Back to Journals » Nature and Science of Sleep » Volume 18

The Efficacy of Therapist-Guided, Internet-Delivered Mindfulness-Based Cognitive Therapy for Chronic Insomnia Disorder: A Randomized Controlled Trial
Authors Zeng Z ![]() , Jiang J, Xie K, Luo N, Guan X, Zhu C, Lu Z, Huang L
, Jiang J, Xie K, Luo N, Guan X, Zhu C, Lu Z, Huang L
Received 13 November 2025
Accepted for publication 16 January 2026
Published 4 February 2026 Volume 2026:18 578770
DOI https://doi.org/10.2147/NSS.S578770
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Zixuan Zeng,1,2,* Jiahui Jiang,1,2,* Kun Xie,3 Na Luo,1 Xiaofeng Guan,2 Chenyi Zhu,1 Zheng Lu,2 Lei Huang2
1School of Medicine, Tongji University, Shanghai, 200331, People’s Republic of China; 2Department of Psychiatry, Tongji Hospital, School of Medicine, Tongji University, Shanghai, 200065, People’s Republic of China; 3Mental Health Education and Counseling Center, University of Shanghai for Science and Technology, Shanghai, 200093, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zheng Lu, Department of Psychiatry, Tongji Hospital, School of Medicine, Tongji University, Shanghai, 200065, People’s Republic of China, Email [email protected] Lei Huang, Department of Psychiatry, Tongji Hospital, School of Medicine, Tongji University, Shanghai, 200065, People’s Republic of China, Email [email protected]
Purpose: Chronic Insomnia Disorder (CID) is prevalent, yet access to effective treatments is limited. Integrating mindfulness with Cognitive Behavioral Therapy for Insomnia (CBT-I) in an accessible online format may fill this gap. This study evaluated the efficacy of a therapist-guided, internet-delivered Mindfulness-Based Cognitive Therapy for Insomnia (iMBCT-I), which has been scarcely investigated.
Patients and Methods: In this open-label, parallel-group randomized trial, 82 participants with CID were assigned to the 8-week of iMBCT-I group (n = 41) or a control group receiving a single online session of sleep hygiene education (SHE, n = 41). The primary outcomes were insomnia severity assessed with Insomnia Severity Index (ISI) and insomnia remission (ISI < 8) rate. Secondary outcomes included sleep quality, sleep diary and actigraphy parameters, depressive and anxious symptoms, and quality of life. The primary and the follow-up time-points were week 8 and week 20, respectively. Statistical analyses followed the intention-to-treat principle.
Results: No serious adverse events were reported. At week 8, the ISI score in the iMBCT-I group showed a significant decrease compared to the SHE group [mean difference, 95% confidence intervals (CI) = 4.00 (2.22, 5.78), p < 0.001, Cohen’s d, 95% CI = 0.99 (0.53, 1.45)]. More participants achieved insomnia remission in the iMBCT-I group [odds ratio, 95% CI = 6.21 (2.24, 17.23), p < 0.001]. The iMBCT-I was also superior on improving sleep quality, sleep onset latency, wakefulness after sleep onset, sleep efficiency, rapid eye movement duration, depressive symptoms and both physical and mental quality of life (all p < 0.05). Linear mixed-effects model showed the maintenance of these effects at the 20-week follow-up for most outcomes.
Conclusion: Therapist-guided iMBCT-I is effective in reducing insomnia severity in adults with CID with benefits sustained for 20 weeks.
Trial Registration: This study has been registered with the Chinese Clinical Trial Registry https://www.chictr.org.cn/ (Registration Number: ChiCTR2400084300).
Keywords: cognitive behavioral therapy, insomnia, mindfulness, randomized controlled trial
Introduction
Chronic Insomnia Disorder (CID) is defined as having persistent difficulties in sleep initiation, maintenance, or early awakening for at least 3 nights each week, lasting for at least 3 months, with daytime function impairment or distress.1 It affects 16% of adults at a global scale, with a higher prevalence in those with physical or mental health conditions.2–4 According to the 2023 China Sleep Research Report, more than 300 million adults in China suffer from insomnia.5 CID disrupts individuals’ physiological, psychological, and social functioning and is also associated with considerable economic burden because of increased healthcare utilization and productivity loss.6–9
Cognitive Behavioral Therapy for Insomnia (CBT-I) is the most recommended first-line treatment for CID.9 It primarily improves sleep by restructuring maladaptive sleep-related cognitions and promoting healthier sleep habits. However, CBT-I has limited efficacy in addressing emotional dysregulation and physiological hyperarousal, which are key factors in chronic insomnia.10 Mindfulness-based interventions, centered on the non-judgmental awareness of present-moment experiences, have been shown to address the cognitive and emotional issues associated with poor sleep mainly by cultivating awareness, attention control, and acceptance.11,12 Unlike CBT-I, mindfulness-based interventions also focus on emotional regulation and metacognitive change, which help in managing stress and physiological hyperarousal, contributing to better sleep outcomes. Thus, mindfulness can be incorporated into CBT-I to enhance treatment outcomes, addressing the aspects that CBT-I alone may not fully resolve.13 Mindfulness-based Cognitive Therapy for Insomnia (MBCT-I), which integrates mindfulness and CBT-I, has shown promising results. For instance, a randomized controlled trial with 216 CID patients in China demonstrated that MBCT-I resulted in significantly greater improvements in insomnia symptoms compared with a sleep psychoeducation and exercise control condition at two months post-intervention.14
Despite the efficacy of CBT-I or MBCT-I, fewer than 1% of patients with CID gain access to them, largely due to barriers such as the shortage of trained therapists, time constraints, geographical limitations, and high treatment costs.15 To address these barriers, digital interventions, which are delivered via the internet or smartphone applications, have emerged and garnered increasing attention in recent years.16,17 Several meta-analyses have shown that both therapist-guided and self-guided digital interventions yield large effects in patients with CID.16,18 However, the therapeutic gains of self-guided digital intervention for insomnia are often smaller than those from therapist-guided formats, largely due to suboptimal adherence, especially because self-guided programs often lack engagement, accountability, and treatment fidelity.19,20
Given that MBCT-I is a promising treatment for CID and that therapist-guided online delivery combines accessibility with high adherence and effectiveness, it is imperative to develop and disseminate the therapist-guided internet-delivered MBCT-I (iMBCT-I). To date, self-guided iMBCT-I applications are not yet available, and therapist guidance has been shown to improve engagement and treatment outcomes. To our knowledge, no research has been conducted on therapist-guided iMBCT-I. Therefore, in this study, we conducted an open-label, single-center, randomized, parallel-group controlled trial to evaluate the effectiveness and feasibility of iMBCT-I for patients with CID. Our primary hypothesis was that patients would demonstrate significant improvements in insomnia symptoms upon completion of the intervention and exhibit good attendance to the 8-week iMBCT-I program. Findings from this study may provide empirical support for the clinical application of iMBCT-I, expand therapeutic options for insomnia, and contribute to the future development of self-guided iMBCT-I programs.
Materials and Methods
This trial was approved by the Tongji Hospital of Tongji University Institutional Review Board (No. 2024–013) and has been prospectively registered at the Chinese Clinical Trial Registry (https://www.chictr.org.cn), registration number: ChiCTR2400084300. The study protocol was published previously, and the results are reported in accordance with the Consolidated Standards of Reporting Trials (CONSORT) 2010 statement (Supplementary Table 1).21,22 Deviations of methods from the original protocol and reasons are provided in Supplementary Table 2.
Randomization, Blinding, and Assessment Points
About 191 individuals showed interest and received the Mini International Neuropsychiatric Interview (MINI) via video call with two psychiatrists independently to determine eligibility. About 82 participants met the eligibility criteria and completed baseline assessments. They were then randomly assigned to the iMBCT-I group (n = 41) or the sleep hygiene education (SHE) group (n = 41) using computer-generated random numbers. Allocation sequences were prepared by an independent statistician and concealed using sealed, opaque, identical envelopes to ensure allocation concealment. The study coordinator assessed baseline information and was not involved in the recruitment or assessment delivery.
This was an open-label trial. Participants could not be blinded to group assignment due to the nature of the interventions. To minimize expectancy bias, participants were informed that both interventions were evidence-based approaches for improving sleep, without indicating which was expected to be superior. Intervention providers in both groups were blinded to the study hypotheses. Data managers and statisticians conducting the analyses were blinded to treatment allocation. Assessments were conducted online at week 0 (baseline), week 8 (primary endpoint for effectiveness evaluation) and week 20 (follow-up).
Inclusion and Exclusion Criteria
Eligible participants were (1) 18–65 years with normal speech and cognitive function, (2) meeting the diagnostic criteria of chronic insomnia disorder defined by the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), as well as an Insomnia Severity Index (ISI) score over 14, (3) being willing to attend the whole intervention program, (4) either maintaining a stable dosage and frequency throughout the study or discontinuing usage for at least 2 weeks (washout period) before enrollment for those who using sleep medication, (5) voluntarily signing the informed consent form.
Exclusion criteria included (1) inability to use online meeting applications or complete any assessment (eg questionnaires, sleep diaries); (2) life-threatening conditions (eg, suicidal ideation, cancer); (3) experiencing circumstances which may affect compliance (eg, pregnancy, dementia, substance abuse); (4) progressive medical illnesses associated with insomnia; (5) previously diagnosed with or currently suspected of psychiatric disorders; (6) conditions that could be aggravated by sleep restriction (eg, uncontrolled hypertension, seizure disorders); (7) having night shift work or other tasks disrupting sleep rhythm; (8) prior or future access to CBT, MBCT, or other mindfulness-based interventions; and (9) other self-reported or diagnosed sleep disorders (eg, sleep apnea, restless leg syndrome, rapid eye movement sleep behavior disorder or hypersomnia).
Intervention
Participants in the iMBCT-I group received eight weekly 1.5-hour group sessions delivered via Tencent Meeting, a widely used and highly stable online meeting platform in China. We ensured virtually face-to-face interaction among all participants by organizing two intervention groups of 20 and 21 members, respectively, considering that Tencent Meeting can display video feeds of up to 25 participants per page. The program was adapted from the original MBCT protocol by Segal et al, which was then tailored for chronic insomnia disorder by Wong et al, incorporating mindfulness practices (eg, body scan, meditation, mindful stretching) alongside cognitive behavioral elements such as sleep hygiene, sleep restriction, and stimulus control.14,23 The iMBCT-I program includes 8 sessions with more details displayed in Supplementary Table 3. Participants were asked to complete daily homework, primarily consisting of mindfulness practices, lasting 20–30 minutes each day. The iMBCT-I programs in both groups were primarily delivered by a clinical psychologist with over three years of formal training in MBCT. A psychiatrist with over 20 years of clinical experience in mindfulness-based interventions and CBT-I supervised the intervention throughout the study, ensuring treatment consistency and fidelity across groups.
Participants in the SHE group received a 1.5-hour online session of sleep hygiene education based on the Sleep Health Management Handbook of the Chinese National Health Commission.24 They were provided with standardized information on the symptoms, prevalence, and consequences of insomnia, as well as practical lifestyle and behavioral recommendations to improve sleep quality. Participants were allowed to revisit the materials after the session. The session was led by another psychiatrist with over three years of CBT-I training.
Measurements
We collected demographic and control measures at baseline, including age, sex, marital status, educational background, occupation, related clinical data (eg, body mass index, BMI), and lifestyle practices (eg, alcohol drinking and smoking).
The primary outcome was insomnia severity assessed with the ISI and insomnia remission.25 A total score of the ISI below 8 points is defined as remission.26 Key secondary outcomes comprised five pre-specified parameters in sleep diary: sleep onset latency (SOL), wakefulness after sleep onset (WASO), total sleep time (TST), sleep efficiency (SE), and the number of awakenings. Other secondary outcomes included sleep quality assessed with the Pittsburgh Sleep Quality Index (PSQI),27 depressive and anxious symptoms assessed with the Patient Health Questionnaire-9 (PHQ-9) and Generalized Anxiety Disorder 7-item scale (GAD-7), respectively,28,29 and quality of life assessed with the 12-item Short Form Health Survey (SF-12).30,31 The SF-12 contains two sub-scales: physical component summary (PCS) and mental component summary (MCS), both of which were evaluated separately throughout analysis in this study. The actigraphy (Huawei Band 8) collected data on WASO, TST, number of awakenings, and duration of deep sleep, light sleep, and rapid eye movement (REM) sleep. This actigraphy device utilizes the HUAWEI TruSleep™ sleep monitoring algorithm, which employs cardiopulmonary coupling (CPC) technology, combining heart rate variability (HRV) data from high-frequency photoplethysmography (PPG) sensors and three-axis accelerometer data to minimize motion interference. Previous validation conducted at Beth Israel Deaconess Medical Center, Harvard Medical School, demonstrated that sleep state classification derived from this actigraphy achieved an accuracy ranging from 79% to 92%, using electrocardiogram-based cardiopulmonary coupling (ECG-based CPC) as the reference standard.32
Satisfaction with iMBCT-I arrangement was measured by a questionnaire that consisted of five items including satisfaction with activity time, group leader, group size, group atmosphere, and homework assignments, along with a single question “Would you like to recommend iMBCT-I to others in need? (Yes/No)”. Adherence to iMBCT-I was assessed by the number of sessions they have attended. Safety was evaluated by monitoring serious adverse events (SAEs), which were defined as untoward medical events resulting in life-threatening situations, such as self-injurious behaviors, suicide attempts, or hospitalization.33 There were no SAEs reported in this trial.
Sample Size
Based on the results of a large randomized controlled trial that compared the online CBT-I with SHE among individuals with CID, the expected reductions in ISI scores were 7.7 for the iMBCT-I group and 3.1 for the SHE group, with a pooled standard deviation of 5.5.34 With a significance level of 0.05 and a power level of 0.9, the minimum sample size was 30 participants per arm. Considering an anticipated dropout rate of 20%, we planned to recruit 80 participants in total. During the actual recruitment process, several eligible participants enrolled at the same time, and therefore a total of 82 participants were eventually included.
Statistical Analysis
Statistical analyses were performed according to the intention-to-treat (ITT) principle, with missing data handled with the last observation carried forward (LOCF) method. Analyses proceeded in three steps. First, descriptive statistics were computed for all baseline demographic and clinical characteristics. Continuous variables were presented as mean ± standard deviation (SD), and categorical variables were summarized as frequencies and percentages n (%). Baseline differences in demographics and other assessments between the iMBCT-I group and the SHE group were examined using independent t-tests or chi-square tests. Second, outcomes at the primary time point (week 8) were evaluated. Independent-sample t-tests or Mann–Whitney U-tests were used to compare between-group comparisons of the change scores in sleep variables, depression, anxiety, and quality of life. Effect sizes were quantified using Cohen’s d (d), calculated as the mean difference in mean change scores divided by the pooled standard deviation of those change scores.35 Third, mixed effect maximum likelihood regressions (without imputing missing data using LOCF) were employed to assess changes in these outcomes from week 0 to week 20. The baseline scores of outcomes were adjusted as covariates in their models. Additionally, we replicated the analyses using per-protocol (PP) dataset to evaluate the robustness of the results. Participants who completed at least four iMBCT-I sessions or the SHE program were included in the per-protocol dataset.36,37 A two-tailed p < 0.05 was considered statistically significant. To adjust for multiple comparisons, the significance level is set at α = 0.025 based on the Bonferroni correction for the primary outcome (the change in the ISI total score and remission rate at week 8). For the family of five key secondary outcomes (SOL, Number of awakenings, WASO, TST and SE in sleep diary), the significance threshold was corrected at α = 0.01. For other secondary outcomes, we did not apply further correction, but reported effect sizes and confidence intervals. All analyses were conducted using SPSS 26.0.
Results
Participants Characteristics
Of the screened 191 participants from June to August 2024, 109 were excluded because of ineligibility (n = 91), refusing participation (n = 8) and other reasons (n = 10). Eligible participants (n = 82) completed baseline assessments and were then randomly assigned to either the iMBCT-I or SHE groups. At week 8, almost all participants completed questionnaire assessment (only one participants in the SHE group lost contact). At week 20, most participants in the iMBCT-I group (n = 36) and the SHE group (n = 35) completed questionnaire assessments. The majority of participants in the iMBCT-I group completed sleep diary and actigraphy assessments, while the adherence was slightly lower in the SHE group (Supplementary Table 4). Participant flowchart is displayed in Figure 1.
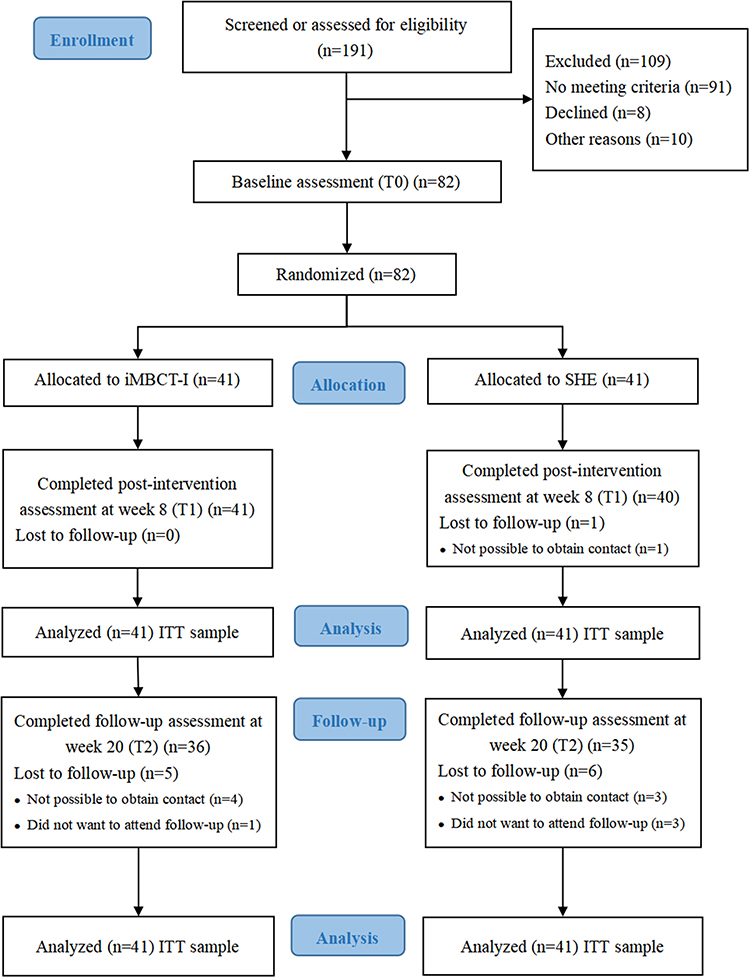 |
Figure 1 Participant Flowchart. Abbreviations: iMBCT-I, internet-delivered Mindfulness-Based Cognitive Therapy for Insomnia; SHE, Sleep Hygiene Education; ITT, intention-to-treat. Note: The CONSORT figure was adapted from Schulz KF, Altman DG, Moher D et al. CONSORT 2010 statement: updated guidelines for reporting parallel group randomized trials. Ann Intern Med. 2010;152(11):726–732.PMID: 20335313. doi: 10.7326/0003-4819-152-11-201006010-00232.21. |
Table 1 presents the baseline characteristics of participants. The average age of all 82 participants was 36.50 ± 12.44. There were 24 males (29.26%) and 58 females (70.73%). About 34 (41.46%) participants were married. Over half of the participants in each group held a bachelor’s degree or higher. In terms of BMI, the majority of participants in both groups fell within the normal weight range (iMBCT-I group: 65.85%; SHE group: 68.29%). Most participants were employed, followed by students, with few retirees or unemployed individuals. At baseline, there were no significant between-group differences in any demographic variables or scale scores (all p > 0.05).
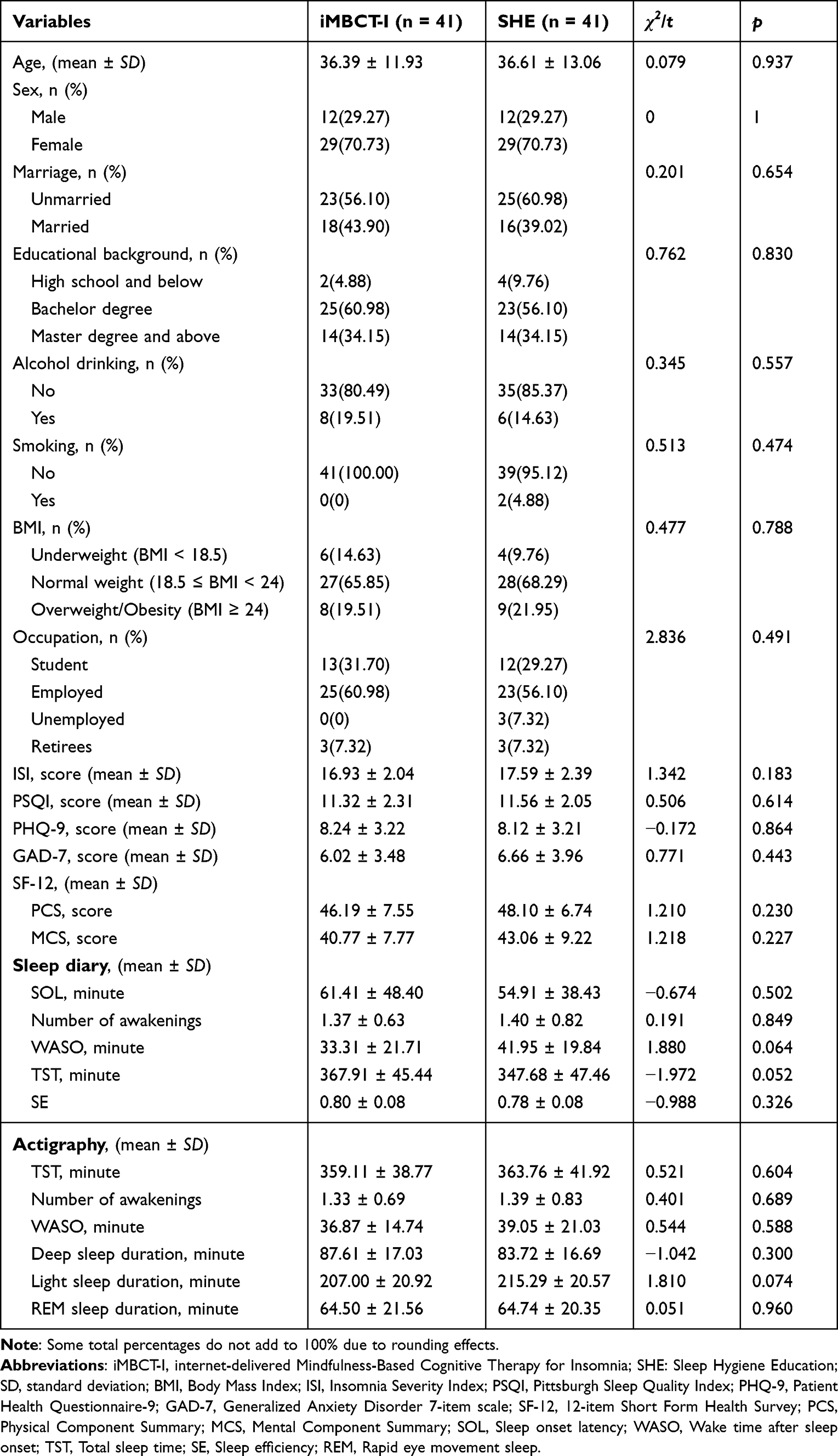 |
Table 1 Participants’ Demographic and Clinical Characteristics at Week 0 |
Effectiveness of iMBCT-I on Insomnia Severity After Intervention
At week 8, participants in the iMBCT-I group demonstrated a greater reduction in ISI scores (mean ± SD, 8.95 ± 3.79) compared with the SHE group (4.95 ± 4.30), and the between-group difference was statistically significant [MD, 95% CI = 4.00 (2.22, 5.78), t = 4.469, p < 0.001, Figure 2A and Table 2]. The effect size was large [d, 95% CI = 0.99 (0.53, 1.45)].35 Insomnia remission (ISI < 8) rates also differed significantly between groups, with 56.10% (23/41) of participants in the iMBCT-I group achieving remission, compared with 17.07% (7/41) in the SHE group (χ2 = −3.963, p < 0.001), corresponding to an odds ratio of 6.21 (2.24, 17.23) (Table 2).
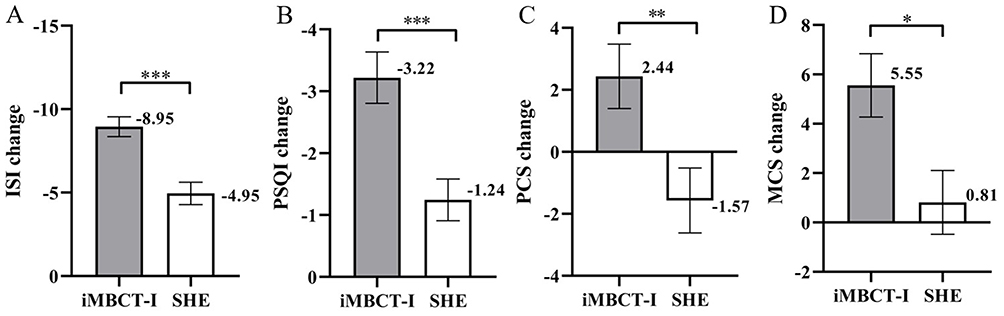 |
Figure 2 Comparison of the Mean Change Scores of ISI, PSQI, PCS, and MCS between the iMBCT-I Group and SHE Group from Week 0 to Week 8 (ITT analysis). Abbreviations: iMBCT-I, internet-delivered Mindfulness-Based Cognitive Therapy for Insomnia; SHE: Sleep Hygiene Education; ITT, intention-to-treat. Note: (A) Changes in Insomnia Severity Index (ISI). (B) Changes in Pittsburgh Sleep Quality Index (PSQI). (C) Changes in physical component summary (PCS) of 12-item short form health survey (SF-12). (D) Changes in mental component summary (MCS) of 12-item short form health survey (SF-12). Error bars represent standard errors; *p < 0.05, **p < 0.01, ***p < 0.001. |
 |
Table 2 Effect Sizes for Primary Outcomes from Week 0 to Week 8 (ITT Analysis) |
Effectiveness of iMBCT-I on Sleep Quality and Sleep Parameters After Intervention
From week 0 to week 8, participants in the iMBCT-I group demonstrated a greater reduction in PSQI scores (mean ± SD, 3.22 ± 2.65) compared with the SHE group (1.24 ± 2.15), and the between-group difference was statistically significant [MD, 95% CI = 1.98 (0.91, 3.04), t = 3.704, p < 0.001, Figure 2B]. The effect size was large (d = 0.82).
Results provided by the sleep diaries (Table 3) showed that compared with the SHE group, participants in the iMBCT-I group had significantly greater decrease in SOL and WASO [MD, 95% CI = 27.07 (−43.67, −10.46), t = −3.244, p = 0.002, d = 0.72; MD, 95% CI = −19.99 (−28.44, −11.53), t = −4.704, p < 0.001, d = 1.04, respectively]. And the iMBCT-I group demonstrated a significant greater increase in SE than the SHE group [MD, 95% CI = 0.08 (0.05, 0.12), t = 4.989, p < 0.001, d = 1.12]. However, no significant between-group differences were observed in the number of awakenings or TST (p > 0.01).
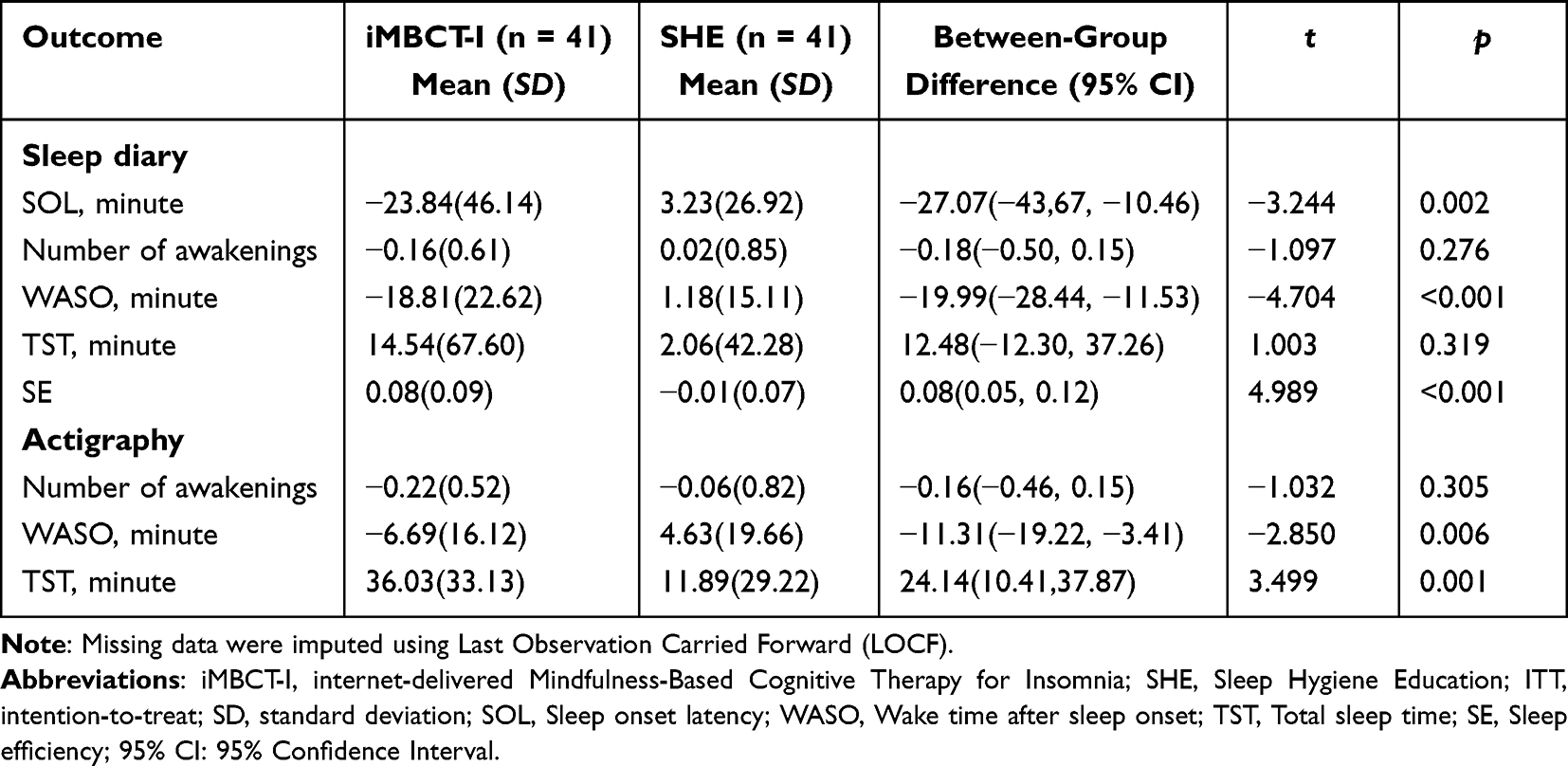 |
Table 3 Comparison of the Mean Change Scores of Sleep Diary and Actigraphy Parameters from Week 0 to Week 8 (ITT Analysis) |
Results collected from actigraphy (Table 3) showed that participants in the iMBCT-I group had significantly greater decrease in WASO than those in the SHE group [MD, 95% CI = −11.31 (−19.22, −3.41), t = −2.850, p = 0.006, d = 0.63]. Besides, the iMBCT-I group exhibited a significantly longer TST compared to the SHE group [MD, 95% CI = 24.14 (10.41, 37.87), t = 3.499, p = 0.001, d = 0.77]. However, there were no significant between-group differences for the number of awakenings [MD, 95% CI = −0.16 (−0.46, 0.15), t = −1.032, p = 0.305].
Regarding sleep architecture (Supplementary Table 5), actigraphy data indicated a significant increase in light and REM sleep duration (minutes) in the iMBCT-I group (14.36 ± 26.04; 22.03 ± 17.68) compared to the SHE group (1.79 ± 23.60, 6.98 ± 12.65), with a statistically significant between-group difference [MD, 95% CI = 12.56 (1.64, 23.49), t = 2.289, p = 0.025, d = 0.51; 15.05 (8.30, 21.81), t = 4.434, p < 0.001, d = 0.98], respectively. However, no significant differences in deep sleep duration were observed between the two groups [MD, 95% CI = −3.47 (−9.46, 2.51), t = −1.154, p = 0.252].
Effectiveness of iMBCT-I on Quality of Life After Intervention
Compared with the SHE group, participants in the iMBCT-I group demonstrated greater improvement in both PCS [MD, 95% CI = 4.01 (1.07, 6.95), t = 2.715, p = 0.008] and MCS [MD, 95% CI = 4.74 (1.12, 8.36), t = 2.606, p = 0.011] scores (Figure 2C and D). The values of Cohen’s d for PCS and MCS were 0.60 and 0.58, respectively, both indicating a moderate effect.
Effectiveness of iMBCT-I on Depressive and Anxiety Symptoms After Intervention
After the intervention, the iMBCT-I group showed a greater improvement in depressive symptoms (PHQ-9) compared to the SHE group [MD, 95% CI = −1.98 (−3.69, −0.26), p = 0.024, d = 0.51]. However, the between-group difference in anxiety symptoms (GAD-7) was not statistically significant (p = 0.839). Details were displayed in Supplementary Figure 1.
Maintenance of the Effectiveness of iMBCT-I at Week 20 Follow-Up
Insomnia remission rates differed significantly between groups, with 48.78% (20/41) of participants in the iMBCT-I group achieving remission, compared with 17.07% (7/41) in the SHE group (χ2 = 9.332, p = 0.002) from week 0 to week 20. To further evaluate whether the therapeutic effectiveness persisted over time, linear mixed-effects models including data from week 0, week 8, and week 20 were performed (Supplementary Table 6). For the primary outcome, iMBCT-I produced a significantly greater reduction in ISI scores compared to SHE across the 20-week follow-up (p < 0.025). Superiority of iMBCT-I was also confirmed on all key secondary outcomes (SOL, number of awakenings, WASO, TST, and SE in sleep diary; all p < 0.01). As for other secondary outcomes, a significant group effect for PSQI (p < 0.001) was observed, with large effect sizes at both Week 8 (d = −1.38) and Week 20 (d = −1.32). Besides, iMBCT-I group showed significantly greater improvement on quality of life both physically (PCS: week 8, d = 0.83; week 20: d = 0.34) and mentally (MCS: week 8, d = 0.61; week 20, d = 0.77). However, no significant group main effects were found for GAD-7 (p = 0.218) or PHQ-9 (p = 0.079). Actigraphy analyses indicated that the iMBCT-I group showed fewer number of awakenings (p = 0.003, d = −0.65), shorter WASO (p < 0.001, d = −1.14), and longer REM sleep duration (p < 0.001, d = 2.53) across the study period. However, the group × time interaction effect was not significant in all outcomes but TST and light sleep duration in actigraphy, indicating that while the iMBCT-I group sustained its superior outcomes, the trajectories of change over time were comparable between the two groups. The trend of changes between the two groups from week 0 to week 20 is shown in the Supplementary Figures 2–4.
Attendance and Satisfaction with the iMBCT-I Program
In the iMBCT-I group, 16 (39.02%) participants completed all sessions, 31 (75.61%) attended at least six sessions. Five participants attended fewer than four sessions primarily due to scheduling conflicts (n = 4) or difficulty with data recording (n = 1). As shown in Table 4, more than three-quarters of participants reported satisfaction with the session schedule, group size, group atmosphere, and homework assignments. Nearly all iMBCT-I participants (97.56%) were satisfied with the group leader. Additionally, 90.24% indicated they would recommend this intervention to others in need.
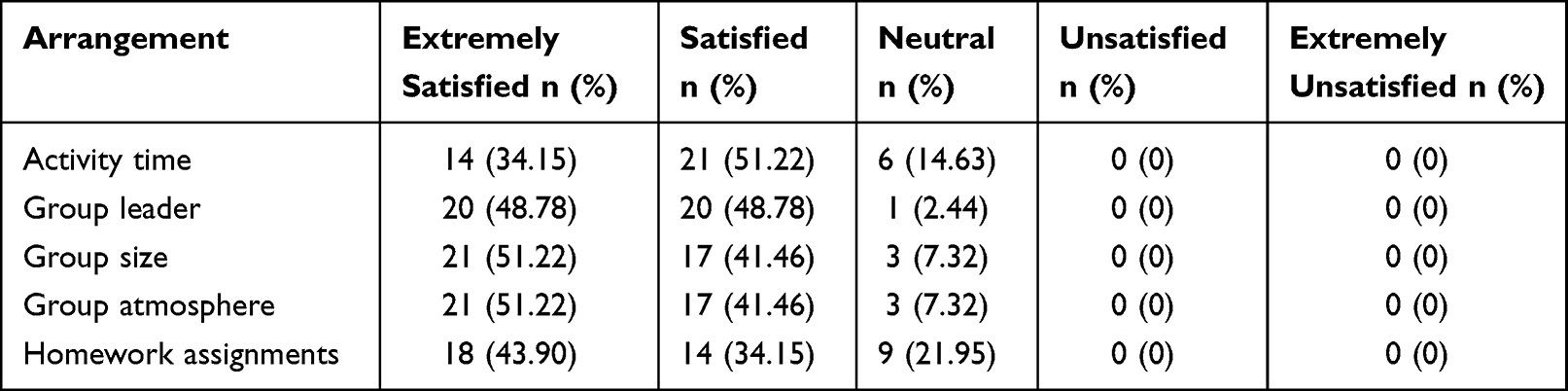 |
Table 4 Participants’ Satisfaction with Program Arrangement in the iMBCT-I Group (n = 41) |
Sensitive Analysis
We repeated the analyses above using the per-protocol dataset as sensitivity analyses. Except the “change in light sleep duration” (a significant between-group difference was observed in the PP analysis), all results were consistent with those from the ITT analysis, suggesting the robustness of the findings (Supplementary Table 7 and 8).
Discussion
To the best of our knowledge, this is the first randomized controlled trial to investigate the efficacy and feasibility of a therapist-guided iMBCT-I in improving sleep-related parameters among people with CID when compared with sleep hygiene education as a control group. At week 8, iMBCT-I showed a greater beneficial effect on insomnia severity than SHE, with a significantly higher remission rate. And there were also significant improvements in sleep quality measured by PSQI, as well as SOL, WASO, SE, REM duration, and quality of life in both physical and mental aspects. And these effects were maintained throughout the 20-week follow-up. Besides, the iMBCT-I might have a tendency to decrease depressive and anxiety symptoms during the 20-week period. With per protocol analyses, the results remained unchanged.
There are many theoretical models proposed to explain the pathophysiology of chronic insomnia, such as the hyperarousal model and the cognitive model.38,39 Among them, the integrative metacognitive model is particularly relevant to our study, as it emphasizes a vicious cycle of cognitive and behavioral processes in initiating and maintaining insomnia.13,40 First, individuals excessively ruminate about sleep, which results in primary arousal (negative anticipatory thoughts about potential daytime consequences of insomnia).41 This primary arousal could trigger negative emotions and physiological activation, followed by secondary arousal (negative metacognitive evaluation or judgment of primary arousal, which causes persistent distress and physiological hyperactivation).13,42 Individuals may then engage in excessive sleep monitoring and selective attention to cues related to falling asleep and gradually develop a pathological demand for controlling or forcing sleep.43 Finally, the negative and distorted cognition about insomnia, such as overestimating the sleep impairment, can reinforce the maintenance of chronic insomnia.44 Our iMBCT-I program systematically provides mindfulness training to cultivate attitudes of present-moment awareness, non-judgement, and acceptance, which enhance relaxation, resilience and emotional regulation. Meantime, CBT-I techniques are incorporated to handle maladaptive sleep beliefs and promote scientific sleep behaviors. Therefore, it may break the cycle of insomnia from multiple dimensions. First, mindfulness practices such as mindful breathing and body scanning may reduce rumination by fostering experiential awareness. This may help individuals notice pre-sleep thoughts and physiological arousal and prevents triggering the primary arousal.45,46 Second, iMBCT-I may influence the primary and secondary arousal by cultivating attention control. The non-judgmental attitude toward sleep difficulties, combined with cognitive restructuring techniques in CBT-I, may reduce catastrophic thoughts about sleep loss, such as worries about poor performance the next day.47 Besides, the CBT-I components, including sleep hygiene education, sleep restriction and stimulus control, may support healthier sleep habits and more adaptive cognitive–behavioral responses to poor sleep.48 These may enhance individuals’ perceived control and confidence in sleep. Meanwhile, the acceptance component of mindfulness practices may reduce the tendency to excessively monitor or force sleep.13 Although we attempt to elaborate the potential mechanism of iMBCT-I through the integrative metacognitive model, this study cannot decide which components worked for the short-term improvement versus maintenance of effects. Also, it should be noted that the proposed mechanisms are theoretical rather than empirically tested in this study. Moreover, non-specific factors such as therapist attention, group support, and expectancy effects cannot be ruled out.49
A recent meta-analysis involving 13 trials comparing the effects of CBT-I, sleep medications and their combination on CID reported a long-term remission rate of 41% for CBT-I, which was the highest among the three approaches.50 Another large-scale study in Finland involving 2,464 physician-referred patients with CID found that the remission rate among completers of therapist-supported iCBT-I was 34%.51 By comparison, our study showed relatively higher remission rates, with 56.10% at week 8 and 48.78% at week 20. This suggests iMBCT-I program should be a promising intervention for CID with strong clinical efficacy. However, we should also be cautious about making direct comparisons, as the study populations, intervention protocol, and follow-up time differ across studies.
This study indicates that iMBCT-I significantly reduced the perceived SOL and increased sleep efficiency. However, the actigraphy in our study only initiated recording after sleep onset, which was unable to capture the pre-sleep time in bed. Thereafter, the observed changes mainly reflected subjective reports. Besides, iMBCT-I was found to reduce WASO and increase the TST, with consistent results across sleep diary and actigraphy. Additionally, actigraphy results suggested that iMBCT-I may influence sleep architecture by increasing REM sleep duration. Findings on sleep architecture should be interpreted carefully, and polysomnography is needed for confirmation.52
These results align with those of Wong et al, who found that eight weeks of face-to-face MBCT-I significantly improved SOL, WASO, TST, and sleep efficiency in CID patients as assessed by sleep diaries.14 Similar results were also reported in a randomized controlled trial of MBCT-I on breast cancer survivors with insomnia, where the sleep parameters were recorded by actigraphy.53 Besides, improvements of SOL and WASO were also observed in patients with recurrent depression, as they were measured by the Bergen Insomnia Scale.54 Furthermore, a meta-analysis of 20 CBT-I studies showed sustained improvements in SOL, WASO, TST, and sleep efficiency compared with inactive controls.55 However, a meta-analysis of 330 insomniacs in 6 RCTs showed mindfulness meditation alone had no significant effects on SOL, TST, WASO or sleep efficiency.56 A potential explanation for this discrepancy could be the absence of core CBT-I components such as sleep restriction and stimulus control, which are critical for improving sleep duration and consolidation.57
Our results of follow-up at week 20 suggest that participants who received iMBCT-I continued to experience improved sleep condition and quality of life after intervention. It indicates that iMBCT-I can also maintain these improvements in the short term. The sustainability of treatment effects may suggest that iMBCT-I facilitates stable behavioral and cognitive changes that support longer sleep health.58 However, due to the lack of follow-up data on participants’ adherence to mindfulness or CBT-I practices after the intervention, it remains unclear whether the sustained effects were attributable to the continued engagement in these practices or to the residual benefits of the 8-week program.
In this study, a significant reduction in depressive symptoms was observed in the iMBCT-I group at week 8, whereas the improvement in anxiety symptoms was not statistically significant. The trend appeared to reverse at the 20-week follow-up, with only anxiety symptoms showing a tendency to alleviation. Given the mild baseline symptoms and exclusion of more severe cases, the study is not powered to evaluate iMBCT-I as a treatment for depression or anxiety; rather, it supports no worsening and some signal of improvement in these domains. Considering the high comorbidity and bidirectional relationship between insomnia and mood symptoms, we adopted strict criteria to exclude participants with significant depressive or anxiety symptoms, aiming to have a more precise examination of iMBCT-I’s efficacy for insomnia.59 Previous studies indicate that many individuals with mood disorders present with insomnia as a primary symptom.60 However, in our study, we did not observe deterioration in mood symptoms in either the iMBCT-I or SHE groups, suggesting that timely intervention for insomnia, even through a simple approach as sleep education, can be beneficial in preventing the exacerbation of mood symptoms.60 Additionally, our results revealed obvious improvements in quality of life in the iMBCT-I group both post-intervention and at follow-up. This may stem from the mindfulness components or could be secondary to improvements in sleep quality.61,62
This trial has several strengths. First, it is one of the earliest to systematically develop and validate an internet-delivered, therapist-guided mindfulness-based cognitive therapy for insomnia, which integrates CBT-I and mindfulness training. This approach provides a novel solution to address the limitations of CBT-I efficacy. Additionally, the internet-based, therapist-guided format may balance the accessibility, efficacy, and adherence. Second, the combination of multi-dimensional objective and subjective assessments provides a comprehensive reflection of participants’ sleep conditions, which can enhance the robustness of the findings.
However, there are also some limitations. First, participants were inevitably aware of their group assignments, which may introduce bias in the self-reported-based outcomes. There was an implicit assumption that the treatment would result in improvement, which could lead to an overestimation of effectiveness. Therefore, the expectancy effects cannot be ruled out and should be considered when interpreting the findings. Future trials should incorporate explicit measures of expectancy and credibility to better disentangle specific and non-specific treatment effects. Second, the duration of the single-session SHE and the 8-week iMBCT-I intervention were not time-matched. This discrepancy suggested that some of the observed effects of iMBCT-I could also be attributable to non-specific factors, such as increased attention by therapists and support by group members, rather than the content of the intervention itself. Third, we did not collect the frequency that participants practice their homework in the follow-up period, so it is hard to draw a conclusion on whether the maintenance of effectiveness was attributed to the persistence of homework practices or the eight-week intervention. Fourth, detailed information on medication class and dosage was not collected sufficiently for adjusted analyses. Although medication use was either washed out prior to enrollment or required to remain stable throughout the intervention period, unrecorded changes in medication use in response to symptom fluctuations during the trial may contribute to residual confounders for the outcomes. Fifth, the follow-up period was relatively short, so it remains unclear how long the efficacy of iMBCT-I maintains. Sixth, small sample size relative to insomnia prevalence, characteristics of participants and the requirement for high digital literacy in this trial may limit the generalizability of the findings. Specifically, the relatively high educational level, high-functioning status with few comorbidities, exclusion of psychiatric conditions and urban (Shanghai) background of the participants may be associated with greater digital literacy, technology acceptance, and adherence, which could have amplified engagement and treatment response in this digital intervention. Seventh, the use of LOCF to handle missing data might introduce bias, as it can overestimate or underestimate treatment effects depending on dropout patterns and the missing data mechanism.63 Additionally, LOCF can underestimate the standard error and p values, increasing the risk of Type I error.63 These limitations should be considered when interpreting the results.
Future research could consider expanding the sample size with a multi-center design to investigate the feasibility and effectiveness of iMBCT-I across diverse demographic groups with a longer follow-up period. It is also worthwhile to design a randomized controlled trial to test whether iMBCT-I is superior to iCBT-I.
Conclusion
The eight-week therapist-guided iMBCT-I shows promising effects in reducing insomnia severity, improving sleep quality and quality of life in adults with chronic insomnia. Patients showed high satisfaction and strong attendance, and these benefits were maintained for at least 20 weeks. However, given the open-label design and the attention-mismatched comparator, improvements in self-reported outcomes may reflect both specific treatment effects and non-specific factors. Limitations such as treatment dose imbalance, sample characteristics and follow-up duration suggest further large-scale and well-controlled trials with long-term follow-up before recommending widespread clinical adoption.
Data Sharing Statement
De-identified individual participant data supporting the findings of this study are available from the corresponding author upon reasonable request, subject to ethical approval and applicable data protection regulations.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Tongji Hospital of Tongji University Institutional Review Board (reference number: 2024-013) on January 31, 2024. All participants provided informed consent before taking part in the study.
Acknowledgment
The authors thank all the participants for their time in this study.
Author Contributions
Zixuan Zeng: Methodology, Writing – original draft, Writing – review & editing; Jiahui Jiang: Formal analysis, Writing – Original draft, Writing – review & editing; Kun Xie: Project administration, Resources, Writing – original draft, Writing – review & editing; Na Luo: Data curation, Writing – Original draft, Xiaofeng Guan: Investigation, Writing – original draft, Writing – review & editing, Chenyi Zhu: Investigation, Project administration, Writing – original draft; Zheng Lu: Conceptualization, Writing – review & editing, Funding acquisition; Lei Huang: Conceptualization, Writing – Review & Editing, Supervision, Project administration, Funding acquisition. All the authors have reached consensus on the journal this article will be submitted. All authors agree to review all versions of the article prior to submission, during revision, acceptance of the final version for publication, and any significant changes introduced during the proofreading phase, and to be responsible for the content of the article.
Funding
This research is funded by STI2030-Major Projects, Grant No. (2021ZD0200600), Shanghai Science and Technology Committee, Grant No. (21Y21900700), 2023 Annual Clinical Research and Cultivation Project of Shanghai Tongji Hospital, Grant No. (ITJ(QN)2302), 2024 Shanghai Municipal Health Commission Seed Grant Program for Medical Technology Research and Translation Grant No. (2024ZZ2063).
Disclosure
The authors declare no conflict of interest.
References
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
2. Benjafield AV, Sert Kuniyoshi FH, Malhotra A, et al. Estimation of the global prevalence and burden of insomnia: a systematic literature review-based analysis. Sleep Med Rev. 2025;(82):102121. PMID: 40627924. doi:10.1016/j.smrv.2025.102121
3. Morin CM, Jarrin DC. Epidemiology of insomnia: prevalence, course, risk factors, and public health burden. Sleep Med Clin. 2022;17(2):173–15. PMID: 35659072. doi:10.1016/j.jsmc.2022.03.003
4. Johansson M, Jansson-Fröjmark M, Norell-Clarke A, et al. The role of psychiatric and somatic conditions in incidence and persistence of insomnia: a longitudinal, community study. Sleep Health. 2016;2(3):229–238. PMID: 29073427. doi:10.1016/j.sleh.2016.05.004
5. Wang J, Zhang Y, Zhang Y. Annual Sleep Report of China 2023. Beijing: Social Sciences Academic Press; 2023.
6. Daley M, Morin CM, LeBlanc M, et al. The economic burden of insomnia: direct and indirect costs for individuals with insomnia syndrome, insomnia symptoms, and good sleepers. Sleep. 2009;32(1):55–64. PMID: 19189779.
7. Taddei-Allen P. Economic burden and managed care considerations for the treatment of insomnia. Am J Manag Care. 2020;26(4 Suppl):S91–S96. PMID: 32282179. doi:10.37765/ajmc.2020.43008
8. Sutton EL. Insomnia. Ann Intern Med. 2021;174(3):ITC33–ITC48. PMID: 33683929. doi:10.7326/AITC202103160
9. Riemann D, Espie CA, Altena E, et al. The European Insomnia Guideline: an update on the diagnosis and treatment of insomnia 2023. J Sleep Res. 2023;32(6):e14035. PMID: 38016484. doi:10.1111/jsr.14035
10. Blanken TF, Benjamins JS, Borsboom D, et al. Insomnia disorder subtypes derived from life history and traits of affect and personality. Lancet Psychiatry. 2019;6(2):151–163. PMID: 30630691. doi:10.1016/S2215-0366(18)30464-4
11. Ong J, Sholtes D. A mindfulness-based approach to the treatment of insomnia. J Clin Psychol. 2010;66(11):1175–1184. PMID: 20853441. doi:10.1002/jclp.20736
12. Ong JC, Manber R, Segal Z, et al. A randomized controlled trial of mindfulness meditation for chronic insomnia. Sleep. 2014;37(9):1553–1563. PMID: 25142566. doi:10.5665/sleep.4010
13. Ong JC, Ulmer CS, Manber R. Improving sleep with mindfulness and acceptance: a metacognitive model of insomnia. Behav Res Ther. 2012;50(11):651–660. PMID: 22975073. doi:10.1016/j.brat.2012.08.001
14. Wong SY, Zhang DX, Li CC, et al. Comparing the effects of mindfulness-based cognitive therapy and sleep psycho-education with exercise on chronic insomnia: a randomised controlled trial. Psychother Psychosom. 2017;86(4):241–253. PMID: 28647747. doi:10.1159/000470847
15. Riemann D, Spiegelhalder K, Espie C, et al. Chronic insomnia: clinical and research challenges--an agenda. Pharmacopsychiatry. 2011;44(1):1–14. PMID: 21161882. doi:10.1055/s-0030-1267978
16. Soh HL, Ho RC, Ho CS, et al. Efficacy of digital cognitive behavioural therapy for insomnia: a meta-analysis of randomised controlled trials. Sleep Med. 2020;75:315–325. PMID: 32950013. doi:10.1016/j.sleep.2020.08.020
17. Hosono T, Niwa Y, Kondoh M. Comparison of product features and clinical trial designs for the DTx products with the indication of insomnia authorized by regulatory authorities. Ther Innov Regul Sci. 2024;58(6):1138–1147. PMID: 39306603. doi:10.1007/s43441-024-00684-9
18. Seyffert M, Lagisetty P, Landgraf J, et al. Internet-delivered cognitive behavioral therapy to treat insomnia: a systematic review and meta-analysis. PLoS One. 2016;11(2):e0149139. PMID: 26867139. doi:10.1371/journal.pone.0149139
19. Hedman-Lagerlöf E, Carlbring P, Svärdman F, et al. Therapist-supported Internet-based cognitive behaviour therapy yields similar effects as face-to-face therapy for psychiatric and somatic disorders: an updated systematic review and meta-analysis. World Psychiatry. 2023;22(2):305–314. PMID: 37159350. doi:10.1002/wps.21088
20. Hwang JW, Lee GE, Woo JH, et al. Systematic review and meta-analysis on fully automated digital cognitive behavioral therapy for insomnia. NPJ Digit Med. 2025;8(1):157. PMID: 40075149. doi:10.1038/s41746-025-01514-4
21. Schulz KF, Altman DG, Moher D, et al. CONSORT 2010 statement: updated guidelines for reporting parallel group randomized trials. Ann Intern Med. 2010;152(11):726–732. PMID: 20335313. doi:10.7326/0003-4819-152-11-201006010-00232
22. Zeng Z, Liu F, Zhu C, et al. A guided internet-delivered mindfulness-based cognitive therapy for insomnia: study protocol for a randomized controlled study. Front Psychiatry. 2025;16:1506183. PMID: 40496827. doi:10.3389/fpsyt.2025.1506183
23. Segal Z, Williams M, Teasdale J. Mindfulness-Based Cognitive Therapy for Depression.
24. Lin L. Sleep Health Management Handbook. Beijing: Chinese Population Press; 2020.
25. Bastien CH, Vallières A, Morin CM. Validation of the insomnia severity index as an outcome measure for insomnia research. Sleep Med. 2001;2(4):297–307. PMID: 11438246. doi:10.1016/s1389-9457(00)00065-4
26. Kallestad H, Scott J, Vedaa Ø, et al. Mode of delivery of cognitive behavioral therapy for insomnia: a randomized controlled non-inferiority trial of digital and face-to-face therapy. Sleep. 2021;44(12). PMID: 34291808. doi:10.1093/sleep/zsab185
27. Buysse DJ, Reynolds CF, Monk TH, et al. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. PMID: 2748771. doi:10.1016/0165-1781(89)90047-4
28. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. PMID: 11556941. doi:10.1046/j.1525-1497.2001.016009606.x
29. Spitzer RL, Kroenke K, Williams JB, et al. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. PMID: 16717171. doi:10.1001/archinte.166.10.1092
30. Ware J, Kosinski M, Keller SD. A 12-item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34(3):220–233. PMID: 8628042. doi:10.1097/00005650-199603000-00003
31. Lam CL, Tse EY, Gandek B. Is the standard SF-12 health survey valid and equivalent for a Chinese population. Qual Life Res. 2005;14(2):539–547. PMID: 15892443. doi:10.1007/s11136-004-0704-3
32. Wearable evaluations. Available from: https://www.dbiom.org/research/wearable-evaluations.
33. Klein JP, Rozental A, Sürig S, et al. Adverse events of psychological interventions: definitions, assessment, current state of the research and implications for research and clinical practice. Psychother Psychosom. 2024;93(5):308–315. PMID: 39074446. doi:10.1159/000540212
34. Ritterband LM, Thorndike FP, Ingersoll KS, et al. Effect of a web-based cognitive behavior therapy for insomnia intervention with 1-year follow-up: a randomized clinical trial. JAMA Psychiatry. 2017;74(1):68–75. PMID: 27902836. doi:10.1001/jamapsychiatry.2016.3249
35. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
36. Teasdale JD, Segal ZV, Williams JM, et al. Prevention of relapse/recurrence in major depression by mindfulness-based cognitive therapy. J Consult Clin Psychol. 2000;68(4):615–623. PMID: 10965637. doi:10.1037//0022-006x.68.4.615
37. Tickell A, Ball S, Bernard P, et al. The effectiveness of mindfulness-based cognitive therapy (MBCT) in real-world healthcare services. Mindfulness. 2020;11(2):279–290. PMID: 32064009. doi:10.1007/s12671-018-1087-9
38. Riemann D, Spiegelhalder K, Feige B, et al. The hyperarousal model of insomnia: a review of the concept and its evidence. Sleep Med Rev. 2010;14(1):19–31. PMID: 19481481. doi:10.1016/j.smrv.2009.04.002
39. Harvey AG. A cognitive model of insomnia. Behav Res Ther. 2002;40(8):869–893. PMID: 12186352. doi:10.1016/s0005-7967(01)00061-4
40. Shallcross AJ, Visvanathan PD. Mindfulness-Based Cognitive Therapy for Insomnia. Cham: Springer International Publishing; 2016:19–29.
41. Tousignant OH, Taylor ND, Suvak MK, et al. Effects of rumination and worry on sleep. Behav Ther. 2019;50(3):558–570. PMID: 31030873. doi:10.1016/j.beth.2018.09.005
42. Carney CE, Harris AL, Moss TG, et al. Distinguishing rumination from worry in clinical insomnia. Behav Res Ther. 2010;48(6):540–546. PMID: 20362977. doi:10.1016/j.brat.2010.03.004
43. Woods H, Marchetti LM, Biello SM, et al. The clock as a focus of selective attention in those with primary insomnia: an experimental study using a modified Posner paradigm. Behav Res Ther. 2009;47(3):231–236. PMID: 19200946. doi:10.1016/j.brat.2008.12.009
44. Tang N, Saconi B, Jansson-Fröjmark M, et al. Cognitive factors and processes in models of insomnia: a systematic review. J Sleep Res. 2023;32(6):e13923. PMID: 37364869. doi:10.1111/jsr.13923
45. Kalmbach DA, Roth T, Cheng P, et al. Mindfulness and nocturnal rumination are independently associated with symptoms of insomnia and depression during pregnancy. Sleep Health. 2020;6(2):185–191. PMID: 32146168. doi:10.1016/j.sleh.2019.11.011
46. Wang J, Yang Q, Cui N, et al. Effectiveness and mechanisms of a digital mindfulness-based intervention for subthreshold to clinical insomnia symptoms in pregnant women: randomized controlled trial. J Med Internet Res. 2025;27:e68084. PMID: 40324172. doi:10.2196/68084
47. Ioverno S, Pallini S, Farina F, et al. The less you judge, the better you sleep: the benefits of mindfulness and forgiveness for insomnia and sleep problems. Bull Menninger Clin. 2022;86(4):324–338. PMID: 36454149. doi:10.1521/bumc.2022.86.4.324
48. Altena E, Ellis J, Camart N, et al. Mechanisms of cognitive behavioural therapy for insomnia. J Sleep Res. 2023;32(6):e13860. PMID: 36866434. doi:10.1111/jsr.13860
49. Coulson NS, Smedley R, Bostock S, et al. The pros and cons of getting engaged in an online social community embedded within digital cognitive behavioral therapy for insomnia: survey among users. J Med Internet Res. 2016;18(4):e88. PMID: 27113540. doi:10.2196/jmir.5654
50. Furukawa Y, Sakata M, Furukawa TA, et al. Initial treatment choices for long-term remission of chronic insomnia disorder in adults: a systematic review and network meta-analysis. Psychiatry Clin Neurosci. 2024;78(11):646–653. PMID: 39188094. doi:10.1111/pcn.13730
51. Stenberg JH, Ritola V, Joffe G, et al. Effectiveness of mobile-delivered, therapist-assisted cognitive behavioral therapy for insomnia in nationwide routine clinical care in Finland. J Clin Sleep Med. 2022;18(11):2643–2651. PMID: 35929590. doi:10.5664/jcsm.10186
52. Cid-Verdejo R, Farías CC, Martínez-Pozas O, et al. Instrumental assessment of sleep bruxism: a systematic review and meta-analysis. Sleep Med Rev. 2024;74:101906. PMID: 38295573. doi:10.1016/j.smrv.2024.101906
53. Zhao Y, Liu J, Lewis FM, et al. Effects of mindfulness-based cognitive therapy on breast cancer survivors with insomnia: a randomised controlled trial. Eur J Cancer Care. 2020;29(5):e13259. PMID: 32424878. doi:10.1111/ecc.13259
54. Evanger LN, Flo-Groeneboom E, Sørensen L, et al. Mindfulness-based cognitive therapy improves insomnia symptoms in individuals with recurrent depression: secondary analyses from a randomized controlled trial. Front Psychiatry. 2023;14:1231040. PMID: 38312915. doi:10.3389/fpsyt.2023.1231040
55. Trauer JM, Qian MY, Doyle JS, et al. Cognitive behavioral therapy for chronic insomnia: a systematic review and meta-analysis. Ann Intern Med. 2015;163(3):191–204. PMID: 26054060. doi:10.7326/M14-2841
56. Gong H, Ni C, Liu Y, et al. Mindfulness meditation for insomnia: a meta-analysis of randomized controlled trials. J Psychosom Res. 2016;89:1–6. PMID: 27663102. doi:10.1016/j.jpsychores.2016.07.016
57. Morin CM. Cognitive-behavioral approaches to the treatment of insomnia. J Clin Psychiatry. 2004;65(Suppl 16):33–40. PMID: 15575803.
58. Luik AI, Marsden A, Emsley R, et al. Long-term benefits of digital cognitive behavioural therapy for insomnia: follow-up report from a randomized clinical trial. J Sleep Res. 2020;29(4):e13018. PMID: 32112507. doi:10.1111/jsr.13018
59. Hombali A, Seow E, Yuan Q, et al. Prevalence and correlates of sleep disorder symptoms in psychiatric disorders. Psychiatry Res. 2019;279:116–122. PMID: 30072039. doi:10.1016/j.psychres.2018.07.009
60. Hertenstein E, Feige B, Gmeiner T, et al. Insomnia as a predictor of mental disorders: a systematic review and meta-analysis. Sleep Med Rev. 2019;43:96–105. PMID: 30537570. doi:10.1016/j.smrv.2018.10.006
61. Fortes PP, Santos-Ribeiro SD, de Salles-Andrade JB, et al. Mindfulness interventions and quality of life in anxiety-related disorders: a systematic review and meta-analysis. J Affect Disord. 2025;373:383–393. PMID: 39740743. doi:10.1016/j.jad.2024.12.103
62. Tay EH, Koh YS, Vaingankar JA, et al. Association between sleep quality and quality of life in Singapore. Qual Life Res. 2024;33(6):1707–1717. PMID: 38472716. doi:10.1007/s11136-024-03621-3
63. Lane P. Handling drop-out in longitudinal clinical trials: a comparison of the LOCF and MMRM approaches. Pharm Stat. 2008;7(2):93–106. PMID: 17351897. doi:10.1002/pst.267
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Systematic Review and Meta-Analysis Protocol to Establish How Common Clinical Acupoint Stimulation-Related Therapies Should Be Used for Managing Insomnia
Guo P, Xu M, Pan J, Lin J, Hu T, Wei Y, Chen Y, Guo Y
Journal of Pain Research 2023, 16:1069-1079
Published Date: 28 March 2023
Magnesium Bisglycinate Supplementation in Healthy Adults Reporting Poor Sleep: A Randomized, Placebo-Controlled Trial
Schuster J, Cycelskij I, Lopresti A, Hahn A
Nature and Science of Sleep 2025, 17:2027-2040
Published Date: 30 August 2025
Effect of Mindfulness Training on the Clinical Pregnancy Rate in Women Undergoing Frozen Embryo Transfer: Study Protocol for a Single-Center, Open-Label, Randomized Controlled Trial
Yi S, Zhang J, Li A, Zhou N, Li J, Cao R, Gao Y, Liu X, Zhai J
International Journal of Women's Health 2026, 18:598680
Published Date: 20 June 2026