Back to Journals » Breast Cancer: Targets and Therapy » Volume 18
The Correlation Between CD8+ Tumor-Infiltrating Lymphocytes and the Efficacy of Neoadjuvant Therapy in Breast Cancer
Authors Feng G, Zhong M, Xie D, Yuan X, Lu S, Zhu J, Gao S, Yi Z, Lin H, Zheng J, Zhou H, Wang Y
Received 11 August 2025
Accepted for publication 14 January 2026
Published 10 March 2026 Volume 2026:18 533799
DOI https://doi.org/10.2147/BCTT.S533799
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Guosheng Feng,1 Mingqiang Zhong,2 Danmin Xie,1 Xianbin Yuan,1 Shui Lu,1 Jianfang Zhu,1 Shan Gao,1 Zhongqiu Yi,3 Haiyong Lin,4 Jinlin Zheng,4 Hongyu Zhou,5 Yanjing Wang5
1Department of Medical Oncology, The People’s Hospital of Guangxi Zhuang Autonomous Region, Nanning, People’s Republic of China; 2Department of Medical Oncology, Zigong First People’s Hospital, Zigong, People’s Republic of China; 3Department of Medical Research, The People’s Hospital of Guangxi Zhuang Autonomous Region, Nanning, People’s Republic of China; 4Department of Medical Oncology, Pingnan Second People’s Hospital, Pangnan, People’s Republic of China; 5Department of Medical Oncology, Qianhai Life Nanning Hospital, Nanning, People’s Republic of China
Correspondence: Guosheng Feng, The People’s Hospital of Guangxi Zhuang Autonomous Region, No. 6 Taoyuan Road, Nanning, Guangxi Zhuang Autonomous Region, 530021, People’s Republic of China, Email [email protected]; [email protected]
Objective: This study aims to investigate the correlation between the CD8+ tumor-infiltrating lymphocytes (TILs) expression and the efficacy of neoadjuvant therapy (NAT) in breast cancer, while previous studies have reported inconsistent findings regarding the predictive value of CD8+ TILs.
Methods: Data from 94 breast cancer patients who underwent NAT between January 2017 and June 2019 were retrospectively analyzed. Preoperative CD8+ TILs expression was evaluated through immunohistochemistry, and its association with clinical and pathological responses to NAT was assessed.
Results: Univariate analysis indicated that tumor stage, axillary lymph node status, and intratumoral CD8+ TILs were correlated with clinical complete response (cCR). Multivariate analysis identified intratumoral CD8+ TILs as an independent predictor of cCR (OR 3.038; p=0.02). Patients achieving pathological complete response (pCR) exhibited significantly higher intratumoral CD8+ TILs expression compared to those without (p=0.04). Univariate analysis also linked estrogen receptor (ER), progesterone receptor (PR), HER2 status, and intratumoral CD8+ TILs to pCR, with multivariate analysis confirming intratumoral CD8+ TILs as an independent predictor (OR 4.036; p=0.02).
Conclusion: Our findings suggest that intratumoral CD8+ TILs are an independent predictor of the efficacy of neoadjuvant therapy in breast cancer. In the future, incorporating intratumoral CD8+ TILs into existing clinicopathological predictive models and combining their assessment with other immune biomarkers may enable the development of more robust predictive tools, thereby providing a solid foundation for truly individualized and precision-based neoadjuvant treatment in breast cancer.
Keywords: Breast cancer, Neoadjuvant therapy, Efficacy prediction, Tumor-infiltrating lymphocytes, CD8+ TILs
Introduction
Breast cancer is the most common malignancy and the leading cause of cancer-related mortality among women in China, posing a substantial public health burden1 Neoadjuvant therapy (NAT) has become a standard treatment strategy for patients with locally advanced and selected early-stage breast cancer. The primary objectives of NAT are to downstage tumors, increase the feasibility of breast-conserving surgery, and provide an in vivo assessment of chemosensitivity to guide subsequent treatment decisions. Patients who achieve a pathological complete response (pCR) after NAT experience significantly prolonged disease-free survival and overall survival2 However, NAT is also associated with potential risks, including tumor progression, treatment-related toxicity, and delays in surgical intervention3,4 Therefore, accurately identifying patients who are most likely to benefit from NAT before treatment initiation remains a critical challenge for maximizing therapeutic efficacy while minimizing associated risks.
Currently, clinical decision-making largely relies on conventional clinicopathological characteristics, such as estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor 2 (HER2), and Ki-67 expression. Nevertheless, the predictive accuracy of existing models remains suboptimal, resulting in a subset of patients being exposed to unnecessary treatment. This underscores the urgent clinical need to identify novel and more effective predictive biomarkers.
The tumor immune microenvironment, particularly tumor-infiltrating lymphocytes (TILs), plays a crucial role in modulating therapeutic response. Among these immune components, CD8+ T lymphocytes, as cytotoxic T cells, are key effectors of antitumor immunity. They exert direct antitumor activity through the release of perforin, granzymes, and proinflammatory cytokines. However, previous studies investigating the predictive value of CD8+ TILs in the context of NAT have yielded inconsistent and sometimes contradictory results4–11 A critical factor contributing to these discrepancies may be the spatial heterogeneity of CD8+ TILs within tumor tissue. Most prior studies have evaluated total TILs without spatial distinction or have focused predominantly on stromal TILs. In contrast, CD8+ T cells that infiltrate tumor nests and directly interact with tumor cells (intratumoral CD8+ TILs) may exhibit distinct functional states and clinical relevance compared with those residing in the tumor stroma. To date, evidence specifically addressing this intratumoral CD8+ TIL subset remains limited, and whether it represents a superior predictive biomarker has yet to be clarified.
Hence, to reconcile inconsistencies in previous reports and to explore biomarkers with enhanced predictive potential, the present study aimed to precisely distinguish and quantitatively assess intratumoral and stromal CD8+ TILs. We systematically investigated their associations with clinical response (cCR) and pathological response (pCR) to neoadjuvant therapy in breast cancer, with the goal of providing a theoretical foundation for the development of more accurate predictive models for treatment efficacy.
Methods
Study Population
We conducted a retrospective analysis of all breast cancer patients who received neoadjuvant therapy at the People’s Hospital of Guangxi Zhuang Autonomous Region between January 2017 and June 2019. The study protocol was approved by the Ethics Committee of the People’s Hospital of Guangxi Zhuang Autonomous Region (approval number: NO.KY-IIT-2021-20) and complies with the Declaration of Helsinki. The informed consent was waived by the committee due to the retrospective design of the study and the use of anonymized clinical data. Collected clinical and pathological variables included patient age, menstrual history, tumor size, lymph node status, histological grade, hormone receptor status, HER2 status, and Ki-67 expression (Supplementary S3).
Patients with HER2-negative breast cancer received neoadjuvant chemotherapy comprising taxanes, anthracyclines, and cyclophosphamide. Those with HER2-positive tumors were treated with anthracyclines and cyclophosphamide followed by sequential taxanes and trastuzumab-based targeted therapy. Following NAT treatment, all patients underwent either modified radical mastectomy or breast-conserving surgery with axillary lymph node dissection.
Exclusion criteria included inflammatory breast cancer, multiple malignancies, acute or chronic injuries, active inflammatory conditions, hematological disorders, liver cirrhosis, or end-stage renal disease. Based on these criteria, a total of 94 patients were included in the analysis (Figure 1). All treatment regimens were designed in accordance with the 2019 CSCO Breast Cancer Guidelines.
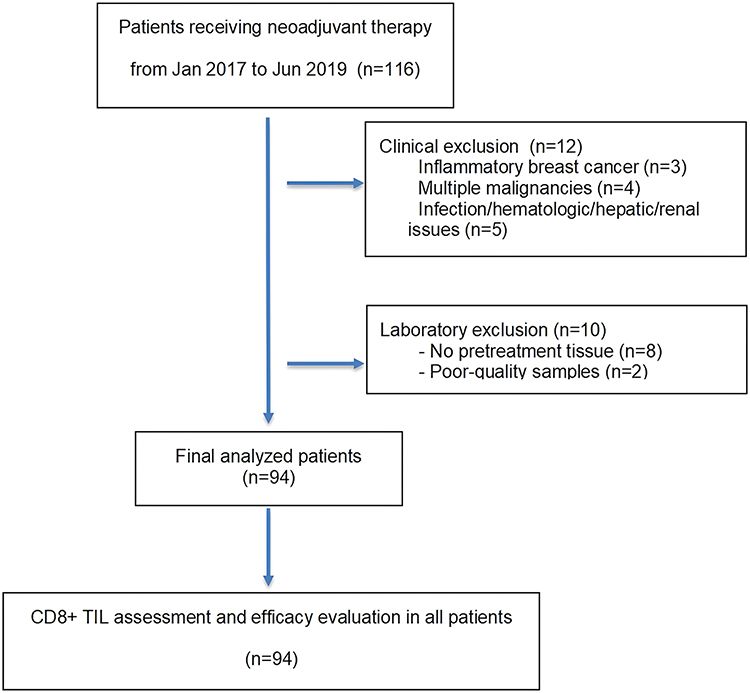 |
Figure 1 Flowchart of patient selection. Abbreviation: CD8+ TIL, CD8-positive tumor-infiltrating lymphocyte. |
Pathological Characteristics
Histological grading was conducted according to the “Histological Grading of Breast Cancer (Modified Scarff-Bloom-Richardson Grading System)” and classified into grades G1-G3. Estrogen receptor (ER) and progesterone receptor (PR) positivity thresholds were set at ≥1% based on immunohistochemical (IHC) evaluation. HER2 positivity was defined as IHC 3+, while cases with IHC 2+ required further assessment of expression status using fluorescence in situ hybridization (FISH) to determine gene amplification. HER2 status was classified as positive if FISH amplification was observed, whereas IHC 1+ was considered HER2 negative. Ki-67 expression levels were categorized as low (<15%), intermediate (15%-30%), or high (>30%). For cases with intermediate Ki-67 levels, additional pathological consultation was conducted for confirmation.The clinical efficacy of NAT was assessed using breast mammography or MRI imaging following the RECIST 1.1 Criteria for Evaluating Solid Tumor Response. Clinical complete remission (cCR) was defined as the disappearance of all detectable breast cancer lesions, with the short axis of all pathological lymph nodes measuring <10mm and tumor markers within normal range. Pathological complete remission (pCR) was evaluated in accordance with the CSCO Breast Cancer Diagnosis and Treatment Guidelines, pCR was defined as the absence of histological evidence of malignancy carcinoma in both the primary breast lesion and regional lymph nodes, or the presence of only in situ carcinoma components.
Detection and Evaluation of CD8+ TILs
The expression of CD8+ TILs in baseline and preoperative primary tumor tissues was evaluated using immunohistochemistry (IHC). The CD8 rabbit anti-human polyclonal antibodies and secondary antibodies were sourced from Beijing Zhongshan Golden Bridge Biotechnology Co., Ltd., and the immunohistochemistry staining kit was procured from Fuzhou Maixin Biotechnology Development Co., Ltd. Formalin-fixed, paraffin-embedded tissue sections were prepared according to standard procedures, including sectioning, deparaffinization, and rehydration. Endogenous peroxidase activity was blocked with 3% hydrogen peroxide, followed by nonspecific protein blocking with 2% bovine serum albumin (BSA) for 10 minutes. The sections were incubated with the primary anti-CD8 antibody (1:200 dilution) overnight at 4 °C and subsequently incubated with the secondary antibody (1:1000 dilution) at 37 °C for 30 minutes. Immunoreactivity was visualized using diaminobenzidine (DAB) chromogen, followed by hematoxylin counterstaining, routine dehydration, and mounting.
For each staining run, both positive and negative controls were included. Tonsillar tissue sections with known CD8 positivity served as positive controls, whereas phosphate-buffered saline (PBS) was used in place of the primary antibody as negative controls. Only staining runs in which control results met predefined expectations were considered valid for subsequent analysis. Based on spatial distribution, CD8+ TILs were classified as intratumoral or stromal. Intratumoral CD8+ TILs were defined as lymphocytes strictly located within tumor cell nests, whereas stromal CD8+ TILs were defined as lymphocytes located within the fibrous connective tissue between tumor cell nests, excluding normal breast stroma beyond the invasive tumor front.12
Quantitative evaluation was performed by manual counting under high-power magnification (×400). When CD8+ TILs were evenly distributed, three representative tumor “hotspot” areas were randomly selected, and the mean CD8+ TIL count within and surrounding the tumor was calculated. In cases of heterogeneous distribution, the fields with the highest and lowest CD8+ TIL densities were excluded, and the mean value was calculated from three randomly selected high-power fields.10
All immunohistochemical evaluations were independently performed by two experienced pathologists who were blinded to the patients’ clinical information. If the discrepancy between the two observers exceeded 20%, the slides were jointly reviewed to reach a consensus. The final CD8+ TIL count was calculated as the average of the mean values obtained by the two pathologists.
Patients were subsequently stratified into low- and high-infiltration groups according to the median CD8+ TIL count, with values ≤ median defined as low infiltration and values > median defined as high infiltration.9
Statistical Analysis
Statistical analyses were conducted using SPSS version 24.0. Continuous variables were presented as mean±standard deviation (SD) and compared between groups using the Mann–Whitney U-test. Categorical variables were expressed as frequencies and percentages, with group comparisons performed using the chi-square test or Fisher’s exact test, as appropriate. To identify factors predictive of cCR and pCR in breast cancer patients undergoing neoadjuvant therapy, univariate and multivariate logistic regression models were applied. All statistical tests were two-sided, with a p-value of <0.05 considered indicative of statistical significance.
For multivariate logistic regression analyses of cCR and pCR, variables were selected based on their significance in univariate analyses. Only variables showing statistical significance in univariate analyses (p < 0.05) were considered. This approach ensured that only variables with potential predictive relevance were considered.
Results
Distribution and Expression of CD8+ TILs
CD8+ TILs were identified via immunohistochemistry, with positive CD8 staining observed in the cytoplasm and cell membrane. A diffuse distribution pattern was observed for CD8+ TILs in both intratumoral and stromal regions, with stromal CD8+ TILs exhibiting higher abundance compared to their intratumoral counterparts (Figure 2).
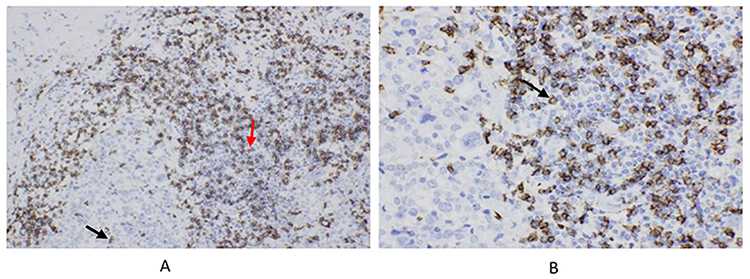 |
Figure 2 Immunohistochemistry slides of CD8+ TILs. (A) Baseline CD8+ TILs under ×200 magnification. Black arrows indicate iCD8+ TILs, and red arrows indicate sCD8+ TILs. Both intratumoral and stromal CD8+ TILs are diffusely distributed, with sCD8+ TILs being more abundant than iCD8+ TILs. (B) Baseline CD8+ TILs under ×400 magnification, showing positive staining of the cell membrane and cytoplasm (indicated by arrows). |
CD8+ TILs and Clinicopathological Characteristics
The Chi-square test revealed significant associations between intratumoral CD8+ TIL infiltration and age, menstrual status, estrogen receptor (ER) status, progesterone receptor (PR) status and molecular subtype (p < 0.05). However, no significant associations were observed between intratumoral CD8+ TIL infiltration and T stage, axillary lymph node status, HER2 status, or Ki-67 index (p>0.05). Additionally, stromal CD8+ TIL infiltration showed no significant correlations with any clinicopathological features (p>0.05). The detailed relationship between baseline CD8+ TILs and clinicopathological characteristics is presented in Table 1.
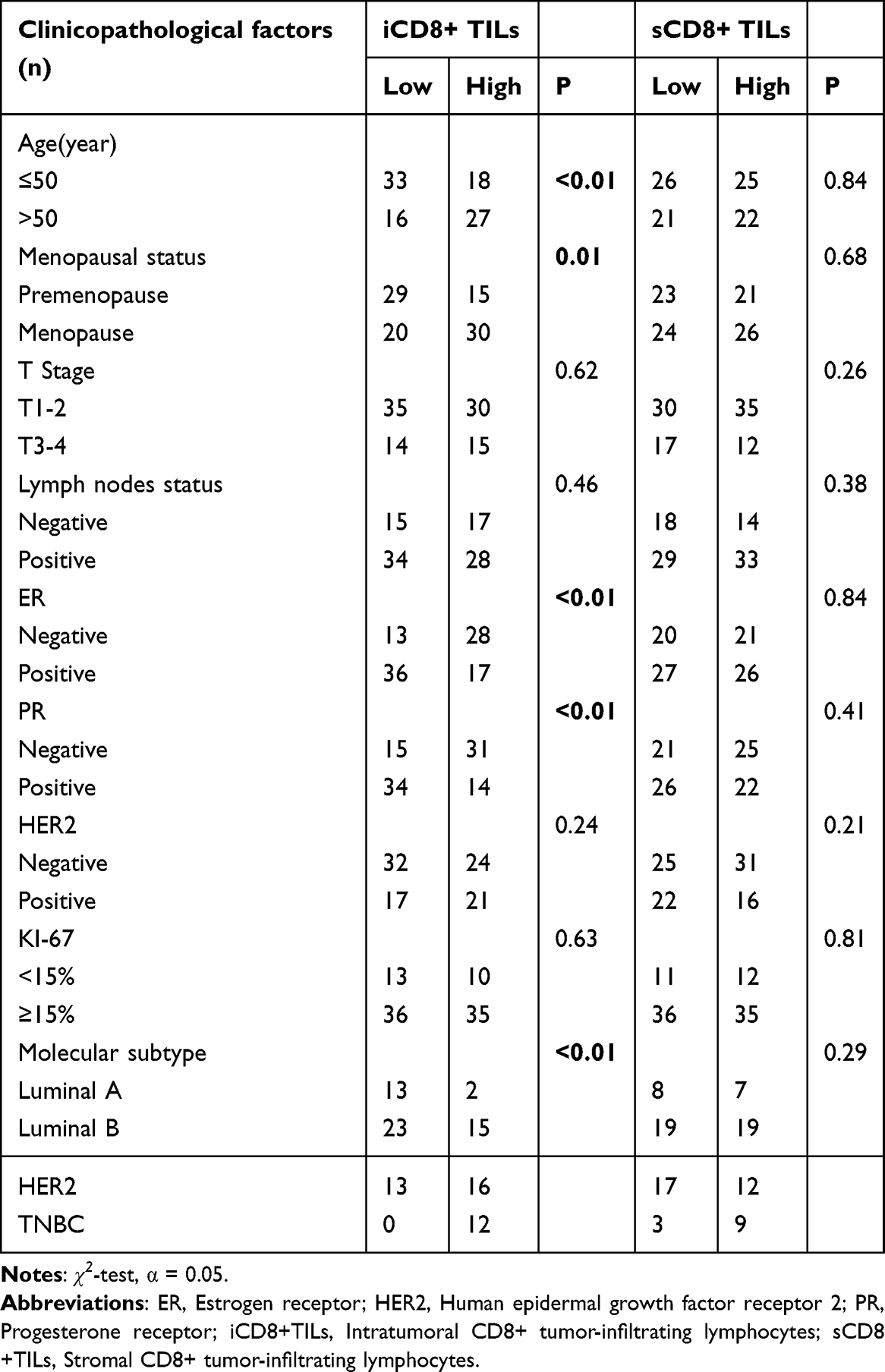 |
Table 1 Baseline CD8+ TIL Expression and Clinicopathological Characteristics |
CD8+ TILs and Clinical Response to Treatment
After neoadjuvant therapy, 30 patients were evaluated as having achieved a clinical complete response (cCR). The Mann–Whitney U-test was performed to evaluate the differences in CD8+ TILs expression between cCR and non-cCR patients. The analysis revealed no statistically significant differences in the expression levels of intratumoral or stromal CD8+ TILs between the two groups (p > 0.05, Supplementary S1 and S2). However, univariate logistic regression analysis identified T stage, axillary lymph node status, and intratumoral CD8+ TILs as factors associated with cCR. Multivariate logistic regression analysis, which included T stage, axillary lymph node status, and intratumoral CD8+ TILs, confirmed intratumoral CD8+ TILs as an independent predictor of cCR (OR 3.038; p = 0.02, Table 2). This apparent discrepancy may be attributable to the fact that the association between intratumoral CD8+ TILs and cCR does not represent a simple distributional shift that can be optimally captured by a non-parametric group comparison, whereas logistic regression may have greater statistical power to detect weaker or non-linear predictive effects.
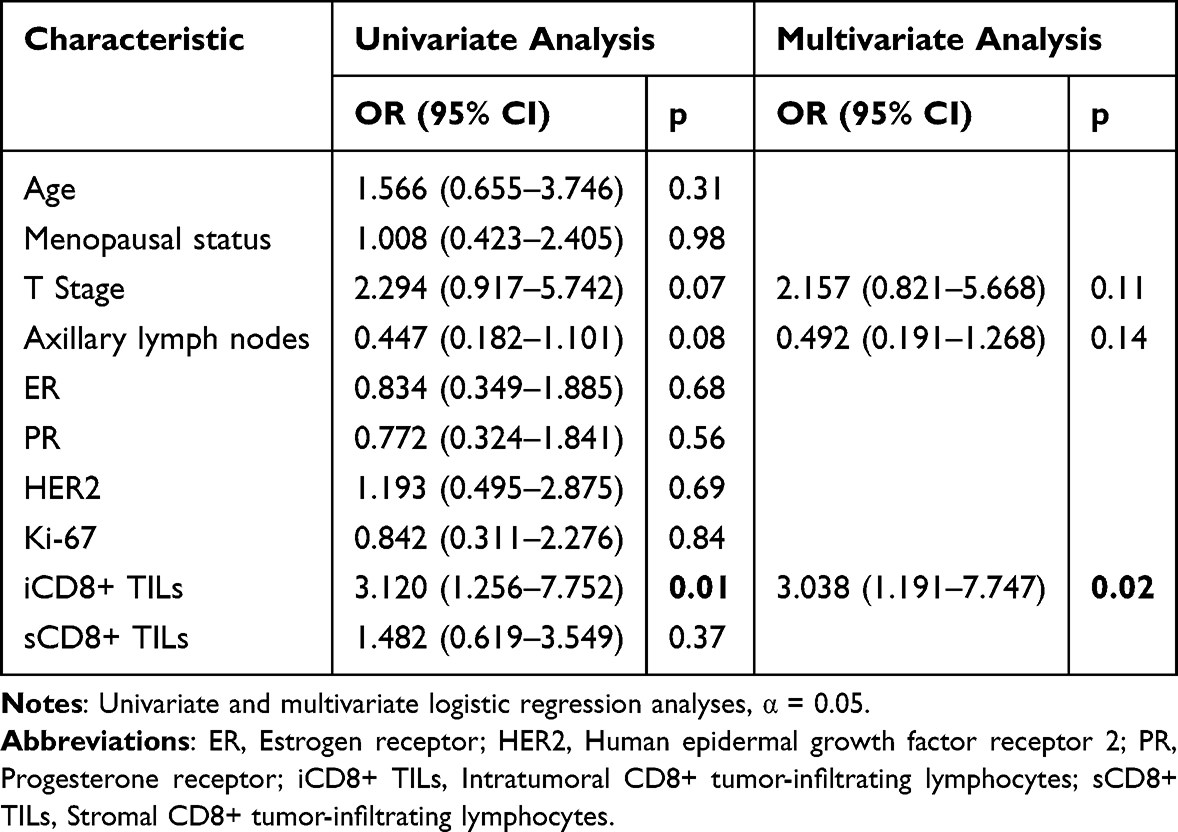 |
Table 2 Univariate and Multivariate Logistic Regression Analysis of Clinical Efficacy |
CD8+ TILs and Pathological Response
A total of 22 patients achieved pathological complete response (pCR) following neoadjuvant therapy. The Mann–Whitney U-test revealed a significant difference in intratumoral CD8+ TILs between patients achieving pCR and those without (p = 0.04, Figure 3). Univariate logistic regression analysis indicated that ER, PR, HER2 status, and intratumoral CD8+ TILs were associated with pCR. While stromal CD8+ TILs did not reach statistical significance in univariate analysis (p = 0.15, Table 3), were not included in the multivariate models.
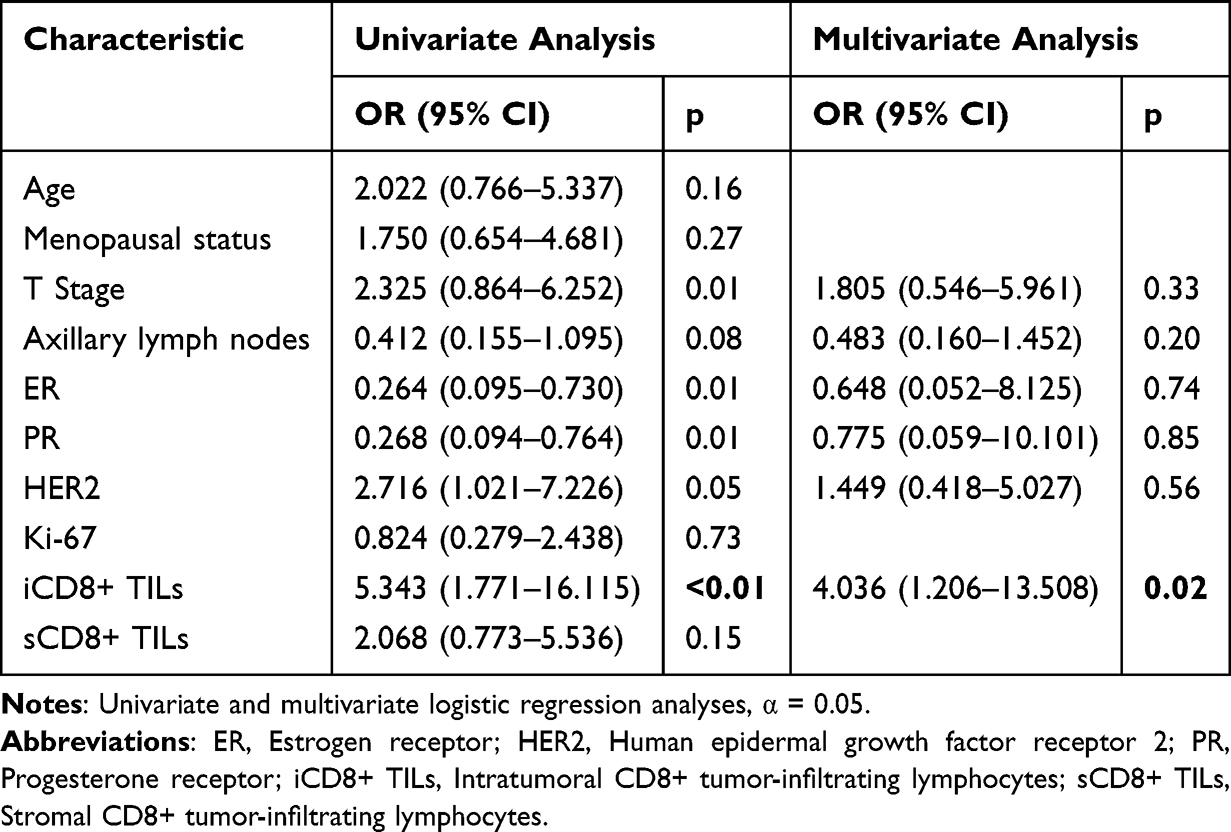 |
Table 3 Univariate and Multivariate Logistic Regression Analysis of Pathological Response |
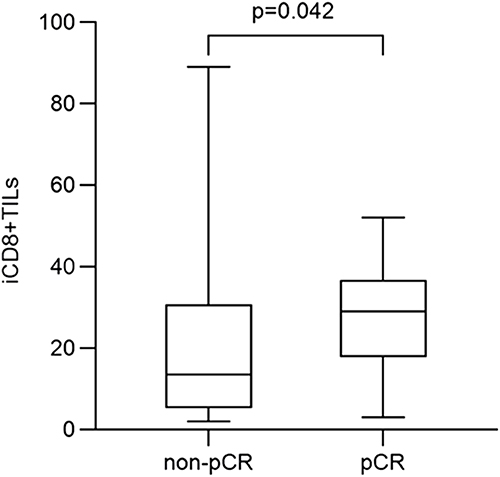 |
Figure 3 Differential expression of iCD8+ TILs. Abbreviations: iCD8+ TILs, Intratumoral CD8+ tumor-infiltrating lymphocytes; pCR, Pathological complete remission. |
Multivariate logistic regression analysis, adjusted for T stage, axillary lymph node status, ER, PR, HER2 status, and intratumoral CD8+ TILs, demonstrated that intratumoral CD8+ TILs were an independent predictor of pCR (OR = 4.036; p = 0.02, Table 3).
Discussion
NAT has become the standard of care for early high-risk and locally advanced breast cancer. NAT not only downstages tumors to facilitate breast-conserving surgery and optimize surgical outcomes, but also informs subsequent precision treatments based on therapeutic responses. The clinical efficacy of NAT plays a critical role in determining the timing of surgical intervention, with pathological complete response (pCR) being closely linked to long-term prognosis.2,3 Although advances such as dual HER2 blockade and antibody-drug conjugates have significantly improved pCR rates, some patients fail to derive clinical benefit, highlighting the urgent need to identify patients who are most likely to benefit while minimizing treatment-related toxicity and cost. TILs have emerged as promising predictive biomarkers. Among TILs, CD8+ TILs play a pivotal role in anti-tumor immunity, but their clinical utility for guiding NAT remains to be fully elucidated.13 This study investigates the association between CD8+ TILs and NAT efficacy, aiming to provide insights to guide clinical decision-making.
Despite progress, limited research has explored the spatial distribution of CD8+ TILs and their impact on NAT outcomes in breast cancer. Prior studies have yielded inconsistent findings. For instance, Previous research by Mao et al. Mao6 and Liu14 et al reported no significant correlation between stromal CD8+ TILs and pCR (p > 0.05). This aligns with our findings, which suggest that stromal CD8+TILs have limited predictive value.While De et al4 similarly found no correlation between intratumoral or stromal CD8+ TILs and pCR (p > 0.05). In contrast, Viriya et al15 demonstrated that high levels of both intratumoral (p = 0.008) and stromal CD8+ TILs (p = 0.002) were associated with increased pCR rates. These discrepancies may arise from differences in study populations, molecular subtype distribution, therapeutic regimens, immunohistochemical protocols, and TIL scoring criteria. Importantly, our study emphasizes the importance of intratumoral CD8+ TILs, which were shown to have a more consistent association with therapeutic outcomes than their stromal counterparts (p = 0.042), likely due to their direct cytotoxic interaction with tumor cells.
Our findings align with those of Viriya et al,14 showing that intratumoral CD8+ TILs significantly differed between pCR and non-pCR patients (p = 0.042). Univariate analysis revealed a strong correlation between intratumoral CD8+ TILs and pCR (OR = 5.34; 95% CI: 1.771–16.115; p < 0.01), and multivariate analysis confirmed intratumoral CD8+ TILs as an independent predictor of pCR (OR = 4.036; 95% CI: 1.206–13.508; p = 0.02). Additionally, our study found that intratumoral CD8+ TILs were also an independent predictor of cCR (OR = 3.038; 95% CI: 1.191–7.747; p = 0.02). These results suggest that patients with high intratumoral CD8+ TILs expression are more likely to achieve both cCR and pCR, underscoring the potential of combining CD8+ TILs with other predictive markers to more effectively identify candidates likely to benefit from NAT and inform clinical decision-making.13–15 By focusing on CD8+ T lymphocytes, and performing a refined evaluation based on their spatial distribution (intratumoral versus stromal), quantitative assessment of intratumoral CD8+ TILs in pretreatment biopsy specimens offer a novel perspective for addressing the longstanding discordance between radiologic or clinical response and pathological outcomes.14
Moreover, Sener et al16 reported inconsistencies between clinical and pathological responses to NAT in breast cancer, a finding corroborated by our study. This raises the clinical dilemma of whether to extend NAT to achieve pCR when clinical response suggests surgical feasibility. While achieving cCR may guide surgical decisions, it does not always correlate with pCR, which is a robust prognostic indicator.2,3 Theoretically, for patients in whom clinical efficacy reliably predicts pathological response, extending NAT not only could mitigate risks, while potentially increasing pCR rates, thereby enhancing survival benefits. In this context, intratumoral CD8+TILs have emerged as potential dual predictor of both cCR and pCR, offering a promising tool to address this discordance. For patients with low intratumoral CD8+ TILs despite achieving cCR, there may be residual disease risk warranting more aggressive surgical or adjuvant intervention. Conversely, high intratumoral CD8+ TILs in patients who do not achieve cCR may indicate ongoing effective intratumoral immune activity, suggesting potential benefit from extended NAT to maximize pCR.
The tumor immune microenvironment is highly complex. CD8+ T-cell activity is modulated by immunosuppressive populations (eg, regulatory T cells), immune checkpoint molecules (eg, PD-L1), tumor mutational burden, and T-cell receptor diversity. Future studies should evaluate multiparametric immune scoring systems integrating intratumoral CD8+ TILs with these additional biomarkers to enhance predictive accuracy and identify patients most likely to benefit from NAT, including strategies combining immune checkpoint inhibitors with chemotherapy.
This study has several limitations, including its retrospective single-center design, relatively small sample size, lack of stratification by molecular subtype, and absence of long-term survival data. Consequently, the prognostic value of CD8+ TILs beyond NAT response remains to be validated. Future prospective, multicenter studies with survival follow-up are warranted to investigate associations between intratumoral CD8+ TILs, disease-free survival (DFS), and overall survival (OS), thereby establishing their role in comprehensive breast cancer management.
Conclusion
Intratumoral CD8+ TILs were significantly associated with both clinical complete response and pathological complete response in breast cancer patients receiving neoadjuvant therapy. These findings suggest that intratumoral CD8+ TILs may serve as a potential predictive biomarker for treatment response. However, given the retrospective design and limited sample size of this study, further prospective investigations incorporating additional immune biomarkers and long-term survival outcomes are required to validate their clinical utility.
Acknowledgments
We sincerely appreciate the support from the Ethical Review Committee of The People’s Hospital of Guangxi Zhuang Autonomous Region for approving this study. We also thank the medical staff at department of pathology for their assistance in pathological examination and analysis.
Disclosure
All authors declare no conflicts of interest in this work.
References
1. Chen W, Sun K, Zheng R, et al. Cancer incidence and mortality in China, 2014. Chin J Cancer Res. 2018;30(1):1–9. doi:10.21147/j.issn.1000-9604.2018.01.01
2. Cain H, Macpherson IR, Beresford M, Pinder SE, Pong J, Dixon JM. Neoadjuvant therapy in early breast cancer: treatment considerations and common debates in practice. Clin Oncol. 2017;29(10):642–652. doi:10.1016/j.clon.2017.06.003
3. Caudle AS, Gonzalez-Angulo AM, Hunt KK, et al. Impact of progression during neoadjuvant chemotherapy on surgical management of breast cancer. Ann Surg Oncol. 2011;18(4):932–938. doi:10.1245/s10434-010-1390-8
4. De Angelis C, Nagi C, Hoyt CC, et al. Evaluation of the predictive role of tumor immune infiltrate in patients with HER2-positive breast cancer treated with neoadjuvant anti-HER2 therapy without chemotherapy. Clin Cancer Res. 2020;26(3):738–745. doi:10.1158/1078-0432.Ccr-19-1402
5. Çetin K, Kökten Ş, Sarıkamış B, et al. The association of PD-L1 expression and CD8-positive T cell infiltration rate with the pathological complete response after neoadjuvant treatment in HER2-positive breast cancer. Breast Cancer Res Treat. 2024;205:17–27. doi:10.1007/s10549-023-07242-1
6. Mao Y, Qu Q, Chen X, Huang O, Wu J, Shen K. The prognostic value of tumor-infiltrating lymphocytes in breast cancer: a systematic review and meta-analysis. PLoS One. 2016;11(4):e0152500. doi:10.1371/journal.pone.0152500
7. Song IH, Heo SH, Bang WS, et al. Predictive value of tertiary lymphoid structures assessed by high endothelial venule counts in the neoadjuvant setting of triple-negative breast cancer. Cancer Res Treat. 2017;49(2):399–407. doi:10.4143/crt.2016.215
8. Zhao J, Meisel J, Guo Y, et al. Evaluation of PD-L1, tumor-infiltrating lymphocytes, and CD8+ and FOXP3+ immune cells in HER2-positive breast cancer treated with neoadjuvant therapies. Breast Cancer Res Treat. 2020;183(3):599–606. doi:10.1007/s10549-020-05819-8
9. Castaneda CA, Mittendorf E, Casavilca S, et al. Tumor infiltrating lymphocytes in triple negative breast cancer receiving neoadjuvant chemotherapy. World J Clin Oncol. 2016;7(5):387–394. doi:10.5306/wjco.v7.i5.387
10. Lee HJ, Seo JY, Ahn JH, Ahn SH, Gong G. Tumor-associated lymphocytes predict response to neoadjuvant chemotherapy in breast cancer patients. J Breast Cancer. 2013;16(1):32–39. doi:10.4048/jbc.2013.16.1.32
11. Liang H, Huang J, Li H, et al. Spatial proximity of CD8+ T cells to tumor cells predicts neoadjuvant therapy efficacy in breast cancer. NPJ Breast Cancer. 2025;11(1):13. doi:10.1038/s41523-025-00728-9
12. Salgado R, Denkert C, Demaria S, et al. The evaluation of tumor-infiltrating lymphocytes (TILs) in breast cancer: recommendations by an International TILs Working Group 2014. Ann Oncol. 2015;26(2):259–271. doi:10.1093/annonc/mdu450
13. Carbognin L, Pilotto S, Nortilli R, et al. Predictive and prognostic role of tumor-infiltrating lymphocytes for early breast cancer according to disease subtypes: sensitivity analysis of randomized trials in adjuvant and neoadjuvant setting. Oncologist. 2016;21(3):283–291. doi:10.1634/theoncologist.2015-0307
14. Liu J, Xu Y, Yu M, et al. Increased stromal infiltrating lymphocytes are associated with circulating tumor cells and metastatic relapse in breast cancer patients after neoadjuvant chemotherapy. Cancer Manag Res. 2019;11:10791–10800. doi:10.2147/cmar.S220327
15. Kaewkangsadan V, Verma C, Eremin JM, Cowley G, Ilyas M, Eremin O. Crucial contributions by T lymphocytes (effector, regulatory, and checkpoint inhibitor) and cytokines (TH1, TH2, and TH17) to a pathological complete response induced by neoadjuvant chemotherapy in women with breast cancer. J Immunol Res. 2016;2016:4757405. doi:10.1155/2016/4757405
16. Sener SF, Sargent RE, Lee C, et al. MRI does not predict pathologic complete response after neoadjuvant chemotherapy for breast cancer. J Surg Oncol. 2019;120(6):903–910. doi:10.1002/jso.25663
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Pretreatment System Inflammation Response Index (SIRI) is a Valuable Marker for Evaluating the Efficacy of Neoadjuvant Therapy in Breast Cancer Patients
Zhang Y, Wu J, Chen W, Liang X
International Journal of General Medicine 2024, 17:4359-4368
Published Date: 25 September 2024
Peripheral TNF-α and CD8+/CD28+ T Lymphocytes as Alternatives for PD-L1 Prediction in Breast Cancer Tumor Microenvironment: Stratified by Neoadjuvant Therapy
Wu J, Ou X, Yuan K, Shi F, Zhou Q, Lyu S, Li Y, Zhao Y, Cao Y, Sun J, Song Q
Breast Cancer: Targets and Therapy 2025, 17:627-637
Published Date: 19 July 2025
Deep Learning Radiomics of Multiparametric MRI for Individualized Prediction of Axillary Lymph Node Response After Neoadjuvant Chemotherapy in Breast Cancer
Li S, Li R, Xu M, Liao J, Cao Z, Gong B, Yan F, Wang M, Tan H
Breast Cancer: Targets and Therapy 2026, 18:568337
Published Date: 21 January 2026
Efficacy and Safety of Neoadjuvant Stereotactic Body Radiotherapy (SBRT) Combined with Chemoimmunotherapy in Locally Advanced Breast Cancer: A Single-Center, Retrospective Pilot Study
Zhai M, Bi J, Ke Z, Hu M, Pi G, Li Y, He H, Li Y, Zheng H, Wu X, Verma V, Shao J, Han G
Breast Cancer: Targets and Therapy 2026, 18:577469
Published Date: 7 March 2026
Inflammatory and Nutritional Biomarkers Predict Response to Neoadjuvant Dual Anti-HER2 Therapy in HER2-Positive Breast Cancer: A Retrospective Cohort Study
Şahinli H, Uyar GC, Yeşilbaş E
Cancer Management and Research 2026, 18:598948
Published Date: 16 April 2026