Back to Journals » Journal of Pain Research » Volume 19
The Effectiveness of Child Life Services in Reducing Pediatric Procedural Pain: A Systematic Review and Three-Level Meta-Analysis
Authors Zhu L, Wang Z, Zhou Z, Ma Z, Dang Q, Fu C, Duan W ![]()
Received 24 December 2025
Accepted for publication 5 July 2026
Published 15 July 2026 Volume 2026:19 588505
DOI https://doi.org/10.2147/JPR.S588505
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Helen Koechlin
Liqin Zhu,1 Zichuan Wang,2 Zihan Zhou,2 Ziqian Ma,2 Qiong Dang,2 Cangcang Fu,1 Wenjie Duan2
1Department of Nursing, Children’s Hospital of Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China; 2Department of Social Work, School of Social and Public Administration of East China University of Science and Technology, Shanghai, People’s Republic of China
Correspondence: Wenjie Duan, Department of Social Work, School of Social and Public Administration of East China University of Science and Technology, 130 Meilong Road, Xuhui District, Shanghai, 200237, People’s Republic of China, Email [email protected] Cangcang Fu, Department of Nursing, Children’s Hospital of Zhejiang University School of Medicine, 3333 Binsheng Road, Binjiang District, Hangzhou, 310052, People’s Republic of China, Email [email protected]
Purpose: To examine the effectiveness of Child Life Services (CLS) in reducing procedural pain among pediatric patients.
Patients and Methods: A registered systematic review and three-level meta-analysis of randomized controlled trials (RCTs) and quasi-experimental studies was conducted following PRISMA 2020 guidelines. Six databases were searched from inception to 2 June 2025. Eligible studies included RCTs comparing CLS with standard care in children aged 0– 18 years undergoing medical procedures. Risk of bias was assessed using RoB 2 for RCTs and ROBINS-I for quasi-experimental studies. Pooled standardized mean differences (Hedges’ g) were estimated using three-level random-effects model. Four categorical moderators were examined: measurement timing, age group, procedure type, and assessor type.
Results: Twelve studies (N = 1,366) were included. CLS significantly reduced procedural pain compared with standard care (g = − 0.72, 95% CI [− 1.19, − 0.24], p =0.007). Heterogeneity was primarily attributable to between-study differences (Level 3 I2 = 85.0%). Assessor type was the only significant moderator (F = 8.68, p =0.008). Within-level analyses revealed that CLS produced significant pain reduction among children 7 years and younger (g = − 0.81, p =0.018), during one-time injections (g = − 0.93, p =0.021), and in post-procedure assessments (g = − 0.66, p =0.027). The overall finding was robust across sensitivity analyses, and no evidence of publication bias was detected.
Conclusion: CLS demonstrates a significant effect in alleviating procedural pain in children. Self-reported pain outcomes show better effects than observer-rated outcomes. While the benefits appear particularly pronounced among younger children and one-time injections, the evidence for older children and surgical contexts warrants further investigation.
Keywords: non-pharmacological intervention, systematic review, three-level meta-analysis, Child Life Services, procedural pain, pediatric
Introduction
Procedural pain is a form of brief, acute pain caused by medical procedures.1,2 As a time-limited condition, it is expected to resolve spontaneously once the inciting stimulus is removed.3,4 The assessments of procedural pain often concentrated in the first 24 hours when intensity is typically highest.5 For non-pharmacologic interventions, pain relief often occurs during or immediately after the intervention.6 Procedural pain is experienced by 68.4% of critically ill ICU patients, and it is often undertreated.7 A similar burden exists in surgical settings, where 82% of patients report postoperative procedural pain.8
Children are similarly affected. Neonates in intensive care units undergo 11.4 painful procedures per day. The frequent procedures include venipuncture, heel lance, and peripheral venous catheter insertion.9 Despite this high frequency, procedural pain in children remains poorly recognized. A study of 242 preterm neonates found that across 10,469 painful procedures, only 32.6% had a documented pain score and only 58.5% received pain-relieving interventions.10 The consequences of this gap extend well beyond the immediate procedure. The neonatal nervous system is developing, repeating painful procedures can lead to lasting harm, such as a reduction in thalamic volume and damage to white matter pathways. These changes can lead to poorer cognitive and motor skills in later years.11 If early pain is not treated, it can also change how children experience pain later on. Those who undergo more painful procedures are more likely to be overly sensitive to pain and have higher levels of pain-related anxiety as teenagers.12 Inadequate pain relief during childhood is further linked to needle phobia and healthcare avoidance, behaviors that compound long-term morbidity.13 As a result, managing pediatric procedural pain is important.
Clinicians use pharmacological and non-pharmacological interventions to reduce procedural pain in children. Non-steroidal anti-inflammatory drugs (NSAIDs) are mostly used to relieve mild pain, while opioids are mostly for the treatment of moderate to severe pain.14 The evidence from meta-analysis indicates that NSAIDs (ibuprofen and acetaminophen) could reduce acute procedural pain in children.15 For children over 6 months of age, intranasal fentanyl at 1.5 to 2 μg/kg provides rapid analgesia.16,17 However, pharmacological treatments are often limited by side effects. Ibuprofen was implicated in 68.6% of 51 reviewed pediatric gastrointestinal bleeding cases.18 NSAIDs are also an important cause of acute kidney injury in children.19 A scoping review indicates that severe neurological impairment is a risk factor for opioid-induced respiratory depression in pediatric patients.20
Non-pharmacological interventions offer a complementary route. A meta-analysis of 3,394 children found that distraction, hypnosis, and combined cognitive behavioural intervention reduced needle-related pain and distress.21 A randomized pilot study assessed a 15-minute medical clown intervention during pediatric IV cannulation. This humor-focused distraction approach lowered 3 to 7-year-olds’ Faces Pain Scale scores from 3.3 to 1.6.22 Distraction redirects attention away from threatening stimuli. Music, videos, and interactive games are common delivery formats.23 But these non-pharmacological methods face practical constraints. Heavy workloads and child non-cooperation were frequently cited barriers for nurses to implementation.24 In prehospital settings, short transfer times preclude most techniques.25 Many psychological techniques presuppose cognitive maturity and require structured pre-procedure training before they yield benefit.6 Developmental heterogeneity also creates difficulty. Children with cerebral palsy may smile or freeze in response to pain rather than showing typical distress cues, making assessment unreliable.26
In response to these implementation limitations of non-pharmacological interventions, Child Life Services (CLS) offer a systematic solution.27 These services were typically led by Certified Child Life Specialists (CCLS). They were required to hold at least a bachelor’s degree, complete a set of required coursework, 600 hours of supervised clinical internship, and pass a standardized certification examination.28 Where full-time staffing is not feasible, the American Academy of Pediatrics recommends part-time or consultative CCLSs to train existing healthcare personnel.29 In procedural pain contexts, CLS typically involves four components: (1) age-appropriate pre-procedural explanation and expectation-setting; (2) individualized distraction during the procedure (e.g, music, games, electronic devices, or bubbles); (3) caregiver coaching in coping strategies;29,30 and (4) post-procedural emotional debriefing.31 In one pediatric RCT, children who received CLS showed significantly lower CHEOPS pain scores than those in standard care. This result indicates that CLS can meaningfully reduce procedural pain.32 Another RCT examined CCLS-led virtual reality distraction during pediatric vaccinations. Children in the intervention group showed fewer pain behaviors based on caregiver and observer ratings.33 One scoping review gives a broader picture of how CLS has been studied across health care settings. This scoping review showed that the number of research publications related to CLS has increased dramatically over the past decade, with more than 50% of the included studies published from 2019 onward. But the intervention content, provider training, clinical setting, and outcome measurement all varied substantially.31 One systematic review included 4 CLS-related RCTs, confirming that CLS can improve pain, anxiety and stress outcomes related to pediatric procedures.30 But all four RCTs carried a medium to high risk of bias. Taken together, the available evidence supports the application of CLS to procedural pain. But researchers need to further integrate its actual intervention effect.
Existing evidence on CLS for pediatric procedural pain shows substantial variation. First, procedural pain responses in children vary widely with age. For 80 children aged approximately 7 years undergoing limb fracture surgery, CLS lowered the FLACC pain score upon return to the ward by 0.71 points compared with control group.34 In contrast, among 100 children aged approximately 8 years undergoing the same type of surgery, the FLACC pain score differed by only 0.13 points.35 Second, pain assessment instruments also contribute to heterogeneity. For 240 preschool children with chronic kidney disease undergoing venipuncture, researchers measured pain with both a self-report scale and an observer-rated scale. The self-reported Wong-Baker FACES score was 3.16 in the CLS group versus 5.98 in the control group. The observer-rated FLACC score was 3.42 in the CLS group versus 5.34 in the control group.36 While both scales detected a statistically significant between-group difference favoring the CLS group, the magnitude of the difference was descriptively larger on the self-report measure than on the observer-rated measure. Third, procedural types introduce further variability. When 77 children received peripheral intravenous punctures, the intraoperative FLACC pain score was 2.5 points lower than the control.37 Conversely, among 130 children undergoing concealed penis surgery, the FLACC score at 6 hours postoperatively was only 0.23 points lower in the CLS group.38 Fourth, the timing of assessment is equally critical. For 100 children undergoing renal biopsy, the intraoperative Faces Pain Scale-Revised (FPS-R) score was 1.5 points lower than the control.39 In contrast, during the post-procedural phase for 121 immunized children, the median FPS-R score showed no statistical difference between the intervention and control groups.40 Considering these sources of heterogeneity, researchers will perform subgroup analyses to robustly estimate the effects of Child Life Services on pediatric procedural pain.
To fill these gaps, this study used a three-level meta-analysis to quantify the overall analgesic effect of CLS on pediatric procedural pain. Four moderators were prespecified to examine whether the effect varied by measurement timing, age group, procedure type, and assessor type. The findings are expected to provide quantitative support for better integrating CLS into multidisciplinary pediatric pain care.
Materials and Methods
Design and Registration
This study was designed as a systematic review and three-level meta-analysis of randomized controlled trials (RCTs) and quasi-experimental studies, conducted in accordance with the Cochrane Handbook for Systematic Reviews of Interventions (Version 6.5).41 The protocol and reporting followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 (PRISMA 2020) guidelines.42 The review was prospectively registered with PROSPERO, the international database of prospectively registered systematic reviews, hosted by the Center for Reviews and Dissemination, United Kingdom (Registration Number: CRD420251020624).
Search Strategy
To ensure comprehensive evidence coverage, a structured search strategy was developed and refined iteratively by the review team. Initial search terms included “child life” and “pain”, and were refined using keywords extracted from relevant articles. Final terms were developed in accordance with the PICOS framework (Population, Intervention, Comparison, Outcome, and Study design) and finalized upon approval by three researchers. The approved terms included “child*”, “procedure*”, “child life”, “pain”, and “randomized controlled trial”.
Six widely recognized digital academic databases were searched: China National Knowledge Infrastructure, Wanfang Data, Web of Science, PubMed, Scopus, and Embase. The final search was conducted on 2 June 2025. To minimize publication bias, a manual search was also performed using Google Scholar and the reference lists of included studies. A summary of database-specific strategies is presented in Box 1, with full search terms provided in Supplementary Table 1.
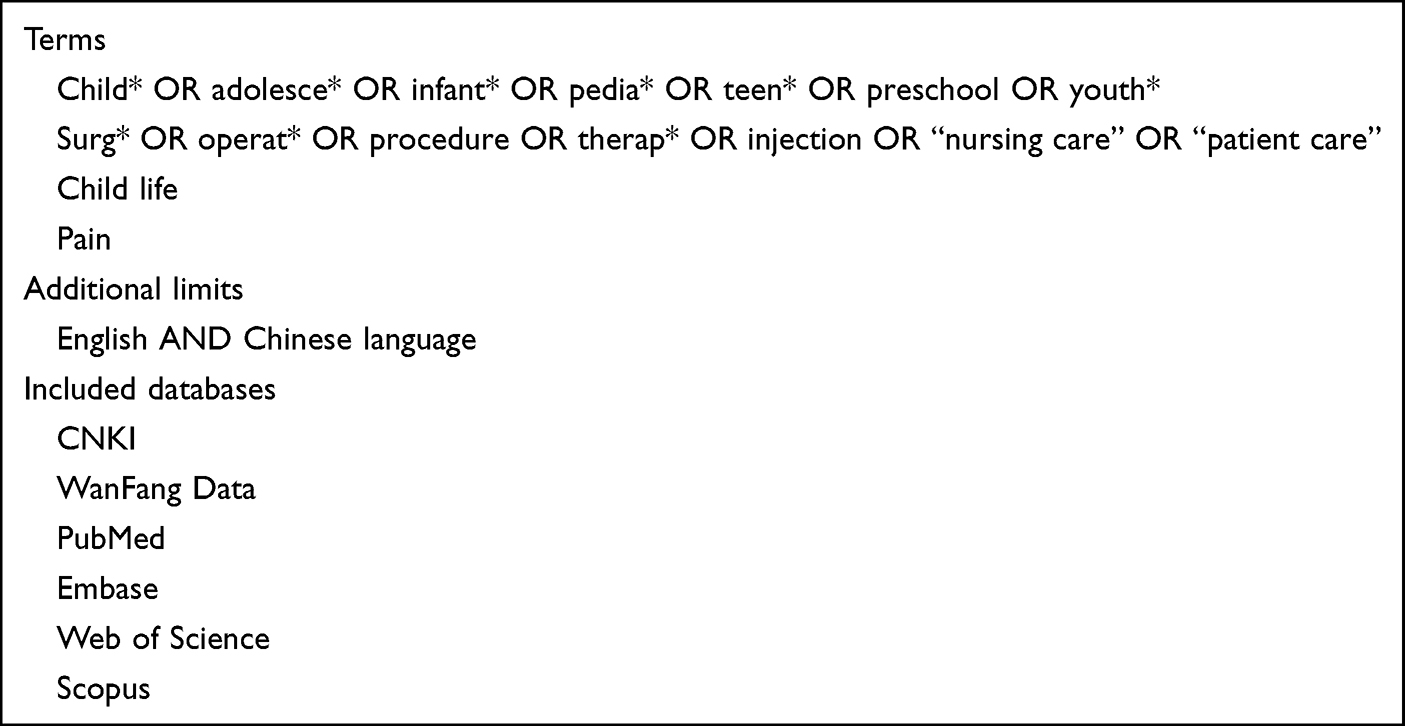 |
Box 1 Literature Search of the Electronic Databases |
Inclusion and Exclusion Criteria
Studies were considered eligible if: (1) the recipients of the interventions were pediatric patients aged 0–18 years old; (2) the intervention consisted of Child Life Services, defined as non-pharmacological interventions delivered by trained professionals and incorporating therapeutic play, medical preparation, distraction, psychological support, and family support as core components;29 (3) the control group received routine or standard care; (4) the pain in pediatric patients was assessed using psychometric scales, objective measures, and scientifically validated tools (e.g, FLACC, CHEOPS, VAS, FPS-R, WBFS); (5) the study design was an RCT or quasi-experimental design (e.g, historical control, non-concurrent control); and (6) the publication was in Chinese or English.
Studies were excluded if they met any of the following criteria: (1) the intervention did not consist of CLS, or contained multiple intervention components in which the effect of CLS could not be isolated; (2) it could not be reliably determined whether pain was assessed within 24 hours after the procedure or surgery. Because acute procedural pain peaks early and resolves spontaneously,1,5 pain measured beyond this window may reflect natural recovery rather than the intervention effect. (3) the data required for effect size calculation were incomplete or unusable; (4) the publication was a review, case report, or conference abstract.
Screening
All records retrieved at that time are included in the screening process. After that, all retrieved records were imported into EndNote 19 software,43 and duplicates were removed. Followed by the eligibility criteria set at the beginning of the research, two reviewers (Z. Zhou and Z. Wang) independently screened the titles and abstracts and discussed the differences in the results till reaching consensus. Subsequently, full-text screening of studies for basic inclusion and exclusion criteria was performed. If there were some different opinions, the full-text articles were discussed. If necessary, a third senior researcher (W. Duan) was consulted.
Risk of Bias Assessment
Risk of bias was assessed using design-appropriate tools. For randomized controlled trials, this study utilized the Revised Risk of Bias (RoB 2) tool to evaluate the risk of bias of the included studies. The assessment targeted the following domains: (1) bias arising from the randomization process, to assess whether the allocation sequence was random and concealed, (2) bias due to deviations from intended interventions, to assess whether awareness of the assigned intervention led participants or providers to deviate from the intended treatment, (3) bias due to missing outcome data, (4) bias in measurement of the outcome, to minimize detection bias, (5) bias in selection of the reported result, to identifyselective reporting. The risk of bias was categorized into three levels:44 (1) low risk: the study provided clear, detailed reporting and implemented robust measures to minimize bias effectively, (2) some concerns: the study raised some concerns in at least one domain but was not judged to be at high risk for any domain, (3) high risk: inadequate methods were employed in specific domains, introducing a substantial risk of systematic bias and potentially compromising the reliability of the findings.
For quasi-experimental studies, the Risk Of Bias In Non-randomised Studies of Interventions (ROBINS-I) tool was employed,45 which evaluates bias across seven domains: (1) bias due to confounding, to assess whether the estimated effect of the intervention is distorted by baseline differences between groups; (2) bias in selection of participants into the study, to evaluate whether selection into the study was related to both the intervention and the outcome; (3) bias in classification of interventions, to determine whether intervention status was misclassified or differentially defined across groups; (4) bias due to deviations from intended interventions, to assess whether systematic differences in how interventions were delivered, co-interventions administered, or adherence monitored introduced bias; (5) bias due to missing data, to evaluate whether incomplete outcome data, loss to follow-up, or exclusion of participants differed between groups and was related to the outcome; (6) bias in measurement of outcomes, to assess whether the method of outcome assessment, including the subjectivity of the measure and blinding of assessors, introduced systematic error; (7) bias in selection of the reported result, to evaluate whether the reported outcomes were selected from multiple measurements or analyses on the basis of the results.
The risk of bias under ROBINS-I was categorized into five levels45: (1) low risk: the study is comparable to a well-performed randomized trial across all domains; (2) moderate risk: the study is sound for a non-randomized design but cannot be considered equivalent to a well-performed randomized trial; (3) serious risk: the study has important methodological problems that substantially weaken confidence in the findings; (4) critical risk: the study is too methodologically compromised to provide any useful evidence on the effect of the intervention; (5) no information: insufficient detail was reported to permit a judgment in one or more domains.
For each included study, the risk of bias assessment was independently performed by two reviewers (Z. Zhou and Z. Wang). Discrepancies were resolved through consultation with a third senior reviewer (C. Fu). Her expert input facilitated consensus. All differences were addressed via thorough discussion to ensure agreement.
Data Extraction
Data extraction was performed by one reviewer using a pre-designed table based on the Cochrane Handbook,46 and another reviewer verified the accuracy of the extracted data. The extracted data encompassed several key categories: (1) author, year/country, (2) study design, (3) characteristics of pediatric patients, (4) intervention characteristics, (5) assessment parameters, (6) pain measurement tool and data. Data were subsequently entered into Review Manager 5 by one author, who carefully checked for completeness and accuracy. To ensure data comparability, for studies reporting only individual dimensional scores, the mean and standard deviation of the total score were calculated before meta-analysis. When studies reported only medians and quartiles, these were converted to means and standard deviations using the recommended statistical formula47 Mean ≈ (Q1 + M + Q3)/3; SD ≈ IQR / (2 × Φ−1((0.75n − 0.125)/(n + 0.25))).
Data Synthesis
All meta-analyses were conducted in R 4.4.3 using the metafor package.48 This study employed standardized mean differences (SMD; Hedges’ g) and a random-effects (RE) model to quantify the effect size of the CLS on children’s pain levels during procedures. Hedges’ small-sample correction was applied.49 The interpretation of Hedges’ g adhered to Cohen’s criteria, where effect sizes of 0.2, 0.5, and 0.8 were classified as small, medium, and large, respectively. Cohen’s conventional benchmarks have been adopted for interpreting standardized mean differences in systematic reviews of pediatric procedural pain.21,41 Negative values indicating lower pain in the CLS group.
Given that multiple effect sizes were nested within the same study, and traditional meta-analytic models assuming independence among effect sizes would produce inflated precision and inflated Type I error rates.50 So all pooled analyses employed a three-level random-effects model with nested random intercepts for individual effect sizes within studies, estimated via restricted maximum likelihood (REML).51 The three variance levels comprised: Level 1 (sampling error), Level 2 (within-study variance), and Level 3 (between-study variance). Significance testing used the Knapp-Hartung method with t-tests.52 Heterogeneity was assessed using the I2 statistic, interpreted as follows: 0–40% represented unimportant heterogeneity, 30–60% moderate heterogeneity, 50–90% substantial heterogeneity, and 75–100% considerable heterogeneity. If substantial heterogeneity was detected we performed moderator analyses to identify its sources. Likelihood-ratio tests (LRTs) were conducted to evaluate whether the three-level model provided a significantly better fit than simpler two-level alternatives.51 For comparison, a conventional two-level random-effects model was also fitted.
Four categorical moderators were examined in this study: (1) timing of assessment (during-procedure vs post-operative). We confirmed with our team of clinically experienced experts that measurements within 24 hours after the procedure can effectively reflect the effectiveness of the intervention. Additionally, many studies on procedural pain also used 24 hours as a time point.53 (2) age group (≥ 8 vs ≤ 7 years). Around 7 to 8 years of age, children typically begin to comprehend the nature of pain, enabling the effective use of self-report pain scales.54 Consequently, this study categorizes children into two groups based on the age threshold of eight years. (3) procedure type (surgery vs one-time injection) The intensity of pain is closely related to the invasiveness of the operation. One-time injections and surgical procedures represent the spectrum of low-invasive and high-invasive interventions, respectively. Surgical procedures are characterized by greater intensity and prolonged duration compared to one-time punctures.55 (4) assessor type (observer-rated vs self-report). For each moderator, per-level pooled effect sizes with 95% confidence intervals were estimated, and omnibus F-tests assessed whether the moderator significantly accounted for heterogeneity. Potential outliers were identified using externally studentized residuals (|rstudent| > 1.96 indicating a potential outlier).56 After finding those potential outliers, this study used Leave-one-study-out analyses to evaluate whether any single study exerted disproportionate influence on the overall conclusion. If the pooled estimate remained significant after sequentially excluding each study, the result was considered robust.
Publication bias was assessed visually using funnel plots and Egger’s regression test. If the funnel plot appeared symmetric and Egger’s regression test was non-significant,57 publication bias was considered unlikely. If the funnel plot displayed asymmetry or Egger’s test reached significance, the trim-and-fill procedure58 was applied to estimate the number of potentially missing studies and to provide a bias-adjusted pooled estimate; if the adjusted estimate did not differ substantially from the original, the meta-analytic result was considered robust to publication bias.
Results
Study Selection
This study retrieved 4,167 records from six Chinese and English databases and imported them all into EndNote 19. After removing 131 duplicates and manual screening, the remained 4,036 articles were reviewed for titles and abstracts. Titles and abstracts of all 4,036 articles were reviewed by two researchers. If there are some controversial records, the expert will be queried. 3,996 articles were excluded based on title, and 17 articles were excluded based on abstract.
Subsequently, the two researchers independently read the 23 articles that met the full-text screening criteria, of which 11 articles were excluded for the following reasons: incomplete data (n = 7), unable to accurately determine whether pediatric patients are within the scope of medical procedures (n = 2), wrong study type (n = 2). Finally, 12 articles that met the requirements were included, and the selection of studies is illustrated in a PRISMA flow diagram (see Figure 1).
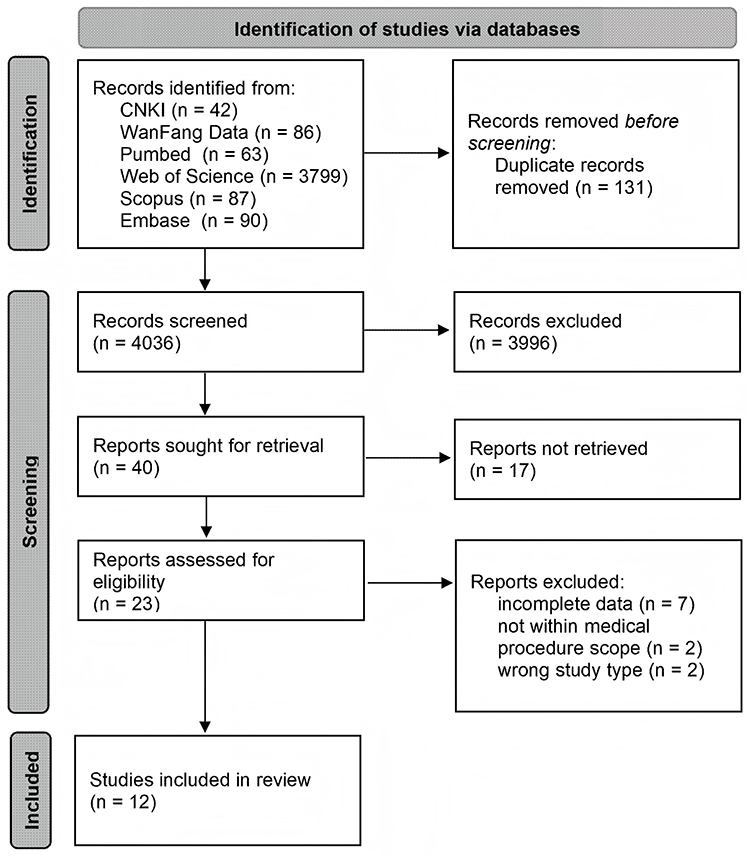 |
Figure 1 PRISMA flow diagram of study selection. |
Study Characteristics
Twelve studies (seven RCTs and five quasi-experimental design) published between 2015 and 2025 were included. These studies enrolled 1,366 participants. Nine were conducted in China,34–39,59–61 two in the United States,40,62 and one in Australia.32 Seven studies evaluated surgical interventions: burn wound dressing,32 limb fracture repair,34,35 concealed penis surgery,38 inguinal hernia surgery,59 cryptorchidism surgery,60 and multiple surgery.61 Five evaluated one-time injections: peripheral intravenous placement in the emergency,62 routine immunization,40 day-surgery peripheral venipuncture,37 venipuncture for chronic kidney disease,36 and renal biopsy.39 Details of each CLS intervention and control condition are provided in Supplementary Table 2.
These studies used five instruments to measure pain. FLACC was used in five studies.34–38 The Visual Analogue Scale (VAS) was used in two studies.59,60 The Faces Pain Scale–Revised (FPS-R),39,40 the Wong-Baker FACES Scale (WBFS),36,61,62 and the Children’s Hospital of Eastern Ontario Pain Scale (CHEOPS)32 each appeared in one or two studies. FLACC and CHEOPS are observer-rated scales. VAS, FPS-R, and WBFS are self-report scales. The 12 studies yielded 24 effect sizes. Study characteristics are summarized in Table 1.
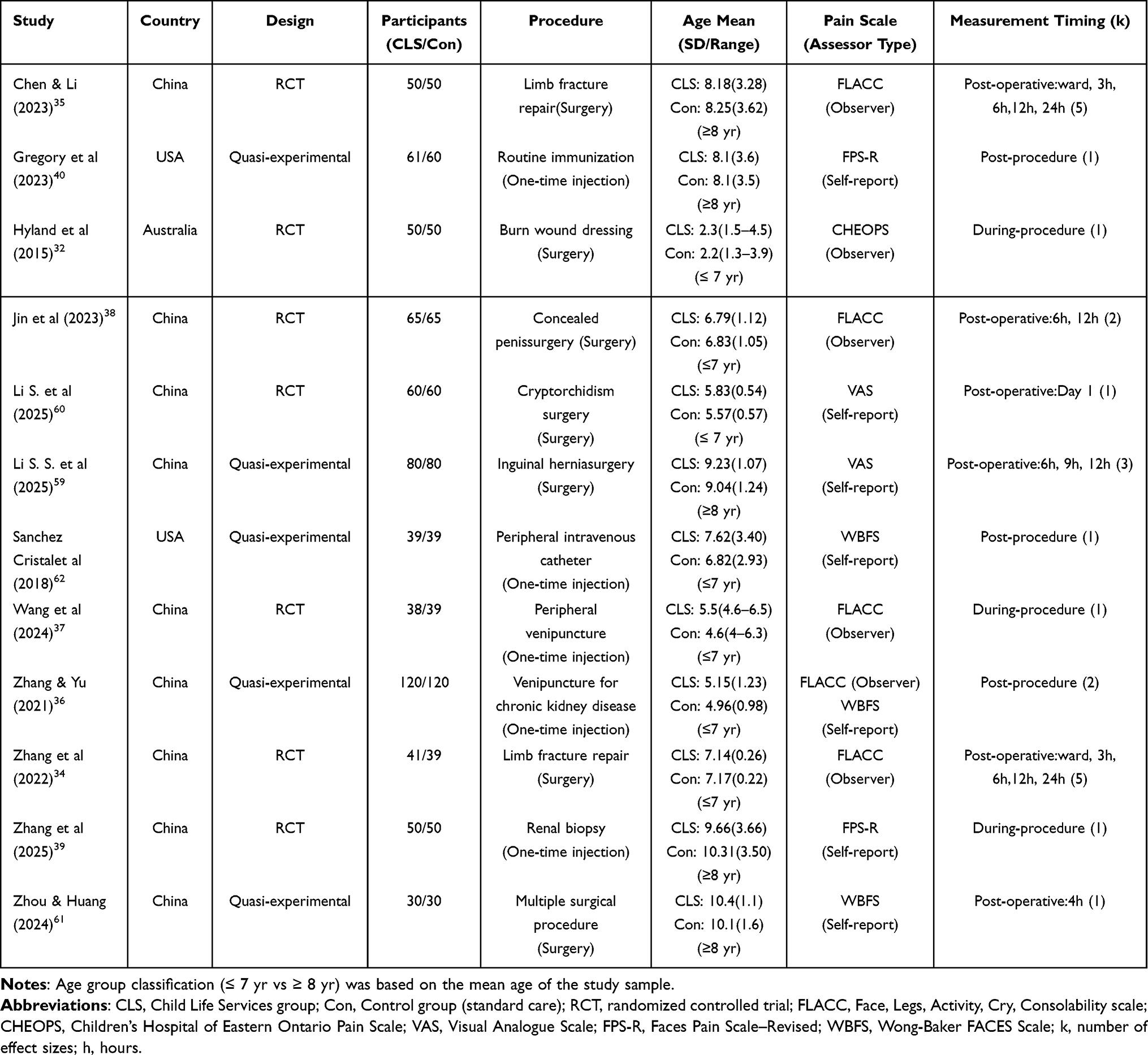 |
Table 1 Characteristics of Studies Included in the Meta-Analysis |
Risk of Bias Assessment
The risk of bias for each included RCT is detailed in Figure 2. Three were rated as having some concerns32,34,37 and four as high risk.35,38,39,60 The bias risk assessment showed that randomization process (Domain 1) had 85.7% low risk and 14.3% some concerns. Deviations from intended interventions (Domain 2) were uniformly rated as some concerns (100%). Unlike a pill or a cream, CLS requires a trained specialist to interact face-to-face with the child. The specialist knows they are delivering the intervention; the child and family also know whether someone is playing with them, and coaching them through the pain. Missing outcome data (Domain 3) and selective reporting (Domain 5) were rated as low risk in all seven RCTs. Measurement of the outcome (Domain 4) had 57.1% high risk and 42.9% low risk. Three studies deployed independent assessors and were rated low risk.32,34,37 Four studies that failed to explicitly mention a separate assessment team were classified as high risk.35,38,39,60 Detailed risk assessment charts for each study are presented in Figure 3.
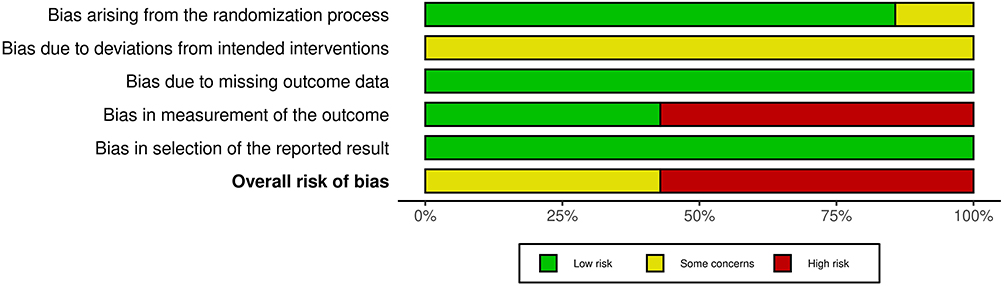 |
Figure 2 Risk of bias summary for randomized controlled trials (Cochrane RoB 2). |
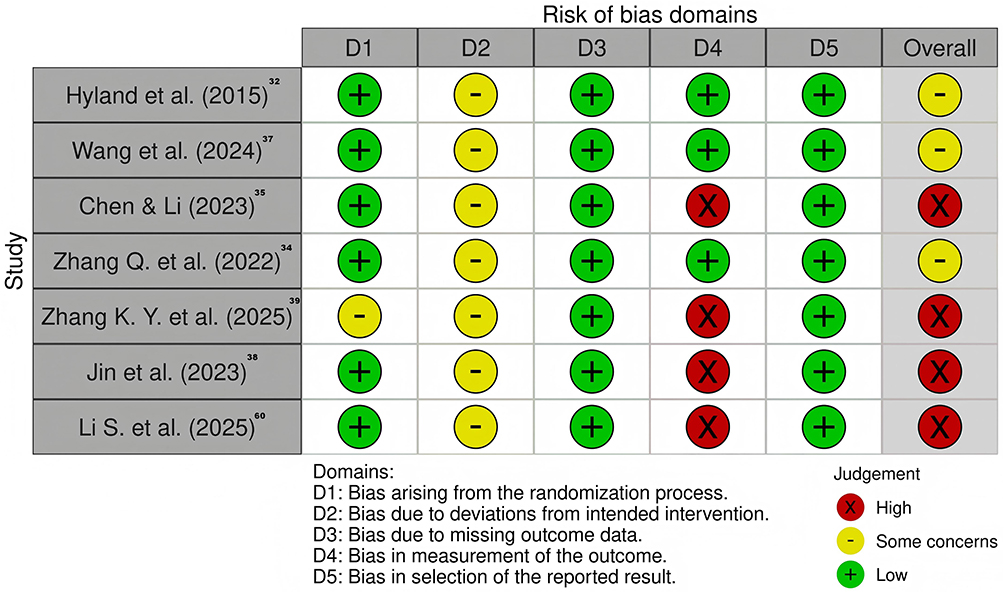 |
Figure 3 Risk of bias traffic light plot for randomized controlled trials (Cochrane RoB 2). |
The risk of bias for the five quasi-experimental studies is detailed in Figure 4. All five received an overall judgment of serious risk of bias (see Figure 5). The domain-level assessment showed that confounding (Domain 1) represented the main source of bias. Four studies (80%) were rated as serious risk and one (20%) as critical risk.61 None of the five studies employed true random assignment to groups. Selection of participants (Domain 2) was rated as low risk in three studies and moderate in two.61,62 Classification of interventions (Domain 3) was rated as low risk in four studies and moderate in one.61 Deviations from intended interventions (Domain 4) and missing data (Domain 5) were uniformly rated as low risk. Measurement of outcomes (Domain 6) was rated as moderate risk in four studies and serious risk in one.59 Because the pain was scored without an independent assessment team. Selection of the reported result (Domain 7) was rated as moderate risk across all five studies. Because they did not repert the published protocols or trial registrations.
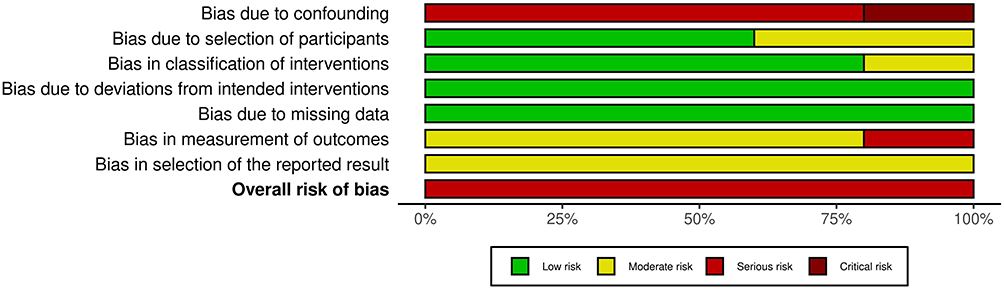 |
Figure 4 Risk of bias summary for quasi-experimental studies (ROBINS-I). |
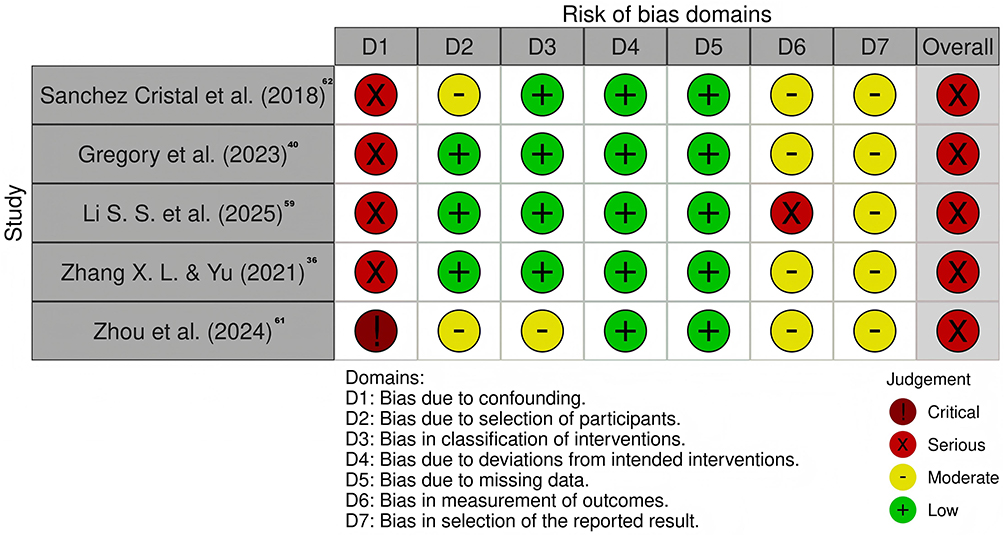 |
Figure 5 Risk of bias traffic light plot for quasi-experimental studies (ROBINS-I). |
Overall Effect of Child Life Services in Reducing Pediatric Procedural Pain
This study used three-level random-effects model to estimate the overall effect of CLS on procedural pain relative to standard care (Figure 6). The results showed that CLS produced a combined effect size of g = −0.72 (p =0.007, 95% CI [−1.19, −0.24]). By Cohen’s convention, this falls in the medium-to-large range, indicating that children who received CLS experienced substantially less procedural pain than those in standard-care control groups. Heterogeneity was substantial under the three-level model (Q(23) = 314.83, p <0.001). Likelihood-ratio tests were conducted to determine the distribution of heterogeneity across levels. The results showed that the within-study variance (Level 2 I2 = 8.1%, tau2 = 0.046, p =0.006), and the between-study variance (Level 3 I2 = 85.0%, tau2 = 0.485, p <0.001) both significant. Considerable heterogeneity was present at the between-study level (I2 > 75%), whereas within-study heterogeneity was unimportant (I2 < 40%).63 The between-study level accounted for the preponderance of the total variance, indicating that study-level characteristics, rather than within-study measurement choices, were the primary source of variability in CLS effectiveness. Therefore, moderator analyses were conducted to identify which study-level factors accounted for this heterogeneity.
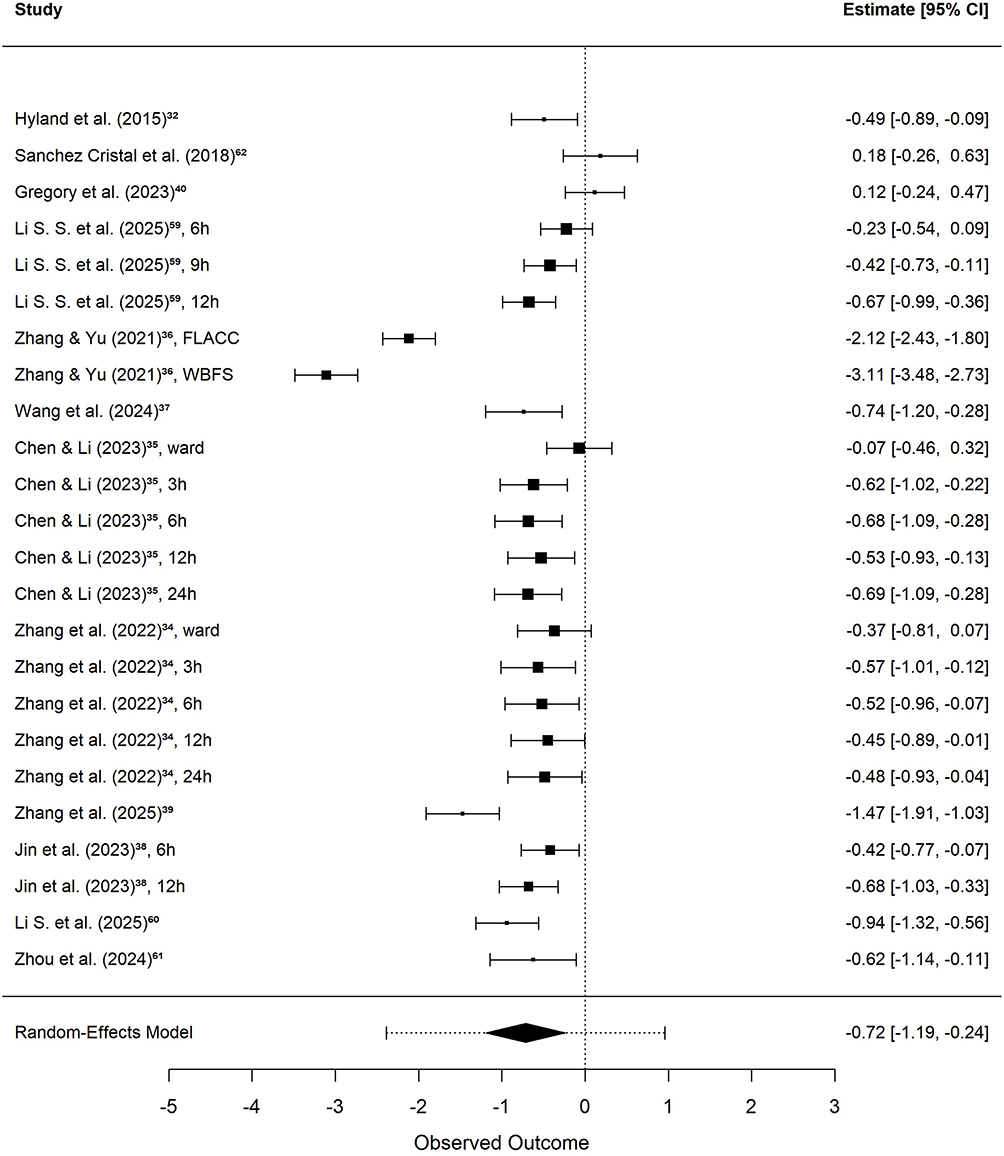 |
Figure 6 Forest plot of standardized mean differences (Hedges’ g) for the effect of CLS on pediatric procedural pain. |
Moderator Analyses
This study examined four categorical moderators: measurement timing, age group, procedure type, and assessor type. The results for each moderator are presented in Table 2. Only one moderator reached statistical significance, so we did not conduct a multiple moderator model.
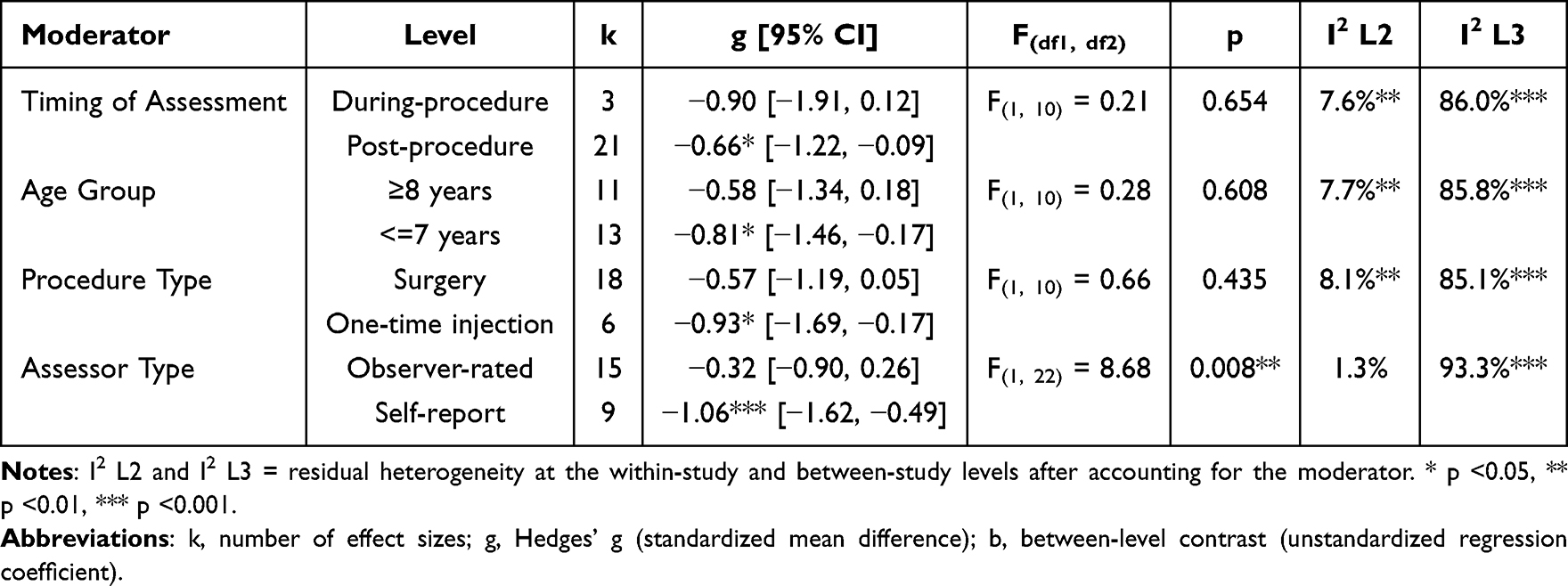 |
Table 2 Moderator Analysis of CLS Effects on Pediatric Procedural Pain |
Assessor type was a statistically significant moderator (F(1, 22) = 8.68, p =0.008). Self-report measures yielded a larger pooled effect (k = 9, g = −1.06, p <0.001) than observer-rated measures (k = 15, g = −0.32, p =0.261). This indicates that the observed benefit of CLS depends partly on who assesses the pain. When children rate their own pain, CLS shows a large and reliable effect.
Age group did not reach significance as a moderator (F(1, 10) = 0.28, p =0.608). The benefit of CLS did not change on whether children were younger or older. Children aged 7 years and younger showed a larger effect (k = 13, g = −0.81, p =0.018) than children aged 8 years and older (k = 11, g = −0.58, p =0.122). The within-group evidence is sufficient to conclude that CLS reduces pain in children aged 7 years and younger.
Procedure type was not a significant moderator (F(1, 10) = 0.66, p =0.435). CLS worked regardless of whether the procedure involved surgery or a one-time injection. One-time injections showed a larger effect (k = 6, g = −0.93, p =0.021) than surgery (k = 18, g = −0.57, p =0.069). The data confirm that CLS reduces pain in one time injections.
Measurement timing did not moderate the overall effect (F(1, 10) = 0.21, p =0.654). During-procedure assessments (k = 3, g = −0.90, p =0.077) yielded a larger effect than post-procedure assessments (k = 21, g = −0.66, p =0.027). The data confirmed that CLS reduces pain when measured after the procedure.
Sensitivity Analyses
Influence analysis identified one outlier from Zhang, Yu.36 To evaluate their impact, we conducted another meta-analysis without it. The leave-one-out results are presented in Figure 7. The three-level random model showed that the overall effect remained significant, g = −0.67 (p =0.003, 95% CI [−1.06, −0.27]). Because the change was modest, both were retained. Leave-one-study-out analyses showed that the pooled g ranged from −0.79 to −0.53 and remained significant at p <0.05 across all 12 iterations. In a conventional two-level model, the same outliers exerted a larger influence on the pooled estimate (g = −0.69 vs g = −0.72), illustrating the benefit of the three-level approach.
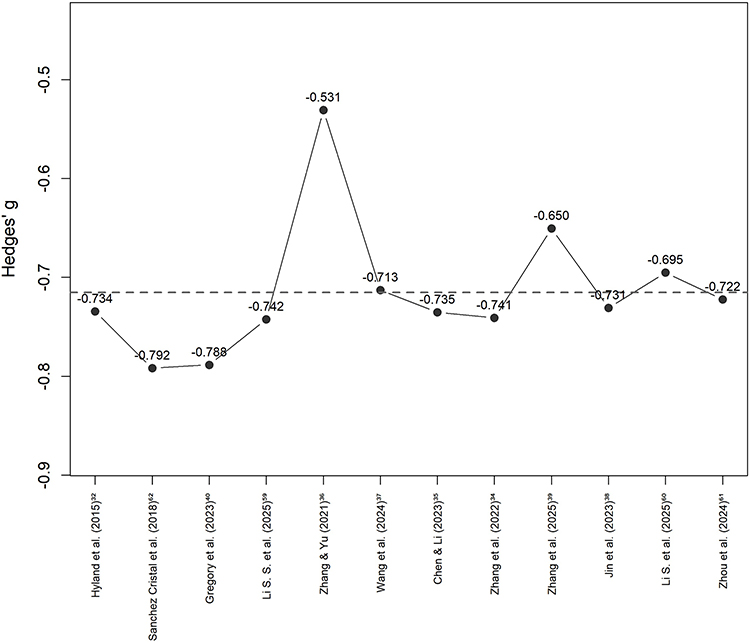 |
Figure 7 Leave-one-out sensitivity analysis plot. |
Publication Bias
The funnel plot (Figure 8) showed no marked asymmetry. The two-level Egger regression test was non-significant (t = 0.65, p =0.523). The three-level Egger test with a modified predictor was also non-significant (F(1, 10) = 3.18, p =0.105). The trim-and-fill procedure imputed seven studies to the left of the mean effect size. After correction, the overall effect size was still significant with g = −0.91 (p <0.001, 95% CI [−1.17, −0.65]). Rosenthal fail-safe N was 2,626, exceeding the threshold of 130. There was no statistical evidence to indicate the presence of publication bias.
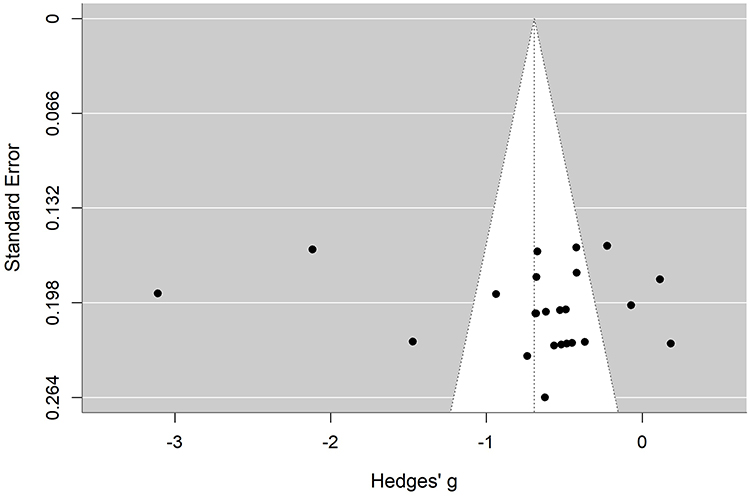 |
Figure 8 Funnel plot for assessment of publication bias. |
Discussion
Main Findings
This systematic review and three-level meta-analysis synthesized evidence from RCTs and quasi-experimental studies. The 24 effect sizes from 12 studies found that CLS significantly reduced pediatric procedural pain compared with standard care. The overall conclusion remaining robust across multiple sensitivity analyses. The benefit was clearest among younger children, during one-time injection procedures, at post-procedure time points, and when pain was assessed through child self-report. Compared with the prior systematic review of CLS,30 the present review quantifies the magnitude of that analgesic effect and identifies the conditions under which it varies. These results provide support for integrating CLS into pediatric medical care as a standardized, non-pharmacological pain management strategy.
Heterogeneity analyses revealed that variability in CLS effects predominantly originated at the between-study level (Level 3). This pattern suggests that study-level characteristics were primary sources of effect variation. Assessor type was the only prespecified moderator that significantly accounted for between-study variance. Age group, procedure type, and measurement timing did not reach significance as moderators. A recent scoping review documented that CLS intervention content, provider qualifications, and clinical settings vary widely across health care systems.31 The between-study heterogeneity observed in the present study converges with this observation, suggesting that residual variability partly reflects real differences in how CLS is implemented. Accordingly, we will discuss four moderators below.
Interpretation of Moderation
Assessor type was the only moderator that significantly influenced the CLS analgesic effect in this study. Child self report measures yielded a large pooled effect, whereas observer rated measures yielded a much smaller and non-significant effect. Observer rated tools such as FLACC measure what the child displays. Self report tools measure what the child feels. CLS deploys therapeutic play, psychological preparation, and coping skills training to target the child’s subjective experience. The child’s own pain report captures the endpoint most proximal to what CLS is designed to change. This finding aligns with the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT) consensus, which established self-reported pain intensity as a core outcome domain for pediatric acute pain clinical trials.64 The IASP 2020 definition of pain also explicitly affirmed that individual self report is irreplaceable in pain assessment.65 A meta analysis of 40 studies with 4,628 children likewise found instrument type to be a significant moderator of child to caregiver pain rating consistency.66 A systematic review of measurement properties for self-report pain intensity measures in children noted that self-report and behavioral observation scores are often discrepant.67 The present findings situate CLS within this broader measurement pattern. Future CLS studies and programs should adopt developmentally matched self-report instruments as the primary outcome. For children aged 6 years and older who can complete self-report, FPS-R carries the strongest current evidence.67 For children younger than 6 years, where no self-report measure has yet met the threshold for recommendation, observer-rated tools such as FLACC remain necessary.
Age did not significantly moderate the analgesic effect of CLS. Among children 7 and younger, the effect was large and was statistically significant. Among children 8 and older, it was moderate and did not reach significance. Within the included 12 studies, younger children were predominantly assessed with observer-rated tools, while older children more often contributed self-report data. Separating the developmental signal from measurement modality requires further evidence. A Cochrane review of psychological interventions for needle-related procedural pain in children similarly noted that age and developmental stage are important considerations when selecting outcome measures, but did not formally test age as a moderator.21 The developmental literature offers a framework for understanding how CLS function across age groups.68–70 Young children cannot regulate emotions well on their own. Their prefrontal cortex remains immature throughout early and middle childhood. They depend on others to soothe and structure the experience of pain. CLS supplies external preparation, distraction, and coaching that younger children cannot yet generate for themselves. Older children are learning to manage distress internally. Cognitive reappraisal and attention direction emerge gradually. They bring partial self-regulation capacity to the medical encounter. So the extra benefit CLS offers therefore be smaller. For younger children, future CLS programs should rely on dolls, pretend medical equipment, and sensory familiarization, with caregivers serving as co-regulators. For older children, the same hands-on methods should be paired with verbal explanation, and children should be invited to plan their own coping strategies. Studies in each age band should collect self-report and observer-rated data in parallel.
Measurement timing did not significantly moderate the analgesic effect of CLS. In the post procedure period, the pooled effect was moderate and statistically significant. In the during procedure period, the point estimate was larger but did not reach significance. Only three studies contributed during procedure data, so it was severely under-powered. The point estimate was large, which suggests that CLS may be doing something meaningful during the procedure. The non-significance could be explained by the difficulty of measuring pain in the procedure room. Pain tools need to be validated for the specific setting where they are used. A tool that works well after surgery may not work the same way during a procedure.71 The during-procedure window also has a signal-to-noise problem. Acute pain, fearful crying, and physiological arousal all peak within seconds. In that moment, it is hard to tell them apart by watching behavior alone. Even devices built for continuous nociception monitoring during surgery give mixed results.72 Distraction as a standalone intervention provides a benchmark for during-procedure effects. A meta-analysis of distraction for invasive procedures in children found that distraction produced a large analgesic effect when measured during the procedure.73 Distraction is the part of CLS meant to work during the procedure. Its effect depends a lot on whether it fits the timing and nature of the procedure.74 So the key CLS ingredient in this phase is itself highly context-dependent, which only adds to the measurement difficulty. A recent meta-analysis of psychosensory interventions in pediatric emergency departments similarly reported that several strategies produced significant post-procedure reductions in heart rate and blood pressure but showed no significant effects on the same physiological markers during the procedure.75 Future studies should treat during-procedure and post-procedure assessment as distinct measurement tasks. For each phase, the pain tool should be selected and validated for that specific context.
Procedure type did not significantly moderate the analgesic effect of CLS. Among one time injections, the effect was large and reached statistical significance. Among surgical procedures, the effect was moderate but did not reach individual significance. A systematic review of psychological interventions for pediatric surgical post-operative pain classified interventions into preparation/education, distraction/imagery, and mixed. It found that preparation/education did not significantly reduce child self-reported pain whereas distraction/imagery was effective. Mixed interventions were excluded from subgroup analyses because they could not be uniquely categorized into a single subgroup.76 CLS is a multicomponent care model encompassing therapeutic play, psychological preparation, and pain-management and coping strategies, with distraction listed as a standard component of pain-management and coping strategies.29 CLS thus contains both a preparation component and a distraction component and corresponds to the mixed category. In injection studies, CLS delivered real-time during-procedure distraction in addition to pre-procedural preparation, and distraction is a widely validated non-pharmacological strategy in pediatric procedures.74 In surgical studies, preoperative CLS preparation content was comparable to that in one time injection studies, but the real-time during-procedure component was absent. Surgical children also received systemic analgesia as part of standard care, and pain scores in this context may be compressed to a low range where scale sensitivity to additional improvement is limited.77 The IMMPACT consensus recommends that pediatric pain assess global treatment satisfaction, physical recovery, and emotional response as core outcome domains in addition to pain intensity.64 Future surgical CLS studies should consider multidimensional assessment to better capture the true clinical value.
Limitation
Several considerations should be taken into account when interpreting the findings. First, the number of eligible studies was constrained by the developmental stage of the CLS field. Over 50% of CLS research has been published in the past five years.31 The elevated risk of bias in the included literature reflects the methodological maturity of a field still in its early accumulation phase. The inherent challenges of blinding in behavioral interventions are common across this evidence base.30 Second, the included studies were heavily concentrated in China. This geographical distribution reflects the uneven global development of CLS, and cross-cultural validation is a necessary next step. Third, only categorical moderators were examined. Continuous variables such as intervention duration and CCLS experience could not be analyzed because the primary studies did not report them consistently. Future CLS research should report the duration of each intervention session, the total number of sessions, the professional background and years of experience of the individual delivering the intervention. Fourth, none of the included studies systematically monitored adverse effects of CLS. While CLS is a low-risk behavioral intervention, the absence of safety data limits comprehensive risk-benefit evaluation.
Conclusion
This systematic review and three level meta analysis demonstrates that Child Life Services significantly reduce procedural pain in pediatric patients. Assessor type is the sole significant moderator. Effects based on child self report are substantially larger than those based on observer ratings, and the latter have not yet reached statistical significance. Age group, procedure type, and measurement timing did not significantly moderate CLS effects. However, within level analyses suggest benefits for younger children and one time injections, though the age-group difference was not statistically confirmed. These non-significant findings require cautious interpretation given the limited statistical power and potential confounding with assessor type. Overall, CLS demonstrates clear clinical value in pediatric procedural pain management. Certified child life specialists should be integrated into multidisciplinary pediatric pain teams. Future CLS research should anchor primary outcomes on developmentally matched self-report instruments and include multidimensional assessment in surgical contexts.
Data Sharing Statement
All data analyzed in this study were extracted from previously published studies. The datasets and analysis code supporting the conclusions of this article are available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Von Baeyer CL, Spagrud LJ. Systematic review of observational (behavioral) measures of pain for children and adolescents aged 3 to 18 years. Pain. 2007;127(1):140–18. doi:10.1016/j.pain.2006.08.014
2. Cohen L, Cousins LA, Martin SR. Acute pain in children, Procedural. In: Gebhart GF, Schmidt RF, editors. Encyclopedia of Pain. Berlin, Heidelberg: Springer; 2013:48–54.
3. Wrona SK, Quinlan-Colwell A, Brown L, Jannuzzi RGE. Procedural pain management: clinical practice recommendations American society for pain management nursing. Pain Manag Nurs. 2022;23(3):254–258. doi:10.1016/j.pmn.2021.11.008
4. American Academy of Pediatrics CoPAoCaFH. American pain society TFoPiI, children, and adolescents. The assessment and management of acute pain in infants, children, and adolescents. Pediatrics. 2001;108(3):793–797. doi:10.1542/peds.108.3.793
5. Bayman EO, Oleson JJ, Rabbitts JA. AAAPT: assessment of the acute pain trajectory. Pain Med. 2021;22(3):533–547. doi:10.1093/pm/pnaa440
6. Chou R, Gordon DB, de Leon-Casasola OA, et al. Management of postoperative pain: a clinical practice guideline from the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council. J Pain. 2016;17(2):131–157. doi:10.1016/j.jpain.2015.12.008
7. Herlianita R, Chang C-J, Pangaribuan SM, Chiu H-Y. Occurrence rate and risk factors for rest and procedural pain in critically ill patients: a systematic review and meta-analysis. Intensive Crit Care Nurs. 2025;88:104002. doi:10.1016/j.iccn.2025.104002
8. Apfelbaum JL, Chen C, Mehta SS, Gan T. Postoperative pain experience: results from a national survey suggest postoperative pain continues to be undermanaged. Anesth Analg. 2003;97(2):534–540. doi:10.1213/01.ANE.0000068822.10113.9E
9. Roofthooft DW, Simons SH, Anand KJ, Tibboel D, van Dijk M. Eight years later, are we still hurting newborn infants? Neonatology. 2014;105(3):218–226. doi:10.1159/000357207
10. Orovec A, Disher T, Caddell K, Campbell-Yeo M. Assessment and management of procedural pain during the entire neonatal intensive care unit hospitalization. Pain Manag Nurs. 2019;20(5):503–511. doi:10.1016/j.pmn.2018.11.061
11. Duerden EG, Grunau RE, Guo T, et al. Early procedural pain is associated with regionally-specific alterations in thalamic development in preterm neonates. J Neurosci. 2018;38(4):878–886. doi:10.1523/JNEUROSCI.0867-17.2017
12. Walker SM. Long-term effects of neonatal pain. Semin Fetal Neonatal Med. 2019;24(4):101005. doi:10.1016/j.siny.2019.04.005
13. Friedrichsdorf SJ, Goubert L. Pediatric pain treatment and prevention for hospitalized children. Pain Rep. 2019;5(1):e804. doi:10.1097/PR9.0000000000000804
14. Krauss BS, Calligaris L, Green SM, Barbi E. Current concepts in management of pain in children in the emergency department. Lancet. 2016;387(10013):83–92. doi:10.1016/S0140-6736(14)61686-X
15. Olejnik L, Lima JP, Sadeghirad B, et al. Pharmacologic management of acute pain in children: a systematic review and network meta-analysis. JAMA Pediatrics. 2025;179(4):407–417. doi:10.1001/jamapediatrics.2024.5920
16. Borland M, Milsom S, Esson A. Equivalency of two concentrations of fentanyl administered by the intranasal route for acute analgesia in children in a paediatric emergency department: a randomized controlled trial. Emerg Med Australas. 2011;23(2):202–208. doi:10.1111/j.1742-6723.2011.01391.x
17. Saunders M, Adelgais K, Nelson D. Use of intranasal fentanyl for the relief of pediatric orthopedic trauma pain. Acad Emerg Med. 2010;17(11):1155–1161. doi:10.1111/j.1553-2712.2010.00905.x
18. Cardile S, Martinelli M, Barabino A, et al. Italian survey on non-steroidal anti-inflammatory drugs and gastrointestinal bleeding in children. World J Gastroenterol. 2016;22(5):1877–1883. doi:10.3748/wjg.v22.i5.1877
19. Misurac JM, Knoderer CA, Leiser JD, Nailescu C, Wilson AC, Andreoli SP. Nonsteroidal anti-inflammatory drugs are an Important Cause of Acute Kidney Injury in Children. J Pediatr. 2013;162(6):1153–1159.e1151. doi:10.1016/j.jpeds.2012.11.069
20. Mauritz MD, Hasan C, Dreier LA, Schmidt P, Zernikow B. Opioid-Induced respiratory depression in pediatric palliative care patients with severe neurological impairment—A scoping literature review and case reports. Children. 2020;7(12):312. doi:10.3390/children7120312
21. Uman LS, Birnie KA, Noel M, et al. Psychological interventions for needle-related procedural pain and distress in children and adolescents. Cochrane Database Syst Rev. 2013;(10). doi:10.1002/14651858.CD005179.pub3
22. Wolyniez I, Rimon A, Scolnik D, et al. The effect of a Medical Clown on pain during intravenous access in the pediatric emergency department: a randomized prospective pilot study. Clin Pediatr. 2013;52(12):1168–1172. doi:10.1177/0009922813502257
23. Chumpitazi CE, Chang C, Atanelov Z, et al. Managing acute pain in children presenting to the emergency department without opioids. JACEP Open. 2022;3(2):e12664. doi:10.1002/emp2.12664
24. Alotaibi K, Higgins I, Day J, Chan S. Paediatric pain management: knowledge, attitudes, barriers and facilitators among nurses - integrative review. Int Nurs Rev. 2018;65(4):524–533. doi:10.1111/inr.12465
25. Murphy A, Barrett M, Cronin J, et al. A qualitative study of the barriers to prehospital management of acute pain in children. Emerg Med J. 2014;31(6):493. doi:10.1136/emermed-2012-202166
26. Massaro M, Pastore S, Ventura A, Barbi E. Pain in cognitively impaired children: a focus for general pediatricians. Eur J Pediatr. 2013;172(1):9–14. doi:10.1007/s00431-012-1720-x
27. Boles J, Fraser C, Bennett K, et al. The Value of Certified Child Life Specialists: Direct and Downstream Optimization of Pediatric Patient and Family Outcomes. Association of Child Life Professionals (ACLP); 2020.
28. Association of Child Life Professionals CLCC. Child life professional certification candidate manual. 2024; Available from: https://www.childlife.org/docs/default-source/certification/candidate-manual.pdf?sfvrsn=10.
29. Romito B, Jewell J, Jackson M, et al. Child Life Services. Pediatrics. 2021;147(1):e2020040261. doi:10.1542/peds.2020-040261
30. Hummel J, Coenen M, Voigt-Blaurock V, Klein C, Jung-Sievers C. “Child Life Specialist” interventions in clinical pediatric care: a systematic review of the effects on mental health outcomes of children and adolescents. Gesundheitswesen. 2023;85(1):39–47. doi:10.1055/a-1676-3852
31. Rosenblatt A, Pederson R, Davis-Sandfoss T, Irwin L, Mitsos R, Manworren R. Child life specialist services, practice, and utilization across health care: a scoping review. JBI Evidence Synth. 2024;22(7):1303–1328. doi:10.11124/JBIES-23-00025
32. Hyland EJ, D’Cruz R, Harvey JG, Moir J, Parkinson C, Holland AJA. An assessment of early Child Life Therapy pain and anxiety management: a prospective randomised controlled trial. Burns. 2015;41(8):1642–1652. doi:10.1016/j.burns.2015.05.017
33. Burns-Nader S, Goldstein E. Effects of virtual reality during pediatric vaccinations. J Child Life. 2023;4(1).
34. Zhang Q, Guo J, Huang Y, Cheng H, Bai F, Xiang Y. Effects of medical game counseling on mental state and pain in school-age children with limb fractures. Chin Nurs res. 2022;36(19):3549–3553.
35. Chen Z, Li W. Application effect of medical game guidance in pain management of school-age children with limb fracture. Chin Health Stand Manag. 2023;14(10):14–17.
36. Zhang X, Yu G. Application of Child Life intervention in venipuncture of children with chronic kidney disease. J Nurs Adm. 2021;21(2):132–135.
37. Wang X, Xie M, Chen B. Application of Child Life concept in peripheral venipuncture in preschool children undergoing day surgery. Fujian Med J. 2024;46(05):80–84.
38. Jin L, Li D, Fang J, Yu L, Hu W. Effects of medical counseling games on children with hidden penis and their families. Chin Med Herald. 2023;20(13):170–175.
39. Zhang K, Zhao W, Huang T, Pu L, Hong Z. Application of medical counseling games in pediatric renal biopsy. Chin General Pract Nurs. 2025;23(8):1470–1473.
40. Gregory SW, Aul AJ, Lodermeier TM, Rodemeyer JL, Weaver AL, Lynch BA. The certified child life specialist: a novel resource in the pediatric primary care clinic for managing children’s pain during routine immunizations. Paediatr Neonatal Pain. 2023;5(3):66–75. doi:10.1002/pne2.12101
41. Higgins JPT, Thomas J, Chandler J, et al. Cochrane Handbook for Systematic Reviews of Interventions.
42. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71 doi:10.1136/bmj.n71.
43. EndNote X9: reference management software. 2018.
44. Steme JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898 doi:10.1136/bmj.l4898.
45. Sterne JAC, Hernan MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919. doi:10.1136/bmj.i4919
46. Li T, Higgins JPT, Deeks JJ. Chapter 5: collecting data. In: Cochrane Handbook for Systematic Reviews of Interventions.
47. Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14(1):135. doi:10.1186/1471-2288-14-135
48. Viechtbauer W. Conducting meta-analyses in R with the metafor package. J Stat Softw. 2010;36(3):1–48. doi:10.18637/jss.v036.i03
49. Hedges LV. Distribution theory for Glass’s estimator of effect size and related estimators. J Educ Stat. 1981;6(2):107–128. doi:10.3102/10769986006002107
50. Cheung MWL. Modeling dependent effect sizes with three-level meta-analyses: a structural equation modeling approach. Psychol Methods. 2014;19(2):211–229. doi:10.1037/a0032968
51. Assink M, Wibbelink CJM. Fitting three-level meta-analytic models in R: a step-by-step tutorial. Quant Methods Psychol. 2016;12(3):154–174. doi:10.20982/tqmp.12.3.p154
52. Knapp G, Hartung J. Improved tests for a random effects meta-regression with a single covariate. Stat Med. 2003;22(17):2693–2710. doi:10.1002/sim.1482
53. Verghese ST, Hannallah RS. Acute pain management in children. J Pain Res. 2010;3:105–123. doi:10.2147/JPR.S4554
54. McGrath PA, Gillsepie J. Pain assessment in children and adolescents. In: Turk DC, Melzack R, editors. Handbook of Pain Assessment.
55. Trottier ED, Ali S, Doré-Bergeron M-J, Chauvin-Kimoff L. Best practices in pain assessment and management for children. Paediatr Child Health. 2022;27(7):429–437. doi:10.1093/pch/pxac048
56. Viechtbauer W, Cheung MW-L. Outlier and influence diagnostics for meta-analysis. Res Synth Methods. 2010;1(2):112–125. doi:10.1002/jrsm.11
57. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–634. doi:10.1136/bmj.315.7109.629
58. Duval S, Tweedie R. Trim and fill: a simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000;56(2):455–463. doi:10.1111/j.0006-341X.2000.00455.x
59. Li S, Yuan T, Li N. Effect of personalized child life therapeutic play intervention on perioperative cooperation, pain and anxiety in children undergoing inguinal hernia surgery. Int J Nurs. 2025;44(2):323–327.
60. Li S, Jin Z, Liu L, et al. The application of narrative medical interventionbased on Child life concept in perioperative care ofchildren with cryptorchidism. Chinese Journal of Human Sexuality. 2025;34(01):14–18.
61. Zhou F, Huang M. Effect of preoperative visit based on Child Life model in children undergoing surgical procedures. Chin J Rural Med Pharmacy. 2024.
62. Sanchez Cristal N, Staab J, Chatham R, Ryan S, McNair B, Grubenhoff JA. Child life reduces distress and pain and improves family satisfaction in the pediatric emergency department. Clin Pediatr. 2018;57(13):1567–1575. doi:10.1177/0009922818798386
63. Deeks JJ, Higgins JPT, Altman DG, et al. Chapter 10: analysing data and undertaking meta-analyses. In: Higgins J, Thomas J, Chandler J, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 6.5. London: Cochrane; 2023.
64. McGrath PJ, Walco GA, Turk DC, et al. Core outcome domains and measures for pediatric acute and chronic/recurrent pain clinical trials: pedIMMPACT recommendations. J Pain. 2008;9(9):771–783. doi:10.1016/j.jpain.2008.04.007
65. Raja SN, Carr DB, Cohen M, et al. The revised international association for the study of pain definition of pain: concepts, challenges, and compromises. Pain. 2020;161(9):1976–1982. doi:10.1097/j.pain.0000000000001939
66. Zhou H, Albrecht MA, Roberts PA, Porter P, Della PR. Consistency of pediatric pain ratings between dyads: an updated meta-analysis and metaregression. Pain Rep. 2022;7(5):e1029. doi:10.1097/PR9.0000000000001029
67. Birnie KA, Hundert AS, Lalloo C, Nguyen C, Stinson JN. Recommendations for selection of self-report pain intensity measures in children and adolescents: a systematic review and quality assessment of measurement properties. Pain. 2019;160(1):5–18. doi:10.1097/j.pain.0000000000001377
68. Thrane SE, Wanless S, Cohen SM, Danford CA. The assessment and non-pharmacologic treatment of procedural pain from infancy to school age through a developmental lens: a synthesis of evidence with recommendations. J Pediatr Nurs. 2016;31(1):e23–e32. doi:10.1016/j.pedn.2015.09.002
69. Wu Y, Wu L, Leng H, Shen Q. Best evidence summary for non-pharmaceutical therapy of procedural pain in children. Chin Nurs res. 2021;35(5):782–788.
70. Perez-Pozuelo JM, Hernandez-Iglesias S, Pereira-Afonso MR, et al. Effectiveness of non-pharmacological methods in reducing pain in pediatric patients and the role of nursing: systematic review. Front Pediat. 2025;13:1729847. doi:10.3389/fped.2025.1729847
71. Cohen LL, Lemanek K, Blount RL, et al. Evidence-based assessment of pediatric pain. J Pediatr Psychol. 2008;33(9):939–955. doi:10.1093/jpepsy/jsm103
72. Bertolizio G, Garbin M, Ingelmo PM. Evaluation of nociception during pediatric surgery: a topical review. J Pers Med. 2023;13(2):260. doi:10.3390/jpm13020260
73. Tran Thi TH, Konara Mudiyanselage SP, Huang M-C. Effects of distraction on reducing pain during invasive procedures in children with cancer: a systematic review and meta-analysis. Pain Manag Nurs. 2022;23(3):281–292. doi:10.1016/j.pmn.2021.12.002
74. Koller D, Goldman RD. Distraction techniques for children undergoing procedures: a critical review of pediatric research. J Pediatr Nurs. 2012;27(6):652–681. doi:10.1016/j.pedn.2011.08.001
75. Bustamante Fernández M, Caes L, Rossel JI, et al. Efficacy of psychosensory interventions for the management of pediatric pain, fear, and distress during emergency care: a systematic review and meta-analysis of randomized clinical trials. Front Pediat. 2026;13. doi:10.3389/fped.2025.1654835
76. Davidson F, Snow S, Hayden JA, Chorney JJP. Psychological interventions in managing postoperative pain in children: a systematic review. Pain. 2016;157(9):1872–1886. doi:10.1097/j.pain.0000000000000636
77. Voepel-Lewis T, Burke CN, Jeffreys N, Malviya S, Tait ARJA, Analgesia. Do 0–10 numeric rating scores translate into clinically meaningful pain measures for children? Anesth Analg. 2011;112(2):415–421. doi:10.1213/ANE.0b013e318203f495
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Efficacy and Safety of Acupuncture for Tinnitus-Associated Insomnia: A Protocol for a Systematic Review and Meta-Analysis
Fan L, Gao Y, Zhou J, Hu H, Gao H
Journal of Pain Research 2022, 15:2957-2965
Published Date: 21 September 2022
A Systematic Review and Meta-Analysis Protocol on How Best to Use Non-Pharmacologic Therapies to Manage Chronic Low Back Pain and Associated Depression
Guo Y, Ma Q, Zhou X, Yang J, He K, Shen L, Zhao C, Chen Z, Tan CIC, Chen J
Journal of Pain Research 2022, 15:3509-3521
Published Date: 4 November 2022
Tezepelumab for Patients with Severe Uncontrolled Asthma: A Systematic Review and Meta-Analysis
Zoumot Z, Al Busaidi N, Tashkandi W, Aljohaney AA, Isse S, Vidyasagar K, Ukwaja KN
Journal of Asthma and Allergy 2022, 15:1665-1679
Published Date: 18 November 2022
The Analgesic Effect and Potential Mechanisms of Acupuncture for Migraine Rats: A Systematic Review and Meta-Analysis
Sun S, Liu L, Zhou M, Liu Y, Sun M, Zhao L
Journal of Pain Research 2023, 16:2525-2542
Published Date: 24 July 2023
Comparison of Balanced Crystalloids versus Normal Saline in Critically Ill Patients: A Systematic Review with Meta-Analysis and Trial Sequential Analysis of Randomized Controlled Trials
Chen Y, Gao Y
Therapeutics and Clinical Risk Management 2023, 19:783-799
Published Date: 11 October 2023