Back to Journals » Psychology Research and Behavior Management » Volume 15
The Effects of Cognitive Training in Healthy Community Residing Thai Elderly: A Randomized Controlled Trial
Authors Phanasathit M ![]() , Nimnuan C, Lohsoonthorn V
, Nimnuan C, Lohsoonthorn V
Received 4 August 2022
Accepted for publication 7 December 2022
Published 20 December 2022 Volume 2022:15 Pages 3709—3720
DOI https://doi.org/10.2147/PRBM.S383526
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Muthita Phanasathit,1,2 Chaichana Nimnuan,3 Vitool Lohsoonthorn1
1Department of Preventive and Social Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 2Department of Psychiatry, Center of Excellence in Applied Epidemiology, Faculty of Medicine, Thammasat University, Pathum Thani, Thailand; 3Department of Psychiatry, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
Correspondence: Vitool Lohsoonthorn, Department of Preventive and Social Medicine, Faculty of Medicine, Chulalongkorn University, 1873 Ratchadamri Road, Pathum Wan, Bangkok, 10330, Thailand, Tel +66 2252 7864 ; +66 2256 4000 Ext. 3701, Email [email protected]
Purpose: Cognitive training intervention (CTI) is defined as any mechanism of action of a non-pharmacological procedure provided to improve cognitive function. CTI in healthy elderly has the potential to improve cognitive function; however, the effects of interactive computerized-CTI in old ages have been inconclusive. The present study aimed to determine the effects of low-technology CTI in community-based populations.
Patients and Methods: The study was a 2-arm parallel single-blinded randomized controlled intervention trial. The main outcome measured global cognitive function utilizing the Thai Mental State Examination (TMSE); the minor outcomes were cognitive subdomains and psychosocial outcomes (ie, quality of life and depression). The primary endpoint assessed the treatment effect at the 12th week (T1), while the secondary endpoint evaluated the carry-over effect at the 24th week (T2).
Results: Eighty-six eligible participants were recruited from a senior society on the edge of Bangkok. At baseline (T0), the mean age and TMSE score among CTI (n = 44) and wait-list (n = 42) groups were similar (age; 66.66 ± 5.52 and 67.52 ± 6.46; TMSE; 28.84 ± 1.38 and 28.83 ± 1.12, respectively). For the CTI group, the mean number of cognitive training sessions was 14.82 ± 7.62. By using intention-to-treat analysis at the primary endpoint, the mean difference score of TMSE in the CTI group was significantly higher than the wait-list group (∆TMSEbetween group at T1-T0 = 0.57; 95% CI = 0.07 to 1.08), while the effect size was 0.48. At the secondary endpoint, there was no significant difference observed between the CTI and wait-list groups (∆TMSEbetween group at T2-T0 = 0.33; 95% CI = − 0.23 to 0.88), while the effect size was 0.25. The cognitive subdomains and psychosocial outcomes were discovered with no significant difference.
Conclusion: CTI showed significant treatment effect for improvement in global cognitive function in healthy Thai elderly but did not demonstrate carry-over effect. This study provided preliminary evidence of the feasibility of implementing low-technology CTI in middle-income countries.
Keywords: cognitive functions, community, elderly, healthy, randomized controlled trial
Introduction
Dementia is a heterogeneous and multifactorial condition with some risk factors being non-modifiable, such as age, ethnicity, sex, and genetic factors.1–3 The potentially modifiable risk factors are grouped by age. In early life, these include a lower education; in midlife, they are linked to cardiovascular disease (ie, hypertension, and obesity) and hearing loss; and in later life, factors are associated with smoking, depression, physical inactivity, social isolation, and diabetes.4,5 Novel trials have focused on non-medical interventions to prevent dementia in healthy aged populations such as encouraging a Mediterranean-style diet,6 promoting exercise and physical activity,7 facilitating opportunities for social engagement,8 and cognitive training interventions (CTI).9–11 Moreover, it has been suggested that CTI in later life has benefits in terms of risk reduction of Alzheimer’s disease (AD)10 and that CTI could potentially increase brain cognitive reserve since cognitive reserve is not a static ability. However, Gates et al reported that the effects of interactive computerized-CTI in middle-ages (aged 45–65 years) and old-ages (≥65 years) were inconclusive and that more high-quality randomized controlled intervention trials (RCTs) were needed.12,13 Several recent systematic reviews and meta-analyses have shown some evidence that CTI in healthy elderly has the potential to improve cognitive function. These studies involved the repeated practice of a set of structured and standardized tasks designed to target one or more cognitive domain through teaching skills and strategies for improving functioning.14,15
CTI is defined as any mechanism of action of a non-pharmacological procedure provided to not only improve cognitive function (ie, attention, learning and memory, language, problem-solving skills, visuoconstructional-perceptual ability, and social cognition), but also enhance cognitively mediated domains of functioning, such as activities of daily living, and behavioral disturbance. The strategy of CTI is categorized into 2 types: compensatory and restorative. Firstly, compensatory interventions are prescribed to develop new methods to perform everyday tasks by working around cognitive impairment. These compensatory interventions employ procedural training to teach complex and higher-order cognitively mediated behaviors, as well as internal and external tactics. Internal tactics involve a kind of information organization activity, while external tactics use environmental cues and note-taking. The second CTI type involves restorative interventions aimed to recover premorbid cognitive function. These include spaced retrieval, attention and memory drills, vanishing cues, errorless learning, reality orientation therapy, and reminiscence therapy. Overall, restorative interventions for AD patients have been found to be more efficacious than compensatory interventions.16
It is well documented that Thailand has recently moved from an aging society to an aged society.17 The proportion of Thai dementia patients who accessed health care services in 2015 was 12.9 per 100,000 people, while AD accounted for the highest prevalence subtype of dementia, with 8.3 per 100,000.18 It is, therefore, paramount that practices to delay the progression of dementia are fully established in the Thai public health care system. Furthermore, due to the lack of familiarity with digital technologies among elderly Thai citizens and a lack of resources, the intervention required the use of simple devices, which are commonly available in low to middle-income countries. It appears the use of simple devices for CTI is novel in this study and aims to increase the feasibility of CTI studies in countries lacking access to advanced digital methods. Consequently, the hypothesis of the present study is that restorative strategic CTI involving low-technology devices could improve cognitive function and psychosocial outcomes (quality of life (QoL) and depression) in healthy Thai elderly in community-based populations.
Materials and Methods
Study Design
The study was a 2-arm parallel single-blinded intervention RCT. The objective was to prove the effects of the CTI when compared to the wait-list group. This trial was registered to the Thai Clinical Trials Registry (TCTR20151013001) and approved by the Institutional Review Board of the Faculty of Medicine, Chulalongkorn University (IRB No.514/58, Date of approval; January 5, 2016). All procedures were performed following the principles stated in the Declaration of Helsinki and informed consent was obtained from the study participants prior to study commencement.
Participants
Eligible participants, who were aged at least 55 years old, were recruited from a social club for the elderly in Nonthaburi Municipal, a suburb of Bangkok, Thailand. The exclusion criteria were 1) elderly who had attended formal education for less than six years; 2) elderly who had visual or hearing impairment which could not be corrected with eyeglasses or hearing aids; 3) elderly who had been diagnosed with dementia or mild cognitive impairment (MCI) (diagnosed by one of the authors, a geriatric psychiatrist, using the Clinical Dementia Rating Scale (CDR) ≥ 0.5);19,20 4) elderly who had been diagnosed with substance use disorders (except tobacco and caffeine); 5) elderly who had psychotic disorders, bipolar disorders or major depressive disorders classified by DSM-5;21 6) elderly who had been diagnosed with neurological diseases (such as stroke, epilepsy, and Parkinson’s disease); and 7) elderly who had been prescribed benzodiazepines, anticholinergics, acetylcholinesterase inhibitors, or N-methyl D-aspartate receptor antagonists.
Randomization
The recruitment process involved posting an advertisement on the elderly center noticeboard, and residents interested in participating contacted the research assistant by telephone. A research assistant enrolled all voluntary participants and concealed their identification data using sequential coding. Following on from this, the research assistant employed each sequential code to assigned participants to the intervention or wait-list arm by a block of four randomization. All administrative tasks and data entry were carried out by the research assistant who was not involved in the interventions and outcome assessment (Figure 1).
 |
Figure 1 Flow diagram of randomization. |
Interventions
The CTI referred to a non-pharmacological intervention that involved a kind of restorative strategy involving the completion of a series of structured tasks to improve cognitive performance in healthy elderly. The exercises targeted 6 cognitive functions (ie, complex attention, executive function, learning and memory, language, visuoconstruction-perceptual ability, and social cognition (see more details on Protocol and Data Sharing). All 6 of these cognitive functions were practiced in each CTI session (30 minutes per session), with each exercise targeting one cognitive domain. The CTI was implemented twice per week and included 24 sessions in 12 weeks overall. Each session comprises 8 sections of 3-minutes each, following the same format: 1) check-in and introduction; 2) cognitive domain practice (6 sections); and 3) summary and feedback section. There was a 1-minute break after each section had ended to enable participants to recover (Figure 2). The sessions took place in a group that was led by the author, who guided the participants through each activity systematically. The CTI was run by an audio-visual digital video disk created by the authors which explained instruction and demonstration in each lesson and involved an individual paper-pencil workbook. The CTI employed speed tests, matching activities, gap completion, and short-answer questions.
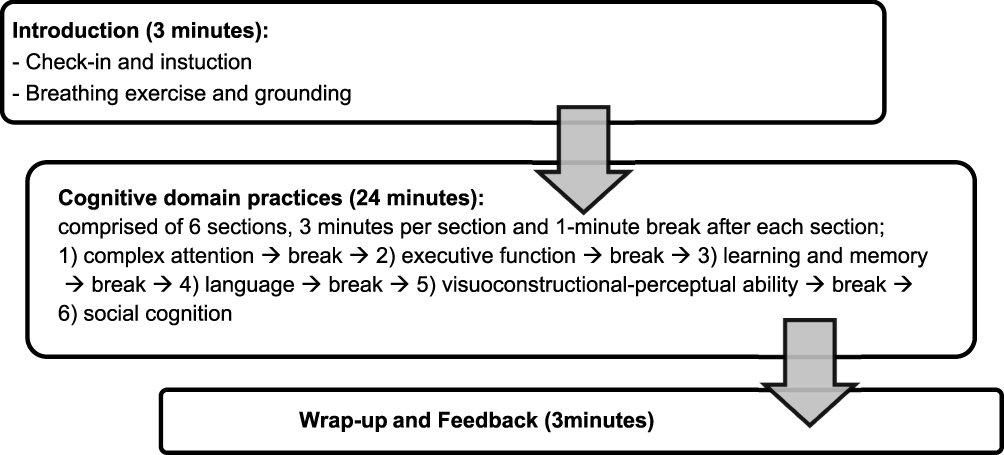 |
Figure 2 Cognitive training intervention (CTI) protocol. |
Participants allocated to the intervention arm received the CTI and engaged in usual recreational group activities during the first 12 weeks of the experimental phase. It is important to note that the usual recreational group activities were informal, voluntary, and part of the day-to-day activities at the elderly center. All CTI sessions were arranged as additional from the regular schedule and took place in a private room and all CTI materials were kept in a locked cabinet. Conversely, participants allocated to the wait-list arm received only the usual recreational group activities, including aerobic exercises, ballroom dance, Thai folk dance, fitness drills, yoga, Tai Chi, Karaoke, musical instrument lessons, Mandarin-Chinese or English lessons, and practice with dharma and meditation. There was no daily record of the type or class of the usual recreational activities each participant took part in because they were deemed non-compulsory. In addition, the researchers did not distinguish between static and physical recreational activities as it was regarded as cumbersome for the elderly participants to record each day. The wait-list group was contacted by the research assistant twice by phone to make appointments for primary and secondary outcome measures. After the experiment phase had ended both CTI and wait-list groups attended usual recreational group activities, following a regular schedule at the elderly center from the 13th week to the 23rd week (Figure 2).
Outcomes
The primary outcome measured global cognitive function by employing the Thai Mental State Examination (TMSE), a neuropsychiatric test for standard mental status examinations for Thai elderly. The total score of the TMSE is 30 points and the cut-off point for the diagnosis of normal (healthy) Thai elderly is over 23 points.22,23
Additionally, there were two secondary outcomes: a measurement of the 8 cognitive subdomains and an evaluation of psychosocial outcomes. The neuropsychological assessment battery was used to evaluate the 8 cognitive subdomains which have good psychometric properties of cognitive assessment in Thai older adults.24,25 This neuropsychological assessment battery consisted of the digit span forward for attention-concentration, the digit span backward for working memory, a word list learning test for verbal memory, a Trial Making-A Test for psychomotor speed, a Trail Making-B Test for executive function, a constructional praxis for visuoconstructional-perception, a word recall exercise for delayed recall memory, and the letter “S” and category fluency tests for language fluency (see more details on Protocol and Data Sharing). This study employed the brief Older People’s Quality of Life Questionnaire (OPQOL-brief)26 and the Thai Geriatric Depression Scale-15 (TGDS-15)27,28 as the tools used for psychosocial evaluation, with permission granted from the original authors.
The original OPQOL-brief was authorized for translation and validation in Thai. The eligible criteria of content validity employed the index of item-objective congruence (IOC),29 which was set at more than 0.80. The Thai version of OPQOL-brief (OPQOL-brief-Th) was adjusted again and back-translated by an English expert after face and content validity were approved by a psychiatrist, a neurologist, a physical physician, a clinical psychologist, and an occupational therapist. These final versions of the OPQOL-brief-Th had reliability measured through a pilot study conducted at the elderly club at Thammasat University Hospital. The internal consistency of the OPQOL-brief-Th was measured by Cronbach’s alpha coefficient, which was 0.93.30 The two-week test-retest reliability of OPQOL-brief-Th was represented by Spearman’s rank correlation coefficient (rs), yielding strong stability (rs=0.76, p<0.01). The TGDS-15 is the Thai version of the 15-item Geriatric Depression Scale used when screening for major depression and a cut-off score of ≥7 points was given high sensitivity (88%) and specificity (75%).28
All cognitive function outcomes were assessed by trained blinded psychologists not involved in the recruitment process and experimental phase. Furthermore, the TGDS-15 and OPQOL-brief-Th were recorded with self-reported questionnaires. All outcomes employed the same version of TMSE, neuropsychological assessment battery, TGSD-15, and OPQOL-brief-Th at 3-time points of measurement. These were 1 week before the implementation of the experimental phase (baseline, T0); 1 week after the ending of the experimental phase (12th week, T1); and at the end of the 24th week (T2). At the primary endpoint, the treatment effect was assessed by calculation of the mean difference scores of the TMSE, neuropsychological battery, TGDS-15, and OPQOL-brief-Th between the 12th week (T1) and baseline (T0) scores. At the secondary endpoint, the carry-over effect was evaluated by the mean difference scores between the 24th week (T2) and baseline (T0).
Sample Size
The sample size was estimated using a 1:1 ratio 2–sample parallel pre-post design of RCT with the continuous outcome of a 2-tailed test.31,32 The effect size was set at 1.0 (difference of the mean of TMSE between the treatment and control group),9 with a 2-tailed significance level of (α) 0.05; the power (β) was set at 0.80. According to this formula, the number of participants allocated to each arm should be 39. The authors estimated a 10% dropout during the study; therefore, the minimum sample size per arm was 44. During the enrollment process, 2 of the 88 participants were excluded due to a history of schizophrenia and cerebrovascular disease. The final 86 participants were randomly assigned to the CTI and wait-list group (Figure 1).
Statistical Methods
The Statistical Package for the Social Science (SPSS) version 17.033 was used to analyze descriptive statistics, such as frequency, percentage, mean, median, standard deviation (SD), and 95% confidence interval (95% CI). The statistical significance was set at a 2-tailed p-value <0.05, and a 2-tailed independent sample t-test was performed to investigate the difference between the mean change of (T1-T0) between intervention and control groups and the difference between the mean change of (T2-T0) between groups, which represented the treatment and carry-over effect of both primary and secondary outcomes, respectively. The effect size (d) was calculated using Glass’s Estimator of Effect Size.34 To compare all outcomes for all participants who were randomized to receive CTI or wait-list, an intention-to-treat (ITT) analysis was performed with the last observation carried forward technique. A per-protocol (PP) analysis was also performed for comparison among participants who completed the treatment originally planned.
Results
Population and Loss to Follow-Up
This trial enrolled 88 elderly participants from September to December 2016; however, two people were excluded due to schizophrenia and cerebrovascular disease. Eighty-six participants completed the baseline neurocognitive function and psychosocial outcomes assessment and were randomly allocated into two arms as shown in Figure 1 (44 to CTI group and 42 to wait-list group). From January to March 2017, the experimental group received CTI while the control group was allocated as the wait-list. The primary and secondary endpoints were assessed in April and June 2017, respectively. Consequently, 86 participants were eligible to receive ITT analysis, while only 67 participants remained on PP analysis. In the CTI group, there were 7 participants (15.09%) who did not receive the allocated intervention owing to surgery, inability to be contacted by phone, and a desire not to attend the cognitive training program; however, one participant still came to the primary and secondary endpoint assessments. In the wait-list group, there were 12 participants (30.00%) who declined to attend the endpoint assessment. Therefore, at the 24th week, the CTI group had 37 participants and the wait-list group had 30 participants.
The baseline demographic and clinical data are presented in Table 1. Most participants in each group were female and had approximately 14 years of education. The mean age in the CTI group was 66.66±5.52 years old, whereas in the wait-list group it was 67.52±6.46 years old. In terms of global cognitive function, the TMSE score among CTI and wait-list groups were similar (28.84±1.38 and 28.83±1.12, respectively). Overall, all participants had a good QoL without depression. For the CTI group, the mean number of visits to cognitive training sessions was 14.82±7.62. All cognitive subdomain scores at the baseline of both groups were similar (see Appendix Table 1 and 2A). Due to the baseline characteristics of CTI and wait-list group being similar, the outcomes were analyzed with unadjusted estimates. Moreover, the PP analysis was not substantially different from the ITT analysis and no protocol deviations or adverse events occurred.
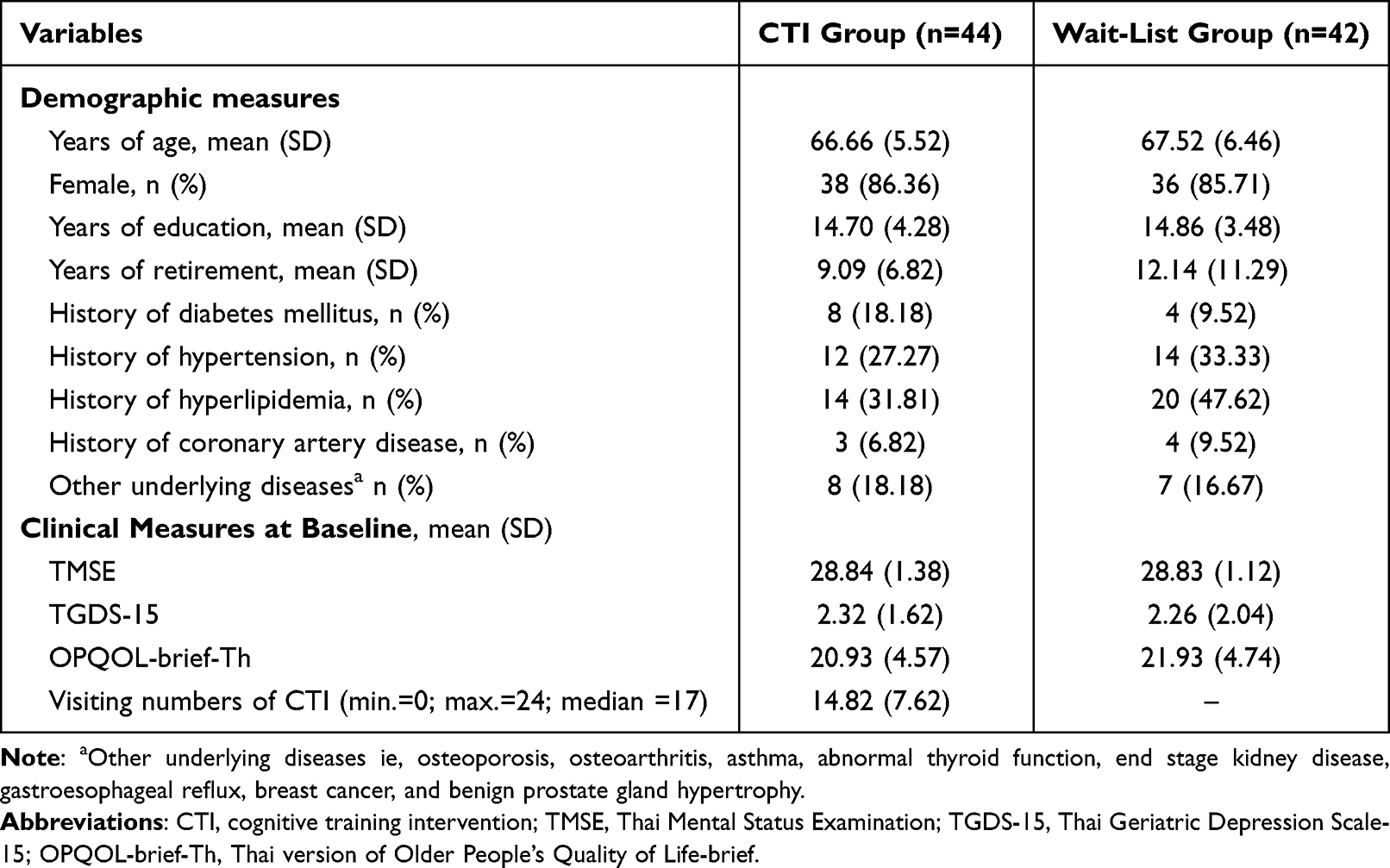 |
Table 1 Baseline Demographic and Clinical Measures of All Participants |
Primary Endpoint
At the primary endpoint, the mean difference in global cognitive function between the 12th week and baseline (∆TMSEwithin group at T1-T0) of the CTI group was 0.45 (95% CI = 0.06 to 0.85); with the wait-list group, it was −0.12 (95% CI = −0.44 to 0.20). A statistical difference was found using ITT analysis between CTI and wait-list groups (∆TMSEbetween group at T1-T0 = 0.57; 95% CI = 0.07 to 1.08), while the effect size was 0.48 (Figure 3). Moreover, the mean difference in the 8 cognition subdomains, TGDS-15, and OPQOL-brief-Th, did not show significant differences between both groups (Table 2).
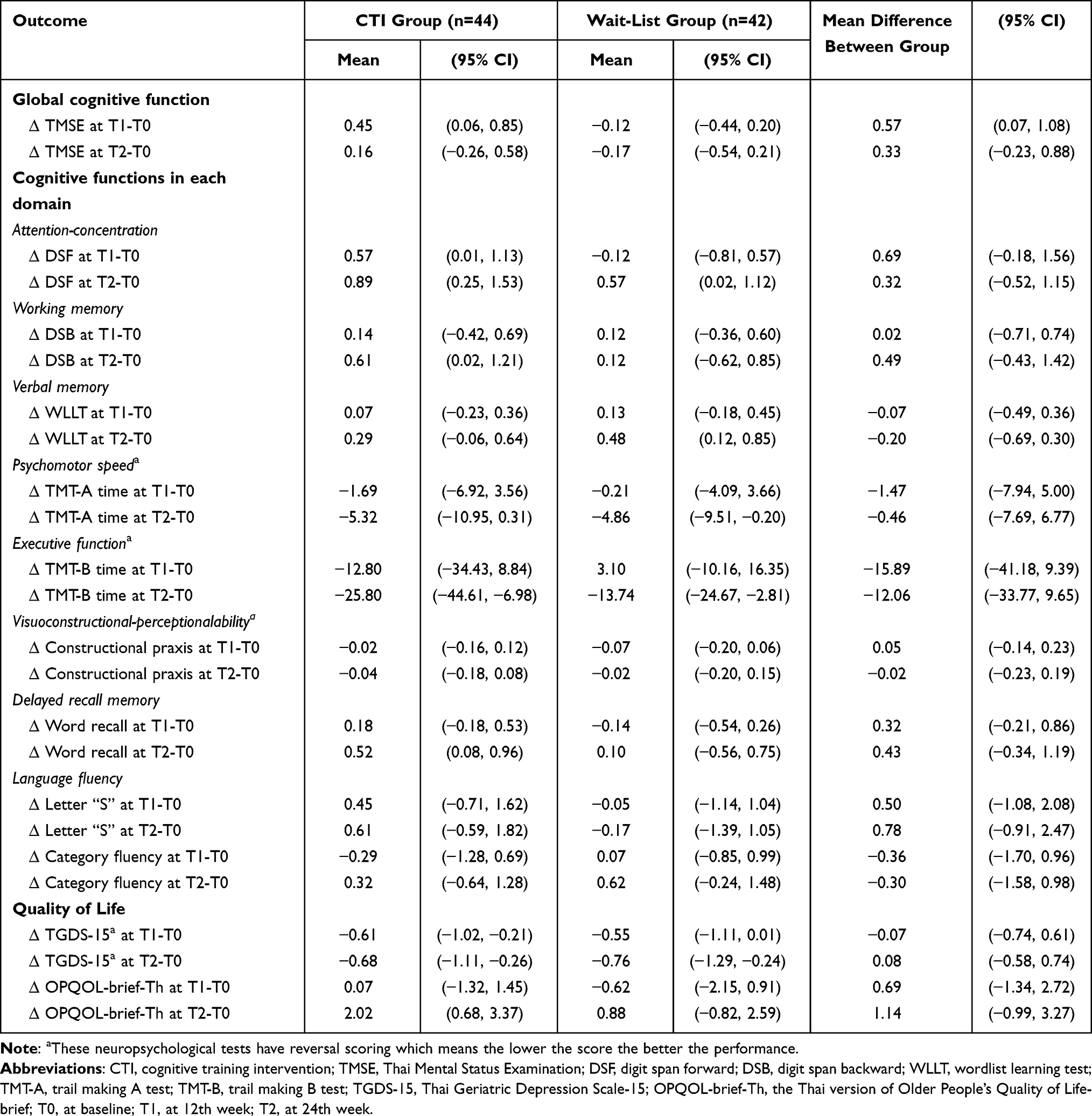 |
Table 2 Treatment Effect and Carryover Effect (Analyses for Intention-to-Treat Using the Last Observation Carried Forward Method) |
 |
Figure 3 Treatment effect and carryover effect. |
Secondary Endpoint
At the secondary endpoint, the mean difference in global cognitive function between the 24th week and baseline (∆TMSEwithin group at T2-T0) of the CTI group was 0.16 (95% CI = −0.26 to 0.58) and the wait-list group was −0.17 (95% CI = −0.54 to 0.21). A comparison between groups showed no significant difference between the CTI and wait-list groups using ITT analysis (∆TMSE between group at T2-T0 = 0.33; 95% CI = −0.23 to 0.88), while the effect size was 0.25 (Figure 3). Additionally, the mean difference in the 8 cognition subdomains, TGDS-15, and OPQOL-brief-Th did not show significant differences between both groups (Table 2).
Per-Protocol Analysis
At the primary endpoint, the mean difference in global cognitive function between the 12th week and baseline (∆TMSEwithin group at T1-T0) of the CTI group (n=37) was 0.49 (95% CI = 0.02 to 0.96) and for the wait-list group (n=30) it was −0.13 (95% CI = −0.58 to 0.31). In a comparison between the groups, the mean difference in global cognitive function in the CTI group was higher than in the wait-list group, but no statistical difference was discovered (∆TMSEbetween group at T1-T0 = 0.62; 95% CI = −0.03 to 1.26). Moreover, there was no significance found between the mean difference in the 8 cognition subdomains, TGDS-15, and OPQOL-Brief-Th across both groups (see Appendix Table 2B).
At the secondary endpoint, the mean difference in global cognitive function between the 24th week and baseline (∆TMSEwithin group at T2-T0) of the CTI group was 0.11 (95% CI = −0.32 to 0.54) and the wait-list group was −0.20 (95% CI = −0.72 to 0.32). In a comparison between groups, there were no significant differences discovered between the CTI and wait-list group (∆TMSE between group at T2-T0 = 0.34; 95% CI = −0.34 to 1.02). Additionally, no significance was found between the mean difference in the 8 cognition subdomains, TGDS-15, and OPQOL-Brief-Th across both groups (see Appendix Table 2B).
Discussion
The findings of this present study have shown that the CTI has had a statistically significant treatment effect on global cognitive function in healthy Thai elderly at the primary endpoint. However, there was no carry-over effect at the secondary endpoint observed. Moreover, in comparison with the control group, there was some evidence of increases in performance in the CTI group indicated in the raw scores, but these differences did not reach a level of statistical significance. This data included improvements in attention-concentration, working memory, verbal memory, psychomotor speed, executive function, visuoconstructional-perceptual ability, delayed recall memory, and letter “S” fluency at the primary and secondary endpoints. The control group in the present study consisted of wait-list participants who attended the usual recreational group activities as regularly scheduled activities at the elderly center. There was neither a single-domain nor multi-domain CTI combined with recreation activities and physical exercise.
These findings support the results from two recent systematic reviews and meta-analyses on CTI studies which demonstrated modest improvements in healthy older adults. In these studies, the standardized mean effects (g) ranged from 0.29 to 0.32 (95% CI = 0.24 to 0.34 and 95% CI = 0.13 to 0.64).14,15 Additionally, the effect size of global cognition in this present study was 0.48, which was similar to previous meta-analyses of CTI in healthy elderly.11,14,15,35,36 Mewborn et al reported that the single domain working memory intervention had the most effect (g = 0.47); however, memory (g = 0.14), processing speed (g = 0.14), and multi-domain (g = 0.31) CTI also displayed significant improvement. This review provided evidence that both RCTs, with an active control group and a passive control group, had significant cognitive function benefits.15 Further results support the idea that CTI may have a more positive effect than cognitive stimulation when the active control group received cognitive activities involved in puzzle completion, reading, and low-challenge computer games.14,15 More specifically, the treatment effect showed a larger impact than the carry-over effect. In addition, age, education, and cognitive status (ie, healthy or MCI) were not moderators of the CTI effect. According to Mewborn et al, the intervention protocol should be less than 30 minutes per session (g = 0.31), 1–2 times/week (g = 0.36), and the total number of sessions should be at least 20 sessions (g = 0.33) to have a larger treatment effect. Furthermore, CTI delivered to individuals showed more impact than when administrated to a group (g = 0.40 and g = 0.24, respectively).15 Consistent with the previous review, the CTI in the present study was congruent by implementing 24 sessions twice a week with 30 minutes of group-based multi-domain training.
The effect size of CTI in this study, which implemented a simple device with low digitalized techniques, demonstrated a moderate effect size similar to that discovered in studies that looked at video game-assisted cognitive training among the elderly. The findings in the present study provide substantial evidence of the benefits of CTI when compared to the use of video games, which only made modest improvements in the executive function of healthy elderly.11,37 For example, Toril et al re-analyzed the mean effect size of 20 individual video game training studies from 1986 to 2013 and discovered a result of 0.37.37 Previous reviews11,37 have concluded that training the elderly with non-action video games improved processing speed, attention, memory, and global cognition; however, these improvements became non-significant after 3-months. Two recent systematic reviews, by Gates et al reported that the effects of interactive computerized-CTI in middle-aged and old-aged individuals on global and subdomain cognitive functions were inconclusive.12,13 Based on the above findings, the present study decided to facilitate the application of CTI by using an audio-visual digital video disk to explain instruction and provide a demonstration in each lesson, alongside an individual paper-pencil workbook. The CTI in the present study was designed to be user-friendly to the Thai older adult population and practical for the large number of digital immigrants that exist in Thai society needing assistance in operating technology.
Despite discovering that the CTI had benefits for cognition in healthy elderly in the short term, this present study found that the CTI did not have any carry-over effect. Valenzuela and Sachdev proposed that there was a dose–response relationship between increases in complex mental activities in later life and the risk of dementia.35 The intensity of the CTI in this present study might be at the minimum frequency and duration that could have a significant impact on cognitive function in healthy elderly. There is evidence from previous studies that significant improvements in cognitive function after training in processing speed, attention, and memory became extinct after a 3-month follow-up.35 Recommendations have been made suggesting that to maintain the benefits of training some boosting sessions would be required.35 This present study measured the effects of a single CTI without any structured physical training and found that the effect size was moderate. To compare the effects of single versus combined CTI and physical training with healthy elderly, Oswald et al discovered that a combination of cognitive and physical training had a more significant effect than single CTI (0.75 and 0.35, respectively). Furthermore, the effect size of the cognitive outcome at the 1-year post-treatment mark demonstrated the same pattern (1.14 and 0.95, respectively).38 The reason why the combination of cognitive and physical training had superior effects than single CTI was explained by Li et al using functional magnetic resonance imaging (fMRI) to estimate functional plasticity in the resting-state connectivity of the prefrontal cortex and medial temporal lobe in elderly at both pre- and post-intervention stages.39 The study concluded that a multimodal intervention could delay the process of aging and improve the functional regions that are most heavily influenced by aging as well as promote both brain and cognition preservation.39 Therefore, it would be valuable for future studies to create an RCT cohort study to compare the effects between single or combined cognitive and physical training in normal cognitive functioning Thai elderly.
The non-cognitive impacts of the CTI consisted of the transfer effect on the psychosocial outcomes (ie, depression and QoL), and functional abilities (ie, activities of daily living (ADLs) and mobility). According to the systematic review of meta-analyses, Gavelin et al discovered that the effects of CTI on psychosocial outcomes for healthy older adults had no significant improvement, with the standardized mean effect (g) being 0.23 (95% CI = −0.11 to 0.57).14 Additionally, CTI presented no significant difference between intervention and control groups on the functional abilities of healthy elderly (g = 0.06, 95% CI = −0.15 to 0.27).14,40 This review also showed some evidence that the computerized-CTI among old adults with dementia had no significant benefits on the psychosocial outcomes. For older adults with mild cognitive impairment, the effects on psychosocial and functional outcomes were inconclusive due to the lack of high-quality RTCs.14 In terms of functional abilities, the majority of RTCs demonstrated no significant improvement in the effect of ADLs between those elderly who were allocated to the computerized-CTI and the control group.14 In another systematic review and meta-analysis carried out by Marusic et al, CTI may be able to exert small effects on mobility (complex gait performance with d = 0.47, 95% CI = 0.13 to 0.81);41 however, evidence for high-quality RCTs still needs to prove the strength of this transfer effect. When implementing CTI in healthy elderly, the assessment of psychosocial outcomes and ADLs could exhibit a ceiling effect and show no significant change. Consistent with the previous analysis, the CTI in the present study could not prove that CTI was able to lead to significant improvements in psychosocial outcomes.
The strengths of the present study were the multi-domains and restorative CTI, which were modified for the Thai community based on elderly implementation and holistic outcome measurement. This included cognition and psychosocial outcomes at the immediate treatment stage and after a 6-month follow-up. This particular CTI was designed to be user-friendly for the elderly and convenient to implement in most elderly clubs in the Thai cultural context. Another strength was the RCT design. With both ITT and PP analyses, this present study could reflect the effects of CTI in real-life situations. This study is the first CTI with RCT design implemented in Thailand. It has provided supportive evidence for the value of CTI in terms of primary dementia prevention for Thai community-based elderly residents that could be applicable to other middle-income countries.
The present study has several limitations. Firstly, the present study was unable to quantify the usual recreational group activities and blind the cognitive tasks between both groups of participants. If there were co-intervention and contamination between the experimental group, which received CTI, and the wait-list group, which received usual care, it would dilute the CTI effect on global cognitive function; as a result, the effect size may be smaller. Secondly, the multi-domains and restorative CTI were added into the existing routines of the usual recreational group activities at the elderly center; consequently, the impact on the effect size was perhaps not as large as it could have been if the CTI was administered as an isolated activity. To prove the hypothesis that multimodal training has a larger impact on cognitive function, future RCTs should compare various multimodal training. In terms of the practice effect, the authors attempted to avoid this confounder by designing the intervention to combine various cognitive exercises of CTI which were not the same as the neuropsychological battery. Furthermore, the measurements of outcomes in each endpoint took a 3-month interval to reduce recall bias. Finally, the effect of improvements in cognition from the CTI in the present study did not assess the short- or long-term impacts on psychosocial well-being, ADLs,14 mobility,41 or a risk reduction of dementia syndrome in healthy elderly. Consequently, further trials should explore transfer effects that include ADLs and mobility. Furthermore, other potential modifiable and non-modifiable risk factors, for instance, education, hearing loss, social isolation, Mediterranean diet, metabolic syndrome, and ApoE4 genetic may also have an impact. Another point of note is that the present study implemented only 3-months of CTI; any future trials should investigate the longer-lasting effects of CTI in RCT cohorts with boosting sessions.
Conclusion
In this RCT, CTI showed a significant treatment effect for improvement in global cognitive function in healthy Thai elderly but did not demonstrate a carry-over effect. This CTI was designed to be user-friendly and simple for the community residing older adult population. This study provided preliminary evidence of the feasibility of implementing low-technology CTI in middle-income countries.
Data Sharing Statement
The data that support the findings of this study are available from now and ending 5 years following the article’s publication, at protocols.io on the following link: dx.doi.org/10.17504/protocols.io.36wgqj92kvk5/v1.
Acknowledgments
The authors would like to acknowledge officers from the Elderly Center of Nakornnonthaburi Municipal and Mrs Morakot Buathang, the director of the Public Health and Environment Division, Bureau of Public Health and Environment, Nakornnonthaburi Municipal for their support throughout the completion of this research study.
Funding
This study was funded by the National Research Council of Thailand (NRCT): FY2017 Thesis Grant for Doctoral Degree Students and the 90th Anniversary of Chulalongkorn University Fund, Batch 33 (4/2016).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chen J-H, Lin K-P, Chen Y-C. Risk Factors for Dementia. J Formos Med Assoc. 2009;108(10):754–764. doi:10.1016/S0929-6646(09)60402-2
2. Hebert LE, Bienias JL, Aggarwal NT, et al. Change in risk of Alzheimer disease over time. Neurology. 2010;75(9):786. doi:10.1212/WNL.0b013e3181f0754f
3. Ritchie K, Carrière I, Ritchie CW, Berr C, Artero S, Ancelin ML. Designing prevention programmes to reduce incidence of dementia: prospective cohort study of modifiable risk factors. BMJ. 2010;341:c3885. doi:10.1136/bmj.c3885
4. Norton S, Matthews FE, Barnes DE, Yaffe K, Brayne C. Potential for primary prevention of Alzheimer’s disease: an analysis of population-based data. Lancet Neurol. 2014;13(8):788–794. doi:10.1016/s1474-4422(14)70136-x
5. Livingston G, Sommerlad A, Orgeta V, et al. Dementia prevention, intervention, and care. Lancet. 2017;390(10113):2673–2734. doi:10.1016/s0140-6736(17)31363-6
6. Valls-Pedret C, Sala-Vila A, Serra-Mir M, et al. Mediterranean diet and age-related cognitive decline: a randomized clinical trial. JAMA Intern Med. 2015;175(7):1094–1103. doi:10.1001/jamainternmed.2015.1668
7. Young J, Angevaren M, Rusted J, Tabet N. Aerobic exercise to improve cognitive function in older people without known cognitive impairment. Cochrane Database Syst Rev. 2015;(4):Cd005381. doi:10.1002/14651858.CD005381.pub4
8. Kuiper JS, Zuidersma M, Oude Voshaar RC, et al. Social relationships and risk of dementia: a systematic review and meta-analysis of longitudinal cohort studies. Ageing Res Rev. 2015;22:39–57. doi:10.1016/j.arr.2015.04.006
9. Wilson RS, Mendes De Leon CF, Barnes LL, et al. Participation in cognitively stimulating activities and risk of incident Alzheimer disease. JAMA. 2002;287(6):742–748. doi:10.1001/jama.287.6.742
10. Valenzuela MJ, Sachdev P. Brain reserve and dementia: a systematic review. Psychol Med. 2006;36(4):441–454. doi:10.1017/s0033291705006264
11. Ballesteros S, Kraft E, Santana S, Tziraki C. Maintaining older brain functionality: a targeted review. Neurosci Biobehav Rev. 2015;55:453–477. doi:10.1016/j.neubiorev.2015.06.008
12. Gates NJ, Rutjes AW, Di Nisio M, et al. Computerised cognitive training for maintaining cognitive function in cognitively healthy people in midlife. Cochrane Database Syst Rev. 2019;3:Cd012278. doi:10.1002/14651858.CD012278.pub2
13. Gates NJ, Rutjes AW, Di Nisio M, et al. Computerised cognitive training for maintaining cognitive function in cognitively healthy people in late life. Cochrane Database Syst Rev. 2019;3:Cd012277. doi:10.1002/14651858.CD012277.pub2
14. Gavelin HM, Lampit A, Hallock H, Sabatés J, Bahar-Fuchs A. Cognition-oriented treatments for older adults: a systematic overview of systematic reviews. Neuropsychol Rev. 2020;30(2):167–193. doi:10.1007/s11065-020-09434-8
15. Mewborn CM, Lindbergh CA, Miller LS. Cognitive interventions for cognitively healthy, mildly impaired, and mixed samples of older adults: a systematic review and meta-analysis of randomized-controlled trials. Neuropsychol Rev. 2017;27(4):403–439. doi:10.1007/s11065-017-9350-8
16. Sitzer DI, Twamley EW, Jeste DV. Cognitive training in Alzheimer’s disease: a meta-analysis of the literature. Acta Psychiatr Scand. 2006;114(2):75–90. doi:10.1111/j.1600-0447.2006.00789.x
17. Prasartkul P. Situation of Thai Elderly 2013. Amarin Printing and Publishing; 2014:126.
18. Prakongsai P. Thailand Health Profile 2011–2015. The Strategy and Planing Divison; 2016. Available from: http://wops.moph.go.th/ops/thp/thp/userfiles/1_artwork54_58.pdf.
19. Hughes CP, Berg L, Danziger W, Coben LA, Martin RL. A new clinical scale for the staging of dementia. Br J Psych. 1982;140(6):566–572. doi:10.1192/bjp.140.6.566
20. Morris JC. The Clinical Dementia Rating (CDR): current version and scoring rules. Neurology. 1993;43(11):2412–2414. doi:10.1212/WNL.43.11.2412-A
21. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
22. Train The Brain Forum Committee (Thailand). Thai mental state examination (TMSE). Siriraj Hosp Gaz. 1993;45(6):359–374.
23. Kanjananopinit S, Charoensak S, Keawpornsawan T. The study of psychometric properties of cognistat Thai version. J Psychiatr Assoc Thailand. 2014;59(4):409–418.
24. Thavichachart N, Worakul P, Karnjananakin P. Alzheimer’s disease Assessment Scale (ADAS): Thai version. J Gerontol Geriatr Med. 2002;3:21–32.
25. Na Chiangmai N, Wongupparaj P. Dementia screening tests in Thai older adults: a systematic review. J Mental Health Thailand. 2020;28(3):252–265.
26. Bowling A, Hankins M, Windle G, Bilotta C, Grant R. A short measure of quality of life in older age: the performance of the brief older people’s quality of life questionnaire (OPQOL-brief). Arch Gerontol Geriatr. 2013;56(1):181–187. doi:10.1016/j.archger.2012.08.012
27. Sheikh JI, Yesavage JA. Geriatric Depression Scale (GDS): recent evidence and development of a shorter version. J Aging Mental Health. 1986;5(1–2):165–173. doi:10.1300/J018v05n01_09
28. Wongpakaran N, Wongpakaran T, Van Reekum R. The Use of GDS-15 in Detecting MDD: a comparison between residents in a Thai long-term care home and geriatric outpatients. J Clin Med Res. 2013;5(2):101–111. doi:10.4021/jocmr1239w
29. Rovinelli RJ, Hambleton RK. On the use of content specialists in the assessment of criterion-referenced test item validity. Dutch J Educ Res. 1977;2:49–60.
30. Phanasathit M. Validity and Reliability of Lawton Instrumental Activities of Daily Living Scale (L-IADL) and Older People’s Quality of Life Questionnaire (OPQOL-Brief): Thai version; 2017.
31. Bernard R. Fundamentals of Biostatistics. Duxbury Press Pacific Grove; 2000.
32. Program - The Thailand Research Fund&Prince of Songkla University. n4Studies: sample size and power calculations for iOS The Royal Golden Jubilee Ph.D. Program - The Thailand Research Fund&Prince of Songkla University; 2014.
33. IBM Corp. SPSS Statistics for Windows, Version 17.0. SPSS Inc; 2008.
34. Hedges LV. distribution theory for glass’s estimator of effect size and related estimators. J Educ Stat. 1981;6(2):107–128. doi:10.2307/1164588
35. Valenzuela M, Sachdev P. Can cognitive exercise prevent the onset of dementia? Systematic review of randomized clinical trials with longitudinal follow-up. Am J Geriatr Psychiatry. 2009;17(3):179–187. doi:10.1097/JGP.0b013e3181953b57
36. Papp KV, Walsh SJ, Snyder PJ. Immediate and delayed effects of cognitive interventions in healthy elderly: a review of current literature and future directions. Alzheimer’s Dementia. 2009;5(1):50–60. doi:10.1016/j.jalz.2008.10.008
37. Toril P, Reales JM, Ballesteros S. Video game training enhances cognition of older adults: a meta-analytic study. Psychol Aging. 2014;29(3):706–716. doi:10.1037/a0037507
38. Oswald WD, Gunzelmann T, Rupprecht R, Hagen B. Differential effects of single versus combined cognitive and physical training with older adults: the SimA study in a 5-year perspective. Eur J Ageing. 2006;3(4):179. doi:10.1007/s10433-006-0035-z
39. Li R, Zhu X, Yin S, et al. Multimodal intervention in older adults improves resting-state functional connectivity between the medial prefrontal cortex and medial temporal lobe. Front Aging Neurosci. 2014;6:39. doi:10.3389/fnagi.2014.00039
40. Tetlow AM, Edwards JD. Systematic literature review and meta-analysis of commercially available computerized cognitive training among older adults. J Cognitive Enhance. 2017;1(4):559–575. doi:10.1007/s41465-017-0051-2
41. Marusic U, Verghese J, Mahoney JR. Cognitive-based interventions to improve mobility: a systematic review and meta-analysis. J Am Med Dir Assoc. 2018;19(6):484–491.e3. doi:10.1016/j.jamda.2018.02.002
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Adherence to Atrial Fibrillation Better Care (ABC) Pathway Management of Chinese Community Elderly Patients with Atrial Fibrillation: A Cross-Sectional Study
Zhang X, Huang J, Weng F, Wen Y, Wang X, Jiang J, Xue Y, Li K
Patient Preference and Adherence 2023, 17:1813-1823
Published Date: 25 July 2023
Barriers and Facilitators to Exercise Compliance for Community Elders with COPD: A Cross-Sectional Study
Xia J, Yang J, Yang X, Zhang S, Guo H, Zhang C
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1965-1974
Published Date: 8 September 2023
The Impact of Online Interactive Platform Services on Oral Health Behaviors in Older Adults With Mild Cognitive Impairment: Protocol for a Randomized Controlled Trial
Yin Q, Chai Z, Tao B, Liu P, Luo Y, Zhao Q, Yang B
Journal of Multidisciplinary Healthcare 2025, 18:663-674
Published Date: 7 February 2025
A Qualitative Study of Patient Experiences in Non-Communicable Disease Management Within Jordan’s Healthy Community Clinics Program

Al-Maghaireh D, Al Nsour A, Alsaqer K, Kawafha MM, Ireifij AE, Farraj R, Abu Hashish S, Abu Fanouneh SN
Journal of Multidisciplinary Healthcare 2025, 18:7089-7101
Published Date: 4 November 2025