")
Back to Journals » Risk Management and Healthcare Policy » Volume 16
Hospital Work Conditions and the Mediation Role of Burnout: Residents and Practicing Physicians Reporting Adverse Events
Authors Jarrar M , Al-Bsheish M , Albaker W, Alsaad I, Alkhalifa E, Alnufaili S, Almajed N, Alhawaj R, Al-Hariri MT , Alsunni AA , Aldhmadi BK, Alumran A
Received 7 October 2022
Accepted for publication 12 December 2022
Published 5 January 2023 Volume 2023:16 Pages 1—13
DOI https://doi.org/10.2147/RMHP.S392523
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Kyriakos Souliotis
Mu’taman Jarrar,1,2 Mohammad Al-Bsheish,3,4 Waleed Albaker,5 Ibtihal Alsaad,2 Eiman Alkhalifa,2 Sara Alnufaili,2 Nour Almajed,2 Reem Alhawaj,2 Mohammad T Al-Hariri,6 Ahmed A Alsunni,6 Badr K Aldhmadi,7 Arwa Alumran8
1Medical Education Department, King Fahad Hospital of the University, Al-Khobar, Saudi Arabia; 2College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 3Health Management Department, Batterjee Medical College, Jeddah, Saudi Arabia; 4Al-Nadeem Governmental Hospital, Ministry of Health, Amman, Jordan; 5Department of Internal Medicine, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 6Department of Physiology, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 7Department of Health Management, College of Public Health and Health Informatics, University of Ha’il, Ha’il, Saudi Arabia; 8Health Information Management and Technology, College of Public Health, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia
Correspondence: Mu’taman Jarrar, Al-Khobar, 34445, Saudi Arabia, Tel +966 54 471 8523, Email [email protected]; [email protected] Mohammad Al-Bsheish, Jeddah, 21442, Saudi Arabia, Tel +966 59 103 6065, Email [email protected]
Background: “Patient Safety” in everyday practices is a target of healthcare leaders, and adverse events reported by healthcare providers directly reflect patient safety in the health system. Recognising how residents and practising physicians rate adverse events concerning their work conditions and burnout must be explored.
Objective: This study aims to explore the mediation effect of burnout dimensions (emotional exhaustion and burnout-interpersonal disengagement) between the effects of work conditions on perceived patient safety by exploring the adverse events that residents and practising physicians reported.
Methods: A quantitative and cross-sectional study collected data from 249 residents and practising physicians in a huge teaching hospital and primary health care centre (PHC) in the Eastern Province of Saudi Arabia. Hayes Macro regression analysis was employed to evaluate the multiple mediation effect of burnout dimensions, with 5000 bootstrapping and a confidence interval (CI) of 95% for statistical inference and p≤ 0.05 for the significance level.
Results: Leadership support (B= 0.39, t= 6.24, p< 0.001) and physician engagement (B=0.43, t=6.50, p< 0.001) were associated with a decreased rate of adverse events to patient safety, whereas workload (B=− 0.23, t=− 3.73, p< 0.001) was negatively associated with an increased rate of adverse events. Burnout was shown to mediate the relationship between the effects of physician’s leadership support (R2=0.26, F=27.50, p< 0.001), work engagement (R2=0.25, F=27.07, p< 0.001) and workload (R2=0.23, F=24.23, p< 0.001) on the rate of adverse events.
Conclusion: This study provides insights into burnout dimensions and their consequences on patient safety indicators (ie, adverse events). Work conditions (ie, leadership support, physician engagement, and workload) directly affect the rate of adverse events and indirectly through mediators like burnout-emotional exhaustion and burnout-interpersonal disengagement.
Keywords: leadership support, physician engagement, workload, burnout, adverse events, patient safety
Introduction
“Patient Safety” depends on healthcare science and everyday practice in different workplaces, offering a way to give care without creating negative impacts for patients under the care of the medical group. Since the Institute of Medicine (IOM) (currently, The National Academy of Medicine) released the report ‘To Err is Human’ in 1999, several initiatives have been established to prevent medical errors, improve patient safety and enhance population health.1–3 Nonetheless, the burden of preventable medical errors has substantially increased during the last two decades; around 98,000 patients die annually in the United States (US).4 Recently, up to 400,000 annual deaths in US hospitals were estimated to result from preventable adverse events.5 Adverse events were considered the third leading cause of death.6,7
In Saudi Arabia, a total of 3041 annual incidents were reported in 2008.8 Moreover, the number of medico-legal complaints in Saudi Arabia increased from 1165 cases in 2007 to 2413 cases in 2013.9 Most of these complaints were against physicians (88.4%).10 The rise in incidents that may jeopardise patient care provided by physicians in Saudi Arabia is alarming.
Responsively, several system reforms were initiated to transform the healthcare system in Saudi Arabia towards safer, and higher quality care in conformity with Vision 2030.11 Patient safety became a focus for system improvement, motivating research in this field. A healthy work condition is essential to enhance the performance of physicians.12 Different factors in the workplace have been found to influence care provided and patient safety (ie, leadership support, physician engagement and workload).
A growing literature has attempted to characterise the impacts of leadership support, physician engagement and workload on patient safety (ie, the incidence of adverse events). Interestingly, most of this literature has examined direct relationships. For instance, leadership support, physician engagement and workload were linked to the perceived care outcomes.13,14 Actively engaged physicians have a lower rate of medical errors.15 However, a high physician workload increases the risk of medical errors and jeopardises patient care.16 Good leadership support is expected to decrease physicians’ dissatisfaction and burnout, thus enhancing their performance.12 Physician involvement and supervisor support considerably affect a worker’s sense of encouragement17 and are associated with their performance.18
The investigation in this study sought to highlight the role of one pandemic psychological work distress, “burnout”, as an intervening factor between the three work conditions in the hospital and the reported adverse events among residents and practising physicians. Burnout was reported to be moderate to high among practising physicians.19 Theoretically, burnout has a significant bio-psychosocial impact,20,21 increasing job withdrawal22 and absenteeism rates.23 Additionally, burnout increases the likelihood of physician turnover, which has costs related to patient health.24 Burned-out physicians are at a higher risk of making poor decisions and medical errors that may jeopardise safety and quality of care.23,25 Furthermore, burnout results in serious consequences to patient health and safety and negatively impacts healthcare organisations.26 Therefore, the assumption is that physicians working in healthy work conditions might be less likely to have burnout, consequently improving their perceived patient safety. Despite some evidence, little is known regarding the role of residents and practising physicians’ burnout as a mechanism through which work conditions affect their perceived patient safety (ie, reported adverse events). Therefore, this study explores the mediation effect of burnout between these associations.
The Theoretical Framework
Studies in human factors have expanded the understanding of human interactions to improve healthcare systems.27–29 The theoretical framework of this study was built using social exchange theory30 and incorporating the model of Systems Engineering Initiative for Patient Safety (SEIPS).31 The social exchange theory concentrates on developing healthy workplace relationships between staff and their managers for the mutual benefit of staff and the institution.32 This encompasses the exchange benefit of providing healthy work conditions for residents and practising physicians, resulting in safer care.
The SEIPS model expands Donabedian’s theory of the quality of care,33 which categorises the components of the health system into structures, processes and outcomes. Donabedian theory supposes that structural input with quality processes leads to improved outcomes. Previous studies have used SEIPS to develop a model in the disciplines of education and healthcare to provide higher quality services.34,35 SEIPS considers human interactions with a work system and provides a better understanding of how physicians’ work conditions (leadership support, physician engagement, and workload) affect patient safety (See Figure 1). Leadership support, physician engagement and workload are structural factors, burnout dimensions (ie, emotional exhaustion and interpersonal disengagement) are processes, and patient safety is the outcome. Incorporating these theories can help better understand the role of physician burnout as a mechanism through which work conditions affect their perceived patient safety (ie, adverse events). Therefore, it advances the body of knowledge and provides insights for policymakers and hospital managers.
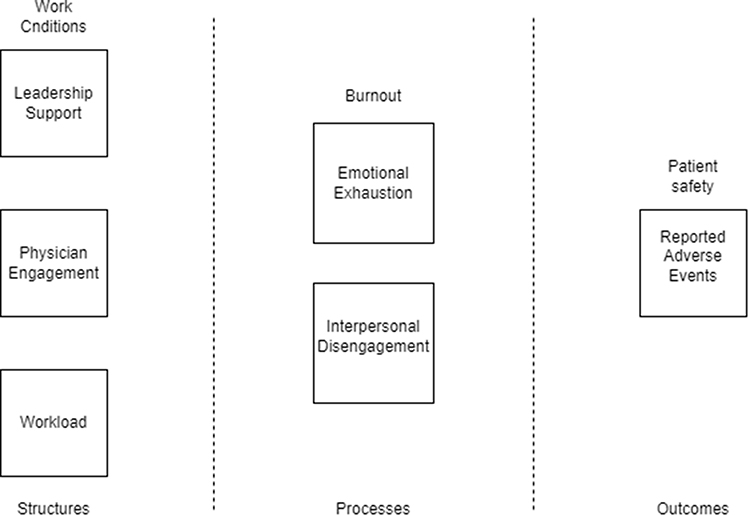 |
Figure 1 The theoretical framework of the study. Provided in a separate file with 300 dpi. |
Methodology
Materials and Methods
A cross-sectional study was conducted in a teaching hospital (with a capacity of 381 beds) and primary health care centre (PHC) in the Eastern Province of Saudi Arabia. The study population consisted of 722 residents and practising physicians, the total number of physicians working in the teaching hospital and PHC. Data were collected from January to March 2019. Inclusion criteria were the physicians who were working in the following departments: internal medicine, general surgery, paediatrics, obstetrics and gynaecology, anaesthesia and emergency medicine, in addition to the physicians working in the PHC. Medical students, interns, rotating residents and training residents from other departments or hospitals were excluded. Informed consent was obtained from all participants. The participants were informed about the study’s aims and that their response was voluntary. A sample size of 248 physicians was considered adequate based on Krejcie and Morgan’s table at a confidence interval of 95%.36 However, some may not participate; therefore, all residents and practicing physicians were invited. Of the 722 surveys distributed, 500 were returned, and 249 complete responses were obtained, achieving an effective response rate of 49.8%.
Ethical Consideration
The Declaration of Helsinki was followed in the conduct of this study. Ethical approval was obtained from the Institutional Review Board of Imam Abdulrahman Bin Faisal University (IRB number-UGS-2018-1-246) to explore the mediation effect of burnout on the association between work conditions and the reported adverse events among residents and practising physicians. Approvals to adopt the study instruments were obtained from the original authors.
Operational Definitions and Instruments
Leadership support refers to the support and empowerment given by a supervisor in the workplace for career development and decision-making,37 whereas physician engagement is a state of willingness, motivation, fulfilment, mental effectiveness and commitment to devote time and effort to healthcare improvement.38 The Practice Environment Scale (PES) tool was used to measure the perceived leadership support (manager’s ability, leadership and support subscale was adopted) and physician engagement (staff participation in hospital affairs sub-scale was adopted).39 This tool was developed originally to measure nurses’ perception of the work environment and has been internationally validated.40
Workload refers to the perceived physicians’ adequacy and duty hours’ length. Regarding workload, the Hospital Survey on Patient Safety Culture that the Agency for Health Care Research and Quality (AHRQ developed was used.41 The staffing section was adopted. This scale in this study was regarded as considering the adequacy of professionals to handle the work and work hours to ensure the best patient care.41
Burnout is a combination of emotional exhaustion and interpersonal disengagement. While emotional exhaustion refers to a state of depletion in emotional resources, being fatigued and unable to cope with job demands, interpersonal disengagement (depersonalisation) refers to being emotionally and cognitively detached and disengaged with a cynical attitude toward others.42,43 The Stanford Physicians Performance (Professional Fulfilment Index (PFI) was adopted for measuring perceived burnout.42 This index includes burnout (emotional exhaustion and interpersonal disengagement) and professional fulfilment subscales.42 The burnout, emotional exhaustion and interpersonal disengagement subscales were adopted, while the professional fulfilment was not, as it was not the aim of the present study. The PFI was adopted as the Maslach Burnout Inventory (MBI), and Oldenburg Burnout Inventory (OLBI), and the one-item burnout measure all provide an imperfect picture of physician burnout concerning patient care. The MBI may not be the best tool for evaluating changes brought on by interventions or other factors during periods less than a year because it requires a respondent to count the frequency of a feeling going back as long as a year. Although no time frame is mentioned in the Oldenburg Burnout Inventory instructions that should be considered when answering questions on burnout, the lack of a period anchor may make it more difficult to understand how scores vary over time.42 The one-item burnout is a dichotomous measure and is likely to lack the sensitivity to change that may be attained with continuous scale measurement.
Patient safety is the extent to which the hospital and healthcare system efficiently prevent adverse events.41 Adverse events are defined as unanticipated, preventable harm or negative outcomes related to patient hospital stays unrelated to his disease process.44 Incident reports, patient records, and the Global Trigger are the most often used instruments for quantifying and measuring adverse events in hospitals.45 However, only 10–20% of adverse events are reported in hospitals, and of those, 90–95% do not seriously harm patients.45 Additionally, the hospitals participating in our study did not grant access to their patient records or information system. Therefore, the current study employed a questionnaire, and physicians were asked to rate the frequency of coming across adverse events in their unit (eg, medical errors, patient falls, hospital-acquired infection and patient complaints). Responses were recorded using a 5-point Likert scale of the study instruments. The study items were adopted at the individual level of analysis.
Data Analysis Approach
Descriptive statistics, Cronbach’s alpha test and exploratory factor analysis were conducted for participants’ demographics and study questionnaire reliability and validity; respectively. Hayes Macro process regression analysis was performed to test for the mediation effect of burnout dimensions. Hayes Macro provides multiple mediation analyses of the burnout dimensions simultaneously and is superior to other approaches, such as Baron and Kenny’s casual step approach and Sobel’s test.46 It provides the indirect effect (a x b) by generating thousands of samples (Bootstrapping) to evaluate multiple mediators.47 A bootstrapping technique at 5000 (CI 95%) was used for statistical inference because it does not assume a normal distribution of responses as implied in Sobel’s test. Mediation effects were interpreted using the classification developed by Zhao et al48 Statistical significance was set at p-value ≤0.05, and Statistical Package for Social Sciences (SPSS) software version 23 was used to perform the analysis.
Results
Participants’ Demographics
Among the 249 physicians who responded to the questionnaire, 139 were males (55.8%), and 110 were females (44.2%) (Table 1). Most were 30 to 39 years old (44.2%), Saudi (67.5%), and married (80.7%). Furthermore, most participants were residents (37.8%) and consultants (34.9%), and nearly all of the respondents (99.2%) worked full-time. Practice experience mostly ranged from 5 to 9 years (25.7%), followed by 1 to 4 years (24.5%), and ≥15 years (23.7%). Physicians from general surgery, internal medicine, obstetrics, and gynaecology departments comprised comparable proportions of the total respondents at 20.1%, 19.7%, and 18%, respectively.
 |
Table 1 Demographics of Studied Participants |
Multivariate Assumptions, Cronbach’s Alpha and Factor Analysis
Multivariate assumptions, Cronbach’s alpha test for reliability and exploratory factor analysis for validity were performed.49 Multivariate assumptions indicated that the data were normal, linear, and free of heteroscedasticity and multicollinearity issues. Cronbach’s alpha results indicated a high level of internal consistency for survey items with a value of 0.85 for leadership support, 0.91 for physician engagement, 0.81 for workload, 0.88 for emotional exhaustion, 0.93 for Interpersonal disengagement and 0.89 for perceived patient safety. Further, factor analysis results with KMO (Kaiser Meyer Olkin) values of more than 0.90 and Bartlett’s significance value of 0.000,49,50 indicate the study sample and instrument were adequate and valid to examine the mediation effect of burnout dimensions between the effect of leadership support, physician engagement, and workload on the perceived patient safety among physicians.
The Mediation Effect of Burnout
The results of “a path” revealed the effect of the independent variables on the mediator. The results, as shown in Table 2 and Figure 2, revealed that leadership support negatively affected burnout-emotional exhaustion (B=−0.53, t=−6.83, p<0.001) and burnout-interpersonal disengagement (B=−0.43, t=−6.16, p<0.001) and was statistically significant. Similarly, physician engagement had a significant negative effect on burnout-emotional exhaustion (B=- 0.67, t=−8.36, p<0.001) and burnout-interpersonal disengagement (B=−0.50, t=−6.74, p<0.001). In contrast, workload positively affected both dimensions of burnout with a larger effect on emotional exhaustion (B=0.48, t=6.39, p<0.001) than on interpersonal disengagement (B=0.15, t=2.08, p<0.05). Leadership support and physician engagement decreased physician burnout, while workload increased the risk of burnout among physicians.
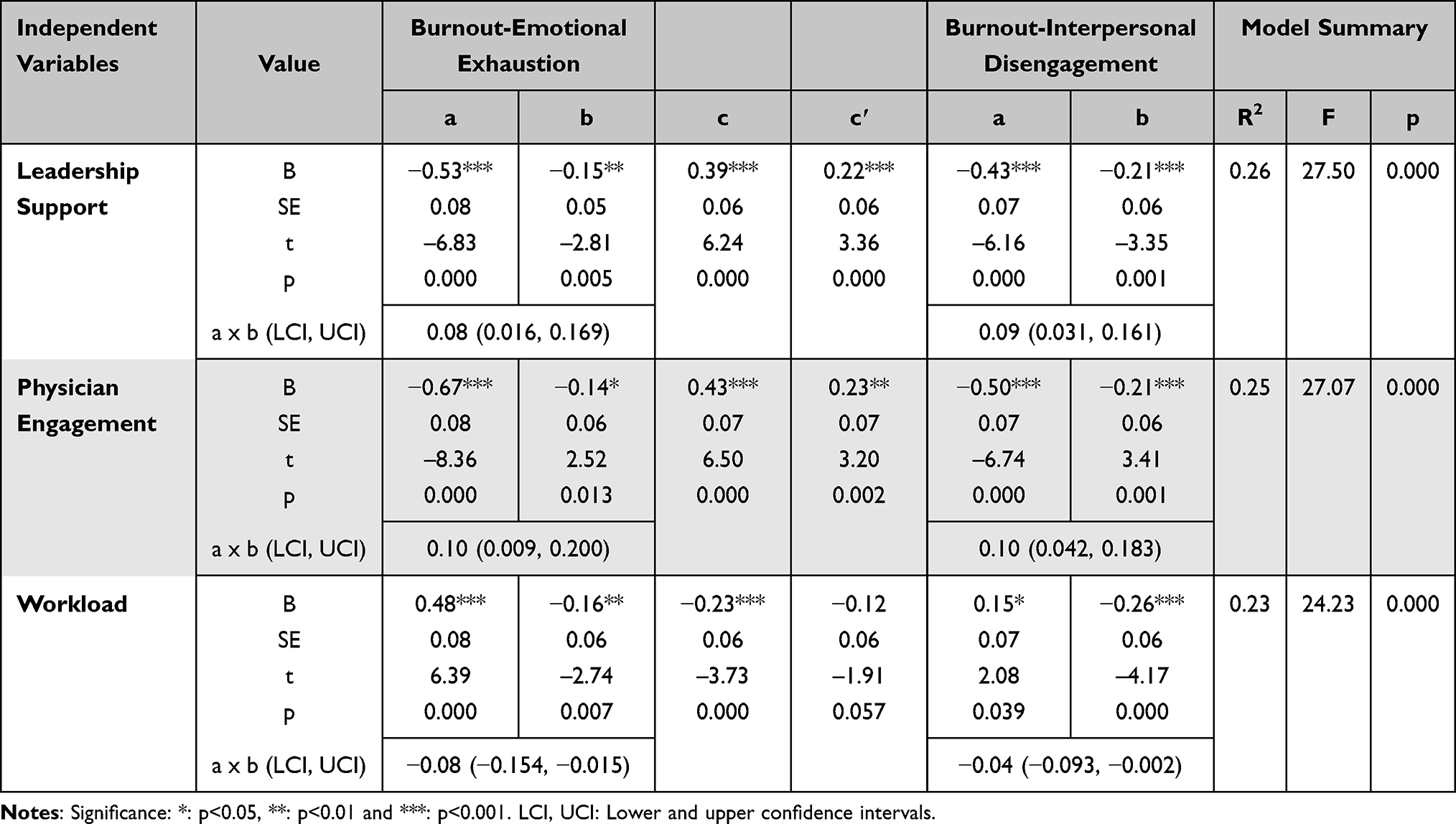 |
Table 2 The Mediation Effect of Burnout Dimensions Between the Effect of Leadership Support, Physician Engagement and Workload on the Residents and Practising Physicians Reported Adverse Events |
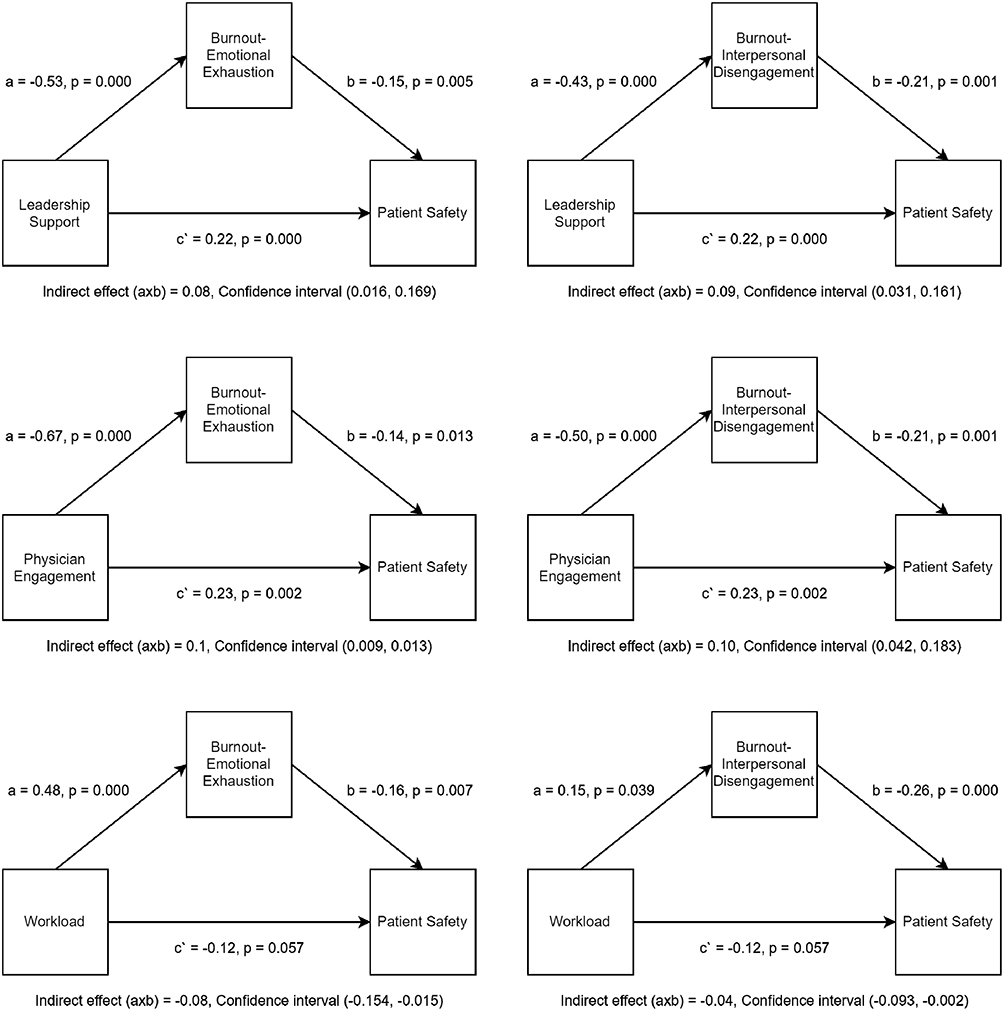 |
Figure 2 The mediation effect of burnout-emotional exhaustion and interpersonal disengagement in the relationship between work conditions and physicians reported adverse events. Provided in a separate file with 300 dpi. |
The results of “c paths” revealed the effect of the independent variables on the dependent variable. The results, as shown in Table 2, revealed that leadership support (B= 0.39, t= 6.24, p<0.001) and physician engagement (B=0.43, t=6.50, p<0.001) positively affected residents and practising physicians reported adverse events. Whereas workload (B=−0.23, t=−3.73, p<0.001) negatively affected residents and practising physicians reported adverse events.
The indirect effect (a x b paths) and the model summary of Hayes Macro regression analysis, as shown in Table 2, revealed that burnout dimensions mediate the relationships between the effects of leadership support (R2=0.26, F=27.50, p<0.001), physician engagement (R2=0.25, F=27.07, p<0.001) and workload (R2=0.23, F=24.23, p<0.001) on the perceived patient safety (residents and practising physicians reported adverse events). The indirect effect (a x b paths), as shown in Figure 2, revealed that burnout-emotional exhaustion (95% CI; 0.016, 0.169) and burnout-interpersonal disengagement (95% CI; 0.031, 0.161) significantly mediated the effect of leadership support on patient safety, where the confidence intervals do not straddle zero. Similarly, the mediation effects of burnout-emotional exhaustion (95% CI; 0.009, 0.200) and burnout-interpersonal disengagement (95% CI; 0.042,0.183) between the effect of physician engagement and patient safety are significant. Because the “a, b and c′ paths” point towards different directions,48 burnout dimensions act as competitive variables in both relationships. Therefore, resident and practising physician burnout suppressed the positive impacts of leadership support and physician engagement on perceived patient safety.
On the other hand, the results revealed that burnout-emotional exhaustion (95% CI; −0.154, −0.015) and burnout-interpersonal disengagement (95% CI; −0.093, −0.002) complement the relationship between workload and patient safety where “a, b and c′ paths” are all pointing towards the same direction.48 Because the effect of the c′ path was insignificant (p>0.05), the effect of workload on patient safety can be considered fully mediated through burnout dimensions. In other words, physicians with high workloads are more prone to burnout, affecting their perceived patient safety.
These results revealed a dual function of burnout dimensions, suppressing the positive impact of leadership support and physician engagement and complementing the effect of workload on the residents and practising physicians who reported adverse events. These findings support the study’s claim that burnout dimensions mediate the relationship between physician work conditions on perceived patient safety.
Discussion
Improving the current work conditions for caregivers has gained international attention, and we found that physicians perceived patient safety (ie, reported adverse events) was directly affected by their work conditions (leadership support, physician engagement, and workload) and indirectly through mediators like burnout dimensions (ie, emotional exhaustion and burnout-interpersonal disengagement).
The findings of this study revealed that respondents perceived patient safety (ie, reported adverse events) as being directly affected by their work conditions (leadership support, physician engagement, and workload) and indirectly through mediators like burnout dimensions (ie, emotional exhaustion and burnout-interpersonal disengagement). To our knowledge, this study is the first to investigate the mediation effect of burnout dimensions between the association of work conditions and the perceived patient safety (ie, reported adverse events) among residents and practising physicians in the KSA. Furthermore, the first of its kind incorporating the model of SEIPS and the social exchange theory. Multiple significant associations and mediation relationships were found.
The direct associations in this study revealed that leadership support and physician engagement were significantly associated with better perceived patient safety. At the same time, physicians with high workloads reported lower patient safety perception ratings (more frequently came across adverse events) in their respective units.
These direct associations with patient safety are well established in previous studies. Leadership support has positive effects on patient safety perception.51 Leadership was found to improve the sense of empowerment, which decreased the rate of adverse events and improved patient safety.52 Health providers who received more support from their leaders had a higher rating of patient safety perception.53 Therefore, physician engagement was found to positively affects patient safety by enabling the physicians to participate in hospital affairs.54–56 These findings were supported by the National Health Service (NHS), which reported a growing need to engage physicians in the planning, improvement and effective achievement of healthcare services.57 Hence, enabled, and actively engaged physicians in planning and the improvement process are associated with their performance58 and, Therefore, less likely to come across adverse events.
Furthermore, previous studies revealed that workload decreased patient safety scores, increased readmission rates, and reduced exposure to harm.59–62 In the current study, this significant association was observed through the indirect effect while not in the direct effect (c′ path). One study demonstrated a similar finding in which increased workload was not found to impair patient safety.43 Therefore, intervening factors can explain these inconsistencies by understanding the mediation role of burnout. Thus, patient safety is affected by a physician’s work conditions and physician-manager interpersonal relationships and by intervening process factors such as physician burnout.
Several studies have explored the relationship between burnout and patient safety.63–65 However, burnout in the current study is a crucial mediator between work conditions and resident and practising physicians’ perceived patient safety (ie, reported adverse events). The results revealed a significant mediation effect of burnout dimensions (ie, emotional exhaustion and burnout-interpersonal disengagement) between work conditions (ie, leadership support, physician engagement, and workload) and perceived patient safety. Hospital physician burnout suppresses the positive impact of leadership support and physician engagement on perceived patient safety and complements the relationship between workload and patient safety.
Even though limited studies have examined the mediation effect of physician burnout between work conditions and patient safety, previous research can justify these results. In the telecommunication industry, favourable work conditions reduce employee exhaustion and interpersonal disengagement, reducing their intention to leave.66 Employees that have supportive leaders and pleasant work conditions have noticeably greater levels of job satisfaction.67 Effective supervision and empowerment have been proven to enhance commitment to safety and reduce unfavourable outcomes.52,68–71 Studies have demonstrated that an increase in manager support decreases burnout72,73 by improving the work environment.55 Likewise, physician engagement is increasingly viewed as a counteractive mechanism against burnout.74 Less engaged physicians have higher levels of burnout;23 Actively engaged physicians rarely encounter adverse events.15 Leadership support and work engagement in the healthcare system are essential, especially for residents and practising physicians whose duty is to deliver direct care to achieve a desirable, safe and effective patient outcome.54,75,76
Efforts and system reforms were initiated to transform the healthcare system in Saudi Arabia towards safer and higher quality care in conformity with Vision 2030.11 However, the current study revealed that workload among physicians increases their perceived burnout, emotional exhaustion and interpersonal disengagement, which in turn significantly affects their perceived patient safety. Consistent with previous studies working long shifts and staffing inadequacy was found to be indirectly related to patient safety.77,78 Inadequate staffing increased the workload on individual workers and burnout.79,80 In turn, burnout was independently associated with a lower perceived patient safety.23,43,73 Therefore, burnout should be incorporated alongside work conditions when addressing the issue of patient safety. Leadership support and physician engagement improved perceived patient safety by reducing burnout, whereas increased workload decreased it through increasing burnout.
An important lesson from this study is that without focusing on human interactions in work systems, preventing patient harm and improving patient safety would not be possible. This study’s model expands the social exchange theory and supports the SEIPS model. The social exchange theory concentrates on developing healthy workplace relationships between staff and their managers for mutual benefit,58 and we expanded it by including physician’s burnout as an intervening process variable. The third generation of the SEIPS model was focused on the patient journey, and it introduced the concept of human-centred design as a core concept for improving patient safety.27 We support and expand this model. We can introduce the concept of a “person-centred journey” by focusing on both the staff and patient, ensuring healthy work conditions and providing appropriate support for engaging physicians to support mutual interactions (work system and patient-physician interactions). Human-centred design must focus on patient and staff journeys to improve patient safety.
Furthermore, integrating the SEIPS model into the social exchange theory can advance the knowledge of the human mutual benefits and interactions. High quality input (structures) does not necessarily lead to the provision of quality outcomes, as intervening factors could suppress or complement the relationships. In the current study hospital physician burnout suppresses the positive impact of leadership support and physician engagement on perceived patient safety and complements the relationship between workload and patient safety.
Furthermore, this study has practical implications for healthcare leaders as they encourage engaging the residents’ physicians in hospital affairs and providing the necessary support. Considering the workload as a major concern to increase physician burnout, managers must restructure duty length and scheduling and maintain adequate staffing levels. Furthermore, continuous quality improvement by opening the discussion with healthcare workers must be routinely conducted; this will overcome job obstacles. Policymakers must devote resources to frequent audits and train future leaders to decrease adverse events and improve the quality of care provided by physicians.
Study Limitations
Although several findings could be added to the literature, this study has limitations. The study design was cross-sectional, and participants were sampled from a single university hospital and PHC, so a causal relationship and generalizability cannot be established. Although residents and practising physicians were involved, the participation of other healthcare workers would enable better conceptualisation of the interaction between different factors in the work environment. Moreover, the differences in the variables between those physicians from different departments might have influenced the overall value of the results. Furthermore, residents and practising physicians responded voluntarily, and 249 of the 722 were provided data for this study as complete responses. Thus, it is possible that selection bias may make their responses not truly representative. Importantly, patient safety was measured from a physician’s perspective via a questionnaire (rate the frequency of coming across adverse events), which might introduce bias; therefore, objective data from the hospital records are needed to determine actual associations in the study model.
Future Directions
There are two directions for future research. First, there is a need to characterise the effect of burnout on patient safety using an objective measure for actual adverse event rates and the effect from the patient perspective. The second is to involve other outcome measures such as patient outcomes, care quality, job satisfaction, and intention to leave to understand the study model better and help optimise physician well-being. Furthermore, future patient safety studies must be influenced by dynamic work conditions within healthcare organisations, including other structural factors, such as collegial relations, task complexity, technologies, and physical environment. Multi-centred studies would be more generalisable. Longitudinal designs should also be considered to record changes in variables over time.
Conclusion
This study is the first of its kind incorporating the model of SEIPS and the social exchange theory to investigate the mediation effect of burnout dimensions between the association of work conditions and perceived patient safety. This study has provided new insights regarding the effect of burnout dimensions and their consequences on patient safety. Furthermore, this study sheds light on the effect of work conditions on patient safety and how burnout influences this relationship. Burnout dimensions have dual roles, and they suppress the positive impact of leadership support and physician engagement and complement the effect of workload on perceived patient safety. Supported and engaged physicians reported lower perceived burnout, which, in turn, increased their perceived patient safety. At the same time, physicians with high workloads are more prone to burnout, which decreases patient safety. It highlighted the importance of human interactions and introduced the concept of a person-centred journey to prevent patient harm and improve patient safety. A multifaceted approach between the individual and the healthcare organisation is required to optimise patient safety and the quality of care and improve physician well-being.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Parikh K, Keller S, Ralston S. Inpatient quality improvement interventions for asthma: a meta-analysis. Pediatrics. 2018;141(5):e20173334. doi:10.1542/peds.2017-3334
2. World Health Organization. Guidance on developing quality and safety strategies with a health system approach; 2008. Available from: http://www.euro.who.int/__data/assets/pdf_file/0011/96473/E91317.pdf.
3. Brusaferro S, Arnoldo L, Finzi G, et al. Hospital hygiene and infection prevention and control in Italy: state of the art and perspectives. Ann Ig. 2018;30(November):1–6. doi:10.7416/ai.2018.2245
4. IOM. To Err is Human: Bulding a Safer Health System. Washington DC: National Academy Press; 1999.
5. James JT. A new, evidence-based estimate of patient harms associated with hospital care. J Patient Saf. 2013;9(3):122–128. doi:10.1097/PTS.0b013e3182948a69
6. Makary MA, Daniel M. Medical error-The third leading cause of death in the US. BMJ. 2016;353(May):1–5. doi:10.1136/bmj.i2139
7. Jarrar M, Al-Bsheish M, Dardas LA, Meri A, Sobri Minai M. Adverse events in Malaysia: associations with nurse’s ethnicity and experience, hospital size, accreditation, and teaching status. Int J Health Plann Manage. 2020;35(1):104–119. doi:10.1002/hpm.2822
8. Arabi Y, Alamry A, Al Owais SM, Al-Dorzi H, Noushad S, Taher S. Incident reporting at a tertiary care hospital in Saudi Arabia. J Patient Saf. 2012;8(2):81–87. doi:10.1097/PTS.0b013e31824badb7
9. Bin GU, Ahmed SM, Faraz A. a review of the frequency of medical error in Saudi Arabia: an emerging concern. J Evid Based Med Health Care. 2015;2(52):8692–8695. doi:10.18410/jebmh/2015/1205
10. Alkhenizan AH, Shafiq MR. The process of litigation for medical errors in Saudi Arabia and the United Kingdom. Saudi Med J. 2018;39(11):1075–1081. doi:10.15537/smj.2018.11.22854
11. MOH. Vision realization office - vision, mission and goals web site; 2018. Available from: https://www.moh.gov.sa/en/Ministry/vro/Pages/default.aspx.
12. Rama-Maceiras P, Parente S, Kranke P. Job satisfaction, stress and burnout in anaesthesia: relevant topics for anaesthesiologists and healthcare managers? Eur J Anaesthesiol. 2012;29(7):311–319. doi:10.1097/EJA.0b013e328352816d
13. Van Bogaert P, Timmermans O, Weeks SM, van Heusden D, Wouters K, Franck E. Nursing unit teams matter: impact of unit-level nurse practice environment, nurse work characteristics, and burnout on nurse reported job outcomes, and quality of care, and patient adverse events-A cross-sectional survey. Int J Nurs Stud. 2014;51(8):1123–1134. doi:10.1016/j.ijnurstu.2013.12.009
14. Al-mugheed K, Bayraktar N, Al-bsheish M, Alsyouf A, Jarrar M. Patient safety attitudes among doctors and nurses: associations with workload, adverse events, experience. Health Care. 2022;2022:1–12.
15. Prins JT, Van Der Heijden FMMA, Hoekstra-Weebers JEHM, et al. Burnout, engagement and resident physicians’ self-reported errors. Psychol Heal Med. 2009;14(6):654–666. doi:10.1080/13548500903311554
16. Wingo MT, Halvorsen AJ, Beckman TJ, Johnson MG, Reed DA. Associations between attending physician workload, teaching effectiveness, and patient safety. J Hosp Med. 2016;11(3):169–173. doi:10.1002/jhm.2540
17. Hopkins J, Fassiotto M, Ku MC, Mammo D, Valantine H. Designing a physician leadership development program based on effective models of physician education. Health Care Manage Rev. 2018;43(4):293–302. doi:10.1097/HMR.0000000000000146.Designing
18. Alswat K, Abdalla RAM, Titi MA, et al. Improving patient safety culture in Saudi Arabia (2012–2015): trending, improvement and benchmarking. BMC Health Serv Res. 2017;17(1):1–14. doi:10.1186/s12913-017-2461-3
19. Vargas M, Spinelli G, Buonanno P, Iacovazzo C, Servillo G, De Simone S. Burnout among anesthesiologists and intensive care physicians: results from an Italian national survey. Inq. 2020;57:0–4. doi:10.1177/0046958020919263
20. Privitera RM. Addressing human factors in burnout and the delivery of healthcare: quality & safety imperative of the quadruple AIM. Health. 2018;10(5):629–644. doi:10.4236/health.2018.105049
21. Huang J. Changes of job burnout in chinese nurses over 2004–2013: cross-temporalmeta-analysis. Curr Psychol. 2018;37(3):583–590. doi:10.1007/s12144-016-9540-1
22. Rabatin J, Williams E, Baier Manwell L, Schwartz MD, Brown RL, Linzer M. Predictors and outcomes of burnout in primary care physicians. J Prim Care Community Health. 2016;7(1):41–43. doi:10.1177/2150131915607799
23. Dewa CS, Loong D, Bonato S, Trojanowski L. The relationship between physician burnout and quality of healthcare in terms of safety and acceptability: a systematic review. BMJ Open. 2017;7:6. doi:10.1136/bmjopen-2016-015141
24. Misra-Hebert AD, Kay R, Stoller JK. A review of physician turnover: rates, causes, and consequences. Am J Med Qual. 2004;19(2):56–66. doi:10.1177/106286060401900203
25. Klein J, Grosse Frie K, Blum K, von Dem Knesebeck O. Burnout and perceived quality of care among German clinicians in surgery. Int J Qual Heal Care. 2010;22(6):525–530. doi:10.1093/intqhc/mzq056
26. Rathert C, Williams ES, Lawrence ER, Halbesleben JRB. Emotional exhaustion and workarounds in acute care: cross sectional tests of a theoretical framework. Int J Nurs Stud. 2012;49(8):969–977. doi:10.1016/j.ijnurstu.2012.02.011
27. Carayon P, Wooldridge A, Hoonakker P, Hundt AS, Kelly MM. SEIPS 3.0: human-centered design of the patient journey for patient safety. Appl Ergon. 2020;84(December2018):103033. doi:10.1016/j.apergo.2019.103033
28. Holden RJ, Carayon P, Gurses AP, et al. SEIPS 2.0: a human factors framework for studying and improving the work of healthcare professionals and patients. Ergonomics. 2013;56(11):1669–1686. doi:10.1080/00140139.2013.838643
29. Lowndes BR, Forsyth KL, Blocker RC, et al. NASA-TLX assessment of surgeon workload variation across specialties. Ann Surg. 2020;271(4):686–692. doi:10.1097/SLA.0000000000003058
30. Blau M, Blau PM. Exchange and Power in Social Life. Am Sociol Rev. 1965;30(5):789–790. doi:10.2307/2091154
31. Carayon P, Schoofs Hundt A, Karsh BT, et al. Work system design for patient safety: the SEIPS model. Qual Saf Heal Care. 2006;15(SUPPL. 1):50–59. doi:10.1136/qshc.2005.015842
32. Cole MS, Schaninger WS, Harris SG. The workplace social exchange network: a multilevel, conceptual examination. Gr Organ Manag. 2002;27(1):142–167. doi:10.1177/1059601102027001008
33. Donabedian A. Evaluating the quality of medical care. 1966. Milbank Q. 2005;83(4):691–729. doi:10.1111/j.1468-0009.2005.00397.x
34. Jarrar M, Al-Bsheish M, Aldhmadi BK, et al. Effect of practice environment on nurse reported quality and patient safety: the mediation role of person-centeredness. Health Care. 2021;9(11):1–17. doi:10.3390/healthcare9111578
35. Jarrar M, Bakr R, Al-bsheish M, Albaker W, Alumran A. Students’ perception of quality of learning experience (structure, process and outcome): discipline versus problem based medical curriculum and the mediation role of process quality. Health Care. 2022;2022:1–10.
36. Draugalis JLR, Plaza CM. Best practices for survey research reports revisited: implications of target population, probability sampling, and response rate. Am J Pharm Educ. 2009;73(8):2–4. doi:10.5688/aj7308142
37. McAuliffe E, Bowie C, Manafa O, et al. Measuring and managing the work environment of the mid-level provider – the neglected human resource. Hum Resour Health. 2009;7(1):1–9. doi:10.1186/1478-4491-7-13
38. Schaufeli WB, Bakker AB, Salanova M. The measurement of work engagement with a short questionnaire: a cross-national study. Educ Psychol Meas. 2006;66(4):701–716. doi:10.1177/0013164405282471
39. Lake E. Development of the practice environment scale of the nursing work index. Res Nurs Health. 2002;25(3):176–188. doi:10.1002/nur.10032
40. Parker D, Tuckett A, Eley R, Hegney D. Construct validity and reliability of the practice environment scale of the nursing work index for queensland nurses. Int J Nurs Pract. 2010;16(4):352–358. doi:10.1111/j.1440-172X.2010.01851.x
41. Sorra J, Gray L, Streagle S, Famolaro T, Yount N, Behm J. AHRQ hospital survey on patient safety culture: user’s guide; 2016.
42. Trockel M, Bohman B, Lesure E, et al. A brief instrument to assess both burnout and professional fulfillment in physicians: reliability and validity, including correlation with self-reported medical errors, in a sample of resident and practicing physicians. Acad Psychiatry. 2018;42(1):11–24. doi:10.1007/s40596-017-0849-3
43. Welp A, Meier LL, Manser T. Emotional exhaustion and workload predict clinician-rated and objective patient safety. Front Psychol. 2014;5(OCT):1–13. doi:10.3389/fpsyg.2014.01573
44. Weingart SN, Zhu J, Chiappetta L, et al. Hospitalised patients’ participation and its impact on quality of care and patient safety. Int J Qual Health Care. 2011;23(3):269–277. doi:10.1093/intqhc/mzr002
45. Griffin F, Resar R IHI global trigger tool for measuring adverse events; 2009.
46. Hayes AF. An Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach.
47. MacKinnon DP, Lockwood CM, Hoffman JM, West SG, Sheets V. A comparison of methods to test mediation and other intervening variable effects. Psychol Methods. 2002;7(1):83–104. doi:10.1037//1082-989X.7.1.83
48. Zhao X, Lynch JG, Chen Q. Reconsidering baron and kenny: myths and truths about mediation analysis. J Consum Res. 2010;37(2):197–206. doi:10.1086/651257
49. Stevens JP. Applied Multivariate Statistics for the Social Sciences.
50. Tabachnick B, Fidell L. Using Multivariate Statistics.
51. Mattson M, Hellgren J, Göransson S. Leader communication approaches and patient safety: an integrated model. J Safety Res. 2015;53:53–62. doi:10.1016/j.jsr.2015.03.008
52. Boamah SA, Laschinger HKS. Effect of transformational leadership on job satisfaction and patient safety outcomes. Nurs Outlook. 2018;66(2):180–189. doi:10.1016/j.outlook.2017.10.004
53. Ammouri AA, Tailakh AK, Muliira JK, Geethakrishnan R, Al Kindi SN. Patient safety culture among nurses. Int Nurs Rev. 2015;62(1):102–110. doi:10.1111/inr.12159
54. Loerbroks A, Glaser J, Vu-Eickmann P, Angerer P. Physician burnout, work engagement and the quality of patient care. Occup Med. 2017;67(5):356–362. doi:10.1093/occmed/kqx051
55. Spaulding A, Gamm L, Menser T. Physician Engagement: strategic considerations among leaders at a major health system. Hosp Top. 2014;92(3):66–73. doi:10.1080/00185868.2014.937970
56. Bakker AB, Demerouti E, Sanz-Vergel AI. Burnout and work engagement: the JDR approach. Annu Rev Organ Psychol Organ Behav. 2014;1(July):389–411. doi:10.1146/annurev-orgpsych-031413-091235
57. Spurgeon P, Mazelan PM, Barwell F. Medical engagement: a crucial underpinning to organisational performance. Heal Serv Manag Res. 2011;24:114–120.
58. Goldstein SM, Ward PT. Performance effects of physicians’ involvement in hospital strategic decisions. J Serv Res. 2004;6(4):361–372. doi:10.1177/1094670503262953
59. Sturm H, Rieger MA, Martus P, et al. Do perceived working conditions and patient safety culture correlate with objective workload and patient outcomes: a cross-sectional explorative study from a German university hospital. PLoS One. 2019;14(1):1–19. doi:10.1371/journal.pone.0209487
60. Lee A, Cheung YSL, Joynt GM, Leung CCH, Wong WT, Gomersall CD. Are high nurse workload/staffing ratios associated with decreased survival in critically ill patients? A cohort study. Ann Intensive Care. 2017;7:1. doi:10.1186/s13613-017-0269-2
61. Park SH, Boyle DK, Bergquist-Beringer S, Staggs VS, Dunton NE. Concurrent and lagged effects of registered nurse turnover and staffing on unit-acquired pressure ulcers. Health Serv Res. 2014;49(4):1205–1225. doi:10.1111/1475-6773.12158
62. Wen J, Cheng Y, Hu X, Yuan P, Hao T, Shi Y. Workload, burnout, and medical mistakes among physicians in China: a cross-sectional study. Biosci Trends. 2016;10(1):27–33. doi:10.5582/bst.2015.01175
63. Tawfik DS, Profit J. Provider burnout: implications for our perinatal patients. Semin Perinatol. 2020;44:4. doi:10.1016/j.semperi.2020.151243
64. Salyers MP, Bonfils KA, Luther L, et al. The relationship between professional burnout and quality and safety in healthcare: a meta-analysis. J Gen Intern Med. 2017;32(4):475–482. doi:10.1007/s11606-016-3886-9
65. Panagioti M, Geraghty K, Johnson J, et al. Association between physician burnout and patient safety, professionalism, and patient satisfaction: a systematic review and meta-analysis. JAMA Intern Med. 2018;178(10):1317–1330. doi:10.1001/jamainternmed.2018.3713
66. Jyoti J, Rani A. Role of burnout and mentoring between high performance work system and intention to leave: moderated mediation model. J Bus Res. 2019;98(December2018):166–176. doi:10.1016/j.jbusres.2018.12.068
67. Bakr RH, Jarrar MK, Abumadini MS, Al S, Larbi EB. Effect of leadership support, work conditions and job security on job satisfaction in a medical college. Saudi J Med Med Sci. 2019. doi:10.4103/sjmms.sjmms
68. Al-Bsheish MA, Mustafa M, Ismail MA. Enhancing safety performance by recognising the role of perceived management commitment to safety in Jordanian healthcare Industry: conceptual framework. Int J Bus Soc Res. 2017;07(01):1–10.
69. Al-Bsheish M, Bin Mustafa M, Ismail M, Jarrar M, Meri A, Dauwed M. Perceived management commitment and psychological empowerment: a study of intensive care unit nurses’ safety. Saf Sci. 2019;118(April):632–640. doi:10.1016/j.ssci.2019.05.055
70. Wagner A, Rieger MA, Manser T, et al. Healthcare professionals’ perspectives on working conditions, leadership, and safety climate: a cross-sectional study. BMC Health Serv Res. 2019;19(1):1–14. doi:10.1186/s12913-018-3862-7
71. Al-Bsheish M, Jarrar M, Mustafa M, Azril M, Meri A, Dauwed M. ICU nurses’ safety performance related to respect for safety and management commitment: a cross- sectional study. Contemp Nurse. 2022;1–23. doi:10.1080/10376178.2022.2104740
72. Shanafelt TD, Gorringe G, Menaker R, et al. Impact of organisational leadership on physician burnout and satisfaction. Mayo Clin Proc. 2015;90(4):432–440. doi:10.1016/j.mayocp.2015.01.012
73. Lewis HS, Cunningham CJL. Linking nurse leadership and work characteristics to nurse burnout and engagement. Nurs Res. 2016;65(1):13–23. doi:10.1097/NNR.0000000000000130
74. Kumar S. Burnout and doctors: prevalence, prevention and intervention. Healthcare. 2016;4(3):37. doi:10.3390/healthcare4030037
75. Halbesleben JRB, Wheeler AR. The relative roles of engagement and embeddedness in predicting job performance and intention to leave. Work Stress. 2008;22(3):242–256. doi:10.1080/02678370802383962
76. Milliken AD. Physician engagement: a necessary but reciprocal process. Can Med Assoc J. 2014;186(4):244–245. doi:10.1503/cmaj.131178
77. Jarrar M, Rahman HA, Minai MS, AbuMadini MS, Larbi M. The function of patient-centered care in mitigating the effect of nursing shortage on the outcomes of care. Int J Health Plann Manage. 2018;(August 2017):1–10. doi:10.1002/hpm.2491
78. Jarrar M, Minai MS, Al-Bsheish M, Meri A, Jaber M. Hospital nurse shift length, patient-centered care, and the perceived quality and patient safety. Int J Health Plann Manage. 2018. doi:10.1002/hpm.2656
79. Chambers CNL, Frampton CMA, Barclay M, McKee M. Burnout prevalence in New Zealand’s public hospital senior medical workforce: a cross-sectional mixed methods study. BMJ Open. 2016;6(11):1–10. doi:10.1136/bmjopen-2016-013947
80. Gregory ME, Russo E, Singh H. Electronic health record alert-related workload as a predictor of burnout in primary care providers. Appl Clin Inform. 2017;8(3):686–697. doi:10.4338/ACI-2017-01-RA-0003
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.