Back to Journals » Drug Design, Development and Therapy » Volume 20
The Effects of Remimazolam Tosylate on Postoperative Memory Function in Young and Middle-Aged Patients Undergoing Laparoscopic Surgery
Authors Liu J, Li M, Zhao K ![]() , Wang H, Wu P, Yin T, He K
, Wang H, Wu P, Yin T, He K ![]() , Yang X, Wang S
, Yang X, Wang S ![]()
Received 18 November 2025
Accepted for publication 28 February 2026
Published 27 March 2026 Volume 2026:20 580654
DOI https://doi.org/10.2147/DDDT.S580654
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Solomon Tadesse Zeleke
Jingya Liu,1 Mengyu Li,1 Kai Zhao,1 Huimin Wang,1,2 Ping Wu,1,3 Tianyue Yin,1 Keqiang He,1 Xinlu Yang,1 Sheng Wang1
1Department of Anesthesiology, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, Anhui, People’s Republic of China; 2Graduate Department, Wannan Medical College, Wuhu, Anhui, People’s Republic of China; 3Department of Anesthesiology, Anhui Provincial Hospital Affiliated to Anhui Medical University, Hefei, Anhui, People’s Republic of China
Correspondence: Sheng Wang, Department of Anesthesiology, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, Anhui, People’s Republic of China, Tel +86 191 5600 7726, Email [email protected] Xinlu Yang, Department of Anesthesiology, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, Anhui, People’s Republic of China, Tel +86 139 6670 0588, Email [email protected]
Purpose: This randomized controlled trial compared the effects of remimazolam tosylate versus propofol on postoperative memory function in young and middle-aged adults undergoing laparoscopic surgery.
Patients and Methods: 228 patients were randomized to receive either remimazolam or propofol (n=114 each) for induction and maintenance of general anesthesia, guided by Bispectral Index (BIS). Memory and cognitive functions were assessed preoperatively and on postoperative days 1 and 3 using the Three-Word Recall Test (TRT), Memory and Executive Screening (MES), and Montreal Cognitive Assessment (MoCA), with a follow-up at one month via the Telephone Interview for Cognitive Status-modified (TICS-m). Serum levels of IL-6, S100β, and NfL were measured preoperatively, at 30 minutes, and 24 hours post-surgery. Perioperative parameters and adverse events were recorded.
Results: The incidence of early postoperative memory decline on days 1 and 3 was significantly lower in the remimazolam group compared to the propofol group (P < 0.05). The remimazolam group also exhibited significantly lower postoperative levels of IL-6 and S100β, more stable hemodynamics, and a reduced incidence of hypotension and bradycardia (all P < 0.05). The incidence of postoperative cognitive dysfunction (POCD) did not differ significantly between groups. Multivariate analysis identified lower educational level, diabetes, propofol use, and longer anesthesia duration as independent risk factors for early postoperative memory decline.
Conclusion: For young and middle-aged patients undergoing laparoscopic surgery, remimazolam reduces the incidence of early postoperative memory decline (within the first three days) and provides superior hemodynamic stability with a milder inflammatory response compared to propofol. However, no significant difference was observed in cognitive function at one month postoperatively, indicating that the benefits are primarily confined to the early recovery period.
Keywords: remimazolam tosylate, propofol, postoperative memory function, laparoscopic surgery
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Zhou has been published for this article.
Corrigendum for this paper has been published.
Introduction
Perioperative neurocognitive disorders (PND) are common central nervous system complications after surgery, primarily encompassing postoperative cognitive dysfunction (POCD) and postoperative delirium (POD).1 They also represent potentially serious complications associated with memory impairment following general anesthesia, characterized by deficits in memory, attention, language comprehension, and social functioning.Studies have shown that subjective cognitive impairment and short-term memory deficits occur in middle-aged patients undergoing both cardiac and non-cardiac surgery. Notably, the incidence of memory impairment after non-cardiac surgery reaches as high as 38.9% at 7 days and 49.0% at 12 months postoperatively.2 Evidence suggests that anesthetic agents may act on multiple ion channels, receptors, and cellular signaling pathways within the central nervous system, thereby affecting cognitive functions such as learning and memory.3 Consequently, the appropriate selection and administration of anesthetics are crucial for patient safety.
Laparoscopic surgery, a major minimally invasive technique, has been widely adopted globally, with clinical adoption rates ranging from 40% to 80%.4 Owing to its benefits of minimal trauma, reduced pain, and fewer complications,5 it is extensively applied across all age groups, with young and middle-aged patients representing a substantial proportion.To satisfy the requirements for artificial pneumoperitoneum and muscle relaxation during such procedures, general anesthesia is the preferred anesthetic modality. Given the high proportion of young and middle-aged patients undergoing laparoscopic surgery and the potential impact of anesthesia on neurocognitive function, comparing the effects of different anesthetic agents has become clinically relevant. Notably, laparoscopic procedures vary in surgical complexity and extent of tissue trauma across different specialties (eg., cholecystectomy, gynecologic surgery, colorectal surgery), which may influence the degree of perioperative stress and neuroinflammatory responses. Acknowledging this heterogeneity provides important context for interpreting postoperative cognitive outcomes.
Propofol is one of the most commonly used sedatives in general anesthesia due to its advantages of rapid induction and recovery. Nevertheless, it is associated with certain adverse effects, such as injection pain and dose-dependent cardiovascular depression.Previous studies have indicated that propofol induces dose-dependent intraoperative amnesia and may even lead to a dissociation between consciousness and memory.6,7 Remimazolam tosylate is a novel benzodiazepine with a short half-life, rapid onset of action, and rapid recovery profile. Emerging evidence suggests that remimazolam may alleviate postoperative cognitive impairment by inhibiting inflammation-associated signaling pathways, attenuating the release of inflammatory cytokines, suppressing oxidative stress, and mitigating neuronal injury.8,9
In clinical practice, anesthesiologists tend to prioritize postoperative recovery in elderly patients and high-risk populations, often paying insufficient attention to young and middle-aged adults with greater demands for memory function. Currently, limited research has been conducted on the effects of remimazolam on postoperative memory function in this patient cohort when administered for both induction and maintenance of general anesthesia. Therefore, this randomized controlled trial was designed to evaluate the impacts of remimazolam tosylate versus propofol on postoperative memory function in young and middle-aged patients undergoing laparoscopic surgery.
Materials and Methods
Ethical Approval
This study was approved by the Ethics Committee of the First Affiliated Hospital of the University of Science and Technology of China (Anhui Provincial Hospital) (Ethics Approval No. 2025KY Lun Audit No. 037) and registered with the China Clinical Trial Registry (Registration No. ChiCTR2500097649).
Inclusion and Exclusion Criteria
Patients aged 18–59 years, with an American Society of Anesthesiologists (ASA) physical status of I–III, a body mass index (BMI) of 18.5–24 kg/m2, and scheduled for laparoscopic surgery under general anesthesia with an anticipated duration of 2–4 hours were eligible for inclusion.Exclusion criteria comprised a history of neurological or psychiatric disorders, or significant craniocerebral trauma; substance or alcohol abuse; known or suspected allergy to the study medications; visual, hearing, or language impairments that could interfere with cognitive testing; exposure to surgeries or medications affecting cognition within one month before or after surgery; use of corticosteroids or non-steroidal anti-inflammatory drugs within one week preoperatively or planned use postoperatively; and a preoperative Three-Word Recall Test (TRT) score <3, Memory and Executive Screening (MES) score ≤75, or Montreal Cognitive Assessment (MoCA) score <26. Patients were withdrawn from the study if they experienced: severe perioperative complications; inadvertent deviation from the anticipated anesthetic duration or changes to the surgical approach; or refusal to cooperate with scale assessments during follow-up or inadvertent use of medications explicitly prohibited by the study protocol.
Sample Size Calculation
Based on a large cohort study reporting an approximate 40% incidence of short-term memory impairment at 7 days after non-cardiac surgery in middle-aged patients,2 we assumed a 40% incidence in the propofol group. To detect a 50% reduction in this incidence in the remimazolam group with a two-sided α of 0.05 and 80% power (1-β= 0.8), an initial sample size of 182 patients was calculated using PASS 15.0 software. Accounting for an anticipated 20% dropout rate, the final sample size was inflated to 114 patients per group, resulting in a total of 228 participants.
Randomization
This prospective randomized controlled trial enrolled young and middle-aged patients undergoing elective laparoscopic surgery at our hospital between February and August 2025. Patients were stratified by gender and educational attainment, then randomly allocated at a 1:1 ratio to the remimazolam group or propofol group via a random number table Allocation sequences were sealed in opaque, sequentially numbered envelopes, which were only accessible to anesthesiologists responsible for anesthetic administration. Patients, follow-up assessors, and data analysts were masked to treatment group assignments.
Anesthesia and Perioperative Care
Upon entering the operating room, peripheral venous access was established, and routine continuous monitoring (Mindray, Shenzhen, China) was commenced, including non-invasive blood pressure, electrocardiography, pulse oxygen saturation (SpO2), and bispectral index (BIS; Covidien IIC, USA). Anesthesia induction was performed after at least 3 minutes of preoxygenation. In the remimazolam group, induction was achieved with remimazolam 0.2–0.3 mg/kg; in the propofol group, induction was achieved with propofol 2.0–2.5 mg/kg.Both agents were administered intravenously via an infusion pump over 1 minute.If adequate sedation (BIS < 60) was not achieved within 1 minute of drug administration, a supplemental dose (remimazolam 0.1–0.2 mg/kg or propofol 0.5 mg/kg) was administered.Following induction, sufentanil 0.5 µg/kg and rocuronium 0.6 mg/kg were administered intravenously.After achieving adequate muscle relaxation, endotracheal intubation and mechanical ventilation were performed.During surgery, the end-tidal carbon dioxide partial pressure (PetCO2) was maintained at 35–45 mmHg. Anesthesia was maintained with remimazolam (0.4–1 mg/kg/h) in Group R and propofol (4–12 mg/kg/h) in Group P, alongside a continuous infusion of remifentanil (0.2–0.4 µg/kg/min) in both groups. Doses of remimazolam or propofol were adjusted to maintain BIS within 40–60. Additionally, cisatracurium was administered intermittently during maintenance to sustain the muscle relaxation required for surgery.
Perioperative hemodynamics were managed with norepinephrine or nicardipine to keep blood pressure within ±10% of baseline, and with atropine or esmolol to maintain heart rate between 50 and 100 beats per minute. Ephedrine was available for use in cases of concurrent hypotension and bradycardia.Infusions of remimazolam/propofol were discontinued upon pneumoperitoneum closure, and remifentanil was terminated upon completion of skin suturing.A patient-controlled intravenous analgesia (PCIA) pump was initiated, containing sufentanil 100 μg and ondansetron 16 mg, with settings as follows: initial bolus 2 mL, background infusion rate 2 mL/h, patient-controlled bolus 2 mL per activation, lockout interval 15 minutes, and maximum hourly limit 8 mL.Patients were transferred to the Post-Anesthesia Care Unit (PACU) immediately postoperatively. Tracheal extubation was performed following spontaneous awakening and recovery of muscle strength. Patients were discharged from the PACU to the ward upon achieving a Steward score >4, with stable vital signs and no complaints of discomfort.
All anesthetic procedures were performed by attending anesthesiologists with at least five years of clinical experience in general anesthesia, who received standardized training on the study protocol prior to patient enrollment.
Data Collection
The primary outcome measure was the incidence of postoperative memory decline in both groups. Meanwhile, mean arterial pressure (MAP) and heart rate (HR) were collected at several key time points, including before anesthesia induction, after tracheal intubation, after pneumoperitoneum establishment, and at emergence.We also recorded intraoperative variables: anesthesia and surgery duration, emergence time, PACU and hospital length of stay, induction dose of the study drugs, the BIS-min value during induction, use of vasoactive drugs, and the incidence of hypotension and bradycardia.Venous blood samples collected at three time points (before anesthesia induction, 30 minutes postoperatively, and 24 hours postoperatively) to measure serum concentrations of IL-6, S100β, and NfL concentrations.Perioperative adverse events, including postoperative nausea and vomiting (PONV), delayed emergence, emergence agitation, and visual analog scale (VAS) pain scores on postoperative day 1, which were monitored and recorded.
Memory and Cognitive Function Assessment
Intra-Hospital Follow-Up
Cognitive and memory function were assessed by a trained investigator on the day before surgery (preoperatively) and on postoperative days 1 (POD 1) and 3 (POD 3). All assessments were conducted in a quiet room by the same investigator, who was blinded to patient group assignments. The Three-Word Recall Test (TRT) and Memory and Executive Screening (MES) Scale were used to evaluate memory function changes, while the Montreal Cognitive Assessment (MoCA) was applied to assess global cognitive function. Postoperative memory decline was defined as a TRT score < 3 and an MES score ≤ 75. Postoperative cognitive dysfunction (POCD) was defined as a MoCA score < 26.
Post-Discharge Follow-Up
Cognitive and memory function were evaluated via telephone interview 1 month postoperatively using the Telephone Interview for Cognitive Status-modified (TICS-m). During the interview, family members were instructed to turn off televisions and radios, remove paper and pens to minimize distractions, maintain a quiet environment, and avoid external interruptions. A TICS-m score > 31 indicated normal cognitive function, while a score < 28 indicated severe cognitive impairment.10
Details of Assessment Scales
(1) Three-Word Recall Test (TRT):This test requires participants to recall three unrelated words shortly after presentation (typically interspersed with several brief intervening questions), serving as an objective measure of short-term memory, a key aspect of cognitive function.We used the Word Recall part of the Mini-Cog24 and applied different words listed in the Three Word Registration for each survey. The TRT is considered a sensitive screening tool for amnesia among individuals with mild cognitive impairment (MCI).11 Scores range from 0 to 3, with lower scores indicating more severe short-term memory impairment; we defined a score less than 3 as TRT abnormality, indicating short-term memory impairment.
(2) Memory and Executive Screening (MES) Scale:The MES consists of two subscales (Memory [M] and Executive [E]) with a total score out of 100. Research indicates that an MES total score ≤75 identifies amnestic mild cognitive impairment (aMCI) with an area under the curve (AUC) of 0.89,a sensitivity of 80%, and a specificity of 83%.12 In addition to assessing core memory functions, the MES comprehensively evaluates executive functions through tasks such as semantic fluency and digit-symbol coding. It enables rapid assessment of impairments in major cognitive domains, including executive function and episodic memory, without ceiling or floor effects.12
(3) Montreal Cognitive Assessment (MoCA):A sensitive and widely used screening tool for MCI, the MoCA demonstrates a sensitivity of 90% and a specificity of 87%.13,14 It assesses cognitive function across eight domains: visual-spatial and executive function, naming, memory, attention and calculation, language, abstraction, delayed recall, and orientation. The total score is 30 points, with 1 additional point added for participants with ≤ 12 years of education.
(4) Telephone Interview for Cognitive Status-modified (TICS-m):One of the most widely used telephone-based cognitive assessment tools, the TICS-m exhibits excellent reliability and validity, with higher validity for MCI than the Mini-Mental State Examination (MMSE).15 The results require adjustment based on years of education: add 5 points for individuals with <8 years of education, add 2 points for 8–10 years, no adjustment for 11–15 years, and subtract 2 points for those with ≥16 years of education. An education-adjusted TICS-m score ≤ 31 is the optimal cutoff for distinguishing cognitively impaired individuals from the general population.10
Enzyme-Linked Immunosorbent Assay
Venous blood samples were collected preoperatively (before anesthesia induction), 30 minutes postoperatively, and 24 hours postoperatively to measure serum concentrations of IL-6, S100β, and NfL. The samples were centrifuged at 3000 × g for 15 minutes at 4 °C, and the separated serum was stored at −80 °C until batch analysis. Serum IL-6, S100β, and NfL concentrations were quantified using enzyme-linked immunosorbent assay (ELISA) kits (Lunchangshuo, Xiamen, China) in accordance with the manufacturer’s instructions.
Statistical Analysis
Statistical analysis was performed using SPSS 30.0 and GraphPad Prism 9.0.Continuous variables were tested for normality with the Kolmogorov–Smirnov test. Those following a normal distribution are reported as mean ± SD and compared with the independent t-test; non-parametric data are reported as median (IQR) and compared with the Mann–Whitney U-test. Categorical data, presented as n (%), were analyzed by the χ2-test or Fisher’s exact test.Univariate logistic regression analysis was performed as the initial step to identify potential risk factors for postoperative memory decline. Variables with P < 0.05 in the univariate analysis were included in a multivariate logistic regression model to adjust for potential confounders. Multicollinearity was assessed using the variance inflation factor (VIF), and the model’s goodness-of-fit was evaluated with the Hosmer-Lemeshow test. The predictive accuracy of the model was determined by the area under the receiver operating characteristic (ROC) curve.P < 0.05 was considered statistically significant.
Results
Patient Characteristics and Baseline Data
The study flow is depicted in Figure 1. Based on the inclusion and exclusion criteria, 228 patients were ultimately enrolled and randomly allocated to the remimazolam (R) group or propofol (P) group. In the remimazolam group, 4 patients were excluded: 2 due to intraoperative changes in surgical approach and 2 due to prolonged anesthesia duration. In the propofol group, 3 patients were excluded (2 due to changes in surgical approach and 1 due to prolonged anesthesia duration). Ultimately, 110 patients in the remimazolam group and 111 patients in the propofol group completed the study per protocol and were included in the final analysis. Baseline characteristics of patients in both groups are summarized in Table 1, with no statistically significant differences between groups (P > 0.05).
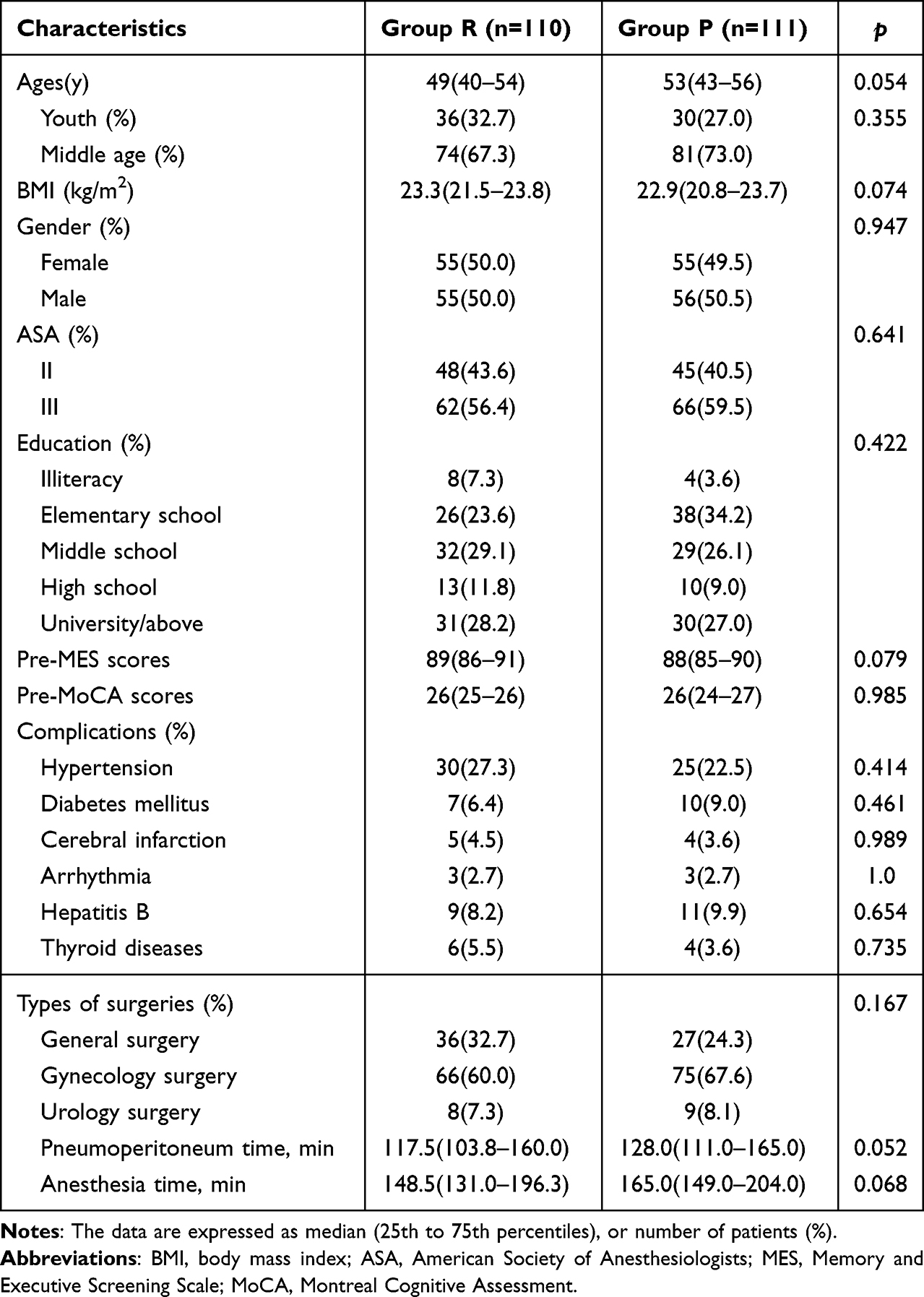 |
Table 1 Basic Characteristics |
 |
Figure 1 Flow Diagram of the Study. |
Memory and Cognitive Outcomes
The incidence of postoperative memory decline in the remimazolam group was significantly lower than in the propofol group on postoperative day 1 (36.4% vs. 53.2%, P < 0.05) and postoperative day 3 (23.6% vs. 37.8%, P < 0.05; Table 2). The incidence of postoperative cognitive dysfunction (POCD) in the remimazolam group was numerically lower than in the propofol group on POD 1 (27.3% vs. 35.1%, P = 0.207), POD 3 (16.4% vs. 22.5%, P = 0.248), and 1 month postoperatively (6.4% vs. 8.1%, P = 0.617); however, these between-group differences were not statistically significant (Figure 2).
 |
Table 2 The Incidence of Postoperative Memory Decline and Postoperative Cognitive Decline in Patients Under General Anesthesia with Different Drugs |
 |
Figure 2 Postoperative changes in memory and cognitive function in two groups of patients. Notes: (A) MAP at different time points in the two groups; (B) HR at different time points in the two groups. |
Hemodynamics and Intraoperative Conditions
Statistical analysis of perioperative hemodynamic parameters showed temporal variations in mean arterial pressure (MAP) and heart rate (HR) in both groups. Significant between-group differences were noted at two time points: after intubation and after pneumoperitoneum (P < 0.05, Figure 3A and B).The use of remimazolam was associated with superior hemodynamic stability, resulting in a lower incidence of hypotension (6.4% vs. 16.2%) and bradycardia (15.5% vs. 30.6%), alongside a reduced requirement for vasoactive agents (atropine and norepinephrine) (Table 3).Compared with the propofol group, the remimazolam group had a significantly higher maximum electroencephalographic (EEG) effect during induction [47 (42–48) vs. 44 (41–48), P < 0.05, Figure 3C], whereas the total remifentanil dosage was significantly lower [8.06 (7.30–9.08) mg vs. 8.82 (7.74–9.79) mg, P < 0.05, Figure 3D].
 |
Table 3 Comparison of the Incidence of Hypotension and Bradycardia and the Use of Vasoactive Drugs Between the Two Groups |
 |
Figure 3 Comparison of MAP, HR and some anesthesia variables in the two groups. Abbreviation: BIS, bispectral index. Notes: (A) MAP at different time points in the two groups; (B) HR at different time points in the two groups; (C) Comparison of BIS-min during induction of anesthesia in the two groups; (D) Comparison of rimazolam dosage between two groups. * indicates p < 0.05. |
Levels of IL-6, S100-β, and NfL
Compared with pre-induction levels, serum concentrations of IL-6 and S100β were significantly increased at 30 minutes postoperatively in both groups (P < 0.05), with no statistically significant difference noted in NfL concentration. At 24 hours postoperatively, IL-6 concentration remained significantly elevated in the propofol group (P < 0.05), whereas no statistically significant differences were observed in S100β or NfL concentrations. Relative to the propofol group, the remimazolam group had significantly lower serum IL-6 and S100β concentrations at both 30 minutes and 24 hours postoperatively (P < 0.05); no statistically significant between-group difference was found in NfL concentration (Figure 4A–C).Additionally, patients with postoperative memory decline had significantly higher serum IL-6 and S100β concentrations at 24 hours postoperatively than those without memory decline (P < 0.05), while no significant difference in NfL concentration was detected between these two subgroups (Figure 4D–F).
 |
Figure 4 Comparison of IL-6, S-100β and NfL levels in patients during perioperative period. Abbreviation: POMD, postoperative memory decline. Notes: (A) IL-6 concentration in the two groups; (B) S-100β concentration in the two groups; (C) NfL concentration in the two groups; (D) IL-6 concentration between patients with or without POMD; (E) S-100β concentration between patients with or without POMD; (F) NfL concentration between patients with or without POMD.* indicates p < 0.05. |
Perioperative Parameters and Adverse Events
Intra-hospital comparisons between the two groups revealed no statistically significant differences in pneumoperitoneum duration, time to emergence, PACU or hospital length of stay (Figure 5A–D). For perioperative adverse events, no significant between-group differences were noted in the incidence of PONV, delayed emergence, emergence agitation, or VAS pain scores at 1 day postoperatively (Figure 5E–H).
 |
Figure 5 Comparison of perioperative parameters between two groups. Abbreviations: PACU, Post-Anesthesia Care Unit; PONV, Postoperative Nausea and Vomiting; POD1, Post-Operative Day 1. Notes: (A) Comparison of pneumoperitoneum duration between the two groups; (B) Comparison of the time to emergence between the two groups; (C) Comparison of PACU stay duration between the two groups; (D) Comparison of hospital length of stay between the two groups; (E) Comparison of the incidence of delayed emergence between two groups; (F) Comparison of the incidence of emergence agitation between two groups; (G) Comparison of PONV cases between the two groups; (H) Comparison of VAS pain scores on the POD1 between the two groups. ns indicates no significance. |
Prognostic Factors for Postoperative Memory Decline
Univariate logistic regression analysis identified age, ASA physical status classification, educational attainment, preoperative MES and MoCA scores, hypertension, diabetes mellitus, anesthetic drugs, anesthesia and pneumoperitoneum time, time to emergence, and the duration of hospitalization as risk factors for postoperative memory decline (Supplement 1). The incidence of postoperative memory decline was positively associated with increasing age, a history of hypertension or diabetes mellitus, ASA physical status III, and longer anesthesia and hospitalization durations.Conversely, higher preoperative MES and MoCA scores, higher educational level, and the use of remimazolam were inversely associated with the incidence of postoperative memory decline.
Variables with univariate significance (P < 0.05) were included in the multivariate logistic regression model to adjust for potential confounders. Assessment of multicollinearity using the variance inflation factor (VIF) revealed a high correlation between anesthesia duration and pneumoperitoneum duration (VIF > 10). After removing confounders, all retained variables exhibited VIF < 2.9 (1.052–2.836), indicating less collinearity. The model demonstrated good fit (Hosmer-Lemeshow test, P = 0.371) and possessed excellent predictive accuracy, as evidenced by an area under the curve (AUC) of 0.937 (95% CI: 0.906–0.968). Finally, educational level, diabetes, the use of propofol (versus remimazolam), and anesthesia time were identified as independent risk factors for early postoperative memory decline (Figure 6).
 |
Figure 6 Multivariate Logistic regression analysis of risk factors associated with postoperative memory decline. Abbreviations: ASA, American Society of Anesthesiologists; MES, Memory and Executive Screening Scale; MoCA, Montreal Cognitive Assessment; OR, Odds Ratio. |
Discussion
The present randomized controlled trial supports the superiority of remimazolam over the conventional anesthetic propofol for reducing postoperative memory impairment in young and middle-aged adults undergoing laparoscopic surgery, with demonstrated benefits in hemodynamic safety and stability. By focusing on this specific demographic, our study addresses a notable gap in clinical neurocognitive function research regarding younger patients. These findings contribute valuable insights to the growing body of literature on anesthetic neuroprotection, particularly within the context of increasingly prevalent laparoscopic procedures.
Postoperative memory decline represents a key component of PND. Previous studies have demonstrated that remimazolam exerts favorable neurocognitive protective effects. In a retrospective analysis of 98 TAVI patients reported a significantly lower incidence of PND within 3 postoperative days in the remimazolam group compared with the propofol group (8% vs. 26%).16 In our study, the incidence of postoperative memory decline in the propofol group was consistent with previous reports,2 while the remimazolam group exhibited a significantly lower incidence. Propofol potentiates GABAA receptors and inhibits NMDA receptors, thereby suppressing long-term potentiation (LTP) and facilitating long-term depression (LTD) in the hippocampal CA1 region. It also promotes serotonin release, consequently affecting learning and memory functions.17–20 Studies indicate that remimazolam significantly mitigates impairment of short-term learning and memory in juvenile mice compared to the traditional benzodiazepine midazolam. The underlying mechanism may involve attenuated hippocampal neuronal apoptosis, downregulated PSD95 expression, and inhibited hippocampal LTP.21 As a novel ultra-short-acting benzodiazepine, remimazolam exerts its pharmacological effects via positive allosteric modulation of GABAA receptors,enhancing GABAergic neurotransmission and inducing anterograde amnesia. Notably, the α5 subunit of GABAA receptors is highly expressed in the hippocampus and critically involved in memory encoding and consolidation.Activation of the α5 subunit by conventional benzodiazepines is considered a key factor contributing to anterograde amnesia and memory impairment.22 Although remimazolam also activates these receptors, it possesses unique pharmacokinetic properties: rapid hydrolysis by tissue esterases, renal or hepatic function-independent metabolism, and a short elimination half-life.23 These features may result in a transient and controllable activation of the α5 subunit, potentially enabling remimazolam to provide effective sedation while significantly reducing persistent intraoperative memory impairment. Consequently, it demonstrates milder postoperative memory deficits and more rapid recovery of cognitive function.
Mild cognitive impairment (MCI) represents an intermediate stage between normal cognition and the onset of dementia.During this phase, patients may exhibit declines in memory or other cognitive functions; however, these do not interfere with activities of daily living and do not meet the diagnostic criteria for dementia.24 Amnestic mild cognitive impairment(aMCI) is a common subtype of MCI, characterized predominantly by memory decline, and is most closely associated with Alzheimer’s disease(AD).25 While clinical attention is often focused on postoperative cognitive function in the elderly patients, we frequently overlook postoperative cognitive outcomes in young and middle-aged patients who reside in learning or working environments requiring higher memory capacity. The TRT is brief and easy to administer, yet its simple memory task places low cognitive demands, potentially leading to underdiagnosis of MCI. The MES scale addresses this limitation, demonstrating high sensitivity and strong specificity in identifying MCI.26 Given that postoperative cognitive changes in young and middle-aged patients are typically subtle, the MES’s high sensitivity to mild cognitive deficits facilitates earlier and more accurate identification of patients at risk for POCD.In the present study, both TRT and MES scores were used as objective indicators of postoperative memory impairment.POCD is clinically characterized by concurrent impairments across multiple cognitive domains, including memory encoding and retrieval, working memory, and executive function.27 The MES scale enables rapid assessment of deficits in key cognitive domains, such as executive function and episodic memory. It comprehensively and precisely reflects the cognitive domains most vulnerable to postoperative impairment, overcoming the limitations of unidimensional assessment while providing direction for subsequent clinical intervention priorities.
Compared with propofol, remimazolam demonstrated superior perioperative hemodynamic stability in our study, significantly reducing the incidence of hypotension and bradycardia, as well as decreasing the requirement for vasoactive agents, which is consistent with previous findings. Propofol frequently induces marked dose-dependent hypotension and bradycardia due to its potent direct vasodilatory and myocardial depressant effects.28 Intraoperative hypotension is a well-established risk factor for PND by inducing cerebral hypoperfusion, particularly impairing function in the highly ischemia-sensitive hippocampal region,29 it triggers neuroinflammation and synaptic dysfunction, potentially leading to postoperative memory impairment.30,31 Therefore, reducing the occurrence of perioperative hypotension may effectively lowers the risk of PND and other neurocognitive complications.32 Notably, patients in the remimazolam group exhibited a higher maximum electroencephalographic(EEG) effect during anesthesia induction compared with the propofol group, suggesting that while remimazolam effectively induced unconsciousness, it produced less synchronized cortical inhibition, preserved more EEG activity, and afforded a wider neural safety margin with improved clinical safety.Concurrently, we observed that remimazolam significantly reduced required remifentanil dosage compared with propofol while maintaining equivalent anesthetic depth. This may be attributed to remimazolam’s analgesic properties, which involve enhanced inhibition of spinal dorsal horn interneurons via GABAA receptor modulation.33 Reduced remifentanil dosage directly diminishes its dose-dependent cardiovascular suppression, contributing to more stable hemodynamics throughout anesthesia. Additional benefits include lower risks of postoperative acute opioid tolerance and hyperalgesia,34 potentially simplifying early postoperative pain management.
Inflammatory responses and elevated S100β protein levels are both significant factors contributing to POCD.35,36 IL-6 mediates early inflammatory responses and tissue damage, with its expression levels correlated with systemic and central nervous system inflammatory states. S100β protein serves as a biomarker for blood-brain barrier integrity and astrocyte injury, and is regarded as a specific predictor of PND.37 In this study, postoperative IL-6 and S100β levels were significantly elevated compared with preoperative baseline in all patients, with notably higher concentrations observed in those with postoperative memory decline. This finding may be associated with surgery-induced release of inflammatory factors and subsequent neuroinflammatory responses. Studies have shown that the activity of α5 GABAA receptors, which are widely distributed in the hippocampus can be activated by anesthetic drugs, also increases during inflammation and that this increase is critical for inflammation-induced memory deficits.38 The remimazolam group exhibited lower concentrations of IL-6 and S100β at both postoperative time points compared with the propofol group, suggesting that remimazolam may attenuate postoperative inflammation and exert a milder impact on cognitive function. Emerging evidence indicates that remimazolam can provide neuroprotective effects by inhibiting neuronal apoptosis and reducing the expression and release of inflammatory factors.39,40 In contrast, propofol’s lipophilicity and potential to activate microglia might exacerbate hippocampal inflammation, thereby contributing to memory impairment. No significant differences in serum NfL levels were observed either between groups or across time points in this study. NfL is a delayed biomarker of neuronal axonal injury. Since a latency period is required for NfL to be released into the bloodstream following axonal injury, the relatively early detection time points selected in this study may explain the lack of observed between-group differences in serum NfL levels postoperatively.
Although the direct pharmacological effects of remimazolam and propofol typically dissipate within hours post-surgery, these agents can initiate a cascade of perioperative events, including neuroinflammation, oxidative stress, and neuronal injury. The downstream consequences of these reactions may persist long after the drugs themselves have been cleared from the system. Furthermore, surgical trauma, systemic inflammatory responses, blood-brain barrier disruption, postoperative pain, and sleep disturbances can all trigger sustained neuroinflammatory reactions and synaptic dysfunction, thereby exerting lasting effects on cognitive function. As highlighted by Yang et al2 the incidence of short-term memory impairment after non-cardiac surgery exhibits a dynamic U-shaped trajectory, suggesting that early and late cognitive outcomes may be driven by distinct yet interconnected mechanisms. While our study did not find a significant difference in the incidence of POCD between the two groups at one month post-surgery, assessing this intermediate time point remains clinically valuable. It serves as a crucial bridge connecting early postoperative changes (postoperative days 1–3) with potential long-term cognitive decline, helping to differentiate between patients who achieve complete short-term recovery and those who may experience persistent or progressive cognitive impairment, thus providing foundational data for future studies with longer follow-up periods. Moreover, for young and middle-aged patients, the ability to return to baseline cognitive function at one month post-surgery is a critical determinant of their quality of life and capacity to resume work. Therefore, while the one-month cognitive assessment does not directly reflect the immediate effects of the drugs, it offers an important perspective on the cumulative impact of multiple perioperative factors on patient prognosis, making it an essential component of comprehensively evaluating anesthetic drug safety and patient outcomes.
To identify the risk factors affecting postoperative memory function, univariate logistic regression analysis was performed and the results were basically consistent with previous studies.41–43 Further multivariate regression analysis revealed that educational attainment, diabetes mellitus, anesthetic drug selection, and anesthesia duration were independent risk factors for postoperative memory decline. Contrary to previous reports identifying age as an independent risk factor for POCD, we found age was not identified as such in the present study, potentially related to our study population selection.Younger patients possess greater physiological reserve capacity than older individuals, enabling them to better tolerate the trauma of anesthesia and surgery. Additionally, laparoscopic surgery is associated with relatively minimal invasiveness, potentially resulting in a lower overall burden of neuroinflammation and physiological stress, thereby attenuating the impact of age as a risk factor. Furthermore, our finding that diabetes increases the risk of postoperative memory decline is consistent with a meta-analysis reporting a 44% elevated POCD risk in diabetic patients.44 We speculate that this may be related to the pathophysiological features of diabetes. Sustained hyperglycemia exhibits neurotoxicity,45 while hypoglycemia can lead to neuronal hypoxia, particularly reducing hippocampal glutathione levels, resulting in impairments in spatial and contextual memory.46 Diabetic patients are more prone to perioperative glycemic fluctuations than non-diabetic patients,47 which may adversely affect their cognitive prognosis. Therefore, in clinical practice, it is essential to develop appropriate perioperative neurocognitive protection strategies for diabetic patients with diverse backgrounds.
The present study has several limitations.First, it was a single-center study, with data collected from only one research center, necessitating further multi-center studies to confirm the generalizability of our findings.Second, although all procedures included were laparoscopic surgeries, invasiveness varies across surgical specialties, which may confound the evaluation of neuroinflammatory responses and cognitive outcomes. Finally, we only evaluated early postoperative changes in memory and cognitive function, without assessing long-term memory and cognitive performance following hospital discharge. Future studies should address this limitation by incorporating long-term neurocognitive prognosis into the research scope to provide more comprehensive evidence.
Conclusion
For young and middle-aged patients undergoing elective laparoscopic surgery, remimazolam tosylate for anesthetic induction and maintenance effectively reduces the incidence of early postoperative memory impairment, lowers the risk of perioperative hypotension and bradycardia, and exhibits superior performance in maintaining hemodynamic stability and mitigating postoperative inflammatory responses. This study validates the safety and efficacy of remimazolam for anesthetic induction and maintenance. Compared with propofol, remimazolam offers distinct clinical advantages in protecting perioperative neurocognitive function in this patient population, supporting its broader clinical application. Further studies with longer follow-up periods are warranted to determine whether these early cognitive benefits translate into sustained improvements in long-term neurocognitive outcomes.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of the First Affiliated Hospital of the University of Science and Technology of China (Anhui Provincial Hospital) (Ethics Approval No. 2025KY Lun Audit No. 037) and registered with the China Clinical Trial Registry (Registration No. ChiCTR2500097649).All study procedures were conducted in accordance with the Helsinki Declaration of 1964 (as revised in 2013). All subjects signed an informed consent form after being made fully aware of the research content and risks.
Funding
National Natural Science Foundation of China, 82272225.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Evered L, Silbert B, Knopman DS, et al. Recommendations for the nomenclature of cognitive change associated with anaesthesia and surgery-2018. Br J Anaesth. 2018;121(5):1005–15. doi:10.1016/j.bja.2017.11.087
2. Yang L, Chen W, Yang D, et al. Postsurgery subjective cognitive and short-term memory impairment among middle-aged Chinese patients. JAMA Network Open. 2023;6(10):e2336985. doi:10.1001/jamanetworkopen.2023.36985
3. Moody OA, Zhang ER, Vincent KF, et al. The neural circuits underlying general anesthesia and sleep. Anesthesia Analgesia. 2021;132(5):1254–1264. doi:10.1213/ANE.0000000000005361
4. Dekker E, Tanis PJ, Vleugels JLA, Kasi PM, Wallace MB. Colorectal cancer. Lancet. 2019;394(10207):1467–1480.
5. Fan Y, Liu X, Wu S, Liu Y. The risk factors for cognitive dysfunction in elderly patients after laparoscopic surgery: a retrospective analysis. Medicine. 2021;100(2):e23977. doi:10.1097/MD.0000000000023977
6. Moon DU, Esfahani-Bayerl N, Finke C, et al. Propofol modulates early memory consolidation in humans. eNeuro. 2020;7(3). doi:10.1523/ENEURO.0537-19.2020
7. Zhang J, Zhang X, Jiang W. Propofol impairs spatial memory consolidation and prevents learning-induced increase in hippocampal matrix metalloproteinase-9 levels in rat. Neuroreport. 2013;24(15):831–836. doi:10.1097/WNR.0b013e328364fe69
8. Yin T, He L, Du Y, et al. Macrophage WNK1 senses intracellular hypo-chlorine to regulate vulnerability to sepsis attack during hypochloremia. Int Immunopharmacol. 2024;139:112721. doi:10.1016/j.intimp.2024.112721
9. Liao YQ, Min J, Wu ZX, Hu Z. Comparison of the effects of remimazolam and dexmedetomidine on early postoperative cognitive function in elderly patients with gastric cancer. Front Aging Neurosci. 2023;15:1123089. doi:10.3389/fnagi.2023.1123089
10. Knopman DS, Roberts RO, Geda YE, et al. Validation of the telephone interview for cognitive status-modified in subjects with normal cognition, mild cognitive impairment, or dementia. Neuroepidemiology. 2010;34(1):34–42. doi:10.1159/000255464
11. Diniz BS, Yassuda MS, Nunes PV, Radanovic M, Forlenza OV. Mini-mental State Examination performance in mild cognitive impairment subtypes. Int Psychogeriatrics. 2007;19(4):647–656. doi:10.1017/S104161020700542X
12. Li X, Zhao Q, Guo Q, Hong Z. Diagnostic value of the memory and executive function screening test in the assessment of cognitive impairment severity in Alzheimer’s disease. Chin J Clin Neurosci. 2013;21(5):548–553.
13. Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatri Soc. 2005;53(4):695–699.
14. Kang JM, Cho YS, Park S, et al. Montreal cognitive assessment reflects cognitive reserve. BMC Geriatr. 2018;18(1):261. doi:10.1186/s12877-018-0951-8
15. Meng C, Zhang X, Bi Z, et al. Telephone interview for cognitive status-modified used in screening cognitive impairment. Chin J Neurol. 2005;38(1):30–33.
16. Kaneko S, Morimoto T, Ichinomiya T, Murata H, Yoshitomi O, Hara T. Effect of remimazolam on the incidence of delirium after transcatheter aortic valve implantation under general anesthesia: a retrospective exploratory study. J Anesthesia. 2023;37(2):210–218. doi:10.1007/s00540-022-03148-2
17. Nagashima K, Zorumski CF, Izumi Y. Propofol inhibits long-term potentiation but not long-term depression in rat hippocampal slices. Anesthesiology. 2005;103(2):318–326. doi:10.1097/00000542-200508000-00015
18. Xie Y, Zeng B, Xu L, Li X. The effects of propofol on long-term depression in hippocampalCAlneurons of rats. J Clin Anesthesiol. 2004;20(12):730–732.
19. Shen Y, Xue X, Lyu H. The research advances of effects of propofol on long-term potentiation and its mechanism. Int J Anesthesiol Resuscitat. 2020;41(7):692–695.
20. Rudolph U, Antkowiak B. Molecular and neuronal substrates for general anaesthetics. Nat Rev Neurosci. 2004;5(9):709–720. doi:10.1038/nrn1496
21. Shi W, Wu X, Yuan C, et al. Effect of remimazolam toluene sulfonate on the cognitive function of juveniles and its mechanism of action. Eur J Med Res. 2024;29(1):543. doi:10.1186/s40001-024-02142-6
22. Zurek AA, Yu J, Wang DS, et al. Sustained increase in α5GABAA receptor function impairs memory after anesthesia. J Clin Investigation. 2014;124(12):5437–5441. doi:10.1172/JCI76669
23. Brohan M, Brohan J, Goudra B. Remimazolam and its place in the current landscape of procedural sedation and general anesthesia. J Clin Med. 2024;13(15):4362. doi:10.3390/jcm13154362
24. Jongsiriyanyong S, Limpawattana P. Mild cognitive impairment in clinical practice: a review article. Am J Alzheimer’s Dis Other Dementias. 2018;33(8):500–507. doi:10.1177/1533317518791401
25. Petersen RC. Mild cognitive impairment: current research and clinical implications. Semin Neurol. 2007;27(1):22–31. doi:10.1055/s-2006-956752
26. Guo QH, Zhou B, Zhao QH, Wang B, Hong Z. Memory and Executive Screening (MES): a brief cognitive test for detecting mild cognitive impairment. BMC Neurol. 2012;12:119. doi:10.1186/1471-2377-12-119
27. Kapoor I, Prabhakar H, Mahajan C. Postoperative cognitive dysfunction. Indian J Crit Care Med. 2019;23(Suppl 2):S162–S164.
28. Li T, Han W, Yang X, et al. Effects of different injection rates of propofol on postoperative cognition in elderly patients undergoing laparoscopic inguinal hernia repair. Drug Des Devel Ther. 2023;17:1741–1752. doi:10.2147/DDDT.S407905
29. Cai J, Tang M, Wu H, et al. Association of intraoperative hypotension and severe postoperative complications during non-cardiac surgery in adult patients: a systematic review and meta-analysis. Heliyon. 2023;9(5):e15997. doi:10.1016/j.heliyon.2023.e15997
30. Xu X, Hu X, Wu Y, et al. Effects of different BP management strategies on postoperative delirium in elderly patients undergoing Hip replacement: a single center randomized controlled trial. J Clin Anesthesia. 2020;62:109730. doi:10.1016/j.jclinane.2020.109730
31. Siepe M, Pfeiffer T, Gieringer A, et al. Increased systemic perfusion pressure during cardiopulmonary bypass is associated with less early postoperative cognitive dysfunction and delirium. Eur J Cardiothorac Surg. 2011;40(1):200–207. doi:10.1016/j.ejcts.2010.11.024
32. Scholz AF, Oldroyd C, McCarthy K, Quinn TJ, Hewitt J. Systematic review and meta-analysis of risk factors for postoperative delirium among older patients undergoing gastrointestinal surgery. Br J Surg. 2016;103(2):e21–28. doi:10.1002/bjs.10062
33. Hoshino R, Ohashi N, Uta D, Ohashi M, Deguchi H, Baba H. Actions of remimazolam on inhibitory transmission of rat spinal dorsal horn neurons. J Pharmacol Sci. 2024;155(2):63–73. doi:10.1016/j.jphs.2024.04.002
34. Zhu K, Wen X, Mei X, Fang F, Zhang T. Mechanisms of remifentanil-induced postoperative hyperalgesia: a comprehensive review. Drug Des Devel Ther. 2025;19:7445–7457. doi:10.2147/DDDT.S550335
35. Hu J, Feng X, Valdearcos M, et al. Interleukin-6 is both necessary and sufficient to produce perioperative neurocognitive disorder in mice. Br J Anaesth. 2018;120(3):537–545. doi:10.1016/j.bja.2017.11.096
36. Peng L, Xu L, Ouyang W. Role of peripheral inflammatory markers in postoperative cognitive dysfunction (POCD): a meta-analysis. PLoS One. 2013;8(11):e79624. doi:10.1371/journal.pone.0079624
37. Schmidt AP, Carmona MJC. Serum biomarkers of brain injury: S100B protein, cognitive dysfunction, and major non-cardiac surgery. Brazilian J Anesthesiol. 2020;70(6):570–572.
38. Wang DS, Zurek AA, Lecker I, et al. Memory deficits induced by inflammation are regulated by α5-subunit-containing GABAA receptors. Cell Rep. 2012;2(3):488–496. doi:10.1016/j.celrep.2012.08.022
39. Shi M, Chen J, Liu T, et al. Protective effects of remimazolam on cerebral ischemia/reperfusion injury in rats by inhibiting of NLRP3 inflammasome-dependent pyroptosis. Drug Des Devel Ther. 2022;16:413–423. doi:10.2147/DDDT.S344240
40. Zhang Z, Xu X, Ma J, et al. Gene deletion of Gabarap enhances Nlrp3 inflammasome-dependent inflammatory responses. J Immunol. 2013;190(7):3517–3524. doi:10.4049/jimmunol.1202628
41. Monk TG, Weldon BC, Garvan CW, et al. Predictors of cognitive dysfunction after major noncardiac surgery. Anesthesiology. 2008;108(1):18–30. doi:10.1097/01.anes.0000296071.19434.1e
42. Wang Z, van Veluw SJ, Wong A, et al. Risk factors and cognitive relevance of cortical cerebral microinfarcts in patients with ischemic stroke or transient ischemic attack. Stroke. 2016;47(10):2450–2455. doi:10.1161/STROKEAHA.115.012278
43. Wei Y, Zhang C, Wang D, Wang C, Sun L, Chen P. Progress in research on the effect of melatonin on postoperative cognitive dysfunction in older patients. Front Aging Neurosci. 2022;14:782358. doi:10.3389/fnagi.2022.782358
44. Liu H, Chen J, Ling J, et al. The association between diabetes mellitus and postoperative cognitive dysfunction: a systematic review and meta-analysis. Int J Surg. 2025;111(3):2633–2650.
45. Tomlinson DR, Gardiner NJ. Glucose neurotoxicity. Nat Rev Neurosci. 2008;9(1):36–45. doi:10.1038/nrn2294
46. Languren G, Montiel T, Ramírez-Lugo L, et al. Recurrent moderate hypoglycemia exacerbates oxidative damage and neuronal death leading to cognitive dysfunction after the hypoglycemic coma. J Cerebral Blood Flow Metabolism. 2019;39(5):808–821.
47. Lipska KJ, Venkitachalam L, Gosch K, et al. Glucose variability and mortality in patients hospitalized with acute myocardial infarction. Circ Cardiovasc Qual Outcomes. 2012;5(4):550–557. doi:10.1161/CIRCOUTCOMES.111.963298
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Remimazolam Tosylate Combined with Low-Dose Propofol Improves Sedation and Safety in Hysteroscopy
Zhang F, Chang H, Qing W, Yu R, Liao Q, Tong J
Drug Design, Development and Therapy 2022, 16:4101-4108
Published Date: 29 November 2022
Comparative Study About Different Doses of Remimazolam in Short Laparoscopic Surgery: A Randomized Controlled Double-Blind Trial
Luo L, Jiang J, Zhang M, Guo Z, Zhang X, Wang F, Yang F
Therapeutics and Clinical Risk Management 2023, 19:829-837
Published Date: 20 October 2023
Esketamine Accelerates Emergence from Propofol Anesthesia in Patients Undergoing Laparoscopic Gynecological Surgery: A Randomized Controlled Trial
Qi Y, Ren Y, Xu W, Chen J, Wang L, Huang H, Zhou M, Wang L
Drug Design, Development and Therapy 2026, 20:608572
Published Date: 3 June 2026