. Trends in Kaposi’s sarcoma and non-Hodgkin’s lymphoma incidence in the United States from 1973 through 1998. J Natl Cancer Inst. 2002;94(16):1204–1210. doi:10.1093/jnci/94.16.1204
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.