Back to Journals » Clinical Interventions in Aging » Volume 21
Disability in Older Adults with COPD: Prevalence, Assessment, and Influencing Factors — A Scoping Review
Authors Huang X, Li H, Yao H, Ma P, Chen H, Zhang Y, Duan W, Yan X
Received 18 March 2026
Accepted for publication 2 June 2026
Published 22 June 2026 Volume 2026:21 610177
DOI https://doi.org/10.2147/CIA.S610177
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Xiangru Huang,1 Haixia Li,2 Hui Yao,2 Pin Ma,2 Hong Chen,2 Yu Zhang,3 Wei Duan,4 Xiaoli Yan5
1School of Nursing, Ningxia Medical University, Yinchuan, Ningxia Hui Autonomous Region, People’s Republic of China; 2Nursing Department, Ningxia Hui Autonomous Region People’s Hospital, Yinchuan, Ningxia Hui Autonomous Region, People’s Republic of China; 3Emergency Department, Ningxia Hui Autonomous Region People’s Hospital, Yinchuan, Ningxia Hui Autonomous Region, People’s Republic of China; 4Department of Respiratory Medicine, Ningxia Hui Autonomous Region People’s Hospital, Yinchuan, Ningxia Hui Autonomous Region, People’s Republic of China; 5Center for Geriatric Medicine, Ningxia Hui Autonomous Region People’s Hospital, Yinchuan, Ningxia Hui Autonomous Region, People’s Republic of China
Correspondence: Haixia Li, Nursing Department, Ningxia Hui Autonomous Region People’s Hospital, 301 Zhengyuan North Street, Jinfeng District, Yinchuan City, Ningxia Hui Autonomous Region, People’s Republic of China, Email [email protected]
Abstract: Chronic obstructive pulmonary disease (COPD) is highly prevalent in older adults. Symptoms such as dyspnea impair daily function and increase the risk of disability. However, no comprehensive synthesis of disability prevalence, assessment tools, and associated factors in this population exists. Therefore, this scoping review aims to identify the prevalence, assessment tools, and influencing factors of disability in this population to inform future interventions. We searched Web of Science, PubMed, Embase, Cochrane Library, CNKI, Wanfang, VIP, and China Biomedical Literature Database from inception to October 31, 2025. Two researchers independently screened, extracted, and analyzed data according to predefined criteria. Twelve studies were included, most of which used cross-sectional designs. These studies reported a wide range of disability prevalence among older adults with COPD (15.00% to 97.00%), reflecting significant heterogeneity across studies. Multiple assessment tools were used; the Katz Index and the Elderly Disability Assessment Scale (EDAS) were the most common. However, few tools had been specifically developed or validated for this population in China. Sociodemographic, disease-related, and psychosocial variables were identified as the main influencing factors. In conclusion, disability in older adults with COPD is a multifactorial condition, and variability in prevalence estimates is largely driven by differences in assessment tools. The predominance of cross-sectional designs precludes causal inference and highlights the need for more rigorous study designs. Future research should focus on developing and prospectively validating COPD-specific assessment tools for mainland Chinese populations, conducting longitudinal studies to clarify disability trajectories, and integrating quantitative and qualitative methods to develop multidimensional intervention strategies.
Keywords: older adults, chronic obstructive pulmonary disease, disability, prevalence, influencing factors
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is a progressive respiratory disorder characterized by persistent airflow limitation and symptoms such as dyspnea, chronic cough, and sputum production.1 In older adults, the incidence of chronic diseases increases significantly as physiological function declines.2 COPD is currently the third leading cause of death worldwide, accounting for approximately 6% of all deaths, following ischemic heart disease and cerebrovascular disease, and its prevalence is projected to continue rising over the next four decades.3 In China, COPD prevalence among older adults remains high, reaching 21.2% in those aged 60–69 years and 35.5% in those aged ≥70 years.4
A study published in The Lancet reported that the global proportion of disability-adjusted life years (DALYs) attributable to years lived with disability (YLDs) from COPD has increased significantly and is projected to rise from 33.8% in 2022 to 41.1% by 2050.5 The International Classification of Impairments, Disabilities, and Handicaps (ICIDH) first defined disability as a limitation or defect in an individual’s ability to perform daily activities and identified it as a key indicator in comprehensive geriatric assessment.6 Since then, research has broadened the definition of disability. According to the International Classification of Functioning, Disability and Health (ICF), disability arises from physiological impairments, psychological factors, and social and environmental influences, rather than from a single factor.7 In older adults with COPD, various clinical manifestations, including progressively worsening dyspnea, chronic hypoxia, systemic inflammation, and muscle atrophy—particularly affecting respiratory and limb skeletal muscles—significantly reduce exercise tolerance, thereby impairing the capacity to perform both basic and instrumental activities of daily living (ADLs and IADLs).8 At the same time, psychological factors such as anxiety and depression further reduce motivation, while social factors such as limited social support and low educational attainment restrict access to nursing and rehabilitation services. These factors interact to influence the onset and severity of disability. Systematic reviews have shown that the prevalence of disability among older adults with chronic diseases, particularly COPD, ranges from 7.4% to 49.8% worldwide.9 Therefore, disability among older adults with COPD arises from interactions among multiple factors and increases the risk of reduced quality of life and adverse clinical outcomes.
Beyond its multifactorial nature, disability is not a static condition but a dynamic process that is slow, progressive, and insidious. Its development typically stem from the long-term accumulation and interaction of multiple risk factors.10 This process may span years or even decades, making early-stage detection challenging. Furthermore, from a preventive perspective, lifestyle-related factors such as physical inactivity, sedentary behavior, and obesity can promote a pro-inflammatory state.11 This state worsens symptoms such as dyspnea and fatigue and accelerates the progression to disability. This multifactorial and prolonged process not only imposes sustained physical and psychological burdens on patients and generates direct economic pressures, but also further exacerbates the burden on the healthcare system. Through early identification, healthcare professionals can systematically assess older adults with COPD, identify individuals at high risk of future disability, and provide a critical window for timely intervention. Therefore, early identification of disability is essential for improving clinical outcomes and strengthening the comprehensive management of older adults with COPD.
Previous studies have investigated the causes of disability in patients with COPD and identified multiple physiological, psychological, and social factors.12 However, existing studies often examine these factors in isolation, such as lung function or physical performance. They rarely integrate prevalence data, assessment tools, and multidimensional determinants into a unified synthesis. Moreover, older adults with COPD form a clinically distinct subgroup. Age-related muscle loss, reduced functional reserve, a higher comorbidity burden, and greater vulnerability to psychosocial stressors increase both the risk and severity of disability compared with younger patients. However, this subgroup remains understudied in the existing literature. As scoping reviews are designed to map existing evidence and identify knowledge gaps within a research field, we adopted this scoping review framework to summarize the prevalence of disability, evaluate assessment instruments, and identify associated factors among older adults with COPD, with the aim of informing future research.
Materials and Methods
Scoping Review Question
This study used the PCC (Participant, Concept, and Context) framework proposed by Peters et al13 to define the study parameters as follows: P (Participant): Patients aged ≥60 years with stable COPD; C (Concept): Disability defined as impairment in basic activities of daily living (ADLs), including eating, dressing, and bathing; C (Context): Any setting in which the patient resides, including hospitals, nursing homes, community settings, or private homes. After team discussion, we formulated the following research questions: (1) What is the current status of disability in older adults with COPD? (2) What assessment tools are currently used to evaluate disability in older adults with COPD? (3) What factors are associated with disability in older adults with COPD?
Data Sources and Search Strategy
A combination of subject headings and free-text terms was used to search four English-language databases (Web of Science, PubMed, Embase, and Cochrane Library) and four Chinese-language databases (CNKI, Wanfang Data Knowledge Service Platform, VIP and China Biomedical Database). In addition, grey literature was searched through the OpenGrey and MedNar websites. The search covered the period from the inception of each database to October 31, 2025.
The search keywords were as follows. (1) Chinese search terms: elderly, senior, old age, aging, senescence, late life, senility; chronic obstructive pulmonary disease or COPD; disability, functional impairment, functional dependence, functional decline, activities of daily living, or ADL; influencing factors, risk factors, associated factors, or predictive factors. (2) English search terms: aged, elder, older adult, older person, older people, older individual, older patient, or old age; COPD or chronic obstructive pulmonary disease; disability, mobility limitation, activities of daily living, or ADL; risk factors, influencing factors, or associated factors.
The search strategies were as follows. (1) For English databases, PubMed was used as an example, and the search strategy is shown in Table 1. (2) For Chinese databases, CNKI was used as an example, and the search strategy is shown in Table 2.
 |
Table 1 Search Strategy for CNKI |
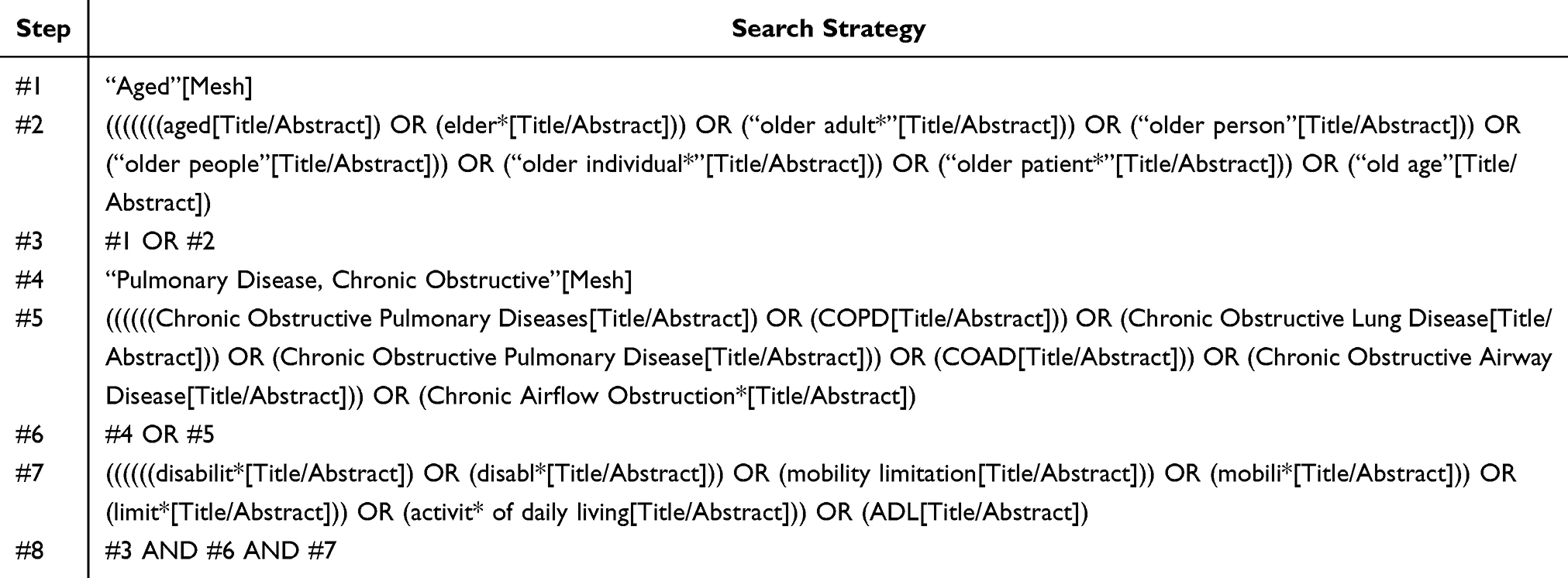 |
Table 2 Search Strategy for PubMed |
Study Selection Criteria
The inclusion criteria were as follows:
- Study population: Patients aged ≥60 years with stable chronic obstructive pulmonary disease (COPD) who met the diagnostic criteria of the 2021 Guidelines for the Diagnosis and Treatment of Chronic Obstructive Pulmonary Disease.2
- Research focus: Studies examining factors associated with disability in older adults with COPD.
- Study design: Original research articles, including quantitative, qualitative, and mixed-methods studies.
- Language: Articles published in English or Chinese.
The exclusion criteria were as follows:
- Full text unavailable.
- Duplicate publications.
Literature Screening and Data Extraction
This study was conducted by a dedicated research team, and all members received standardized methodological training. The literature screening process was carried out in three steps after the documents were imported into NoteExpress 3.5 for management and duplicate removal. First, two reviewers each randomly selected five articles for pre-screening. Titles and abstracts were independently reviewed, and relevance to the research questions was discussed until consensus was reached.Subsequently, all titles and abstracts were independently screened based on predefined inclusion and exclusion criteria. Finally, full-text articles that passed the initial screening were reviewed in detail. A secondary screening was conducted using the exclusion criteria, and the retained results were cross-checked. Data from articles with final agreement were extracted, summarized, and entered into an Excel spreadsheet. The extracted data included the first author, country, year of publication, study design, sample source, sample size, assessment tool, disability prevalence, and influencing factors.
Results
Results of the Literature Search
A total of 9621 records were retrieved in this study. After screening and exclusion, 12 studies were finally included. The literature screening process is shown in Figure 1.
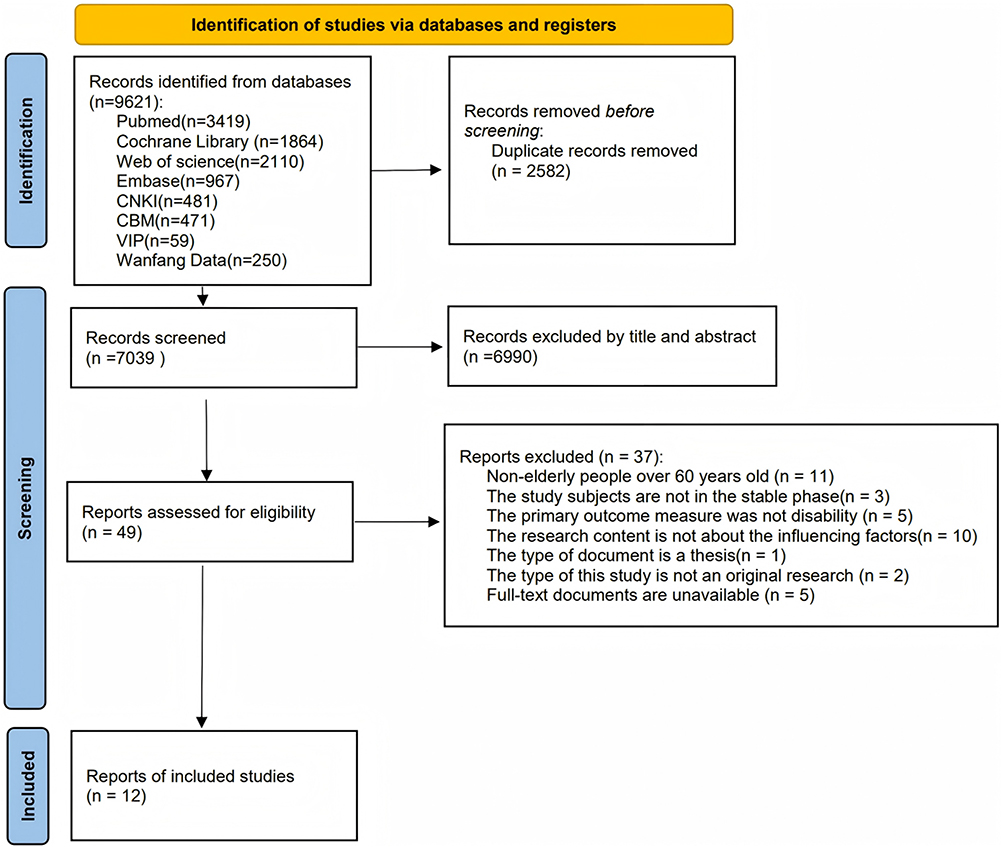 |
Figure 1 PRISMA flowchart of the scoping review. |
Basic Characteristics of the Included Studies
Twelve studies were included,14–25 including publications in both English14,15,18–20 and Chinese16,17,21–25 from China, Turkey, and Spain between 2006 and 2022. Sample sizes ranged from 80 to 6,047 participants. In particular, one study15 provided only subgroup data and results from univariate analyses (denoted by “/”). The basic characteristics of the included studies are shown in Table 3.
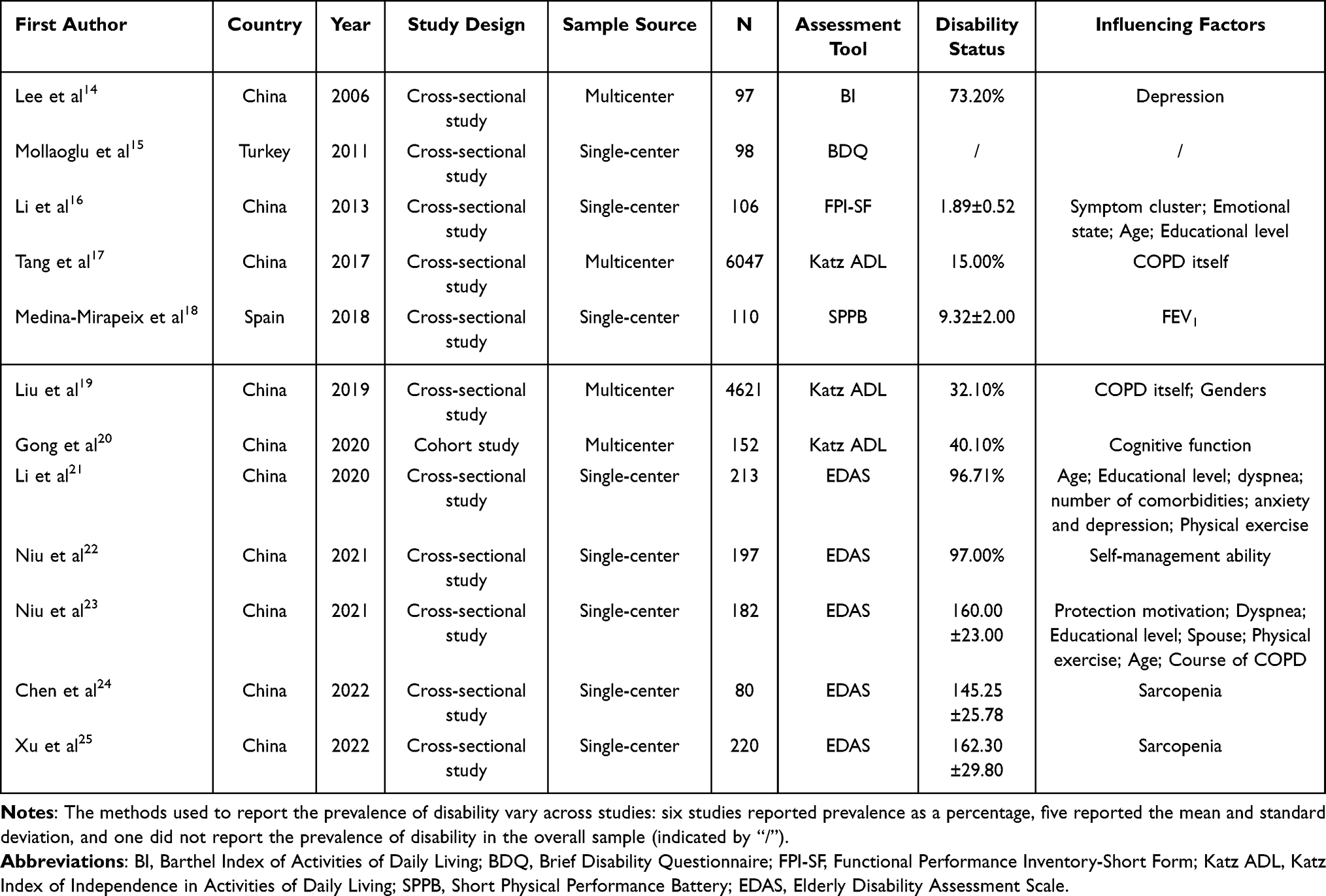 |
Table 3 Basic Characteristics of the Included Studies (n = 12) |
Current Status of Disability in Elderly Patients with COPD
- Study design: Cohort study (n=1),20 Cross-sectional study (n=11).14–19,21–25
- Study population: all elderly patients with COPD in a stable phase.
- Disability prevalence: six of the 12 included studies reported disability prevalence, ranging from 15.00% to 97.00%.14,17,19–22
- Assessment tools: six assessment tools were identified, including the BI (n=1), BDQ (n=1), FPI-SF (n=1), Katz ADL (n=3), SPPB (n=1), and EDAS (n=5). Detailed information is shown in Table 3.
Influencing Factors of Disability in Elderly Patients with COPD
Sociodemographic Factors
Sociodemographic factors were frequently reported in relation to disability among older patients with COPD. Advanced age,16,21,23 lower educational level,16,21,23 female sex,19 and absence of a spouse23 (Being without a spouse may increase the risk of functional limitations among older adults with COPD due to insufficient social support) were identified as factors associated with the presence of disability.
Disease-Related Factors
Disease-related characteristics were also commonly examined. Greater severity of symptom clusters,16 (A cluster of symptoms comprising shortness of breath, pain, anxiety, tension, sadness, sleep disturbances, and numbness and tingling in the hands and feet is significantly associated with functional status). COPD diagnosis itself,17,19 lower FEV1,18 severe dyspnea,21,23 a higher number of comorbidities,21 longer disease duration,23 and sarcopenia24,25 were reported to be associated with the presence of disability. Indicators reflecting worse pulmonary function and greater disease burden were more frequently linked to the occurrence of functional impairment.
Psychological and Behavioral Factors
Psychological and behavioral factors constituted another important category. Anxiety and depression,14,21 negative emotional states,16 cognitive impairment,20 low levels of physical activity,21,23 poor self-management,22 and low protection motivation23 (Low motivation to protect one’s health may increase the risk of disability among older adults with COPD by undermining their ability to maintain healthy behaviors) were identified as factors associated with the presence of disability. The above situation is shown in Figure 2.
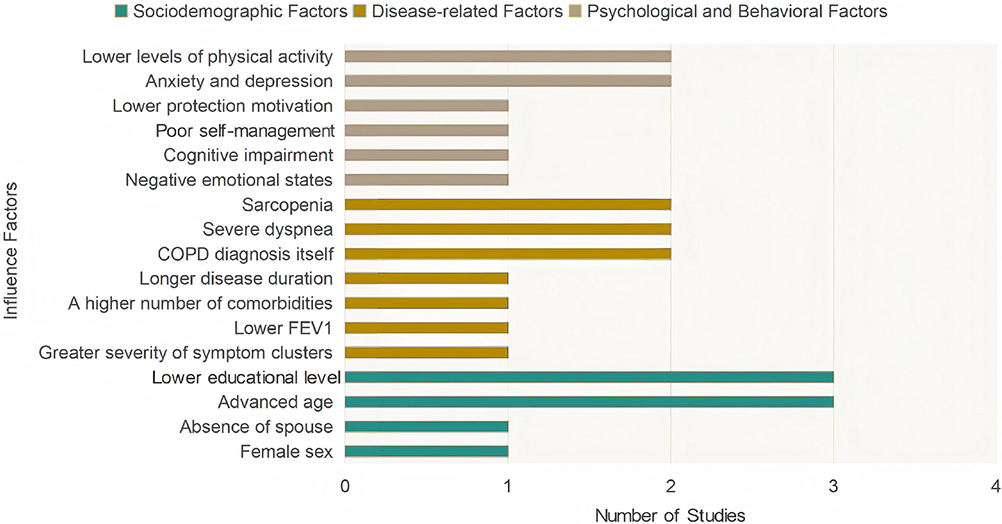 |
Figure 2 Distribution of factors influencing disability in older adults with COPD. Notes: Factors are grouped into three domains: sociodemographic factors (green), disease-related factors (yellow), and psychological and behavioral factors (brown). The length of each bar indicates how many of the 12 included studies identified that factor as significantly associated with disability in older adults with COPD. |
Discussion
Risk Identification and Development of Targeted Predictive Tools
Currently, reported rates of disability among older adults with COPD vary widely across studies (15.00%–97.00%). These differences in prevalence estimates are likely attributable to several factors. First, differences in sample sources (single-center versus multi-center studies), sample sizes (80 to 6,047 participants), and geographic settings may contribute to heterogeneity across study populations. Second, one cohort study reported a prevalence of 40.10%, whereas cross-sectional studies demonstrated greater variability, suggesting that differences in study design may also contribute to variations in prevalence estimates. Finally, differences in assessment tools are likely to be the most important contributor to this heterogeneity.
Due to differences in assessment scope and measurement sensitivity, various instruments may lead to substantial variation in identifying disability in older adults with COPD. For example, the Barthel Index primarily assesses 10 basic activities of daily living, including bathing, dressing, eating, toileting, transferring, and other activities, and has been associated with a reported disability prevalence of 73.20%.26 In contrast, the Katz Index focuses on six basic activities of daily living, with reported prevalence ranging from 15.00% to 40.10% across studies.27 Although these traditional geriatric scales are simple and widely used, they were not originally developed for patients with respiratory diseases. As a result, they may not adequately capture COPD-specific functional impairments, such as exertional dyspnea. In contrast, disease-specific tools may more sensitively capture COPD-related functional limitations. The SPPB provides objective performance-based measures through balance, gait speed, and chair stand tests.28 However, its use requires trained personnel and specialized equipment, which limits its feasibility in community and primary care settings. In this review, only one study conducted in Spain used the SPPB and reported a mean SPPB score of 9.32 ± 2.00 in the assessment of disability among older adults with COPD.18 This finding suggests that, although the included studies from China primarily relied on self-reported ADL measures, objective performance-based assessment tools may be more commonly used to assess disability in Western clinical settings. The study by Mollaoglu et al,15 conducted in Turkey, did not report disability outcomes for the overall sample and provided data only for specific subgroups. The BDQ used in that study primarily assesses dyspnea severity and emotional responses during daily activities; however, it places greater emphasis on symptom burden than on specific ADL performance.29 However, it focuses on symptom burden rather than specific ADL performance. The FPI-SF covers multiple domains, including daily living activities, housework, physical exercise, and social activities, and can more comprehensively reflect the daily functional performance of COPD patients.30 However, its psychometric validation in older COPD populations remains limited. Notably, the EDAS was associated with reported disability rates as high as 96.71%–97.00% across five studies. Grounded in the ICF framework, this scale includes seven domains, namely mental function, organ function, communication, activities, self-care, family life, and economic and social life.31 Its broader scope compared with traditional ADL scales increases sensitivity to mild functional limitations, which may partly explain higher disability detection rates. However, the EDAS emphasizes general functioning and social participation rather than COPD-specific activity limitations. Among currently available tools, the London Chest Activities of Daily Living Scale(LCADL) is theoretically more appropriate for COPD patients because it was specifically designed to assess COPD-related functional impairment and has been validated in respiratory populations.32 Nevertheless, the LCADL has several limitations. For example, the scale does not account for the impact of oxygen therapy on activity capacity. In addition, omission of certain items or non-response may distort total score calculation, thereby introducing information bias and underestimating the patient’s true level of disability. In contrast, the Manchester Respiratory Activities of Daily Living Questionnaire (MRADL) was specifically developed for patients with chronic obstructive pulmonary disease (COPD) and has been translated and validated in Chinese populations as the Chinese version of the MRADL Questionnaire (C-MRADLQ). The C-MRADLQ uses a 6-point scale (0–5) and includes 21 items across four domains: mobility, kitchen tasks, housework, and leisure activities. The total score ranges from 0 to 105, with higher scores indicating better functional performance.33 Nevertheless, the C-MRADLQ has primarily been validated in Hong Kong populations and has not been widely used in research settings in mainland China. Therefore, given the diversity of disability assessment tools and differences in clinical settings, tool selection should be based on a comprehensive consideration of clinical objectives, resource availability, and the characteristics of the target population. In resource-limited settings, the Katz Index or Barthel Index remains a practical strategy for routine screening of basic functional abilities because of their simplicity and widespread use. If clinical conditions permit objective assessment, the SPPB may serve as a reliable tool for evaluating physical function and fall risk. If broader functional dimensions, such as social participation, need to be assessed, the EDAS has high applicability; however, caution is warranted when interpreting its prevalence estimates because of the influence of its high sensitivity. If the goal is to precisely quantify COPD-specific activity limitations, the LCADL or C-MRADLQ may be preferable choices, although their validity in mainland Chinese populations requires further validation. Accordingly, within the context of Chinese research, a single scale is insufficient to fully characterize the overall profile of disability in this population. When conditions permit, a multidimensional assessment strategy that balances basic ADL performance with disease-specific functional limitations is recommended.
In summary, although COPD-specific instruments such as the LCADL and its Chinese adaptation, the C-MRADLQ, are available, all 12 studies included in this review relied on general assessment scales, and neither instrument has yet been applied to the assessment of disability in older adults with COPD in mainland China. These findings suggest that future research should first prioritize the introduction and validation of COPD-specific instruments, such as the C-MRADLQ, across different regions of mainland China, rather than continuing to rely on general scales that may fail to capture disease-specific functional impairments. Moreover, disability can be prevented and reversed.34 Therefore, early identification and timely intervention are crucial. Future studies could leverage machine learning and big data to develop disability risk prediction models for older adults with COPD, which could inform personalized intervention strategies.
Identifying Key Influencing Factors for Disability in Older Adults with COPD
The findings of this review can be interpreted within the COPD disability framework proposed by Locke et al, which is based on the disability process model developed by Jette and Verbrugge.35 This framework conceptualizes COPD-related disability as a dynamic process in which pathophysiological changes progressively lead to functional impairments, including respiratory and non-respiratory impairments, followed by functional limitations, and ultimately disability. This trajectory is influenced by both risk factors and other factors, including individual, social, and environmental factors. Within this framework, the disease-related factors identified in this review, such as reduced FEV1, sarcopenia, comorbidities, and longer disease duration, primarily correspond to impairments and functional limitations in COPD. Sociodemographic factors, including age, sex, educational level, and spousal support, act as risk factors that influence the overall progression from impairment to disability. Psychological and behavioral factors, such as depression, anxiety, cognitive impairment, and poor self-management ability, are considered other factors that may further affect patients’ functional maintenance and disease management. Importantly, these factors do not operate in isolation but may interact across different domains, collectively contributing to the progression of disability in this population. In addition to the three core domains discussed above, emerging mechanistic factors such as systemic inflammation and sleep disturbance may also play cross-domain mediating roles in the progression of disability. These factors may further accelerate functional decline by intensifying interactions among physiological dysfunction, psychological responses, and behavioral adaptation. These mechanisms are discussed in greater detail below.
Sociodemographic Factors
Age
Age was identified as an important factor associated with disability. Previous analyses of disability among older adults in China have shown that the prevalence of disability increases with age, with a particularly sharp rise among individuals aged ≥85 years and an approximate 7-percentage-point increase between age groups.36 This pattern may be explained by age-related physiological changes. With advancing age, individuals experience progressive physical decline, deterioration in overall health, and reduced organ function, which can substantially limit their capacity to perform daily activities. The risk becomes even greater among those with chronic diseases.37 In addition, aging is often accompanied by reduced appetite, inadequate protein intake, and loss of muscle mass, which may further accelerate functional decline and increase the likelihood of disability.38
Educational Attainment
Previous studies have reported that older adults with lower levels of education are more likely to experience disability than those with higher educational attainment. This disparity may be partly explained by their limited health literacy and inadequate understanding of disease-related knowledge. When facing health problems, individuals with lower educational attainment may have greater difficulty recognizing symptoms and adopting appropriate coping strategies, which may delay timely management, lead to worsening health conditions, and ultimately increase the risk of disability.39,40 Therefore, strengthening health education and disease knowledge dissemination in both hospital and community healthcare settings may be particularly important for older adults with COPD who have lower educational attainment. Such efforts may help them modify unhealthy lifestyle behaviors and develop appropriate health awareness.
Gender
Among older adults with COPD, women have a significantly higher risk of limitations in activities of daily living (ADL) than men. This disparity may result from several factors, including lower muscle strength, long-term engagement in physical labor, cumulative physical strain from caregiving roles, and relatively limited access to medical and social support among women.19 Furthermore, female patients may experience higher levels of negative emotions, greater sensitivity to symptoms such as dyspnea and pain, and a stronger tendency to avoid physical activities, which may further increase the risk of disability. Previous studies have also shown that older women have significantly higher disability rates than men and are more likely to experience functional decline. Therefore, future studies should consider developing targeted interventions that address gender-related differences.41
Spouses
As primary caregivers during the treatment and rehabilitation of older adults with COPD, spouses provide not only daily care but also important psychological support.42 Insufficient spousal support may lead to emotional distress and reduced motivation for physical activity, and prolonged inactivity may further increase the risk of disability. Efil et al43 reported that patients with COPD often limit their activities because of symptoms such as dyspnea, whereas emotional and practical support from spouses may reduce the perceived severity of breathlessness during daily activities and help patients maintain functional independence. Furthermore, a lack of spousal encouragement may negatively affect treatment adherence, which may result in delayed medical visits or inappropriate medication use. Some patients may also discontinue treatment because of financial constraints, which may worsen their condition and accelerate the progression of disability.
It is worth noting that sociodemographic factors do not act in isolation; rather, they interact with disease severity and patients’ psychological states in complex ways, contributing to the overall progression of disability. For example, older women with lower educational levels and limited social support often face barriers in accessing rehabilitation services and maintaining self-management. These disadvantages may not only exacerbate the impact of respiratory impairment on physical function but also highlight the need for targeted support in this vulnerable subgroup.
Disease-Related Factors
Symptom Clusters
Patients with COPD frequently experience multiple concurrent symptoms, typically ranging from 7 to 18, and these symptoms often show interrelated patterns that form symptom clusters.44 Previous studies have reported that emotional and respiratory symptom clusters are among the most common symptom patterns observed in patients with COPD.45 Studies also suggest that symptom clusters involving pain, fatigue, and emotional disturbances can substantially impair functional status and quality of life. These symptoms may interact synergistically and reinforce one another, which can further limit daily activities and social participation. Through these mechanisms, symptom clusters can further deteriorate overall functional status and may ultimately lead to disability.46
COPD and Dyspnea
Because of airflow limitation and dyspnea, patients with COPD often experience reduced exercise tolerance during physical activity, presenting with fatigue and shortness of breath. Recurrent exacerbations and repeated hospitalizations may lead to a gradual decline in patients’ physical activity levels over time. This decline may further aggravate respiratory dysfunction and ultimately contribute to the development of disability. In addition, clinical symptoms that occur after disease onset, including cough, sputum production, and progressive dyspnea, may trigger varying degrees of fear and depression, which may further accelerate disability progression.47,48
FEV1
COPD is characterized by varying degrees of airflow limitation, often manifested as reductions in FEV1. As the disease progresses, patients’ breathing patterns may change, which may lead to lung hyperinflation and diaphragmatic compression. Such changes may result in downward displacement of the diaphragm and limitation of diaphragmatic movement. In severe cases, diaphragmatic atrophy and weakness may develop, further impairing lung function.49 In addition, declining FEV1 may increase susceptibility to dyspnea and fatigue during physical exertion, which may directly limit patients’ ability to perform daily activities such as walking, climbing stairs, lifting objects, and other routine tasks. Meanwhile, reductions in exercise tolerance and in the sense of safety during physical activity may prompt patients to adopt activity-avoidance behaviors, which may indirectly accelerate the process of functional decline.18 Therefore, patients should adhere to standardized pharmacological treatment to prevent acute exacerbations, perform daily breathing exercises to improve ventilation efficiency, and undertake appropriate endurance training under medical supervision to enhance overall lung function. These measures may help reduce the risk of functional deterioration and improve patients’ quality of life.
Number of Comorbidities
Comorbidities are highly prevalent among patients with COPD. Previous studies have shown that more than 90% of patients have at least one comorbid condition, and nearly half present with four or more comorbidities, which significantly affect prognosis.50,51 Inflammatory responses are considered a key mechanism linking COPD with multiple diseases and can accelerate damage to target organs. In addition, inflammatory responses not only exacerbate pulmonary damage but may also damage the vascular endothelium and promote atherosclerosis, leading to reduced physical mobility in patients and an increased risk of disability. Evidence from epidemiological studies further supports this association. For example, one study reported that 92.15% of patients with COPD aged ≥60 years had multimorbidity, and a higher number of comorbidities was associated with a greater likelihood of disability.52 In addition, the coexistence of multiple chronic conditions may complicate treatment and increase overall symptom burden through interactions among multiple organ systems. This may reduce patients’ exercise capacity and daily activity levels, thereby hindering functional recovery and further increasing the risk of disability.
Prolonged Disease Course
COPD is characterized by complex pathology, a prolonged disease course, and recurrent exacerbations. As disease duration increases, patients’ clinical symptoms tend to become more severe, resulting in declines in multiple aspects of bodily function.53 This decline may manifest as progressively worsening dyspnea, reduced muscle mass, and impaired or atrophied skeletal muscle function, among others. Together, these changes increase the risk of disability.
Sarcopenia
The more severe dyspnea is in patients with COPD, the more likely the body is to develop hypoxia, thereby slowing muscle metabolic processes. Reduced quality of life further limits physical activity, and prolonged bed rest together with insufficient exercise can lead to muscle atrophy and contribute to the development of sarcopenia.54 As a common geriatric syndrome, sarcopenia is mainly manifested by impaired muscle function and reduced muscle strength. Sarcopenia increases the risk of falls, fractures, and disability in older adults and impairs their ability to perform daily activities and maintain quality of life. Among patients with chronic conditions such as COPD, the incidence of sarcopenia tends to increase.55
These disease-related functional impairments form the physiological basis of disability; however, their impact on function is influenced by sociodemographic factors as well as patients’ psychological responses and behavioral adaptations. Taking multimorbidity as an example, although the accumulation of comorbidities increases treatment complexity and symptom burden, patients with higher educational levels and better self-management skills often show greater ability to cope with complex therapies and maintain functional independence. Therefore, the progression of disability depends not only on biological interactions between diseases but also reflects the interaction between pathological stress and psychosocial resources.
Psychological and Behavioral Factors
Negative Emotions, Particularly Anxiety and Depression
Due to the chronic nature of COPD, patients not only experience significant impairments in physiological health, such as lung function, but also face prolonged treatment and persistent physical discomfort, which intensify psychological burdens and trigger various negative emotions, among which anxiety and depression are particularly prominent and common in Chinese patients.56,57 As the disease progresses, patients with COPD often develop anxiety due to fears of breathlessness, concerns about engaging in physical activity, and worries about future disease progression or even death. This anxiety can lead patients to avoid activities and reduce social interaction, thereby contributing to the onset of disability. Simultaneously, depression may reinforce negative perceptions of the disease and promote a sedentary lifestyle, reducing motivation and interest in daily activities. These behavioral and psychological changes further decrease physical activity and social engagement, ultimately increasing the risk of disability.48
Cognitive Impairment
Performing daily activities requires intact cognitive functions, including planning, problem-solving, memory, and attention. If cognitive function declines, older adults may encounter difficulties performing daily activities. Over time, these difficulties may reduce participation in activities, thereby increasing the risk of disability.58 Evidence suggests that cognitive impairment is closely linked to older adults’ ability to perform activities of daily living, and those with declining cognitive function are more likely to experience disability.59 Cognitive impairment often coexists with anxiety and depression, and these factors may interact to jointly influence the course of disability. Feng Xiaochun et al60 reported that depression mediates the relationship between cognitive impairment and disability. Older adults with chronic diseases are at higher risk of depression, and depressive states are frequently accompanied by abnormalities in neural regions such as the amygdala and hippocampus. These neural abnormalities may directly impair cognitive function, thereby contributing to disability.
Self-Management Capacity
Self-management capacity among older adults with COPD is negatively correlated with disability severity, that is, lower self-management capacity is associated with more severe disability.61 Effective self-management encourages patients to adopt health-promoting beliefs and actively modify lifestyle behaviors, thereby improving quality of life and reducing acute exacerbations.62 In the prevention, treatment, and management of chronic diseases, recovery depends not only on professional healthcare services but also on patients’ active engagement in daily disease management. Patients with stronger self-management abilities are more likely to adhere to treatment, maintain healthier lifestyles, and respond more effectively to disease-related symptoms. These behaviors may help maintain functional capacity and potentially reduce the risk of disability in older adults with COPD.
Protection Motivation
Protection Motivation Theory emphasizes influencing health behavior decisions by regulating individuals’ cognitive processes and highlights the role of internal cognitive factors in behavior change. It enhances patients’ awareness of health management and promotes active engagement in health-related actions by guiding them to identify and reflect on unhealthy behaviors and cognitive biases, encouraging them to share experiences related to unhealthy lifestyle behaviors, and facilitating peer exchange of experiences. Based on this process, strengthening patients’ understanding of healthy lifestyles can motivate them to increase physical activity and adopt healthier behavioral habits, thereby reducing the risk of disability onset.63,64
Exercise
Exercise behavior among patients with COPD is often unsatisfactory, and exercise adherence tends to decline gradually over time after hospital discharge. This may be attributed to several factors, including advanced age, dyspnea, and insufficient social support, which may lead patients to develop avoidance toward exercise or daily activities. As a result, patients may reduce exercise and lower their overall activity levels. This trend may further exacerbate muscle wasting and disease progression, creating a vicious cycle that ultimately increases the risk of disability.65,66 From a functional perspective, regular physical activity plays an important role in maintaining muscle strength, exercise tolerance, and overall physical function in patients with COPD.
In summary, psychological and behavioral factors are important contributors to the progression of disability and may form a bidirectional feedback relationship with sociodemographic and disease-related factors described above. When patients face the dual challenges of dyspnea and sarcopenia, depression and anxiety may further reinforce avoidance of daily activities. Furthermore, due to lower educational levels and limited social support, patients often exhibit reduced self-management capacity and lower motivation for health protection, which makes it difficult for them to actively adopt healthy compensatory behaviors and may ultimately lead to progressive functional decline.
Emerging Mechanistic Factors and Their Interactions with Core Domains
In addition to the aforementioned sociodemographic, disease-related, and psychological and behavioral factors, recent studies suggest that additional mechanistic factors may also contribute to disability progression, although evidence in elderly patients with chronic obstructive pulmonary disease (COPD) remains limited. Systemic inflammation is one emerging factor that has received increasing attention. Patients with COPD often exhibit elevated levels of inflammatory markers, such as IL-6, TNF-α, and CRP, and chronic inflammation may contribute to disability progression through multiple pathways. At the disease-related level, persistent inflammation may promote muscle atrophy and accelerate the development of sarcopenia, thereby contributing to impaired physical function. In addition, inflammation may disrupt osteoclast activity and osteoblast differentiation, accelerate osteoporosis progression, increase fracture risk, and further limit the ability to perform daily activities.67 Inflammatory cytokines are also closely associated with depression and cognitive decline, suggesting that systemic inflammation may represent a potential mechanistic link between disease-related and psychological factors.68 Therefore, systemic inflammation may act not only as a biological factor but also as a potential mediator in the transition from physiological dysfunction to psychological and functional decline. Sleep disturbance is another potential factor that has received limited attention despite its possible clinical relevance. COPD-related respiratory impairment may lead to nocturnal hypoxemia and hypercapnia, which can contribute to sleep disruption and poor sleep quality. Chronic sleep deprivation may further exacerbate inflammatory responses and metabolic disturbances, potentially creating a bidirectional cycle between respiratory dysfunction and sleep disturbance and further aggravating disease-related functional impairment.69,70 Furthermore, poor sleep quality is associated with increased fatigue, reduced willingness to engage in physical activity, and impaired cognitive function.71 These changes may further affect patients’ psychological and behavioral states and contribute to functional decline. Conversely, reduced physical activity may lead to respiratory muscle deconditioning and worsened nocturnal hypoxemia, potentially perpetuating a cycle between sleep disturbance and functional decline.
In summary, because most included studies employed cross-sectional designs and lacked biomarker data and systematic sleep assessments, the mediating roles of these potential mechanisms in disability progression remain unclear. Overall, this review suggests that disability in older adults with chronic obstructive pulmonary disease (COPD) is not attributable to a single factor but arises from the interaction of sociodemographic, disease-related, and psychological and behavioral factors.12 This finding suggests that future research should move beyond the isolated examination of individual risk factors and focus on interactive mechanisms across domains. For example, future studies may examine whether depression moderates the relationship between dyspnea and functional limitation. In addition, comprehensive intervention strategies that address physiological, psychological, and behavioral domains may help delay functional decline and improve outcomes.
Limitations
Although this scoping review describes the current status of disability and its influencing factors among older adults with COPD, several limitations may affect the generalizability and reliability of the findings. First, this study primarily conducted a descriptive analysis of the included literature and did not perform a formal quality assessment. Because the included studies differed substantially in methodological design and sample size, the quality of the studies underlying this review varied considerably. This heterogeneity may introduce certain biases and limitations when interpreting the relevant findings. Second, many of the included studies were cross-sectional, which prevents confirmation of causal relationships between the identified factors and disability in older adults with COPD. Furthermore, most of the included studies were conducted in China, with only a few conducted in other countries, such as Turkey and Spain. This geographical distribution reflects the current state of the literature and suggests that research on disability among older adults with COPD remains geographically concentrated, potentially limiting the generalizability and external validity of the findings. Countries differ in healthcare systems, socioeconomic conditions, and rehabilitation resources, and these factors may influence both the prevalence of disability among older adults with COPD and its related factors. Future research should include large-scale, multicenter, prospective studies conducted in more countries and across diverse cultural contexts. Such studies may help compare the similarities and differences in disability progression among older adults with COPD across different healthcare systems and sociocultural environments and further validate the stability and cross-cultural applicability of existing findings.
Conclusion
This scoping review systematically summarizes disability among older adults with COPD from three perspectives: prevalence, assessment tools, and influencing factors. Current evidence suggests that disability in this population is multidimensional and dynamic, and is closely associated with interactions among sociodemographic, disease-related, and psychological and behavioral factors. However, current assessment and understanding still rely primarily on general geriatric assessment tools, and validated COPD-specific assessment instruments for mainland Chinese populations remain lacking. This limitation may affect the accuracy of disability estimation and the sensitivity of clinical identification. From a clinical perspective, the marked variation in prevalence and the multifactorial nature of disability suggest that assessment of older adults with COPD should extend beyond isolated physiological indicators to incorporate multidimensional factors such as psychological, cognitive, and social support factors, thereby enabling more comprehensive clinical identification and management. At the same time, this multifactorial nature also highlights the need for intervention strategies to shift from single-target approaches to comprehensive, multilevel management models. In light of these findings, future research should focus on three key areas. First, COPD-specific assessment tools suitable for mainland Chinese populations, such as localized versions of the C-MRADLQ or LCADL, should be developed and prospectively validated to establish standardized and sensitive measurement standards. Second, longitudinal cohort studies are needed to clarify the dynamic trajectories of disability and their potential causal pathways. Third, quantitative and qualitative methods should be combined to further explore patients’ lived experiences and unmet care needs, thereby informing more targeted intervention strategies.
Acknowledgement
Xiangru Huang is the sole first author and Haixia Li is the sole corresponding author, in this article.
Funding
This study was supported by the Special Project for Central Guidance on Local Science and Technology Development in the Ningxia Hui Autonomous Region, with ethics approval number [2024]-ZDYF-078.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Wang Z, Lin J, Liang L, et al. Global, regional, and national burden of chronic obstructive pulmonary disease and its attributable risk factors from 1990 to 2021: an analysis for the Global Burden of Disease Study 2021. Respir Res. 2025;26(1):2. doi:10.1186/s12931-024-03051-2
2. Kai Z. Analysis of the prevalence and influencing factors of chronic diseases in the elderly in China underthe background of population aging. Master’s degree. Nanjing University of Posts and Telecommunications; 2021. doi:10.27251/d.cnki.gnjdc.2021.001461.
3. Li M, Hanxiang C, Na Z, et al. Burden of COPD in China and the global from 1990 to 2019: a systematic analysis for the Global Burden of Disease Study 2019. BMJ Open Respir Res. 2023;10(1):1. doi:10.1136/bmjresp-2023-001698
4. Changhonmg Z, Jianhua L, Jianqing Z, et al. Epidemiology of Chronic Obstructive Pulmonary Disease in the Elderly Population and Its Influencing Factors. Chin J Gerontol. 2023;43(19):4851–16.
5. Collaborators GF. Burden of disease scenarios for 204 countries and territories, 2022–2050: a forecasting analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403(10440):2204–2256. doi:10.1016/s0140-6736(24)00685-8
6. WHO. International Classification of Impairments, Disabilities, and Handicaps: A Manual of Classification Relating to the Consequences of Disease; 1980.
7. WHO. International Classification of Functioning, Disability and Health: ICF. World Health Organization; 2001.
8. Jiménez Buñuales MT, González Diego P, Martín Moreno JM. International classification of functioning, disability and health (ICF) 2001. Rev Esp Salud Publica. 2002;76(4):271–279. doi:10.1590/s1135-57272002000400002
9. Lisy K, Campbell JM, Tufanaru C, Moola S, Lockwood C. The prevalence of disability among people with cancer, cardiovascular disease, chronic respiratory disease and/or diabetes: a systematic review. Int J Evid Based Healthc. 2018;16(3):154–166. doi:10.1097/xeb.0000000000000138
10. Xuehui W. Research on Theoretical Rethinking and Measurement of Disability among Chinese Older Population. Ningxia Soc Sci. 2020;5:147–155.
11. Mattioli AV, Coppi F, Nasi M, Pinti M, Gallina S. Long COVID: a New Challenge for Prevention of Obesity in Women. Am J Lifestyle Med. 2023;17(1):164–168. doi:10.1177/15598276221111054
12. Yuping L, Jianping S. Research progress of disability in patients with chronic obstructive pulmonary disease. J Nurs Sci. 2020;35(01):102–106.
13. Peters MDJ, Marnie C, Tricco AC, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evid Implement. 2021;19(1):3–10. doi:10.1097/xeb.0000000000000277
14. Lee IF, Lee DT, Mackenzie AE. Correlates of functional limitations in older Chinese patients with chronic obstructive pulmonary disease in Hong Kong. Heart Lung. 2006;35(5):324–333. doi:10.1016/j.hrtlng.2006.05.004
15. Mollaoglu M, Fertelli TK, Tuncay F. Fatigue and disability in elderly patients with chronic obstructive pulmonary disease (COPD). Arch Gerontol Geriatr. 2011;53(2):e93–e98. doi:10.1016/j.archger.2010.07.001
16. Yanling L, Lu C, Lina S, Ying W, Haisong Z. The Impact of Chronic Obstructive Pulmonary Disease Symptom Complex on Functional Status in Elderly Patients. Guangdong Med J. 2013;34(21):3319–3322. doi:10.13820/j.cnki.gdyx.2013.21.032
17. Haibo T, Xufeng Z, Jian Z, et al. Study on chronic obstructive pulmonary disease and disability among rural elderly in China. Occupation Health. 2017;33(19):2663–2665+2669. doi:10.13329/j.cnki.zyyjk.2017.0796
18. Medina-Mirapeix F, Bernabeu-Mora R, Sánchez-Martínez MP, Montilla-Herrador J, Bernabeu-Mora M, Escolar-Reina P. Mobility limitations related to reduced pulmonary function among aging people with chronic obstructive pulmonary disease. PLoS One. 2018;13(5):e0196152. doi:10.1371/journal.pone.0196152
19. Liu M, Yue Y, He Y. Association between chronic obstructive pulmonary disease and activity of daily living among oldest-old in China: based on Chinese Longitudinal Health Longevity Survey. Int J Chron Obstruct Pulmon Dis. 2019;14:1959–1966. doi:10.2147/copd.S215803
20. Gong B, Shang S, Wu C. Association between cognitive declines and disability in activities of daily living in older adults with COPD: evidence from the China health and retirement longitudinal study. BMJ Open. 2020;10(10):e040098. doi:10.1136/bmjopen-2020-040098
21. Yuping L, Jianping S, Hongxia W, Guifang N, Liping L. Investigation on the current status and influencing factors of disability in elderly chronic obstructive pulmonary diseases patients. Nursing Pract Res. 2020;17(12):5–9.
22. Guifang N, Jianping S, Yuping L, Zhilan Y, Ruili S. Correlation analysis between self-management ability and disability in elderly patients with COPD. Chin Evidence Based Nurs. 2021;7(06):795–798.
23. Guifang N, Jianping S, Yuping L, Hua Z, Zhilan Y, Ruili S. Correlation between protective motivation and disability in elderly patients with COPD. Chinese Remedies & Clinics. 2021;21(20):3365–3368.
24. Pei C, Jingfeng W, Xinfang W, Fuxiao Y, Jing J. Observation of the Effect of Sarcopenia on Disability and Quality of Life in Elderly Patients with Stable Chronic Obstructive Pulmonary Disease. J Chin Foreign Medi Pharmacy Res. 2022;1(8):9–11. doi:10.3969/j.issn.2096-6229.2022.08.003
25. Jie X, Hong W, Jing D, Fuchao L, Jie N. The Impact of Sarcopenia on Disability and Quality of Life in Elderly Patients with Stable Chronic Obstructive Pulmonary Disease. Chin Prevent Med. 2022;23(02):146–149. doi:10.16506/j.1009-6639.2022.02.012
26. Mahoney FI, Barthel DW. FUNCTIONAL EVALUATION: THE BARTHEL INDEX. Md State Med J. 1965;14:61–65.
27. Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. STUDIES OF ILLNESS IN THE AGED. THE INDEX OF ADL: a STANDARDIZED MEASURE OF BIOLOGICAL AND PSYCHOSOCIAL FUNCTION. JAMA. 1963;185:914–919. doi:10.1001/jama.1963.03060120024016
28. Guralnik JM, Winograd CH. Physical performance measures in the assessment of older persons. Aging. 1994;6(5):303–305. doi:10.1007/bf03324256
29. Stewart AL, Hays RD, Ware Jr JE. The MOS short-form general health survey. Reliability and validity in a patient population. Med Care. 1988;26(7):724–735. doi:10.1097/00005650-198807000-00007
30. Leidy NK, Knebel A. In search of parsimony: reliability and validity of the Functional Performance Inventory-Short Form. Int J Chron Obstruct Pulmon Dis. 2010;5:415–423. doi:10.2147/copd.S13389
31. Ming Y, Li L, Jiaojiao J, et al. Development of the elderly disability assessment scale (II): the selection of items for the formal version. Chin J Rehabil Med. 2014;29(03):212–217.
32. Carpes MF, Mayer AF, Simon KM, Jardim JR, Garrod R. The Brazilian Portuguese version of the London Chest Activity of Daily Living scale for use in patients with chronic obstructive pulmonary disease. J Bras Pneumol. 2008;34(3):143–151. doi:10.1590/s1806-37132008000300004
33. Siu DCH, So CT, Lau CWL, et al. The Manchester Respiratory Activities of Daily Living Questionnaire: reliability and Validity of the Chinese Version with Pictorial Enhancement. Int J Chron Obstruct Pulmon Dis. 2021;16:91–100. doi:10.2147/copd.S283769
34. Boyd CM, Landefeld CS, Counsell SR, et al. Recovery of activities of daily living in older adults after hospitalization for acute medical illness. J Am Geriatr Soc. 2008;56(12):2171–2179. doi:10.1111/j.1532-5415.2008.02023.x
35. Locke E, Thielke S, Diehr P, et al. Effects of respiratory and non-respiratory factors on disability among older adults with airway obstruction: the Cardiovascular Health Study. COPD. 2013;10(5):588–596. doi:10.3109/15412555.2013.781148
36. Jinying W, Tianran L. The Age Mode of Elderly Disability in China and the Disabled Population Projection. Population J. 2020;42(05):57–72. doi:10.16405/j.cnki.1004-129X.2020.05.005
37. Denninger T. Disability and age-observations from an intersectional perspective. Z Gerontol Geriatr. 2020;53(3):211–215. doi:10.1007/s00391-020-01693-7
38. Yuanyuan L, Jin C, Xiujuan Y, Lingjie X, Dandan L. Influencing factors of disability degree and correlations of disability with malnutrition and sarcopenia in elderly hospitalized patients with disability. J Clin Med Pract. 2024;28(07):67–71.
39. Bin L, Mengfei G. Research on the Disability Situation and Influencing Factors of Elderly People Aged 65 and Over in China: analysis Based on 2018 CLHLS Data. J Chongqing Technol Business Univ. 2024;41(06):130–141.
40. Zehui J, Cai X, Jun Z. Analysis of the Current Situation and Influencing Factors of Disability of the Elderly based on the Theory of Health Ecology. Health Econom Res. 2025;42(05):7–10+15. doi:10.14055/j.cnki.33-1056/f.2025.05.018
41. Xinping L, Zhanhong Z, Yong W. Research on gender differences in functional trajectories among older adults and their influencing factors:an empirical analysis based on CHARLS data from 2011 to 2020. J Nanjing Med Univ. 2025;25(06):557–566.
42. Jingjing Z, Zhihua W, HuiYing W, Yanling W, Yongrui W. Multidimensional Care Incorporating Partner Involvement in Goal Implementation: intervention Outcomes for Elderly COPD Patients. Int J Nurs. 2022;41(10):1857–1863. doi:10.3760/cma.j.cn221370-20200705-00480
43. Efil S, Kalkan Ugurlu Y, Akça Doğan D, Budak D. Perceived Spousal Support and Activities of Daily Living in Individuals With COPD. West J Nurs Res. 2024;46(6):436–444. doi:10.1177/01939459241248218
44. Christensen VL, Holm AM, Cooper B, Paul SM, Miaskowski C, Rustøen T. Differences in Symptom Burden Among Patients With Moderate, Severe, or Very Severe Chronic Obstructive Pulmonary Disease. J Pain Symptom Manage. 2016;51(5):849–859. doi:10.1016/j.jpainsymman.2015.12.324
45. Fei F, Koffman J, Zhang X, Gao W. Chronic Obstructive Pulmonary Disease Symptom Cluster Composition, Associated Factors, and Methodologies: a Systematic Review. West J Nurs Res. 2022;44(4):395–415. doi:10.1177/0193945921995773
46. Xiaoting Q, Fengxiang S, Zhimei L, Ke S, Kaixuan W. Study on Potential Categories of Symptom Clusters in COPD Patients and Risk Prediction Analysis. J Qilu Nursing. 2021;27(01):42–45.
47. Zhuozhuo C. Analysis of the Impact of Multimorbidity and COPD Comorbidities on ADL Based on CHARLS Data and Hospitalized COPD Patients. Master’s degree. Guangzhou Medical University; 2025. doi:10.27043/d.cnki.ggzyc.2025.000733.
48. Keil DC, Stenzel NM, Kühl K, et al. The impact of chronic obstructive pulmonary disease-related fears on disease-specific disability. Chron Respir Dis. 2014;11(1):31–40. doi:10.1177/1479972313516881
49. Feifei K. The Effectiveness of Breathing Training in Patients with Chronic Obstructive Pulmonary Disease. Med J Chinese People’s Health. 2020;32(19):165–167.
50. Dian C, Huanyu L, Congxi Z, Lanhe C, Shurun L, Yahong C. Interpretation of Global Strategy for the Diagnosis, Treatment,Management and Prevention of Chronic Obstructive Pulmonary Disease 2025 Report. Chinese General Practice. 2025;28(16):1937–1949.
51. Trudzinski FC, Jörres RA, Alter P, et al. Sex-specific associations of comorbidome and pulmorbidome with mortality in chronic obstructive pulmonary disease: results from COSYCONET. Sci Rep. 2022;12(1):8790. doi:10.1038/s41598-022-12828-8
52. Liu X, Cao Y, Shi Y, Ding H. Association between multimorbidity and disability among elderly with chronic obstructive pulmonary disease in Shanghai, China: a cross-sectional study. BMC Geriatr. 2025;25(1):901. doi:10.1186/s12877-025-06488-2
53. Jing G. A Survey on the Correlation Between Disease Perception, Self-Management, and Quality of Life Among COPD Patients. Modern Nurse. 2022;29(12):102–105. doi:10.19793/j.cnki.1006-6411.2022.36.027
54. Chang W, Shimiao H, Wenhui M, Lina S. Influencing factors and predictive models of sarcopenia complicated with chronic obstructive pulmonary disease in the elderly. Chin J Gerontol. 2025;45(19):4658–4661.
55. He J, Li H, Yao J, Wang Y. Prevalence of sarcopenia in patients with COPD through different musculature measurements: an updated meta-analysis and meta-regression. Front Nutr. 2023;10:1137371. doi:10.3389/fnut.2023.1137371
56. Haohao L, Zhuoqun L. Influence of chronic diseases on depressive symptoms among older adults. Chin J Health Educ. 2024;40(06):525–530. doi:10.16168/j.cnki.issn.1002-9982.2024.06.009
57. Huang K, Huang K, Xu J, et al. Anxiety and Depression in Patients with Chronic Obstructive Pulmonary Disease in China: results from the China Pulmonary Health [CPH] Study. Int J Chron Obstruct Pulmon Dis. 2021;16:3387–3396. doi:10.2147/copd.S328617
58. Wenlong T. Study on the Current Status and Influencing Factors of ADL among Rural Elderly Patients with Chronic Disease in Shandong Province: Based on the Cumulative Complexity Model. Master’s degree. Shandong University; 2024. doi10.27272/d.cnki.gshdu.2024.004447.
59. Ai F, Li E, Dong A, Zhang H. Association between disability and cognitive function in older Chinese people: a moderated mediation of social relationships and depressive symptoms. Front Public Health. 2024;12:1354877. doi:10.3389/fpubh.2024.1354877
60. Xiaochen F, Yongqiang W, Xin W, et al. The impact of activities of daily living on cognitive function in elderly individuals with chronic comorbidities:the chain mediating effects of social participation and depression. Mod Preventive Med. 2024;51(19):3576–3582. doi:10.20043/j.cnki.MPM.202405325
61. Yang Z. Effects Of Health Literacy And Self-Management Ability On Disability In Patients With COPD. Master’s degree. Yanbian University; 2022. doi:10.27439/d.cnki.gybdu.2022.000499.
62. Wang T, Tan JY, Xiao LD, Deng R. Effectiveness of disease-specific self-management education on health outcomes in patients with chronic obstructive pulmonary disease: an updated systematic review and meta-analysis. Patient Educ Couns. 2017;100(8):1432–1446. doi:10.1016/j.pec.2017.02.026
63. Aihong X. Effect of Protective Motivation Theory-based Nursing Intervention on Self-care Ability of Elderly Patients with Chronic Diseases. J Nursing. 2021;28(16):47–51. doi:10.16460/j.issn1008-9969.2021.16.047
64. Wenying L. The Effect of Nursing Interventions Based on Protective Motivation Theory on Health Behaviors and Lung Function in Elderly COPD Patients. Inner Mongolia Med J. 2023;55(01):123–125+128. doi:10.16096/J.cnki.nmgyxzz.2023.55.01.035
65. Di Y, Meizhu D. Qualitative study of kinesiophobia in pulmonary rehabilitation in patients with chronic obstructive pulmonary disease. Clin Res Pra. 2025;10(31):36–40. doi:10.19347/j.cnki.2096-1413.202531009
66. Huan T, Guihua C, Qin L, Xixin Z, Xiucen W, Penghua S. Analysis of distribution characteristics on exercise behavior stages and its predictive factors in patients with chronic obstructive pulmonary disease after discharge. Chin J Nurs. 2024;59(17):2084–2092.
67. Inoue D, Inoue R. Mechanisms of osteoporosis associated with chronic obstructive pulmonary disease. J Bone Miner Metab. 2024;42(4):428–437. doi:10.1007/s00774-024-01527-1
68. Strollo HC, Nouraie SM, Hoth KF, et al. Association of Systemic Inflammation with Depressive Symptoms in Individuals with COPD. Int J Chron Obstruct Pulmon Dis. 2021;16:2515–2522. doi:10.2147/copd.S322144
69. Huang T, Mariani S, Redline S. Sleep Irregularity and Risk of Cardiovascular Events: the Multi-Ethnic Study of Atherosclerosis. J Am Coll Cardiol. 2020;75(9):991–999. doi:10.1016/j.jacc.2019.12.054
70. Hui T, Deshuai L. Influencing factors of sleep quality in patients with chronic obstructive pulmonary disease. Med J Chinese People’s Health. 2025;37(16):5–7.
71. Chen J, Chen X, Mao R, et al. Hypertension, sleep quality, depression, and cognitive function in elderly: a cross-sectional study. Front Aging Neurosci. 2023;15:1051298. doi:10.3389/fnagi.2023.1051298
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effects of a Mind-Body Program for Chronic Pain in Older versus Younger Adults
LaRowe LR, Bakhshaie J, Vranceanu AM, Greenberg J
Journal of Pain Research 2023, 16:3917-3924
Published Date: 15 November 2023
The Double-Edged Sword of Intergenerational Support: A Cross-Sectional Study on Caregiver Burden Among Chinese Families Caring for Stroke Survivors with Disabilities
Yang G, Hu P, Bao S, Shu M, Dong J, Yu Y
Journal of Multidisciplinary Healthcare 2026, 19:605802
Published Date: 9 June 2026