Back to Journals » Drug Design, Development and Therapy » Volume 20
Esketamine Accelerates Emergence from Propofol Anesthesia in Patients Undergoing Laparoscopic Gynecological Surgery: A Randomized Controlled Trial
Authors Qi Y ![]() , Ren Y
, Ren Y ![]() , Xu W, Chen J
, Xu W, Chen J ![]() , Wang L, Huang H, Zhou M, Wang L
, Wang L, Huang H, Zhou M, Wang L
Received 11 March 2026
Accepted for publication 26 May 2026
Published 3 June 2026 Volume 2026:20 608572
DOI https://doi.org/10.2147/DDDT.S608572
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Muzammal Hussain
Yu Qi,1– 3,* Ying Ren,1,3,* Wenjing Xu,1,3,* Jiao Chen,2,3 Long Wang,2,3 Hanchao Huang,1,3 Meiyan Zhou,2,3 Liwei Wang1– 3
1The Clinical College of Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China; 2Department of Anesthesiology, Xuzhou Central Hospital, Southeast University, Xuzhou, Jiangsu, People’s Republic of China; 3Department of Anesthesiology, Xuzhou Central Hospital, Xuzhou, Jiangsu, People’s Republic of China
*These authors contributed to the work equally
Correspondence: Meiyan Zhou, Email [email protected] Liwei Wang, Email [email protected]
Purpose: While esketamine has shown promise in enhancing the quality of anesthesia recovery, its effect on a critical recovery endpoint—extubation time—has yielded inconsistent results across clinical studies. Therefore, this study investigated the effect of esketamine on extubation time in patients undergoing general anesthesia.
Methods: In this single-center, randomized, double-blind, placebo-controlled trial (RCT), we enrolled 154 patients scheduled for elective laparoscopic hysterectomy. Patients were randomly assigned to receive either intravenous esketamine (a bolus of 0.2 mg/kg at induction, followed by a continuous infusion of 0.125 mg/kg/h) or an equivalent volume of normal saline as placebo. For all patients, a transversus abdominis plane (TAP) block was performed with 0.25% ropivacaine at the end of surgery. The primary analysis was conducted according to a modified intention-to-treat (mITT) principle, including all randomized patients who received the allocated intervention and had the primary outcome assessed. The sample size was calculated to provide 90% power to detect a 4-minute difference in extubation time. The primary outcome was the time to extubation in the post-anesthesia care unit (PACU). The Bonferroni correction was applied to secondary outcomes to adjust for multiple comparisons.
Results: A total of 141 patients completed the study (Esketamine group: n=70; Control group: n=71). Compared to the control group, the esketamine group had a significantly shorter extubation time (23.2 ± 5.2 minutes vs. 28.5 ± 5.3 minutes; mean difference − 5.3 minutes, 95% CI: − 7.1 to − 3.5; P< 0.001). PACU stay duration was also reduced (60.2 ± 7.3 minutes vs. 65.8 ± 6.9 minutes; P< 0.001). Furthermore, patients receiving esketamine reported lower postoperative pain scores and required less opioid consumption, with no significant increase in adverse effects.
Conclusion: Adjunctive low-dose esketamine during propofol-based total intravenous anesthesia significantly shortens extubation time and PACU stay, reduces intraoperative opioid consumption, and no significant increase in adverse effects was observed in this cohort. The reduction in postoperative pain scores did not remain significant after Bonferroni correction and requires further confirmation.
Keywords: esketamine, propofol, extubation time, laparoscopic surgery, quality of recovery
Introduction
The Enhanced Recovery After Surgery (ERAS) protocol advocates for a series of evidence-based perioperative interventions aimed at mitigating the surgical stress response, reducing complication rates, and accelerating patient recovery.1 Within this paradigm, achieving an early, smooth, and high-quality emergence from general anesthesia is paramount, with extubation time serving as a key objective indicator of this process. Although the minimal clinically important difference (MCID) for extubation time has not been formally established, even modest reductions—on the order of 4–5 minutes—are generally regarded as clinically meaningful, because they can facilitate earlier PACU discharge, improve patient throughput, and support ERAS goals.
Esketamine, the dextrorotatory enantiomer of ketamine, is a high-affinity N-methyl-D-aspartate (NMDA) receptor antagonist whose perioperative value extends beyond analgesia. Recently, its potential to enhance the quality of anesthesia recovery has garnered significant attention.2 However, the clinical evidence regarding its effect on postoperative extubation time remains inconsistent. For instance, some studies have reported that esketamine prolonged emergence and extubation times in patients undergoing laparoscopic gynecological surgery and modified radical mastectomy.3,4 Conversely, other investigations have demonstrated a significant reduction in extubation time in patients receiving esketamine for thoracoscopic lung cancer surgery,5 and total hip or knee arthroplasty.6 In contrast, a study on opioid-sparing anesthesia with esketamine found no difference in extubation time compared to traditional anesthesia in gynecological day surgery.7
These discrepant findings may be attributed to several factors, including surgical type, anesthetic regimen, and the dose and timing of esketamine administration. A recent comprehensive meta-analysis of 18 randomized controlled trials further confirmed that perioperative esketamine or ketamine improves early subjective quality of recovery and reduces pain severity, but the specific effect on extubation time remains inconsistent across the included studies.2 Notably, recent basic research has elucidated a potential neural mechanism: low-dose esketamine accelerates emergence from isoflurane anesthesia by activating glutamatergic neurons in the paraventricular thalamus (PVT).8 This finding provides a biological basis for the hypothesized “arousal-promoting” effect of esketamine. Despite this, high-quality research investigating the impact of esketamine on the emergence process within the more commonly used clinical model of propofol-based total intravenous anesthesia (TIVA) remains scarce.
We hypothesized that adjunctive low-dose esketamine would significantly shorten postoperative extubation time compared to placebo in patients undergoing laparoscopic gynecological surgery under propofol-based TIVA.
Materials and Methods
Study Design
This prospective, randomized, double-blind, placebo-controlled clinical trial was conducted at Xuzhou Central Hospital, China, between October 2023 and March 2025. The study protocol was approved by the Ethics Committee of Xuzhou Central Hospital (Approval No. XZXY-LK-20230406-047), and written informed consent was obtained from all participants prior to enrollment. This study was conducted in accordance with the Declaration of Helsinki. The trial was registered at Chinese Clinical Trial Registry (ChiCTR2300074484) and adhered to the Consolidated Standards of Reporting Trials (CONSORT) guidelines.
Participants
Inclusion Criteria
Patients were eligible if they were aged 18–75 years, had an American Society of Anesthesiologists (ASA) physical status of I–III and a body mass index (BMI) of 18–28 kg/m2, and were scheduled for elective total laparoscopic hysterectomy under general anesthesia. Additional requirements included being mentally sound without communication difficulties and providing voluntary written informed consent. The upper BMI limit of 28 kg/m2 was chosen because laparoscopic hysterectomy in patients with higher BMI is associated with increased surgical complexity and a higher risk of conversion to laparotomy, which could introduce variability in recovery independent of the study intervention.
Exclusion Criteria
ASA physical status IV or higher; uncontrolled hypertension, pulmonary hypertension, elevated intracranial or intraocular pressure; severe arrhythmia; untreated or inadequately treated hyperthyroidism; a history of psychiatric disorders, chronic pain, or central nervous system diseases; and a history of alcohol addiction. Patients who experienced a change in surgical procedure, required an alteration in anesthesia, developed unexpected severe complications, or required postoperative admission to the intensive care unit (ICU) were also excluded from the final analysis.
Randomization and Blinding
Eligible patients were randomly assigned in a 1:1 ratio to either the Esketamine group (Group K) or the Control group (Group C) using a computer-generated randomization sequence (SPSS software, version 26.0, IBM Corp.) prepared by an independent statistician who was not involved in patient enrollment or outcome assessment. Group allocations were concealed in sequentially numbered, opaque, sealed envelopes (SNOSE). No formal statistical test of concealment integrity was performed; however, no protocol violations or accidental unblinding events occurred during the study period.
To maintain blinding, the study medications were prepared in identical syringes and labeled according to the randomization code by a researcher not involved in patient management or data collection. The attending anesthesiologist administered the study drug according to the label without knowing the actual group allocation. Patients, anesthesiologists, investigators responsible for perioperative data collection, postoperative follow-up, and outcome assessment, as well as the statisticians, were all blinded to group assignments throughout the study.
Anesthesia and Monitoring
All patients adhered to standard preoperative fasting. Upon arrival in the operating room, standard monitoring was initiated, including five-lead electrocardiogram (ECG), pulse oximetry (SpO2), non-invasive blood pressure (NIBP), bispectral index (BIS), and core temperature. Peripheral intravenous access and a radial arterial catheter (inserted under local anesthesia) were established for fluid administration and invasive arterial pressure monitoring, respectively. To minimize procedural variability, all laparoscopic hysterectomies were performed by one of two attending gynecologists using a standardized four-port laparoscopic approach with a uniform uterine manipulator and electrosurgical devices.
Anesthesia Induction and Maintenance
Anesthesia was induced with intravenous propofol (2–3 mg/kg), sufentanil (0.3–0.5 µg/kg), and cisatracurium (0.15–0.2 mg/kg). Concurrently, patients in the Esketamine Group received a bolus of esketamine 0.2 mg/kg, while those in the Control Group received an equivalent volume of normal saline.
Following induction and confirmation of adequate muscle relaxation (≥3 minutes of mask ventilation), tracheal intubation was performed. Mechanical ventilation was instituted with a lung-protective strategy: tidal volume 6–8 mL/kg of predicted body weight, respiratory rate 12–14 breaths/min, fraction of inspired oxygen (FiO2) 0.5, positive end-expiratory pressure (PEEP) 5 cmH2O, and end-tidal carbon dioxide (EtCO2) maintained at 35–45 mmHg.
Anesthesia was maintained with continuous infusions of propofol (4–12 mg/kg/h, titrated to a BIS of 40–60) and remifentanil (0.1–0.5 µg/kg/min). The study drug (esketamine 0.125 mg/kg/h or matching placebo saline) was also infused continuously. Intermittent boluses of cisatracurium (0.03 mg/kg) were administered as needed for muscle relaxation. All anesthetic and study drug infusions were discontinued simultaneously upon skin closure, with the exception that the study drug infusion was terminated 10 minutes prior to the anticipated end of surgery, as a pragmatic measure to reduce the potential for residual drug effects during emergence.
Intraoperative Management and Adverse Event Control
Hemodynamics were maintained within 30% of baseline values. Hypertension (>30% above baseline) was treated with deepening anesthesia via additional propofol or remifentanil. Hypotension (>30% below baseline) was corrected with intravenous norepinephrine. For postoperative nausea and vomiting (PONV) prophylaxis, all patients received intravenous tropisetron 2 mg at the end of surgery.
Thermal Management
Patient normothermia was maintained using forced-air warming blankets, fluid warmers (set to 37°C), and by keeping the ambient operating room temperature at a minimum of 21°C.
Transversus Abdominis Plane Block
Following surgery completion and prior to tracheal extubation, all patients received a bilateral ultrasound-guided transversus abdominis plane (TAP) block administered by an experienced anesthesiologist. A total of 30 mL of 0.25% ropivacaine (15 mL per side) was injected to provide early postoperative analgesia for the abdominal wall.
Extubation Criteria
Tracheal extubation was performed in the PACU when patients met all of the following objective criteria: (1) adequate spontaneous ventilation with tidal volume >6 mL/kg of predicted body weight and respiratory rate between 12 and 25 breaths/min; (2) end-tidal CO2 consistently <45 mmHg; (3) hemodynamic stability, defined as heart rate and mean arterial pressure within 20% of preoperative baseline values for at least 5 minutes without vasoactive support; and (4) ability to follow simple verbal commands (eye opening, hand grip, sustained head lift for 5 seconds). Extubation was performed by the attending anesthesiologist, who was blinded to group assignment.
Postoperative Pain Management
Upon arrival in the Post-Anesthesia Care Unit (PACU), all patients were connected to a patient-controlled intravenous analgesia (PCIA) pump. The PCIA regimen for both groups was identical, consisting of sufentanil (0.03 µg/kg/h) diluted to a total volume of 100 mL, with a continuous background infusion of 2 mL/h for 48 hours, a bolus dose of 1 mL, and a lockout interval of 15 minutes.
Rescue analgesia with intravenous flurbiprofen axetil 50 mg was administered for a Numerical Rating Scale (NRS, 0–10) pain score of ≥4. The PCIA infusion was temporarily suspended in cases of respiratory depression, confusion, or hemodynamic instability, regardless of the NRS score, and was resumed after clinical resolution of these symptoms.
Outcome Measures
Primary Outcome
The primary outcome was the time from the simultaneous discontinuation of all anesthetic and study drug infusions to successful tracheal extubation in the PACU.
Secondary Outcomes
(1) PACU stay duration; (2) Intraoperative hemodynamic fluctuations (blood pressure, heart rate); (3) NRS pain score and Ramsay sedation score at 30 minutes after extubation in the PACU; (4) Total intraoperative consumption of propofol and opioids (converted to morphine milligram equivalents, MME); (5) Incidence of adverse reactions (eg., dizziness, somnolence, nausea, vomiting) and neuropsychiatric adverse events (eg., hallucinations, delirium) within 72 hours postoperatively.
Sample Size Calculation
The sample size was calculated based on the primary outcome of postoperative extubation time. Data from our pilot study (n=30, 15 per group, conducted in September 2023; these participants were not included in the main trial) indicated a mean extubation time of 26.5 ± 9.4 minutes in the control group and 22.5 ± 7.2 minutes in the esketamine group. To detect this difference with a two-sided α of 0.05 and a statistical power (1-β) of 90%, a minimum of 69 patients per group was required. Anticipating a potential dropout rate of 10%, we planned to enroll 77 patients per group, for a total sample size of 154. The calculation was performed using PASS 15.0 software (NCSS, LLC, Kaysville, UT, USA).
Statistical Analysis
The primary analysis was conducted according to a modified intention-to-treat (mITT) principle, defined as including all randomized patients who received the allocated study drug, underwent the planned surgical procedure, and had the primary outcome assessed. All 141 patients in the mITT population had complete primary endpoint data; therefore, no imputation method was required. Thirteen patients (7 in the esketamine group, 6 in the control group) were excluded post-randomization due to loss to follow-up or changes in surgical plan.
All statistical analyses were performed using SPSS software (version 26.0, IBM Corp.) and GraphPad Prism (version 9.0, GraphPad Software). The normality of data distribution was assessed using the Shapiro–Wilk test. Continuous data are presented as mean ± standard deviation (SD) for normally distributed variables and as median (interquartile range, IQR) for non-normally distributed variables. Between-group comparisons for normally distributed continuous data were conducted using the independent samples t-test; non-normally distributed variables were analyzed using the Mann–Whitney U-test. Categorical data are expressed as numbers (percentages) and were compared using the Chi-squared (χ2) test or Fisher’s exact test, as dictated by cell count assumptions. Cohen’s d effect sizes with 95% confidence intervals were calculated for the primary outcome and key secondary outcomes.
The primary outcome, extubation time, was compared between groups using the independent samples t-test. A two-sided P-value < 0.05 was considered statistically significant for the primary outcome. To control for the increased risk of Type I error, the Bonferroni correction was applied to the analysis of all secondary outcomes, with the adjusted significance threshold set at P < 0.005 (0.05 divided by 10 secondary comparisons).
Results
A total of 207 patients were assessed for eligibility during the study period. Of these, 53 were excluded: 25 declined to participate and 28 did not meet the inclusion criteria for the following reasons: BMI >28 kg/m2 (n=12), ASA physical status IV (n=5), history of chronic pain or psychiatric disorders (n=7), and inability to provide informed consent (n=4). The remaining 154 patients were randomized, with 77 allocated to the Esketamine group (Group K) and 77 to the Control group (Group C). During the trial, 13 patients were lost to follow-up or excluded from the final analysis (7 in Group K: 4 lost to follow-up, 3 due to changes in surgical plan; 6 in Group C: 4 lost to follow-up, 2 due to changes in surgical plan). Consequently, 141 patients completed the study and were included in the final analysis (70 in Group K, 71 in Group C). The flow of participants through the screening, randomization, and follow-up phases is detailed in the CONSORT diagram (Figure 1).
 |
Figure 1 Flow of participants through the study. |
The baseline demographic and clinical characteristics of the two groups were comparable (Table 1). No statistically significant differences were observed between the groups with respect to age, ASA physical status, height, weight, BMI, intraoperative fluid intake, urine output, preoperative laboratory values, or surgery duration (all P > 0.05). As the study focused on gynecological surgery, all participants were female.
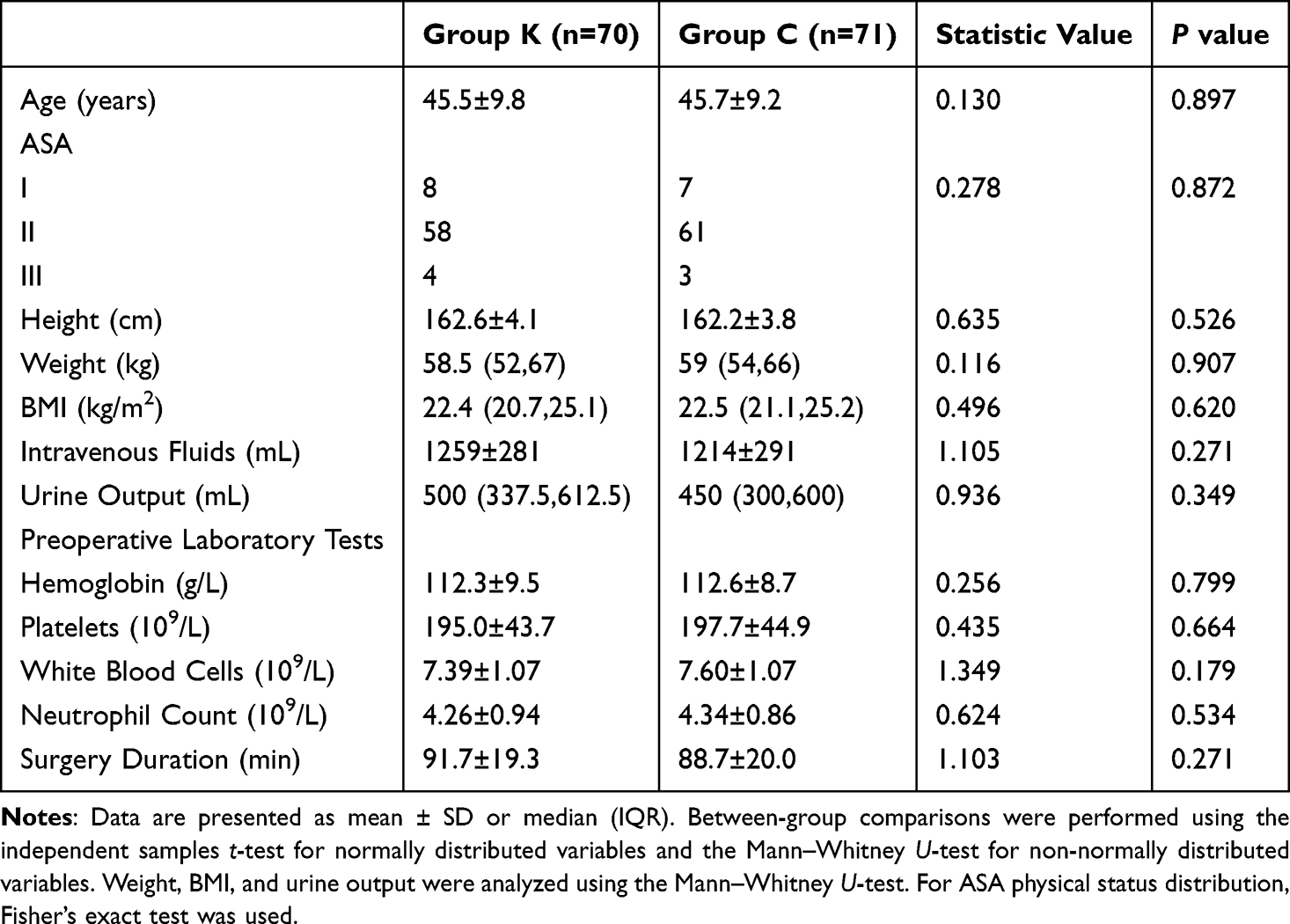 |
Table 1 Baseline Characteristics |
Primary Outcome
Patients in the esketamine group achieved a significantly shorter extubation time compared to the control group (23.2 ± 5.2 min vs. 28.5 ± 5.3 min; mean difference −5.3 min, 95% CI −7.1 to −3.5; Cohen’s d = 1.01, 95% CI 0.76–1.25; P<0.001), representing a relative reduction of 18.7% (Figure 2A).
 |
Figure 2 Primary and secondary outcomes related to recovery time. (A) Time to extubation (minutes). (B) Duration of stay in the Post-Anesthesia Care Unit (PACU, minutes). Data are presented as violin plots with mean ± SD. ***P < 0.001 versus Control group. Cohen’s d = 1.01 (95% CI 0.76–1.25) for extubation time; Cohen’s d = 0.79 (95% CI 0.55–1.03) for PACU stay duration. |
Secondary Outcomes
PACU Stay Duration
The duration of stay in the Post-Anesthesia Care Unit (PACU) was significantly shorter for Group K than for Group C (60.2 ± 7.3 min vs. 65.8 ± 6.9 min; mean difference −5.6 min, 95% CI −8.0 to −3.2; Cohen’s d = 0.79, 95% CI 0.55–1.03; P<0.001), corresponding to a relative reduction of 8.6% (Figure 2B).
Postoperative Pain and Sedation
At 30 minutes post-extubation, the median NRS pain score was significantly lower in Group K compared to Group C (3 [IQR: 2–3] vs. 3 [IQR: 3–4]; P=0.020). However, after applying the Bonferroni correction for multiple secondary outcome comparisons (adjusted α = 0.005), this difference did not reach the adjusted significance threshold. We therefore present this finding as exploratory and requiring independent confirmation. In contrast, Ramsay sedation scores did not differ significantly between the groups (P=0.101) (Figure 3A and B).
 |
Figure 3 Postoperative pain and sedation scores at 30 minutes in the PACU. (A) Pain scores assessed by the Numerical Rating Scale (NRS). (B) Ramsay Sedation Scale Scores. Data are presented as median (IQR). The between-group difference in NRS pain scores (P = 0.020) did not remain significant after Bonferroni correction for multiple secondary outcome comparisons (adjusted α = 0.005). |
Intraoperative Drug Consumption
Analysis of intraoperative drug consumption revealed a significant opioid-sparing effect of esketamine. The total opioid consumption, converted to morphine milligram equivalents (MME), was lower in Group K than in Group C (466.56 ± 113.01 MME vs. 516.21 ± 111.40 MME; P=0.002). However, there was no significant difference in total propofol consumption between the two groups (553.06 ± 122.59 mg vs. 536.16 ± 118.41 mg; P=0.326) (Figure 4A and B).
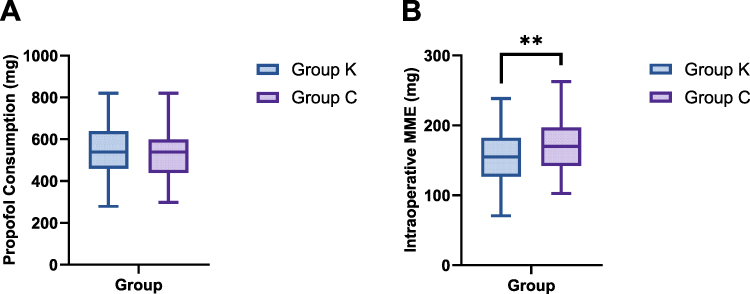 |
Figure 4 Intraoperative consumption of propofol and total opioids. (A) Propofol (mg). (B) Total opioid consumption, presented as morphine milligram equivalents (MME).Data are presented as mean ± SD. **P < 0.01 versus Control group. |
Safety Evaluation
The incidence of adverse reactions within 72 hours postoperatively was comparable between the groups, including dizziness (12.9% vs. 8.5%; risk difference 4.4%, 95% CI –5.8% to 14.6%), somnolence (10.0% vs. 7.0%; risk difference 3.0%, 95% CI –6.4% to 12.3%), and nausea and vomiting (18.6% vs. 21.1%; risk difference –2.6%, 95% CI –15.5% to 10.4%; all P > 0.05). No neuropsychiatric adverse events, such as delirium, hallucinations, nystagmus, or pruritus, were reported in either group throughout the observation period (Table 2). However, given the sample size, the study was not adequately powered to detect uncommon adverse events, and these safety findings should be interpreted accordingly.
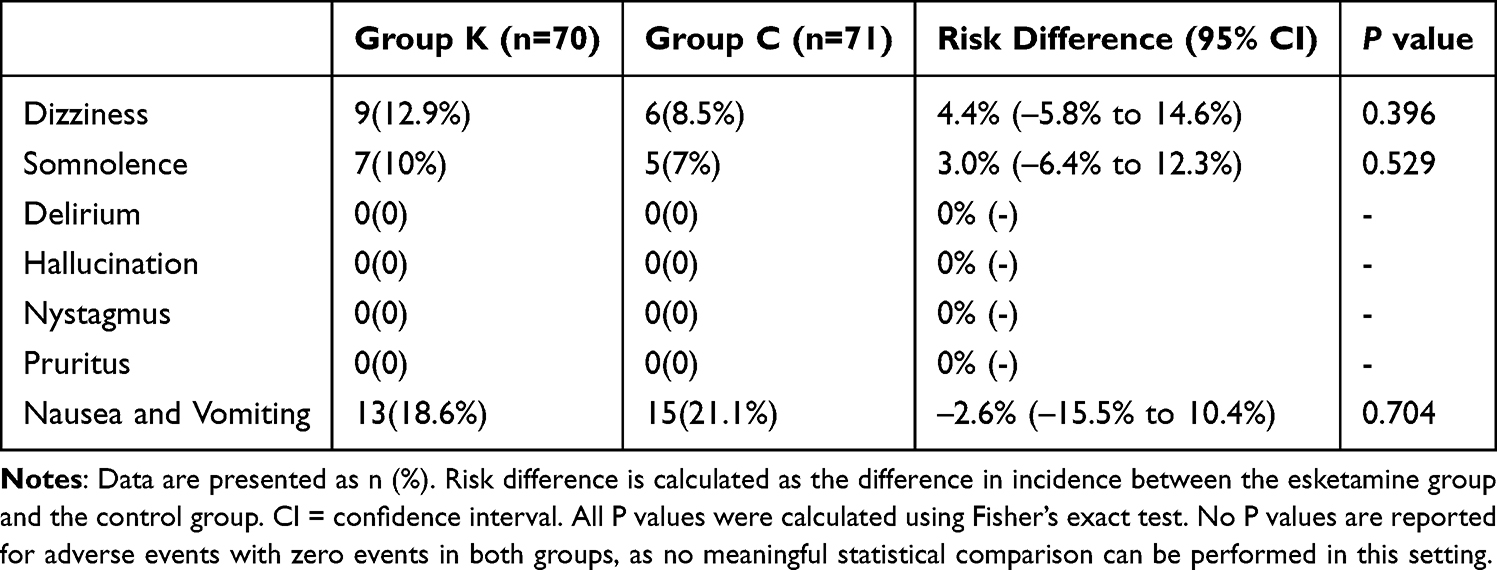 |
Table 2 Occurrence of Postoperative Adverse Reactions Within 72 Hours. n (%) |
Discussion
In this randomized, double-blind, placebo-controlled trial, we demonstrated that adjunctive, low-dose esketamine (0.2 mg/kg at induction + 0.125 mg/kg/h maintenance) during propofol-based total intravenous anesthesia significantly accelerated postoperative recovery in patients undergoing laparoscopic gynecological surgery. Specifically, it shortened extubation time by 18.7% and reduced PACU stay duration by 8.6%. These findings have important clinical implications, offering a reliable pharmacological strategy to optimize the emergence process, particularly for surgical patients under Enhanced Recovery After Surgery (ERAS) protocols who demand a rapid and smooth recovery. The 5.3-minute absolute reduction in extubation time, corresponding to an 18.7% relative decrease, may translate into meaningful improvements in PACU throughput and resource utilization in high-volume surgical settings. However, it should be noted that no validated minimal clinically important difference (MCID) has been established specifically for extubation time; whether this magnitude of reduction represents a clinically meaningful improvement at the individual patient level warrants further investigation.
The accelerated emergence observed in our study is likely mediated by multiple, synergistic mechanisms. The primary mechanism appears to be the significant opioid-sparing effect of esketamine, a direct consequence of its potent N-methyl-D-aspartate (NMDA) receptor antagonism. This is unequivocally supported by the marked reduction in intraoperative remifentanil consumption and total morphine milligram equivalents (MME) in the esketamine group. The consequent decrease in opioid usage mitigates their dose-dependent respiratory depressant effects. Furthermore, as Jonkman et al9 have shown, esketamine may directly enhance ventilatory sensitivity to CO2, creating a synergistic effect with its opioid-sparing property to actively counteract opioid-induced respiratory depression.10
Beyond these well-established peripheral benefits on respiratory function, a potential central pro-arousal mechanism may also contribute to the hastened recovery of consciousness. Recent fundamental research indicates that low-dose esketamine accelerates emergence from isoflurane anesthesia in mice by activating glutamatergic neurons in the paraventricular thalamus (PVT).8 Although it has been shown that propofol also suppresses PVT neuronal activity,11 it is important to emphasize that the PVT-mediated arousal mechanism has only been directly demonstrated under inhalational anesthesia in rodents and has not been validated under propofol-based TIVA in humans. Whether esketamine partially antagonizes propofol-induced PVT suppression in the clinical setting remains a biologically plausible but unverified hypothesis. Our study lacked the neurophysiological monitoring required to directly test this pathway; dedicated studies incorporating electroencephalographic or other neuromonitoring modalities will be needed to clarify the central mechanisms involved.
Regarding postoperative recovery quality, esketamine demonstrated a unique advantage in balancing analgesia and sedation. Its NMDA receptor antagonism effectively inhibits central sensitization in the spinal cord dorsal horn, which likely explains the significantly lower postoperative NRS pain scores in the esketamine group.12 Concurrently, esketamine’s modulatory effects on prefrontal cortex neurotransmitter systems,13,14 may help maintain emotional stability, enabling patients to achieve a smooth emergence without excessive sedation, as reflected by the comparable Ramsay sedation scores between the groups.
It should be noted that all patients in this study received bilateral ultrasound-guided TAP block with ropivacaine, which provided standardized and effective postoperative analgesia for the abdominal wall. While this approach minimized confounding from variable postoperative analgesic regimens, it may also have attenuated the observable differences in pain scores and opioid consumption between groups, potentially underestimating the analgesic benefit of esketamine.
The generalizability of our findings to other populations should be considered carefully. This study enrolled exclusively female patients undergoing a specific laparoscopic procedure; whether similar benefits would be observed in male patients, elderly individuals, or those with significant organ dysfunction remains uncertain. Furthermore, although the reductions in extubation time, PACU stay, and opioid consumption observed here are encouraging, formal cost-effectiveness analyses would be valuable to determine whether these improvements translate into net economic benefit for healthcare systems.
Safety Considerations and Sex Differences
This study paid particular attention to the safety profile of esketamine in a specific population. Despite its known psychoactive potential, no neuropsychiatric adverse events, such as delirium or hallucinations, were observed within 72 hours postoperatively under our protocol (low dose, discontinuation 10 minutes before surgery end, all-female cohort). The incidence of other common adverse reactions was comparable to the control group, suggesting that this dosing regimen has a manageable safety profile. It is worth emphasizing that sex is a critical factor influencing the pharmacokinetics of esketamine. Studies indicate that females generally have higher hepatic CYP3A4 activity than males, potentially leading to a faster clearance rate of esketamine.15,16 This pharmacokinetic difference may have contributed to the favorable balance between efficacy and safety observed in our all-female cohort. However, whether this dose regimen would achieve a similarly optimal profile in male patients is unknown; extrapolation to male patients should therefore be approached with caution and requires prospective investigation to rule out potential drug accumulation and associated risks.
Limitations
This study has several limitations that warrant consideration. First, the absence of electroencephalogram (EEG) or advanced neurophysiological monitoring precludes direct investigation into the mechanisms underlying esketamine’s arousal-promoting effects. Second, our study population was exclusively female, which, while appropriate for gynecological surgery, limits the generalizability of our findings to male patients. Third, 13 of 154 randomized patients (8.4%) were excluded from the final analysis because of loss to follow-up or changes in surgical plan. Although the numbers were balanced between groups and the reasons were unrelated to the study intervention, this post-randomization exclusion could introduce attrition bias. We therefore used a modified intention-to-treat (mITT) approach rather than a strict ITT analysis; the estimates may differ slightly from those obtained if all randomized patients had been included. Additionally, as a single-center investigation, our findings require validation in larger, multi-center trials.
Conclusion
In patients undergoing laparoscopic gynecological surgery, the adjunctive use of low-dose esketamine with propofol-based total intravenous anesthesia significantly shortens extubation time and PACU stay and reduces intraoperative opioid consumption. The observed reduction in postoperative pain scores did not remain statistically significant after adjustment for multiple comparisons and should be interpreted as exploratory. No increase in adverse effects was observed in this cohort, though the study was not powered to detect uncommon events. This strategy may serve as a useful adjunct that may enhance perioperative care within ERAS protocols. Future studies should incorporate neurophysiological monitoring to elucidate central mechanisms and evaluate the generalizability of these findings in broader surgical and demographic populations.
Trial Registration
Chinese Clinical Trial Registry Identifier: ChiCTR2300074484.
Data Sharing Statement
The datasets used during the current study are available from the corresponding author (Liwei Wang) on reasonable request.
Author Contributions
Yu Qi, Ying Ren, and Wenjing Xu should be regarded as co-first authors. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by New Round of Xuzhou PengchengTalent Program- High-level Healthcare Talent Recruitment and Development Project (Project Number: XWRCHT20220017 and XWRCHT20210033), Jiangsu Province’s Key Discipline / Laboratory of Medicine (Project Number: JSDW202231).
Disclosure
All authors declare that they have no conflicts of interest.
References
1. Ljungqvist O, Scott M, Fearon KC. Enhanced recovery after surgery: a review. JAMA Surg. 2017;152(3):292–11. doi:10.1001/jamasurg.2016.4952
2. Hung K-C, Kao C-L, Ho C-N, et al. The impact of perioperative ketamine or esketamine on the subjective quality of recovery after surgery: a meta-analysis of randomised controlled trials. Br J Anaesth. 2024;132(6):1293–1303. doi:10.1016/j.bja.2024.03.012
3. Chen L, He W, Liu X, Lv F, Li Y. Application of opioid-free general anesthesia for gynecological laparoscopic surgery under ERAS protocol: a non-inferiority randomized controlled trial. BMC Anesthesiol. 2023;23(1):34. doi:10.1186/s12871-023-01994-5
4. Huang Z, Liu N, Hu S, Ju X, Xu S, Wang S. Effect of dexmedetomidine and two different doses of esketamine combined infusion on the quality of recovery in patients undergoing modified radical mastectomy for breast cancer - a randomised controlled study. Drug Des Devel Ther. 2023;17:2613–2621. doi:10.2147/DDDT.S422896
5. Zhang C-L, Yan Y, Zhang Y, et al. Effects of esketamine combined with dexmedetomidine on postoperative delirium and quality of recovery in elderly patients undergoing thoracoscopic radical lung cancer surgery: a randomized controlled trial. CNS Spectr. 2024:1–10. doi:10.1017/S1092852924002177.
6. Ma C-B, Zhang C-Y, Gou C-L, et al. Effect of low-dose esketamine on postoperative delirium in elderly patients undergoing total hip or knee arthroplasty: a randomized controlled trial. Drug Des Devel Ther. 2024;18:5409–5421. doi:10.2147/DDDT.S477342
7. Zhu T, Zhao X, Sun M, et al. Opioid-reduced anesthesia based on esketamine in gynecological day surgery: a randomized double-blind controlled study. BMC Anesthesiol. 2022;22(1):354. doi:10.1186/s12871-022-01889-x
8. Duan W-Y, Peng K, Qin H-M, et al. Esketamine accelerates emergence from isoflurane general anaesthesia by activating the paraventricular thalamus glutamatergic neurones in mice. Br J Anaesth. 2024;132(2):334–342. doi:10.1016/j.bja.2023.10.038
9. Jonkman K, van Rijnsoever E, Olofsen E, et al. Esketamine counters opioid-induced respiratory depression. Br J Anaesth. 2018;120(5):1117–1127. doi:10.1016/j.bja.2018.02.021
10. Imam MZ, Kuo A, Smith MT. Countering opioid-induced respiratory depression by non-opioids that are respiratory stimulants. F1000Res. 2020;9:F1000. doi:10.12688/f1000research.21738.1
11. Liu P-F, Wang Y, Zhang R, Xu L, Li J-B, Mu D. Propofol modulates inhibitory inputs in paraventricular thalamic nucleus of mice. Neurosci Lett. 2021;756:135950. doi:10.1016/j.neulet.2021.135950
12. Duan C, Zhu Y, Zhang Z, et al. Esketamine inhibits the c-Jun N-terminal kinase pathway in the spinal dorsal horn to relieve bone cancer pain in rats. Mol Pain. 2024;20:17448069241239231. doi:10.1177/17448069241239231
13. Wang Y, Zhang Y, Wang K, et al. Esketamine increases neurotransmitter releases but simplifies neurotransmitter networks in mouse prefrontal cortex. J Neurophysiol. 2022;127(2):586–595. doi:10.1152/jn.00462.2021
14. Rizzo A, Garçon-Poca MZ, Essmann A, et al. The dopaminergic effects of esketamine are mediated by a dual mechanism involving glutamate and opioid receptors. Mol Psychiatry. 2025;30:3443–3454. doi:10.1038/s41380-025-02931-3
15. Saland SK, Kabbaj M. Sex Differences in the Pharmacokinetics of Low-dose Ketamine in Plasma and Brain of Male and Female Rats. J Pharmacol Exp Ther. 2018;367(3):393–404. doi:10.1124/jpet.118.251652
16. Waxman DJ, Holloway MG. Sex differences in the expression of hepatic drug metabolizing enzymes. Mol Pharmacol. 2009;76(2):215–228. doi:10.1124/mol.109.056705
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Low-Dose Esketamine as an Adjuvant to Propofol Sedation for Same-Visit Bidirectional Endoscopy: Protocol for a Multicenter Randomized Controlled Trial
Song N, Shan XS, Yang Y, Zheng Z, Shi WC, Yang XY, Li Y, Tan AP, Liu H, Peng K, Ji FH
International Journal of General Medicine 2022, 15:4733-4740
Published Date: 6 May 2022
Effect of Dexmedetomidine and Two Different Doses of Esketamine Combined Infusion on the Quality of Recovery in Patients Undergoing Modified Radical Mastectomy for Breast Cancer - A Randomised Controlled Study
Huang Z, Liu N, Hu S, Ju X, Xu S, Wang S
Drug Design, Development and Therapy 2023, 17:2613-2621
Published Date: 28 August 2023
Comparative Study About Different Doses of Remimazolam in Short Laparoscopic Surgery: A Randomized Controlled Double-Blind Trial
Luo L, Jiang J, Zhang M, Guo Z, Zhang X, Wang F, Yang F
Therapeutics and Clinical Risk Management 2023, 19:829-837
Published Date: 20 October 2023
Effect of Esketamine-Based Opioid-Sparing Anesthesia Protocol on the Quality of Early Recovery After Urological Surgery: A Randomized Clinical Trial
Qi Y, Li W, Ren Y, Sun J, Zhu Y, Wang L, Zhou M, Wang L
Drug Design, Development and Therapy 2025, 19:2005-2016
Published Date: 17 March 2025
Effect of Different Doses of Esketamine on Postoperative Recovery in Patients Undergoing Gynecologic Laparoscopic Surgery, a Randomized, Double-Blind, Single-Center Clinical Study
Li T, Han L, Wu Z, Chen Y, Wang Y
Drug Design, Development and Therapy 2025, 19:2833-2843
Published Date: 11 April 2025