Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
The Double-Edged Sword of Intergenerational Support: A Cross-Sectional Study on Caregiver Burden Among Chinese Families Caring for Stroke Survivors with Disabilities
Authors Yang G, Hu P, Bao S, Shu M, Dong J, Yu Y ![]()
Received 28 February 2026
Accepted for publication 4 June 2026
Published 9 June 2026 Volume 2026:19 605802
DOI https://doi.org/10.2147/JMDH.S605802
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Gege Yang,1 Pinglang Hu,2 Shaorui Bao,2 Meichun Shu,3 Jingjing Dong,2 Yueting Yu2
1Department of Geriatrics, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, 325000, People’s Republic of China; 2Department of Neurology, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, 325000, People’s Republic of China; 3Department of Infectious Diseases, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, 325000, People’s Republic of China
Correspondence: Yueting Yu, Email [email protected]
Objective: This cross-sectional study examined the association between intergenerational support (IGS) and caregiver burden (CB) among Chinese family caregivers of stroke survivors with persistent disabilities and explored potentially modifiable factors associated with CB.
Methods: In a cross-sectional survey of 683 stroke survivors (≥ 6 months post-discharge) and their primary family caregivers, we assessed sociodemographic and caregiving characteristics, functional disability (Katz ADL), intergenerational support (adapted IGSS), caregiver burden (CBI), and caregiver self-efficacy (GSES). Multiple linear regression was used to examine factors independently associated with caregiver burden.
Results: The mean caregiver burden score was 44.72 ± 17.57. Higher burden was associated with patient dementia (B = 6.316, p < 0.001), greater disability severity (B = 3.103, p = 0.006), only-child status (B = 4.260, p = 0.003), and higher education of the involved adult child (university: B = 16.204, p < 0.001). Lower burden was associated with higher child income (B = − 1.869, p = 0.036), stronger IGS (B = − 0.556, p = 0.002), and greater caregiver self-efficacy (B = − 5.411, p < 0.001).
Conclusion: Family caregivers of stroke survivors with disabilities in China experience substantial caregiver burden. Patient dementia, greater disability severity, only-child status, and higher education of the involved adult child were associated with higher burden, whereas higher child income, stronger intergenerational support, and greater caregiver self-efficacy were associated with lower burden. These findings suggest that family-centered support, caregiver self-efficacy enhancement, and services for high-risk families may serve as hypotheses for future intervention development.
Keywords: intergenerational support, disability, caregiver burden, associated factors, stroke, China, cross-sectional study
Introduction
Stroke represents a major global health challenge and remains a leading cause of long-term disability and mortality worldwide.1,2 In China, demographic aging and epidemiological shifts have contributed to a growing population of stroke survivors living with persistent disabilities, most of whom rely primarily on family-based care.3–5 However, rapid sociodemographic changes - including the transition from extended to nuclear families, increased geographic mobility of adult children, and rising female workforce participation - have strained traditional intergenerational support systems.6–8 Consequently, caregiving responsibilities have become increasingly concentrated on spouses or single adult children, who often lack adequate training and support.9,10
Intergenerational support (IGS), encompassing financial, instrumental, and emotional exchanges between generations, serves as a crucial informal resource for sustaining family caregiving.11,12 Existing studies have examined caregiver burden among families of stroke survivors and have identified patient disability, dementia, caregiver psychological resources, and social support as important correlates.13,14 Nevertheless, several gaps remain. First, few studies have specifically examined how bidirectional IGS is associated with caregiver burden in families caring for stroke survivors with persistent disabilities. Second, limited evidence has considered the changing Chinese family context, particularly the pressures created by only-child family structures and work-care conflict among adult children.15,16 Third, previous studies have often described associated factors without explicitly situating them within a conceptual framework that links caregiving demands, family resources, and caregiver appraisal.
Guided by the stress-buffering perspective and intergenerational solidarity theory, this study conceptualized patient disability and dementia as caregiving demands, IGS and caregiver self-efficacy as family and psychological resources, and adult child characteristics as contextual factors that may either alleviate or intensify caregiver strain. On this basis, the present study aimed to: (1) assess levels of perceived IGS and CB among caregivers of stroke survivors with disabilities; (2) examine the association between IGS and CB; and (3) identify factors independently associated with CB to inform targeted support strategies. Because this was a cross-sectional study, the research questions focused on associations rather than causal pathways.
Methods
Study Design and Participants
A cross-sectional survey was conducted at a tertiary hospital in Wenzhou, China. Participants were stroke survivors discharged from the neurology department for more than 6 months between January and December 2024 and their primary family caregivers. The 6-month post-discharge threshold was selected to focus on the relatively stable post-acute phase, when persistent disability and routine family caregiving patterns are more likely to have been established.17 Potential participants were identified via telephone follow-up, and surveys were administered during scheduled outpatient visits.
Inclusion criteria were: (1) confirmed stroke diagnosis; (2) persistent disability, defined as activities of daily living impairment, or cognitive impairment (dementia) at ≥6 months post-discharge; (3) spouse alive; (4) at least one adult child (≥18 years) alive; (5) primary caregiver being a family member; and (6) provision of informed consent.
Exclusion criteria were: (1) history of multiple stroke hospitalizations; (2) comorbid malignancy or other severe cardiopulmonary or organ diseases; and (3) all children aged <18 years.
Sample size: Based on the principle requiring 5–10 participants per variable for multiple regression, and considering 25 key variables, the minimum sample size was estimated at 125–250. Accounting for an anticipated 20% attrition and non-response rate, the target sample size was set at 150–300. A total of 800 questionnaires were distributed. After excluding incomplete or invalid responses (n = 110), 690 questionnaires were collected. Further exclusion of 7 invalid questionnaires resulted in a final sample of 683 participants (effective response rate: 85.4%). The study protocol was approved by the Hospital Ethics Committee (Approval No.: (2023) No. 220). This study complies with the Declaration of Helsinki.
Measurement Instruments
Sociodemographic and Caregiving Characteristics
A structured questionnaire collected information on: (1) patients (age, gender, occupation, education, income, insurance type, disability type, and number of children); (2) spouses (age, gender, education, and employment status); and (3) the primary involved adult child (age, gender, marital status, whether they had children of their own, education, employment, and income). The “primary involved adult child” was operationally defined as the adult child identified by the primary family caregiver as being most involved in the patient’s daily care, care-related arrangements, or emotional support after discharge. Daily caregiving duration was categorized as <4 hours (h), 4–8 h, 8–12 h, or ≥12 h.
Functional Disability Assessment
The Katz Activities of Daily Living (ADL) Scale18 was used to evaluate patients’ independence in six basic activities: bathing, dressing, toileting, transferring, feeding, and continence. Disability severity was classified as mild (1–2 impaired tasks), moderate (3–4 impaired tasks), or severe (5–6 impaired tasks). Cronbach’s α in this study was 0.830.
Intergenerational Support
We employed an adapted 6-item Intergenerational Support Scale (IGSS) originally developed by Xi’an Jiaotong University.19 The scale assesses bidirectional support across two dimensions: Parent-to-Child support (financial, instrumental, and emotional) and Child-to-Parent support (financial, instrumental, and emotional). Each item is rated on a 5-point Likert scale (0–4), with total scores ranging from 0 to 24. Higher scores indicate stronger intergenerational support. Cronbach’s α was 0.708, and test-retest reliability at a 1-week interval was 0.87.
Caregiver Burden
Caregiver burden was measured using the 24-item Chinese version of the Caregiver Burden Inventory (CBI),20,21 which comprises five subscales: time-dependence, developmental, physical, social, and emotional burden. Items are rated from 0 to 4, with total scores ranging from 0 to 96. Higher scores reflect greater burden. Cronbach’s α was 0.924.
Caregiver Self-Efficacy
The General Self-Efficacy Scale (GSES)22 was used to assess caregivers’ confidence in managing caregiving challenges. The 10-item Chinese version employs a 4-point response scale, with total scores ranging from 0 to 40. Higher scores indicate stronger self-efficacy. Cronbach’s α was 0.894.
Data Collection
Convenience sampling was used. Potential participants meeting the inclusion criteria were identified via telephone follow-up of patients discharged more than 6 months earlier. After confirming eligibility and interest, questionnaires were administered during scheduled outpatient visits by trained researchers after written informed consent was obtained. To reduce information bias, researchers used standardized instructions and checked questionnaires for missing items immediately after completion.
Statistical Analysis
Data were analyzed using SPSS 25.0 (IBM Corp., Armonk, NY, USA). Continuous variables are presented as mean ± standard deviation (SD), and categorical variables as frequency (n) and percentage (%). Univariate analyses of differences in CBI total scores across categorical variables were performed using one-way ANOVA or independent t-tests, as appropriate. Variables showing a significant association in univariate analysis, together with clinically relevant variables, were considered for entry into a multiple linear regression model with CBI total score as the dependent variable. Dummy variables were created for categorical predictors with more than two levels, including health insurance and child education level. The reference categories are specified in the regression table Model assumptions were evaluated to improve the transparency of statistical reporting. Linearity and homoscedasticity were examined using residual plots; residual normality was assessed using histograms and normal probability plots; and multicollinearity was assessed using variance inflation factors (VIFs), with VIF values below 10 regarded as indicating no severe multicollinearity. Residual independence was verified using the Durbin-Watson statistic. To prevent inconsistent reporting and account for model complexity, the adjusted R2 is used as the primary metric for model fit. Statistical significance was set at p < 0.05 (two-tailed).
Results
Characteristics of Stroke Survivors with Disability and Caregivers
A total of 683 stroke survivors with disability and their primary family caregivers were included in this study. The mean age of the patients was 69.48 ± 9.63 years, ranging from 44 to 92 years, and 404 patients were male (59.2%). Most patients had a junior high school education or below, and farmers accounted for the largest occupational group. Regarding economic and medical insurance status, 246 patients (36.0%) had a monthly income below 3,000 RMB, and most were covered by the New Rural Cooperative Medical Scheme.
Spouses were the primary caregivers in 532 cases (77.9%), whereas adult children served as primary caregivers in 151 cases (22.1%). The mean age of spouses was 67.09 ± 11.25 years, and most spouses were not employed. The mean age of the involved adult children was 37.66 ± 9.39 years, with a nearly balanced gender distribution. Most involved adult children were married with children, employed, and had a middle/high school education level. Only-child families accounted for 25.5% of the sample.
Regarding clinical and caregiving characteristics, most patients had mild (368, 53.9%) or moderate disability (269, 39.4%), while 46 patients (6.7%) had severe disability. Physical disability only was observed in 380 patients (55.6%), cognitive impairment only in 66 patients (9.7%), and both physical and cognitive impairment in 237 patients (34.7%). Daily caregiving duration was predominantly 4–8 hours (373, 54.6%), followed by <4 hours (197, 28.8%), 8–12 hours (89, 13.0%), and >12 hours (24, 3.5%). These sociodemographic, clinical, and caregiving characteristics are summarized in Table 1.
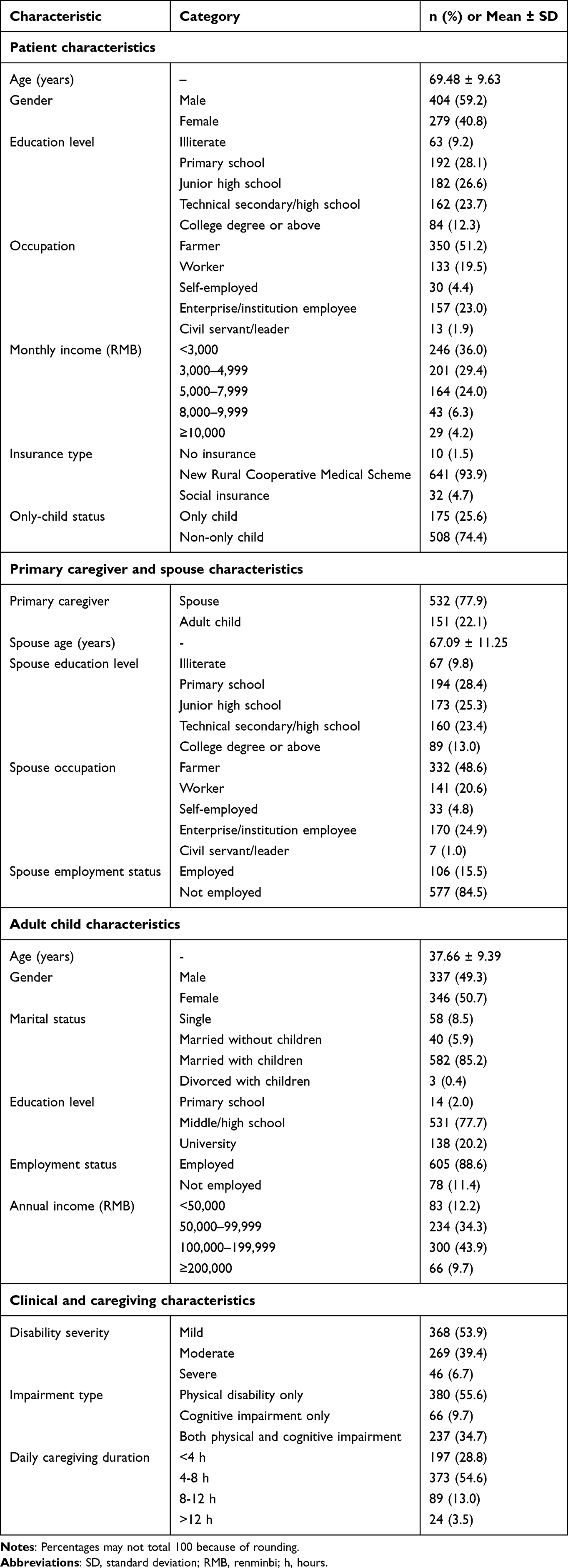 |
Table 1 Sociodemographic and Caregiving Characteristics of Participants (n = 683) |
Levels of Intergenerational Support (IGS)
The overall IGS score was 22.68 ± 3.72 (Table 2). Parent-to-Child support (11.45 ± 2.08) and Child-to-Parent support (11.23 ± 2.42) scores were comparable. Emotional support scores were generally the highest subcomponent within each dimension.
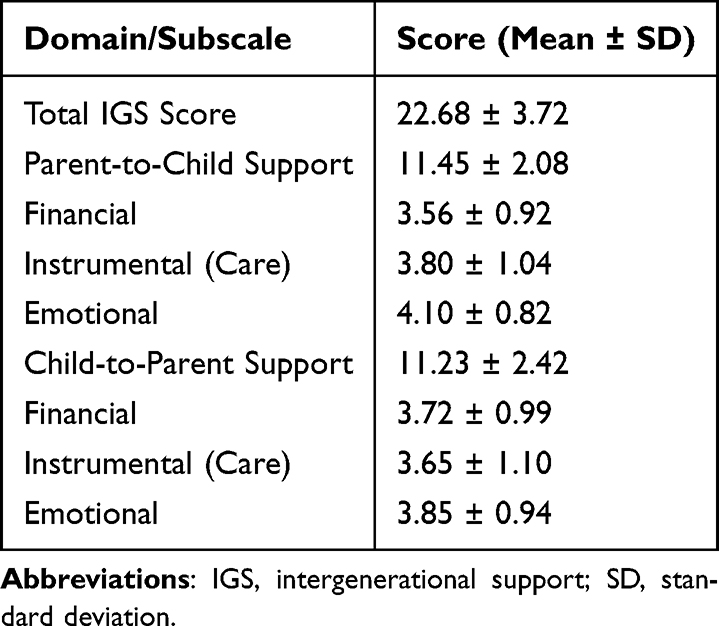 |
Table 2 Scores of Intergenerational Support (IGS) |
Levels of Caregiver Burden (CB) and Self-Efficacy
Caregiver burden was substantial (total CBI score: 44.72 ± 17.57). Time-dependence burden (12.28 ± 4.26) and developmental burden (11.35 ± 5.16) were the highest subscale scores, followed by physical (7.61 ± 4.08), emotional (7.25 ± 5.38), and social burden (6.23 ± 3.88) (Table 3). Caregiver self-efficacy (GSES) was moderate (27.18 ± 6.33).
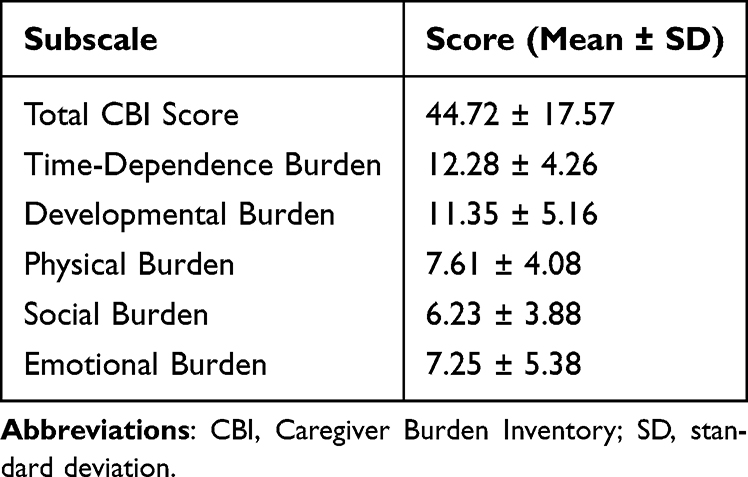 |
Table 3 Scores of Caregiver Burden Inventory (CBI) |
Univariate Analysis of Factors Associated with Caregiver Burden
Univariate analysis identified several factors significantly associated with higher CBI scores (p < 0.05, Table 4). These included patient-related factors (dementia, greater disability severity, and longer daily caregiving duration), child-related factors (only-child status, child education level, lower income level, unemployment, and having no children of their own), and contextual or resource-related factors (health insurance type, lower IGS, and lower caregiver self-efficacy). Caregiver role, patient age, gender, occupation, education, income, and spouse characteristics were not significantly associated with CBI scores in univariate analyses.
 |
Table 4 Univariate Analysis of Factors Associated with Caregiver Burden |
Multiple Linear Regression Analysis of Factors Associated with Caregiver Burden
Variables significant in univariate analysis (p < 0.05), together with clinically relevant variables, were entered into the multiple linear regression model (Table 5). The final multiple linear regression model was statistically significant, F(13, 668) = 33.932, p < 0.001. The model explained approximately 38.6% of the variance in caregiver burden (adjusted R2 = 0.386). The Durbin-Watson statistic was 1.677, suggesting no substantial autocorrelation of residuals. VIF values ranged from 1.030 to 9.441. Most predictors showed low VIF values; however, the two dummy variables for adult child education had relatively higher VIFs, likely reflecting the small size of the primary-school reference group. Therefore, the association between adult child education and caregiver burden should be interpreted cautiously. It is important to note that while variables such as “child employment status” and “health insurance type” showed significant associations in the univariate analysis (Table 4), they did not retain independent predictive power in the final model. This suggests that their effects were likely confounded by or absorbed into stronger socioeconomic predictors, specifically child income and education level, which were retained as core factors. In the final model, factors associated with higher CBI scores were patient dementia (B = 6.316, p < 0.001), greater disability severity (B = 3.103, p = 0.006), only-child status (B = 4.260, p = 0.003), and higher education level of the involved adult child (middle/high school: B = 14.966, p = 0.001; university: B = 16.204, p < 0.001), compared with primary school education. Factors associated with lower CBI scores were higher child income (B = −1.869, p = 0.036), higher IGS score (B = −0.556, p = 0.002), and higher caregiver self-efficacy (B = −5.411, p < 0.001).
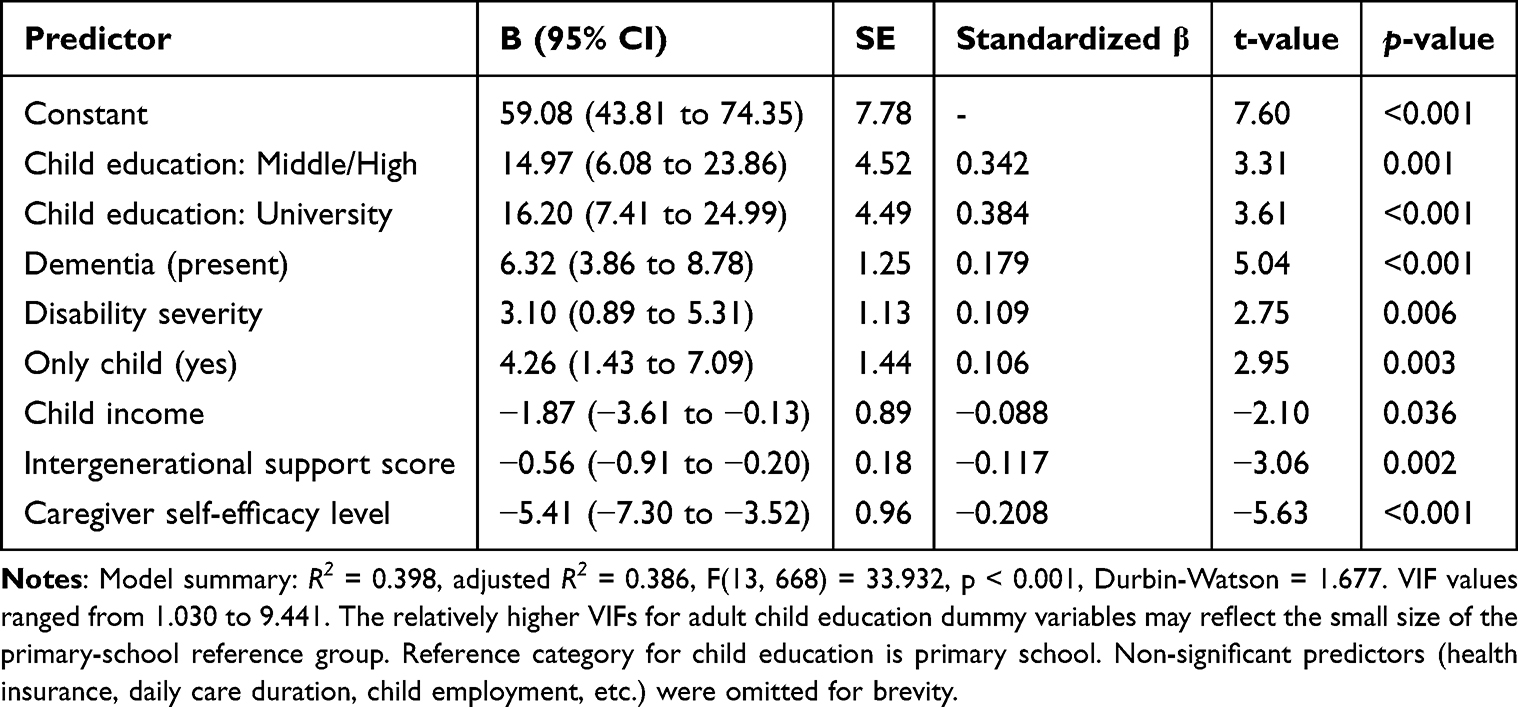 |
Table 5 Multiple Linear Regression Analysis of Factors Associated with Caregiver Burden |
Discussion
This cross-sectional study provides insights into the substantial burden experienced by family caregivers of stroke survivors with persistent disability in China and highlights the associations of intergenerational support (IGS) and caregiver self-efficacy with caregiver burden. Guided by the stress-buffering framework, patient dementia and disability severity may be interpreted as major caregiving-related stressors associated with higher perceived burden. In contrast, stronger intergenerational support and higher caregiver self-efficacy may represent psychosocial resources associated with lower perceived burden. However, given the cross-sectional design, these findings should be interpreted as associations rather than evidence of causal or buffering effects.
Magnitude and Context of Caregiver Burden
The mean caregiver burden score in our study indicates a substantial level of burden and is higher than that reported in some earlier regional studies.23–25 This may reflect several intersecting factors: (1) demographic and epidemiologic shifts, including population aging and extended survival with disability; (2) weakened informal support networks due to declining fertility, urbanization, and geographic dispersal of adult children; (3) increasing complexity of home-based care, which may involve rehabilitation, medication management, and management of cognitive or behavioral symptoms; and (4) persistent gaps in formal long-term care services and financial protection mechanisms in China. The high expressed need for respite care in our survey further underscores the shortage of supportive services for family caregivers.
Patient-Related Factors: Core Caregiving Demands
Patient dementia was strongly associated with higher caregiver burden, which is consistent with previous longitudinal and cross-sectional studies.26–28 Cognitive impairment may increase care complexity through behavioral and psychological symptoms, communication difficulties, impaired safety awareness, and the need for constant supervision. Greater severity of physical disability was also independently associated with higher burden.29 Severe ADL limitations often require more intensive and physically demanding assistance, including transfers, toileting, feeding, and continence care. These findings reinforce the need for targeted support for caregivers managing combined physical and cognitive impairment.
The Complex Role of Adult Child Characteristics
Our findings highlight the nuanced position of adult children in the caregiving dynamic. The positive association between only-child status and caregiver burden reflects the structural strain of China’s “4-2-1” family model, where an absence of siblings eliminates shared caregiving and financial distribution. Although variables such as child employment and health insurance were significant in univariate analyses, they did not retain significance in the adjusted multivariate model, suggesting that these variables may not have independent associations with caregiver burden after adjustment for income and education. Higher child income was associated with lower burden, likely acting as a resource buffer to afford formal care services. Conversely, higher education of the involved adult child was associated with higher caregiver burden in this study, this finding warrants a more nuanced, interpretive analysis. Rather than a direct causal link, we hypothesize three underlying mechanisms: highly educated adult children often occupy demanding professional roles with limited flexibility, creating severe friction between career advancement and caregiving obligations; educated children may hold higher internal standards for care quality and patient outcomes, leading to greater psychological strain when these ideals encounter the realities of persistent disability; those with higher education may be more acutely aware of the social and professional milestones sacrificed for caregiving, which amplifies the subjective sense of burden. However, it must be noted that this interpretation is primarily hypothetical; without direct measures of work flexibility or cultural expectations, empirical longitudinal research is required to substantiate these mechanisms.
Protective Factors: IGS and Caregiver Self-Efficacy
Higher IGS was associated with lower caregiver burden, supporting the stress-buffering perspective. Emotional support may reduce isolation and psychological distress, instrumental support may reduce direct workload, and financial support may increase access to formal or paid assistance. Importantly, IGS should not be viewed only as the presence of adult children, but as the quality and availability of bidirectional support within the family.
Caregiver self-efficacy was also associated with lower burden. Caregivers who have stronger confidence in managing caregiving challenges may be more likely to use proactive coping strategies, seek information, solve problems, and regulate emotional stress. This finding suggests that caregiver training, psychoeducation, problem-solving support, and peer support interventions may be promising strategies for future testing. Nevertheless, because of the cross-sectional design, it is also possible that caregivers experiencing lower burden report higher self-efficacy; longitudinal research is needed to clarify the direction of this association.
Implications and Recommendations
The findings have practical implications but should be interpreted as hypothesis-generating rather than definitive evidence of intervention effects. First, healthcare teams may consider screening for high-risk caregiving situations, especially dementia, severe disability, only-child family status, low family support, and low caregiver self-efficacy. Second, family-centered interventions may help clarify care roles, improve communication, and facilitate feasible emotional, instrumental, and financial support from adult children. Third, caregiver self-efficacy may be strengthened through skills training in ADL assistance, dementia-related symptom management, communication techniques, and stress management. Fourth, the results support the need for broader service development, including accessible home- and community-based services, respite care, and workplace policies that support employed family caregivers. These recommendations require further evaluation in intervention and policy studies.
Limitations and Future Directions
This study has several limitations. First, the use of convenience sampling from a single hospital may introduce selection bias, potentially limiting the generalizability of our findings to rural populations or families not engaged in outpatient follow-up. Second, our cross-sectional design strictly precludes causal inference; therefore, all identified predictors should be viewed as significant correlates or associations rather than definitive causes. Third, some important factors were not measured, including caregiver physical and mental health, size and quality of broader social support networks, objective financial strain, specific care tasks, work flexibility, patient behavioral symptoms beyond dementia diagnosis, cultural expectations, and response bias. Fourth, the finding regarding child education requires cautious interpretation because potential mechanisms were not directly assessed. Future studies should use longitudinal and mixed-methods designs to examine burden trajectories and clarify mechanisms underlying the associations observed here. Intervention studies are also needed to test whether strengthening IGS and caregiver self-efficacy can reduce caregiver burden.
Conclusion
Family caregivers of stroke survivors with disabilities in China experience substantial caregiver burden. Patient dementia, greater disability severity, only-child status, and higher education of the involved adult child were associated with higher burden, whereas higher child income, stronger intergenerational support, and greater caregiver self-efficacy were associated with lower burden. These findings highlight the importance of identifying high-risk caregivers and developing family-centered, skills-based, and service-supported strategies. However, causal relationships cannot be inferred from this cross-sectional study, and future longitudinal and intervention research is needed.
Data Sharing Statement
The data and analytical code that support the findings of this study will be made publicly available in a permanent repository upon article acceptance.
Ethics Statement
The study was approved by the Ethics Committee of The First Affiliated Hospital of Wenzhou Medical University (Approval No.: (2023) No. 220). All participants provided written informed consent. This study complies with the Declaration of Helsinki.
Acknowledgments
The authors thank all participants for their contribution to this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by Wenzhou Science and Technology Bureau Project (No. Y2023676) and Zhejiang Provincial Medical and Health Science and Technology Plan Project (No. 2023565814).
Disclosure
The authors declare no conflicts of interest.
References
1. GBD 2021 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet Neurol. 2024;23(10):973–11. doi:10.1016/S1474-4422(24)00238-5
2. Ding Q, Liu S, Yao Y, et al. Global, regional, and national burden of ischemic stroke, 1990-2019. Neurology. 2022;98(3):e279–e290. doi:10.1212/WNL.0000000000013115
3. Naoki T, M JM, Masako O, et al. Disagreement about perceptions of patient disability between the stroke patient and caregiver: a cross sectional study exploring the association to patient and caregiver quality of life. Aging Mental Health. 2022;27(9):1–9. doi:10.1080/13607863.2022.2116400
4. Lin Q, Dong X, Huang T, et al. Care dependency in older stroke patients with comorbidities: a latent profile analysis. Front Aging Neurosci. 2024;16:1366380. doi:10.3389/fnagi.2024.1366380
5. Septian BR, Wulandari TB. Home-based palliative care needs among caregivers of stroke patients in Yogyakarta, Indonesia: a qualitative phenomenology. Front Nurs. 2025;12(3):383–391. doi:10.2478/FON-2025-0042
6. Zhang HM, Gao J, Zhang N, et al. Systematic review of qualitative studies on the care experience of stroke patients’ family members. Chin Nurs Res. 2019;33(19):3308–3324. (Chinese).
7. Garnett A, Ploeg J, Markle-Reid M, et al. Factors impacting the access and use of formal health and social services by caregivers of stroke survivors: an interpretive description study. BMC Health Serv Res. 2022;22(1):433. doi:10.1186/s12913-022-07829-2
8. Meng LY, Jin Y, Zuo ZQ, et al. A review of the scope of intervention programs for caregivers’ care abilities in stroke patients. Gen Nurs. 2024;22(13):2377–2382. (Chinese).
9. Qiao XC. The elderly care problem of China’s first generation of younger and older population: an analysis from the perspective of life course. Soc Policy Res. 2025;1:15–41. (Chinese).
10. Wang P, Zhang N, Shang JY, et al. The impact of family structure transformation on intergenerational support for rural elderly from an age perspective. South Popul. 2024;39(1):18–32. (Chinese).
11. Yang X. A Study on the Care Competence of Clinical Stroke Caregivers [dissertation]. Shihezi: Shihezi University; 2018. (Chinese).
12. Han Y, Pan SF, Song CX, et al. A study on the functional status of elderly people in nursing homes based on ICF-RS analysis. Chin J Rehabil. 2025;40(3):162–166. (Chinese).
13. Fang L, Dong M, Fang W, et al. Relationships between care burden, resilience, and depressive symptoms among the main family caregivers of stroke patients: a cross-sectional study. Front Psychiatry. 2022;13:960830. doi:10.3389/fpsyt.2022.960830
14. Yu YT, Lin YC, Shu MC. Factors influencing the medical seeking behavior of stroke patients with disability from the perspective of intergenerational support. Nurs Rehabil. 2024;23(1):1–6. (Chinese).
15. Yang JH. Eight major changes in family structure and policy responses. J Demogr. 2025;47(1):33–48. (Chinese).
16. Chen H, Liu Y, Wu XL, et al. A comparative study on the level of disability among the elderly in China: based on data from four national surveys. South Popul. 2021;36(5):1–12. (Chinese).
17. Wang M, Wang K, Xie B, et al. Understanding the needs of family caregivers of stroke patients with disabilities: a phenomenological study using the timing it right theory. PLoS One. 2025;20(6):e0325671. doi:10.1371/JOURNAL.PONE.0325671
18. Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged: the Index of ADL, a standardized measure of biological and psychosocial function. JAMA. 1963;185(12):914–919. doi:10.1001/jama.1963.03060120024016
19. Zhang WJ, Li SZ. The impact of intergenerational support behavior of children on the life satisfaction of rural elderly. Popul Res. 2005;29(5):73–80. (Chinese).
20. Novak M, Guest C. Application of a multidimensional caregiver burden inventory. Gerontologist. 1989;29(6):798–803. doi:10.1093/geront/29.6.798
21. Yue P, Fu Y, Shang SM, et al. Reliability and validity test of the Caregiver Burden Questionnaire. Chin J Ment Health. 2006;20(8):562–564. (Chinese).
22. Wang CK, Hu ZF, Liu Y. A study on the reliability and validity of self-efficacy scales. Appl Psychol. 2001;7(1):37–40. (Chinese).
23. Chen YY, Zhang CN. Path analysis of the influencing factors of family caregivers’ burden for disabled elderly. Contemp Nurse. 2022;29(2):1–5. (Chinese).
24. Zhang P, Li X, Ma KK, et al. Correlation between sense of coherence and caregiver burden among primary caregivers of stroke patients. Chin Gen Pract Nurs. 2021;19(19):2724–2727. (Chinese).
25. Cattaneo A, Vitali A, Regazzoni D, et al. The burden of informal family caregiving in Europe, 2000-2050: a microsimulation modelling study. Lancet Reg Health Eur. 2025;53:101295. doi:10.1016/j.lanepe.2025.101295
26. Magan CK, Mofford K. Understanding allostatic load and the physiological impact of chronic stress in family caregivers: a scoping review. Aging Mental Health. 2025;1–13. doi:10.1080/13607863.2025.2570824
27. Connors MH, Seeher K, Teixeira-Pinto A, et al. Dementia and caregiver burden: a three-year longitudinal study. Int J Geriatr Psychiatry. 2020;35(2):250–258. doi:10.1002/gps.5239
28. Rys B, Bak E. Factors determining the burden of a caregiver providing care to a post-stroke patient. J Clin Med. 2025;14(9):2184. doi:10.3390/jcm14092184
29. Ghazawy ER, Mohammed ES, Mahfouz EM, et al. Determinants of caregiver burden of persons with disabilities in a rural district in Egypt. BMC Public Health. 2020;20(1):1156. doi:10.1186/s12889-020-09254-8
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Influence of Acupuncture and Other Clinical Factors on the Recovery of Limb Motor Function in Patients After Stroke: A Retrospective Study
Wu B, Ding Y, Peng M, Wang X, Li Y, Cheng X
Journal of Multidisciplinary Healthcare 2023, 16:463-474
Published Date: 21 February 2023
Caregiver Burden and Its Associated Factors Among Family Caregivers of Hospitalized Patients with Neurocritical Disease: A Cross-Sectional Study
Wei L, Zhao X, Chen X, He Y, Liu J, Xian J, Yang Y
Journal of Multidisciplinary Healthcare 2024, 17:5593-5603
Published Date: 26 November 2024
Multidimensional Analysis of Frailty and Its Influencing Factors in Hospitalized Elderly Stroke Patients
Zhou H, Han Y, Xie D, Zheng K, Zhu H, Zhou Z, Ji Y
Clinical Interventions in Aging 2025, 20:1741-1755
Published Date: 11 October 2025
Disability in Older Adults with COPD: Prevalence, Assessment, and Influencing Factors — A Scoping Review
Huang X, Li H, Yao H, Ma P, Chen H, Zhang Y, Duan W, Yan X
Clinical Interventions in Aging 2026, 21:610177
Published Date: 22 June 2026
"I Did What I Could Manage”: Caregiver Burden and Rational Triage of Stroke Discharge Instructions in Rural Uganda – A Qualitative Study
Kakongi N, Owokuhaisa J, Asiimwe D, Nuwahereza A
Journal of Multidisciplinary Healthcare 2026, 19:619550
Published Date: 22 July 2026