Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Barriers and Facilitators to Exercise Compliance for Community Elders with COPD: A Cross-Sectional Study
Authors Xia J ![]() , Yang J, Yang X, Zhang S, Guo H, Zhang C
, Yang J, Yang X, Zhang S, Guo H, Zhang C
Received 2 June 2023
Accepted for publication 23 August 2023
Published 8 September 2023 Volume 2023:18 Pages 1965—1974
DOI https://doi.org/10.2147/COPD.S424137
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Jieqiong Xia,* Jing Yang,* Xiaoli Yang, Siqi Zhang, Honghua Guo, Caihong Zhang
International Nursing School, Hainan Medical University, Haikou, Hainan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Siqi Zhang; Honghua Guo, International Nursing School, Hainan Medical University, No. 3 Xueyuan Road, Longhua District, Haikou, Hainan, 571199, People’s Republic of China, Email [email protected]; [email protected]
Background and Aim: Exercise compliance was known as important to improve long-term health conditions for Chronic obstructive pulmonary disease (COPD) patients, however, little was known about the determinants which affect their exercise compliance. This study aimed to investigate factors related to exercise compliance of COPD elderly patients.
Methods: This cross-sectional study included elderly patients with stable COPD participants. Random cluster sampling and a survey, including the Exercise Compliance Scale, mMRC Dyspnea Index Scale, Social Support Scale, Anxiety Self-Assessment Scale, and Self-rating Depression Scale, were used. Data were analyzed using Spearman correlation and backward logistic regression.
Results: 124 participants (45.90%) had poor exercise compliance while 146 had good compliance (54.10%). The backward logistic regression showed household monthly income (¥ 501–¥ 1500: OR=21.54, P< 0.05; ¥ 3001–¥ 5000: OR=32.76, P< 0.05), two chronic comorbidities (OR=17.13, P< 0.05), and the moderate dyspnea (OR=16.87, P< 0.05) might help to improve exercise compliance. While female COPD patients (OR=0.11, P< 0.01) who had server dyspnea (OR=0.02, P< 0.05) and depression (OR=0.84, P< 0.05) might have more difficulties adhering to exercise.
Conclusion: Low exercise compliance in community-dwelling elderly COPD patients could be affected by sex, monthly income level, number of chronic comorbidities, dyspnea, and depression.
Keywords: chronic obstructive pulmonary disease, exercise compliance, elderly, community
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by chronic cough, expectoration, chest tightness, shortness of breath, and dyspnea, with clinical features such as slow progression, a long course, severe illness, and great harm.1,2 According to the 2020 Global Strategy for Prevention, Diagnosis, and Management of COPD,3 among people over the age of 40 in the world, the estimated prevalence of COPD is 5–16% while people over 60 years of age might exceed 27%. More than 5.4 million people are predicted to die from COPD and related diseases by 2060. In 2018, results of the “Chinese Adult Lung Health Study” showed that prevalence of COPD in adults aged 20 years or above in China was 8.6%, and those aged more than 40 years were as high as 13.7%. The number of COPD patients in China is estimated to be nearly 100 million.4
Currently, COPD prevention and treatment guidelines for countries around the world suggest exercise as a rehabilitation method for non-drug treatment of COPD5 Exercise can not only effectively improve patients’ symptoms, such as dyspnea,6 but also improve exercise tolerance, daily activities, pulmonary function, and quality of life.7–10 The incidence of re-exacerbations, readmission, and mortality would then be lowered in COPD patients over a lengthy period of time.11–13 Public health guidelines recommend that patients with chronic diseases should maintain moderate-to-vigorous physical activity for more than 5 days a week, at least 30 min per day (total ≥ 150 min/week).14 However, even though most patients know having regular exercise would improve their long-term body function, a low level of exercise compliance is still a major concern for COPD patients who are sedentary and have low intrinsic motivation to exercise.15 Studies have shown that patients’ cognition of exercise and physical and psychological problems such as fatigue, mobility impairment, breathing problems, depression, and disappointment could create barriers to COPD patients for their exercise compliance.16
At present, research on the exercise of COPD patients with COPD in China is limited, and rehabilitation exercises are mainly suitable for patients who stay in hospitals. Exercise compliance and its influencing factors in community-dwelling elderly patients with stable COPD are currently unknown. Therefore, this study aimed to develop a cross-sectional survey to examine exercise compliance of stable COPD patients in several communities in Haikou.
Methods
This cross-sectional study was conducted in Haikou, the capital city with the most diverse population in Hainan Province, between April and July 2021.
Sampling and Participants
Random cluster sampling was used in this study. The sample size was calculated based on the Equation N=4Uα2S2/δ2, and Uα=1.96, δ was set as 0.25S,17 so N = 246, and considered there might be a 10% loss rate, so we finally decide the size could be 271.
According to the 10% prevalence of COPD patients aged > 60 in China18 and the number of permanent residents in Haikou (2,873,358), the number of COPD patients in Haikou City was approximately 287,335. Haikou has 211 districts, and each district has approximately 1361 COPD patients.
The research team randomly encoded all districts into a random number table, then selected one district and included all COPD patients who satisfied the inclusion criteria for this study: ① aged ≥ 60; ② consistent with the COPD diagnosis guideline made by the Chinese Medical Association (2021);19 ③ had at least three months of GOLD pulmonary rehabilitation training;20 ④ able to understand the content of the questionnaire. Participants were excluded if they had ① other serious diseases and were unable to cooperate; ② mental illness or inability to express thoughts; ③ no exercise due to trauma or other reasons. If recruitment in this district failed to reach 271 participants, another random selection was conducted until the sample size was reached. Finally, we selected three districts.
Questionnaire and Scales
The demographic questionnaire was designed to investigate age, sex, marital status, lifestyle, occupation before retirement, education level, monthly household income, chronic comorbidity, COPD history, hospital stays, exercise training, and smoking status.
The exercise compliance questionnaire was designed based on the existing exercise compliance surveys,21–23 which had three dimensions and 17 questions. The three dimensions were physical activity (8 items), effect supervision (3 items), and advice-seeking (6 items). Each question applied a 4-Point Likert Scale ranging from “I can’t do it at all”, “occasionally I can do it”, “basically I can do it”, to “I can do it completely.” The total score of the questionnaire was 68. The compliance index was calculated based on the compliance score and the compliance index (compliance score/68) ×100. compliance scores greater than 75 were identified as high compliance, 50–75 was moderate, and low.22 The questionnaire was pilot tested and reviewed by five professionals (three respiratory experts, one statistician, and one rehabilitation training expert). Cronbach’s α was 0.83, and the content validity was 0.92.
The Modified Medical Research Council (mMRC) Dyspnea Scale24 divides COPD dyspnea into five levels. Grade 0: no dyspnea except vigorous workout; Grade I: Difficulty in breathing when moving quickly or climbing a hill; Grade II: walking slower than peers due to dyspnea or need to stop due to dyspnea when walking at own pace; Grade III: need to stop breathing after walking approximately 100 m or a few minutes; Grade IV: Difficulty in breathing when leaving the room or dressing and undressing. mMRC grade 0, mild dyspnea; grade 1, moderate while grade 2–4, severe dyspnea.
Social Support Rating Scale (SSRS) employed one made by Xiao et al25 The scale consists of three dimensions: objective support (3 items), subjective support (4 items), and utilization of social support (3 items). The total SRSS score was the sum of the scores of the 10 items. A higher score indicated higher social support received, with an overall score of 66 points. 45–66 points were deemed a high level of social support, while 23–44 points are considered medium, and less than 22 points are considered low. The retest credibility of the scale was 0.92, and the consistency coefficient of each item is between 0.89–0.95.
Self-rating anxiety scale (SAS) and Self-Rating Depression Scale (SDS)26 were used. Both scales were filled according to the frequency of symptoms showing in each item and applied Likert 4-point system. The calculation is based on one to four points for the negative description, while the positive is calculated in reverse order. The sum of the scores of the 20 items multiplied by 1.25 was the standard score of each participant. A SAS score greater than 50 was considered anxiety, while 50–59 was mild, 60–69 was moderate, and 70 was severe. An SDS score larger than 53 indicated depression, while 23–62 indicated mild, 63–72 indicated moderate depression, and > 73 indicated severe depression.
Data Collection
Contact information of COPD patients with COPD was obtained from the health records of three randomly selected communities. The research team explained the purpose, meaning, and requirements of this study to the participants and their families through phone calls. After obtaining consent, patients with COPD in the stable stage who met the inclusion criteria were investigated anonymously. The questionnaires were distributed and collected individually. Participants were requested to complete the questionnaire independently. All the questionnaires were screened for missing values when they were returned to the research team.
Data Analysis
SPSS26.0 statistical software was used to analyse the data obtained. Demographic data are presented as X±s and percentages (%). The t-test and chi-square test were used to test the differences between groups. Spearman’s rank correlation analysis was used to investigate the strength and direction of the association between variables. Backward logistic regression analysis was performed to investigate determinants of exercise compliance. Statistical significance was set at P≤0.05.
Validity, Reliability and Rigor
All investigators were members of the research team. Training on the research purpose, questionnaire content, and data collection methods was conducted for all investigators prior to collection. Each participant was coded before analysis. Two researchers double-checked all questionnaires while inputting all data into the software to ensure accuracy. Data cleaning was done by two researchers together. The questionnaire was deleted if its missing values were more than 10%. Less than 10% would use mean to replace the missing item.
Ethical Consideration
This study was conducted in accordance with the Principles of the Declaration of Helsinki and was reviewed and approved by Hainan Medical University (LLXJSHL002).
Results
Social Demographic of the Respondents
In total, 270 questionnaires were finally distributed, and the effective response rate of 99.6%. The participants were predominantly male (n=164, 60.7%), of elder age (68.6±5.3 years), married (n=197, 73%), and currently non-smoking (n=141, 52.2%). Most lived with spouses (n=177, 66.5%), 47 cases (17.4%) lived alone, and nearly a quarter lived with children or grandchildren. Nearly half of respondents had primary school education (n=128, 47.4%), while the rest stopped at middle school (n=96, 35.6%) and high school (n=46, 17%). Occupation of the Participants before retiring were mainly farmers (n=111, 41.1%) and workers (n=88, 32.6%). For the monthly household income, over 70% could have ¥1501–5000 per month (a currency exchange rate of US $1=¥6.5 at then), while close to 10% of them less than ¥500. Most COPD participants have a chronic comorbidity (n=183, 67.8%), while 70 patients had two (n=70, 25.9%). 36.9% had been admitted to the hospital 1–2 times previously, and 47% had 3–4 times. Close to 70% of patients have more than five years of COPD history. In terms of exercise training, only 9.3% preferred to attend hospital and community exercise training, while the rest four exercise training had similar number of participants (Table 1).
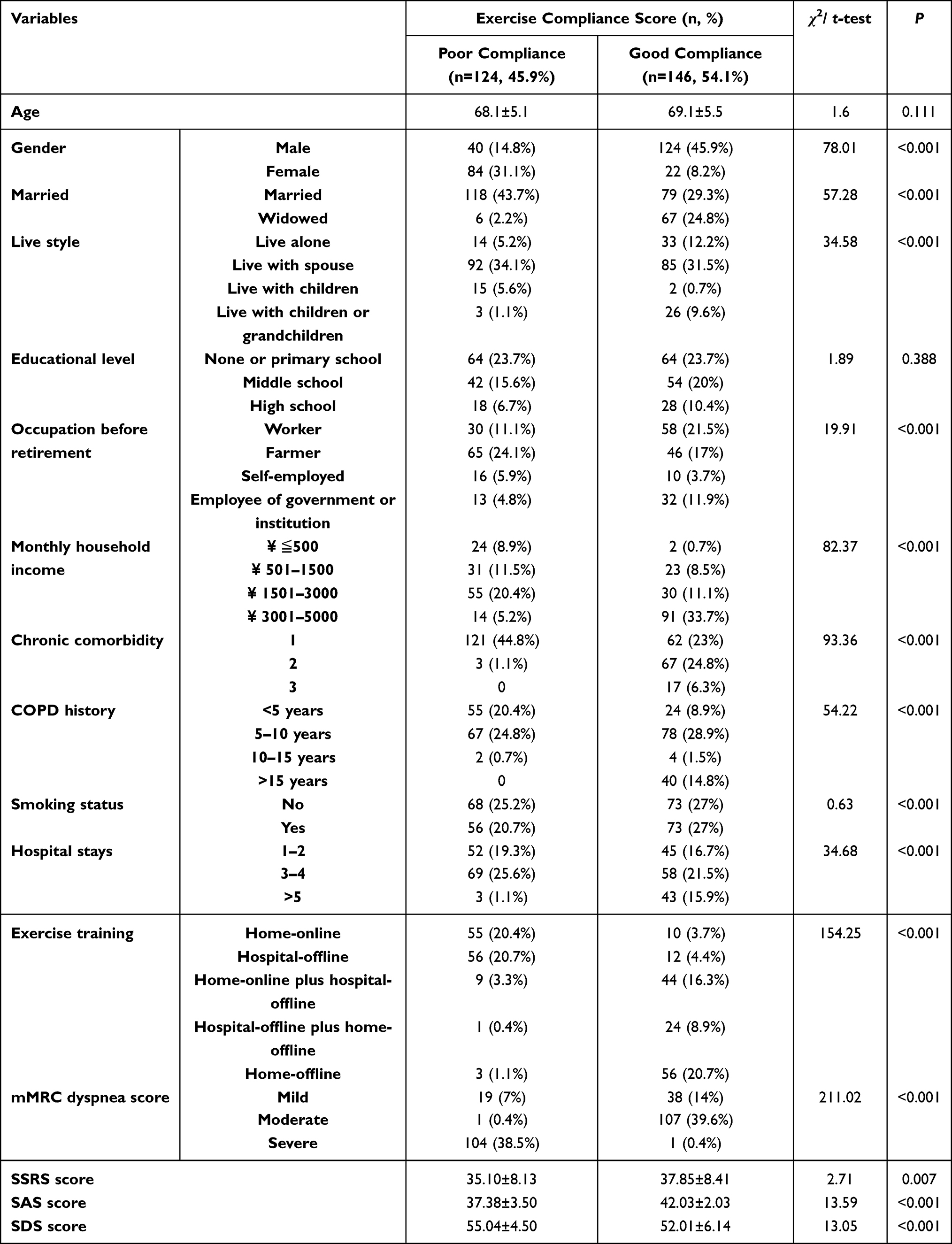 |
Table 1 The Exercise Compliance Score Across Social Demographic Variables (n=270) |
Exercise Compliance, mMRC Dyspnea, SAS, SDS, and Social Support
The overall score of the exercise compliance questionnaire of 270 patients was 54.1±6.5. In its three dimensions, the physical activity score was 26.9±3.9, effect supervision 9.6±1.9, and advice seeking 17.7±1.1 (Table 2). In total, 124 participants (45.90%) had poor compliance and 146 had good compliance (54.10%). Regarding the mMRC dyspnea score, moderate or severe dyspnea was 108 cases (40%) and 105 cases (38.9%) respectively. The social support score of the participants was 36.6±8.4. The SAS score ranged from 39.9±3.6, so no one was deemed anxious. The score of SDS was 68.8±5.6, and among them, 136 (50.4%) had mild depression cases and 10 cases (3.7%) were moderate, and 124 cases (45.9%) had no depression (Table 1).
 |
Table 2 Exercise Compliance, mMRC Dyspnea, SAS, SDS and Social Support |
The Exercise Compliance Score Across Social Demographic Variables
Table 1 shows that there was a statistically significant difference between poor and good exercise compliance according to sex, marital status, lifestyle, occupation before retirement, household monthly income, chronic comorbidity, COPD history, hospital stay, exercise training, mMRC dyspnea score, SSRS score, SAS score, and SDS score (P<0.001). There was no significant difference between the two exercise compliance levels at different ages, education levels, or smoking statuses (P>0.05).
The Correlation Between Exercise Compliance and Social Demographic Variables
Spearman correlation analysis showed that exercise compliance was correlated with some demographic factors, such as sex, marital status, household monthly income, chronic comorbidity, COPD history, hospital stay, exercise training, mMRC dyspnea score, SSRS score, SAS score, and SDS score (P<0.001), but not with lifestyle or occupation before retirement (P> 0.05) (Table 3).
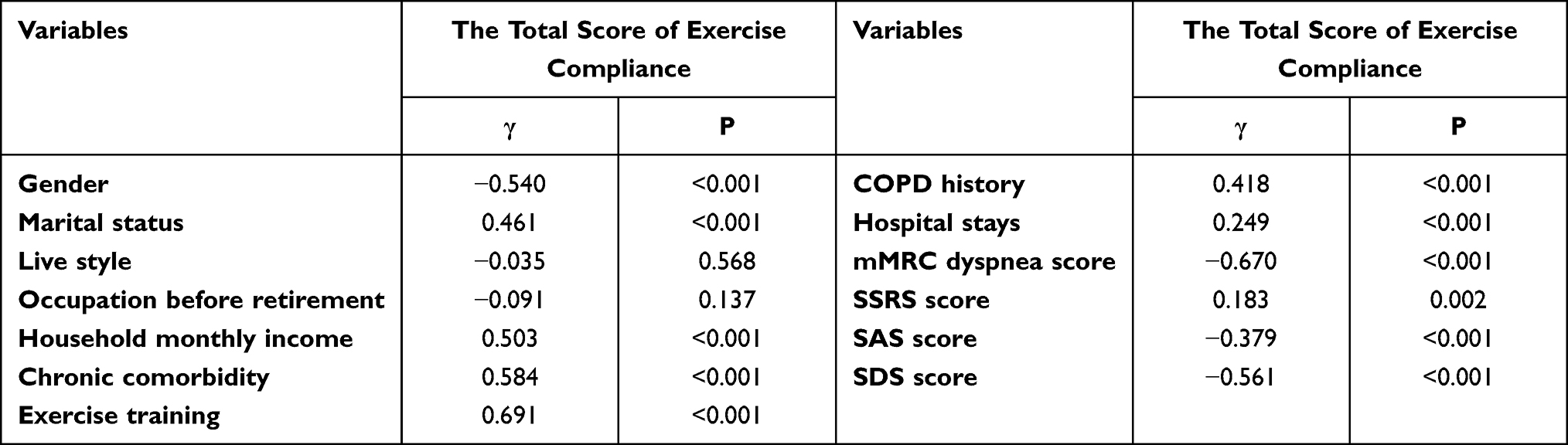 |
Table 3 Correlation Analysis Between Exercise Compliance and Basic Data in Elderly Patients with Stable COPD (N=270) |
Facilitators and Barriers to Exercise Compliance
The backward logistic regression analysis results showed that compared with males, elderly women with COPD had lower exercise compliance (OR=0.11, P<0.01). Participants who had family income ¥501 to ¥1500 (OR=21.54, P<0.05) had lower exercise compliance than those who had ¥3001-¥5000 (OR=32.76, P<0.05) per month. Compared to participants with one chronic comorbidity, those with two comorbidities (OR=17.13, P<0.05) showed more exercise compliance. Those with moderate dyspnea (OR=16.87, P<0.05) had higher exercise compliance than those with mild breathing difficulties. As dyspnea became more severe, COPD patients were reluctant to exercise (OR=0.02, P<0.01). Exercise compliance was poorer with higher depression scores (OR=0.84, P<0.01) (Table 4).
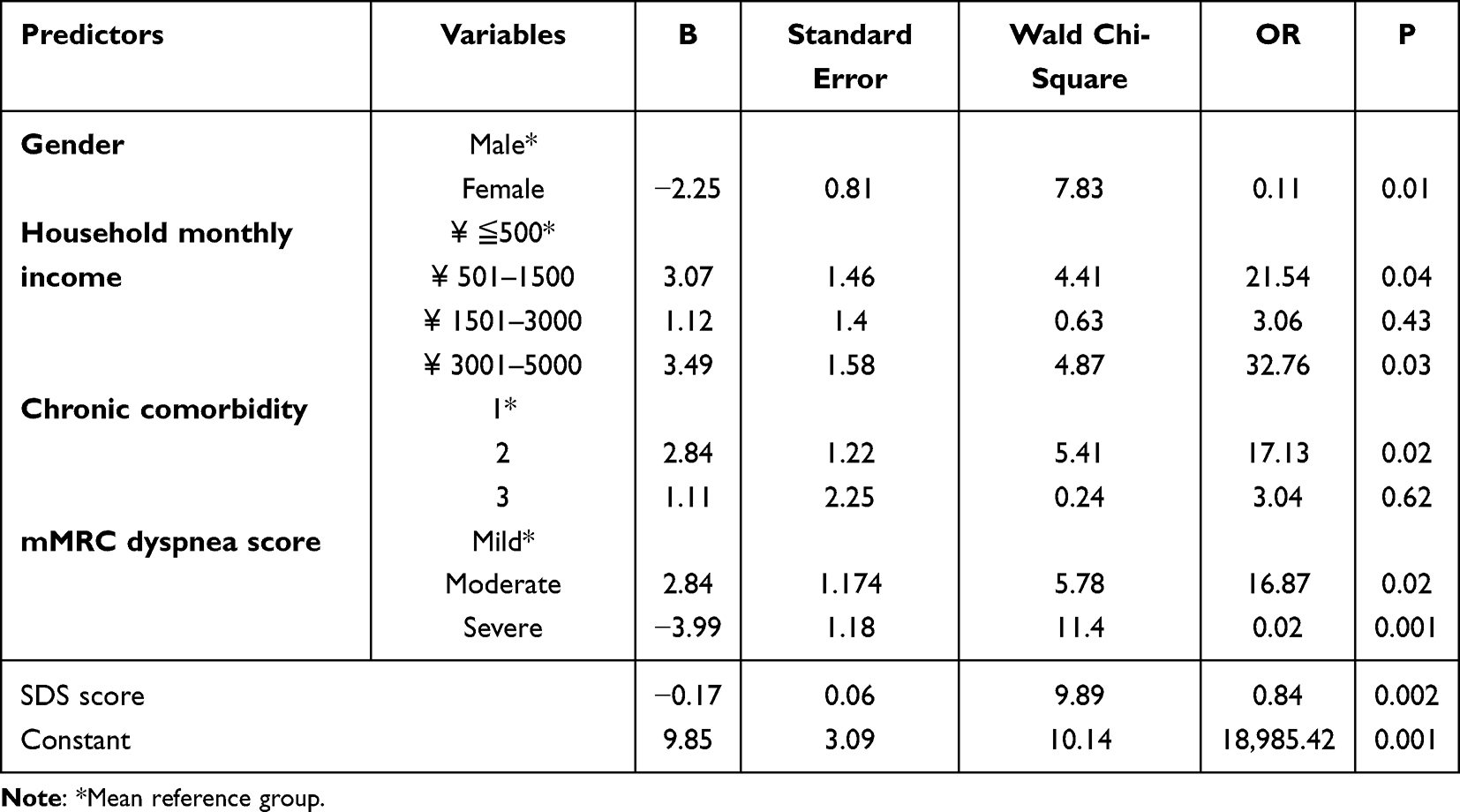 |
Table 4 Logistic Regression Analysis of Exercise Compliance (N=270) |
Discussion
Compliance refers to a behavior in which a patient would like to do what his or her doctor suggested and is consistent with the medical advice for a long time, which would, to a large extent, affect the effect of exercise.27 At present, there is no scale of exercise compliance for patients with COPD; therefore, this study applied a self-designed exercise compliance scale, especially for community-dwelling patients. The results showed that the exercise compliance score of elderly patients with stable COPD in the community was relatively low compared with that of patients in the hospital.28 45.9% was A poor level of exercise compliance and 50.50% was good, which was not ideal compared to other chronic patients, such as heart failure.29 This may be due to COPD caused symptoms, such as dyspnea, fatigue, skeletal muscle dysfunction, and frailty, which would undermine patients’ motivation to exercise.30 Community health workers should pay more attention to the exercise situation of patients with COPD to ensure compliance.
Female participants in this study had lower exercise compliance than male participants, which is similar to the findings of McCarron et al.31 This may be because of the maternal role in the Chinese family structure. They defaulted as housekeepers who voluntarily took responsibility for looking after others through other daily activities such as shopping, cleaning, and cooking. This may have resulted in insufficient exercise duration. Some may even treat these activities as a type of exercise that can achieve the same effect. Therefore, after discharge from the hospital, their “patient” role would be replaced by the “caregiver” role in the family atmosphere, and their motivation to adhere to exercise training became low. For community-dwelling female patients with COPD, qualitative studies exploring the reasons for low exercise adherence are needed. Research comparing daily activity consumption with current exercise training to design a more fittable program is needed to improve compliance.
Monthly Household income is another factor affecting exercise compliance, which has been substantiated by research.32,33 In this study, compared with participants with a monthly income less than ¥500, elderly COPD patients with monthly incomes of ¥501–¥1500 and ¥3001–¥5000 had better exercise compliance. The reason for this might be that low-income COPD patients have a lower awareness of the benefits of exercise. Moreover, insufficient financial support limits access to hospital rehabilitation training. Exercise compliance of participants with monthly household income between ¥1500 and ¥3000 showed no significant difference compared to those with less than ¥500 family income per month. This might be because these participants mostly lived in urban villages, who might have had a better income but limited awareness and access to comprehensive hospital rehabilitation training. Community health services in these areas are often as undeveloped as those in the villages. Therefore, urban villages should be considered when planning for community rehabilitation services.
The mMRC dyspnea index score reflects the breathing difficulty of COPD patients, and the patient’s lung function during exercise directly affects their comfort. In this study, patients with moderate dyspnea showed higher exercise compliance; however, severe dyspnea impeded compliance. Patients with two types of chronic comorbidities had better exercise compliance; however, patients with three comorbidities showed no differences. To some extent, this meant that when the patient realized a serious condition, they adhered to exercise to improve their body function. However, severe dyspnea and multiple comorbidities would block their activities. This was in accordance with many studies34–36 which showed that patients with higher dyspnea scores had poorer adherence to pulmonary rehabilitation. Therefore, before exercise training, the patient’s respiratory function and comorbidities should be comprehensively evaluated, and medication management and home oxygen therapy should be provided to create an individualized exercise plan for each patient.
The participants showed no anxiety, while 54.10% of them were depressed, of which mild depression accounted for 50.40% had moderate depression 3.70%. Studies have also reported a high incidence of anxiety and depression in patients with COPD.37,38 Owing to the long disease course and progressive aggravation, patients with COPD face various pressures. In addition, chronic cerebral hypoxia caused by the disease and brain cell degeneration induced by medications can lead to anxiety and depression.39 The regression analysis results of this study were consistent with the findings of Pierobon et al,40 who showed that anxiety and depression were independent predictors of pulmonary rehabilitation compliance, and that a higher degree of depression would lead to lower patient compliance. The cure rate for depression in COPD patients was only 30%.41 Mental stress in COPD patients is common but has long been neglected in clinical practice. Further research on improving exercise compliance is needed to include psychologists to continuously assess patients’ mental states and to implement early interventions.
Currently, COPD exercise rehabilitation programs are designed using a combination of home- or hospital-based online and offline interventions. Offline hospital exercise training was mainly conducted during the patient’s hospital stay, under the supervision of health professionals. Most offline home training was organized before discharge through pre-training, delivering home-based rehabilitation booklets, watching videos, and follow-up phone calls after discharge. Some programs would also design home online training or integration of the two types, and many studies have found the significance of COPD exercise outcomes through online and offline exercise training.42–44 In this study, most participants attended hospital-offline training, but most showed good compliance with home-offline training organized by community health services. This might be because home-offline training was near and easy to access, and was more suited for elderly patients (> 60 years of age in this study) who preferred face-to-face interactions. Participants had low engagement in hospital-offline exercise, but relatively higher compliance with programs that integrated home-online and hospital-offline exercise training. This might be due to the long commute time and cost, as well as their poorer physical condition, which made offline hospital training more difficult after discharge. However, with the polarization of information technology among elderly people in China during COVID-19, participants who had been educated in the hospital before discharge might be more interested in following home-online exercise training.
Limitation
This study has some limitations. For example, it merely investigated exercise compliance in elderly COPD patients in Haikou City. It is suggested that COPD patients of different age groups and regions should be more comprehensively investigated in future research. In addition, due to the research design, details of the current exercise training program (such as intervention time, setting, and methods) were missed in the questionnaire design. Further large-scale investigations could categorize the current COPD exercise training in China to systematically and pragmatically evaluate the compliance of patients to each type of exercise.
Conclusion
The exercise compliance of community-dwelling elderly COPD patients was not ideal, and sex, monthly income level, number of chronic comorbidities, dyspnea, and depression could have an impact on it. Attention should be paid more to the screening and intervention of high-risk groups in both hospital and community-level healthcare settings.
Ethics Statement
This study was conducted based on Principles of Declaration of Helsinki and has been ethically reviewed and approved by Hainan Medical University (LLXJSHL002).
Funding
This research was funded by 2019 Hainan Provincial Basic and Applied Research Program (Natural Science Field) High-level Talent Project Funding (2019RC233).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hogg JC, Timens W. The pathology of chronic obstructive pulmonary disease. Annu Rev Pathol. 2009;4:435–459. doi:10.1146/annurev.pathol.4.110807.092145
2. Akgun KM, Crothers K, Pisani M. Epidemiology and management of common pulmonary diseases in older persons. J Gerontol a Biol Sci Med Sci. 2012;67(3):276–291. doi:10.1093/gerona/glr251
3. Global initiative for chronic obstructive lung disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2020 REPORT) [EB/OL]; 2019. Available from: https://goldcopd.org/goldreports/.
4. Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in china [the China Pulmonary Health (CPH) study]: a national cross-sectional study. Lancet. 2018;391(10131):1706–1717. doi:10.1016/S0140-6736(18)30841-9
5. InformedHealth.org. Chronic Obstructive Pulmonary Disease (COPD): Non-Drug Treatments. Cologne, Germany: Institute for Quality and Efficiency in Health Care (IQWiG); 2006.
6. Zwerink M, van der Palen J, van der Valk P, et al. Relationship between daily Physical activity and exercise capacity in Patients with COPD. Respir Med. 2013;107:242–248. doi:10.1016/j.rmed.2012.09.018
7. Miravitlles M, Hurst JR, Calverley PM, et al. Management of COPD exacerbations: a European Respiratory Society/American Thoracic Society guideline. Eur Respir J. 2017;49(3):1–16.
8. Burchette JE, Campbell GD, Geraci SA, et al. Preventing hospitalizations from acute exacerbations of chronic obstructive pulmonary disease. Am J Med Sci. 2017;353(1):31–40. doi:10.1016/j.amjms.2016.06.006
9. Feifei H, Wen Z, Lian C, et al. Application progress of pulmonary rehabilitation in patients with acute exacerbation of chronic obstructive pulmonary disease. Chin Gen Med. 2017;20(18):2176–2182.
10. Lewis N, Gelinas JCM, Ainslie PN, et al. Cerebrovascular function in Patients with chronic obstructive Pulmonary disease: the impact of exercise training. Am J Physiol Heart Circ Physiol. 2019;316(2):380–391. doi:10.1152/ajpheart.00348.2018
11. Spielmanns M, Meier A, Winkler A, et al. Pulmonary rehabilitation after acute exacerbation of COPD reduces the rate of re-exacerbations. Dtsch Med Wochenschr. 2017;142(2):10–19.
12. Chunyun Z, Zhangsheng L, Yimin C. Effects of pulmonary rehabilitation exercise training on chronic obstructive pulmonary disease. J Liaoning Univ Tradit Chin Med. 2010;12(2):88–89.
13. Moore E, Palmer T, Newson R, et al. Pulmonary rehabilitation as a mechanism to reduce hospitalizations for acute exacerbations of COPD: a systematic review and meta-analysis. Chest. 2016;150(4):837–859. doi:10.1016/j.chest.2016.05.038
14. Garber CE, Blissmer B, Deschenes MR, et al; American college of sports medicine Position Stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc. 2011;43(7):1334–1359. doi:10.1249/MSS.0b013e318213fefb
15. Collado-Mateo D, Lavín-Pérez AM, Peñacoba C, et al. Key factors associated with adherence to physical exercise in patients with chronic diseases and older adults: an umbrella review. Int J Environ Res Public Health. 2021;18(4):2023. doi:10.3390/ijerph18042023
16. Kosteli MC, Heneghan NR, Roskell C, et al. Barriers and enablers of Physical activity engagement for patients with COPD in primary care. Int J Chron Obstruct Pulmon Dis. 2017;28(12):1019–1031. doi:10.2147/COPD.S119806
17. Ni P, Chen JL, Liu N. The sample size estimation in quantitative nursing research. Chin J Nurs. 2009;45:378–380.
18. Guoshuang Q, Haoyu W, Chuanhua Y. The prevalence and trend of COPD and YLD in China. Public Health Prev Med. 2019;30(2):4–8.
19. The Chronic Obstructive Pulmonary Disease Group of the Respiratory Branch of the Chinese Medical Association, the Chronic Obstructive Pulmonary Disease Working Committee of the Respiratory Doctors Branch of the Chinese Medical Doctor Association. Guidelines for the diagnosis and treatment of chronic obstructive pulmonary disease (2021 revision). J Chin Tuberc Respir J. 2021;44(3):170 205. doi:10.3760/cma.j.cn112147-20210109-00031
20. Global Initiative for Chronic Obstructive Lung Disease, Inc. 2021 gold reports - global initiative for chronic obstructive lung disease, GOLD. Global Initiative for Chronic Obstructive Lung Disease, Inc; 2021. Available from: https://staging.goldcopd.org/2021-gold-reports/.
21. Fengjuan L. Postoperative Functional Exercise Compliance and Its Influencing Factors in Breast Cancer Patients. Guangdong: Sun Yat-Sen University; 2008.
22. Jianhui Y. Study on the Relationship Between Health Literacy, Functional Exercise Compliance and Rehabilitation Training Effect in Stroke Patients. Qingdao: Shandong; 2020.
23. Xiaolan C. Development of Pulmonary Rehabilitation Program for Patients with Chronic Obstructive Pulmonary Disease During Hospitalization. Jiangsu: Soochow University; 2019.
24. Jing C. Analysis of Compliance and Influencing Factors of Home Pulmonary Rehabilitation in Patients with Stable COPD. Changchun: Jilin University; 2021.
25. Shuiyuan X. The theoretical basis and research application of “social support rating scale”. J Clin Psychiatry. 1994;1994(2):98–100.
26. Quanquan D. Clinical validity of self-rating anxiety and depression scale. Chin J Ment Health. 2012;26(09):676–679.
27. Trostle JA. The history and meaning of patient compliance as an ideology. In: Gochman DS, editor. Handbook of Health Behavior Research II. Boston, MA: Springer; 1997.
28. Pehlivan E, Yazar E, Balcı A, Kılıç L. Comparison of compliance rates and treatment efficiency in home-based with hospital-based pulmonary rehabilitation in COPD. Turk Thorac J. 2019;20(3):192–197. doi:10.5152/TurkThoracJ.2019.18060
29. Van Genderen S, Plasqui G, Lacaille D, et al. Social role participation questionnaire for patients with ankylosing spondylitis: translation into Dutch, reliability and construct validity. RMD Open. 2016;2(1):e000177. doi:10.1136/rmdopen-2015-000177
30. Marengoni A, Vetrano DL, Manes-Gravina E, et al. The relationship between chronic obstructive pulmonary disease and frailty: a systematic review and meta-analysis of observational studies. Chest. 2018;154(1):21–40. doi:10.1016/j.chest.2018.02.014
31. Mccarron EP, Bailey M, Leonard B, et al. Improving the uptake: barriers and facilitators to pulmonary rehabilitation. Clin Respir J. 2019;13(10):624–629. doi:10.1111/crj.13068
32. Zhu Y, Mao Y, Sun Y, et al. The compliance and efficacy of out-of-hospital rehabilitation in patients with chronic obstructive pulmonary disease. Chin J Gerontol. 2012;32(24):5403–5404.
33. Olivia T, Saravana K, Kylie J. Barriers to and enablers of Physical activity in Patients with COPD following a hospital admission: a qualitative study. Int J COPD. 2014;9:115–128. doi:10.2147/COPD.S54457
34. Sabit R, Griffiths TL, Watkins AJ, et al. Predictors of poor attendance at an outpatient pulmonary rehabilitation program. Respir Med. 2008;102(6):819–824. doi:10.1016/j.rmed.2008.01.019
35. Cote CG, Celli BR. Pulmonary rehabilitation and the BODE index in COPD. Eur Respir J. 2005;26(4):630–636. doi:10.1183/09031936.05.00045505
36. Li Y, Li Y. Comparison of pulmonary rehabilitation time compliance and influencing factors in COPD patients in different periods Analysis. Tianjin Pharm. 2016;44(07):917–920.
37. Caixia K, Shouqian C, Xiu L, et al. Study on the correlation between anxiety, depression and social support in COPD patients. Gen Nurs. 2021;19(12):1684–1688.
38. Miguel Diez J, Hernandez Barrera V, Puente Maestu L, et al. Prevalence of anxiety and depression among chronic bronchitis patients and the associated factors. Res Pirol. 2011;16(7):1103–1110.
39. Zang F, Jiang X, Wang W. Effects of chronic obstructive pulmonary disease with hypoxemia on cognitive dysfunction. China J Pract Neuroll Dis. 2018;21(19):2114–2117.
40. Pierobon A, Sini BE, Ranzini L, et al. COPD patients’ self-reported adherence, psychosocial factor and mild cognitive impairment in pulmonary rehabilitation. Int J Chron Obstruct Pulmon Dis. 2017;12:2059–2067. doi:10.2147/COPD.S133586
41. Yao L, Zhao X, Zhao Y. Influencing factors of family rehabilitation compliance in patients with stable moderate to severe COPD. J North China Univ Sci Technol. 2018;20(3):205–209.
42. Gloeckl R, Schneeberger T, Jarosch I, et al. Pulmonary rehabilitation and exercise training in chronic obstructive pulmonary disease. Dtsch Arztebl Online. 2018;115(8):117–123.
43. Sandoz J, Roberts M, Cho J-G, et al. Magnitude of exercise capacity and quality of life impreovement following repeat pulmonary rehabilitation in patient with COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:1085–1091. doi:10.2147/COPD.S131778
44. Burkow TM, Vognild LK, Johesen E, et al. Promoting exercise training and physical activity in daily life: a feasibility study of a virtual group intervention for behaviour change in COPD. BMC Med Inform Decis Mak. 2018;18(1):136. doi:10.1186/s12911-018-0721-8
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Effects of Cognitive Training in Healthy Community Residing Thai Elderly: A Randomized Controlled Trial
Phanasathit M, Nimnuan C, Lohsoonthorn V
Psychology Research and Behavior Management 2022, 15:3709-3720
Published Date: 20 December 2022
Adherence to Atrial Fibrillation Better Care (ABC) Pathway Management of Chinese Community Elderly Patients with Atrial Fibrillation: A Cross-Sectional Study
Zhang X, Huang J, Weng F, Wen Y, Wang X, Jiang J, Xue Y, Li K
Patient Preference and Adherence 2023, 17:1813-1823
Published Date: 25 July 2023
Clinically Important Deterioration (CID) and Ageing in COPD: A Systematic Review and Meta-Regression Analysis According to PRISMA Statement
Manzetti GM, Ora J, Sepiacci A, Cazzola M, Rogliani P, Calzetta L
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2225-2243
Published Date: 10 October 2023
Exploring the Impact of Adequate Energy Supply on Nutrition, Immunity, and Inflammation in Elderly Patients with Chronic Obstructive Pulmonary Disease
Gao H, Cheng X, Zuo X, Huang Z
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:1391-1402
Published Date: 19 June 2024